
5
The Background of Smoking Bans
This chapter provides background information on smoking bans, including a brief discussion of the history of tobacco policies that led to bans and the current status of bans in the United States and globally. More comprehensive reviews of the history of smoking bans and the scientific evidence and societal forces for and against them can be found in The Health Consequences of Involuntary Exposure to Tobacco Smoke: A Report of the Surgeon General (HHS, 2006) and the Institute of Medicine (IOM) report Ending the Tobacco Problem: A Blueprint for the Nation (IOM, 2007). The committee here discusses some of the issues around smoking bans that are relevant to the evaluation and interpretation of the literature on the effect of bans on the incidence of acute coronary events. Specifically, it discusses different types of smoking bans; the enforcement of bans; activities which often accompany bans, such as educational and outreach programs; and the effect of bans on individual behaviors, such as smoking.
HISTORY OF U.S. SMOKING POLICIES
The first surgeon general’s report on the adverse health effects of smoking was published in 1964 (HHS, 1964). Within a year of that report, the first law requiring the labeling of cigarette packages with health warnings was passed (the Cigarette Labeling and Advertising Act of 1965); it was followed a few years later by bans on cigarette advertising on television and radio (the 1969 Public Health Cigarette Smoking Act). By 1972, another report of the surgeon general, The Health Consequences of Smoking, discussed the potential adverse effects of secondhand-tobacco smoke
in people with preexisting disease (HHS, 1972). Table 5-1 lists some of the scientific reports and the clean-air policies implemented in the United States since the 1972 report; these milestones are detailed further in the surgeon general’s 2006 report (HHS, 2006). Restrictions on smoking in public places, government buildings, and airplanes were implemented in the 1970s, most of which limited but did not ban smoking. In 1973, Arizona became the first state to have some smoke-free public places, and the Civil Aeronautics Board requested no-smoking sections on all commercial airline flights (Koop, 1986). In the 1980s, several reports—The Health Consequences of Involuntary Smoking: A Report of the Surgeon General (HHS,
TABLE 5-1 Summary of Milestones in Decreasing Indoor Tobacco Smoke in the United Statesa
|
Year |
Event |
|
1971 |
The surgeon general proposes a federal smoking ban in public places. |
|
1972 |
The first report of the surgeon general to identify secondhand smoke as posing a health risk is released. |
|
1973 |
Arizona becomes the first state to restrict smoking in several public places. The Civil Aeronautics Board requires no-smoking sections on all commercial airline flights. |
|
1974 |
Connecticut passes the first state law to apply smoking restrictions in restaurants. |
|
1975 |
Minnesota passes a statewide law restricting smoking in public places. |
|
1977 |
Berkeley, California, becomes the first community to limit smoking in restaurants and other public places. |
|
1983 |
San Francisco passes a law to place private workplaces under smoking restrictions. |
|
1986 |
A report of the surgeon general focuses entirely on the health consequences of involuntary smoking, proclaiming secondhand smoke a cause of lung cancer in healthy nonsmokers. The National Research Council issues a report on the health consequences of involuntary smoking. Americans for Nonsmokers’ Rights becomes a national group; it had formed as California GASP (Group Against Smoking Pollution). |
|
1987 |
The U.S. Department of Health and Human Services establishes a smoke-free environment in all its buildings, affecting 120,000 employees nationwide. Minnesota passes a law requiring all hospitals in the state to prohibit smoking by 1990. A Gallup poll finds, for the first time, that a majority (55%) of U.S. adults favor a complete ban on smoking in all public places. |
|
1988 |
A congressionally mandated smoking ban takes effect on all domestic airline flights of 2 h or less. New York City’s ordinance for clean indoor air takes effect; the ordinance bans or severely limits smoking in various public places and affects 7 million people. California implements a statewide ban on smoking aboard all commercial intrastate airplanes, trains, and buses. |
|
Year |
Event |
|
1990 |
A congressionally mandated smoking ban takes effect on all domestic airline flights of 6 h or less. The U.S. Environmental Protection Agency (EPA) issues a draft risk assessment of secondhand smoke. |
|
1991 |
The National Institute for Occupational Safety and Health issues a bulletin recommending that secondhand smoke be reduced to the lowest feasible concentration in the workplace. |
