
3
Influences on Children’s Health
Children’s health is determined by the interaction of amultitude of influences, reflecting complex processes. We divide these influences into biological, behavioral, and environmental (physical and social) even though our model of children’s health views their effects as highly intertwined and difficult to isolate. This chapter provides a summary of published literature and a framework for understanding those influences.
OVERVIEW
Biological influences as discussed in this chapter include genetic expressions, prenatal influences, as well as biological constraints and possibilities created by perinatal and postnatal events plus prior states of health. Behavioral influences include the child’s emotions, beliefs, attitudes, behaviors, and cognitive abilities that affect health outcomes. Environmental influences are wide-ranging and include infectious agents, toxins such as lead and air pollution, and social factors such as loving interactions with caregivers, socioeconomic resources in the family and community, and peer relationships, segregation, racism, culture, the availability and quality of services, and policies that directly or indirectly affect these other interactive influences (see Box 3-1).
The role and effect of biological, behavioral, and environmental influences change as children grow. For example, a pharmacological agent like thalidomide is highly toxic within a narrow window during pregnancy but not afterward, an attachment to a caring adult is especially critical during infancy, and peer influences appear to grow steadily from toddlerhood through adolescence. Even within
|
BOX 3-1 Children’s biology Children’s behavior Physical environment
Social environment
Services Policy |
a childhood stage, health influences can act in very different ways because of the differing cultural interpretations that families attach to them.
While biology, behavior, and environmental categories are useful for organizing our discussion, it is important to understand that healthy development is not the product of single, isolated influences or even types of influences. Warm and nurturing parenting is an important family influence, but prematurity or visual impairment can make an infant unresponsive to a mother’s initial nurturing. Mothers may react with apathy or disinterest, which produces even more withdrawal on the part of the infant (Lozoff, 1989). While simplified schematics or models help to organize understanding of the influences on children’s health both during childhood and beyond, life is not as simple as these models suggest.
One caveat should be kept in mind in reading through the following review of evidence. Few of the cited studies drew their evidence from randomized experiments. And few if any of the nonexperimental studies included all relevant variables in their data and analyses. Thus, the findings reported in these studies are likely to suffer from exclusion of potentially important categories of influences, so that the associations that are reported as being important may be due to their associations with a more important or equally important characteristic, or due to interactions with other types of factors so that their effect may be manifested
primarily or only in certain population groups. A related problem is that few of the cited studies include data that represent the whole population of children. Thus, the findings that are reported as significant may be significant only in the population studied or similar populations. Nonetheless, the committee found the evidence to be sufficiently compelling to warrant inclusion when there was a plausible, well-supported connection between the influence and health.
Moreover, inferences about the relative importance of the variety of influences are heavily dependent on the nature of the theoretical models that underlie statistical analysis. If more proximal influences are mixed with more distal ones, they may appear to have stronger effects, even in situations in which more distal factors are operating on a multiplicity of proximal influences and therefore have cumulatively greater effect overall. Thus, future research should adapt more appropriate pathway techniques to help to sort out the patterns by which the influences interact to produce different states of health.
Finally, the relative lengths of the following sections are not meant to signify the relative importance of the influences. For some, the prevalence is less well known than for others. From the viewpoint of influences on population or subpopulation health, the relative frequency of the different influences is at least as critical as the degree of the risk that they pose to individuals. Additional research is needed to refine understanding of the relative contribution of each of the influences and the relevance of each across a variety of social and cultural groups.
CHILDREN’S BIOLOGY
A child’s biology determines how physiological processes unfold and how organ systems adapt to outside influences. Biological response patterns, including responses to stress, novel situations, and primary relationships, can directly and indirectly influence other biological, cognitive (learning), and behavioral processes. The term “biological embedding” has been used to describe how the external environment influences and shapes the biological environment (including the central nervous system), which in turn changes the way the individual interacts with the external environment (Hertzman, 1999).
Genes
DNA provides the blueprint for life. The units of heredity, or genes, are specific sequences of DNA that code for proteins that affect the particular physiology and anatomy of an individual. All cells contain the full array of genes but, depending on the cell type, some are expressed while others are not; for example, certain genes coding for proteins in the retina are expressed in the cells of the eye, but not in the pancreas cells.
Disruptions in genes can be caused by events before, during, or after conception and may produce disorders immediately or later in life. A parent can pass on
a defective or abnormal gene or set of genes, a malfunction can occur during combination of maternal and paternal DNA, or exposure to an outside substance or condition can occur after conception that alters the genes in the fetus. Physical and social environments (e.g., family, community, school, culture) interact with and influence these biological processes.
Influences of Genes on Responses to Different Environments
Classically, genes have been considered to be the “instructions” for building proteins, although it is clear now that they have other functions as well. A gene may affect health as a result of the interaction of its protein product with another aspect of a child’s biology. The combinations of these interactions may result in an enhanced, worsened, or inconsequential change in health status. For example, sometimes an alteration in the gene (i.e., mutation) is identified due to the presence of a particular disease state, or it can be deduced that an individual with the mutation has a high probability of developing a particular disease. Understanding the biological pathway of the disease and its interactions with other biological processes facilitates treatment options by modifying the causal path. In the case of Huntington’s disease, for example, the disorder appears to be in part mediated by glutamate excitotoxicity; giving patients a substance that blocks this effect (glutamate receptor antagonists) interrupts this pathway and may retard the manifestation of the disease (Ferrante et al., 2002). The influence of genes on health always exists in an environmental context; in the next sections we describe how genes affect behavior and the physical and social environments.
Genes and Behavior. That genes affect behavior has been amply demonstrated in honeybees (Ben-Shahar et al., 2002) and higher animals (Ruby et al., 2002; Chester et al., 2003; Hendricks et al., 2003). Examples in humans are being rapidly discovered, including genes that influence the relationship between exposure to trauma and susceptibility to posttraumatic stress disorder (Stein et al., 2002), genetic polymorphisms that protect against alcoholism (Wall, Carr, and Ehlers, 2003), mutations that result in sleep disorders (Wijnen et al., 2002), and several genes that are associated with simple phobias (Gelernter et al., 2003).
Genes and the Physical Environment. The physical environment includes ubiquitous agents (e.g., ultraviolet light, amino acids and sugars in the diet, noise, speech) and somewhat less universally encountered ones (e.g., loud music, medications, pollutants). Some genes result in poor outcomes following common environmental exposures (e.g., phenylketonuria with phenylalanine, galactosemia with galactose, xeroderma pigmentosa with ultraviolet light exposures). Individuals with these genotypes are likely to be affected by the disease because they have a high chance of being exposed to the physical environmental agent. In some cases, the physical environment can be modified to improve outcomes
(e.g., a phenylalanine-free or galactose-free diet may improve IQ, no sunlight or ultraviolet exposure may reduce skin cancers). There are also gene alterations resulting from uncommon physical environmental exposures that affect health. Examples include a higher risk of lung cancer in individuals lacking glutathione S-transferase mu who smoke (Perera et al., 2002) and noise-induced hearing loss in some individuals exposed to high levels of noise—the gene or genes in this case are just being discovered (Kozel et al., 2002). These genes are known as susceptibility genes. An example of a positive susceptibility gene to a physical environmental agent may be that for perfect pitch. It appears that individuals with exposure to music and a family history of perfect pitch are more likely to acquire perfect pitch (Alfred, 2000).
Genes and the Social Environment. The identification of genes that confer susceptibility to adverse or beneficial responses following exposure to diverse social environments has only just begun. In one study, abused children with a genotype conferring high levels of neurotransmitter-metabolizing enzyme monoamine oxidase A expression were less likely to develop antisocial problems in adulthood (Caspi et al., 2002). The risk of developing alcohol abuse or dependence also appears to have both a genetic susceptibility and a family influence (Macciardi et al., 1999; McGue et al., 2001), as does the risk for relapse and poor outcomes with schizophrenia (Campbell, 2001).
Characteristics of Gene-Environment Interactions
The expression of certain genetic characteristics depends on the environment in which they occur. Thus, gene expressions that lead to a disease in one context may not lead to a disease, or may result in a different disease, in another context (Holtzman, 2002). Inheriting a single copy of the hemoglobin S gene makes an individual resistant to malaria (Aidoo et al., 2002). However, inheriting two such genes gives the individual sickle cell anemia, a severe disease. Outside of malaria-endemic areas, sickle cell trait, the inheritance of one copy of hemoglobin S, has no known adaptive benefit and may be maladaptive. A single cystic fibrosis gene has been postulated to be protective against diarrheal diseases such as cholera, conferring a survival advantage to individuals who carry one copy of the gene (Rodman and Zamudio, 1991). However, individuals with two such genes have cystic fibrosis, a severe disorder with altered pulmonary and gastrointestinal function. Other examples of genes with positive influence also exist in given environments. The gene or genes that confer protection from cancer (Gonzalez et al., 2002; Reszka and Wasowicz, 2002) have been described.
Genes may confer susceptibility only during a specific span of time, referred to as a critical period. For example, 20 percent of children are extremely sensitive to thalidomide during a critical 15-day period from day 20 to day 35 of gestation, although the gene or genes responsible for this enhanced sensitivity have not yet
been identified (Finnell et al., 2002). Presumably there are narrow windows of rapid development throughout childhood, including puberty, but critical windows of sensitivity to disruption have not been adequately described (Selevan et al., 2000). The complex interrelationships between genetics and environmental stimuli are not clearly defined and are an active area of current research.
Gene Expression
Understanding of the genome has rapidly expanded the study of the ways in which genes interact with diverse influences (e.g., physical and social environments) to affect health. Expression of genes (the amount of the protein encoded for by the gene) has a profound influence on the health of the individual. Gene expression is determined by many factors, such as promoters, regulators, mutagens/carcinogens/teratogens, X-inactivation, message stability, rate of protein degradation, prior exposures, all of which are affected by the environment. Interactions between genes and the environment influence different physiological pathways and adaptation (Holtzman, 2001) and may lead to adaptive or maladaptive phenotypes. An interesting example is the hygiene theory of childhood asthma, which postulates that children living in hygienic, low-pathogen environments develop an imbalance between two types of immune cell classes (TH1 and TH2). Children with an imbalance of TH1 and TH2 are more likely to develop allergies and asthma when confronted with allergens. When children live in low-hygiene, high-pathogen environments, they develop a strong system of immune regulators (a balance between TH1 and TH2 cells), and they are less likely to develop allergies or asthma (Yazdanbakhsh et al., 2002). Children living on farms or in homes with at least two cats or dogs in the first year of life have been shown to have significantly lower rates of allergic sensitization tested at 6–7 years (Ownby et al., 2002).
Healthy development depends on gene expression being responsive to changes in the environment. For example, the radical change in the environment at birth is responsible for changing the expression of genes to enable the baby to make the transition from intrauterine to extrauterine life. These include the production of proteins that close the ductus arteriosus (Kajino et al., 2001), alter lung liquid absorption (Matalon and O’Brodovich, 1999), produce barrier function in the skin (Harpin and Rutter, 1983), produce immunoglobulins, and alter gene expression in brain development. Thus, to be healthy, newborns must make profound changes in gene expression as they transition from intrauterine to extrauterine environments.
Converging findings from genetics and molecular biology demonstrate that a host of internal and external signals can stimulate or inhibit gene expression, including subtle factors such as the light-dark cycle (Hegarty, Jonassent, and Bittman, 1990) and tactile stimulation (Mack and Mack, 1992). This pattern of contingency is now recognized as part of the normal process of development in
embryology and developmental biology, and there is a growing body of literature demonstrating how factors, including internal neural and hormonal events and external sensory events, activate or inhibit gene expression during individual development (see Davidson, 1986, 2001; Gilbert, 2000; Holliday, 1990).
Body Stores
Chemicals in the environment (air, water, dirt, dust, food) move into the body across such biological barriers as skin, lungs, and the gastrointestinal system. Exposure is considered to be contact of the agent with the biological barrier; following exposure, the agent crosses the barrier and is found inside the body (the internal dose). After uptake or absorption across the barrier, chemical agents (including drugs) are distributed throughout the body, metabolized, and eliminated (U.S. Environmental Protection Agency, 2003; Atkinson et al., 2001).
The rate of elimination varies substantially for different agents; some are eliminated in a matter of minutes; others may be found in the body for years following exposure. The amount of chemical/biochemical/vitamin/mineral stored or measured in the body is called the “body stores” or “body burden” of that agent. The committee has adopted the term “body burden” in this report. Body burdens of a chemical or drug represent the amount of cumulative exposure and, in some instances, can be transferred to another individual (e.g., from a mother to the fetus or infant through the placenta or in breast milk).
