
4
Measuring Children’s Health
This chapter outlines the nature of existing data in light of the committee’s conceptualization of children’s health. It begins with an overview of the available data and outlines two types of gaps in current data collection that need to be filled in order to make them more useful: gaps in the conceptualization of health and gaps in measurement. The chapter closes with a discussion of approaches to filling these gaps and an outline of new ways of approaching the concept and measurement of children’s health.
CURRENT APPROACHES
As noted in Chapter 2, children’s health has traditionally been assessed by evaluating indices that include the proportion of newborns born small or too early, infant mortality rates, disease-specific incidence and mortality rates, and proxy-reported ratings of health or activity limitations. Available data come from several sources: vital statistics, surveys, and clinical and administrative datasets (U.S. Department of Health and Human Services, 1981).
Vital statistics are part of a standardized state and national system for reporting data on births and deaths. They provide information on births and on rates and causes of death in childhood and adulthood. These systems have been ongoing for more than a century and, while there are a variety of new challenges that arise in the interpretation and use of these data, they are well recognized as important both within countries as well as for international comparisons. In the United States they are used to calculate rates of birthweights, identify birth defects, and track rates and causes of death. An annual compilation of the trends in
these data is published (see MacDorman et al., 2002). Another source of standardized reporting of data is the mandated reporting of communicable diseases, which is required of all health care providers and laboratories, to state health departments and, ultimately, the Centers for Disease Control and Prevention (CDC). This system is used to track major infectious diseases and their state and national trends. Outbreaks involving children and patterns of sexually transmitted diseases among adolescents are regularly monitored. In addition, the Maternal and Child Health Bureau (MCHB) has established 6 standard outcome measures that are reported for all states, as well as 18 performance measures.1
Survey data have the advantage of providing national estimates of self-reported or, more usually in the case of children, proxy-reported conditions in childhood. The United States collects a great deal of survey data about children, but few surveys are specifically designed to focus on measuring children’s health. For many decades the measurement of children’s health at the national and state levels has been included in measurement systems that have focused primarily on measuring adult health. This is particularly ironic since the current national system of health statistics had its origins at the early 1900s with assessment of the health of women and the birth of their children (Hutchins, 1997) yet has evolved to focus on adults. The preoccupation of the health care system during the latter part of the 20th century with the prevalence, impact, and cost of chronic diseases in adults and the elderly led to a predominant focus on specific chronic diseases. This focus on chronic disease, along with a long preoccupation with health care costs, has centered national health data collection on their prevalence, the utilization of services for managing them, and the current health expenditures associated with them. In many disease-oriented surveys, children appear to be healthy because of their low prevalence of chronic disorders commonly diagnosed in adults. This orientation and the relatively low price tag for the delivery of child health services have led to an incomplete understanding of children’s health (Schlesinger and Eisenberg, 1990). Until recently, there were only a few special one-time or periodic supplements, such as the Child Health Supplements to the National Health Interview Survey (NHIS) in 1981 and 1988 that focused on children’s health.
National Child Health Data Collection Efforts
Many federal agencies are now involved in collecting regular and periodic health information about children (see Box 4-1). The National Center for Health Statistics (NCHS), which is a part of the CDC, has several ongoing surveys that concern the health and health care use of children in the United States (Brown,
|
1 |
For additional information, see http//www.ahcpr.gov/chtoolbx/measure5.htm and https://performance.hrsa.gov/mchb/mchreports/Search/core/cormenu.asp. |
2001), including the National Immunization Survey, a telephone survey that collects vaccination data on children between 19 and 35 months. Most major ongoing national data collection efforts also continue to include children in general population surveys. This is true of the annual NHIS and the National Health and Nutrition Examination Survey (NHANES), as well as other special surveys that NCHS supports or administers from time to time. NCHS collaborates with the Agency for Healthcare Research and Quality (AHRQ) to conduct the Medical
|
BOX 4-1 DEPARTMENT OF HEALTH AND HUMAN SERVICES Centers for Disease Control and Prevention/National Center for Health Statistics
Center for Disease Control and Prevention/National Center for Chronic Disease Prevention and Health Promotion
Maternal and Child Health Bureau/Health Resources and Services Administration
Agency for Healthcare Research and Quality
National Institute of Child Health and Human Development
DEPARTMENT OF EDUCATION National Center for Education Statistics (NCES)
DEPARTMENT OF LABOR
NOTE: See Appendix A for a brief description of each of these data sources and the relevant web link and Appendix B for an outline of the data elements corresponding to the health conditions, functioning, and health potential domains for 12 of the current surveys. |
Expenditure Panel Surveys, which also include data on various aspects of children’s health (as reported by proxies, usually parents). Other nationally representative data are collected directly from adolescents through the Youth Risk Behavior Survey (YRBS) conducted by the CDC and the National Household Survey of Drug Use and Health, conducted by the Substance Abuse and Mental Health Services Administration for persons 12 years and older.
A fairly recent addition to the portfolio of the NCHS is the State and Local Area Integrated Telephone Survey (SLAITS), which uses the same design approach and sampling frame as the ongoing National Immunization Survey. SLAITS is a survey platform designed to collect state- and local-level health care data. It can be used by other federal, state, or local government agencies or private organizations to conduct additional data collection by purchasing use of the platform and time for other surveys. It has been used by other federal and state government agencies as the vehicle for several new surveys for children and has produced a great deal of additional information in a fairly short time frame. This mechanism of using telephone interviews of parents has recently been providing important national and state-level estimates of children’s health from families that have access to telephones in their homes.
The MCHB of the Health Resources and Services Administration, which has its administrative roots in the Children’s Bureau established in 1912 (Hutchins, 1997), has been a historically consistent federal advocate for the measurement of children’s health. The MCHB has recently used the SLAITS mechanism to conduct three surveys that expand national and state-level data on the health of children. In 2000, MCHB used SLAITS to conduct the largest survey to date on the health of children who have special health care needs (van Dyck et al., 2002). It is the first national survey that was designed to allow state-level estimates, in addition to national estimates, of all measures, including the number of children with special health care needs. The goal, contingent on adequate future funding, is to administer it periodically to generate trend and performance evaluation information.
