
Over the past decade, federal, state, tribal, and local governments, the Institute of Medicine (IOM), and other entities have embarked on developing crisis standards of care (CSC) plans and guidance (e.g., AHRQ, 2005; Devereaux et al., 2008; IOM, 2009, 2012; Ohio Hospital Association and Ohio Department of Health, 2011; Phillips and Knebel, 2007; State of Michigan, 2013; Timbie et al., 2012). CSC planning is intended to help the emergency response system—including emergency management, public health, behavioral health, emergency medical services (EMS), health care organizations and providers—provide patients with the best care possible given the circumstances. In catastrophic disasters involving an overwhelming demand for medical care, CSC planning is also intended to enable more effective use of the limited resources through fair, just, and equitable processes for making decisions about who should receive treatments when there are not enough resources to provide patients with the level of care they would usually receive.
As this body of work continues to evolve, the need for guidance on how to incorporate indicators and triggers that aid decision making about the provision of care in disasters has been identified as a gap. Indicators are measurements or predictors of change in demand for health care service delivery or availability of resources. Triggers are decision points that are based on changes in the availability of resources that require adaptations to health care services delivery along the care continuum.1 Advance planning about indicators and triggers involves considering what information about demand and resources is available across the health care spectrum, how this information is shared and integrated, how this information drives actions, and what actions might be taken to provide the best health care possible given the situation. Because of the stress, complexity, uncertainty, and time sensitivity inherent in a crisis situation, it is important that these discussions occur in advance. The development and use of indicators and triggers helps enable good decision making.
This report provides an overview of key considerations relevant to the development of indicators and triggers and a toolkit designed to facilitate discussions among stakeholders in developing indicators and triggers for their own organizations, agencies, regional health care coalitions, and states. The toolkit provides
____________________
1 “The surge capacity following a mass casualty incident falls into three basic categories, depending on the magnitude of the incident: conventional, contingency, and crisis. These categories also represent a corresponding continuum of patient care delivered during a disaster. As the imbalance increases between resource availability and demand, health care—emblematic of the health care system as a whole—maximizes conventional capacity; then moves into contingency; and, once that capacity is maximized, moves finally into crisis capacity. A crisis situation may lead to an overwhelming demand for services and result in shortages of equipment, supplies, pharmaceuticals, personnel, and other critical resources, necessitating operational adjustments” (IOM, 2012, p. 1-6)
key questions and example indicators and triggers for the major components of the emergency response system: emergency management, public health, behavioral health, EMS, hospital and acute care, and out-of-hospital. The toolkit is designed to be scalable for use at multiple levels, from the facility, organization, and agency levels up through the whole community’s emergency response system. Discussions need to occur at all levels so they include the level of detail about organizational capabilities that is needed for operational decision making, within the context of integrative planning for a coordinated response. These discussions will help the stakeholders develop the capabilities described in both the Hospital Preparedness Program (HPP) and the Public Health Emergency Preparedness (PHEP) cooperative agreements (ASPR, 2012a; CDC, 2011).
At the request of the Assistant Secretary for Preparedness and Response (ASPR) at the Department of Health and Human Services (HHS), the National Highway Traffic Safety Administration (NHTSA) in the Department of Transportation, and the Veterans Health Administration, in the fall of 2012 the IOM convened the Committee on Crisis Standards of Care: A Toolkit for Indicators and Triggers. The task was to prepare a conversation toolkit to guide stakeholders through the process of developing indicators and triggers that may govern their health system’s transition across the continuum of care, from conventional standards of care to contingency surge response and standards of care to crisis surge response and standards of care, and back to conventional standards of care. Box 1-1 presents the statement of task.
This committee was made up of experts in the fields and sectors responsible for implementing CSC, including public health, emergency medicine, nursing, pediatrics, EMS, emergency management, and disaster behavioral health. Appendix C contains biosketches of the committee members. The work of the current committee builds on the work of a previous IOM committee, the Committee on Guidance for Establishing Standards of Care for Use in Disaster Situations (IOM, 2009, 2012). The work of that committee is described below.
