
2
Children’s Health: A New Conceptual Framework
Historically, the definition of children’s health has received little consideration separate from that of adults. Although views of adult health have evolved from a focus on morbidity and mortality to consider broader aspects of health, considerations specific to children have generally been excluded. This chapter lays out a new definition and conceptualization of children’s health. It reviews the ideas that led to the committee’s definition and puts forth a model of how health evolves in children. It summarizes the principles underpinning the model and the ways that different influences operate. Finally, the chapter outlines the domains of children’s health that serve as a basis for measuring it.
Although many of the principles outlined in this chapter also apply to adults, they are particularly salient for children. The committee’s charge calls for a focus on children, an emphasis the committee thinks is warranted given the historic lack of attention to children’s health in relation to adult health. However, those involved in population health issues more broadly may want to consider the potential applicability of the definition and conceptual model outlined in this report to adults.
VIEWS ON CHILDREN AND CHILDREN’S HEALTH
The roles of children have changed throughout human history and across different levels of social organization. Children in agrarian and early industrial societies were expected to participate in the work of the family from early childhood, helping other family members in household activities and caring for one another. Many died while still very young, and those who survived were expected
to contribute to the family’s economic situation and, eventually, to the support of their aging parents. There was little collective commitment to the provision of education or services to improve health and only limited knowledge of the environmental factors that influence healthy development. Modern societies generally have less urgent need for children to enter the workforce, and the technological age demands a longer period of schooling and greater skill level from its workforce.
Awareness of and commitment to protecting the health of children and to their nurturance has increased in recent decades (see Zelier, 1994). Observational and empirical research in the 20th century, led by individuals such as John Watson (behaviorism), Arnold Gesell (maturational stage theory), Sigmund Freud (psychoanalytic theory), Jean Piaget (cognitive development theory), Erik Erickson (psychosocial theory), John Bowlby (attachment theory), Urie Bronfenbrenner (ecological theory), and Arnold Sameroff (transactional theory), created the concepual basis for understanding the cognitive, emotional, and social importance of childhood and the roles played by both family and societal forces.
The social transformation of childhood in modern societies reflects a retreat from the view that parents have full and unlimited jurisdiction over their children to one in which the welfare of children is increasingly understood as a shared social responsibility which requires investments in education, health care, and other institutions. At the same time, there has been a growing body of evidence that children’s development is influenced both by their families and by the social forces and cultural norms that society produces. Thus, children’s health, development, achievements, and social attainments have come to require the interest, guidance, and protection of both families and society—not just for the intrinsic value of children but for society’s collective future. This view of childhood is embedded in the very foundation of such social institutions as schools and the health care system, which play important roles in preparing children for the challenges of modern times and ensuring that, as they grow and develop into adults, they are prepared for life in an increasingly complex world.
From a public policy perspective, this emerging view was crystallized in the major social changes that took place in the 19th and 20th centuries and was manifested in national policies for providing health care to indigent populations, free and compulsory public education, mandatory immunizations that both protect individual children and provide group immunity against widespread epidemics of infectious diseases, policies for protection of the welfare of children, and the creation of the juvenile justice and child welfare systems (Katz, 1997; Cravens, 1993; Levine and Levine, 1992).
In the United States, these policies resulted in the creation of the Children’s Bureau in 1913, which later evolved into the present-day Maternal and Child Health Bureau (Hutchins, 1997); a federal agency to oversee education; later the establishment of the National Institute of Child Health and Human Development; and the creation of subsidized health care benefits for particularly needy
children. In more recent years, such collective concern for the health and welfare of children has increased the commitment to improve children’s health services, as reflected in the passage of Medicaid, extensions of Medicaid, and legislation creating the State Child Health Insurance Program. Although the sustainability of some of these initiatives remains in doubt and the trajectory of public interest in children has not been one of continuously increasing concern and commitment, over the course of the past three centuries there has been considerable progress in increasing societal commitment to children.