Body burdens can improve or harm health, based on their biological characteristics and presence during certain periods of development. Maternal body burdens of either lead or polychlorinated biphenyls (PCBs) impair the cognitive function of offspring if present during critical periods during fetal development (Gomaa et al., 2002; Lai et al., 2002). A body burden of lead in the bones of young children has been associated with poor social behavior (Needleman et al., 2002; Wald et al., 2001), poor cognitive performance or development (Lanphear et al., 2003; Rogan and Ware, 2003), and impaired pubertal progression (Selevan et al., 2003). The relative impact of body burdens varies with developmental stage. Relatively lower body burdens of organic mercury will reduce cognitive development in young children more than at older ages (U.S. Environmental Protection Agency, 2000c; National Research Council, 2000).
Some body burdens can have positive impacts on healthy development. For example, maternal body burdens of folate during the early first trimester of pregnancy significantly reduce the risk of a baby with a neural tube defect (Wald et al., 2001). Adolescents with higher levels of folate also have a significantly decreased risk of juvenile hypertension (Kahleova et al., 2002), and adults with high folate stores appear to be at substantially lower risk of cardiovascular disease (Wald, Law, and Morris, 2002). Some body stores that are beneficial at lower levels can become harmful at higher levels: a baby’s appropriate body burdens of iron will improve cognitive outcome, but an inappropriately high body burden of iron
potentiates oxidative stress (Rao and Georgieff, 2001) or can cause iron overload disease. Low maternal or fetal levels of vitamin A are associated with developmental disease, as are high levels.
The impact of some body burdens vary across time and, to be understood, must be assessed at different times. For example, a maternal body burden of PCBs causes exposure to both the fetus and to the newborn via breast milk. Body burdens at one time may also impact measures of health in later time frames. A child who has received treatment for Hodgkin’s lymphoma, increasing the genotoxic body burden, is at risk for secondary cancers (Hack et al., 2002).
Early Programming
While not without controversy (Huxley et al., 2002), there is a growing literature on the potential role of “perinatal programming,” referring to the processes in which specific influences during critical or sensitive periods of development can have lifetime consequences by altering metabolic pathways and other physiological systems. This appears to be a special case of the more general phenomenon of how environmental influences can be embedded in biology during critical and sensitive periods of development.
In humans, the relationship between fetal growth, postnatal growth, and the risk of such diseases as hypertension, coronary heart disease, and non-insulin-dependent diabetes have been frequently studied (Bertram and Hanson, 2002; Barker, 1998). Both human epidemiological and animal experimental studies support the hypothesis that relative undernutrition in the fetus results in significant and relatively permanent changes in important physiological systems (Nathanielsz, 1999). Perinatal programming indicates that sensitive or critical periods of development may have lifelong effects and influence the development of chronic diseases later in life (Ingelfinger, 2003). However, it does not discount the potential effect of the external environment (Seckl, 1998; Ingelfinger and Woods, 2002; Falkner, 2002; Roseboom et al., 2001) in modifying the effects.
Fetal undernutrition is believed to induce persistent changes in several metabolic pathways, but the exact mechanisms are only now being pieced together through a range of animal experiments and human measurement studies (Seckl, 1998; Barker, 1998). Because it is likely that events occurring at other times modify prior influences, there is a growing interest in understanding the predisease pathways and biological changes that occur prior to the recognition of a vast array of clinical outcomes. Currently many of these predisease markers are either below current limits of detection or produce changes that are not currently measured on a routine basis (Lucas et al., 1999; Keller et al., 2003; Ingelfinger, 2003).
Examples of such programming during particular sensitive or critical periods of development are coming to light. For example, low numbers of nephrons are associated with hypertension, and it has been shown that individuals whose mothers experienced severe protein-calorie malnutrition during the third trimester,
when nephron development takes place, are most at risk of hypertension (Roseboom et al., 2001; Keller et al., 2003). Outcomes associated with programming early in life may also promote health. For example, rats receiving high levels of licking and grooming as pups are less fearful compared with rats that received low levels of licking and grooming (Francis et al., 2002). The mechanism for this change in behavioral programming appears to be the influence of maternal licking on gene expression during a critical period of development and subsequent changes in the development of synaptic receptor sites for specific neurotransmitters (Francis et al., 1999).
Similar environmental influences on the development of behavioral pathways have been described in rhesus monkeys (Champoux et al., 2002), and studies of premature human infants show substantially greater increases in body weight after introduction of massage therapy (Field, 2002). In contrast, disruption of maternal bonding during infancy has been shown to have profound negative effects on later relationships (National Research Council and Institute of Medicine, 2000).
CHILDREN’S BEHAVIOR
As used in this report, behavior refers to a child’s emotions, beliefs, cognitions, and attitudes, as well as his or her overt behaviors. Some behaviors are planned and deliberate; others are reflexive, impulsive, and contingent on environmental circumstances. A child’s emotions, beliefs, and attitudes affect health, principally through the way they modify a child’s explicit and overt behaviors, such as his or her health and life-style choices. These in turn alter the child’s eventual health outcomes. Examples include social and interactional behaviors (e.g., compliance with parental requests, peer interactions), health preventive behaviors (e.g., avoiding smoking, driving with a seat belt, choosing good friends), or illness-management-related behaviors (e.g., behavioral adherence with a treatment regimen or health care appointments).
Health-related behaviors may be health promoting (those that increase the likelihood of future health, such as regular balanced diet and exercise) or health impairing (those that adversely cause actual morbidity or mortality, such as smoking, drinking, or reckless driving). A body of recent research suggests how these behaviors develop and describes the role of family, peers, and social environment, including media, in shaping this developmental process (Tinsley, 2003). While behaviors like smoking, drinking, and exercise are known to affect later health, it is not clear how these behaviors develop in childhood (McGinnis and Foege, 1999).
Often these health behaviors are considered proxies for health, even though they may not necessarily constitute health per se. Some health policies attempt to change youth behaviors that are thought to affect health. An example is the re-
quirement for regular school attendance, which may both reflect current health and exert effects on a given child’s likelihood of future health.
Behavioral influences on children’s health are often reciprocal, both influencing and influenced by parents, peers, and others. For example, parenting style, family traditions, and peer influences affect not only fairly simple youth behaviors, such as compliance with behavioral requests or participation in health prevention programs (Patterson and Fisher, 2002), but also more complex behaviors, such as participation with disease management regimens. This section focuses on the internal psychological factors that underpin children’s behavior, with implications for subsequent health outcomes.
Emotions, Attitudes, and Beliefs
In addition to the influence of explicit behaviors on health, a child’s internal emotional, attitude motivation, or belief states may exert effects on health. For example, research on both adults and children has shown direct relationships between internal attitudinal and personality factors and health outcomes, perhaps through mechanisms that link internal emotions, attitudes, and beliefs with stress reactions and immune responses (Berry and Worthington, 2001; Herbert and Cohen, 1993; Kiecolt-Glaser, 1999, Lawler et al., 2000). Thus, external events perceived as stressful by a child may function as triggers for an asthma or inflammatory bowel disease flare, over and above any biological exposure or adherence to therapy (Rietveld and Prins, 1998; Santos et al., 2001). Presumably such effects are conveyed through a child’s emotional arousal states, which in turn result in physiological changes, such as increased pulse and elevated blood pressure, glycemic, and immune responses. This research has solid empirical support in both the adult human and animal research fields (McEwen, 1998; Seeman et al., 1997), but it is less firmly established for children.
Behavioral Adaptations
The hallmark of childhood is the constant exposure to new developmental challenges. As children acquire new physical and cognitive skills and experiences, their behaviors change. They explore, practice, and experiment and as a result they change and are changed. The resulting behaviors are both manifestations of their health and have significant implications for it. At each new exposure, the child may respond in a variety of ways that in turn unleash a variety of reactions in his or her caregiver and in others around him.
From birth, infants recognize, prefer, and are soothed preferentially by their mother’s voice (Mehler et al., 1978; DeCasper and Fifer, 1980). They suckle more in response to it (Mehler et al., 1978), and mothers in turn are gratified by their ability to sooth their children (Klaus et al., 1972). Thus the beginnings of attachment are initiated. As an infant continues his or her explorations and trials, which
themselves influence health, they produce reactions from caretakers that in turn further affect the infant’s behavior and health. One of the first developmental challenges faced by an infant is adaptation to extrauterine life. Low-birthweight infants experience more difficult transitions and are more likely to be fussy during social interactions and less likely to smile and vocalize (Beckwith and Rodning, 1992; Barnard and Kelly, 1990). These infant reactions in turn impose stresses on the parent, which may affect the child’s health through impaired attachment. If the parent responds in a fashion that induces further stress in the infant, the increased stress in turn may affect the infant’s ability to secrete adequate amounts of growth hormone (Skuse et al., 1996), potentially leading to growth impairment or failure to thrive.
Attempts to make this transition are met with a variety of parental and cultural responses, all of which influence infants in ways that facilitate or impede their development. Nearly a quarter of infants respond to new stimuli in a negative fashion (Kagan et al., 1998); their early infancy imposes a series of challenges that are especially daunting and many are found to still be socially wary and exhibit evidence of physiological stress at age 6 years (Kagan et al., 1987).
Emotional development and the establishment of social relationships are among the greatest challenges of infancy and early childhood. Emotions are fundamental for human attachments, social interactions, and self-satisfaction. Therefore, the extent to which infants evoke sympathetic and empathetic emotions in others and eventually develop these emotional expressions themselves greatly influences their subsequent health. Children who do not attain these skills are more likely to encounter rejection from caretakers and peers (Dodge et al., 2003; Schultz et al., 2000). The complex interplay of genetics, parenting, and societal reactions illustrates just how precarious the early years are and how central infant behavior is for subsequent health (Rutter, 1998).
Attitudes, Beliefs, and Circumstances
The effects of individual, family, and community attitudes and beliefs on health behavior have been well described. A substantial body of research has been conducted on issues related to adherence to treatment regimens, both among parents of younger children and among adolescents (McQuaid et al., 2003; Volovitz et al., 2000; Davis et al., 2001). This work focused initially on asthma and diabetes and more recently on substance use and HIV/AIDS treatment (Manne, 1998). Current research is informed by several related theoretical models of behavior, all of which take into account youths’ attitudes, beliefs, and subjective perceptions about the risks of negative outcomes, as well as the perceived benefits and difficulties of treatment (Hochbaum, 1956; Ajzen, 1991; Rogers, 1983; Bandura, 1994).
In accordance with these models, data suggest that both parents’ and youths’ attitudes are moderately predictive of subsequent health care behaviors, whether
in the context of seizures (Kyngas, 2001; Kyngas et al., 2000), asthma (Kyngas, 1999), diabetes (Wysocki et al., 2000; Ott et al., 2000), or sexual risk avoidance (Stanton et al., 1996; St. Lawrence et al., 1995; Jemmott and Jemmott, 1994).
These conceptual considerations lead directly to specific interventions, such as motivational enhancement strategies to encourage youths’ substance abuse treatment compliance (Carroll et al., 2001), engaging them in sexual risk prevention activities (Stanton et al., 1996; St. Lawrence et al., 1995), and using collaborative goal-setting strategies in enhancing adolescent diabetes self-care (Delamater et al., 2001). In addition, these theories help explain why and how child compliance may be positively (or adversely) affected by peer and family support (LaGreca and Bearman, 2002; LaGreca et al., 2002; Liss et al., 1998), as well as the support available through a good relationship between the youth and his or her health care team (DiMatteo, 2000; Kyngas et al., 2000). The effect of and the need for support may vary as a function of age (Steinberg, 1999).
Research has documented the impact of chronic illness on child and adolescent adjustment (DiMatteo, 2000; Kyngas et al., 2000). Not infrequently, depression, anxiety, low self-esteem, or other adjustment difficulties may ensue as a result of the underlying illness, increasing risk for treatment nonadherence (Wise et al., 2001; Murphy et al., 2001; Davis et al., 2001) or worsening the outcome of the primary illness (Kuttner et al., 1990; Hauser et al., 1990). Available evidence suggests that good communication skills and the development of positive relationships with the clinical team may offset the effects of negative emotions on health care adherence (Buston, 2002; García and Weisz, 2002; Shaw, 2001).
Emotion, Cognition, and External Influences
The importance of cognitive ability and understanding inappropriate health-related behaviors must also be considered. Children’s ability to understand safety rules and health behaviors increases with age (Morrongiello et al., 2001). Over time they acquire the capacity to conceptualize and understand the longer term consequences of their behaviors on their health (Thomas et al., 1997). Conversely, children with developmental disabilities or impaired language ability often show increased difficulties in adhering to necessary behaviors, including health-maintaining ones (Stansbury and Zimmerman, 1999).
