
7
Substance Abuse and Cigarette Use
This chapter discusses enlistment standards and related issues in the general areas of substance use and abuse, specifically alcohol, drugs, and cigarettes. While there are specific enlistment standards that relate to alcohol and drug abuse, currently there are no enlistment standards with respect to smoking cigarettes. There has been considerable interest, however, in whether smoking impacts military effectiveness, and both the Army and the Navy have undertaken longitudinal studies to examine (among other things) the effect of cigarette smoking on attrition and other outcomes. Some studies suggest that preservice smoking is related to behavioral issues that correlate with injury and attrition.
The chapter has two sections, one for alcohol and drug abuse and one for cigarette use.
ALCOHOL AND DRUG ABUSE
Current Requirements and Enlistment Standards
The general U.S. Department of Defense (DoD) requirements relating to alcohol and drug abuse are set forth in DoD Directive 1304.26 under “Moral Character.” The DoD standard is quite general, stating only that individuals should be disqualified “who have exhibited antisocial behavior or other traits of character that would render them unfit to associate with military personnel.” Military leaders generally agree that individual performance and unit morale would suffer greatly if individuals were allowed to be drunk or be high on drugs while on duty.
As with most moral character standards, the specific standards for alcohol and drug abuse are set by each Service, although there are some broad similarities across them. Generally, a history of more severe types of alcohol and drug abuse or dependence is disqualifying, but limited “recreational” use of marijuana does not now require a waiver. Prior to 1990, even limited use of marijuana required a waiver, but that waiver requirement was phased out by the Services during the early 1990s. Alcohol use does not require a waiver unless the recruit tests positive at the physical.
Between these two extremes, the Services distinguish several degrees of severity of drug and alcohol abuse, and there are some important differences among the branches. The specific standards for each level of severity are summarized in Table 7-1. The table shows that drug trafficking, the most severe abuse, is disqualifying for all Services, and alcohol dependence is disqualifying for all Services except the Navy (which requires a waiver if no longer dependent). All Services also agree that limited or recreational use of marijuana use does not require a waiver.
If an applicant has a positive test for drugs other than marijuana during the physical, the Air Force will disqualify but the other three Services will issue a waiver if the applicant reapplies one year later and the retest is negative. The Army, Navy, and Marine Corps will issue a waiver for a positive test for marijuana or alcohol if a retest is negative six months after the original positive test. The Air Force is more stringent and, in fact, a positive test for marijuana is disqualifying. The Air Force will issue a waiver for a positive alcohol test if the recruit gets treatment and is alcohol-free for two years.
Limited preservice use of drugs other than marijuana and alcohol has the most diverse standards. The Army does not require a waiver, while the Marine Corps will issue a waiver after the applicant fills out a drug abuse screening form. The Air Force will issue a waiver for nonnarcotics, such as amphetamines and barbiturates, but narcotics are disqualifying. Finally, the Navy also distinguishes between nonnarcotic and narcotic drugs. In the case of nonnarcotics, the Navy does not require a waiver if the use was more than one year prior to screening, but narcotics use requires a waiver if use was over one year prior. Use within the past six months is disqualifying.
Youth Characteristics and Supply Issues
Trends in Substance Abuse
Current enlistment standards reflect the reality that some consumption of alcohol is commonplace among youth, despite the fact that in most
TABLE 7-1 Summary of Military Standards for Alcohol and Drug Abuse
|
Type of Use/Abuse |
No Waiver Required |
Waiver Possible |
No Waiver Possible |
|
Drug trafficking |
|
|
All Services |
|
Alcohol/drug dependence |
|
Navy: If no longer dependent |
Army, Air Force, Marine Corps |
|
Positive test for other drugs |
|
Army: If retest negative after one year Navy: Same as Army Marine Corps: Same as Army |
Air Force |
|
Positive test for marijuana or alcohol |
|
Army: If retest negative after six months Navy: Same as Army Marine Corps: Same as Army Air Force: Alcohol—if treated and abstains for two years |
Air Force: Marijuana |
|
Chronic marijuana use |
|
Navy: No use in past year Navy: If used during past year |
Army, Air Force, and Marine Corps |
|
Limited Use of Other Drugs |
|||
|
Stimulants and depressants |
Army: Must disclose Navy: Use more than one year ago |
|
Navy: Use within six months |
|
Narcotics |
Army: Must disclose |
Navy: Use over one year ago |
Navy: Use within six months |
|
Limited use of marijuana |
All Services |
|
|
|
SOURCE: HumRRO, Moral Character Enlistment Standards, preliminary report (1998). |
|||
states it is illegal to consume any alcoholic beverage under age 21. Moreover, occasional or “recreational” use of marijuana is also fairly common among youth, and the military decided during the early 1990s that occasional use of marijuana would not be disqualifying under moral character standards. Supply issues are therefore more focused on heavy or chronic use of illicit drugs or alcohol, especially when they indicate drug depen-
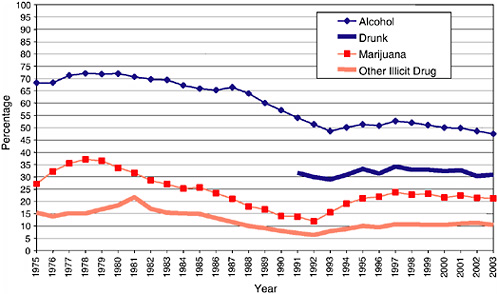
FIGURE 7-1 Trends in substance abuse by high school seniors during the past 30 days.