To gather stakeholder input, the current committee held an open meeting in January 2013. Panelists from different stakeholder perspectives were invited, including public health, emergency management, EMS, health care coalitions, home health, long-term care and nursing homes, behavioral health, specialty burn care, and information management. The committee also sought input on the task from representatives of the federal government, including ASPR and NHTSA. The committee met in closed session in conjunction with the open meeting and once again in March 2013 to review the evidence and draft the report.
In addition, the committee reviewed relevant literature. The MEDLINE/PubMed and Scopus databases were searched using the following terms (in a variety of combinations): indicator, metric, measure, trigger, predictor, warning, precipitating factors, health system indicator, health system trigger, and health system measure, combined with the terms disaster, surge capacity, surge capability, medical surge, crisis standards of care, and allocation of scarce resources.2 Abstracts were reviewed and selected for relevance to the topic at hand. Finally, the committee examined previous efforts to determine indicators and triggers in publicly available state and local crisis standards of care plans.
____________________
2 The committee would like to thank Alicia Livinski of the National Institutes of Health Library for her help in conducting these searches.
BOX 1-1
Statement of Task
An ad hoc committee will conduct a study and prepare a short report that develops a conversation toolkit, which can be used by stakeholders in the development of crisis standards of care plans to guide the identification of clinical and administrative indicators that may govern the transition from conventional and contingency surge response and standards of care to crisis surge response and crisis standards of care, and the return to conventional standards of care. This conversation toolkit will be structured around a series of potential scenarios and prospective surveys that can be used to help identify indicators and triggers and facilitate a conversation among health care providers and other relevant stakeholders, but with specific emphasis on both the National Disaster Medical System and emergency medical services responders. The committee will develop this toolkit and base its recommendations on currently available policies, protocols, published literature, and other available guidance documents and evidence, as well as its expert judgment.
ORGANIZATION OF THE REPORT AND HOW TO USE THE TOOLKIT
This chapter provides a brief introduction to the concepts in crisis standards of care that are particularly relevant to indicators and triggers, as well as a discussion of the importance of developing indicators and triggers. This chapter summarizes certain key concepts from earlier IOM work on crisis standards of care. These reports contain extensive information and resources about developing CSC plans, including templates for planning and implementing CSC (IOM, 2009, 2012). These reports also cover in more detail key areas that are outside of the scope of full discussion in this report, including legal, ethical, and palliative care issues.
Chapter 2 discusses how to develop useful indicators and triggers, limitations and issues associated with indicators, and systems-level issues related to indicators and triggers. Chapters 3 through 9 form the toolkit. Chapter 3 provides the overarching framework for the toolkit and should be read first by everyone. Chapters 4 through 9 are customized for each component of the emergency response system: emergency management (Chapter 4), public health (Chapter 5), behavioral health (Chapter 6), EMS (Chapter 7), hospital and acute care (Chapter 8), and out-of-hospital care (Chapter 9). Because integrated planning across the emergency response system is critical for a coordinated response, it is important to read the toolkit introduction (Chapter 3) as well as the discipline-specific chapters.
This toolkit aims to provide the basis for discussions about indicators and triggers, and includes example indicators and triggers that are intended to help stakeholders start discussions specific to their own situations rather than serve as definitive lists. Indicators and triggers need to be discussed and developed at the agency, jurisdiction, and regional levels because of variability in daily resource availability and demand, infrastructure and available information, and actions that may be taken in response to an indicator or a trigger. The toolkit should be used to facilitate planning discussions in advance of a disaster so these discussions can occur without the stress, complexity, uncertainty, and time pressure of a disaster situation.
The discussion toolkit is structured around two scenarios, a series of key questions for discussion, and
a set of example tables. The example indicators and triggers encompass both clinical and administrative indicators and triggers. The committee included two scenarios (one slow-onset [influenza pandemic] and one no-notice incident [earthquake]) to make the discussions more vivid and to stimulate discussion. The scenarios also serve to help participants achieve an understanding of what the different components of the emergency response system would be facing during a catastrophic disaster and what they would be focused on, providing a necessary common picture to support discussions across these components. Scenario-based planning is the first component of the “hybrid planning approach” that is strongly advocated by the Federal Emergency Management Agency (FEMA) in its comprehensive preparedness guide and also described as the approach that health and public health planners commonly use (ASPR, 2012a; FEMA, 2010). This approach was also used in the recent discussion guides on pandemic influenza planning that were prepared at the request of the Centers for Disease Control and Prevention (ORISE 2013a,b,c).