EVOLVING CONCEPTS OF HEALTH
Notions of health have also evolved over the last century. At the turn of the 20th century, when infectious diseases posed the greatest threat to health, health was viewed as the absence of disease or injury. Disease causation was usually described using simple causal models, epitomized by the germ theory (i.e., an infectious agent alone was responsible for disease) and theories of Mendelian inheritance (i.e., a single gene alone produced the effect observed), in which cause and effect were immediate. Even if not always observable, the mechanisms were simple, singular, and presumably understood.
Public health monitoring and surveillance systems instituted at the beginning of the 20th century focused on measures of survival and used mortality rates for different conditions and age groups (neonatal, infant, and child) as the predominant measures of health. During the first half of the 20th century, the growing and changing medical profession and the health care delivery system also defined health as the absence of disease. Common indicators of health included the numbers or rates at which a disease affected members of a population. The International Classification of Diseases and Related Health Problems (ICD), which dates back to an 1891 international statistical congress, was originally codified as a standard for health measurement by classifying causes of mortality. The ICD was adopted by the World Health Organization (WHO) in 1948 and has been revised every 10 years. It is used as the basis for diagnostic coding in the United States and throughout the world. It makes possible systematic recording, analysis, interpretation, and comparison of both morbidity and mortality data across geographic, national, and temporal boundaries (Chatterji et al., 2002).
This classification continues to develop with evolving notions of health. The new International Classification of Functioning, Disability, and Health focuses not only on impairments of body parts and systems, but also on individual participation in daily activities and on the interaction between disorders and environments that alter functioning (Chatterji et al., 2002).
Changing patterns of morbidity and mortality, routine treatment of infectious diseases, and the increased prevalence of chronic conditions caused shifts in ideas about health. Models of health promotion and disease prevention began to account for the influence of dietary and exercise behaviors, as well as for expo-
sures to multiple influences over longer time frames. This is well illustrated in how various behavioral influences (e.g., poor diet, lack of exercise) interact with genetic influences to affect the development of obesity and how multiple influences (e.g., genes, exposure to allergens and antigens, family behaviors, physical and social environments, health services) affect the development and severity of childhood asthma (Evans and Stoddart, 1990, 2003).
In the United States, the high cost of chronic conditions and the high proportion of elderly people who have one or more of these conditions have led to a primary focus on these aspects of health. As multiple influences on health became better understood, the notion of health as a positive capacity and a prerequisite for a range of human accomplishment took root, elevating the importance of both disease prevention and health promotion (Breslow, 1999).
Precise definitions of health, emphasizing negative, normative, and positive notions of health, have been debated for centuries (Institute of Medicine, 2001b, p. 21). Over time, there has been growing recognition that health is more than the absence of disease. This concept was most dramatically articulated in 1948 by WHO with the following definition (which remains their current definition): “Health is a state of complete physical, mental, and social well-being, not merely the absence of disease or infirmity.”
Several recent reports from the National Academies have reviewed issues in the definition and measurement of health for various specific purposes. These include studies focused on (a) better understanding of the interplay of biological, behavioral, and social influences on health outcomes (Institute of Medicine, 2001b); (b) improving performance monitoring of community health services (Institute of Medicine, 1997); and (c) defining the future research agenda in the behavioral and social sciences for the National Institutes of Health (National Research Council, 2001). Each of these previous reports, as well as several others, highlights the advantages and disadvantages of various definitions, but in none has the primary focus been directed toward children’s health issues. Each, however, emphasizes the importance of notions of positive health and the interplay of multiple individual and environmental factors.
Many critiques of previous definitions focus on their breadth: what is included and what is excluded. For example, while the WHO’s broad and comprehensive definition of health has been used extensively to exhort and advocate for new health interventions and policies, it has also been criticized as being overly inclusive of all human endeavors and very difficult to apply for the purposes of health measurement (Institute of Medicine, 2001b; Young, 1998; Evans and Stoddardt, 1990). Similarly, while there are advantages to biologically based definitions of health, including the specification of precise biomarkers, such definitions cannot capture all the important and commonly understood components of health, such as the capacity to respond to stress or resist disease.
