
6
The Role of Social Networks and Social Integration
Over the past 50 years, social epidemiologists have tracked the impacts of social ties on health. Early studies focused on widowhood. By the late 1970s, several investigators had begun to examine the influence of social networks, social support, and aspects of community engagement on a number of health outcomes. After following nearly 7,000 adults in Alameda County, California, over a 9-year period, Berkman and Syme (1979) found that people with fewer social and community ties were significantly more likely to have died. The mortality rate for the men with the fewest ties was 2.3 times that for the men with the most ties, while the mortality rate for the women with the fewest ties was 2.8 times that for the women with the most ties. The effect of social ties on mortality was independent of such factors as the health of the survey participant at the beginning of the study; socioeconomic status; and smoking, drinking, obesity, and level of physical activity.
In the 30 years since the publication of that paper, researchers have studied the effects of social networks on health and mortality from a variety of angles and often with an increasingly rich set of covariates or potential confounders (Holt-Lunstad et al., 2010; House et al., 1982). They have found that various aspects of social ties—including structural characteristics of social networks, such as the size of one’s network of friends and family members, and the resources that flow through networks, such as the support one receives from the network—influence health in a number of ways. Recent, more formal analysis of social networks (Christakis and Fowler, 2007) suggests that they transmit a number of both health-promoting and risk-related behaviors capable of mediating many of the relationships
between social network structure and health outcomes. Thus, aspects of social networks ranging from structure to function are related to mortality, morbidity, cognitive and physical function, and a range of health behaviors.
As with other factors considered in this volume, while associations between social ties and mortality and health may be strong, it is often difficult to be sure of the causal direction. People who are social isolates may differ from those who are highly socially integrated in many ways. Some of these differences may also be related to their health. In some cases, poor health can be linked to social withdrawal.
The question addressed in this chapter is whether international differences in the distribution of social networks and social support, and the risks related to them, might play a role in the divergence in life expectancy among countries. To answer this question, this chapter first takes a closer look at the pathways by which social networks can affect health and mortality and the evidence for these linkages. It then examines how social networks in the United States compare with those in other countries and considers the evidence that those differences play a role in the divergence in life expectancy trends.
PATHWAYS LINKING SOCIAL NETWORKS TO HEALTH AND MORTALITY
There are a number of mediating pathways by which aspects of social networks might plausibly impact health. Most obviously, the structure of network ties influences health via the provision of many kinds of support, from financial to instrumental and emotional (Berkman and Glass, 2000). Support is often transactional in nature, potentially involving giving as well as receiving, and occurs within a normative framework of exchange over the life course that may vary across countries and cultures. Some exchanges improve access to resources and material goods. For instance, social networks have been shown to be associated with an individual’s likelihood of getting a job (Granovetter, 2003). Other types of support, such as emotional support, may impact health by reducing physiological stress responses. Social networks can also impact health through social influence whereby individuals obtain normative guidance about behaviors. Finally, negative interactions leading to conflict, abuse, or neglect can have powerful impacts on subsequent health outcomes via a number of behavioral and biological pathways.
Linking the kinds of social interactions described above to health outcomes logically requires a set of pathways by which the effects of social interaction affect health. These can be pathways that link social interaction to behaviors, psychological states, or more directly to physiological responses tied to health. Previous research has linked aspects of social
networks and the resources that flow through them to behaviors related to tobacco and alcohol consumption, physical activity, dietary patterns, and sexual behaviors. By establishing and enforcing normative behaviors, networks may influence work- and school-related behaviors, criminal behaviors, and other social behaviors. Networks may also influence patterns of self-esteem, efficacy, competence, and other conditions leading to mental health outcomes. Finally, increasing evidence suggests that social networks and related functions impact physiological processes directly by several pathways. Invoked most frequently is a stress pathway linked to neuroendocrine regulation, inflammation, and immune function (Gruenewald et al., 2009; Loucks et al., 2006a, 2006b; Uchino, 2006). Berkman (1988) hypothesizes that social isolation or the negative aspects of social ties influence health by accelerating the rate of aging. Social isolation, conflict, or lack of support may be viewed as a chronically stressful condition to which the organism responds by aging more rapidly. This acceleration would be especially evident in cardiometabolic functions that decline with age.