PREVIOUS IOM WORK ON CRISIS STANDARDS OF CARE
During the spring of 2009, the IOM’s Forum on Medical and Public Health Preparedness for Catastrophic Events hosted a series of regional meetings on crisis standards of care. These regional meetings were intended to build on early work in this area, including efforts by the Government Accountability Office, the Agency for Healthcare Research and Quality, the New York State Task Force on Life and the Law, and the American College of Chest Physicians Task Force for Mass Critical Care (AHRQ, 2005; Devereaux et al., 2008; GAO, 2008; Powell et al., 2008). Discussions at the regional meetings identified the development of national guidance on standards of care during disaster situations as a crucial area for improving the nation’s preparedness (IOM, 2010).
Later that year, in the midst of the 2009 H1N1 pandemic, the ASPR asked the IOM to convene a committee of experts to develop guidance that health officials could use to establish and implement standards of care during disasters. The resulting letter report defined crisis standards of care as
A substantial change in usual health care operations and the level of care it is possible to deliver, which is made necessary by a pervasive (e.g., pandemic influenza) or catastrophic (e.g., earthquake, hurricane) disaster. This change in the level of care delivered is justified by specific circumstances and is formally declared by a state government in recognition that crisis operations will be in effect for a sustained period. The formal declaration that crisis standards of care are in operation enables specific legal/regulatory powers and protections for health care providers in the necessary tasks of allocating and using scarce medical resources and implementing alternate care facility operations. (IOM, 2009, p. 3)3
The report also described five key elements that should underlie all CSC plans:
1. A strong ethical grounding that enables a process deemed equitable and just based on its transparency, consistency, proportionality, and accountability;
2. Integrated and ongoing community and provider engagement, education, and communication;
____________________
3 The 2009 and 2012 reports emphasize the importance of the state’s role and of appropriate state declaration to recognize the need for crisis standards of care. However, it is also important that disaster planning, including planning for CSC, occur at all levels. Particularly in a no-notice disaster, the transition to crisis may need to be implemented immediately, although an appropriate declaration should be made as soon as possible and/or the authorities of the state director of public health should be used to implement actions (where applicable and appropriate).
3. The necessary legal authority and legal environment in which CSC can be ethically and optimally implemented;
4. Clear indicators, triggers, and lines of responsibility; and
5. Evidence-based clinical processes and operations.
In 2010, ASPR, the Department of Veterans Affairs (VA), and NHTSA asked the IOM expert committee to reconvene to provide concepts and guidance to help state and local officials apply the CSC framework the committee created earlier. In its 2012 report, Crisis Standards of Care: A Systems Framework for Catastrophic Disaster Response, the committee examined the effect of its 2009 report, and developed underlying principles, concepts, planning milestones, and templates to guide the efforts of professionals and organizations responsible for CSC planning and implementation (IOM, 2012).4 Like all of the IOM CSC work, this report took an all-hazards approach. The 2009 and 2012 reports have been referred to in HHS’s Hospital Preparedness Program and Public Health Emergency Preparedness cooperative agreements (ASPR, 2012a; CDC, 2011).
The following sections present key concepts from the 2009 and 2012 reports, with a specific focus on those that are relevant to indicators and triggers.