SOURCE: Johnston et al. (2004).
dence. In examining trends in youth characteristics, then, we distinguish between mere use of alcohol or marijuana and more chronic indicators of abuse, such as being drunk or using illicit drugs other than alcohol.
The best information on trends in substance abuse for the youth population comes from long-term national surveys conducted by the Monitoring the Future project at the University of Michigan. These surveys started in 1975, so the project has produced nearly 30 years of long-term data on use of cigarettes, alcohol, and drugs. The survey samples 8th, 10th, and 12th grade students, but for the purpose of recruiting standards, the high school senior group provides the most relevant data.1
Figure 7-1 shows trends in alcohol and illicit drug use for high school seniors from 1975 to 2003. All substance abuse measures discussed in this chapter are based on use during the past 30 days, which is more indicative of chronic or regular usage. There are two indicators for alcohol: any consumption and being drunk (a measurement that began in 1991). Interestingly, alcohol consumption dropped significantly between 1980 and
1993, from a high of over 70 percent to a low of about 50 percent. It has fluctuated only slightly since that time, standing at about 47 percent in 2003. The percentage of those who were drunk in the past 30 days has changed very little between 1991 and the present, standing at just over 30 percent in 2003.
Marijuana use also shows a steep drop between 1978 and 1992, from a maximum of 37 percent to a low of 12 percent. The rate began rising again in the early 1990s and reached a more recent maximum of just under 25 percent in 1997, and it has remained at about that level since that time. The use of other illicit drugs is about half the level of marijuana, and it shows a similar pattern but with somewhat less pronounced swings. The rate of other illicit drug use has remained very close to 10 percent for the past eight years or so. On the basis of the recent trends shown here, it is reasonable to assume that these rates will probably remain at about the same levels for the next 5 to 10 years.
Substance Abuse by Gender and Race/Ethnicity
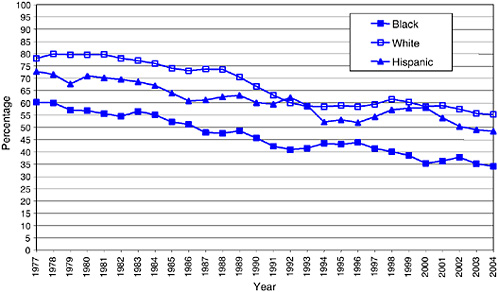
Figures 7-2a and 7-2b show the trends in alcohol consumption separately for six gender-by-race groups. Both gender and race/ethnicity are related to rates of alcohol use, but the gender effects are much smaller than the race effects. Interestingly, both male and female white youth have the highest rates of alcohol consumption and black youth the lowest. Hispanic youth are in between but are closer to whites than blacks in their consumption rates. During the early part of this time span, white male rates were about 10 points higher than white female rates, starting in 1985 or so the difference has been only about 5 points. By 2004, about 55 percent of white young men report recent drinking compared with 50 percent of white young women.
Alcohol use for black youth is substantially lower than for white youth, and this is true for both genders. Like white youth, the trends for blacks show substantial declines since 1975, and the difference between genders is somewhat larger. In 2004 the rate of recent drinking was 35 percent for black young men compared with 25 percent for black young women. Again, Hispanics rates are about 5 points below white rates for both genders.
Illicit drug use by race and gender is shown in Figures 7-3a and 7-3b. Interestingly, total illicit drug use among young men differs very little among the three races, particularly in the past 10 years or so. Generally, black youth reveal the lowest rates, and in 2004 the rates are 28 percent for white, 25 percent for Hispanic, and 22 percent for black young men. The race differences are larger for young women. The trend patterns are similar to those for the total youth population, but black young women have
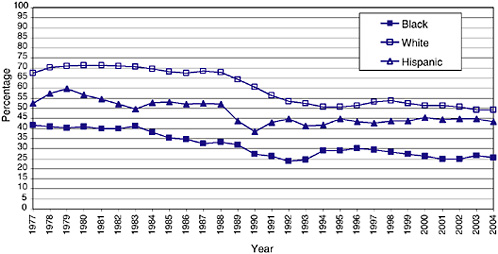
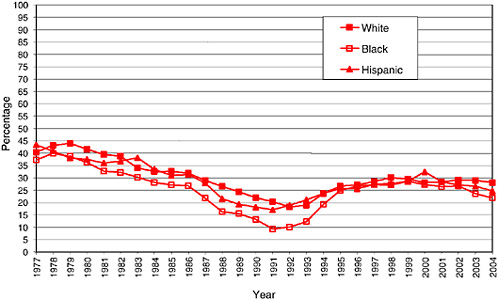
rates that are consistently 10 points below white young women. In 2004 the rates of illicit drug use are 23 percent for white, 16 percent for Hispanic, and 13 percent for black young women.
Substance Abuse and Military Performance
What is the evidence on the relationship between substance abuse and military performance? The primary outcome for evaluating moral character standards has been attrition rates. Since serious substance abusers are ineligible for enlistment in the first place (e.g., chronic alcoholism, dependence on illicit drugs), the main question here concerns waivers granted for less serious forms of substance abuse as outlined in Table 7-1. Since occasional use of marijuana no longer requires waivers, we are restricted to evaluating attrition for enlistees who enter with some type of drug or alcohol waiver.
Attrition rates for all major waiver categories were obtained from the Defense Manpower Data Center (DMDC) for fiscal year (FY) 2000 through FY 2003 (see the tables in Appendix B for the full attrition analysis). Waiver categories are distinguished for alcohol abuse only, marijuana use only, both drugs and alcohol, and illicit drugs other than marijuana. We combined the marijuana category with the drug and alcohol category (which had small numbers) and requested 12-, 24-, and 36-month attrition rates.