While attitudinal, motivational, cognitive, and emotional factors may all exert direct effects on health-related behaviors, the role of environmental factors in these behaviors should not be underestimated. For example, under some circumstances, behavioral factors may contribute less to youths’ actual health care behaviors than making available a more easily used medication, such as a long-acting form of medication in the case of birth control (Stevens-Simon et al., 2001; Omar et al., 2002) or providing more stable living situations in the case of adolescents’ likelihood of adhering to an HIV/AIDS drug regimen (Conanan et al.,
2003). In addition, children’s behaviors may directly affect parents’ ability to adhere to a treatment regimen (Searle et al., 2000), just as parental response styles may affect the likelihood of a child’s complying with specific requests (Patterson and Fisher, 2002).
Cultural construction of health and disease may also affect compliance with certain treatments by both parents and children. For example, in many cultures, so-called teething diarrhea is considered to be a normal part of growth and development and thus health-seeking behavior or adherence to treatment regimens for the “illness” would be unlikely (Stanton et al., 1992).
In sum, all these psychological factors, whether a child’s perceptions of peer norms, self-efficacy beliefs, attitudes about health and health care, or level of motivation to pursue specific health care behaviors, contribute to health-related choices and behaviors. With increasing age, children’s behaviors, such as substance use, academic performance, violence, suicide, and auto accidents, constitute a major influence on future health. According to findings from the Global Burden of Disease study, these behavioral aspects of health are likely to exert even greater prominence in coming decades, as behavioral and life-style-related health conditions (e.g., auto accident injuries, consequences of smoking, depression) increase in their relative effect on children’s health and illness (Murray and Lopez, 1996).
Complicating this point, however, is the fact that certain behaviors and emotions can serve both as health influences and outcomes. Determining when a behavior is an influence rather than a health outcome can be difficult, because children’s current behaviors can affect both future behaviors and subsequent health outcomes. Regardless of the classification and especially due to the inability to distinguish behaviors as health influences or outcomes, data on children’s health behavior are an important component of a system that seeks to track child health and health behaviors.
PHYSICAL ENVIRONMENT
The physical environment affects children’s health by exposing them to a wide variety of external conditions. These include chemical, biological, and physical influences that exert their impact by being taken into the body (e.g., lead, methyl mercury, persistent organic pollutants) or interacting with body surfaces (e.g., ultraviolet light, physical abuse, particulate matter in air pollution) or the senses (e.g., noise, odors). The built environment affects the ways in which children are differentially exposed to some of these influences. Exposure is the sum of all exposure factors over the course of time, including the home, school, child care, and play areas. Exposures during the prenatal period can also affect children’s health.
Prenatal Exposures
Although exposures of the ovum or the sperm prior to conception may have profound health effects on a child, including development of an abnormal fetus,1 in this section we focus on prenatal influences. In most cases, exposures of the fetus are from maternal exposure. Exposures of the mother during pregnancy can come from many sources; common sources include maternal occupation, substance use, diet and water consumption, and paraoccupation (occupational chemicals or other hazards brought home by other family members). The strongest workplace exposure associations are lead, mercury, organic solvents, ethylene oxide, and ionizing radiation and poor reproductive outcome, including birth defects (Agency for Toxic Substance and Disease Registry, 1993; Schardein, 2000).
Use of tobacco, alcohol, and illicit drugs also have harmful effects. Tobacco use during pregnancy is a major cause of fetal and newborn morbidity and mortality (small for gestational age, persistent pulmonary hypertension, sudden infant death syndrome, poorer intellectual functioning) (Nicholl, 1989; Golding, 1997; Day et al., 1992; Kline, 1987; U.S. Environmental Protection Agency, 1992; Bearer et al., 1997). Heavy drinking during pregnancy is the cause of fetal alcohol syndrome (FAS), the leading known cause of mental retardation (Abel and Sokol, 1987; Sokol, Delaney-Black, and Nordstrom, 2003). Conservative estimates place the incidence of FAS at 0.33/1,000 live births (Abel and Sokol, 1991). More common effects include alcohol-related birth defects, alcohol-related neurodevelopmental defects, and subtle effects on a variety of behavioral, educational, and psychological tests resulting from low to moderate levels of drinking during pregnancy (Institute of Medicine, 1996). While the effects of maternal prenatal use of cocaine, opiates, and methamphetamines on infant cognitive development and behavior remain controversial (owing to confounding environmental factors) (Bays, 1990; Tronick and Beeghly, 1999), the effects on maternal-infant interactions are more established (Breiter et al., 1997; Singer, 2000).
There are multiple short critical periods during the development of a fetus when a short, acute exposure may cause a problem. For this reason, exposures need to be tracked as highs and lows on a daily basis rather than as monthly averages. For example, water quality is regulated by monthly averages. However, a daily peak may exceed a threshold of concern and still be within the regulatory limit.
A recent review concluded that neural tube defects and small-for-gestational-
age births are moderately associated with contaminated drinking water (i.e., trihalomethanes) (Bove et al., 2001). Oral clefts, cardiac defects, and complete nasal obstruction (choanal atresia) were found in studies evaluating trichloroethylene-contaminated drinking water (Bove et al., 2001). Food may also contain environmental teratogens. A well-known example is the epidemic of cerebral palsy that followed maternal consumption of fish contaminated with organic mercury in Minimata Bay, Japan (Harada, 1978).
Childhood Exposures
Characterization of exposures over time depends on developmental stage and the mechanism by which the agent produces its effect (EPA exposure guidelines, 2003). Multiple types of exposure may interact to produce their effect by the same mechanism, as for example the exposure to multiple insecticides that interfere with cholinesterases (National Research Council, 1993). Children have unique susceptibilities to chemical exposures (see Box 3-2).
Air Pollutants
Six outdoor air pollutants are regulated by the Clean Air Act: ozone, respirable particulate matter, lead, sulfur dioxide, carbon monoxide (CO), and nitrogen oxides. The effects of repeated or long-term exposure to outdoor air pollutants on the developing lungs of children are not well understood. Indoor air pollution, which is generally not regulated (one notable exception being laws prohibiting indoor smoking in public spaces), results primarily from (1) the products of combustion, such as CO, nitrogen dioxide, particulates, and sulfur dioxides; (2) volatile organic compounds, such as formaldehyde, benzene, and trichloroethylene; (3) the products of tobacco smoking (approximately 3,800 chemicals); and (4) molds.
Health effects from these diverse indoor air pollutants include respiratory irritation with cough and wheezing, exacerbation of asthma, allergic responses, cancer, and central nervous system effects (headache, nausea) (American Academy of Pediatrics, 2003). Exposure to asbestos, leading to lung cancer, is also a concern due to the prevalence of asbestos in schools and some homes (U.S. Environmental Protection Agency, 1987; American Academy of Pediatrics, 1987).
Water Pollutants
Some water pollutants are biological agents, some are chemical agents, and some are radionuclides (physical agents). Biological agents generally come from fecal contamination and include such bacteria as salmonella and E. coli, such viruses as hepatitis A and rotavirus, and such parasites as Cryptosporidium parvum. Chemicals in water include such metals as lead, mercury, and arsenic, such natu-
|
BOX 3-2 Children are more susceptible than adults to chemical exposures, and their exposure varies, depending on their physical location, breathing zones, oxygen consumption, types and amount of food and water consumed, and normal behavioral development. Specific exposures over time depend on developmental stage and the mechanism by which the agent produces its effect (EPA exposure guidelines, 2003). Estimates of chemical exposure are often retrospective, because it is difficult and costly to monitor exposures as they occur. Even if the total duration or dose of exposure is the same for two children, different patterns and timing of exposure may result in different health effects. For example, ingestion of nitrates in well water may reduce hemoglobin to methemoglobin, which is incapable of transporting oxygen (Lukens, 1987). However, if the nitrates are ingested at a slow enough rate for enzymes to change methemoglobin back to hemoglobin, no deleterious health effects occur. This is an example of a threshold effect; the health effect will not occur until the dose from the exposure reaches a particular level in the body. Physical location. The newborn is usually held by or near the mother, or spends extended periods in a single environment (e.g., a crib), rather than several different environments. Infants and toddlers who are frequently placed on the floor, carpet, grass, or a blanket are exposed to chemicals associated with these surfaces, such as formaldehyde and volatile organic chemicals from synthetic carpet (Bernstein, 1984), pesticide residues from flea bombs (Fenske et al., 1990), dust mites, pet dander, and detergent residues. Preambulatory children also may experience sustained exposure to noxious agents because they cannot remove themselves from their environment. For example, the premobile infant must be protected from sunburn by the caregiver (Lowe et al., 2002). Breathing zones. The breathing zone for a child, which varies based on height and mobility, is typically much lower than that of an adult. Chemicals that are heavier than air, such as methyl mercury, large particulates (Leaderer, 1990), and radon (Blot et al., 1990) accumulate in lower breathing zones. The presence of mercury in latex house paint in a child’s breathing zone results in acrodynia, a hypersensitivity reaction to mercury, also known as pink disease, and prompted legislation mandating the removal of mercury from house paint (Centers for Disease Control and Prevention, 1990b). |
ral toxins as Pfiesteria toxins, organic chemicals including pesticides, PCBs, trichloroethylene, and chlorination by-products, such inorganic ions as nitrates, and such radionuclides as radon. Systems affected by these contaminants include the central nervous system, the gastrointestinal system, and the hematological system. Many of these chemicals are also carcinogens. Children have been found to be at higher relative risk of gastrointestinal illness from contaminated water (Wade et al., 2003). In addition, children are both more highly exposed and more susceptible to the contaminants found in water. For example, lead in drinking
|
Oxygen consumption. Because children have a larger surface-to-volume ratio, they also have a higher metabolic rate and greater oxygen consumption (twice as much for a 6-month-old child as an adult) and minute ventilation, which is volume times respiratory rate (more than three times greater for a newborn than an adult). Exposure to any air pollutant is therefore greater on a weight-adjusted basis. For example, if radon is present, a 6-month-old child will receive twice the exposure of an adult (World Health Organization, 1986.) The increased respiratory exchange is also associated with increased vulnerability to CO poisoning. Quantity and quality of food and water consumed. Children need to consume more calories and water per pound of body weight than adults given their higher metabolic rate. An average infant consumes 5 ounces of formula per kilogram of body weight (equivalent to an adult drinking 30 12-oz cans of soda a day). If the food or liquid contains a contaminant, children may receive more of it relative to their size than adults, making them particularly vulnerable to pollutants in water. Even the most natural of foods, breast milk, whose salutary benefits have been universally acknowledged (World Alliance for Breastfeeding Action, 1992), is affected by environmental pollutants (Ong et al., 1985; Pluim et al., 1994; Rogan et al., 1986). The diet of children is less diverse and contains more milk products and certain fruits and vegetables than the typical adult diet, and, as a result, children may be exposed to more dangerous levels of pesticides and other chemical residues than adults (Zeise et al., 1991; National Research Council, 1993). Normal behavioral development. Children’s normal behavioral development also influences environmental exposures. Children typically pass through a stage of intense oral exploratory behavior from about age 6 months to 2 years. This also places children at risk in environments with high levels of lead dust, such as houses painted with lead-based paint (Chao and Kikano, 1993), wood used in playground equipment that is treated with arsenic and creosote (Kosnett, 1990), and toxic ingredients in sand or arts and crafts materials. Given their exploratory nature, ambulatory children may wander into unusual situations for play, such as used drums, mud puddles, and empty lots, environments that have the potential for dangerous exposures. As they become adolescents, they gain more and more freedom from parental authority, often having their physical strength and stamina peak before they acquire the ability to think abstractly (Campbell, 1976). Adolescents often misjudge or ignore risks (Perry and Silvis, 1987), which may result in their placing themselves in situations with greater risk than an adult would willingly face. |
water was found to be the cause of lead poisoning in several infants whose blood lead exceeded 10 mcg/dl (Baum and Shannon, 1997; Shannon and Graef, 1992).
Food Contaminants
Food contaminants can be broadly categorized as either pathogenic or toxic. Pathogenic agents include bacteria, viruses or parasites, bacterial toxins, aquatic organisms that elaborate toxins, and toxins that accumulate in the food chain,
such as domoic acid. Toxic chemicals in food can be divided into three categories: (1) pesticides that have been deliberately applied to the food source; (2) colors, flavors, or preservatives deliberately added to food during processing; and (3) chemicals that inadvertently enter the food chain, such as PCBs, heavy metals, and persistent pesticides such as DDT. Particular effects of food contaminants on children include such behavior changes as hyperactivity (Carter et al., 1993) and developmental neurotoxicity from pesticide exposure in food (National Research Council, 1993).