From a medical perspective, health is still defined largely as freedom from injury, disease, or disability. However, the medical community is increasingly
concerned that definitions of health that focus on the absence of disease ignore other aspects of health as well as future health. This void has become more of an issue as the knowledge base and the capacity to measure influences on health have increased.
From a population health perspective, operational definitions of health that focus on measures of morbidity and mortality have also been criticized, because they do not account for the intersection of health and behavior (Evans and Stoddardt, 1990; Institute of Medicine, 2001b). They also fail to incorporate mechanisms for linking health to the multiple influences on health outcomes. The Institute of Medicine (1997) concluded that a broad definition of health that embraces well-being as well as the absence of illness is necessary for effective community efforts aimed at improving health.
Building upon the abundant evidence that children’s health has special characteristics, the committee sought a comprehensive and integrative definition and conceptualization of health that reflects the dynamic nature of childhood, is conceptually sound, is based on the best scientific evidence, and provides a basis for both measuring and improving children’s health. A recent collaborative effort of the 15 member states of the European Union Health Monitoring Programme came to a similar conclusion. Although the specific elements of their model differ, CHILD—Child Health Indicators of Life and Development—proposed an approach to measuring children’s health that embraces the importance of development, the need to consider a range of influences in order to adequately understand and measure it, and the need for data to stimulate action (Rigby and Kohler, 2002). Policy makers in the United States may want to consider possible adaptation of the CHILD system to the context, priorities, and data mechanisms available in the United States.
The committee was also cognizant of the increased emphasis on the prevention of health threats and impairments in children, as well as on the increasingly broad mandate for child health professionals in the United States to involve themselves with multidisciplinary efforts to maximize health. Such efforts are reflected in the publication of Bright Futures, a guideline for the care of children (Green and Palfrey, 2002). Bright Futures has designed training and education for families, health professionals, and communities on health promotion and prevention strategies. Recognizing that health and well-being are a result of interactions of many biological, psychological, social, cultural, and physical factors, it strives for comprehensive health promotion and a productive relationship between the child health professional, children, parents, and the community.
A NEW DEFINITION OF CHILDREN’S HEALTH
For the purpose of this report, health is a characteristic of a child or group of children, whether current, past, or future, and is defined by the committee in the following way:
Children’s health is the extent to which individual children or groups of children are able or enabled to (a) develop and realize their potential, (b) satisfy their needs, and (c) develop the capacities that allow them to interact successfully with their biological, physical, and social environments.
The definition proposed echoes the principles developed at the Ottawa Charter in 1986 that embraced positive aspects of health and declared that to “reach a state of complete physical, mental and social well-being, an individual or group must be able to identify and realize aspirations, to satisfy needs, and to change or cope with the environment. Health is, therefore, seen as a resource for everyday life, not the objective of living. Health is a positive concept emphasizing social and personal resources, as well as physical capacities” (Ottawa Charter for Health Promotion, 1986). The committee refined this perspective in its definition of children’s health to reflect the heightened importance of a developmental perspective and the fact that health results from the interplay of multiple influences.
The committee’s definition views health as a positive resource that gives children the ability to interact with their surroundings and to respond to life’s challenges and changes. Moreover, it incorporates development in the definition and specifies a fundamental principle of development—the optimization and maintenance of function over time. At the same time, it focuses on the intrinsic characteristics of children and their resources for interacting with the environment.
DOMAINS OF HEALTH
Based on the committee’s expertise, current conceptualizations reflected in various internationally endorsed classification schemes, and current research, the committee defined three domains of health as fundamental to the assessment of children’s health: health conditions, functioning, and health potential. This section discusses the conceptualization of these domains. Chapter 4 outlines current approaches to measuring the domains.
The process of developing a vibrant, flexible, and responsive measurement strategy for representing the health of children in the United States depends not only on a definition of health and the conceptual and theoretical underpinning of that definition, but on how the nation operationalizes health in the assessment of an individual child and populations of children. Specifying and relating the multiple domains of health are the central challenge of health measurement (Chatterji et al., 2002). This section specifies the domains that should be considered part of a national framework for measuring children’s health.