Also in 2000 the MCHB, along with NCHS, CDC, and the American Academy of Pediatrics, sponsored the National Survey of Early Childhood Health (NSECH) using the SLAITS platform to assess the health of children ages 4 to 35 months, the content and quality of well-child health care, and steps parents can take to promote the health and development of their young children.2 It was a one-time pilot survey conducted with 2,068 families nationwide (National Center for Health Statistics, 2002b).
More recently, the MCHB sponsored another survey using the SLAITS plat-
form, the National Survey of Children’s Health (NSCH). NSCH is designed to assess the physical and emotional health of children from birth through age 17 and, like the National Survey of Children with Special Health Care Needs will provide state-level as well as national estimates.
Another child health module that has been added to the SLAITS platform is the Child Well-Being and Welfare module, although to date it has been used by only two states, Texas and Minnesota. The National Center for Environmental Health in CDC is using the SLAITS platform to obtain national and select state-level data on predictors of asthma. Although not focused on children, the survey includes them.
Although all of the national surveys aim to obtain representative national samples, survey methodology has some inherent weaknesses. These include the inevitability of some response bias (such as the inability of the SLAITS platform to obtain information about families without telephones in their homes or of household interviews to obtain data on the homeless), issues about whether or not the interviews are conducted in multiple languages, and of cultural validation of questions across groups. In addition, since each minute of questions on large-scale surveys is extremely costly, there is always pressure to ensure that the time is used efficiently. This often leads to many areas being assessed superficially (and in some cases tailored to adults) and to a distinct preference against the inclusion of standardized psychometrically validated instruments, which contain multiple questions, to measure complicated constructs.
One notable exception to the lack of inclusion of psychometrically validated measures has been in the area of child mental health, for which behavioral inventories have been included in the Child Health Supplements in 1981 and 1988. However, overall there has been a paucity of measurement and monitoring of child and adolescent mental health, despite the fact that this is a major cause of morbidity.
In addition to the surveys mentioned above, other agencies, such as the National Institutes of Health, often fund or themselves mount national surveys, such as the National Longitudinal Survey of Adolescent Health (called ADD-Health). For the most part, these are investigator-initiated efforts. They often break new ground in measuring influences or implementing new methods, or provide detailed information about particular aspects of children’s health. For example, ADD-Health provides valuable data on a range of adolescent health influences, including peers; the Fragile Families and Child Well-being Study provides the first national look at the influence of father involvement among low-income, unmarried, first-time parents and a married comparison group3 (although the early waves of this study are not concentrated on health); and linkage of geocoded
|
3 |
For additional information, see http://crcw.princeton.edu/fragilefamilies/index.asp. |
survey data with census data was advanced by investigator-initiated efforts. Investigator-initiated surveys do not always take advantage of advances in government-mounted surveys, nor are government-mounted surveys quick to adopt the advances from investigator-initiated efforts. Coordination and linkage of surveys, as well as sharing of knowledge regarding survey methodology, should be improved across both government and investigator-initiated surveys. The federally sponsored Developing a Daddy Survey (DADS) initiative may have relevant lessons for such coordination efforts. DADS is a public-private effort to better understand fatherhood and father involvement in children’s lives by adding questions to several national surveys.
The National Institute of Child Health and Human Development is leading an effort to develop the National Children’s Study, a longitudinal study designed to examine the effects and interactions of a broad range of environmental influences on children’s health (including traditional factors, such as chemical, physical, and biological factors, as well as other factors, such as family structure and economics, neighborhood factors, and local and state policy). As envisioned, the study will follow 100,000 children from before birth through age 21. A wide range of individuals, researchers, organizations, and federal agencies have been involved in the planning and design of the study. During the course of the committee’s deliberations, the exact specifications of the study were not clear, and funding had not been secured.4
The National Center for Educational Statistics (NCES) has several noteworthy national surveys of children’s well-being. The birth cohort of the Early Childhood Longitudinal Study (ECLS-B) is in the process of gathering data on children’s health, development, care, and education from birth through 1st grade from a sample of 10,600 children born in 2001. The Early Childhood Longitudinal Study, Kindergarten Class of 1998–1999 (ECLS-K) focuses on children’s early school experiences, beginning with kindergarten and following children through 5th grade. Its sample is also nationally representative and numbers just under 20,000. The National Household Education Surveys program provides descriptive data on the educational activities of the U.S. population, both children and adults. The ECLS-B and the ECSL-K collect substantial data on environmental factors but relatively little information on health.
Appendixes A and B list the nation’s major data resources for measuring and tracking children’s health and its influences. It is clear that there are many surveys that tap various aspects of health. Our review shows both the gaps and the considerable overlap and duplication. What is less apparent is that, when an aspect of health is covered, it is often covered using diverse methods, which may include unreliable ways of eliciting information or employ techniques that produce conflicting and inconsistent information. For example, although many surveys in-
|
4 |
For additional information, see http://www.nationalchildrensstudy.gov. |
clude a question about the overall rating of a child’s health, this information may not always be obtained from someone with the same relationship to the child. In some surveys it is answered by a respondent who may not be the child’s primary caretaker and in others by a parent or the person who is most knowledgeable about the child’s health. Questions about the child’s functioning have inconsistent wording across surveys. When wording is inconsistent over a period of time, it is difficult to know to what extent changing rates of identification are a result of those changes (Newacheck et al., 2003).
It has been recognized for some time that data could be collected and used more efficiently if they were better coordinated across agencies. The U.S. Department of Health and Human Services Data Council, responsible to the secretary of health and human services, was intended to accomplish this, but it has not focused on the need for new approaches to the conceptualization of children’s health or on the consequent appropriate data collection and dissemination.