Infectious Agents
Children also are a demographic subgroup prone to infectious diseases because of their exploratory behavior, lack of prior exposure to most infectious agents, and association with other children. Substantial advances in vaccines have reduced rates of many infectious diseases during the past decades. Nonetheless, infectious agents remain a major threat to children’s health, particularly with the increase in antibiotic resistance among various infectious organisms and the emergence of new infectious agents (i.e., new strains of flu).
Children are highly exposed and susceptible to some infections that are spread by droplets from coughing and sneezing. Respiratory syncytial virus, the leading cause of serious upper and lower respiratory tract infection in infants and children, accounts for 125,000 hospitalizations and 450 deaths annually in the United States, and it may predispose children to asthma later in life. Annual epidemics occur from November to April, and virtually all infants are infected by age 2 (Black, 2003). Cytomegalovirus infection is spread in child care centers through both urine and saliva containing live virus; rates for preschool-age children in the United States range from approximately 5 to 30 percent (Centers for Disease Control and Prevention, 1985). Children are also particularly susceptible to other infectious agents, such as rotavirus and Norwalk virus, salmonella, and E. coli O157:H7, which cause diarrhea and dehydration and sometimes severe complications.
Children are also more highly exposed to vector-borne (e.g., via ticks, fleas) or certain zoonotic (e.g., hosted by dogs, cats, horses) pathogens due to their increased time outdoors, play activities, and behaviors. Vector-borne pathogens include Lyme disease, highest among 5–9-year-olds (Centers for Disease Control and Prevention, 2002a), and Rocky Mountain spotted fever, most prevalent under age 10 (Centers for Disease Control and Prevention, 2000b). Some arboviruses, which are transmitted by different species of mosquitoes, preferentially infect the young (e.g., La Crosse encephalitis carried by a woodland mosquito; Centers for Disease Control and Prevention, 1990a, 1998a). Cat scratch disease, carried by cats, has an estimated annual incidence of 22,000 cases, with the highest age-specific incidence in children less than age 10. Up to 25 percent of
these cases result in severe systemic illness (Centers for Disease Control and Prevention, 2002a).
Noise
Few studies have estimated children’s exposure to noise or the effect of noise on children’s health, but there is suggestive evidence of its effect. Children appear to be routinely exposed to more noise than the recommended upper limit proposed by the U.S. Environmental Protection Agency in 1974 (De Joy, 1983; Roche et al., 1982). Noise-induced hearing loss in one or both ears among children ages 6 to 19 was found to be 12.5 percent (or 5.2 million children) (Niskar et al., 2001) and more frequent among high school students actively involved in farm work compared with peers not involved (Broste et al., 1989). In a sample of 1,218 children, 1 in 20 school-age children had minimal sensorineural hearing loss and 37 percent of the children with this hearing loss failed at least one grade (K–12) (Bess et al., 1998). Even mild hearing loss is associated with increased social and emotional dysfunction among school-age children.
Noise exposure in childhood is associated with a stress response (Tafalla and Evans, 1997—in male college students), headaches (Odegaard et al., 2003), sleep deprivation (Corser, 1996; Cureton-Lane and Fontaine, 1997), elevated blood pressure and heart rate (Matheson et al., 2003; Evans et al., 2001; Regecova and Kellerova, 1995), and poor performance including reading comprehension and long-term memory (Matheson et al., 2003; Stansfeld et al., 2000).
Radiation
Exposure to ultraviolet B radiation from sunlight exposure and the use of tanning equipment during childhood can result in substantial morbidity and mortality later in life. Health risks from exposure vary with skin type and include sunburn, skin cancer (the most common malignant neoplasm in the U.S. adult population), phototoxicity and photoallergy, skin aging, and cataracts. Approximately 80 percent of lifetime sun exposure occurs before the age of 18. Episodic high exposures sufficient to cause sunburn, particularly during childhood and adolescence, increase the risk of melanoma (Saraiya et al., 2003).
Ionizing radiation comes from both natural and manmade sources. Natural sources include radon, cosmic radiation, and ingested radon and fallout. Manmade sources include medical X-rays and some consumer products. The consequences of exposure for children’s health include birth defects from prenatal exposures (microcephaly, mental retardation), neurological damage in younger children, and cancer (American Academy of Pediatrics, 1998).
Home, School, and Work Settings
The quality of their housing influences children’s health. Housing conditions can contribute to the incidence of asthma, injuries, and lead poisoning (Manuel, 1999). As children age, they spend more time in physical locations outside the home, such as child care, school, and workplace settings that expose them to new physical environments. Thus, parents’ choice of child care facility may affect both indoor and outdoor (e.g., playgrounds, backyards) exposures. For example, child care exposure to cigarette smoke may differ from exposure in children’s own homes (Wright et al., 1989).
School-age children spend 35 to 50 hours per week in and around school buildings. In some communities, schools have been built on relatively undesirable land, such as landfill sites like Love Canal. Schools are often located on old industrial sites or near highways, resulting in exposure to auto emissions and air pollution (Frumkin, 2003). Many school buildings are old and poorly maintained, leading to exposures to air pollutants, radon, asbestos, pesticides, and lead (Etzel and Balk, 1999). The U.S. General Accounting Office reported that 20 percent of primary and secondary schools had indoor air quality problems; more than half had environmental pollutant or building ventilation problems that could affect air quality (U.S. General Accounting Office, 1995). Radon above the EPA’s action level was found in 2.7 percent of schools surveyed during the 1990–1991 school year (U.S. Environmental Protection Agency, 1992). Asbestos, used extensively in schools until the 1970s, was still present in more than 8,500 schools in 1980, potentially exposing over 3 million students (U.S. Environmental Protection Agency, 1987).
Many adolescents have jobs that may expose them to occupational hazards (Pollack et al., 1990). Every year, at least 70 children die from work-related incidents (Centers for Disease Control and Prevention, 1996) and more than 65,000 are injured severely enough to seek care in emergency departments (Brooks et al., 1993). Under the Fair Labor Standards Act of 1938, which regulates work hours and safety, children younger than 18 are prohibited from working with hazardous chemicals in nonagricultural jobs. Prohibitions on chemical work in agriculture extend only to age 16, and work by children and adolescents on their own family farms is unregulated at the national level. During 1992–1995, 155 deaths were reported among agricultural workers age 19 and younger; 64 (41 percent) of these youths were working in their family’s business (Derstine, 1996). For each death, many more experience nonfatal injury (Rivara and Barber, 1985), usually from farm machinery or exposure to toxins.
Child Injury and the Provision of Safe Environments
Injuries are the leading cause of death among children between ages 1 and 19, accounting for more deaths than homicide, suicide, congenital anomalies, cancer, heart disease, respiratory illness, and HIV combined (Centers for Disease Con-
trol, 10 leading causes of death, 1997). Although the total number of unintentional injury deaths has declined by more than 40 percent during the past 20 years (CDC Injury Mortality Stats), the rates of childhood injury are much higher in the United States when compared with other developed countries. In 2001, unintentional injuries consttuted 70 percent of all injury deaths to children and adolescents (0 to 20 years) in the United States (National Center for Health Statistics, 2004).
The enormous impact of injury on children’s health is manifest by the fact that approximately 18 hospitalizations and 233 emergency department visits occur for every injury death (Grossman, 2000). As injury deaths continue to decline, nonfatal injuries continue to be important causes of child morbidity and disability and substantially reduce quality of life, especially among adolescents. However, it should be noted that data collection on nonfatal injuries is incomplete.
The elements of a safe and healthy physical environment differ according to a child’s developmental stage. The American Academy of Pediatrics has conducted extensive reviews of the literature to establish the evidence-based recommendations in The Injury Prevention Program, an age-appropriate prevention education program (www.aap.org/family.tipmain.org/) for physicians and families. Recommendations include counseling parents on use of infant car seats, never leaving infants and toddlers alone in pools or bathtubs, the use of safety equipment for in-line skating and skateboarding, and firearm safety.
The use of playground equipment is the leading cause of injuries to children in school and child care environments, with 211,000 children receiving emergency department care annually for injuries sustained on playgrounds (Centers for Disease Control and Prevention, 1999a). Factors influencing playground injury prevention include supervision, age-appropriateness of equipment, suitable fall surfaces, and equipment maintenance. Supervision has been shown to be inconsistent, age appropriateness is infrequently indicated, and many playgrounds have had equipment with significant safety issues (Sibbald, 2002).
Automobile crashes are the leading cause of death among children over a year old. In 2000, 2,343 children under age 15 were killed in traffic crashes, including 1,668 who were passengers, 469 who were pedestrians, and 175 who were on bicycles. That same year, 291,000 children under 15 years of age were injured in traffic crashes, including 248,000 who were passengers and 22,000 who were pedestrians. On an average day, 6 children are killed and 797 are injured in motor vehicle crashes.
The determinants of motor-vehicle-related injuries and fatalities are well recognized. Some relate to behavioral issues, such as speeding, failing to yield to pedestrians at crossings, and driving while intoxicated; others relate to automobile design and features, including impact absorption, seat belts, air bags, and similar features. Still others relate to roadway features. Public health interventions addressing these factors, from seat belts to traffic signals and from law enforcement to public education and the development of bike paths, have achieved dramatic reductions in injury and fatality rates (Rivara, 1999).
The Built Environment
The built environment may be defined as the part of the physical environment created by human actions—buildings and parks, roads and trails, neighborhoods and cities. This section illustrates the importance of the built environment by describing how land use and related transportation patterns that characterize an entire metropolitan area affect injuries, air quality, and physical activity patterns (Frumkin, 2003).
Injuries
The built environment contributes to motor-vehicle-related morbidity and mortality among children by creating places that rely heavily on increasing driving time in cars and by developing certain kinds of roads that may be unusually hazardous for drivers, pedestrians, or both. Modern suburban roads may be especially dangerous. Major commercial thoroughfares and feeder roads that combine high speed, high traffic volume, and frequent “curb cuts” for drivers entering and exiting stores may pose a special hazard. In general, the prevention of injury by one-time structural changes, such as highway or automobile engineering, is more effective than actions that require repeated use, such as bicycle helmets (Layde et al., 2002).
The epidemiology of pedestrian injuries among children has been well studied and includes several factors that relate directly to the built environment: high traffic volume and speed, absence of play space, and possibly one-way streets (Pitt et al., 1990; Roberts et al., 1995; Schieber and Thompson, 1996; Rivara, 1999; Wazana et al., 2000; DiMaggio and Durkin, 2002). Large boulevards are riskier than residential streets (Kraus et al., 1996), and denser census tracts are safer than those with low density (Lightstone et al., 2001). However, the effect of residential density is complex (Rivara and Barber, 1985; Rao et al., 1997; Posner et al., 2002).
Across the country, the pattern seen for driver and passenger fatalities is repeated for pedestrian fatalities, with lower annual rates in denser cities (National Highway Traffic Safety Administration, 2001). Data from Atlanta show that as that city has sprawled in recent years, the pedestrian fatality rate increased even as the national rate declined slightly (Centers for Disease Control and Prevention, 1999a). The most dangerous stretches of road were those with multiple lanes, high speeds, no sidewalks, long distances between intersections or crosswalks, and roadways lined with large commercial establishments and apartment blocks (Centers for Disease Control and Prevention, 1999a).
Reviews of injury prevention from motor vehicles in children focus almost entirely on seat belts, car seats, air bags, and other engineering approaches or on law enforcement and education (Pitt et al., 1990; Durbin, 1999; Towner and Ward, 1998; Rivara and Aitken, 1998; Rivara, 1999). Primary prevention, in contrast, includes strategies for traffic calming (Roberts et al., 1994; Liabo et al., 2003)
and strategies to reduce driving or children’s time in and near motor vehicles. These strategies all relate directly to features of the built environment.
Air Quality
In environments where automobiles and trucks are the principal means of transportation, the emissions from these mobile sources figure prominently as a source of air pollution. Although vehicle engines have become far cleaner in recent decades, the sheer quantity of vehicle miles releases large amounts of carbon monoxide, carbon dioxide, particulate matter, nitrogen oxides, and hydrocarbons into the air. Nitrogen oxides and hydrocarbons, combined with sunlight, form ozone. Cars and trucks account for a substantial amount of the emissions of such chemicals.