The concepts draw on various frameworks that have been proposed to account for the multiplicity of influences on health over the past several decades (Canadian Government, 1974; Laframboise, 1973; Epstein, 1996; Wilkinson, 1992; Marmot and Syme, 1976; Marmot et al., 1984, 1997; Berkman and Syme, 1979; Evans and Stoddart, 1990; Institute of Medicine, 1997, 1999; Halfon and
Hochstein, 2002; Black et al., 1980; Acheson, 1998; Starfield and Shi, 1999). Several previous attempts to develop a way to measure health have been reviewed. Most were developed primarily for adults rather than for children and focus on negative aspects of health. The concepts proposed by the committee take a broader view of health and are consistent with the conclusions of other recent Institute of Medicine committees and the pioneering work in other nations to reconceptualize children’s health and to measure and monitor it (Institute of Medicine, 1997, 2001b; Eiser, 1997; Eiser and Morse, 2001).
Domains to Consider and Criteria We Have Used
Measuring the multifaceted nature of health requires distinctions among domains of health in order to assess and track its different aspects. Because health is dynamic (i.e., both changing and changeable), constantly developing, and affected by multiple factors concurrently, it is inherently difficult to measure. This has important implications for defining and depicting domains and subdomains.
The components of health are not easily slotted into self-contained and non-overlapping categories. The committee viewed several criteria as crucial for identifying domains to guide the measurement of health. These include the need to:
-
Use current scientific evidence about the domains and the influences on health and be responsive to new knowledge about influences on health.
-
Be comprehensive in capturing multiple aspects of health.
-
Allow for comparisons across diverse populations and developmental stages. That is, the domains should be consistent across developmental stages although different measures may be used for assessment.
-
Be useful for assessing the nature and magnitude of the effects of different policies and interventions on health outcomes of children.
-
Recognize that previous and current health status influence subsequent health.
Given the extended time frames and latent effects of different exposures and changes in individual characteristics, some aspects of health may not be amenable to immediate accountability and manipulation. Therefore, in some areas it may not be practicable, credible, or possible to assess the effect of policy, program, or process changes on morbidity, mortality, and the incidence of health conditions. Instead, it may be necessary to rely on validated intermediate outcomes as proxies for such ultimate outcomes, such as measuring known influences on health. Finally, it should be self-evident that measures must accurately reflect all of these qualities of the model.
The committee proposes that health be viewed as having three distinct but related domains: health conditions, a domain that deals with disorders or illnesses
of body systems; functioning, which focuses on the manifestations of individual health in daily life; and health potential, which captures the development of health assets that indicate positive aspects—competence, capacity, and developmental potential (see Table 2-1). Ideally, the science, if sufficiently advanced, would guide the measurement of the individual’s ability to respond successfully to future threats to health.
Health Conditions
Health conditions refer to alterations in health status reflected as disease, injuries, or impairments or as pathophysiological manifestations of disorder (signs and symptoms). Health conditions are usually classified using the ICD, which is currently in its tenth edition (ICD-10). Developed for epidemiological purposes, the ICD system permits standardized and systematic recording and analysis of health conditions, injuries, and many common symptoms. Different categories are used in the ICD to classify certain conditions. They may be acute and self-limited, acute but likely to recur, or chronic; they may be anatomical, physiological, or psychosocial. They include a wide range of specific as well as nonspecific conditions and syndromes.
Functioning
The functioning domain reflects the direct and indirect effects of one or more health conditions and their treatments as well as problems resulting from multiple health problems on the daily life and activities of the child. It includes all aspects of physical, psychological, cognitive, and social functioning as they express themselves in children’s daily activities and behavior.