|
1992 |
Hospitals applying to the Joint Commission on Accreditation of Healthcare Organizations for accreditation are required to develop a policy prohibiting smoking by patients, visitors, employees, volunteers, and medical staff. EPA releases its report classifying secondhand smoke as a group A carcinogen (known to be harmful to humans), placing secondhand smoke in the same category as asbestos, benzene, and radon. |
|
1993 |
Los Angeles passes a ban on smoking in all restaurants. The U.S. Postal Service eliminates smoking in all facilities. Congress enacts a smoke-free policy for Special Supplemental Food Program for Women, Infants, and Children (WIC) clinics. A working group of 16 state attorneys general releases recommendations for establishing smoke-free policies in fast-food restaurants. Vermont bans smoking in all public buildings and in many private buildings open to the public. |
|
1994 |
The U.S. Department of Defense prohibits smoking in all indoor military facilities. The Occupational Safety and Health Administration proposes a rule that would ban smoking in most U.S. workplaces. San Francisco passes a ban on smoking in all restaurants and workplaces. The Pro-Children Act requires persons who provide federally funded children’s services to prohibit smoking in their facilities. Utah enacts a law restricting smoking in most workplaces. |
|
1995 |
New York City passes a comprehensive ordinance effectively banning smoking in most workplaces. Maryland enacts a smoke-free policy for all workplaces except hotels, bars, some restaurants, and private clubs. California passes comprehensive legislation that prohibits smoking in most enclosed workplaces. Vermont’s smoking ban is extended to include restaurants, bars, hotels, and motels except establishments holding a cabaret license. |
|
1996 |
The U.S. Department of Transportation reports that about 80% of nonstop scheduled U.S. airline flights between the United States and foreign points will be smoke-free by June 1, 1996. |
|
1997 |
President Clinton signs an executive order establishing a smoke-free environment for federal employees and all members of the public visiting federally owned facilities. The California EPA issues a report determining that secondhand smoke is a toxic air contaminant. Settlement is reached in the class-action lawsuit brought by flight attendants exposed to secondhand smoke. |
|
1998 |
The U.S. Senate ends smoking in the Senate’s public spaces. California law takes effect banning smoking in bars that do not have a separately ventilated smoking area. The Minnesota tobacco-document depository is created as a result of a tobacco-industry settlement with Minnesota and BlueCross BlueShield of Minnesota. U.S. tobacco companies are required to maintain a public depository to house more than 32 million pages of previously secret internal tobacco-industry documents. |
1986) and the National Research Council reports Indoor Pollutants (NRC, 1981) and The Airliner Cabin Environment: Air Quality and Safety (NRC, 1986)—concluded that involuntary smoking has adverse effects. Increasing activity of nonsmokers’ rights organizations and shifts in public opinion led to implementation of more comprehensive bans, including bans on smoking on some domestic flights and in some government buildings (HHS, 2006). By 1986, 41 states and the District of Columbia had statutes that restricted smoking to some extent, but that were not as strong or extensive as most bans currently in place (Bayer and Colgrove, 2002; IOM, 2007). In 1992, the U.S. Environmental Protection Agency (EPA) released The Respiratory Health Effects of Passive Smoking: Lung Cancer and Other Disorders (EPA, 1992), which concluded that “environmental tobacco smoke (ETS) in the United States presents a serious and substantial public health impact.” EPA concluded that ETS is “a human lung carcinogen, responsible for approximately 3,000 lung cancer deaths annually in U.S. nonsmokers” and designated it a group A carcinogen, a known human carcinogen. EPA also cited other respiratory health effects in that report. As can be seen in Table 5-1, following the release of that report and with an increasing body of evidence demonstrating the adverse health effects of secondhand smoke, during the 1990s state and local governments across the country enacted an increasing number of more restrictive bans, including bans on smoking in most workplaces in some states. In the late 1990s and early 2000s, some states implemented comprehensive smoking bans that prohibited smoking in most workplaces and all public places, including previously exempted bars and restaurants (HHS, 2006). The first report about the association between cardiovascular risk and secondhand smoke appeared in 1985 (Garland et al., 1985).