CONTINUUM OF CARE: CONVENTIONAL, CONTINGENCY, AND CRISIS
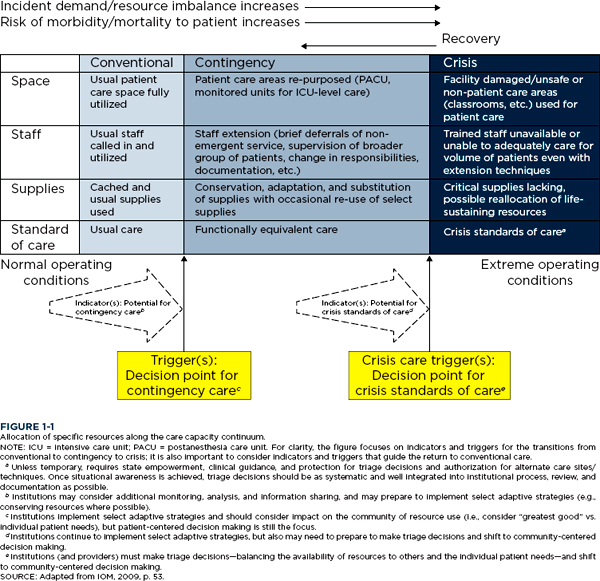
Rather than focusing exclusively on the most extreme circumstances, the committee that authored the 2009 and 2012 reports, as well as the current committee, envision surge capacity as occurring along a continuum based on resource availability and demand for health care services. One end of this continuum is defined by conventional care, which describes services that are provided in health care organizations on a daily basis. In the middle of the continuum, contingency care provides care that is functionally equivalent to usual patient care (e.g., one medication substituted for another that is not usually used in that circumstance but provides the same or a similar effect). At the far end of the continuum is crisis care, when the best possible care is provided to the population of patients as a whole because of the very limited resources available. Changes are made in the methods and locations of care delivery that present significant increased risk of adverse outcomes, and decision making shifts from patient-centered to population-centered outcomes. These levels of care are described in Box 1-2. Figure 1-1 illustrates how a surge response may shift across the continuum from conventional to crisis care based on the demand and supply mismatch that may occur over time, particularly as it affects the availability of patient care spaces; staff; and needed supplies, equipment, and pharmaceuticals.
A key observation is that transitions along the continuum of care do not always occur abruptly. For example, a slow-onset incident such as an influenza pandemic may result in a relatively gradual transition through the continuum, while an improvised nuclear device detonation near a downtown medical center may require an immediate transition to crisis care. Along this continuum, indicators demonstrate the potential for movement toward a different level of care: from conventional to contingency, from contingency to
____________________
4 The 2012 report and associated materials are available at http://www.iom.edu/crisisstandards.
BOX 1-2
Conventional, Contingency, and Crisis Care
Conventional capacity: The spaces, staff, and supplies used are consistent with daily practices within the institution. These spaces and practices are used during a major mass casualty incident that triggers activation of the facility emergency operations plan.
Contingency capacity: The spaces, staff, and supplies used are not consistent with daily practices, but provide care that is functionally equivalent to usual patient care. These spaces or practices may be used temporarily during a major mass casualty incident or on a more sustained basis during a disaster (when the demands of the incident exceed community resources).
Crisis capacity: Adaptive spaces, staff, and supplies are not consistent with usual standards of care, but provide sufficiency of care in the context of a catastrophic disaster (i.e., provide the best possible care to patients given the circumstances and resources available). Crisis capacity activation constitutes a significant adjustment to standards of care.
SOURCE: Hick et al., 2009.
crisis, or from crisis back toward conventional.5 The triggers are decision points, based on changes in the availability of resources, which require adaptations to health care services delivery along the care continuum.
A SYSTEMS APPROACH TO CATASTROPHIC DISASTER RESPONSE
Successfully responding to a catastrophic disaster will require integrated planning, coordination, cooperation, and consultation of many response disciplines and agencies, including state and local governments, EMS, health care organizations, and health care providers in the community. The 2012 report developed a systems framework for catastrophic disaster response, which includes, but is not limited to, the development and implementation of CSC plans.6 This framework is illustrated in Figure 1-2; certain elements are discussed briefly below, but much greater detail is available in the 2012 report.7
In this framework, ethical considerations and the legal authority and environment form the foundation. As emphasized in both the 2009 and 2012 reports, it is critical that ethical decision making underlies all
____________________
5 The 2009 and 2012 reports described indicators as being those data points occurring at the boundary of conventional to contingency care that demonstrated the potential for movement toward crisis standards of care. These reports focused on triggers as delineating the movement into crisis standards of care. The current report expands the focus to examine indicators and triggers across the entire continuum. This report describes indicators for all transitions along the continuum. It also uses the term crisis care trigger to describe triggers for the transition from contingency to crisis, and the term trigger to describe triggers at other boundaries along the continuum. Figure 1-1 has been updated to reflect this expanded focus.
