
Health of the Elderly in India: Challenges of Access and Affordability
Subhojit Dey, Devaki Nambiar, J. K. Lakshmi, Kabir Sheikh, and K. Srinath Reddy
India, the world’s second most populous country, has experienced a dramatic demographic transition in the past 50 years, entailing almost a tripling of the population over the age of 60 years (i.e., the elderly) (Government of India, 2011). This pattern is poised to continue. It is projected that the proportion of Indians aged 60 and older will rise from 7.5% in 2010 to 11.1% in 2025 (United Nations Department of Economic and Social Affairs [UNDESA], 2008). This is a small percentage point increase, but a remarkable figure in absolute terms. According to UNDESA data on projected age structure of the population (2008), India had more than 91.6 million elderly in 2010 with an annual addition of 2.5 million elderly between 2005 and 2010. The number of elderly in India is projected to reach 158.7 million in 2025 (United Nations Department of Economic and Social Affairs, 2008), and is expected, by 2050, to surpass the population of children below 14 years (Raju, 2006).
Summary figures mask the unevenness and complexities of the demographic transition within India across Indian states with different levels of economic development, cultural norms, and political contexts. Projected estimates of population structure in 2025 for North India retain a “pyramidal” shape, while for south India, the share of the elderly population is expected to expand considerably. Linear growth in the population of the elderly is expected in the next 100 years, with steeper gradients of increase in central and east India and leveling off of absolute numbers of elderly in the north, south, west, and northeast (Aliyar and Rajan, 2008).
A few important characteristics of the elderly population in India are
noteworthy. Of the 7.5% of the population who are elderly, two-thirds live in villages and nearly half are of poor socioeconomic status (SES) (Lena et al., 2009). Half of the Indian elderly are dependents, often due to widowhood, divorce, or separation, and a majority of the elderly are women (70%) (Rajan, 2001). Of the minority (2.4%) of the elderly living alone, more are women (3.49%) than men (1.42%) (Rajan and Kumar, 2003). Thus, the majority of elderly reside in rural areas, belong to low SES, and are dependent upon their families.
While the southern states (Andhra Pradesh, Karnataka, Kerala, and Tamil Nadu) may be considered the biggest drivers of aging in India, other Indian states (notably Haryana, Himachal Pradesh, Maharashtra, Orissa, and Punjab) are also experiencing an elderly population boom, largely in rural areas (Alam and Karan, 2010). Large-scale studies of the health behaviors of this growing elderly Indian population are scarce. However, information gathered from numerous surveys and regional and local studies point to the high prevalence of several risky behaviors, such as tobacco and alcohol use (Goswami et al., 2005; Gupta et al., 2005; Mutharayappa and Bhat, 2008), and physical inactivity (Rastogi et al., 2004; Vaz and Bharathi, 2004). With these stressors, predictably, aggregate data comparing the 52nd (1995-1996) and 60th Rounds (2004) of the National Sample Survey (NSS) suggest a general increase in the reports of ailments and utilization of healthcare services among the elderly (Alam and Karan, 2010; Rao, 2006). Access to services, however, is uneven across the country.
An analysis of morbidity patterns by age clearly indicates that the elderly experience a greater burden of ailments (which the National Sample Survey Organisation defines as illness, sickness, injury, and poisoning) compared to other age groups (see National Sample Survey Organisation, 2006, Fig. 1), across genders and residential locations. The elderly most frequently suffer from cardiovascular illness, circulatory diseases, and cancers, while the non-elderly face a higher risk of mortality from infectious and parasitic diseases (Alam, 2000; Kosuke and Samir, 2004; Shrestha, 2000). In developed countries advancing through demographic transition, there have been emerging epidemics of chronic non-communicable diseases (NCDs), most of which are lifestyle-based diseases and disabilities (Gruenberg, 1977; Waite, 2004). In contrast, India’s accelerated demographic transition has not been accompanied by a corresponding epidemiological transition from communicable diseases to NCDs (Agarwal and Arokiasamy, 2010). As indicated in Figure 15-1, the Indian elderly are more likely to suffer from chronic than acute illness. There is a rise in NCDs, particularly cardiovascular, metabolic, and degenerative disorders, as well as communicable diseases (Ingle and Nath, 2008). While cardiovascular disease is the leading cause of death among the elderly
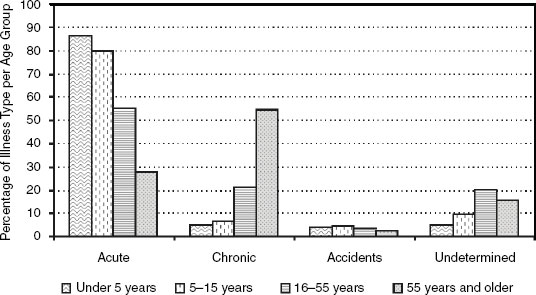
FIGURE 15-1 Burden of illness type among Indians.
SOURCE: Dror, Putten-Rademaker, and Koren (2008).