According to the American Nonsmokers’ Rights Foundation’s U.S. Tobacco Control Laws Database©,1 as of January 4, 2009, “a total of 30 states, along with Puerto Rico and the District of Columbia, have laws in effect that require 100% smokefree workplaces and/or restaurants and/or bars.” It estimated that 70.2% of the U.S. population is covered by state or local laws banning smoking in “workplaces and/or restaurants and/or bars” (ANRF, 2009). Despite those increases in smoking bans, as recently as 1999–2004, the National Health and Nutrition Examination Survey (NHANES) estimated, on the basis of detectable serum cotinine, that 46.4% of U.S. nonsmokers ages 4 years and older were exposed to
secondhand smoke as people continue to be exposed in their homes and cars and in regions without smoking bans (CDC, 2008). That was a sharp decrease from the 1988–1994 NHANES data, in which the estimate was 84%, and supported an overall downward trend in secondhand-smoke exposure in the United States.
GLOBAL TOBACCO POLICIES
In addition to the United States, many countries (or portions of countries) around the world have implemented smoking restrictions and bans. They include Canada, Italy, and Scotland, where some of the key surveillance studies reviewed by this committee were conducted.
The growing global support for reducing tobacco use and secondhand-smoke exposure is evident from the World Health Organization Framework Convention on Tobacco Control (WHO, 2005). First proposed by the World Health Organization (WHO) in 1999, the treaty was adopted by the World Health Assembly in 2003. It commits ratifying nations to “protect present and future generations from the devastating health, social, environmental and economic consequences of tobacco consumption and exposure to tobacco smoke by providing a framework for tobacco control measures to be implemented by the Parties at the national, regional and international levels in order to reduce continually and substantially the prevalence of tobacco use and exposure to tobacco smoke” (WHO, 2005). Article 8 of the treaty commits parties “to protect all persons from exposure to tobacco smoke.” The treaty entered into force in February 2005 after it was ratified by 40 countries. As of July 30, 2009, 168 of the 192 WHO member states are signatories, and 166 WHO member states had ratified the treaty and become parties, covering 86.24% of the world population (WHO, 2009). The 2007 WHO report Protection from Exposure to Second-hand Tobacco Smoke (WHO, 2007) recommends that member states enact, implement, and enforce laws requiring workplaces and public places to be 100% smoke-free and pursue educational programs and activities to reduce secondhand-smoke exposure in homes.
The data in Figure 5-1, from the WHO Report on the Global Tobacco Epidemic, 2008—The MPOWER Package, however, show that “only 5% of the world’s population is covered by comprehensive smoke-free laws” as defined by WHO (2008), so much work remains. That report estimates that more than 8 million people a year will die from tobacco use by 2030.
ISSUES SURROUNDING SMOKING BANS
The regulations implemented with a smoking ban do not emerge from a vacuum, and the very activities that are often necessary for the enactment
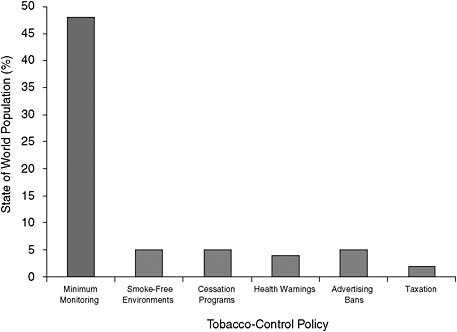
FIGURE 5-1 Share of the world population covered by tobacco-control policies.
SOURCE: Modified from WHO, 2008.
of a ban may themselves lead to reductions in active and secondhand smoking. As can be seen in Figure 5-2 (IARC, 2008), the health of nonsmokers after the implementation of a smoke-free policy can be affected not only by reduced secondhand-smoke exposure but also by concurrent changes (such as home smoking bans and decreases in smoking by people in other environments) attributable to increased awareness in the community, increased spontaneous cessation, and higher cessation success rates. The latter factors might have additional implications for the period over which followup is performed because their own timing might influence the effectiveness of a ban. Therefore, in evaluating and interpreting studies of the effects of smoking bans on health outcomes, the other concurrent activities must also be taken into consideration. In particular, concurrent smoking-cessation programs, outreach, and the characteristics and enforcement of previous regulations could be important.