Alcohol Abuse and Other Illicit Drugs
We found that in recent years the Services have granted very few waivers for alcohol abuse alone or other illicit drugs alone. For the past several years, fewer than 76 persons each year entered with alcohol abuse waivers, and only about 100 had waivers for illicit drug use other than marijuana. The very small number of waivers means that attrition rates cannot be reliably measured; therefore, the impact of these two behaviors on attrition rates was not evaluated for these two categories. Regardless of attrition, the number of waivers is so small that there is no reason to change enlistment standards for these two conditions and no reason to consider the effectiveness of in-service treatment programs. In effect, the Services accept very few individuals who test positive for alcohol or illicit drugs other than marijuana.
Marijuana Use
As mentioned earlier, no waiver is required for persons reporting limited marijuana use before entry and the drug test is negative at the physical examination. However, a substantial number of waivers are
TABLE 7-2 Attrition Rates for Accessions with Marijuana Waivers
|
|
Attrition rates (by percentage) |
|||
|
|
Accessions |
12-month |
24-month |
36-month |
|
Marijuana waivers |
||||
|
FY 2000 |
|
|||
|
Men |
2,168 |
17 |
27 |
34 |
|
Women |
180 |
31 |
42 |
48 |
|
Total |
2,348 |
18 |
28 |
35 |
|
FY 2001 |
|
|||
|
Men |
2,604 |
16 |
30 |
37 |
|
Women |
253 |
27 |
38 |
46 |
|
Total |
2,857 |
17 |
31 |
38 |
|
No waiver |
||||
|
FY 2000 |
|
|||
|
Men |
119,282 |
14 |
21 |
26 |
|
Women |
29,386 |
20 |
28 |
34 |
|
Total |
148,668 |
15 |
22 |
27 |
|
FY 2001 |
|
|||
|
Men |
125,831 |
13 |
20 |
25 |
|
Women |
29,940 |
19 |
27 |
34 |
|
Total |
155,771 |
14 |
22 |
27 |
granted for marijuana usage as indicated by a positive test at the physical (the Air Force does not grant waivers for this condition; see Table 7-1).
Table 7-2 shows the number of accession and attrition outcomes for persons given marijuana waivers compared with accessions and attrition outcomes for persons without any type of waiver for FY 2000 and FY 2001. The number of waivers range from 2,000 to 3,000 per year, which is only about 1.5 percent of total accessions. Interestingly, 12-month attrition rates are only slightly elevated for persons with marijuana waivers, by about 3 percent in both years (18 and 17 percent versus 15 and 14 percent, respectively). Also, it should be noted that attrition rates are somewhat higher for female drug waivers than male drug waivers, although the number of women receiving waivers is very small.
Attrition rates at 24 months are more elevated for those with marijuana waivers; the difference is 6 percent in FY 2000 and 9 percent in FY 2001. Even this difference is modest. Finally, the difference gets somewhat larger by 36 months. After three years of service, attrition rates are elevated by about 10 percentage points for marijuana waivers compared with persons with no waivers. It should be noted that this difference is
substantially less than the attrition rate difference for high school graduates compared with nongraduates shown in Chapter 3.
It appears that those with marijuana waivers get through the training period with no higher likelihood of leaving the services prematurely than those without waivers. The fact that attrition rises at a somewhat higher rate over time for those with waivers could indicate the effect of the random testing program on those with waivers who continue to use marijuana; the longer a marijuana user stays in the military, the more likely he or she will be caught by the test and dismissed.
Cost-Performance Trade-Off Analysis
It is unclear at this point whether a formal cost-performance analysis would suggest any changes to the enlistment standards being used for substance abuse behavior. First, we have observed only a small number of waivers for alcohol dependence or nonmarijuana drug use, so as long as these numbers remain low, these waivers do not impact appreciably on recruiting numbers. Second, attrition rates for marijuana use are only slightly elevated at the 12-month point, when a cost-performance analysis is most pertinent, because this is the period when the largest training investments occur. Moreover, the attrition differences at 24 and 36 months are greater but still modest at the 24-month point. On one hand, it is not clear whether these elevated rates would justify changes in the waiver policy, because the longer persons stay in the Service past 12 months (the maximum length of most training periods), the more likely they are to repay the initial training investment. On the other hand, there are relatively few of these waivers (1.5 percent), which means excluding all of them would not have a very large impact on recruiting costs. A formal cost-performance trade-off analysis would be required to test whether stricter standards for marijuana waivers would be cost-effective.
Conclusions and Recommendations
Few persons enter the military with serious substance abuse, but about 1.5 percent of accessions enter with a marijuana waiver. Attrition is not significantly elevated at 12 months of military service for those with marijuana waivers, but it is modestly elevated at 24 and 36 months of service. It is unclear at this point whether a cost-performance analysis would suggest any changes to the current standard, since the savings from reduced training costs may or may not exceed the additional costs of recruiting.
Recommendation 7-1: We recommend that DoD undertake a formal cost-performance trade-off analysis to determine whether a stricter standard for marijuana waivers would be justified on cost-effectiveness grounds.
CIGARETTE USE
Current Standards and Requirements
Cigarette smoking has periodically surfaced as an issue in the U.S. military. Historically the military has been seen as a safe haven for smokers, a place where smoking was not only accepted but often encouraged. As far back as 1898, when the Navy’s surgeon general threatened to ban cigarettes aboard ships, he was forced to back down because of a potential mutiny (Moyer, 2000; Patrone, 1996). By World War I, American soldiers began receiving tobacco rations, which were promoted by such military leaders as General John J. Pershing, commander of American forces in France (London, Whelan, and Case, 1996:40): “Tobacco is indispensable as a daily ration. We must have thousands of tons of it without delay. It is essential for the defense of democracy.”