(Jha et al., 2006), multiple chronic diseases afflict them: chronic bronchitis, anemia, high blood pressure, chest pain, kidney problems, digestive disorders, vision problems, diabetes, rheumatism, and depression (Angra et al., 1997; Kumari, 2001; Raju, 2000; Roy, 1994; Shah and Prabhakar, 1997). Concurrently, the prevalence of morbidity among the elderly due to re-emerging infectious diseases is quite high, with considerable variations across genders, areas of residence, and socioeconomic status (Goldman, Korenman, and Weinstein, 1995; Gupta and Sankar, 2002; Kumar, 2003; Mini, 2008; National Sample Survey Organisation [NSSO], 1996; Radha et al., 1999; Rajan, Misra, and Sharma, 1999; Sudha et al., 2006). It is projected that NCD-related disability will increase and contribute to a higher proportion of overall national disability, in step with the greying of the population (Kowal et al., 2010). However, a very significant shortcoming of most of the above studies is the use of self-reported data, which, in the absence of autopsies and physician examinations of patients, represents enormous lacunae in data on the conditions affecting the elderly. More detailed studies are needed, other than surveys, to extract information on the epidemiology of health conditions experienced by the elderly.
This mixed disease burden among the Indian elderly places unique demands on the country’s public healthcare system. In developing our conceptual model of elderly health in India, we began with a perusal of the larger health scenario in India, finding that “health care, far from helping people rise out of poverty, has become an important cause of house-
hold impoverishment and debt, the average national health indicators, though showing improvements in recent decade, hide vast regional and social disparities.” Although some privileged individuals enjoy excellent health outcomes, others experience “the worst imaginable conditions” (Patel et al., 2011, p. 4). Among the elderly, we observed a number of barriers: from pathological progression (Lynch, Brown, and Taylor, 2009) to family nuclearization and dependency (Gupta and Sankar, 2002; Rajan and Prasad, 2008), from reductions in earning potential (Selvaraj, Karan, and Madheswaran, 2010) to the salience of pre-existing inequities on the axes of gender, caste, and religion (Chatterjee and Sheoran, 2007; Goel et al., 2003; Goldman, Korenman, and Weinstein, 1995; Gupta and Sankar, 2002; Kumar, 2003; Mini, 2008; National Sample Survey Organisation [NSSO], 1996; Radha et al., 1999; Rajan, Misra, and Sharma, 1999; Sudha et al., 2006). Across the board, we found that the elderly population (and subpopulations that form it) does not receive care commensurate to the conditions it suffers (access) and, second, that even where the care is physically accessible, costs of accessing this care hinder uptake (affordability).
The aim of this chapter, therefore, is to characterize and describe specific challenges in the domains of access and affordability, and the likely determinants of such challenges that must be addressed in the design and implementation of future health policymaking in India. Throughout, we aim to reveal areas where data gaps remain. A semi-structured literature review and secondary research methodology based upon Pope and colleagues (2000) was developed by the study authors with the collaborative assistance of two research assistants. All researchers undertook a literature review, drawing upon key informant experts in health systems research, government policy clearinghouses, and a review of scholarly journal articles, books, and program documentation comprising nongovernmental organization and government reports, presentations, and documents. All resources, including studies, reports, and policy briefs, were consolidated and summarized in league tables and discussed by the co-authors to determine key findings and themes under the headings of access and affordability. We discuss our findings in eponymous sections, following which we outline future policy directions under a universal health coverage framework that are pertinent to elderly health.
ACCESS: A CONTINUING CONCERN
Social Determinants of Access
A closer look at the literature on access to healthcare reveals variation across an age gradient. Older Indians have reported higher rates of outpatient and inpatient visits (Alam and Karan, 2010). The age gradient in
elderly health access is overlaid by social determinants of health. For one, there is a feminization of the elderly population; according to the 2001 census, the gender ratio among the Indian elderly aged 60 years and older is 1,028 females for 1,000 males (Rajan and Aliyar, 2008). It is expected that by 2016, 51% of India’s elderly will be women (in rural areas, this proportion will be much higher) (Kumari, 2001; Rao, 2006). More women report poor health status as compared to males, and yet a far greater proportion of men are hospitalized as compared to females (87 versus 67 per 1,000 aged persons) (Rajan and Sreerupa, 2008).
Unmet health needs are more pronounced among the 33.1% of the elderly in India who in 2001 were reported to have lost their spouses (Rajan and Aliyar, 2008), of whom a larger relative proportion is female (50% of female elderly are widows versus only 15% of male elderly who are widowers). Studies have shown that widows are disproportionately vulnerable to disability, illness, and poor healthcare utilization (Sreerupa, 2006) due to a number of mobility, employment, property, and financial constraints (Dreze, 1990).
In addition to gender and marital status, religion, caste, education, economic independence, and sanitation have bearing on elderly health. Count modeling of data from the 52nd Round of the NSS indicates that the number of diseases suffered by an elderly person, calculated independently for rural (Poisson Model) and urban populations (Negative Binomial Model), include age, gender, literacy, availability of drinking water and a toilet facility, and household monthly consumption expenditure (Alam, 2006). Another study of Uttar Pradesh (UP) and Maharashtra found that the older elderly (70 years and older) were significantly less likely to seek treatment compared to the 60-69 age category, while Muslims were between 62% and 49% more likely to seek treatment in UP and Maharashtra, respectively, compared to Hindus (Agrawal and Arokiasamy, 2009). This study found that elderly in scheduled tribe/scheduled caste (SC/ST) categories were 54% less likely and other backward classes (OBC) 35% less likely to seek treatment for existing ailments in Maharashtra compared to other castes. Finally, high school graduates were twice as likely in UP and four times as likely in Maharashtra to seek treatment compared to the illiterate group. However, in the above-mentioned study, a majority of the elderly suffered from multiple morbidity conditions, which makes interpreting the presented results difficult. The absence of rigorously designed studies that assess the types and severity of various disease conditions in the elderly further highlights this fact. Rajan (2006), using data from the same survey, concluded that 9.5% of rural inhabitants and 4.2% of urban inhabitants report lack of access to day-to-day requirements of medicine, close to double that of clothing and food.