Ozone levels do not vary over a small scale, from block to block. A child in the suburbs may sustain ozone exposure that is as high as, or even higher than, the exposures of an inner-city child. In contrast, particulate matter less than 2.5 microns diameter (Pm2.5), which can affect respiratory function, may vary from block to block. A child living near a busy intersection or near a heavily traveled truck route may sustain considerably more particulate exposure than a child living in a quieter neighborhood several blocks away.
Children who live, attend school, or play near busy roads or in crowded urban areas, where they are exposed to the exhaust from automobiles and trucks, may experience acute and chronic respiratory effects. In addition, children who live in metropolitan areas with heavy traffic, especially in parts of the country conducive to ozone formation for biogeophysical and meteorological reasons, may be exposed to high levels of ozone during the warm months of the year.
Physical Activity
The built environment plays a major role in promoting or hampering physical activity in children. Schools, parks, and even sidewalks that are integrated into the design of a community can encourage physical activity. For example, physical activity among youth increases when schools offer such facilities as basketball courts and sports fields (Frumkin, 2003). A considerable body of research shows that sprawl—as measured by low residential density, low employment, low “connectivity”—is associated with less walking and bicycling and with more automobile travel than denser communities (U.S. Environmental Protection Agency, 2001; Holtzclaw et al., 2002; Cervero, 2002; Cervero and Ewing, 2001).
SOCIAL ENVIRONMENT
Humans are social creatures. While social influences are important for children of all ages, their nature and form change over the course of childhood. In
this section we describe the dynamic nature of the constituents of children’s social environment and illustrate how these environmental influences manifest themselves.
Family Influences
Families are fundamental to children’s well-being and have a profound direct and indirect influence on the challenges they encounter and the resources available for their needs. The range of needed inputs is broad and includes material resources, time, interpersonal connections, and institutions that parents and communities may use to promote children’s development (National Research Council and Institute of Medicine, 1995b). Culturally, differing beliefs about normative development, appropriate parenting roles, and gender roles are important influences on the family (García Coll and Pachter, 2002) (see Box 3-3).
Family influences include both family demography and processes. Family demography consists of the readily measured facts of family life—composition (e.g., one versus two biological parents), financial status, and parental education. Family processes consist of the ways in which family influences operate to affect children’s well-being. They include parenting styles, the provision of family environments, and health habits that may be beneficial or detrimental to children’s heath. We also include in this category two parental characteristics that affect parenting—mental health and substance abuse.
Family and other environmental factors can be sources of either risk or resilience for the developing child, and it is crucial to understand that the child’s response to a specific stressor is influenced by a confluence of other influences. Thus, while in general a specific influence may be negative or positive, may be of greater or lesser impact at a given developmental stage, and may show its effects at the time or at some time in the future, it is often the presence and absence of other
|
BOX 3-3 Family demographics
Family processes
|
risk and resilience factors that determine how an individual child will be affected (Rutter, 1990).
Although the nature and degree of family influences on children change over time, both experimental and nonexperimental evidence indicates that the family continues to have direct influence on a child’s decision making well into adolescence (Larson, 1974; Romer, 1994). Two studies have shown that parental monitoring has positive effects not only on their children’s performance in the classroom, but also in terms of positive health outcomes; these children had higher grades, greater self-reliance, lower rates of sexual risk behaviors and substance abuse, and also less anxiety, depression, and involvement in delinquent behaviors (Wu et al., 2003; Steinberg et al., 1991).
Family Demography
Socioeconomic Status (SES). Poverty in the United States is disproportionately concentrated among children (U.S. Census Bureau, 2002). The health and development of poor children are compromised relative to U.S. children living in higher income families (Brooks-Gunn and Duncan, 1997). Mortality from infectious diseases is 2.5 times more common and accidental deaths are twice as common among U.S. children in the poorest than among the richest 10 percent of the population. Overall mortality and cancer-related mortality are twice as high among the lowest income quintile compared with the highest income quintile (Shah et al., 1987).
Underlying most explanations for the link between low SES and impaired health are the diminished resources available to families living in poverty. Case et al. (2002) use U.S. data from national health surveys to show that children in higher compared with lower income families are healthier and appear less likely to have their childhood health conditions (e.g., asthma) manifested as poorer general child health, although Currie and Stabile (2002) found that the links between poverty and disease progression appear to be weaker for Canadian than U.S. children.
Low-income parents are also at greater risk for depression and other forms of psychological distress, such as low self-worth and negative beliefs about control, which can impair their ability to use available assets (Gazmararian et al., 1995; Pearlin and Schooler, 1978; Rosenberg and Pearlin, 1978). Nationally representative survey studies show that psychological distress is more prevalent among low-income populations because they experience more negative life events and have fewer resources with which to cope with adverse life experiences (Kessler and Cleary, 1980; McLeod and Kessler, 1990).
The relationship between poverty and child health has been a focus of attention for decades (Egbuonu and Starfield, 1982), and a relationship between low SES and poor health has been well known at least since the beginning of the 18th century. However, only recently have we come to realize that increments to socio-
economic position are positively associated with health at virtually all social levels (Marmot, 1999).
While this social gradient in health is now certain for nonelderly adults, evidence for its existence in children and youth is less well documented. A recent review of evidence from studies of younger children and adolescents indicates the existence of gradients in some but not all aspects of health (Starfield et al., 2002a). Case et al. (2002) documented increasing income gradients in health across childhood in several U.S. national surveys. Currie and Stabile (2002) found similar patterns in Canadian data.
Family Composition and Size. All families do not look alike. One-third (33.2 percent) of all births in America in 2000 were of children born to an unmarried mother (Centers for Disease Control and Prevention, 2000a), and 22.4 percent of all children live with a single parent (Centers for Disease Control and Prevention, 2000b). Longitudinal national survey studies reveal that children reared in families with two biological parents tend to complete more schooling and engage in less risky behavior (McLanahan and Sandefur, 1994), particularly if their SES is high. In a large birth cohort observational study conducted in Great Britain, children of single mothers or living with stepfathers were 50 percent more likely to have been admitted to the hospital and more than twice as likely to have had multiple admissions than children living with both biological parents (Butler and Golding, 1986).
How much of the difference can be attributed to family structure itself in contrast to the prior and often continuing stress of a divorce or separation is not clear. Intact marriages are associated with higher incomes, more male role models, fewer residential moves, and more discipline and supervision than marriages that break up (McLanahan and Sandefur, 1994). Amato and Keith’s (1991) meta-analysis of 92 studies addressing the impact of divorce on children found that its impact depends on their ages. Among preschool children, divorce generally had small negative effects on their social adjustment but no effects in other domains. By contrast, children of primary school age appeared to suffer greater negative effects from divorce. The authors note that the better designed studies included in the meta-analysis found smaller effects from the divorce.
Economic and other family resources available to children also vary by family size, since more children often mean less time and money expenditure per child. Although the simple correlations between number of siblings and a host of positive outcomes are almost universally negative (Blake, 1989), the extent to which these negative correlations represent causal impacts remains in dispute (Guo and VanWey, 1999). For some aspects of development, larger families may confer advantages, as when the presence of siblings allows a child to gain experience with relations among “peers.”
Family Processes
Parenting. Much has been written regarding the effect of parenting style on child development, how parental challenges and tasks change with maturation of the child, and how parenting style varies by ethnicity, which in turn influences the impact of parenting style on outcome. Baumrind (1971) proposed the prevailing conceptual framework, which applies throughout childhood and has facilitated understanding of the effect of three different styles of parenting: permissive (warm and undemanding), authoritarian (cold and demanding), and authoritative (warm and demanding).
Authoritative parenting is associated with social responsibility and self-assertion among children (Dornbusch et al., 1985) and lower levels of adolescent risk behavior and higher levels of achievement during the adolescent years (Steinberg et al., 1989). Harsh, punitive disciplinary practices are thought to feed into the cycle of anger and aggressive behavior developed by some children and youth (Petit, 1997). Patterson’s theory of the socialization of aggression, well supported by decades of research, argues that aggressive children are trained to be competitive and parents are trained to encourage their competitiveness (Patterson, 1995; Patterson et al., 1991, 1992).
While a substantial observational and intervention literature supports this general framework, important variations in these elements of parenting are manifested in different cultural contexts (Steinberg et al., 1992; Wu et al., 2003). For example, in the context of Chinese immigrant families, Chao (1994) argues that parental control efforts are related to the goals of training children to have harmonious relations with others, which is considered essential to maintain the integrity of the family. In the context of black families, Brody et al. (1998) argue for the concept of “no-nonsense” parenting, which is thought to protect youths from dangerous surroundings.
Although these basic approaches to parenting appear to apply throughout a child’s life course, the tasks facing parents change as the child develops, and thus parenting must change. For example, beyond tending to the infant’s biological needs, the task for the parent of infants and young toddlers is the establishment of secure attachments (Rutter, 1998). Later in childhood and adolescence, parental monitoring (knowledge of the child’s activities and friends) assumes greater importance, along with the other tasks of employing discipline for antisocial behavior, employing effective problem-solving skills, and supporting the development of prosocial skills (Patterson, 1982; Patterson and Stouthamer-Loeber, 1984).
There is some evidence that religiosity among adolescents contributes to lower rates of violence, substance abuse, and emotional distress; it has also been related to more health-promoting behavior, such as proper nutrition, exercise, later onset of sexual intercourse, increased academic competence, and higher levels of life satisfaction (Resnick et al., 1997; Wallace and Forman, 1998; Wallace et al., 2003; Barnes et al., 2000). It is unclear to what extent these effects are related
to religion or religiosity rather than parenting, community values, or attributes of youth who tend to be religious.
Family Learning Environments. All children do not enter school equally equipped to master its associated challenges. A substantial literature demonstrates the extent to which parental practices can augment or impede the development of language and reading skills in young children and that acquisition of these early skills predicts later success in school (Hart and Riseley, 1995; Senechal and LeFevre, 2002; Zill, 1996). The quantity of speech directed toward children is a strong correlate of the child’s subsequent vocabulary and emergent literacy skills (Hart and Risley, 1995; Huttenlocher et al., 1991; Dickinson and DeTemple, 1998). The literature linking parental reading to infants and toddlers with emergent literacy skills led the American Academy of Pediatrics to recommend that pediatricians “prescribe” reading to parents beginning when their children are 6 months old.
Seminal work by Bradley and Caldwell (1980) identified important aspects of the home environment that are related to children’s well-being. Their widely used Home Observation for Measurement of the Environment (Bradley and Caldwell, 1984) scale assesses the type and frequency of interactions and learning experiences that parents provide for their children, both inside and outside the home. Stimulation, emotional support, structure, and safety are associated with the well-being of both low-income and high-income children (Bradley et al., 1994).
Parents and family environment represent an important determinant of childhood eating patterns and childhood obesity (Hart et al., 2003). Although relatively little research has assessed the nutritional environments provided by parents (especially obese parents) for overweight children, existing data suggest a strong environmental contribution confounded by genetic interactions. While the need to design effective family-based eating programs is clear, the evidence base for the effectiveness of such programs in the prevention or reduction of childhood obesity is limited (Birch and Davidson, 2001).
Parents’ cultural backgrounds have been associated with the learning environments provided to children of all ages. Parents tend to promote not only those skills that they value, but also those they have mastered (Moll et al., 1992). In a recent study, immigrant parents of different cultural backgrounds—Cambodian, Dominican, and Portuguese—differed significantly with regard to the areas of their children’s education in which they were involved (García Coll and Weisz, 2002). These differences existed even when a large majority of parents in all groups reported valuing education and having high aspirations for their children’s educational attainment.
Parental Mental Health. Parental depression and psychological distress can have powerful negative effects on child well-being. Depression has been estimated to
affect about 10 percent of all mothers and 20 percent of poor mothers (Dickstein et al., 1998). Depressed mothers are more likely to respond to their children with withdrawal, diminished energy, or emotion or to express feelings of hostility and rejection toward their children (Frankel and Harmon, 1996; Field, 1995). Depression appears to be a robust influence irrespective of family income (Miller, 1997; Radziszewska et al., 1996).
Reviews of observational studies suggest that children of depressed mothers compared with those of nondepressed mothers are more likely to show higher levels of aggression, sociobehavioral problems including poorer peer relations and reduced ability for self-control, and poorer school performance (e.g., Cummings and Davies, 1994). Other reviews have found that children of depressed parents are at substantially greater risk to develop depression themselves (Downey and Coyne, 1990). Not all children of depressed mothers manifest adverse outcomes (Cummings and Davies, 1994), leading to the hypothesis that the adverse effects of maternal depression are most evident when compounded by other sources of stress, such as physical abuse, marital discord, and substance abuse (Seifer, 1996; Sameroff and Fiese, 1989). Numerous studies have documented a positive relationship between parental stress levels and rates of child abuse and neglect (Sachs et al., 1999; Hall et al., 1991; Luttenbacher, 2002; Wind and Silvern, 1994; Rodriguez and Green, 1997).