Alterations in functioning have been used informally by health care providers to measure the significance of injuries and to gauge the effects of acute and
TABLE 2-1 Domains of Health
|
Health Conditions |
Functioning |
Health Potential |
|
Alterations in health status due to disease, disability, or injury |
Physical, cognitive, emotional, and social functioning and deficits |
Competency and capacity in physical, cognitive, emotional, social well-being, and developmental potential |
|
Symptoms |
Functional deficit, disability (disability days, bed days) |
Resilience |
|
|
Restriction in activity (total and by specific conditions), morbidity burden |
|
chronic health conditions. While measures of physiological function fall within the realm of health conditions, not all physiological alterations have a significant health effect in terms of altering functioning (e.g., changes in the pigmentation of the hair) (Ustun et al., 2002). There is rarely a one-to-one correspondence between a diagnosis and its translation into a level of impairment in daily life. Two individuals with the same abnormal laboratory value or radiological finding may have very different life experiences, with one unaffected or only mildly affected in his or her daily life and the other experiencing major dysfunction.
In addition, the functional expression of a condition is heavily influenced by the various ways in which it is modified by other factors intrinsic to the child (e.g., personality, comorbid conditions, genetic endowment) and the environment. For example, a child who lives in a one-story house will experience fewer limitations in function when experiencing joint or muscle disease than one living in a five-story walk-up apartment.
Similarly, the level of compensatory mechanisms and treatments available (e.g., durable medical equipment, implants, medications) will change the expression of the condition in terms of the child’s functioning. Measures of functioning also have great meaning because of their implications for caregiving, dependence, and the ability to participate in social roles. Another advantage of these measures is that they permit a look at the effects of multiple conditions as well as the effects of the conditions and their treatments, including side-effects. They provide a common measure for assessing the health of children across conditions (Stein et al., 1987; Stein and Jessop, 1990).
Limitations in mobility, usual activities, or full participation in school are important aspects of physical function. Psychological function includes a wide range of functions, both cognitive (e.g., alertness, confusion, problem-solving ability, receptive language ability) and emotional (e.g., affect, mood, temperament). Given the profound developmental growth that takes place over the life course of a child, these subdomains constantly change, which creates significant challenges for accurate measurement of psychological deficits. For example, a specific disease can cause a child to regress in emotional or cognitive capacity. However, without repeated measurement of that child’s function, it would be difficult to determine whether a regression had taken place.
Social functioning refers to limitations imposed on children in the realm of their usual activities and relationships. For a young child, the subdomains of social role function include the ability to engage in ordinary play and the ability to attend school and participate in all school-related activities. Social functioning also includes measures of social integration and social connection, including the ability to make and keep friends and to play a supportive or instrumental role in the lives of others. Culture contributes in major ways to the definition of appropriate social functioning, and thus this domain may have different meaning for different subgroups.
Alterations in function include physical, cognitive, emotional, and social
impairments and measures of functional disability (e.g., disability days, bed days, limited activity days) and diminished developmental opportunities due to disadvantage caused by health condition, stigma, and social valuation. Measurement of these alterations in functioning may include gross and fine motor deficits; oral motor skills in a young child; alterations in physical growth and weight; and restrictions in activity, mobility, and self-care, as well as impairments in psychological functioning (i.e., cognitive functioning, such as problem solving, receptive and expressive language) and in social roles, such as attachment, relational capacity, affect, mood, behaviors, and school dropout rates.
Health Potential
Health potential includes both health assets that provide the capacity to respond to physical, psychological, and social challenges and risk states that increase vulnerability to other aspects of poor health. Health potential includes subdomains that the research literature has indicated are important measures of a child’s capacities and reserves. Included in this domain are positive developmental assets and health capacities that provide and indicate ability to form positive relationships, regulate emotional and cognitive states, and respond to multiple challenges, including exposures to disease and psychological and physical stress, among others. While to some extent this might be looked on as the positive aspect of functioning, that is, the capacity to function in the face of threats to one’s health, we have chosen to distinguish this domain as unique because of the inherent bias toward defining functioning only as normal or deficient. Few if any measures of functioning capture this more positive aspect of a person’s assets and resources and of the characteristics that make them resilient.
Other characteristics described as resilience factors that fall within this domain include curiosity, responsiveness, reflection, imagination, self-efficacy, problem-solving ability, self-sufficiency, optimism, and disease resistance and recovery (Starfield et al., 1993). All are characteristics that add to a child’s ability to deal with and bounce back from adversity.