Although broader trends of economic dependence are changing, kinship systems and social support still have strong bearing on access to healthcare among the elderly (see discussion below). A strong link can be established between ownership of property and kin-based caregiving arrangements. Traditional arrangements structured shared domicile of the elderly in their ancestral homes along with younger generations, who would later inherit this property (Rajan, 2006). While strong cultural emphasis was and continues to be placed upon respect for the elderly (Sivamurthy and Wadakannavar, 2001), kin conflict and such other broader considerations as caste order have historically hampered access to health (Cohen, 1998). Propertyless elders have a relatively higher likelihood of residence in old-age homes, living alone, and being looked after by relations other than their children when widowed (Kodoth and Rajan, 2008). More recently, arrangements of “living apart but together” are increasingly common, where joint family co-residence is discontinued but strong social support is immediately available, particularly in times of health crises (Sokolovsky, 2001). Given this variable provision of support, “discourses of neglect” may emerge, where in their everyday lives, the needs and problems of the elderly are invisible to those who offer them support in times of acute ill health (Sokolovsky, 2001). Moreover, research in India has shown that it is not the quantity but rather the quality of particular ties that relate to health. In some cases, having a continuous engagement or strong tie with a neighbor or child may have a more health-protective impact than having many (weak) ties to a host of family and community members (Sudha et al., 2006).
While systematic studies are rare, there have been increasing reports of material exploitation, financial deprivation, property grabbing, abandonment, verbal humiliation, and emotional and psychological torment in India, all of which compromise the mental and physical health of the elderly (Shankardass, 2009). In 2007, the Maintenance and Welfare of Parents and Senior Citizens Bill raised the profile of such practices, issuing penalties for abuse and neglect of elders exacted by members of their extended/joint family. At the same time, Delhi saw a tripling of police reports of elderly seeking protection in an 18-month period, and Mumbai’s police helpline for seniors was receiving more than 80 calls daily (Datta, 2007). Reports of murder, rape, burglary, and violence inflicted upon the elderly remain and are more commonly reported in Indian metropolitan areas. (It is unclear whether they are more common, due to possible under-reporting or publication bias.)
The stigma of aging, as well as the health and social conditions the elderly commonly face (such as dementia, depression, incontinence, or widowhood), is another social barrier to access of health, manifest in the Indian case in unique ways (World Health Organization [WHO],
2002). Patel and Prince’s qualitative study (2001) on the cultural perceptions of mental health needs among the aged in Goa, India, revealed that despite being frequently observed in the elderly population, certain mental health deficits were not acknowledged as health needs. Conditions like dementia are viewed as normal aging and depression construed as the result of neglect by family. Such cases were therefore not considered the purview of health professionals and were more frequently acknowledged and addressed by community health workers. Access to mental health services in the medical sector are limited, and, thus, most care and support was provided ad hoc, informally, and in the family. Consequently, “dependency anxiety” was a common phenomenon among the elderly, i.e., elderly felt the need to curtail their dependence upon the family and felt anxious about informing them about their health problems (Patel and Prince, 2001). The stigma of widowhood has been examined at length and leads to profound social ostracism that impinges not only on access to healthcare, but also a broader range of fundamental human rights, such as the right to shelter, food, property, and information (Chen, 1998; Dreze, 1990).
Physical Determinants of Access
A key physical barrier to access is that many elderly require home-based care, a need arising from illness-related confinement following an age gradient. Elderly confinement to the home is consistent in both rural and urban areas (Aliyar and Rajan, 2008). Sample survey data suggest that as many as 64 per 1,000 population in rural areas and 67 per 1,000 population in urban areas are confined to the home. For those aged 80 and older, as many as one in five are confined. Reduced mobility hinders health-seeking.
While health-seeking is hindered, health needs tend to increase through the life course and across geographies. According to NSSO data, 28.3% of the aged in rural areas and 36.8% in urban areas suffer from one disease or another (Kumari, 2001). The greater reported morbidity in urban areas is misleading. Census data reveal higher proportions of people aged 60 and older in rural areas (7.7% of the population in 2001) as compared to urban areas (6.7%), meaning that in absolute terms, the need for elderly care is slightly higher in rural areas. Moreover, higher rates of morbidity and hospitalization in urban areas are to be expected given that most geriatric services are in urban areas and at the tertiary level (Ingle and Nath, 2008). In contrast, the lack of infrastructure and health service reach in rural areas is worrisome since of the 72% of the elderly population that is not working, 69% is rural (Kumari, 2001). Moreover, longitudinal data suggest the greatest deterioration in health status has
been of females living in urban areas (Husain and Ghosh, 2010). There is an acute need for expanding access to geriatric care beyond the tertiary level, in rural areas, and in service of the female elderly.