National Data Syntheses
There have been several national efforts to use secondary national data to produce annual reports on the health or well-being of children (see Box 4-2). These reports are used by policy makers at the federal, state, and local levels and by others interested in children’s health issues to understand trends. Although they can be useful tools to monitor specific indicators over time, they do not enable understanding of the dynamics of children’s health or the interaction of influences and health.
For the past 15 years, the MCHB has published an annual report entitled Child Health USA that includes data on child health indicators, as well as state-specific data on selective indicators. It also includes trends and progress toward
|
BOX 4-2 America’s Children and the Environment America’s Children: Key National Indicators of Well-Being Child Health USA KIDS COUNT Child Trends Data Bank NOTE: See Appendix C for web links for these syntheses and examples of the indicators tracked. |
meeting the goals and objectives in the next decade as set out in the federal reports (Health Resources and Service Administration, 2002).
Over the past 10 years, several other federal efforts have created a greater focus on children’s health, particularly on aspects of health traditionally defined as “well-being.” In 1994 the Office of the Assistant Secretary for Planning and Evaluation (ASPE) created an annual publication entitled Trends in the Well-Being of America’s Children. In the same year, a Federal Interagency Forum on Child and Family Statistics was instituted and was formally established in 1997 by executive order. The forum is a formal structure for collaboration among 20 federal agencies that produce or use statistical data on children and families. Since 1998 it has produced a report, America’s Children: Key National Indicators of Well-Being, now produced on a biannual basis, which presents secondary data on economic security, health, behavior, social environment, and education. ASPE is currently developing a report, Social Indicators: Measures of Children, Family and Community Connections, to better understand family indicators in the domains of family structure; family functioning; family, work, and child care; school involvement and civic engagement; and social connections. The Environmental Protection Agency has produced two editions of America’s Children and the Environment, which presents trend data on environmental contaminants in air, water, food, and soil; biomonitoring data; and data on childhood diseases associated with factors in the physical environment.
Another source of secondary information is the databank maintained by Child Trends, Inc., which provides ready access to a wide range of current data sources pertinent to children’s health and its influences. Finally, KIDS COUNT, a project of the Annie E. Casey Foundation, uses census data to produce national and state-level indicators of child well-being. KIDS COUNT produces an annual data book, makes data available on their web site, and funds a network of state-level projects (see Box 4-3).
Healthy People 2010, a national initiative that defines objectives to identify the most significant preventable threats to health and establish national goals related to these objectives, specifies numerous indicators to track the health of the U.S. population. While there are multiple indicators specific to children throughout the numerous identified objectives, with the exception of those relevant to adolescents, there have been limited efforts to use this mechanism to develop a comprehensive focus on the health of children, and the indicators specific to children are not presented in an integrated format.
Other Potential Sources
Other potential sources of information on children’s health are clinical and administrative data derived from records or billing information supplied by health care providers. There are large datasets on enrollees in private health insurance plans and in state Medicaid and the State Child Health Insurance Plan. Another
large administrative dataset is the AHRQ’s National Hospital Discharge Data Set. However, these sources vary in the degree to which they are representative of conditions in the population, because they undercount individuals with poorer access, tend to be health insurer specific, and because of the considerable evidence that coding is often inaccurate. Issues related to how to interpret data for which
|
BOX 4-3 KIDS COUNT, a national and state-level project aimed at assessing the status of children in the United States, was initiated by the Annie E. Casey Foundation in the late 1980s. The initiative is designed “to contribute to public accountability for different child outcomes, resulting in a model for data-driven advocacy for children, their families, and their communities.” KIDS COUNT publishes an annual data book that presents state-level data on the educational, social, economic, and physical well-being of children using indicators from multiple data sets. The Casey Foundation also funds a national network of state-level KIDS COUNT projects that provides a more in-depth and detailed view of children in their state. The 10 measures used to rank states on overall child well-being include:
The project has also published a series of special reports, such as:
For more information, see www.kidscount.org. |
there are no clear denominators and the unreliability of coding are serious. In the first case, there is no way of knowing how to interpret rates of diagnoses, since the population is not stable over time, with people going in and out of practices and plans. In the second, there are obstacles to overcome in order to ensure that coding is consistent. Of concern is the bias frequently introduced by the requirements for reimbursement of medical services, which often influences the ways in which diagnoses are reported. Another limitation is that some sites or plans, especially managed care plans, do not collect data on patients but, rather, on visits. Other concerns relate to how issues of cultural mistrust, perceived racism, or stereotyping may introduce measurement errors when providers and patients are from different cultural, ethnic, and racial backgrounds. Some of these latter problems exist in survey data as well.
State and Local Approaches
At the state and local levels, the measurement of children’s health has been even more variable. Other than infant mortality and other mandated perinatal indicators that are collected as part of national vital statistics, as well as the recent SLAITS surveys that have sufficient power to allow state estimates, state and local data collection is inconsistent across jurisdictions. In 1998 ASPE, in collaboration with the Administration for Children and Families and the David and Lucile Packard Foundation, implemented a state-level initiative to build on the work of the Federal Inter-Agency Forum on Child and Family Statistics. This initiative funded 14 states over a 2-year period to develop and track various state-level indicators of children’s health and well-being and “to institutionalize the use of indicators in state and local policymaking” (http://aspe.hhs.gov/hsp/cyp/childind98, accessed February 25, 2003).
Federally required reporting largely reflects categorical program funding, which often relies on measures of service utilization as proxy measures of health and is driven by funding allocation rather than a well-developed strategy to measure the health of children. In the past decade, some of that has begun to change due to new initiatives originating at the federal and local levels. First, the federal MCHB now requires that all states develop indicators of program performance and measures of the health of mothers and children as a requirement of receiving maternal and child health funding. With a specified set of indicators, states are now collecting and aggregating data on child and family health issues, but there is considerable latitude in how these indicators are measured and hence a lack of standardization. In many states, the demand for indicators has also trickled down to the local level. This move to require a common set of indicators may ultimately form the basis for a common set of metrics on children’s health across states.