Smoking-Cessation Programs and Outreach and Their Effect on Smoking Behavior
Published reports often lead to changes in smoking behavior and policy change. For example, as can be seen in Figure 5-3, the overall increase in
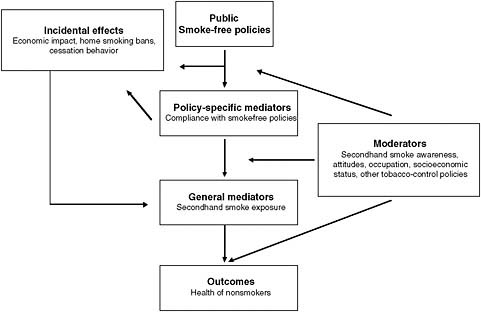
FIGURE 5-2 Factors contributing to the health of nonsmokers after implementation of a public smoke-free policy.
SOURCE: Modified from IARC, 2008.
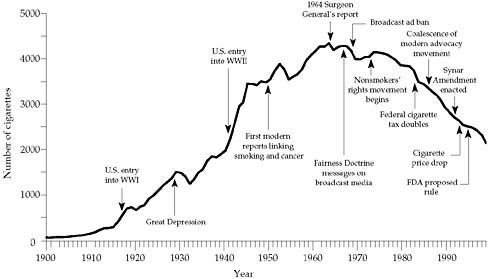
FIGURE 5-3 Adult per capita cigarette consumption and major smoking and health events, United States, 1900–1999.
NOTE: FDA, U.S. Food and Drug Administration.
SOURCE: HHS, 2000.
per capita cigarette consumption in the U.S. population ended after the publication of the surgeon general’s 1964 report on the health effects of smoking (HHS, 2000). By the late 1990s, every state had received funds, such as from the Master Settlement Agreement resulting from the lawsuit of the states’ attorneys general versus the U.S. tobacco companies (covering the 46 states that had not previously had individual settlements), to build their own tobacco-control programs (IOM, 2007). State and local efforts to implement smoking bans sometimes have a multiprong approach, accompanying smoking bans with media outreach, school-based programs, changes in tobacco pricing, or support for cessation programs.
A portion of the overall decline in smoking prevalence and intensity over the past 25 years can be attributed to general tobacco-control interventions (price increases and stronger antismoking culture). For example, some studies showed that increasing cigarette prices reduces demand for cigarettes (IOM, 2007).
The WHO Report on the Global Tobacco Epidemic, 2008—The MPOWER Package emphasized tobacco-control strategies that include taxation, advertising bans, smoke-free policies on smoke-free environments, and enforcement of existing bans (WHO, 2008). WHO estimated that a 70% increase in tobacco price could prevent up to about 25% of all tobacco-related deaths worldwide (WHO, 2008). Tobacco companies often have offered coupons to offset the price increase, and the coupons circumvent the increase in price to the consumer (Chaloupka, 2002). Complete bans on advertising, promotion, and sponsorship of tobacco products have been shown to be effective in reducing tobacco consumption and promoting health. In addition to advertising bans, WHO recommends health warnings on tobacco packages, cessation programs, and treatment of tobacco dependence in all member states (WHO, 2008). According to WHO, resources for enforcement of smoke-free legislation and bans on advertising, promotion, and sponsorship of tobacco products require only small expenditures to yield major health benefits. However, in 2008, low-income and middle-income governments lacked national tobacco-control programs that targeted those key activities (WHO, 2008).
Even if there is not an active multiprong approach, the approval and implementation of a smoking ban at the local or state level usually involves much public debate, which itself increases public awareness of the health effects of smoking and secondhand smoke (IOM, 2007). Therefore, smoking behaviors often change before and beyond the restrictions put into place by legislation (for example, quitting or voluntary smoke-free workplace policies in anticipation of a ban, reduction in smoking in homes), and such changes would contribute to the magnitude of changes in health outcomes seen after the implementation of a smoking ban.
On an individual level, many smokers voluntarily refrain from smok-
ing in some situations, for example, in their homes or cars or around their children. Among the possible reasons for that are increased awareness of health risks, wanting to be favorable role models, a desire for an odor-free environment, a change in social acceptability of smoking, or a desire to hide tobacco use (IOM, 2009). If those practices are adopted before a ban rather than following it, the apparent effect of the ban will be attenuated from the full effect and it can be difficult to assess how the ban itself changed exposure to secondhand smoke and to predict when a decrease in exposure might be expected to affect disease rates.
Comprehensive programs and voluntary actions could lead to larger decreases in smoking prevalence and a subsequent decrease in adverse health effects. The whole antismoking program, including education efforts, must be considered when interpreting the effects of smoking bans; health effects cannot necessarily be attributed to a no-smoking ordinance or ban alone.