EVOLUTION OF THE COMMITTEE’S MODEL
The committee sought to develop a model of health that depicts how a variety of influences interact over time to produce health. One model that reflects considerable progress in this regard is put forward in Healthy People 2010 (U.S. Department of Health and Human Services, 2000) (see Figure 2-1). It shows the interaction of biology and behavior and the interactions of the physical and social environments on both. It also reflects the influence of public policies and interventions and of access to quality health care on the health of individuals and groups.
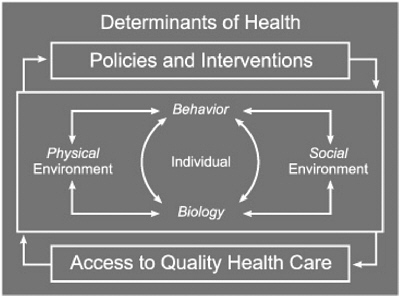
FIGURE 2-1 Model used by the Healthy People 2010 report.
SOURCE: U.S. Department of Health and Human Services (2000, p. 30).
For the committee, the model falls short for use with children because it does not reflect the dynamic and developmental nature of children’s health and is too narrow in its view of determinants or influences on health; for example, it fails to articulate the importance of cultural factors or to recognize the importance of services other than health care. Health results from complex interactions of many aspects of the child’s environment, genetic endowment, and behavioral responses that constantly influence and affect one another. Several principles of this dynamism are critical to a full model of children’s health.
Health and Development
Development is important in the biological and behavioral processes that determine health capacities, optimize function, preserve health, and lead to the presence or absence of disease throughout life. Cumulative experience, inherent adaptive capacities, dynamic interactions with physical, social, and cultural environments, and genetic predisposition all interact to determine developmental trajectories (Institute of Medicine, 2001b; National Research Council and Institute of Medicine, 2000; Hertzman, 2000; Halfon and Hochstein, 2002). A growing body of scientific research specifies the biological mechanisms and physiological
pathways that determine the way health develops (Halfon and Hochstein, 2002; Keating and Hertzman, 1999). Early health is an influence on future health. Health and health influences interact throughout childhood. Several considerations relevant to children’s health are developmental in nature: critical and sensitive periods in children’s development, the importance of timing and multiple time frames, the age-specific patterns and distributions of children’s health influences, the importance of transitions, and the long reach of childhood.
Sensitive and Critical Periods
Children’s development includes both sensitive and critical periods. Sensitive periods refer to times when a child is especially receptive to certain kinds of environmental influences or experiences, good or bad, and the ideal time to provide or to avoid them. Critical periods refer to times when certain experiences or influences have a deterministic (positive or negative) effect; the health effect would not occur from the same exposures at other times (Ben-Shlomo and Kuh, 2002).
Many examples of influences on children’s health have vastly differing effects at different developmental ages and stages. Although the terms sensitive and critical are used interchangeably in this report, the committee recognizes that there are relatively few, if any, critical periods outside the biological area. Examples of critical developmental periods include exposure to specific influences during fetal development (e.g., rubella, folic acid, ionizing radiation) or during adolescence (e.g., mumps). The need for appropriate stimulation and interaction in infancy and early childhood in order to develop appropriate vision, language skills, and attachment is an example of a sensitive period. The timing of experiences and exposures to certain health influences are important considerations when assessing children’s health. In addition, exposures and experiences during sensitive and critical periods affect not only the current health of children but also their future health and functional capacities.
Timing and Multiple Time Frames
The timing of specific influences on the development of health conditions and health trajectories is important to consider when measuring children’s health (Halfon and Hochstein, 2002). Assessment of health at a single point in time provides only a snapshot of a dynamic process. It is also important to consider the developmental trajectory of the health of a child over time, both for individuals and within groups. What may appear as good or impaired health at one stage may change over time. Some influences may exert their effects rapidly, while others remain latent and alter subsequent health or cumulate (often in conjunction with other influences) to manifest their effects much later in life.