CityMatCH, a national organization of local maternal and child health agencies, also has facilitated the enhanced collection and reporting of local maternal and child health data. For example, CityMatCH provides city-specific data re-
ports of national comparative data regarding specific health problems, such as infant mortality and low birthweight. Another local data collection enhancement has grown out of the recent focus on the development of healthy cities and communities, which has focused on promoting population health and launching community-wide health improvement initiatives. Similar offshoots specifically focused on children’s issues have resulted in development in many localities of community health reports (Halfon et al., 1998; Fielding et al., 1999), made possible by increasing data and information processing and dissemination at the local level. Many of these community health reports focus on children and family health issues, and in many locations across the United States these reports have also been based on new data collection or data synthesis projects.
A network of children’s preventive services tracking registries is now operating in six states and New York City as a result of a Robert Wood Johnson Foundation initiative, All Kids Count.5 These data systems are developing the prototypes for a nationwide system of integrated population-based registries that could be linked with primary care providers to ensure that all children have a “medical home” and that public health officials and other policy makers have population-based data on all children. The rationale for some of these efforts is to demonstrate that local data systems could support the reports of health care providers in activities to promote the health and development of children (Halfon and Hochstein, 2002). These initiatives are very promising. However, it is important to note that only a relatively small proportion of communities are involved or assessing indicators or measures in the same way.
IMPROVING MEASUREMENT OF CHILDREN’S HEALTH
In looking at the current compilation of information about children’s health in terms of the committee’s conceptual framework, we outline data collection efforts by domain and then look further at the steps that should be taken to improve measurement strategies. While we have chosen to organize this discussion into three discrete domains, it must be emphasized that there is no single universally accepted approach to the delineation of domains of health. Thus to some extent the division is always somewhat arbitrary. Nevertheless, in our view the domains we identified are consistent with current thinking as reflected in the recently adopted International Classification of Functioning as it applies to children (Simeonsson et al., 2003) and with current research in this field.
Existing sources of data contain many items related to aspects of children’s health as conceptualized in this report, although not organized around the specific domains suggested below. Most current indicators of health are in fact proxy measures, single items that do not clearly fall into a single domain or cannot be combined to measure the domains fully.
|
5 |
For additional information, see http://www.allkidscount.org. |
Health Conditions
The first domain, which we call health conditions, contains information on disease, impairment, injury, and symptoms. Most of the items come from vital statistics (in the form of low birthweight and death by cause data), from clinical or administrative data as reported on claims or encounter forms, from injury reporting systems, or from registries. Some surveys also collect data on proxy-reported (or occasionally, in the case of adolescents, on self-reported) health conditions, injuries, and impairments. There are differences in the ways that the principal data agencies (i.e., CDC, NCHS, MCHB, and AHRQ) define specific diseases and measure them. Also, agencies use different age categories, even within childhood. As a result, the country has various estimates for the prevalence of health conditions, making it difficult to compare sources of data regarding conditions and to understand reasons for the differences in estimates.
Another concern is that the cumulative data from most surveys provide estimates for prevalence, but not for the incidence, of individual diagnosed conditions, and there is little information about the overall health of individual children. That is, surveys often look at one or two disease entities, rather than a profile of how diseases cluster in groups of individuals. Diseases are not randomly distributed in the population (Starfield, 1991; Kunitz, 2002), and an accumulating literature (Starfield, 2001; Long et al., 1994) documents the magnitude of this co-occurrence (comorbidity), which is especially pronounced in childhood, when the overall prevalence of health conditions is low but unexpected co-occurrence of different types of illnesses and impairment is higher than would be expected by chance distributions (van den Akker et al., 1998).
Despite this knowledge, most data collection efforts do not describe or facilitate explanation of the clustering of health conditions in specific individuals or population subgroups. There is considerable and robust evidence that children with ongoing health conditions, such as asthma or diabetes, are more likely to have other types of conditions as well. For example, a large literature, for both adults and children, demonstrates that mental health problems are more common in children with chronic physical conditions than in the overall child population (Harris et al., 1996; Long et al., 1994; Stein and Silver, 2002). Thus another concern about the currently available data is that they focus on individual conditions, rather than on the health of groups of individuals.
Given the recent estimates by the surgeon general (U.S. Department of Health and Human Services, 1999) that approximately 1 in 10 (11 percent) of children of ages 9–17 have a significant behavioral or emotional disorder with substantial impairment in current functioning, it may be surprising that there are no assessment approaches currently in place that track child and adolescent emotional health in all of its important aspects.
Generally missing are data on physical and emotional symptoms. Both clinical records and surveys are potential sources of data on symptoms; their coding
would be facilitated by more widespread use of the International Classification of Primary Care (ICPC) (Lamberts et al., 1993) or potentially by the newly adopted International Classification of Functioning, Disability and Health (ICF), discussed in the next section. The ICPC was developed by the World Association of National Colleges and Academies, an international association of family physicians, for use in the coding of presenting problems in primary care. It codes a wide variety of types of problems, diagnoses, and other types of reasons for visits (e.g., medication refill, administrative reasons, well-person care) and is compatible with the World Health Organization’s International Classification of Diseases.
Functioning
The second domain, which we call functioning, is generally represented by single items or nested items in health surveys. These questions generally explore limitations in functioning related to school or play, which are considered the main functional arenas of children. The utility of existing data and a more complete range of data on physical, cognitive, emotional, and social functioning, as well as disability and restriction of activity, would be enhanced by adoption of the ICF, as it becomes better known by practitioners and survey organizations. This system is designed to inventory different aspects of participation in a wide range of daily activities and to assess the structural and environmental barriers that impede or facilitate functioning. However, it has not yet been adapted to be rapidly used in clinical care or in surveys. The domain of functioning could also benefit from more detailed descriptions of levels of functioning in a range of settings and roles.