Social Networks and Mortality
Numerous studies from many industrialized countries in North America, Europe, and Asia have shown that aspects of social networks or social support are related to mortality, including mortality from all causes combined (Berkman et al., 2004; Blazer, 1982; Eng et al., 2002; Fuhrer and Stansfeld, 2002; Kaplan et al., 1988; Khang and Kim, 2005; Orth-Gomer and Johnson, 1987; Orth-Gomer et al., 1993, 1998; Penninx et al., 1998; Pinquart and Duberstein, 2010; Pinquart and Frohlich, 2009; Seeman, 1996; Sugisawa et al., 1994). Although all of these studies are longitudinal in the sense of including a mortality follow-up after baseline assessment of social networks, they vary widely in their ability to control for important covariates or to disentangle the extent to which such covariates are mediators along the pathway from social networks to increased mortality risk. Furthermore, networks themselves develop in the context of individual exposures over a life course, some of which may be related to health.
Focusing on some of the more salient aspects of the above-mentioned mortality studies helps identify areas for further work. For instance, it appears that different aspects of social networks may be more important at different ages, or for men or women, or in different countries. In a followup to the original Alameda study (Berkman and Syme, 1979), Seeman and colleagues (1987) report that over a 17-year period, the subjects with stronger social networks and community ties were significantly less likely to die. The types of social ties with the greatest effect on mortality differed by age. For adults 60 and younger, marital status had the greatest association with the risk of dying, while for those over 60, the most meaningful
relationships for health were those with close friends and relatives. A large-scale prospective study conducted in Japan with more than 11,000 subjects aged 40–69 found important gender differences: for men the key factor related to health was participation in hobbies, clubs, or community groups, while for women the factors that increased risk were being single and having little contact with close relatives (Iwasaki et al., 2002). A 7-year study in Israel found that the two social factors influencing mortality among a group of older Jewish–Israelis were contact with friends and attendance at synagogue (Litwin, 2007). And a 6-year study of 7,500 women from four different communities in the United States found mortality risks to be significantly lower among women with higher social network scores, although the authors conclude that much of the protection older women receive from a large social network is actually due simply to being married (Rutledge et al., 2003).
In a paper prepared for the panel, Banks and colleagues (2010) perform a similar analysis for both males and females using comparable data on the older population in the United States and England. Once again, marriage (including cohabitation) is the element of social networks and interactions found to be protective against mortality. This is strongly the case for both males and females in England, but in the United States the effects are not statistically significant. In England, where the data permit the cleanest analysis, any association of mortality with memberships in clubs and organizations is shown to be simply a consequence of the inclusion of membership in sports and health clubs in the participation measure, so the likelihood is strong that a reverse causal mechanism generated this relationship. In the United States, any overall effect of networks, contact, and participation is shown to be due to a significant protective effect for those who attended religious meetings regularly.
Berkman and colleagues (2004) examined an occupational cohort of employees who were stably employed to minimize the possibility that socially isolated subjects were more likely to also be economically disadvantaged or disabled. They found that socially isolated men had a mortality risk 2.7 times greater than that of the men with the highest level of social integration; the corresponding figure for women was 3.6 times greater (Berkman et al., 2004). The risks were greatest for cancer mortality, a finding at odds with some but not all of the data from the United States. Kawachi and colleagues (1996) examined mortality risks among 32,000 U.S. men aged 42–77 and found that socially isolated men were 1.9 times more likely to die from cardiovascular disease and 2.2 times more likely to die from accidents and suicide than men who had the highest level of involvement in social networks (Kawachi et al., 1996).
There is also evidence that social networks are linked to mortality from breast cancer. In a study of 2,800 women diagnosed with breast cancer
between 1992 and 2002, women who had been socially isolated before the diagnosis were more than twice as likely to die from the disease as women with a high level of social support. The researchers conclude that the increased mortality was likely an indirect effect of the lack of social connections and that the reason the socially isolated women had an increased mortality risk was that they did not receive as much aid, care, and support from friends, children, or family members (Kroenke et al., 2006).