Even in cases where services are available, uptake is low because of lack of health promotion and community outreach. Goel and colleagues (2003) undertook a survey of 354 elderly rural inhabitants in Meerut, Uttar Pradesh, of whom only 53% were even aware of the geriatric welfare services available in their area and only 4% reported ever using them. Even in south India, where healthcare utilization is generally higher, evidence suggests similar trends. Another observational study of 213 elderly in Udupi, Karnataka, found that only 35.7% were aware of geriatric welfare services and 14.6% had used them (Lena et al., 2009).1
AFFORDABILITY: A COMPLEX CONUNDRUM
Affordability Through Income, Employment, and Assets
India has no population-wide mechanisms of social security. Given this scenario, Indians have to work as long as possible in order to support themselves (Mathew and Rajan, 2008). Employer insurance and pension schemes are available only to as low as 9% of rural males and 41.9% of urban males who are in the formal sector; among females, the figures are lower still (3.9% rural, 38.5% urban) (Rajan and Aiyar, 2008). The rest of the workforce comprises casual and self-employed workers who are not entitled to formal retirement benefits and, in order to afford healthcare in their early years, face the paradoxical challenges of remaining both healthy and employed in old age. Those in the formal sector may experience a halving of their incomes, which, in the face of rising inflation, leaves smaller proportions of income that may be allocated to health (Mathew and Rajan, 2008). As a result, a considerable proportion of the elderly are employed. An analysis of the Worker Population Ratios (WPRs) depicts that 56.79% of elderly males and 16.32% of elderly females were engaged in employment (proportions are higher in rural
____________
1 A corollary to confinement and multiple and chronic morbidity profile typical of the elderly is that multidrug use and polypharmaceutical use is common, heightening the propensity for inappropriate drug prescription and health-harming sequelae. A study of the elderly in Gujarat found that almost one-quarter in a sample of more than 400 patients received at least one inappropriate drug prescription according to Beer’s 2003 criteria, most commonly for upper respiratory tract infection (URTI), abdominal pain, and congestive cardiac failure (Zaveri, Mansury, and Patel, 2010). Harugeri and colleagues (2010) found in a tertiary care facility that almost one-quarter of elderly patients engaged in potentially inappropriate medication use and, further, that the drug profile among the elderly is more varied than gold standard (Beer’s) criteria used to assess medication use.
areas) (Mathew and Rajan, 2008). Among the elderly participating in the workforce, a majority (nearly 95%) is either self-employed or involved in casual labor with a maximum number of elderly being self-employed (79%) (Mathew and Rajan, 2008). Such employment arrangements may offer limited remuneration and require the elderly to keep working: NSS data suggest that almost one-fourth of males and one-sixth of females are employed even in the 80-84 age group (Mathew and Rajan, 2008).
In view of increasing the financial security of the elderly, higher tax exemption has been provided for the elderly, and the exemption age has also been reduced from 65 to 60 in the 2011 budget. Also, a new category called “very senior citizen” for elderly above 80 years of age has been introduced for greater tax exemption (Highlights of Union Budget 2011-2012, 2011). Notwithstanding these most recent developments, the overall pattern of employment in old age has required the pursuit of financial security up to later periods in life. The declining health and energy of the elderly discourages employers from hiring them in the regular workforce, forcing the elderly to opt for self-employment and casual labor, particularly in rural areas, where employment opportunities are generally low (Mathew and Rajan, 2008).
In the absence of state-level measures of providing social security, security in old age may be assured through movable or immovable property assets. In India, which is largely patriarchal, the ownership of land, house, or property is mostly owned and devolved among men with exceptions on the southwest coast and in the northeast (where matrilineal societies have existed) (Agarwal, 1994). Thus, ownership of property and assets is strongly affected by prevailing social norms related to gender and socioeconomic status (Agarwal, 1994; Agnes, 1999; Chen, 1998; Dreze, 1990). In the case of women, the basis of property rights not only is generally weak but also seems to be eroding. Ownership rights vary for women depending on their status as daughters or widows (Agarwal, 1994; Chen, 2000; Dreze, 1990). NSS data show that more than twice the number of male elderly own property or assets compared to female elderly in both urban and rural areas, a difference that is moderated by socioeconomic status (i.e., lower strata have greater gender disparities in property ownership) (Kodoth and Rajan, 2008). Transfer of property to children results in propertylessness, a phenomenon more common among rural elderly men and urban widowed women with sons. Lack of property means lack of assets or a safety net to rely on as health costs escalate through old age (Agnes, 1999).
Paying for Healthcare
Apart from individual-level socioeconomic issues that adversely affect affordability, a number of systemic factors underpin the reduced ability of
people, particularly the elderly, to pay for healthcare. Although all forms of healthcare payments are available in India, 83% of healthcare expenses are private out-of-pocket (OOP) expenditures (Duggal, 2007). India’s relatively unaccountable and inefficient public system of healthcare has led to the evolution of a highly varied, unregulated, and mostly expensive private sector that provides most healthcare, rendering Indians increasingly vulnerable to catastrophic health expenditures and poverty (Pal, 2010).