Several measures of child functioning are available, such as Functional Status II (R) (Stein and Jessop, 1990), the Wee FIM (Msall et al., 1994), and the Rand measure (Eisen et al., 1979). Each of these measures focuses on a different part of the spectrum of functioning, from unimpaired to severely impaired. Virtually all these instruments depend on the capacity of the clinician or parent respondents to assess a child’s performance of activities compared with a theoretical norm and to report accurately on aspects of health and on deviations from normal. The reporting individual must be able to observe accurately and to interpret and communicate the observations in a reliable way. Functional status measures do, however, have the advantage of being applicable to children with a wide range of conditions of varying types, and of including the effects of multiple health conditions (comorbidity) and their treatment (Stein et al., 1987; Starfield, 1992). In many ways these measures represent the summation of multiple health impairments and treatments on the daily lives of children.
Health Potential
The third domain, which we call health potential, is severely underrepresented in existing data sources. Specific indicators of competency and capacity are as-
pects of developmental status that are rarely measured in surveys or assessed in administrative data. While single items, such as susceptibility to illness (“seldom gets sick”), are sometimes included, most measures of health potential exist for research purposes. They have only rarely been used in clinical settings or ascertained in community surveys. The concept of resilience, until recently, has not been included as part of health. Encompassed in the concept of resilience are such characteristics as protection against (immunization or immunity to or resistance to) illness, problem-solving ability (or “coping”), health-promoting behaviors, physical fitness, and constructive peer and social relationships. These data have been collected in a few local unpublished evaluations of new health programs.
Thus, the country lacks even basic information on the frequency or distribution of characteristics of resilience and other aspect of positive health in childhood and on its variability across the population. Although there is some information on immunization status, it is not generally linkable with other health information. There is no coordinated or linkable data on other aspects of health potential.
PROFILES AND INTEGRATIVE MEASURES
When more than one dimension of health is measured, the question arises of how to compile the information about the different components of health to facilitate a population perspective. One approach is to create profiles that characterize health according to the patterns of scores in each domain of health. This allows for understanding of differences in patterns of health across subgroups of the population. It is a necessary component of understanding the ways that variations in health along specific dimensions affect future health over time and how influences of health may affect one dimension more than another.
The creation of profiles of health is an achievable goal. As mentioned earlier, there is potential for combining current indicators into domains and further incorporating domains into profiles that represent integrated measures at the individual level, which can be aggregated to subpopulation and population levels. Not only might such profiles describe the health of individuals and populations generically, but they also could provide the basis for describing the clustering of good and poor health within and across populations and population subgroups (Riley et al., 1998b; Starfield et al., 2002; Starfield, Robertson, and Riley, 2002). There are research tools that assess such profiles, but these are not widely known, generally have a large number of questions, and have not yet been incorporated into thinking about the assessment of well-being across diverse populations. Profiles can capture information about the health of individuals as well as the health of populations and their subgroups (Starfield, 1974; Riley et al., 1998; Riley, Green, Forrest et al., 1998).
Beyond the creation of profiles, many favor the creation of integrative measures that would in effect sum the various components into single score or index
of health.6 Such indices exist in other areas, such as in economics, and although the elements in their calculation may be controversial, they have demonstrated utility in following patterns over time and across communities. In the case of constructing an overall integrative measure of children’s health, it would be ideal to incorporate the values that individuals, groups, or society assign to the duration of survival as modified by conditions, impairments, and deficits in psychological, social, or physical functioning and also to assess the individual’s health potential. Integrative measures should characterize the special aspects of children’s health, such as developmental capacities.
A good measure of health would include a summary score of relevant strengths and deficits that are combined across several components or constructs of development, as is the case for attempts to measure school readiness, which aim to include a child’s physical and neurodevelopmental function, cognitive capacity, language function, and social emotional development. Although such measures may not routinely assess health conditions or health impairments, they may provide a composite evaluation of a child’s potential to thrive in an educational setting and help forecast that child’s or group of children’s health, emotional, and social needs (Janus and Offord, 2000).
One approach that has gained in popularity, especially in tracking the health of children in drug treatment trials and other forms of research, is the use of measures of health-related quality of life. These instruments include a wide range of health-related elements, including some of the ones mentioned above. However, they also include a subjective (and in the case of young children, a parental) assessment of pain and other symptoms, general well-being (including some elements that are not consistently thought of as health), and in some cases even parental mental health and stress. Most are lengthy and almost all are proprietary (i.e., not in the public domain). As a result, they have relatively limited acceptability for measuring the health of populations. Thus, we have chosen not to discuss them in any detail here.
Another approach that we reviewed is the use of disability-adjusted life years. These summary scores are predicated on ascribing an economic value to the loss of active and productive contribution to society, primarily in economic terms. These techniques discount the benefits of improvements in children’s health, since they place little value on the payoffs that do not result in immediate earnings. Thus they favor improvements in the health of adults who are actively contributing to the community over children’s health, since the benefits of improved
health for children often accrue well into the future, after they have become adults. To some, this leads to an unwarranted bias in favor of productive ill adults over childrearing, immunization, and other investments relevant to children’s health.
With the possible exception of overall attempts to quantify a child’s school readiness, few measures in current use provide actual profiles of different aspects of children’s health, and there is a paucity of integrative measures that cover the age range from infancy through adolescence. Analyses of extant national surveys do not contain profiles or integrative measures of children’s health. The only generic measure that is widely available comes from survey-based self- (or, more often, proxy) reports of whether health is subjectively perceived as excellent, very good, good, fair, or poor. In terms of the validity of this question, it is known that lower ratings, as for adults, are associated with poorer health. In children this is manifest by more illness in the previous 12 months and more impairments that limit participation (Alaimo et al., 2001). Children with chronic conditions and functional limitations are more likely to be rated in fair or poor health (Hogan, Rogers, and Msall, 2000; Newacheck and Halfon, 1998; McGauhey et al., 1991; McGauhey and Starfield, 1993). Recent data also indicate that reports on this single item are correlated with scores on the different domains of health when elicited from children in health surveys, and that poorer health ratings are associated with higher utilization of health services in the following year (Riley et al., submitted). However, the predictive validity of these single item ratings for both adults and children may not be the same in diverse population subgroups. One report on children suggests that it may differ in various racial and ethnic groups and that this is not entirely due to differences in other measures of health status such as chronic illness and reported disability (Siegel et al., 2004).