The practice of tobacco rations ended in 1975. Military veterans are also familiar with the expression, “The smoking lamp is lit,” a centuries-old nautical term to indicate that smoking was permitted. For many years, military exchanges sold cigarettes with large price discounts, free from the warning labels required on cigarette packages sold in the civilian market (Evans, 1998).2
As it turned out, the smoking lamp was lit quite often in the military. This may help to explain why three-quarters of all military veterans have smoked, according to studies in the late 1990s (Harris, 1997).3 In 1996, DoD estimated that 448,000 active-duty members were smokers (32 percent of the total force), and that smoking costs DoD about $530 million annually in health expenses, along with $345 million in lost productivity. The Worldwide Survey of Substance Abuse Among Military Personnel indicated that the proportion of military members who smoked declined
during the 1980s and 1990s, as it did in the civilian world. At the same time, smokeless tobacco gained popularity, especially in the Marine Corps, where almost half of all young men under the age of 25 were reported to be users (Moyer, 2000).
Many of the military’s smokers picked up the habit before entering military service. A 1988 survey of Navy recruits, for example, suggested that 28 percent were cigarette smokers when they began boot camp. Around the same period, the Worldwide Survey of Substance Abuse showed that nearly half of the Army’s enlisted personnel in the junior pay grades (E-1 to E-3) were smokers, while the comparable rates for the other Services were 39 percent in the Marine Corps, 37 percent in the Navy, and 29 percent in the Air Force (Moyer, 2000:13).
Results from the DoD Survey of Health-Related Behaviors conducted in 2002 shows that cigarette smoking is widespread in all branches of the military, although not more widespread than among civilians with comparable demographic characteristics (Bray, 2004). This particular survey (discussed further in a later section) also indicates that nearly one-third of the military’s smokers brought the habit with them when they joined.
Currently, there are no enlistment standards with respect to the use of tobacco or cigarette smoking. However, there has been considerable interest in the military research community on the consequences of smoking on a variety of outcomes, such as health costs and first-term attrition. Several studies have found that cigarette smokers have elevated first-term attrition rates and have suggested that tobacco smoking—perhaps in combination with other applicant characteristics—might be the basis for improved screening techniques. Consequently, this section presents a summary of enlistment standards issues with regard to cigarette smoking and discusses steps DoD might consider in dealing with smoking behavior.
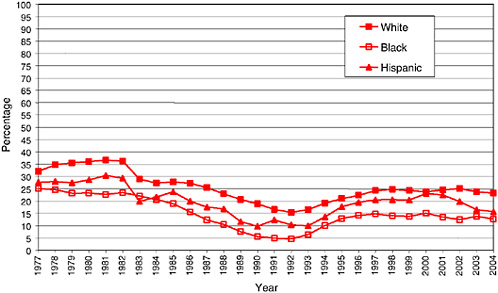
Youth Characteristics and Supply Issues
Figure 7-4 shows trends in cigarette smoking during the past 30 days for all high school seniors from 1977 to 2004. Two indicators are used: the percentage who smoked cigarettes at any time during the past 30 days and those who smoked daily. The rate of recent daily smoking is probably a better indicator of nicotine dependence; and this rate is about 10 points lower than recent episodic smoking. Generally, both indicators of smoking rates declined during the 1970s, remained fairly flat during the 1980s, and began increasing during the 1990s (when marijuana use also began rising). Cigarette smoking rates reached a peak in 1997, and then the rates began declining. By 2003, both rates had reached historic lows of 24 percent for any smoking and 16 percent for daily smoking. The Monitoring

FIGURE 7-4 Cigarette smoking in the past 30 days, high school seniors.
SOURCE: Johnston et al. (2004).
the Future data strongly suggest that cigarette smoking is on the decline among high school seniors in the United States.
Unlike illicit substances, cigarette smoking is illegal only for youth under age 18, and many states have aggressive policies that penalize retailers who sell cigarettes to underage youth. Accordingly, the prevalence of cigarette smoking among high school seniors may not accurately reflect smoking behaviors in the total youth population. Indeed, the National Survey on Drug Use and Health (NSDUH) reveals much higher prevalence rates among older youth and young adults (http://www.oas.samhsa.gov/nhsda).
Figure 7-5 presents the prevalence of any cigarette smoking during the past 30 days by detailed age categories for the total U.S. population. Prevalence rates increase sharply every year during the teens, rising from about 15 percent at age 15 to a peak of about 45 percent at ages 20 or 21. The rate then remains relatively flat until about age 23, when it begins declining, and it then declines steadily thereafter until it reaches a low of about 10 percent for persons 65 and over. Importantly for our purposes, the rate of cigarette smoking for young adults ages 20 to 22 is nearly double the rate for high school seniors.

FIGURE 7-5 Any cigarette smoking in the past 30 days, total population by age, 2002 and 2003.
SOURCE: Johnston et al. (2004).
The NHDUH also reports smoking rates by gender and race/ethnicity (<http://www.samhsa.gov/nhsda/2k3tabs/Sect2peTabs1to56.htm>, Table 2.27B [accessed 2003]). For youth ages 18 to 25 in 2003, the rate of smoking during the past 30 days was 52 percent for men compared with 38 percent for women. Consistent with the data on illicit drug use, white youth have the highest rates of smoking at 50 percent, while both blacks and Hispanics have considerably lower rates of cigarette smoking at 34 and 36 percent, respectively. It should be noted that gender differences are much smaller for high school seniors, perhaps because of the legality issue.