According to 2005 estimates, per capita expenditure on health is 125 Indian Rupees (INR), of which per capita OOP expenditure is 100 INR. The largest proportion of this OOP expenditure is spent on outpatient expenditures (74 INR), which overlaps to a great extent with the purchase of drugs (72 INR) (IIPS, 2007). The elderly, due to increased morbidity from chronic diseases, have long-term healthcare needs and a large likelihood of having health expenditures in general and OOP expenditures in particular. The need for healthcare increases with age. Those above 65 years spend on average 1.5 times on healthcare compared to those in the 60-64 year age category (Mahal, Berman, and Indicus Analytics, 2002). The elderly have little recourse as insurance does not cover outpatient or drug purchase. Moreover, insurance plans only cover inpatient hospital expenses (Shahrawat and Rao, 2011), and, thus, even insured elderly have a higher chance of falling into poverty, given that catastrophic expenditure occurs due to outpatient and drug expenses. In fact, the probability of catastrophic OOP expenses in households with elderly is much higher as compared to households without elderly members (Pal, 2010). Evidence suggests that if OOP payments for either medicines or outpatient care were removed, only 0.5% of people would fall into poverty due to health spending (Shahrawat and Rao, 2011).
Financial protection for health spending in India is largely in the form of savings and insurance. However, insurance in India is limited not only by its low coverage of conditions, but also by low coverage of populations. The National Family Health Survey of 2004-2005 indicates that only 10% of households in India had at least one member of the family covered by any form of health insurance (IIPS, 2007). Overall, the insurance market in India remains limited and fragmented in its presence. Benefits are accessed by only a few privileged sections of the population, such as those in the formal and civil service sectors like defense, civil services, and the railways, even after retirement long into old age (Acharya and Ranson, 2005; Ellis, Alam, and Gupta, 2000; Ranson, Sinha, and Chatterjee, 2006; Shiva Kumar et al., 2011). Lack of employment and income affect elderly utilization of medical insurance, as these populations are often incapable of paying regular insurance premiums. Finally, insurance companies often explicitly exclude the elderly due to age limits or eligibility restrictions for those with pre-existing conditions. This results in heightening the
estrangement of the aged from a healthcare system and policy environment that has historically lagged in supporting the financially weak.
UNIVERSAL HEALTH COVERAGE: STRATEGIC DIRECTIONS AND DATA NEEDS
A pathway to national health reform has been envisioned by the Planning Commission in the lead-up to the 12th Five-Year Plan for India. In October 2010, a High-Level Expert Group (HLEG) was convened by the Planning Commission to recommend changes in health financing, drug procurement, community participation in health, health management, and physical and financial norms for health and human resources. Situating elderly health in a broader framework of universal access and affordability of Universal Health Coverage (UHC) has potential to transform the structural conditions that hamper the well-being of the aged. We summarize some of the ways in which UHC may serve these functions, throughout indicating the evidence gaps that will be required for these functions to be met.
Key UHC reforms pertinent to access include the provision of additional human resources at the Sub-Health Centre level (per 5,000 population), as well as the introduction of an additional Community Health Worker (like an Accredited Social Health Activist) in rural and low-income urban areas. These reforms would ensure that in addition to existing priorities of maternal and child health, emerging priorities in NCD control, as well as action on social and physical barriers to access, can be addressed locally (i.e., in tandem with Village Health and Sanitation Committees and their urban equivalent). Future research may help determine the scope of care at the Sub-Health Centre level and the range of promotive services provided at the village/community in order to cater to the needs of India’s elderly.
It has been proposed by the HLEG, moreover, that an essential package of care (comprising primary-, secondary-, and tertiary-level services) be cashless at point of service through the use of a National Health Entitlement Card (which would also serve as an identifier for Electronic Medical Records, carrying patient histories and care-seeking profiles). This provision will be particularly useful for the elderly poor, and will require innovation and an expansive exercise in data collection and compilation on both the user and provider sides. To this end, methodological contributions from ongoing cohort studies such as the Longitudinal Study on Aging in India (LASI) and parallel efforts internationally will be highly valuable.
A number of regulatory mechanisms under the aegis of a newly proposed National Health Regulatory and Development Authority will
ensure health system support, accreditation, and continuous health systems evaluation. This process may benefit, again, from the growing base of research on elderly users of the health system, who may have a longer duration of interactions with the system as well as great variation in terms of need and burden, influenced by varying social determinants. Health systems evaluation will additionally have to reflect age-specific morbidity and mortality patterns, as well as that of intersectional elderly groups (the widowed elderly, aged of religious minority status, and others).
Ensuring the functioning of entitlements to health under the UHC is an increase in overall health spending from 1.2% of gross domestic product to 3% by 2022, funded through general taxation. It is anticipated that this will, in turn, reduce private OOP spending to 33% of total spending in the same period, thereby increasing the affordability of health among the most vulnerable. The phasing of this reduction, with its anticipated and unanticipated consequences for the elderly, will have to be carefully mapped and characterized in future research studies.
The creation of state essential drugs and medical device lists—for both allopathic and traditional medicine systems—is also proposed to ensure that price inflation is curbed for critical products. Data on which critical products are already used, and in what combinations, is a critical area of research as populations age and the need grows ever more urgent to balance cost containment against monitoring and control of drug resistance in India. Here, too, the burden of both (over)medication and resistance may be disproportionately faced by the elderly. Patterns and priorities will have to be determined based on routine and careful examination of the evidence among the Indian elderly.
CONCLUSION
The growth of the elderly population in the coming decades will bring with it unprecedented burdens of morbidity and mortality across the country. As we have outlined, key challenges to access to health for the Indian elderly include social barriers shaped by gender and other axes of social inequality (religion, caste, socioeconomic status, stigma). Physical barriers include reduced mobility, declining social engagement, and the limited reach of the health system. Health affordability constraints include limitations in income, employment, and assets, as well as the limitations of financial protection offered for health expenditures in the Indian health system.