Patterns and Distribution of Children’s Health Influences
The patterns and distribution of children’s health influences are age specific. A child’s development occurs explosively in the first years of life, gradually becomes slower with advancing age, and again accelerates during adolescence, so that their relative salience varies with age or developmental stage (Bogin, 2001). For example, in young children, family-related influences are a major factor on health and development, with neighborhood, schools, and peer group playing a greater role as individuals age (Nordio, 1978; Rutter et al., 1997; Wadsworth, 1999; Halfon and Hochstein, 2002).
Transitions
Transitions present special challenges and windows of opportunity. As children move from one stage to another, new demands and stresses may influence their health. At several points (e.g., birth, entry into school, puberty) children must negotiate new environments that challenge adaptive mechanisms in new ways. At the same time, transitions provide an opportunity for growth and mastery and are critical times for interventions (Baltes, 1997; Brazelton, 1995; Graber and Brooks-Gunn, 1996).
The Long Reach of Childhood
There is growing awareness that childhood has a long reach on future health. Several recent reports have emphasized the importance of prenatal and early postnatal development on lifelong health and well-being (Institute of Medicine, 2001b; National Research Council, 2001). For example, birthweight has been shown to be directly related to later cardiovascular disease (Barker, 1998; BenShlomo and Kuh, 2002).
Influences on Health Are Multiple, Interactive, and Changing
In the committee’s view, another set of changes to the model of children’s health should adequately represent the multiple and interacting influences on health.
Multiple Influences
At any given time, multiple present and past influences affect children’s current health. Health results from the interaction of genetics and children’s environments. As discussed in Chapter 3, there are many ways in which the environment interacts with and affects the expression of genetic potential, or vice versa. While biological, psychological, behavioral, social, cultural, economic, and physical in-
fluences are individually important, these factors usually do not operate alone, but interact with one another over time (Engle, 1977; Sameroff and Fiese, 2000). Factors in the social, physical, and cultural environments can influence individual biological and behavioral manifestations of health, suggesting that biology and behavioral outcomes are not often independent (Institute of Medicine, 2001b). Our model presents the multiple influences on children’s health in the following categories: children’s biology and behavior; their social environments, including family, community and culture; their physical environments; services; and policy.
Influences Interact
Multiple influences co-occur and interact over time. Individuals influence and are influenced by their families and the social networks and organizations in which they participate (e.g., child care, schools, places of worship), the community of which they are part, and the society in which they live (Institute of Medicine, 2001b). This concept of intertwined influences (Bronfenbrenner, 1979; Bronfenbrenner and Ceci, 1994; Boyce et al., 1998) also captures the dynamic interactions among these constantly changing and interacting contexts.
Evidence from research on human development indicates that these multiple contexts broaden and deepen for individuals as they age, serving to channel and reinforce influences into developmental pathways (Boyce et al., 1998; Dawson et al., 1994, 2000; Halfon and Hochstein, 2002). Many influences co-occur, so that the effects of poverty, for example, may occur through multiple factors, such as poor nutrition, educational opportunity, and neighborhood violence (Bronfenbrenner and Ceci, 1994). The nature and strength of such interactions differ across the life span, and early influences may set in place a series of vulnerabilities and strengths that change the effects of later influences.
A NEW CONCEPTUAL MODEL
To more accurately reflect the dynamic process of multiple, interacting influences from which children’s health evolves, the committee proposes a new conceptual model. Our model builds on the categories of Healthy People 2010 but adds to them and views them as a kaleidoscope. In a kaleidoscope, individual pieces of colored glass are arrayed in a fixed form but in a variety of colors and shapes based on how the specific colors and shapes of glass interact when the kaleidoscope is turned. So too do the results of specific influences on health change as the influences change and interact over time and throughout development to produce health (see Figure 2-2).