What about cigarette smoking among military personnel? Since most first-term military personnel are over age 18, the Monitoring the Future data do not offer a good comparison group for smoking behaviors in the military. There is a fairly recent survey of health behavior among military personnel, and this survey also made a comparison with the civilian population using NSDUH data for similar age groups (Bray et al., 2002).
Table 7-3 compares the percentage reporting any smoking in the past 30 days of military and civilian populations broken down by gender and age groups. The DoD study used the 2001 NSDUH results for the civilian
TABLE 7-3 Any Smoking During the Past 30 Days (percentage)
|
Age/Gender |
DoD |
Civiliana |
|
Men |
||
|
18 to 25 |
45 |
42 |
|
26 to 55 |
24 |
25 |
|
All ages |
33 |
32 |
|
Women |
||
|
18 to 25 |
30 |
27 |
|
26 to 55 |
22 |
22 |
|
All ages |
26 |
24 |
|
Total |
||
|
18 to 25 |
40 |
42 |
|
26 to 55 |
24 |
24 |
|
All ages |
31 |
32 |
|
N |
41,367 |
8541 |
|
aBased on the National Household Survey on Drug Abuse for 2001. SOURCE: Adapted from Bray et al., Department of Defense Survey of Health Behaviors (2002). |
||
comparisons, and it also standardized civilian rates on sociodemographic characteristics so they would be comparable to the military population. Thus the civilian smoking rates shown in this table are not strictly comparable to the smoking rates shown in Figure 7-5.
Two important findings are revealed by the DoD study. First, there is almost no difference in cigarette smoking rates between military and civilian populations of comparable ages and gender. Second, there is a very substantial difference in smoking rates by age group, especially for men. Military men ages 18 to 24 are nearly twice as likely to smoke as those ages 25 to 55 (45 versus 24 percent, respectively). The age difference for women is less pronounced but still significant (30 versus 22 percent). The younger age group overlaps considerably with first-term enlistees, while the older age groups would be comprised primarily of career force members. It should be noted that the prevalence rates for nonsmokers in Table 7-3 are similar to the Army and Navy rates of nonsmokers among recruits discussed in the next section.
The military-civilian comparison discussed to this point has focused on any cigarette use in the past 30 days. The Monitoring the Future data
show that daily cigarette smoking was substantially lower than any smoking during the past 30 days. Similarly, the 2002 DoD Health Survey distinguished a subcategory of “heavy smoking.” The rate of heavy smoking in the military was 13 percent in 2002, which is virtually the same as the rate of heavy smoking in 1998 (no comparisons with the civilian population were offered). There were few important differences across the Services, with the exception of the Air Force, in which heavy smoking was 10 percent. The rate of Navy heavy smoking in the DoD survey is similar to its rate of heavy drinking in the Navy study reported in a later section.
Cigarette Smoking and Military Performance
The fact that younger military and civilian populations have similar rates of smoking says nothing about whether smoking has adverse effects on military performance. It is well-documented in medical research that smoking leads to a higher risk of certain diseases, particularly emphysema, cancer, and heart disease. However, most of these diseases do not usually manifest themselves until a person is older, and therefore smoking may not create significant health care costs during the first term of enlistment. Smoking does, however, have adverse affects on physical fitness and on attrition. The following sections treat these in turn.
Injury Risk
In 2000, Jones et al. identified smoking as an injury risk factor that should be addressed in implementing a comprehensive injury prevention program for the military. In a cohort study of nearly 2,000 Army recruits, Altarac and colleagues (2000) identified smoking as a risk factor for injury during basic training. Using a multivariate analyses and controlling for age, education, race, body mass index, and physical fitness, he found that the risk of any injury during basic training was 1.5 times higher in smokers than nonsmokers for men (95 percent confidence interval, CI: 1.1, 2.0) and 1.6 times higher for women (95 percent confidence interval, CI: 1.2, 2.2). The results also showed a modest dose-response relationship between the number of cigarettes smoked in the month prior to basic training and the risk of injury. Similar relationships between smoking and injury in military training have been found in the Army and the Marine Corps (Jones, 1993b; Jones, Shaffer, and Snedecor, 1999) and among Norwegian conscripts (Heir and Eide, 1997). The latter study showed that smokeless tobacco was also related to injury.
A number of recent observational studies have noted that smoking is associated with musculoskeletal disorders and disabilities in the military (Lincoln et al., 2003; Dunn et al., 2003) and civilian workforces (Khatun,
Ahlgren, and Hammarstrom, 2004; Palmer et al., 2003; Thorbjornsson et al., 2000; Leino-Arjas, 1998), even after adjustment for other covariates. Furthermore, smoking has been identified as a risk factor for exercise-related injury in women (Gilchrist et al., 2000).
The mechanisms by which smoking increases the risk of injury warrant detailed investigation. Hier and Eide (1997) proposed a number of these, including reduced regional blood flow to working tissue, metabolic and circulatory effects, and neuromuscular effects. Furthermore, smoking may limit the ability of the recruit to maintain healthy bone and to repair tissue micro damage, which may lead to chronic injury during the repetitive stresses imposed during basic training.
Attrition
High rates of attrition are costly to the military, and a general goal of recruiting policies is to screen out persons with a high likelihood of early attrition. Attrition at 12 months or at the end of specialty training is the most costly type of attrition, because training expenditures are at their maximum and enlistees have not yet contributed any productive man-hours in their jobs or units. Attrition at 3 months is somewhat less costly because of smaller training investments, while attrition at 36 months (or even 24 months) is less costly because trained man-hours have recouped at least some of the initial training investment.