Thus, in interpreting the results of studies that looked at a possible relationship between smoking bans and acute coronary events, caution must be taken not to attribute a decrease in adverse events solely to a reduction in secondhand smoke or to attribute a decrease in secondhand smoke solely to bans; other factors rather, contribute to the decreases. One major change that could occur with the implementation of smoking bans is a decrease in smoking—both through an increase in the number of people who quit smoking and through a decrease in the number of cigarettes smoked by smokers. As Figure 5-3 shows, the fall in per capita use of smoking preceded the common use of bans, which themselves resulted in decreased cigarette use and therefore less secondhand smoke exposure (HHS, 2000).
Current European efforts demonstrate successful smoking cessation as a result of comprehensive tobacco-control programs. An assessment of cross-sectional data from national health surveys in 18 European countries found quitting ratios2 high (above 45%) in several countries, including Sweden, England, the Netherlands, Belgium, and France (Schaap et al., 2008). The study found a positive association between a national score on a tobacco-control scale and quitting ratios among all age–sex groups. Similarly, a prospective cohort survey in Ireland found steep declines in reported smoking in workplaces (48% reduction), restaurants (82%), and bars and pubs (93%) as a result of the implementation of comprehensive smoke-free workplace legislation in that country (Fong et al., 2006). The study reported that 46% of Irish smokers reported that they were more likely to quit smoking (although that is not the same as actually quitting) as a result of legislation enactment (Fong et al., 2006). In Australia, Wakefield and colleagues (2008) used monthly smoking-prevalence data from 1995
to 2006 to assess the effect of television antismoking campaigns and of smoke free–restaurant laws. The study found that when the population was exposed about four times per month to antismoking advertising campaigns, smoking prevalence decreased by 0.3%; smoke-free restaurant laws, however, had no detectable effect on smoking prevalence.
In the United States, Fichtenberg and Glantz (2002) evaluated 26 studies of the effects of smoke-free workplaces in 2002; they found weak but significant inverse associations between completely smoke-free workplaces and smoking prevalence (3.8% reduction in prevalence; 95% confidence interval [CI], 2.8–4.7%) and daily cigarette consumption in continuing smokers (3.1 fewer cigarettes; 95% CI, 2.4–3.8). Messer et al. (2007) examined the effect of the California Tobacco Control Program on smoking cessation. The retrospective study assessed smoking history of 57,918 non-Hispanic white ever-smokers using data from the 1992–2002 Tobacco Use Supplements of the Current Populations Survey, monthly surveys conducted by the U.S. Census Bureau (Messer et al., 2007). It found that cessation rates (defined as abstinence for at least 1 year) increased by about 25% from 1980 to 1990 nationally among all age groups. Cessation rates averaged 3.4% per year in the 1990s. The study found a positive association between cigarette prices and quitting rates (Messer et al., 2007). Albers et al. (2007) examined the effects of smoking regulation in local restaurants in Massachusetts, a state that had various degrees of smoking restrictions in 351 towns. Adult smokers who had previously attempted to quit were about 3 times (odds ratio, 3.12; 95% CI, 1.51–6.44) more likely to attempt to quit in the 2 years after implementation of a smoking ban if they lived in towns with strong smoking regulations than if they did not, but no difference in smoking cessation was seen. The IOM report Ending the Tobacco Problem: A Blueprint for the Nation (IOM, 2007) concluded that comprehensive state tobacco programs can lead to substantial reductions in tobacco use. Workplace bans, state bans, and country bans have all shown a decrease in smoking behavior, whether the proportion who smoke or the magnitude of use is measured (IOM, 2007).
Previous Regulations and Characteristics and Enforcement of Smoking Bans
Other factors that could affect the results of studies of smoking bans and acute coronary events are the extent of smoking restrictions in place before the bans, the characteristics of the smoking bans themselves, and how well the bans are enforced.
As is evident in Table 5-1, smoking bans have been implemented at the city, county, and state level at various times in the United States. When the effect of a smoking ban on an adverse health effect is studied, the extent of
reduction in the adverse effect depends in part on the extent of a restriction or partial ban that existed before the ban under study. For example, some locations had previously implemented partial bans, and some regions within the locations studied (for example, New York City and several other large counties in the New York state study) had previously implemented comprehensive bans (Juster et al., 2007). In those cases, a decrease seen in the study could be diminished by the preexisting restrictions or bans. Similarly, in studies that have comparison populations, partial restrictions in the control locations could affect the magnitude of differences seen.