Overcoming Conceptualization Gaps
The approaches summarized provide some important descriptive data about the prevalence of diseases and some information on overall functioning, but these strategies provide little information about the overall health of individual people or groups of people, how their health varies over time, or even the proportion of the population who have more than one condition. They do not reflect the dynamic, multidimensional concept of health that we have proposed, nor do they assess the health potential of children. Childhood implies developmental plasticity. It follows therefore that the best measures of health should reflect this plasticity and most especially children’s current and capacity for continued health. They should also detect very early or “pre-stages” of illness as represented by intrinsic and extrinsic predisposition to overt pathology and be able to assess and quantify the spectrum of health in a population of children.
Thus, the first challenge is to delineate methods for measuring the dynamic, developmental, and multidimensional concept of health, including health poten-
tial. At a minimum, this requires a consensus about the most important or critical components of health and an increased priority on the importance of monitoring children’s health as a matter of national interest. It is also complicated by a number of issues: specific constituencies with a focus on subsets of issues, concerns about the stability and meaning of different domains at any given point for current health, lack of clarity about the current meaning of a given level of health across diverse populations of children, and incomplete information about the predictive validity of a given measure. However, in the committee’s view, with concerted focus, resolution of these issues is possible and much of the missing data are obtainable within a reasonable time frame. Mapping trajectories through ongoing collection of data that adopts the same conceptual framework would enable rapid strides to be made in both measuring and understanding children’s health and would make it possible to identify and address the needs of subgroups with poorer health.
Overcoming Methodological Gaps
The continuous changes in children as they age can complicate the measurement of their health and require altering the yardsticks used to assess health at various developmental stages. Different individual items may be required to measure domains and subdomains across developmental stages. Inconsistency of the measure or items requires that one sort out how much change reflects measurement error and how much reflects true change in the domain being assessed. This is true even when the same measurement strategy is used consistently over time, because reliability of particular measures may differ systematically between younger and older children.
Another issue that complicates measurement is the need for proxy respondents. Very young children cannot answer questions for themselves, and even school-age children may not be able to respond about some domains of health, because they have not yet developed the ability to perform the level of abstract thinking necessary to answer certain kinds of questions. Those with impairments or disabilities may develop the ability to respond for themselves at a later age than is usual. As a result, it is necessary to obtain data from adult caretakers, parents, or clinicians, at least through the early school-age period. This may produce changes in responses if parental caretakers change over time or when children become old enough to respond for themselves. Parents from diverse backgrounds may also bring different notions of health and disease and may provide different information as a function of the interviewer’s background.
Improving Reliability and Validity
Measures of complex concepts such as emotional health and resilience are not often captured in single-item questions. Rather, they require a collection of
items to tap the various components that are included in the concept. Well-standardized procedures must be used to assess whether the purported measure is actually doing the job of measuring the concept. This process involves collecting different types of data and subjecting them to analyses to determine if they meet customary standards of reliability (i.e., consistently measures the concept) and validity. Tests of validity are further subdivided into assessments to determine whether the measure behaves in an expected way in relationship to other measures, where they exist, and in relationship to what is known about predictors—for example, of good and poor health. In particular, issues of reliability and validity are compounded when back-translations are needed (Erkut et al., 1999b) and when cross-cultural testing is not available (Scientific Advisory Committee of the Medial Outcomes Trust) (Lohr et al., 2002).
Measures must be quantifiable and reflect the broad range of health outcomes while remaining valid, meaningful, and culturally relevant. The importance of these standards for the measurement of children’s health is threefold. First, few measures of these important aspects of children’s health meet these standards, and even fewer do so across the full age spectrum (infancy through adolescence) or across subpopulations of different races, ethnicity, or cultures. There is a need for more research in this area to develop better and more sensitive measures that can then be used in large-scale data collection.
Second, there is a need for brevity and efficiency in measures and hence a strong bias in designing surveys against using multi-item measures and scales in large population monitoring activities and in clinical settings because of the expense of administration of each additional question. Organizations that monitor the health of populations aim to do so with single items or with a small set of items, rather than with scales. Yet reducing complex issues to single items is problematic at best. In the area of children’s health, this process is further complicated by the paucity of well-developed psychometrically sound instruments for measuring health that span the age range. As a result, with some occasional notable exceptions, primarily in the area of children’s mental health, NCHS and others have traditionally used single items preferentially. Newer measurement techniques have been developed that in some cases allow for truncating the number of items that need to be obtained (item response theory) (Hays et al., 2000; Bjorner et al., 2003; Ware, 2003), but even these techniques require extensive measurement development and administration in data collection of a substantial number of items in order to measure a construct as complex as functioning (Moore et al., 2002).
Third, there has been reluctance to invest in the development of instruments and in the funding of the amount of testing that is required to refine an instrument and to determine its reliability and validity across the age spectrum and across diverse populations.
As our conceptual model and definition have highlighted, children have special health attributes that distinguish them from adults. Their unique develop-
mental aspects mean that one must consider not only what domains of health are measured but also how and when to measure health. The timing of measurement is important relative to critical and sensitive periods of development and relative to critical transitions and turning points in children’s lives.
Other Methodological Challenges
The committee noted a number of other methodological challenges to current health efforts. First, manifestations of health may vary from setting to setting (for example, in school and at home), so what is noted by an observer in one setting may not be seen in a different setting. As a result, information discrepancies are common when multiple informants are used and procedures must be employed that connect the information and observations provided by different informants.
Second, young children and even older youth tend to not be accurate reporters of their own experiences and behaviors, in part by virtue of cognitive immaturity in younger children and because of concerns about the consequences of candid disclosure in older youth.