Several recent studies have assessed the effect of cigarette smoking on first-term attrition. Studies were carried out for the Air Force (Klesges et al., 2001), the Army (Strickland, 2004), and the Navy. The Air Force study found that 12-month attrition rates were 19.4 percent for smokers compared with 11.8 percent for nonsmokers. The authors state: “The results of the current investigation suggest that smoking is the single best indicator of premature discharge over one year of training from the U.S. Air Force” (Klesges et al., 2001:9). This study estimated that the higher attrition rate of preservice smokers represents $18 million in higher training costs annually for the Air Force.
We think the Air Force study did not use the correct methodology to arrive at this estimate. We assume that the average cost of training per recruit up to 12 months is $20,000. Applying the formulas presented in Chapter 3, we estimate that the cost of attrition due to smoking (given the Air Force attrition rates and recruiting statistics) would be closer to $38 million per year. However, this is only half of the cost analysis. In order to determine whether screening out smokers would be cost-effective (ignoring, for the time being, the question of whether smokers could be identified in an operational screening environment), we have to also consider
TABLE 7-4 12-Month Attrition Rates by Smoking Status
|
|
No Attrition |
Attrition |
Total |
% Attrition |
% Prevalence |
|
ARMYa |
|||||
|
None |
12,232 |
2,031 |
14,263 |
14.2 |
49.7 |
|
<Daily |
4,585 |
781 |
5,356 |
14.6 |
18.7 |
|
Daily |
7,024 |
2,043 |
9,067 |
22.5 |
31.6 |
|
Totals |
23,841 |
4,855 |
28,686 |
16.9 |
100.0 |
|
NAVYb |
|||||
|
None |
3,482 |
811 |
4,293 |
18.9 |
49.2 |
|
Light |
2,201 |
741 |
2,942 |
25.2 |
33.7 |
|
Heavy |
951 |
547 |
1,498 |
36.5 |
17.2 |
|
Totals |
6,634 |
2,099 |
8,733 |
24.0 |
100.0 |
|
aSmoking defined by frequency of smoking during 6 months before the delayed entry program. bSmoking defined by volume “until recently”; heavy = 1 pack a day or more. |
|||||
the higher recruiting costs associated with excluding a significant portion of the youth population.
A summary of 12-month attrition rates for the Army and Navy studies is shown in Table 7-4. We stress that the Army and Navy studies defined smoking differently. The Army distinguished among frequency categories, with daily smoking being the highest (during the six months before the delayed entry program); the Navy distinguished the quantity of recent smoking, with a pack or more a day being defined as a heavy smoker.
For the Army, the 12-month attrition rate was 22 percent for daily smokers compared with 14 percent for nonsmokers. This 8-point difference is comparable to the 7-point difference found for the Air Force. The Army study also found that there is no elevated attrition for light smokers, consisting of everyone who smoked less than daily. The prevalence of daily smoking is 32 percent; therefore, excluding daily smokers from the Army would clearly raise recruiting costs appreciably, thereby under-scoring the importance of a cost-performance trade-off analysis.
In the Navy study, the 12-month attrition of heavy smokers (those smoking at least a pack a day) is nearly twice that of nonsmokers, 36 percent compared with 19 percent. The attrition rate of light smokers (25 percent) is also elevated, but to a much lesser extent. The prevalence of heavy smokers is only 17 percent; excluding them would therefore not raise recruiting costs as much as excluding daily smokers in the Army. Of
course, there may not be a reliable method for distinguishing between heavy and light smokers.
We cannot be certain as to the reasons for different results in the Army and Navy studies. It could simply be the different definitions, with the Army measuring frequency and the Navy measuring quantity. There is some support for this interpretation in the data themselves, since the Navy’s prevalence of heavy smoking is much smaller than the Army’s prevalence of daily smoking. On one hand, it is quite likely that some daily smokers smoke less than a pack a day, and therefore heavy smokers are a subset of daily smokers. On the other hand, there is some concern about the representativeness of the Navy sample, because the overall 12-month attrition rate of 24 percent is much higher than the 17 percent reported by the Defense Manpower Data Center for the Navy in 2001 and 2002.4
Both studies of Army and Navy recruits suggest a relationship between preservice smoking and behavioral factors. In the detailed study of the 1999 Army cohort, McCloy and Putka (2004) found that smoking prior to the delayed entry program demonstrated significant predictive relationships among three types of in-unit attrition: (1) overall, (2) moral character, and (3) pregnancy or parenthood. They put this finding in perspective, comparing it with the predictive strength of education (McCloy and Putka, 2004:355):
For the Army FY 1999 cohort in-unit sample from the First Term Project, the rates are 34.2 percent and 21.5 percent (Overall attrition) and 21.9 percent and 10.2 percent (Moral Character) [for smokers and nonsmokers], respectively. [T]he odds ratios for this item rival those of Education Tier for Overall in-unit attrition (ranges of 1.33-1.86 for [pre-DEP smoking]; ranges of 1.38-1.99 for Education Tier).