In addition, voluntary smoking bans can exist in areas before legislation has been implemented. For example, many hotel chains, some restaurant chains, airlines and other mass transit systems, office buildings, health-care facilities, schools, and individually owned establishments instituted bans long before counties, cities, or states legislated bans. Categorizing a county as not having a smoking ban may fail to reflect the fact that the average smoker could spend a substantial amount of time in an occupational setting that prohibits smoking in and outside a building, could eat dinner in a restaurant that prohibits smoking, and could shop in stores that prohibit smoking. This is increasingly the case. In 1993, 46.5% of employees in the United States were covered by smoking restrictions; by 1998–1999, 69.3% were covered by smoking restrictions (Shopland et al., 2004). Such prohibitions have increased, so it is more difficult to attribute even temporal changes in tobacco use or exposure in a defined geographic area to the lack or presence of a smoking ordinance. That could contribute to an underestimate of the actual effect had there been no prior ban. In contrast, many bans have allowed smoking outside public buildings or more than some stated distance from entrances. Although it is possible that outside smoking could attenuate the benefits of a smoking ban, the concentrations of secondhand smoke in those areas, and the safety or hazardousness of such areas in human populations has yet to be evaluated.
If smoking bans decrease acute coronary events, the inclusiveness of a ban (for example, the types of buildings and establishments included and the number of exemptions allowed) would be expected to affect the magnitude of the decrease. Different bans can cover or exempt different types of establishments or locations (such as restaurants with bars, bowling alleys, bingo halls, and outdoor seating areas). In interpreting studies of smoking bans, especially in comparing results of different studies, it is important to consider the types and extent of different bans. In addition, if a ban is not complied with or enforced, changes in health effects would not be expected. For example, the Clean Indoor Air Act was enacted in 1985 by the Florida legislature, but enforcement usually depended on filing of complaints with the Department of Health (American Lung Association, 2009).
CONCLUSIONS
The issues raised in this chapter are relevant to the interpretation of the major studies that are the subject of this report. Recommendations for future studies are in Chapter 6.
-
All the epidemiologic studies being reviewed should be evaluated in light of the amount of contextual data that are taken into account, including measurements both before and after bans and measurements comparing locales with and without bans.
-
When study results are compared, it may be impossible to separate contextual factors associated with a ban—such as public comment periods, information announcing the ban, and notices about the impending changes—from the effect of the ban itself.
-
The time from onset of a ban and concurrent activities to manifestation of disease can vary with the timing (and nature) of enforcement, and latency periods for cardiovascular incidents in people with different magnitudes of risk. Those factors, therefore, need to be considered in examining epidemiologic evidence.
REFERENCES
Albers, A. B., M. Siegel, D. M. Cheng, L. Biener, and N. A. Rigotti. 2007. Effect of smoking regulations in local restaurants on smokers’ anti-smoking attitudes and quitting behaviours. Tobacco Control 16(2):101-106.
American Lung Association. 2009. SLATI state information: Florida. (Accessed April 1, 2009, from http://slati.lungusa.org/state-teml.asp?id=9.)
ANRF (American Nonsmokers’ Rights Foundation). 2009. Overview list—how many smoke-free laws? (Accessed March 1, 2009, from http://www.no-smoke.org/goingsmokefree.php?id=519.)
Bayer, R., and J. Colgrove. 2002. Science, politics, and ideology in the campaign against environmental tobacco smoke. American Journal of Public Health 92(6):949-954.
CDC (Centers for Disease Control and Prevention). 2008. Disparities in secondhand smoke exposure—United States, 1988–1994 and 1999–2004 MMWR—Morbidity & Mortality Weekly Report 57(27):744-747.
Chaloupka, F., K. M. Cummings, C. P. Morley, and J. K. Horan. 2002. Tax, price and cigarette smoking: Evidence from the tobacco documents and implications for tobacco company marketing strategies. Tobacco Control 11(90001):i62-i72.
EPA (Environmental Protection Agency). 1992. Respiratory health effects of passive smoking: Lung cancer and other disorders. Washington, DC: Environmental Protection Agency.
Fichtenberg, C. M., and S. A. Glantz. 2002. Effect of smoke-free workplaces on smoking behaviour: Systematic review. BMJ 325(7357):188.