The authors of a recent meta-analysis of 87 studies that examines the effects of social support on cancer mortality report that large social networks, positive social support, and being married all are correlated with decreased mortality from cancer. However, the authors conclude that the effects are generally larger for younger patients (Pinquart and Duberstein, 2010). Another recent meta-analysis concludes that the quality of social relationships has an effect on mortality that is comparable to that of quitting smoking and greater than that of other risk factors such as obesity and physical activity (Holt-Lunstad et al., 2010); however, many of the results underlying this study lack statistical controls for some of the factors that are correlated with both mortality and social relationships. Much work remains to be done to understand the links between social networks and mortality. Nonetheless, the preponderance of the evidence indicates that social ties and social support do affect mortality among adults.
Social Networks and Physical and Mental Health
In general, studies that have examined the effects of social networks on physical health have less consistently found evidence of a relationship than those looking at effects on mortality. Nevertheless, a number of studies show a link between social ties and social support and the development of such illnesses as heart disease, stroke, and cancer.
In the above-referenced study of 32,000 U.S. men aged 42–77, Kawachi and colleagues (1996) found that over 4 years, men who were socially isolated—not married, having fewer than six friends and family members, and not a member of any church or social organization—were 121 percent more likely to suffer a stroke than those men with the greatest degree of social connection. However, they were no more likely to suffer a nonfatal heart attack.
Broadly speaking, studies that have looked at the effects of social support on heart disease have had mixed results, but a majority—unlike the work of Kawachi and colleagues (1996)—have found at least some effect. When Lett and colleagues (2005) reviewed the body of research on this issue, they concluded that subjects with low levels of social support were more likely to develop coronary heart disease and to have it worsen than those with high levels of support, and the risk ratio between the two groups
appeared to lie between 1.5 and 2.0, depending on the study. The authors note, however, that there was little consistency across studies in the way social support was defined and measured and furthermore, that there was little experimental evidence that increasing social support helps reduce the risk of heart disease.
Banks and colleagues (2010) found no relationship between a summary social network index and the prevalence of high blood pressure or diabetes among older men in either the United States or England. In the United States, men with high levels of social ties had a greater prevalence of heart disease. Among women in both countries, high levels of social ties were related to fewer of these health problems, with the exception of obesity (which is linked to diabetes). The authors also found inconsistent effects of social interaction and social network measures on subsequent mortality in the two countries. Overall, then, the results of this study mirror the highly mixed nature of the existing empirical evidence linking social networks to physical health.
More consistent findings with regard to social networks and domains of health relate to mental functioning rather than morbidity or physical health. Study after study has shown that social networks and social participation delay various types of cognitive decline in older adults, while those older adults with few social ties deteriorate much more quickly. Bassuk and colleagues (1999) followed 2,800 adults aged 65 and older living in New Haven, Connecticut, and found that those with no social ties were significantly more likely to decline cognitively than those who had a large number of such ties. In particular, those with no social ties were 2.2 times as likely to have declined cognitively after 3 years, 1.9 times as likely after 6 years, and 2.4 times as likely after 12 years (Bassuk et al., 1999). A more recent study shows social integration to be inversely related to memory decline among Health and Retirement Study (HRS) participants (Ertel et al., 2008).
Similar results have been found in other countries. Fratiaglioni and colleagues (2000, 2004) report an association between limited social networks and increased risk of incident dementia. Zunzunegui and colleagues (2003) found social isolation to be related to cognitive decline in an older Spanish sample. One prospective study in Taiwan that followed nearly 2,400 older adults over 7 years found no relationship between social networks and cognitive functioning but did find a clear effect of social activities on tests of cognitive function. Subjects who reported participating in one or two social activities and in three or more such activities failed 13 and 33 percent fewer of the cognitive tasks, respectively, than those who reported participating in no social activities (Glei et al., 2005).
Given the evidence that various aspects of social ties and networks and the functions of such networks are consistently related to mortality and often to other health outcomes as well, a natural question is whether
differences in the distribution or risk of social networks might help explain cross-country differences in life expectancy.