6 The format of the 2012 report was designed to reflect its purpose of providing a resource manual for all stakeholders involved in a disaster response. The first volume describes the overall framework and legal issues, and discusses the crosscutting themes of ethics, palliative care, and mental health. The next four volumes are each aimed at a key stakeholder group: state and local governments, EMS, hospitals and acute care facilities, and out-of-hospital and alternate care sites. Lastly, there is a volume on public engagement.
7 The framework provides the overall systems approach; tactical-level responses are not included in Figure 1-2.
aspects of disaster planning and response to ensure that the needs of the community are met and the response is fair, just, and equitable. The 2009 report discusses the duty to plan by noting that “in an important ethical sense, entering a crisis standard of care mode is not optional—it is a forced choice, based on the emerging situation. Under such circumstances, failing to make substantive adjustments to care operations—i.e., not to adopt crisis standards of care—is very likely to result in greater death, injury, or illness” (IOM, 2009, p. 15). The other foundational element of the framework is the legal authority and environment that support the necessary and appropriate actions during a disaster response. Detailed consideration of legal issues is outside of the scope of this project, but issues related to legal indicators and triggers are raised briefly in Chapter 2 and examples are given in Chapter 5, the public health portion of the toolkit. For additional discussion and
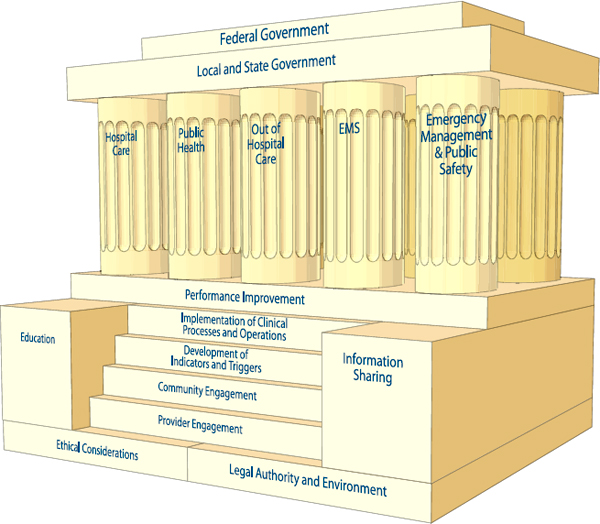
FIGURE 1-2
A systems framework for catastrophic disaster response.
NOTE: Ethical considerations and legal authority and environment form the foundation that undergirds crisis standards of care (CSC) planning and implementation. The steps represent key elements needed to implement disaster response. Education and information sharing are the cornerstones of the framework; together with the process of performance improvement, they support the key elements of CSC planning and enable midcourse corrections during the implementation of the framework. The response functions are performed by each of the five components of the emergency response system: hospitals and acute care, public health, out-of-hospital care, prehospital and emergency medical services (EMS), and emergency management/public safety. These components are interdependent in their contribution to the structure; they are joined by the roof, representing the overarching authority, additional resources, and protections offered by local, state, and federal governments.
SOURCE: IOM, 2012, p. 1-32.
details about the ethical and legal foundation, and other components of the framework described below, see the 2009 and 2012 reports.
The development of indicators and triggers was identified as a key step in the development of CSC plans (IOM, 2012). Following the release of the 2012 report, the development of indicators and triggers was specifically noted in the Hospital Preparedness Program and Public Health Emergency Preparedness cooperative agreements (ASPR, 2012a; CDC, 2011). The 2012 report contains extensive details about the roles and responsibilities for each component of the emergency response system, along with templates that identify core functions and tasks in both the planning and implementation of CSC. These templates use the same structure as the PHEP and HPP capabilities.
The emergency response system framework described above is consistent with the approach being
encouraged by most local, state, and federal government agencies. Communities across the country are increasingly working to integrate and coordinate multiple emergency response disciplines under a single planning and response approach. FEMA, the federal agency chiefly responsible for coordinating crisis and consequence management, has emphasized a “whole of community” approach to catastrophic disaster planning (FEMA, 2011). The Department of Homeland Security (DHS) Office of Health Affairs and ASPR have collaborated on multiple efforts, ranging from chemical terrorism response to improving community resiliency (Cibulsky and Kirk, 2010; DHS, 2011). Along with DHS and ASPR, CDC, the Food and Drug Administration, the National Institutes of Health, the Department of Defense, the VA, and the Department of Agriculture are working together to explore the advances of medical countermeasures for use in biodefense, chemical response, and radiological emergencies, led by the Biomedical Advanced Research and Development Authority (BARDA) (ASPR, 2013a). These attempts demonstrate the importance of multiagency and multidisciplinary involvement in planning for the complex and challenging environment of large-scale disaster response.