The Navy study made use of a biographical questionnaire, the Assessment for Security Positions and Enlistment (ASPEN), which included a wide range of questions to gather behavioral information on recruits. In an effort to better understand the relationship between preservice smoking and first-term attrition, Flyer and Eitelberg (2005) cross-tabulated the smoking variable with responses to other questions on ASPEN that could be associated with a behavioral problem. Among the types of behavioral
problems associated with smoking were high school misbehavior, criminal offenses, drug use, psychological difficulties, and trouble dealing with authority. For example, 27 percent of nonsmokers admitted to having been suspended from high school at least once; this compares with 42 percent of light smokers and 50 percent of those who smoked heavily. At the same time, 20 percent of nonsmokers indicated that they had “been in trouble with police for nontraffic offenses”; by comparison, 34 percent of light smokers and 43 percent of heavy smokers indicated that they had likewise been in trouble with police. Furthermore, 32 percent of nonsmokers admitted to “causing problems in high school,” compared with 51 percent of light smokers and almost double the proportion (60 percent) of heavy smokers; and while 39 percent of nonsmokers admitted to “cutting class” often or occasionally in high school, the comparable proportions were 57 percent for light smokers and 64 percent for heavy smokers. These authors also found that first-term attrition rates are considerably higher for recruits who experienced certain preservice behavioral problems—such as suspension from high school, trouble with police, cutting class, or causing other disruptions in high school—than for those who have relatively clean preservice records. In addition, recruits who were suspended from high school have a first-term attrition rate ranging from 53 percent (three or more suspensions) to 41 percent (one or two suspensions), compared with 33 percent of recruits without any history of high school suspension.
The findings linking behavioral problems to smoking are supported by the earlier work of Tyas and Pederson (1998; see also Maney et al., 2004), who reviewed over 220 studies to synthesize and integrate information on the psychosocial correlates of adolescent smoking. Some of the more interesting trends—at least in helping to understand military attrition—fall under the behavioral category, which is further divided by factors related to school, risk-taking and deviance, and lifestyle. For example, under the category of school, smoking behavior was found in studies to be consistently related to educational aspirations and commitment. At the same time, under the categories of risk-taking and deviance, the following were associated with smoking initiation: having a history of trouble with the police, carrying a weapon, alcohol and other drug use, riding with a drinking driver, physical altercation, not wearing a seatbelt, and so on. Also found to be related to smoking was not following a healthy lifestyle.
As Flyer and Eitelberg (2005) observe, a substantial body of research continues to show that adolescent smokers are more likely than their nonsmoking counterparts to engage in risk-taking and deviant behavior. In addition, smoking has been linked with a greater likelihood of depression, as well as certain other psychiatric problems in teenagers, although the relationships are still largely unexplained. Studies of the psychosocial
correlates of smoking may offer important clues and insight as to why preservice smokers, regardless of education or other demographic factors, have a consistently higher rate of first-term attrition from the military.
The following sections discuss two ways in which smoking behaviors could be used in the screening process. The first is based on the cost-performance trade-off model as described in Chapter 3. This method can suggest whether screening daily or heavy smokers would be cost-effective considering the trade-off between the savings from reduced attrition and the increased recruiting costs. It is crucial to note that this discussion represents the hypothetical situation in which information about an individual’s smoking status is known. In an operational setting, reliance on self-reports of smoking is probably not feasible. Awareness that smoking at some level is disqualifying would in all likelihood result in underreporting, if not complete denial, of smoking. However, it is useful to determine whether or not it would be cost-effective to screen out some (e.g., heavy) smokers were it possible to identify them accurately.
The second approach is a less formal analysis of the relationship between smoking and a variety of other behavioral factors, especially those that are already used in screening, such as education. This approach is based on the likelihood that smoking can serve as a marker for a set of behaviors linked to attrition that are more feasibly assessed during the screening process. The identification of factors accounting for the smoking-attrition link may lead to mechanisms for screening these factors directly.
Cost-Performance Trade-off Analysis
The cost-performance trade-off model tries to answer the question of whether the savings in lower attrition costs will more than compensate for the higher recruiting costs if heavy or daily smokers are disqualified for enlistment. We try to answer this using the Army and Navy smoking attrition and prevalence data shown in Table 7-4. We reiterate that this analysis represents an exercise to determine the consequences of screening out some categories of smokers should it be possible to identify smoking status at point of entry. The committee recognizes that smoking status relies on self-report, and that accurate self-reports cannot be expected in an environment in which recruits know that certain levels of smoking are disqualifying.
The Navy Example
In Figure 7-6, we consider the costs and benefits of reducing the proportion of heavy smokers among recruits by 25, 50, and 100 percent.
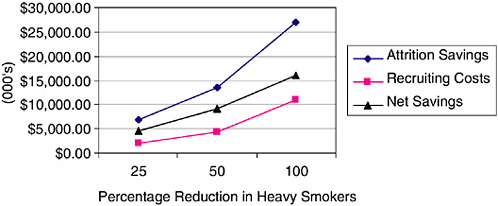
FIGURE 7-6 Benefits and costs from reducing heavy smoker percentage of recruits.
Attrition savings are greater than the increase in recruiting costs at all enlistment standards considered. Net benefits are maximized by excluding all heavy smokers. According to this analysis, almost $5 million could be saved if all heavy smokers were disqualified for service in the Navy.5 By screening out heavy smokers, the expected first-year aggregate attrition rate for Navy recruits would decline from 19.7 to 18.1 percent, a decline of 1.6 percent.
We now consider whether costs are further reduced if an enlistment standard restricting light smokers is imposed. We assume, in this analysis, that heavy smokers have already been made ineligible for enlistment. We also assume that the number of nonsmoking and light-smoking recruits increased proportionately to compensate for the loss of the heavy smokers. Hence, nonsmokers account for about 59 percent of recruits and light smokers constitute 41 percent.
The difference in first-year attrition rates between nonsmokers and light smokers is about 6.3 percent, much more modest than the difference in first-year attrition between heavy smokers and nonsmokers of about 17.6 percent. Moreover, light smokers constitute about 41 percent of recruits.6 However, because light smokers are a large proportion of re-
cruits, disqualifying them would have a significant effect on aggregate attrition, reducing first-year attrition from 21.4 to about 18.9 percent.