Among the most significant findings that emerged in developing this review was the incompleteness of data on the burdens of access and affordability among elderly populations in India. A major reason for this is that routine health data collection in India is not designed to reflect
or characterize pathological progression: a process wherein, by virtue of being alive longer than others, the elderly are more likely to experience a pathology, leading to impairment, functional limitations, and ultimately disability (Lynch, Brown, and Taylor 2009). Many routine data collection procedures (National Sample Surveys, Census data, or death certificates) in India do not capture pathological progression nor do they disaggregate morbidity and disability outcomes among the elderly (as discussed at some length by Alam and Karan, 2010).
Recommendations under the UHC framework have prioritized primary and secondary prevention and health promotion, with the goal of creating enabling environments for healthy lifestyles, early detection, and routine screening among the aged and avoiding institutionalization. In order to ensure these needs are met, a concomitant program of dedicated research is required on how various UHC elements affect and may cater more appropriately to the growing demographic of Indian elderly.
REFERENCES
Acharya, A., and K. Ranson. (2005). Health care financing for the poor: Community-based health insurance schemes in Gujarat. Economic and Political Weekly 40:4,141-4,150.
Agarwal, B. (1994). Gender and command over property: A critical gap in economic analysis and policy in South Asia. World Development 10:1,455-1,478.
Agarwal, G., and P. Arokiasamy. (2010). Morbidity prevalence and health care utilization among older adults in India. Journal of Applied Gerontology 29(2):155-179.
Agnes, F. (1999). Law and women of age. A short note. Economic and Political Weekly 30:51-54.
Alam, M. (2000). Ageing in India: A country profile. Bold 10(3):5-22.
Alam, M. (2006). Ageing in India: Socio-economic and Health Dimensions. New Delhi: Academic Foundation.
Alam, M., and A. Karan. (2010). Elderly Health in India: Dimensions, Differentials, and Over Time Changes. Building Knowledge Base on Ageing in India: A series of Programmatic and Research Studies. New Delhi: United Nations Population Fund.
Aliyar, S., and S.I. Rajan. (2008). Population Projections for India, 2001-2101. Thiruvananthapuram: Centre for Development Studies.
Angra, S.K., G.V.S. Murthy, S.K. Gupta, and V. Angra. (1997). Cataract related blindness in India and its social implications. Indian Journal of Medical Research 106:312-324.
Chatterjee, C., and G. Sheoran. (2007). Vulnerable Groups in India. Mumbai: The Centre for Enquiry into Health and Allied Themes.
Chen, C. (1998). Widows in India: Social Neglect and Public Action. New Delhi: Sage.
Cohen, L. (1998). No Aging in India. Berkeley: University of California Press.
Datta, D. (2007). Home alone. India Today, July 16. Available: http://www.indiatoday.com/itoday/20070716/cover.html.
Dreze, J. (1990). Widows in Rural India. London: Development Economics Research Programme.
Dror, D.M., O. Putten-Rademaker, and R. Koren. (2008). Cost of illness: Evidence for a study of five resource-poor locations in India. Indian Journal of Medical Research 127:347-361.
Duggal, R. (2007). Poverty and health: Criticality of public financing. Indian Journal of Medical Research 126:309-317.
Ellis, R.P., M. Alam, and I. Gupta. (2000). Health insurance in India: Prognosis and prospects. Economic and Political Weekly 35:207-217.
Goel, P.K., S.K. Garg, J.V. Singh, M. Bhatnagar, H. Chopra, and S.K. Bajpai. (2003). Unmet needs of the elderly in a rural population of Meerut. Indian Journal of Community Medicine XXVIII:165-166.
Goldman, N., S. Korenman, and R. Weinstein. (1995). Marital status and health among the elderly. Social Science and Medicine 40(12):1,717-1,730.
Goswami, A., V.P. Reddaiah, S.K. Kapoor, B. Singh, S.N. Dwivedi, and G. Kumar. (2005). Tobacco and alcohol use in rural elderly Indian population. Indian Journal of Psychiatry 47(4):192-197. doi:10.4103/0019-5545.43050.
Government of India. (2011). National Programme for the Health Care of the Elderly (NPHCE), Operational guidelines. New Delhi: Government of India.
Gruenberg, E. (1977). The failure of success. Milbank Memorial Fund Quarterly/Health and Society 55:3-24.
Gupta, P.C., P.K. Maulik, P.K. Pednekar, and S. Saxena. (2005). Concurrent alcohol and tobacco use among a middle-aged and elderly population in Mumbai. National Medical Journal of India 18(2):88-91.
Gupta I., and D. Sankar. (2002). Health of the Elderly in India: A Multivariate Analysis Discussion Paper 46. New Delhi: Institute of Economic Growth. Available: http://iegindia.org/dis_ind_46.pdf.
Harugeri, A., J. Joseph, G. Parthasarathi, M. Ramesh, and S. Guido. (2010). Potentially inappropriate medication use in elderly patients: A study of prevalence and predictors in two teaching hospitals. Journal of Postgraduate Medicine 56(3):186-191.
Highlights of Union Budget, 2011-2012. (2011, February 28). The Times of India, p. A1.