Parental Substance Abuse. Many studies have documented associations between maternal alcoholism and child developmental outcomes. In one study, drinking by female caregivers predicted a less cohesive and organized family environment and higher levels of domestic violence (Jester et al., 2000). Parental substance use also affects a parent’s ability to nurture and supervise. Although in the past women have been less likely than men to use illicit substances, rates have been increasing in women (National Institute of Justice, 1989; Ebrahim and Gfroerer, 2003).
Environmental tobacco smoke has been shown to cause many different health effects in exposed children, including cancer, asthma, increased severity of respiratory syncytial virus, and increased incidence of ear infections (U.S. Environmental Protection Agency, 1992). Parental tobacco use is one factor associated with children’s starting to smoke (Nichols et al., 2004; Andersen et al., 2004). Recent studies also demonstrate an interaction between maternal smoking and genetic predisposition to increased rates of attention deficit hyperactivity disorder in children (Kahn et al., 2003).
Maternal infant bonding appears to be key mechanism; a recent review of 23 articles showed that 14 found recognizable negative impacts on maternal-child interactions among substance-abusing mothers, and three found a dose-response relationship with impact or an accentuation of impact related to continued substance use postnatally (Johnson, 2001).
Community Environment
Moving beyond the family, there is considerable evidence that community conditions can affect children’s healthy development, especially in the case of children growing up in the most dangerous and socially disorganized communities (National Research Council and Institute of Medicine, 2000; Brooks-Gunn and Duncan, 1997). Community influences can originate in neighborhoods, schools, or other organizations and can operate through children’s peer groups, the adults with whom children come into contact, or the larger set of social and cultural practices in neighborhoods. Specifically, ethnic enclaves differ not only in socioeconomic characteristics but also in their adaptive culture (García Coll et al., 1996—see Box 3-4).
As with our discussion of family influences, we organize our discussion of neighborhood and community influences using the distinction between demography and processes. Community demography consists of readily measured characteristics (e.g., poverty, adult unemployment, crowding). Processes consist of the ways in which neighborhoods and communities operate to affect children’s well-being.
There are many definitions of a neighborhood or community environment (Brooks-Gunn and Duncan, 1997). In empirical studies, it is typically a geographic area defined by the Census Bureau (tracts, which are locally defined community areas). But there are social definitions of communities that transcend geographic boundaries and can vary across families and ethnic groups (Jarrett, 1997).
Community Demography
Neighborhood Demographic and Economic Characteristics. The socioeconomic characteristics of a community have a strong association with such indi-
|
BOX 3-4 Community demographics
Community processes
|
vidual health outcomes as infant mortality, birthweight, mental health, and cardiovascular status (Diez-Roux, 2002; Ellen et al., 2001). Several studies in various locations have found that even when controlling for important risk factors, such as income, race, smoking, body mass index, and alcohol consumption, residents of lower SES communities had higher rates of poor health than residents of higher SES communities (Malmstrom et al., 1999; Yen and Syme, 1999).
Yet a striking result in broad-based studies of neighborhood effects on children is that there are many more differences in families and children within neighborhoods than between them. Chase-Lansdale et al. (1997) found that, at most, 2 percent of the variation in behavior problems among 5- and 6-year-olds can be explained by a collection of neighborhood demographic and economic conditions, such as poverty, male joblessness, and ethnic diversity. Duncan et al. (2001) have shown that less than 5 percent of the variation in youth delinquency can be explained with knowledge of the neighborhood of residence. These findings must be tempered by the way in which more proximate and more distal influences are interpreted statistically.
Community Processes
National Research Council (1990), Coulton (1996), and Sampson et al. (2002) provide general summaries of ways in which neighborhood and community processes may affect children’s development, including:
-
institutional explanations, in which the neighborhood’s institutions and resources (e.g., schools, quality of food markets, health care facilities, public health, and police protection) rather than neighbors per se make the difference;
-
stress theory, which emphasizes social and psychological conditions, such as community violence, as well as the importance of exposure to such physical toxins as lead in soil and paint;
-
social organization theory, based on the importance of role models and values consensus in the neighborhood, which in turn limit problem behavior among young people; and
-
epidemic theories, based primarily on the power of peer influences to spread problem behavior.
Since adolescents typically spend a good deal of time away from their homes, explanations of neighborhood influences emanating from peer-based epidemics, role models, schools, and other neighborhood-based resources would appear to be more relevant for them than for younger children. However, interactions between preschool children and their kin, neighbors, religious communities, and child care and health systems suggest that neighborhood influences begin long before adolescence (Chase-Lansdale et al., 1997).
Schools and Early Education Programs. Among community institutions, formal schooling plays a major role in shaping children’s development. Completed schooling is a strong correlate of such successful adult outcomes as longevity, career attainments, and avoiding crime (Fuchs, 1983), as well as such two-generation outcomes as successful parenting (Hoff-Ginsberg and Tardiff, 1995).
Nevertheless, researchers have long worried about the potentially spurious nature of these associations. Are they truly the result of the schooling, or do they instead reflect the greater ability or motivation that leads some children to complete more schooling? The most sophisticated studies strongly suggest causal impacts of schooling on earnings as well as other positive outcomes, with the apparent social rate of return to investing in additional years of schooling averaging around 10 percent (Card, 1999). Roughly speaking, this means that investing $10 in interventions that successfully promote the attainment of an additional year of schooling produces a $1 annual increment to participants’ earnings. The relative roles of schooling, income, and occupation in affecting adult health are a matter of considerable debate (Krieger, Williams, and Moss, 1997; Daly et al., 2002).
Education prior to school entry appears to matter as well. Reviews of experimental evaluations of high-quality early childhood education programs have concluded that intensive programs improve children’s short-term cognitive development and long-term academic achievement, as well as reduce grade retention of children in special education (Barnett, 1995; Farran, 2000; Karoly et al., 1998) and rates of academic failure, delinquent behavior, and adolescent pregnancy rates (Hawkins et al., 1992). Furthermore, some of these programs also improve children’s long-term social behavior, as indicated by fewer arrests and reports of delinquent behavior. Indeed, the payoffs to early education programs may well exceed those of formal schooling (Heckman, 1999).
Schools can also have an effect on student behaviors, the ability to arrive at school ready to learn, and overall health. School health programs have increased substantially over the past several decades in recognition of the connection between health and learning. The Institute of Medicine recommended in 1997 that all students in elementary, middle, and junior high school receive sequential health education to help shape their behaviors. The report noted that skills training, peer involvement, social learning theory, and community involvement have the greatest effect on school health education.
Finally, research has confirmed the direct relationship between physical activity and long-term health. School physical education programs over the past decade have in fact shifted toward an emphasis on physical fitness rather than competitive sports. Although there is limited research on the effect of physical education on health, there is some evidence that participation among middle and high school students is below national objectives (Lowry et al., 2001; McKenzie et al., 2000).
Violence. Children’s exposure to community violence in the United States, particularly among poor children living in urban settings, is strikingly high (Osofsky et al., 1993; Purugganan et al., 2000). The most extreme form of community violence, reflected in homicide rates, reached its peak in the early 1990s and has since been on a decline (Cole, 1999). Between 1985 and 1991, the homicide rate among youth ages 15–19 increased 154 percent, surpassing that of other age groups (Buka et al., 2001). Although the United States is experiencing a welcome decline in violence (Cole, 1999), homicide rates for youth remain among the highest compared with other age groups (http://www.ojp.usdoj.gov/bjs/homicide/teens.htm). Moreover, investigators estimate that homicide rates reflect only a small fraction (1/100th) of the violence witnessed or experienced by today’s youth (Rosenberg and Mercy, 1986).
An emerging literature suggests that the long-term consequences of childhood exposure to community violence are similar to those noted for child victimization. Children’s exposure to violence has been linked to a number of adverse health consequences, including depression, withdrawal, anxiety, posttraumatic stress disorder, fatigue due to sleep disturbance, poor school performance, participating in harmful events, having negative beliefs and attitudes toward others, and aggressiveness (Dyson, 1990; Pynoos et al., 1987; Kendall-Tackett, 2002; Buka et al., 2001; Zuckerman et al., 1995; Groves et al., 1993; Martinez and Richters, 1993). It is important to note, however, that this emerging literature lacks specificity, as it is currently not clear which types of exposure to violent events pose the greatest threat to children in terms of resulting in impaired social and emotional development and functioning.
Social Organization of Neighborhoods and Schools. Communities vary greatly in the degree to which people know each other, care about each other, and even share responsibility for each others’ children. These connections among people—social networks and the norms of reciprocity and trustworthiness that arise from them—are sometimes referred to as “social capital.” A higher level of social organization in a neighborhood is associated with better family and child outcomes (see National Research Council and Institute of Medicine, 1995b, p. 13; Sampson et al., 2002). Neighborhoods in which parents frequently come into contact with one another and share values are more likely to monitor the behavior of and potential dangers to children (Sampson, 1992; Sampson and Groves, 1989; Sampson et al., 1997).
Social organization is affected by the degree of sprawl in a community; increased sprawl restricts the time and energy people have available for civic involvement and reduces the opportunities for spontaneous, informal social interactions. Sprawl also is associated with decreased use of public facilities, reducing opportunities to mingle with other people, segregating people, and disrupting continuity of community across the life span. There also is evidence that mixed-use, walkable neighborhoods contribute to social capital, as measured by know-
ing one’s neighbors, participating in political life, trusting other people, and being socially active (Frumkin, 2002, 2003; Leyden, 2003).
The basic ingredients of neighborhood social organization can also be present in schools, although the ratio of ingredients differs (National Research Council and Institute of Medicine, 1995b). Schools can serve both as protective influences and as risk factors. Students may feel connected to the class, and a well-run class may in turn increase their feelings of connectedness (National Research Council, 2001). When students feel cared for at their school, they are less likely to use illicit substances, engage in violence, or initiate sex and are more likely to report higher levels of emotional well-being (Resnick et al., 1997).
Peer Influences. Peers and friends are important throughout childhood. Poor social acceptance is problematic for children during childhood and beyond. Socially rejected, aggressive 3–5-year-old children have demonstrated stress hormone levels in the top third of their class, often spiking to the “stress” level (National Research Council and Institute of Medicine, 2000). And children demonstrating difficulties with aggression and peer rejection in middle school are more likely than other children to have demonstrated such problems during their toddler years (Rutter, 1998). Children who were rejected during the school years are disproportionately represented among adults with psychiatric problems (Coie et al., 1992) and among those with subsequent legal altercations (Kupersmidt and Coie, 1990), although the pathway of influence is not well established in these studies.
Middle adolescence is the age of the adolescent subculture. The importance of the peer group increases, as well as the pressures to conform to it. At this time, the adolescent is seeking a stable (affiliative) rather than a distinct identity (Greydanus et al., 1990). Risky behaviors become important during this time both as a means to bond to a peer group and for youth who desire to confront adults (Greydanus et al., 1990). But peer group association can also be positive; for example, the strong orientation toward academic achievement among Asian Americans has a stronger association with having Asian peers than with Asian parents (Steinburg et al., 1992).
Multiple datasets spanning several decades and across cultural and geographic niches underscore the importance of peers, peer influence, and the selection of peers as friends as factors associated with adolescent behaviors and perceptions of the world (Jessor and Jessor, 1977; Stanton et al., 1994; Romer, 1994). Thus, for adolescents, like their younger counterparts, peer relations continue to play a role in both adolescence and beyond.
Electronic Media
Electronic media (television and video, video and computer games, and the Internet) have become an integral part of everyday life for many children in the
United States and thus warrant explicit discussion. Children spend more time watching television than in any other single activity except sleep (Huston and Wright, 1997). Children between the ages of 2 and 17 spend an average of 4.5 hours a day in front of screens, watching television, playing video games, and using the computer (Woodard and Gridina, 2000). The potentially adverse consequences of television viewing led the American Academy of Pediatrics to recommend that children under 2 years old should not watch television, and older children should not have television sets in their bedrooms (American Academy of Pediatrics, 1999b).
Violent Media Content and Aggressive Behavior. The association between viewing violent television programs and aggression has been well established (Bushman and Huesmann, 2001; Friedrich-Cofer and Huston, 1986; Huesmann and Eron, 1986). Across methodologies (laboratory experiments, field studies, and longitudinal studies) and measures, research has converged on findings that viewing television violence affects both short-term and long-term aggressive behavior (Friedrich-Cofer and Huston, 1986). A comprehensive meta-analysis of 217 studies of the association between antisocial behavior and media violence revealed the correlation between the two to be sizable: .31 (Paik and Comstock, 1994), a correlation only slightly smaller than that between smoking and lung cancer (Bushman and Anderson, 2001).