The analysis suggests that an enlistment standard for light smokers, however, would not be cost-effective. The net benefits are negative, and significantly negative, under any standard that limits the proportion of light smokers in the Navy solely on the basis of their smoking behavior.
The Army and Air Force Examples
We now conduct the same type of trade-off analyses for the Army. In the case of the Army, recruits were classified as “nonsmokers,” “less than daily smokers,” and “daily smokers.” The recruit population shares and the 12-month attrition rates are shown in Table 7-4. Immediately, we observe that the attrition rate differences between smokers and nonsmokers are much less dramatic in the Army compared with the Navy. Because the differences in the attrition rate between nonsmokers and less than daily smokers are insignificant, we combine them into a single category for the purposes of analysis. This new category “nonsmokers or infrequent smokers” constitutes 68.4 percent of the recruit population and has an attrition rate of 14.3 percent.
If daily smokers in the Army were ineligible to enlist, the savings in reduced attrition costs would be about $38,400,000. However, the additional recruiting costs resulting from eliminating 32 percent of the market more than offset the savings from lower attrition. The loss that would accrue from such a policy would be about $21,000,000 per year. Policies that would restrict, but not eliminate, daily smokers would also increase costs.
Although a formal analysis was not carried out for the Air Force, the similarity with the Army attrition rates suggests that screening out smokers as identified by the Air Force study would not be cost-effective.
Using Behavioral Factors to Screen Recruits
Flyer and Eitelberg (2005) found that the behavioral issues that may help to explain the relationship between preservice smoking and first-term attrition are similar in many ways to those underlying the relationship between dropping out of high school and early release from the military. Moreover, there is an interaction between education and level of smoking such that certain levels of smoking can magnify the effects of education on attrition.
This point is illustrated in Table 7-5, which presents 12-month attrition rates by education category. The table shows that recruits with Gen-
TABLE 7-5 Navy 12-Month Attrition Rates by Smoking Status and Education
|
Education |
Smoking Status |
% Attrition |
Number in Sample |
|
HSDG |
Nonsmoker |
17 |
3,482 |
|
HSDG |
Light |
22 |
2,007 |
|
GED or NG |
Nonsmoker |
24 |
347 |
|
ALT |
Nonsmoker |
26 |
464 |
|
ALT |
Light |
32 |
446 |
|
HSDG |
Heavy |
33 |
912 |
|
GED or NG |
Light |
33 |
489 |
|
ALT |
Heavy |
40 |
248 |
|
GED or NG |
Heavy |
44 |
338 |
|
Total sample |
|
24 |
8,733 |
|
HSDG = high school diploma graduate; ALT = alternate credential, such as home schooling, adult education, etc.; GED or NG = General Educational Development or not a high school graduate. |
|||
eral Educational Development (GED) certificates or alternate credentials who were nonsmokers had attrition rates somewhat lower than high school graduates who smoked (24 to 26 versus 33 percent). In addition, and perhaps more important, those recruits with GEDs or alternate certificates who were heavy smokers had very high attrition rates (40 to 44 percent), even higher than heavy smokers who were high school graduates.
Given the fact that smoking behavior can magnify the relationship between education and attrition, the question becomes how this information can be used to the military’s advantage in screening applicants for enlistment. Several options are worth considering, all without seeking to eliminate all smokers or reduce the pool of prospective recruits. First, assuming that there are unobtrusive ways of determining nonsmoking status, military recruiters could target nonsmoking graduates with high school diplomas because they have the lowest level of attrition among all groups. Second, given that an appreciable number of applicants with GEDs and alternative certificates will be accepted, the Services could target or give priority to the nonsmokers in this group, who have attrition rates only a few points higher than graduates with high school diplomas. Third, if it became feasible to assess quantity of smoking for applicants with GEDs and alternate certificates, then those who were heavy smokers
might be candidates for screening out because of their extremely high rates of early attrition.
Information on preservice smoking behavior is gathered during health screening. Since preservice smoking behavior is an attrition concern as will as a health concern, DoD might consider asking applicants about their smoking behavior during other phases of the application or enlistment process. Applicants who indicate that they smoke, or who are identified as possible smokers during screening or examination, might then be asked to complete a biodata questionnaire to determine if they fit in a high-risk category for first-term attrition. At this point, continued evaluation might be warranted to determine suitability for military service.
CONCLUSIONS AND RECOMMENDATIONS
While cigarette smoking is not permitted during basic and advanced training, smoking is commonplace during the first term, especially among men. However, smoking in the military is no more commonplace than in civilian populations of comparable ages. With respect to military performance, there is evidence that smoking before entry is associated with injury during basic training, probably arising from its adverse effects on numerous physiological characteristics. In addition, studies across all three Services show elevated attrition rates for smokers, although the degree of elevation differs appreciably among the Services, perhaps due to different definitions of the frequency and quantity of smoking. It is clear that screening out all smokers or even frequent smokers would not be feasible simply because of their prevalence. Since smoking is correlated with other recruit characteristics related to lower performance outcomes, further research might identify subgroups of recruits with a set of behavioral characteristics that justify higher priority on entry than other subgroups.
Recommendation 7-2: Further research is needed on the relationship between preservice smoking and military performance, including attrition and other indicators. The research should be conducted across the Services using the same definitions of frequency and quantity of smoking, and the correlates of smoking with other recruit characteristics should be studied. Studies should include the costs and benefits of policy and force management options for dealing with the issue of preservice smoking.

