Third, privacy concerns are also important, because some health-related phenomena may be associated with embarrassment, stigma, or even legal consequences (e.g., substance use, unprotected sex, suicidal ideation, aggression or violence, victimization).
Fourth, many health-related phenomena, whether positive or negative, are experienced by many youngsters at one time or another over the course of their development, so it may be unclear when they become important in terms of current or future health. For example, many youth experience suicidal ideation, many are intermittently depressed or anxious, and many experiment with drugs or unprotected sex, but not all of those who do have serious health issues. To distinguish what is normal from what is unhealthy or of concern, measurement experts often attempt to qualify the presence or absence of a given condition by adjectives related to severity, frequency, or duration, for example, extreme sadness, frequent drug use, ability-limiting illness. However, most qualifying terms such as “extreme” or “frequent” are also subjective and could be interpreted differently by informants of different cultural backgrounds. Even if one attempts to demarcate normal from abnormal with more specific modifiers (e.g., sadness lasting all day, most days, for two weeks or more), knowledge about what constitutes normal and abnormal is lacking and may vary by age of the child.
Meaningful measurements of health across regions and populations often require reliance on multiple informants, reconciliation of discrepant information across informants, combining different measures across informants and settings, demonstration that the measurements are not simply normal variations (e.g., extreme in terms of frequency, duration, or severity or in short- and long-term prognosis) of impairment in functioning or compromise in future health. As a
result of the above concerns there should be support in all data collection activities for methodological efforts to ensure reliability and validity.
Even when longitudinal surveys have gathered health information at multiple points in time, it is rare when analyses of these data have taken advantage of the latest statistical methods. Both hierarchical linear models (Raudenbush and Bryk, 2002) and latent variable growth curve models (e.g., Duncan et al., 1999) can be applied to the problem of understanding the nature and determinants of developmental trajectories.
Appendix B indicates whether measures on the most common federal surveys deal with specific aspects of health and mental health conditions (e.g., depression), whether multiple informants are utilized, and the extent to which empirically established most-valid informants are used for particular health constructs, whether for a risk or an actual health condition. As can be seen from the tables in the appendix, the sole exception to the general failure to attend to these issues is the current iteration of the NHANES study, which is gathering in-depth information from parent and youth informants in such a manner that actual health conditions can be distinguished from high-risk behaviors. The difficulty in doing so is not simply a problem of survey design but has to do with how the mental health, education, and medical fields conceptualize mental health and illness. Many physical and mental health disorders are on a spectrum with common day-to-day problems experienced by everyone. The absence of clear, critical indicators for mental health and illness with strong face validity and an empirical basis for clear medical necessity and impairment in functioning is an important conceptual and methodological hurdle that has not been fully addressed by health researchers and policy makers.
Another methodological problem concerns the representativeness of samples (Brown, 2001). With the exception of major national surveys conducted as ongoing activities of NCHS, AHRQ, and NCES, most samples are representative only of particular communities or regions, usually with time-limited funding sources as a part of an investigator-initiated research study (e.g., National Institute of Health funding). While some of these regional studies are longitudinal, there is generally no clear ongoing commitment to funding or approach that is part of a health-monitoring strategy with explicit ties to policy. Even well-conceived and nationally representative recurring surveys (such as NHIS) are often limited (at least partly due to resource constraints) by failure to use in-depth assessment approaches, failure to use most-valid informants, and failure to link influences with health conditions reflecting disease burden and policy import.
Opportunities to Improve the Conceptual Basis for Health Assessment
The conceptualization of children’s health is challenging. Health in childhood extends far beyond diseases, disabilities, and impairments that are typical indicators of adult health. Childhood health is characterized by developmental
plasticity, which is not a major facet of adult health. There are critical and sensitive periods of development with major impact on future health outcomes. Early health experiences contribute heavily to subsequent health trajectories.
Measurement strategies should capture what these principles embody. In particular, strategies should capture changes in particularly sensitive periods of development and map how health during one period influences and predisposes to subsequent states of health.
Mapping the health trajectories of individual children or entire populations of children requires consideration of what measures in a specific domain can be linked across developmental periods to create a conceptually consistent measurement trajectory, and also what group of measures across domains can be assembled to account for an aggregate trajectory. Conceptual work related to school readiness illustrates what could be done for a variety of health domains (see Figure 4-1). Measuring specific dimensions of a child’s health at birth and at several other ages (e.g., 1, 3, and 5) in a consistent manner could result in a composite health trajectory and a way to plot aspects of children’s health in much the same way that one currently plots growth trajectories either for individual children or a population as a whole.
Without a strategy to develop composite indicators, it will not be possible to track health across developmental stages. A domain and subdomain structure should be consistent across developmental stages, even if specific individual items
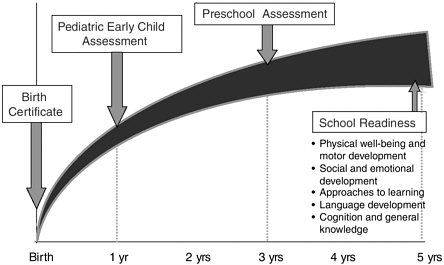
FIGURE 4-1 Systematic data collection for tracking school readiness trajectories.
SOURCE: Halfon et al. (2004).
representing the domain or subdomain differ from one developmental stage to another.
It seems especially important to develop good tools to assess the health of children at major transitions, such as entry into preschool or the beginning of adolescence because these represent critical points at which potential health problems may interfere with the developmental tasks. Measurement strategies should be devised to elicit not only important milestones in development but also the trajectory of characteristics that affect the attainment of those milestones at expected times. For example, most children babble and make simple words before they start saying phrases, and they make declarative statements before they ask questions. But it is unknown how much the variation in the acquisition of those skills affects overall language development except in the most extreme situations.