Because of the interactive nature of video games, both researchers and the public are particularly concerned about the effects on children of violent content in such games (Calvert and Tan, 1994). As with television, research has converged to suggest that playing violent video games contributes to aggressive behavior (Anderson and Bushman, 2001; Bensley and Van Eenwyk, 2001; Sherry, 2001), but in this case the research is mainly drawn from smaller (i.e., Ns of 50 to 150), largely white and middle-class convenience samples.
Media Use and Obesity. Not all empirical studies have established a positive association between television or video game use (or both) and increased weight or obesity in youth. The most widely cited study is by Dietz and Gortmaker (1985), who report that the prevalence of obesity in a large epidemiological sample of adolescents ages 12–17 increased 2 percent for each additional hour of television watched per week. Subsequent studies have confirmed this relationship (Dietz and Gortmaker, 1985; Robinson and Killen, 1995; Robinson et al., 1993; McMurray et al., 2000; Durant et al., 1994).
One way in which television viewing or video game use is thought to be related to increased weight in children is that time spent with these media displaces physical activity. Evidence for the displacement of physical activity by television is mixed, with some studies documenting decreases in participation in physical activities following the introduction of television into small, mainly rural, communities (Brown et al., 1974; Williams, 1986), but more representative
observational studies reporting little or no relationship between physical activity and television viewing (Robinson and Killen, 1995; Robinson et al., 1993; Durant et al., 1994).
A second hypothesis links television viewing, in particular, to increased caloric intake either from eating during viewing or as a result of food advertising on television, which tends to emphasize high-calorie, high-fat foods with poor nutritional content (Story and Faulker, 1990). There is some evidence that amount of television viewing is related to children’s requests for, and parental purchases of, highly advertised foods (Taras et al., 1989) and that television advertising may produce incorrect nutritional beliefs in children (Ross et al., 1981). There is also experimental evidence that there are direct effects of exposure to advertising for high-calorie foods on children’s snack choices and consumption (Gorn and Goldberg, 1982; Ross et al., 1981).
Effects of Sexual Messages and Sexual Content. Throughout childhood, adolescence, and young adulthood, people continually learn more about sex, with media being a major source of information (Brown et al., 2002; Dorr and Kunkel, 1990; Wartella et al., 1990). The average child will have viewed over 14,000 sexual simulations and sexual innuendos each year (Derkson and Strasburger, 1994). Experimental studies conducted largely with convenience samples of white, middle-class young adults (often college students) have documented negative effects of nonviolent but dehumanizing pornography, especially on attitudes toward women (Kenrick et al., 1989; McKenzie-Mohr and Zanna, 1990; Weaver et al., 1984). However, the evidence is particularly disturbing in the case of violent pornography. Two major reviews of the literature, one using meta-analytic techniques (Allen et al., 1995a) and the other a conceptual review (Malamuth and Impett, 2001), both conclude that sexual violence has been found to be arousing to sex offenders, force-oriented men, and sometimes even to “normal” young men if the woman is portrayed as being aroused by the assault.
Media Use, Cognitive Development, and Academic Skills. Theory and popular perception have proposed that because television viewing involves so little mental effort, it retards cognitive development and the development of such academic skills as reading (Healy, 1990; Winn, 1985). In the case of television, there is a large body of theory and empirical data showing that both the content and form of television programs affect children’s intellectual development and social behavior (Huston and Wright, 1997). Longitudinal studies have found that watching general-audience entertainment programming can have deleterious consequences on both academic and social outcomes (Anderson et al., 2001; Friedrich-Cofer and Huston, 1986; Huesmann and Eron, 1986). But both field experiments and longitudinal studies indicate that watching educational programming in early childhood is positively related to cognitive skills (Ball and Bogatz, 1970; Rice et al., 1990; Zill, 2000), school readiness (Wright et al., 2000),
and adolescent academic achievement (Anderson et al., 2001).
Much less is known about the effects of video games and computer technologies, but some theorists have proposed that the interactive character of these activities makes them more potent than television as sources of sensorimotor skill, intellectual stimulation, and messages about violence and other social behaviors (Calvert and Tan, 1994; Cocking and Greenfield, 1996; Greenfield, 1994). Researchers have demonstrated academic gains in young children of both genders, using developmentally appropriate software (i.e., software allowing children to control the program and make decisions) in academic settings in such skill areas as verbal ability, problem solving, and creativity (Haugland and Wright, 1997).
Cultural Environment
Culture is often defined by the ideas, beliefs, and values coupled with the rituals and practices of social groups, including but not limited to families. Betancourt and Lopez suggest that culture refers to “a distinct system of meaning or a cognitive schema that is shared by a group of people or an identifiable segment of the population” (García Coll and Magnuson, 2000, p. 97). Miller and Goodnow define cultural practices as “actions that are repeated, shared with others in a social group, and invested with normative expectations and with meanings or significances that go beyond the immediate goals of the action” (National Research Council and Institute of Medicine, 2000, p. 60). Thus, practices to prevent and promote health and provide treatment have to make sense and be congruent with these systems of meanings and practices. In addition, any self-report on health is embedded in these cultural constructions.
In the United States, the relationship of culture to health outcomes and their measurement is particularly significant because of the growth in diverse populations. It is estimated that by 2050, children of color will account for a majority of children in this country (Institute of Medicine, 1997). Consequently, dominant notions of health—mostly based on middle-class, northern European beliefs and practices—are increasingly out of alignment with the traditions, customs, and beliefs of those with other ancestries.
Culture affects health in many ways. One is by promoting daily activities and routines that reflect culturally defined goals and values that interact and influence developmental processes, inclusive of health (Gallimore et al., 1993; Rogoff, 1990). These routines can include, for example, health-promoting habits such as culturally prescribed foods and activities that provide adequate nutrition and caloric intake or patterns of mother-infant interaction (e.g., Harwood, 1992).
Culture also affects health by providing caregivers (and eventually children themselves) with an understanding of development and health: culture offers the context for defining what is a problem, explaining why the problem exists, providing possible treatments, and indicating who should respond (Groce and Zola,
1993; Harwood et al., 1999). Similarly, culture also provides a framework for the use of home remedies. There are studies on the use of cupping and coining, traditional practices in some cultures that have been confused with child abuse (Moy, 2003; Bullock, 2000; Hansen, 1998). Cupping, a practice used by various cultures including Chinese, Arabic, and Jewish, involves attaching cups on one’s back and creating a vacuum to evacuate a malady and increase blood flow to the region, leaving marks that can be confused with the result of trauma to the area. Similarly, coining is the practice of rubbing the edge of a coin on one’s skin as a treatment for an illness. Other examples of the importance of cultural meaning of health and disease definitions are the “empacho” theory used by Latin Americans (food is claimed to be “stuck” to the intestines causing vomiting, diarrhea, or early satiety—many families seek the help of folk healers or home remedies consisting of such dangerous substances as lead and mercury) and the use of “hot-cold” remedies, which were mentioned in Chapter 1 (Nuñez and Taft, 1985; Risser and Mazur, 1995).
In the United States, variables such as language proficiency, acculturation level, and recency of migration have all been identified as important sources of variability within cultures (Gutierrez et al., 1988) with significant impact on health. Biculturalism (identifying simultaneously with two cultures) rather than linear acculturation (adopting a single cultural identification over time) has been found to be related to better outcomes (Gil et al., 1994; Szaponick et al., 1981).
An interesting finding in the health literature is what has been termed the “Latino epidemiological paradox” (Markides and Coreil, 1986) or “the immigrant paradox” (Fuligni, 1997; Portes and Rumbaut, 2001), whereby recent immigrants who tend to be more economically deprived and less acculturated, or individuals from Hispanic backgrounds in general, tend to have better health outcomes than other groups from the same ethnic backgrounds or non-Hispanics (Hayes-Bautista et al., 2002; Hayes-Baustista, 2003). The mechanisms behind these surprising findings are not well understood. One possibility is that of selection bias; that is, first-generation immigrants to the United States may be the healthiest and most motivated subset of potential immigrant families. But it has also been hypothesized that traditional cultural practices serve as protective factors.
These and other findings have led investigators to posit cultural differences as sources of both risk and resilience (García Coll et al., 1996; García Coll and Magnuson, 2000). In other words, culture does not constitute a source of vulnerability or risk per se, but cultural differences can become a source of risk when (1) cultural differences are seen as deficits that need to be remedied or fixed, (2) cultural differences lead to mismatches between caregivers or the child themselves and members of dominant institutions, and (3) cultural differences lead to experiences of discrimination and diminished life opportunities due to segregation. There is evidence that these sources of stress are not limited to low-income
populations but are experienced by groups with higher socioeconomic backgrounds as well (McAdoo, 1981; Tatum, 1987).
Discrimination
A sparse but growing literature on discrimination, particularly regarding race and ethnicity, documents its effect on health. Krieger (2000) reviewed 20 research articles that used instruments to measure self-reported experiences of discrimination: the most common association with discrimination (10 studies) was with mental health; the second (5 studies) was with hypertension. Unfortunately, all studies concerned adults only.
A more recent review confirmed the findings of a substantial association between racial/ethnic discrimination and mental health, with additional associations with various physical health measures (Williams et al., 2003). In one study, simulated racial discrimination was associated with physiological dysfunction, which was associated with subsequent poor health (Harrell et al., 2003); again, the studies included adults only.
Van Ryn and Fu (2003) proposed a pathway through which health provider behavior in clinical or public health settings contributes to discrimination. In this case, the pathway would be as relevant to children as to adults, as adults generally accompany children in health services encounters and act as proxy for them. Nazroo (2003), reviewing evidence on ethnic discrimination from the United Kingdom, concluded that social and economic inequalities, underpinned by racism, are a fundamental source of ethnic inequalities in health across population subgroups. Chaturvedi (2001) suggested that recognition of different kinds of effects from racism, including on children, could help to sort out the pathways by which the multifactorial and interacting influences affect various aspects of health. To that effect, a recent review (McKenzie, 2003) provided added evidence for an effect of racism on health, including the documentation of racism as well as the mechanisms by which it operates.
SERVICES
Although few would debate the relevance of health services to improving individual health, many have actively debated the contribution of health services to the health of populations. In recent decades, writers such as Thomas McKinley have made strong arguments that improvements in population health have come more from improvements in other spheres (particularly nutrition) than from interventions provided by health services (McGinnis et al., 2002). Although there is increasing recognition of the effect of services in the behavioral and social arenas on health (Institute of Medicine, 1997, 2000), evidence regarding specific outcomes of these programs is limited.
In contrast, the medical literature is replete with reports of the effectiveness of specific biomedical interventions that influence the course of particular diseases. John Bunker has gone further and estimated that health services in general account for about half of improvements in health (measured as increases in life expectancy) in the most recent half-century (Bunker, 2001). While his monograph demonstrates the important role of health services, it reinforces the simultaneous importance of other influences.
The effect of social factors on health, and the possibility of their remediation, does not detract from the importance of health services, at least in part because one of the correlates of social factors is differential access to and appropriate use of health and other services. Documentation of the overall effect of services specifically on children’s health is more limited. A 1985 publication on the importance of health services on the incidence, prevalence, and severity of 16 important conditions in childhood (Starfield, 1985b) illustrated the importance of access to health services. However, this study provided no quantitative estimates of the total magnitude of effect of health services on the child population, and it predated numerous new vaccines and other general environmental improvements that have further reduced morbidity and mortality. It was also based on a model of health that was more disease-oriented than the multifaceted conceptualization of health proposed in this report.
In more recent years, it has become clear that the nature of health services, rather than simply their presence, is important. For example, an accumulating number of studies, both in the United States and abroad (as well as international comparative studies) have shown the importance of a strong primary care orientation in health services systems (Starfield et al., 1998). The benefits of a strong primary care orientation are even more salutary for children than for adults (Shi and Starfield, 2002).
Comprehensive, high-quality center-based early education has been demonstrated to improve a range of educational outcomes (National Research Council and Institute of Medicine, 2000). A growing literature supports the ability of early intervention services to intervene and modify developmental health trajectories in children who are at risk of developing developmental, behavioral, and mental health conditions (Ramey et al., 1992; Karoly et al., 1998; Olds and Kitzman, 1993; Olds et al., 1997, 1998, 1999). The availability and configuration of services in a given community can be logically assumed not only to affect a range of children’s health outcomes, but also to create a context for and to affect the range of other influences.