Husain, Z., and S. Ghosh. (2010). Is health status of elderly worsening in India?: A comparison of successive rounds of National Sample Survey data. Munich Personal RePEc Archive. Report No. 25747. Available: http://mpra.ub.uni-muenchen.de/25747/1/MPRA_paper_25747.pdf.
Indian Institute of Population Sciences. (2007). NFHS-3. National Family Health Survey, 2005-06. Mumbai: Indian Institute of Population Sciences. Available: http://www.mohfw.nic.in/nfhs3/index.htm.
Ingle, G.K., and A. Nath. (2008). Geriatric health in India: Concerns and solutions. Indian Journal of Community Medicine 33:214-218.
Jha, P., V. Gajalakshmi, P.C. Gupta, et al. (2006). Prospective study of one million deaths in India: Rationale, design, and validation results. PLoS Medicine 3:18.
Kodoth, P., and S.I. Rajan. (2008). Property and assets as economic security. Pp. 83-114 in Institutional Provisions and Care for the Aged: Perspectives from Asia and Europe, S.I. Rajan, C. Risseeuw, and M. Perera. (Eds.). New Delhi: Anthem Press.
Kosuke, I., and S. Samir. (2004). On the estimation of disability-free life expectancy: Sullivan’s method and its extension. Journal of the American Statistical Association 102:1,199-1,211.
Kowal, P., K. Kahn, N. Nawi, N. Naidoo, S. Abdullah, A. Bawah, et al. (2010). Ageing and adult health status in eight lower-income countries: The INDEPTH WHO-SAGE Collaboration. INDEPTH WHO-SAGE Supplement. Global Health Action 3. Published online doi: 10.3402/gha.v3i0.5302. Available: http://www.globalhealthaction.net/index.php/gha/article/view/5302/6049.
Kumar, V. (2003). Health status and health care services among older persons in India. Journal of Aging & Social Policy 15(2/3):67-83.
Kumari, R.S.S. (2001). Socio-economic Conditions, Morbidity Pattern and Social Support among Elderly Women in a Rural Area. Medical College, Thiruvananthapuram, Kerala.
Lena, A., K. Ashok, M. Padma, V. Kamath, and A. Kamath. (2009). Health and social problems of the elderly: A cross-sectional study in Udupi Taluk, Karnataka. Indian Journal of Community Medicine 34:131-134.
Lynch, S.M., S.J. Brown, and M.G. Taylor. (2009). The demography of disability. In International Handbook of Population Aging, Peter Uhlenberg (Ed.). London: Springer-Verlag.
Mahal, A., P. Berman, and Indicus Analytics. (2002). Estimating Baseline Health Expenditures on the Elderly in India. Draft. Harvard School of Public Health, Department of Population and International Health.
Mathew, E.T., and Rajan, S. I. (2008). Employment as Old Age Security. Pp. 68-82 in Institutional Provisions and Care for the Aged: Perspectives from Asia and Europe, S.I. Rajan, C. Risseeuw, and M. Perera (Eds.). New Delhi: Anthem Press.
Mini, G.K. (2008). Socioeconomic and demographic diversity in the health status of elderly people in a transitional society, Kerala, India. Published online in Journal of Biosocial Science 10.
Mutharayappa, R., and T.N. Bhat. (2008). Is lifestyle influencing morbidity among elderly? Journal of Health Management 10(2):203-217. doi:10.1177/097206340801000203.
National Sample Survey Organization. (1996). The Aged in India: A Socio-economic Profile, 1995-96. National Sample Survey 52nd Round Report. New Delhi: Ministry of Statistics and Programme Implementation, Government of India.
National Sample Survey Organisation. (2006). Morbidity, Health Care and the Condition of the Aged. National Sample Survey, 60th Round, Report no. 507 (60/25.0/1). New Delhi: Ministry of Statistics and Programme Implementation, Government of India.
Pal, R. (2010). Analysing Catastrophic OOP Health Expenditure in India: Concepts, Determinants and Policy Implications. Mumbai: Indira Gandhi Institute of Development Research.
Patel, V., and M. Prince. (2001). Ageing and mental health in a developing country: Who cares? Qualitative studies from Goa, India. Psychological Medicine 31:29-38.
Patel, V., A.K. Kumar, V.K. Paul, K.D. Rao, and K.S. Reddy. (2011). Universal health care in India: The time is right. The Lancet 377(9764): 448-449.
Pope, C., S. Ziebland, and N. Mays. (2000). Qualitative research in health care. Analysing qualitative data. British Medical Journal 320(7,227):114-116.
Radha Devi, D., S. Santhosh, A. Asharaf, and T.K. Roy. (1999). Aged in a Changing Society: A Case Study of Kerala. Mumbai: International Institute.
Rajan, R.G., and E.S. Prasad. (2008). A pragmatic approach to capital account liberalization. Journal of Economic Perspectives 22(3):149-172.
Rajan, S.I. (2001). Social assistance for poor elderly: How effective? Economic and Political Weekly:613-617.
Rajan, S.I. (2006). Population Ageing and Health in India. Mumbai: Centre for Enquiry into Health and Allied Themes.
Rajan, S.I., and S. Aiyar. (2008). Population ageing in India. Pp. 39-54 in Institutional Provisions and Care for the Aged: Perspectives from Asia and Europe, S.I. Rajan, C. Risseeuw, and M. Perera (Eds.). New Delhi: Anthem Press.