INTERNATIONAL COMPARISONS OF SOCIAL NETWORKS AND EFFECTS ON HEALTH AND MORTALITY
Few if any studies directly address the question of whether social factors might explain some of the differences in life expectancy among various high-income countries. However, a great deal of research compares social networks among various countries, and some of that research also includes information on the connection between social networks and mortality in the countries under consideration. Ideally, one would wish to assess the variability in the distribution of social networks and support in many countries. Second, one would like to identify whether risks associated with social isolation and various health outcomes are the same within each country. For social networks and support to help explain cross-country differences in life expectancy, at least one of two conditions must be met. First, a different fraction of the population needs to be exposed to risk factors across countries. Alternatively, the health risk (“toxicity”) associated with risk factors might differ among countries. For common risk factors, even small differences in toxicity could have large population health effects. Differences in toxicity could occur if population differences in exacerbating or compensatory factors influenced the risk of disease. For instance, if countries had public policies protecting citizens against the deleterious health effects of extreme poverty, those health effects might not manifest themselves even though poverty was present.
The United States and England
Perhaps the most directly relevant study on these issues is the report prepared for the panel by Banks and colleagues (2010) comparing the effects of social networks and social integration in the United States and the United Kingdom. The investigators compared data from the HRS in the United States and the English Longitudinal Study of Ageing (ELSA) in the United Kingdom. Exploiting the relative comparability of the data items, they derived a social network index combining information on the presence of a spouse or partner; the frequency of meeting up with children, family, and friends; and membership in clubs or organizations. In addition, they were able to derive comparable measures of both negative and positive social support from children, close family members, and friends.
One key finding was the remarkable similarity in the distribution of social support and networks among older adults in the United States and England (see Figure 6-1). The differences that did appear were second order,
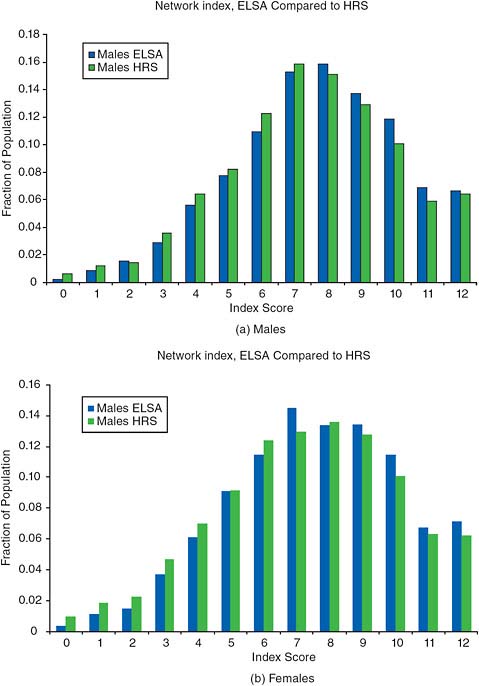
somewhat nuanced, and not all indicative of weaker networks or less support in the United States. As an example, American men and women receive more positive support from their children than do their British counterparts, but also more negative support (Banks et al., 2010), a finding similar to that reported in a recent international study (Silverstein et al., 2010).
Given the similarities in the levels and distribution of social support and networks in these two populations, rather large differences would have to exist in the health consequences of these social circumstances for this to be a candidate explanation for differences in morbidity between the two countries. But the authors also found very little consistent or compelling association between levels of social networks and the prevalence of a variety of physical health measures, and only a weak association between social networks and subsequent mortality; what effects were found were associated primarily with the presence of a spouse/partner. The authors conclude that differences in morbidity and mortality between these two countries cannot be explained by current differences in social ties, support, and networks. By extension, the same argument would hold true for life expectancy.
Other International Comparisons
Given the similarity of the distribution of social ties and networks between the United States and England, more powerful evidence might be expected to come from other international comparisons where variation in these social risk factors is greater. A small number of studies have compared social ties in the United States with those in other countries and looked at how differing social networks may affect health and mortality in those countries.