Addressing the Need for Data on Health Characteristics of Subpopulations
Vulnerable Subpopulations
Disparities in health by race and ethnicity are well documented (Institute of Medicine, 2002b, 2003) and demand national attention. A large subpopulation of children also has poorer health due to social disadvantage. Children in lower income families have more severe health problems and worse health prognoses than children in higher income families. Except for most large national surveys that collect data on family income and parental education, few or no data are collected to provide a systematic understanding of differences in health in population subgroups based on socioeconomic status.
In addition, there are specific subpopulations of children that deserve special attention because of their extra vulnerability to poor health. Localized studies and long-term follow-up studies of specific populations of children (e.g., children who are abused or neglected or in foster care) indicate that some have poorer health (including mental health) and more developmental problems and seriously compromised long-term health trajectories. At present there is limited systematic collection of health-related data on most of these subpopulations at either a local or a national level. A similar situation holds for children with special health care needs due to chronic and debilitating medical or mental health conditions, children in special education school systems, children with severe emotional and behavioral disorders, and institutionalized children. Each of these vulnerable subpopulations of children is poorly reflected in health measurement attempts. Moreover, most surveys intentionally exclude institutionalized children, many of whom have severe health impairments. The very small size of some of these special populations require targeted special studies.
Age-Related Subpopulations
In addition to gaps in the measurement of the health of subpopulations defined by current health and social adversity, there are also gaps associated with age and development, particularly a lack of data related to the middle childhood years. While the NHIS, NHANES, and other national data collection efforts include data on all children, sample size and response burden issues usually preclude the kind of detailed information that is necessary to assess the health of children relative to their developmental age and stage or membership in particular subgroup populations. The NHIS contains a few questions specific to young children, school-age children, and adolescents, and the new MCHB-sponsored NSCH will provide a few more questions relevant to age and developmental stage questions. However, neither of these surveys provides the information needed to develop a comprehensive picture of the health of young children, to better understand the role of various risk and protective factors during early childhood, to assess their access to personal or public health services, or to measure the impact of health care on health. Until the NSECH was piloted, there had not been a data collection effort targeted on the health, health care content, quality of health care, or home health behaviors of families with young children. Since the NSECH is not a part of the regular national survey series, there is no guarantee that there will be ongoing collection of such relevant early childhood health data (Halfon, Olson, Inkelas et al., 2002). Similarly, while there has been recent emphasis on the importance of early childhood and the first 5 years of life as well as considerable focus on adolescents, there has not been the same kind of focus on middle childhood. Relative to adolescents and early childhood, this is a vastly ignored developmental period with regard to the collection of information on health and health influences. Ongoing monitoring of health risk through state administration of the YRBS provides some information on health, although only for those ages 12 to 17 (Brown, 2001).
Addressing the Need for Data on Functioning and Positive Aspects of Health
Standard surveys often ask about whether children are limited in the amount of play (for children under 5 years), or school they experience, but there are few other assessments of their overall functioning. Since many children with even severe impairments are able to play, and most are able to attend school, especially under current policies, this is only a gross estimate of their overall functioning. There are currently few other attempts to assess the overall functioning of children on a population basis, in part because of the relative paucity of measures available to assess functioning, and in part because many of the existing measures require the administration of multi-item questionnaires or other assessments. More work is needed in developing tools that are efficient and valid in this domain.
Although there are some data on health risks, there are very few data on positive health measures and other health and developmental assets, including characteristics that help to ward off threats to ill health. Similarly, there are no coordinated or linkable data regarding states of “resilience,” such as physical fitness and nutritional status. While many communities throughout the United States have engaged in the measurement of positive youth behaviors and developmental assets as part of their own local interest or projects, it is important to consider how measuring the developmental assets of young people can be encouraged in all communities and the data made available to public and private entities interested in fostering positive health development in their youth.
In March 2003, Child Trends convened a national conference of leading researchers to review the state of the art in measurement of positive development. The conference concluded (Child Trends, 2003) that a theory of positive development was still lacking, and that many if not most of the measures that have been developed still lack demonstration of validity. Two areas were included under the broad rubric of positive development: (1) positive feelings, attitudes, and beliefs and (2) skills, behaviors, and competencies. The role of culture in the first of these two categories was recognized as a major consideration in interpreting the value of the measures. Other major issues were related to data collection and to the choice of type of respondent. Further work on theory development and research on positive measures was recommended, a direction with which the committee concurs.
CONCLUSION
In the near future, it may be possible to determine the early origins for many significant adult health conditions, such as adult-onset diabetes mellitus, coronary heart disease, and hypertension, as well as to have information about the risk of developing common childhood diseases such as asthma, attention deficit hyperactivity disorder, and some metabolic and diet-related conditions. There is already success in predicting the likelihood of rare Mendelian diseases. Whether there will be similar success in predicting many common adult conditions remains to be seen. At present there is no mechanism for assessing the distribution of genetic risk profiles in the population or relating them to the environmental influences that are likely to determine the actual likelihood of ensuing disease and disability as well as resilience. Developing better data collection mechanisms to array environmental influences in relation to biological or genetic factors is an area in which greater gaps in measurement are likely to be felt in just a few years.
Although there are data that indicate that children are not thriving, many current measures cannot capture either their successes or their failures. The committee’s view is that the nation must move ahead in developing a more comprehensive measurement strategy that captures the dynamic nature of childhood, assesses all the domains of health, and tracks composite trajectories of children’s
health. Strengths and deficits in the current measurement strategies have been highlighted. Measures that assess health potential and provide more comprehensive assessment of functioning, as well as for composite measurements of health, need to be developed. Deficiencies in the assessment of health and influences on health during middle childhood and of special population subgroups also need to be addressed.
Movement toward frontiers in health assessment in children will be facilitated by the development of new tools from current and recent research efforts. A variety of instruments is available, many of which have been employed to good advantage in investigations of the outcomes of research interventions. The potential to adapt these tools for use in large population surveys should be explored.

