Rajan, S.I., and S. Kumar. (2003). Living arrangements among Indian elderly: New evidence from National Family Health Survey. Economic and Political Weekly 38(3):75-80.
Rajan, S.I., and Sreerupa. (2008). Disease, disability and healthcare utilization among the aged. Pp. 39-54 in Institutional Provisions and Care for the Aged: Perspectives from Asia and Europe, S.I. Rajan, C. Risseeuw, and M. Perera (Eds.). New Delhi: Anthem Press.
Rajan, S.I., U.S. Misra, and P.S. Sharma. (1999). India’s Elderly: Burden or Challenge? New Delhi: Sage.
Raju, S. (2006). Ageing in India in the 21st Century: A Research Agenda. Mumbai: The Harmony Initiative. Available: http://harmonyindia.org/hdownloads/Monograph_FINAL.pdf.
Raju, S. (2000). Ageing in India: An overview. In Gerontological Social Work in India: Some Issues and Perspectives, M. Desai and S. Raju (Eds.). New Delhi: B.R. Publishing.
Ranson, M.K., T. Sinha, M. Chatterjee, et al. (2006). Making health insurance work for the poor: Learning from SEWA’s community-based health insurance scheme. Social Science & Medicine 62:707-720.
Rao, M. (2006). Economic and Financial Aspects of Ageing in India. Paper presented at the UN Regional Workshop on Gender-Responsive Health Security for the Elderly, September 18-19, Seoul, Republic of Korea. Available: http://www.unescap.org/esid/gad/issues/Socialprotection/Report-RegWkshp-HealthSecurity-18-19Sep06-Seoul.pdf.
Rastogi, T., M. Vaz, D. Spiegelman, K.S. Reddy, A.V. Bharathi, M.J. Stampfer, W.C. Willett, and A. Ascherio. (2004). Physical activity and risk of coronary heart disease in India. International Journal of Epidemiology 33:759-767. doi:10.1093/ije/dyh042.
Roy, G.S. (1994). Morbidity related epidemiological determinants in Indian aged: An overview. Pp. 114-125 in Public Health Implications of Ageing in India, C.R. Ramaachandran and B. Shah (Eds.). New Delhi: Indian Council of Medical Research.
Selvaraj, S., A. Karan, and S. Madheswaran. (2010). Elderly Workforce in India: Labour Market Participation, Wage Differentials and Contribution to Household Income. Unpublished report, Public Health Foundation of India, New Delhi.
Shah, B., and A.K. Prabhakar. (1997). Chronic morbidity profile among elderly. Indian Journal of Medical Research 106:265-272.
Shahrawat, R., and K.D. Rao. (2011). Insured yet vulnerable: Out-of-pocket payments and India’s poor. Online published in Health Policy and Planning (April 21, 2011). doi:10.1093 /heapol/czr029.
Shankardass, M. (2009). No one cares about elder abuse in India. One World South Asia. Available: http://southasia.oneworld.net/opinioncomment/no-one-cares-about-elder- abuse-in-india.
Shiva Kumar, A.K., C.C. Lincoln, M. Choudhary, G. Shiban, V. Mahajan, A. Sinha, and A. Sen. (2011). Financing health for all: Challenges and opportunities. The Lancet Special Issue India: Towards Universal Health Coverage:92-103.
Shrestha, L.B. (2000). Population aging in developing countries. Health Affairs 19(3):204-212.
Sivamurthy, M., and A.R. Wadakannavar. (2001). Care and support for the elderly population in India: Results of a survey rural North Karnataka. Available: http://www.iussp.org/Brazil2001/s50/S55_P04_Sivamurthy.pdf.
Sokolovsky, J. (2001). Living arrangements of older persons and family support in less developed countries. Population Bulletin of the United Nations, Spl. Issue (Living arrangements of older persons-Critical issues and policy responses) 42/43:162-192.
Sreerupa (2006). Gender, Ageing and Widowhood: Health Vulnerability and Socio-Economic Influences. M.Phil Dissertation, submitted to Jawaharlal Nehru University, New Delhi.
Sudha, S., C. Suchindran, E.J. Mutran, S.I. Rajan, and P.S. Sarma. (2006). Marital status, family ties and self-rated health among elders in South India. Journal of Cross-Cultural Gerontology 21:3-4.
United Nations Department of Economic and Social Affairs, Population Division. (2008). World Population Prospects (2008 Revision). Available: http://esa.un.org/unpp/index.asp?panel=2.
Vaz, M., and A.V. Bharathi. (2004). Perceptions of the intensity of specific physical activities in Bangalore, South India: Implications for exercise prescription. Journal of the Association of Physicians in India 52:541-544.
Waite, L.J. (2004). Ageing, health, and public policy: Demographic and economic perspectives. Population and Development Review 30(Suppl.):239-265.
World Health Organization. (2002). Reducing Stigma and Discrimination against Older People with Mental Disorders. Geneva: World Health Organization and World Psychiatric Association. Available: http://whqlibdoc.who.int/hq/2002/WHO_MSD_MBD_02.3.pdf.
Zaveri, H.G., S.M. Mansuri, and V.J. Patel. (2010). Use of potentially inappropriate medicines in elderly: A prospective study in medicine out-patient department of a tertiary care teaching hospital. Indian Journal of Pharmacology 42(2):95-98.
