Figure 3-1 presents a theoretical framework modified from Halfon and Lawrence (2003) to illustrate how services can direct or modify a course of healthy development; modify predisease pathways; and minimize the risk of exposures before they occur, thereby actively promoting the development of health capacities. Services can reduce exposure to health-compromising events. For example, there is strong evidence that multiple doses of pneumococcal vaccine lead to
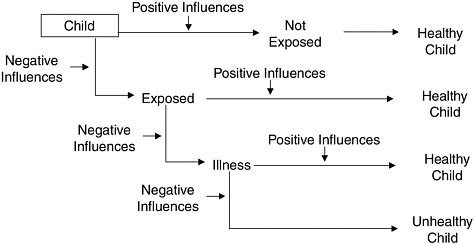
FIGURE 3-1 Where services can effect change in healthy development.
SOURCE: Adapted from Halfon and Lawrence (2003).
significant decreases in otitis media (ear infections) and subsequent hearing loss (Fireman et al., 2003). Public health activities to improve nutrition and public health education campaigns have resulted in health improvements. For example, introduction of folic acid in grain-based products decreased the risk of neural tube defects (Fletcher and Fairfield, 2002). The Back to Sleep campaign, aimed at educating adults on proper infant sleeping position, has been credited with a dramatic reduction in the occurrence of sudden infant death syndrome (Willinger et al., 1998).
Services can modify the relationship between exposure and the onset of disease once the child has been exposed—thereby altering the nature of the exposure outcome pathway. Children exposed to a case of meningitis may receive prophylactic antibiotics to avoid coming down with the disease themselves. Newborn screening identifies infants with phenylketonuria, enabling dietary modification that avoids adverse manifestations of the disorder.
Another way in which services influence health outcomes is to modify or reduce a disease or to promote a specific rehabilitation or habilitation process. For example, the lives of children with cystic fibrosis have been transformed and their prognoses improved as a result of service delivery systems that have lengthened life expectancy and improved functional capacity (Schechter, 2003).
Services relevant to children’s health include a broad array of interventions, such as health promotion and preventive services, diagnostic, treatment, and rehabilitative services, educational programs, and a variety of social services. They include specific health interventions, such as immunizations, as well as programs of integrated services that systematically address prevention, promotion, treat-
TABLE 3-1 Illustrative Services for Children, Youth, and Families
|
Prevention-Oriented |
Treatment-Oriented |
Long-Term Care, Home and Community-Based Care |
|
Early intervention programs; early literacy Infectious disease control Nutritional services Lactation services Exercise programs Safe sex education Injury prevention programs Topic-specific health education targeted at schools, child care, and parenting Media campaigns Environmental risk abatement programs (e.g., lead) Vision and hearing screenings AIDS education, testing, and counseling Smoking and substance abuse prevention Prenatal care; pre- and postpregnancy counseling Immunizations and well-baby care Developmental, behavioral, and mental health assessment and guidance Genetic screening and counseling |
High-risk mother and infant care services Emergency medical services Smoking and substance abuse cessation programs Acute medical care Mental health, behavioral treatment, and therapy Chronic disease management Medication management, rehabilitation therapies Crisis intervention High-risk mother and infant care services Emergency medical services Smoking and substance abuse cessation programs Acute medical care Mental health, behavioral treatment, and therapy Chronic disease management Crisis intervention |
Long-term inpatient mental health care Chemotherapy, cancer radiation treatment Convalescent and rehabilitation care Child protective services Home visiting Home health care Child care School-based clinics Case management care coordination Caregiver respite After-school programs Peer support groups for adolescents Social skills development, stress management School-based special education and rehabilitation for developmental delay, learning disability, mental health problems and programs for gifted and talented students |
ment, and risk reduction simultaneously, as is the case in model chronic disease management programs (American Academy of Pediatrics, 2002). Services function at several different levels, including the level of the individual child, family, and community, as well as larger social, physical, and policy environments.
Table 3-1 lists a range of potential services relevant to children’s health that reflects the committee’s conceptualization of it. While not exhaustive, this list depicts a continuum of services designed to improve the health of children and the functions they serve. It includes services provided by the personal and public health system, as well as the environmental health, education, and social service systems. Prevention-oriented services are shown to include health promotion services that are focused at the population level (e.g., injury prevention, anti-smoking campaigns), as well as services that are part of ambulatory health care provided through the primary care system (e.g., immunizations). Treatment-
oriented services include those that are provided in clinical encounters and ambulatory care settings (e.g., acute medical care), as well as those that are provided in hospitals (e.g., emergency services). Long-term, home, and community-based care includes community-based rehabilitative services designed to restore function (e.g., physical therapy), as well as habilitative services designed to maintain the development of function (e.g., speech or language therapy for children with language impairments).
Research is warranted to tease out the role that a range of services play in mediating and modifying influences so children can stay healthy, as well as supporting and promoting their optimal health. Improved specification of the effects of services, better targeting and customizing of services for specific populations, and improved monitoring of the effect of specific services on population health measures should be considered important research and analysis priorities.
POLICY
The health of children in the United States is affected by laws, rules, and regulations developed at the national, state, and local levels. These governmental actions determine the availability of publicly supported services and often regulate the provision of privately administered services. They are integral to how communities operate.
Policies directed specifically at health or health care services, such as eligibility for publicly funded insurance (Currie and Gruber, 1996a) or requiring a child to be immunized prior to starting school (Briss et al., 2000), have both intuitive and documented effects on children’s health. But many improvements in children’s health over the past century were also influenced by policies in areas other than health. Prominent examples include improvements in children’s health as a result of the decision to include vitamins in food products (e.g., vitamin D in dairy products and folic acid in cereals and breads) and fluoride in drinking water (Centers for Disease Control and Prevention, 2001); drinking water and food quality standards (Environmental Protection Agency, 1996; Perdue et al., 2003); educational and child care standards and programs (e.g., the Individuals with Disabilities Education Act); and environmental emissions and engineering safety standards (Perdue et al., 2003).
Innumerable serious injuries and deaths have been prevented by traffic safety standards, such as car seats and speed limits (Sleet et al., 2003; Farmer et al., 1999), consumer product safety standards (Sleet et al., 2003), and such building codes as requiring fencing around swimming pools and safety protections on high-voltage electrical equipment (Stevenson et al., 2003).
The policy environment also affects children’s health in less obvious ways. For example, welfare policy decisions play a role in families’ SES and even child achievement (see discussion below), and education policies play a role in the availability and quality of schools in a given community (Chase-Lansdale et al., 2003).
Although many policies affect children’s health, most are developed and implemented without formal consideration of their effect on children. It is beyond the scope of this report to provide a comprehensive review of all policies that have had an impact—or could have an impact—on children’s health. Instead, we illustrate the importance of policy with discussions of fluoridated water, children’s health insurance, and welfare reform.
Fluoridated Water
Fluoridation of drinking water has contributed to reductions in dental caries in both children and adults (National Research Council, 1993), and the Centers for Disease Control and Prevention (CDC) has highlighted water fluoridation as a significant public health achievement (Centers for Disease Control and Prevention, 1999b). Cross-sectional studies conducted in the mid-1900s showed water fluoridation to have an effect on dental caries and prompted policies to fluoridate water in many cities throughout the United States. A review of studies on the effectiveness of water fluoridation conducted in the United States between 1979 and 1989 found that caries were reduced between 8 and 37 percent among adolescents (Newbrun, 1989). There is some evidence that water fluoridation has been particularly beneficial for communities of low socioeconomic status (National Research Council, 1993; Riley, Lennon, and Ellwood, 1999), perhaps attributable to their disproportionate burden and lower access to dental care. Evidence of the effectiveness of water fluoridation in reducing dental caries has led to other approaches to introduce fluoride, including the addition of fluoride in toothpastes and topical fluoride treatment by dental professionals.
There has been some debate about whether water fluoridation increases the risk of a range of other health conditions, including cancer, osteoporosis, and Down syndrome. A review by the National Research Council (NRC) in 1993 concluded that there was no credible evidence to support these claims. The NRC is currently conducting a study to review the evidence since 1993 and advise EPA on the adequacy of its current water fluoride standards in the context of the variety of fluoride sources now available.
Health Insurance
The role of health insurance for health care access and service use2 has been a focal point of health policy and specifically children’s health policy over several
decades. In contrast to all other industrialized nations and despite frequent incremental attempts to expand health insurance coverage, a substantial proportion of children remain uninsured, and many more have inconsistent or inadequate health insurance (http://www.census.gov/prod/2003pubs/p60-224.pdf). While health insurance is an important contributor to access to and use of health services (Starfield, 2000a; Currie and Gruber, 1996a), it is far from the only factor. The availability and distribution of providers, the functioning of the primary care system, and multiple nonfinancial barriers are also important variables that affect health care access and use (Starfield et al., 1998; Halfon, Inkelas, and Wood, 1995).
The two primary publicly funded programs that provide health insurance for children—Medicaid and the State Child Health Insurance Program (SCHIP)—require families to demonstrate initial and continuing financial eligibility. Implemented in the 1960s, Medicaid coverage increased dramatically during the 1980s and early 1990s as a result of major policy changes in laws that sought to expand Medicaid eligibility (Currie and Gruber, 1996a). Although participation in Medicaid programs is far from universal (Cutler and Gruber, 1996), and most uninsured children still receive medical care, the increased access to health care afforded by Medicaid has been associated with better birth outcomes (Currie and Gruber, 1996b), lower rates of preventable illness (Starfield, 1985a) and improved efficiency of medical care delivery (Dafny and Gruber, in press).
In 1997, SCHIP was initiated to provide further health insurance coverage for uninsured children. SCHIP provided additional funds to states to expand their health insurance coverage by either using Medicaid expansion or, alternatively, developing state-run health insurance programs for children. Despite these efforts to expand insurance coverage, far-from-universal SCHIP program take-up and other factors still left 9.2 million children without health insurance coverage in 2001 for the full year (http://www.census.gov/prod/2003pubs/p60-224.pdf; LoSasso and Buchmueller, 2002). An additional number lack insurance for part of the year. States with policies that facilitate eligibility and certification procedures have been shown to have higher rates of enrollment (Dick et al., 2003).
Health insurance of any type cannot facilitate access to health care services when the necessary resources are not present. In the absence of national health insurance, national health policy has supported the development of a safety net of services in the form of community health centers in areas with a shortage of health facilities and personnel. Currently there are about 800 such centers across the country, all of which provide high-quality primary care services. Recent evaluations indicate that the presence of these centers improves the health of children and reduces racial disparities among the populations who receive services from them (Politzer et al., 2001; Shi and Starfield, 2000).
Welfare Policy
From a policy perspective, it is important to ascertain to what extent policies directed at families or adult family members, even if not explicitly targeted on child well-being, in fact alter children’s chances of healthy development. We illustrate this kind of policy analysis with the welfare reform law (the Personal Responsibility and Work Opportunity Reconciliation Act of 1996), which was directed first and foremost at increasing the employment and reducing the welfare dependence of mothers.
Evidence on the likely effects of welfare reforms comes both from random-assignment experiments and from longitudinal survey studies (National Research Council and Institute of Medicine, 2003). A key finding from the experiments is that effects on the achievement and behavior of younger children were consistently more positive in programs that provided financial and in-kind supports (earnings supplements) for work than in those that did not. The packages of work supports were quite diverse, ranging from generous earnings supplements provided alone to more comprehensive packages of earnings supplements, child care assistance, health insurance, and even temporary community service jobs. At the same time, these experiments produced evidence of negative effects on adolescent achievement across all types of programs, although a prominent nonexperimental study did not replicate the negative adolescent results (Chase-Lansdale et al., 2003). Systematic approaches to evaluate the effect of policies on children of this sort are the exception, rather than the rule, and few other systematic attempts can be identified.
CONCLUSION
This chapter provides a discussion of evidence concerning the influence of various types of characteristics on the health of children. Although imperfectly understood, the important role of interactions of these influences, which may differ in kind and amount at different ages and stages of development, is amply supported by the evidence. Notably absent from most of the discussion, however, is the relative importance of the various types of influences on children’s health at different ages. For the most part, evidence for the influences comes from studies of the relative risk imposed by them. However, exposure to influences differs in frequency from one influence to another. Influences that have a high relative risk may be of only minor importance to the health of the population of children if they are relatively uncommon. In order to understand the effect of these factors on the health of children, such information is critical (see Goodman et al., 2003).














