Japan is a particularly interesting country to compare with the United States, both because it has significantly higher life expectancy and because the countries have very different cultures. Janevic and colleagues (2000) examined the relationships between social ties and health in Japan and the United States, looking in particular for any differences between men and women. They found relatively few national differences, and those differences did not appear to play a major role in the relationship between social ties and health, leading the authors to conclude that this relationship may vary little from country to country. Their data did indicate that older people in the United States receive more emotional and instrumental support from their networks than do older Japanese, but Americans also have more negative social relationships. The authors note that it was the type and quality of support received, rather than the particular structure of the social networks, that had the largest effect on health.
Antonucci and colleagues (2001) compared the relationship between social networks and health in four countries: the United States, Japan,
France, and Germany. In particular, they were interested in what happens to the social networks of older adults when they become ill or widowed. One might expect that becoming ill or losing a spouse would change a person’s social network in various ways. The network might shrink, for example, as contact faded with friends and even family members. The data showed that network structure did indeed change in various ways in response to illness or losing a spouse, but only in three of the countries; the social networks of older adults in the United States remained stable in the face of such losses. The authors conclude that older adults in the United States may be somewhat more protected from the effects of illness and loss of a spouse because of the stability of their social networks in the face of such losses.
The potential power of a multicountry comparison is further evidenced by the final section of the Banks et al. (2010) paper. Using data from the 2006 and 2007 Gallup World Poll, the authors document differences in a variety of social integration and participation measures across nine of the countries considered in this study (see Table 6-1). Once again, the implications of their findings for explaining the life expectancy and health disadvantages of the United States are rather mixed. The United States has a relatively low rank with respect to marriage or living with a partner, although not as low as England, while Japan is the one country with notably higher levels of marriage among older persons. The indicator of number of hours spent in the last day with family and friends is not available for the United States, but the hours are longer in Japan than in other countries. On the other hand, on two other indicators of community integration—religious participation and volunteering—the United States ranks highest.
One can also examine international differences in some of the psychosocial outcomes that have been linked to social integration using the same Gallup data (see Table 6-2). In the Gallup poll, people report their levels of stress, worry, sadness, depression, and anger in the last day—all states that would potentially be buffered by strong social relationships. No one country stands out as reporting poorer psychosocial well-being, and differences in reports of these states vary markedly across countries. People in the United States reported the most stress, people in Japan the most depression, and people in France the most anger, while people in Denmark and the Netherlands reported relatively low levels of most of these states. The variation exhibited in these measures across countries suggests that a more sophisticated and in-depth multicountry analysis exploiting such data might yield useful evidence in the future.
Change Over Time in Social Networks
Finally, it is useful to look at differential trends in social integration across countries. Living alone is one indicator of social integration that can
TABLE 6-1 Social Network Measures by Country: Gallup World Poll, 2006–2007
|
Country |
Proportion Married or Living with Partner |
Proportion Attended Religious Services in Past Week |
Hours Spent with Friends and Family Yesterday |
Proportion Volunteered Time to an Organization in Past Month |
|
Males |
||||
|
United States |
0.58 |
0.46 |
N.A. |
0.43 |
|
Canada |
0.60 |
0.29 |
N.A. |
0.33 |
|
Denmark |
0.59 |
0.14 |
7.08 |
0.23 |
|
France |
0.61 |
0.14 |
6.86 |
0.29 |
|
Italy |
0.60 |
0.51 |
8.41 |
0.22 |
|
Japan |
0.66 |
0.21 |
7.55 |
0.26 |
|
Netherlands |
0.57 |
0.21 |
6.60 |
0.36 |
|
Spain |
0.57 |
0.23 |
7.46 |
0.13 |
|
United Kingdom |
0.54 |
0.20 |
7.16 |
0.21 |
|
Females |
||||
|
United States |
0.51 |
0.46 |
N.A. |
0.43 |
|
Canada |
0.63 |
0.33 |
N.A. |
0.42 |
|
Denmark |
0.64 |
0.21 |
7.26 |
0.25 |
|
France |
0.55 |
0.19 |
6.50 |
0.28 |
|
Italy |
0.62 |
0.59 |
8.66 |
0.21 |
|
Japan |
0.67 |
0.23 |
10.75 |
0.24 |
|
Netherlands |
0.59 |
0.26 |
8.33 |
0.38 |
|
Spain |
0.59 |
0.33 |
7.83 |
0.16 |
|
United Kingdom |
0.45 |
0.29 |
7.53 |
0.25 |
|
SOURCE: Adapted from Banks et al. (2010, Tables 8-7 and 8-8). Reproduced with permission. |
||||
be tracked across time for many countries. The likelihood of living alone among older people increased markedly in Europe and the United States after 1950 and particularly from 1970 to 1990, but this trend has stabilized or reversed in many countries since then. In 2000 older women in the United States were less likely to live alone than those in many Northern European countries (e.g., Great Britain, the Netherlands, Sweden, Germany, Austria) (Tomassini et al., 2004).