In our model, the various influences are presented as overlapping circles that interact within the broader context of policy and services. The relative importance of individual influences varies over time as children move into new developmental stages and the influences interact; the pattern of health that emerges
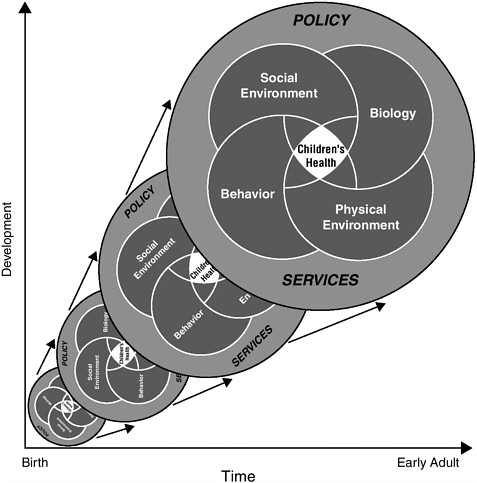
FIGURE 2-2 A new model of children’s health and its influences.
also varies. The model illustrates that the effect of influences will vary based on both time and stage of development. Since development is an uneven process, with periods of rapid growth and periods of relative quiescence, it is not synonymous with time, nor is it the same from child to child, and the interaction of various influences changes with both time and developmental stage.
As children age, the kaleidoscope turns and the patterns change, reflecting their changing health. At some ages, these turns are very rapid, reflecting substantial developmental change; at others they are less so (though still more rapid than in adults). Each turn incorporates the previous elements, including the child’s former health, and casts them in new light. All affect the child’s present and future
health into adulthood and old age. Because this notion of health is not static, multiple time frames must be addressed. With each turn of the shaft, the pattern will be altered, if only slightly; some effects may not manifest until later in a child’s life. The spheres, representing influences, overlap each other so that the final pattern is not just a collection of distinct health influences, but rather a display of the interactions among the spheres of influence. The relative salience of different influences also varies by developmental stage. Although the figure shows each sphere to be of equal size, the relative sizes of the spheres are dynamic.
Criteria for the Measurement of Children’s Health
The criteria used in other national, state, and local health measurement initiatives can inform understanding of how health is and should be measured. Certain common criteria emerge from a review of several of these other efforts as useful guideposts for selecting individual domains and indicators as well as in selecting a set of indicators (Institute of Medicine, 1999, 2001b; National Committee for Quality Assurance, and others). The committee has adopted a common set of criteria for guiding the selection of domains and indicators and for assessing the gaps that currently exist in the information collected on children’s health. Thus, measures of children’s health (domains and indicators) should be important, valid and reliable, meaningful, culturally appropriate and relevant, sensitive to change, and feasible to collect.
-
Important—the domains and indicators should account for all important aspects of current or future health outcomes.
-
Reliable and valid—measures should be reproducible over repeated measurements and observers. Validity implies that a measure has meaning in terms of the intended concept in a way that meets several different types of scrutiny.
-
Meaningful—domains and indicators should capture the special health attributes of children including their developmental vulnerability and potential, patterns of morbidity and mortality that distinguish children from adults, as well as their evolving independence. They should also provide a way to assess and track disparities that may start in childhood and be compounded over time.
-
Culturally appropriate and relevant—measures should reflect the full array of health as understood by different subgroups and should be psychometrically demonstrated to assess comparable domains across groups.
-
Sensitive to change—measures should be sufficiently sensitive to measure meaningful changes. For example, a measure that would distinguish only between alive and dead would have relatively little use in assessing the changes in health of a child or group of children over time.
-
Feasible to measure—measures should be sufficiently useful and practical for information collection that they generate a constituency that has the political will to use them.
Measurement of Children’s Health
Additional features are crucial for the measurement of children’s health to be useful from a policy perspective. In the committee’s view, any approach to measurement should:
-
Contend with the relationships between health at one point in time and future prospects (health expectancy).
-
Allow for gradations of measurement, as well as thresholds that can be used to facilitate decisions about which individuals or populations are in need of intervention. Thus it should be useful at different points on the spectrum, for example from excellent to poor health.
-
Track changes in children’s health over time and consider developmental stages.
-
Be developed in a manner that protects privacy and confidentiality.
As this report makes clear, few measures currently meet these standards.

