Fong, G. T., A. Hyland, R. Borland, D. Hammond, G. Hastings, A. McNeill, S. Anderson, K. M. Cummings, S. Allwright, M. Mulcahy, F. Howell, L. Clancy, M. E. Thompson, G. Connolly, and P. Driezen. 2006. Reductions in tobacco smoke pollution and increases in support for smoke-free public places following the implementation of comprehensive smoke-free workplace legislation in the Republic of Ireland: Findings from the ITC Ireland/UK survey. Tobacco Control 15 Suppl 3:iii51-iii58.
Garland, C., E. Barrett-Connor, L. Suarez, M. H. Criqui, and D. L. Wingard. 1985. Effects of passive smoking on ischemic heart disease mortality of nonsmokers. A prospective study. American Journal of Epidemiology 121(5):645-650.
HHS (U.S. Department of Health and Human Services). 1964. Smoking and health: Report of the advisory committee of the surgeon general of the public health service. Washington, DC: U.S. Department of Health, Education, and Welfare.
———. 1972. The health consequences of smoking. Atlanta, GA: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health.
———. 1986. The health consequences of involuntary smoking: A report of the surgeon general. Atlanta, GA: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health.
———. 2000. Reducing tobacco use: A report of the surgeon general. Atlanta, GA: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health.
———. 2006. The health consequences of involuntary exposure to tobacco smoke: A report of the surgeon general. Atlanta, GA: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Coordinating Center for Health Promotion, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health.
IARC (International Agency for Research on Cancer). 2008. Methods for evaluating tobacco control policies. Vol. 12, IARC handbooks of cancer prevention in tobacco control. Lyon, France: WHO.
IOM (Institute of Medicine). 2007. Ending the tobacco problem: A blueprint for the nation. Washington, DC: The National Academies Press.
———. 2009. Combating tobacco in military and veteran populations. Washington, DC: The National Academies Press.
Juster, H. R., B. R. Loomis, T. M. Hinman, M. C. Farrelly, A. Hyland, U. E. Bauer, and G. S. Birkhead. 2007. Declines in hospital admissions for acute myocardial infarction in New York state after implementation of a comprehensive smoking ban. American Journal of Public Health 97(11):2035-2039.
Koop, E. C. 1986. A society free of smoking by the year 2000? World Health Forum 7:225-231.
Messer, K., J. P. Pierce, S. H. Zhu, A. M. Hartman, W. K. Al-Delaimy, D. R. Trinidad, and E. A. Gilpin. 2007. The california tobacco control program’s effect on adult smokers: (1) smoking cessation. Tobacco Control 16(2):85-90.
NRC (National Research Council). 1981. Indoor air pollutants. Washington, DC: National Academy Press.
———. 1986. The airliner cabin environment: Air quality and safety. Washington, DC: National Academy Press.
Schaap, M. M., A. E. Kunst, M. Leinsalu, E. Regidor, O. Ekholm, D. Dzurova, U. Helmert, J. Klumbiene, P. Santana, and J. P. Mackenbach. 2008. Effect of nationwide tobacco control policies on smoking cessation in high and low educated groups in 18 European countries. Tobacco Control 17(4):248-255.
Shopland, D. R., C. M. Anderson, D. M. Burns, and K. K. Gerlach. 2004. Disparities in smoke-free workplace policies among food service workers. Journal of Occupational & Environmental Medicine 46:347-356.
Wakefield, M. A., S. Durkin, M. J. Spittal, M. Siahpush, M. Scollo, J. A. Simpson, S. Chapman, V. White, and D. Hill. 2008. Impact of tobacco control policies and mass media campaigns on monthly adult smoking prevalence. American Journal of Public Health 98(8):1443-1450.
WHO (World Health Organization). 2005. WHO framework convention on tobacco control.
———. 2007. Protection from exposure to second-hand tobacco smoke: Policy recommendations. Geneva: World Health Organization.
———. 2008. WHO report on the global tobacco epidemic, 2008: The MPOWER package. Geneva: World Health Organization.
———. 2009. Parties to the WHO framework convention on tobacco control. (Accessed March 31, 2009, from http://www.who.int/fctc/signatories_parties/en/index.html.) Geneva: World Health Organization.
