Whether one lives alone or with others in old age is determined by marriage rates, mortality rates, past fertility rates, income levels, and policies on providing both income and housing for older persons (Macunovich et al., 1995; Wolf, 1995). Decreases in the death of a spouse have generally increased the likelihood of living with a spouse, but in many countries these increases have been offset by increases in divorce rates. Because the Japanese have both lower mortality and lower divorce rates, they are most
TABLE 6-2 Psychosocial Measuresa and Availability of Social Supportb Among Those Aged 50+: Percentage Responding Yes to Questions, Gallup World Poll, 2006–2007
|
Country |
Stress |
Worry |
Sadness |
Depression |
Anger |
Support Available |
|
United States |
35 |
28 |
19 |
11 |
12 |
96 |
|
Italy |
31 |
44 |
29 |
13 |
17 |
86 |
|
Canada |
31 |
27 |
16 |
8 |
12 |
95 |
|
Australia |
30 |
26 |
20 |
11 |
10 |
93 |
|
United Kingdom |
27 |
28 |
29 |
14 |
10 |
97 |
|
Japan |
24 |
26 |
11 |
15 |
20 |
92 |
|
France |
23 |
32 |
25 |
6 |
31 |
89 |
|
Denmark |
14 |
22 |
15 |
6 |
11 |
94 |
|
Netherlands |
17 |
35 |
20 |
5 |
7 |
89 |
|
aQuestions asked: Did you experience stress during a lot of the day yesterday? Did you experience worry during a lot of the day yesterday? Did you experience sadness during a lot of the day yesterday? Did you experience depression during a lot of the day yesterday? Did you experience anger during a lot of the day yesterday? bQuestion asked: If you were in trouble, do you have relatives or friends you can count on to help you whenever you need them, or not? SOURCE: Data from Gallup World Poll Data. See http://www.gallup.com/video/106357/introducing-gallup-world-poll.aspx [accessed January 12, 2011]. |
||||||
likely among the populations of the countries studied here to be married in old age; clearly, however, cultural differences are the reason older people in Japan are less likely to live alone than those in any of the other countries (Palloni, 2002). The past high fertility of U.S. cohorts relative to those in the other countries adds to the likelihood that older Americans will live with a child and is one reason they have both a relatively low level of and recent reductions in solitary living. Thus, the available evidence does not support the hypothesis that social networks among the U.S. elderly weakened sharply in the 1980s and 1990s while remaining strong in other countries.
Discussion
Data do not currently exist with which to test detailed hypotheses relating to differences in the causal effects of social ties and networks across multiple countries, or even to document the distribution of such ties and networks on a detailed and fully comparable basis. Furthermore, almost no information is available concerning trends in social networks and their effects on health and mortality. Most of the data concern social networks
at one point in time, generally near the present. Nonetheless, at this point there appears to be little reason to believe that social networks played a role in the divergence in life expectancy trends among high-income nations from 1980 to 2005. As for explaining the current gap in life expectancy, the details of the networks may vary from country to country, but countries appear to differ relatively little in the overall level of support individuals receive from their social networks. Thus at present, the available data do not support the notion that social networks play an important role in international variations in longevity.