The next two sections briefly discuss the roles of emergency management and state and local governments in developing and implementing CSC plans and, in particular, in facilitating information sharing. A discussion of the roles of VA Medical Centers and Military Treatment Facilities, including the use of indicators and triggers in these facilities, is included in Chapter 2.
Emergency Management
Because the successful implementation of CSC efforts requires full mobilization and participation of the entire emergency response system, local and state offices of emergency management can play an important role in serving as the conveners of subject matter experts and stakeholders responsible for the development of CSC plans. The 2012 report includes emergency management as a key component of the emergency response system, but the concepts presented in this section provide additional details beyond those included in that report. Table 1-1 summarizes the ways in which Emergency Support Functions (ESFs) work together to support public health and medical response, with emergency management providing coordination of these efforts.
The supportive efforts of emergency management, focused on the integration of the emergency response functions, begin with their role in running local (home ruled), regional, and/or state emergency operations centers (EOCs) and Multiagency Coordination Systems, and extend to the information that is exchanged under the auspices of such efforts. Some of this information may be specified by public health or state regulatory requirements, for example, the reporting of select infectious disease outbreaks that may have implications for the larger community, including those that may herald the onset of a bioterrorism attack. Other agencies, such as those involved in the delivery of out-of-hospital care, including mental health services and EMS agencies, may need to share important information that would be protected under the Health Insurance Portability and Accountability Act (HIPAA) outside an emergency situation. Such information is sometimes not shared on account of uncertainties pertaining to the range and applicability of these existing regulations. Sharing clinical data, particularly deidentified data, can be an important adjunct to the creation of real-time awareness needed to help inform decision makers, particularly during epidemics. This is where
TABLE 1-1
Roles and Responsibilities of the Emergency Support Functions (ESFs)
| Examples of the Ways in Which ESFs Work Together to Support Public Health and Medical Response, with Emergency Management Providing Coordination of These Efforts | |
| ESF-1 – Transportation |
Aviation/airspace management and control
Aquatic/waterfront management and control
|
| ESF-2 – Communications |
Restoration and repair of communications infrastructure
|
| ESF-3 – Public Works and Engineering |
Infrastructure protection, emergency repair and restoration
|
| ESF-4 – Firefighting |
Provide support to wildland, rural, and urban firefighting operations
|
| ESF-5 – Emergency Management |
Coordination of incident management and response efforts across entire event (short term or sustained)
|
| ESF-6 – Mass Care, Emergency Assistance, Housing, and Human Services |
Support the ability and maintain the lead role to provide mass care and sheltering
|
| ESF-7 – Logistics Management and Resource Support |
Provide incident logistics planning, management, and sustainment capability
|
| Examples of the Ways in Which ESFs Work Together to Support Public Health and Medical Response, with Emergency Management Providing Coordination of These Efforts | |
| ESF-8 – Public Health and Medical Services |
Ensure coordination of health and medical response in these specific areas (see remainder of Table 1-1):
|
| ESF-9 – Search and Rescue |
Search and rescue operations
|
| ESF-10 – Oil and Hazardous Materials Response |
Hazardous materials (chemical, biological, radiological, etc.) response
|
| ESF-11 – Agriculture and Natural Resources |
Provide for animal welfare needs, coordination of response to plant disease and pest response
|
| ESF-12 – Energy |
Energy infrastructure assessment, repair, and restoration
|
| ESF-13 – Public Safety and Security |
Ensure access to public safety and security support
|
| ESF-14 – Long-Term Community Recovery | Social and economic community impact assessment Long-term community recovery assistance to states, local governments, and the private sector to restore damaged health care facilities Analysis and review of mitigation program implementation to prevent future damage to health care organizations (e.g., moving generators to roofs in flood-prone areas) Stress management and personal resilience resources assessment for public health and medical staff Analysis and review of repatriation of families and households that require home care (e.g., home ventilator patients) |
| ESF-15 – External Affairs |
Emergency public information and protective action guidance
|
SOURCE: Adapted from FEMA, 2008b.
public health should work with emergency management to ensure that appropriate data are shared to the level needed for response.
Information crucial to the monitoring of key indicators governing the change in delivery of health care services is likely to be most easily gathered, analyzed, and shared through the EOC during an incident. Given the usual functioning of EOCs, this is the single physical location where representatives from across the emergency response system are co-located, further facilitating the exchange of key information and the request for desired resources. In a sustained health incident, emergency management may still need to be connected to the remainder of the components of the emergency response system. It is possible to create a “virtual” EOC connection, particularly useful for slow-onset or sustained incidents such as an influenza pandemic, in which the monitoring function will persist for weeks or months. The need to staff a “physical location,” in this example, is less important than having the connectivity to share information with the emergency response community over the period of time that the response conditions are affected by the incident.
Emergency management agencies can help broker efforts to coordinate and analyze a variety of information sources, including from utilities and private enterprise, in the context of large-scale disaster incidents that will be marked by many different data feeds; sources of information, including the use of social media inputs; and the need to “roll up” information to make it usable and actionable. It is understood that the State Public Health Emergency Coordination Center8 would play a critical role in working with emergency management, particularly as it relates to the indicators and triggers being evaluated for CSC implementation, as further elaborated below.
State and Local Governments
State and local governments play a critical role in collecting information and providing access to such information on a day-to-day basis as well as during times of crisis. Specific to the planning efforts required for crisis standards of care implementation, state and local governments—but particularly the state departments of health (with active engagement of state EMS offices and prehospital care agencies)—will be key conveners of the CSC stakeholders, and will help to develop the protocols and identify the areas of greatest interest pertaining to data flow and information exchange. The 2009 and 2012 reports provided extensive discussion of the roles of state and local governments, with a particular focus on state and local departments of health (or other most relevant entity, depending on the state/local structure), in planning and implementing CSC (IOM, 2009, 2012).
The Medical Surge Capacity and Capability (MSCC) framework outlines a tiered system of relationships among individual health care organizations, health care coalitions, and local, state, and federal governments (Barbera and Macintyre, 2007, 2009). Figure 1-3 shows the integration of CSC planning and response into the MSCC framework, including specific entities that develop and help implement CSC, such as state and regional disaster medical advisory committees (or equivalent), triage teams, clinical care committees, and palliative care teams. For additional information about the roles of these entities, see Table 2-2 in the 2012 report, as well as the 2009 report (IOM, 2009, 2012).
Integrated planning within and across tiers is critical for a coordinated response, as all entities should
____________________
8 Depending on the state, this may be referred to in a variety of ways, including state (public) health emergency coordination center, department of (public) health operation center, or state (public) health operation center.
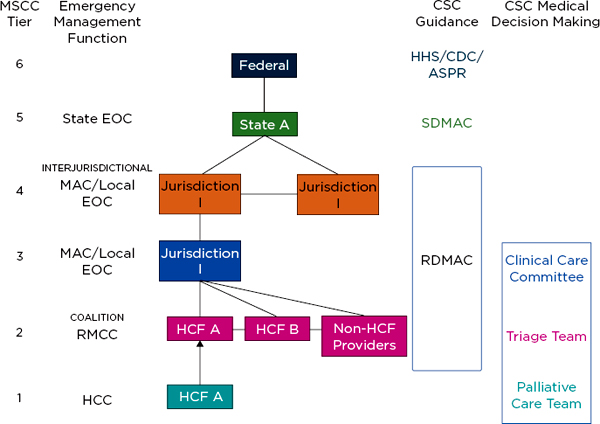
FIGURE 1-3
Integrating crisis standards of care planning into the Medical Surge Capacity and Capability framework.
NOTES: See Table 2-2 in IOM (2012) for further detail and description of the functions of these entities. The clinical care committee, triage team, and palliative care team may be established at MSCC tiers 1, 2, or 3. The RDMAC may be established at MSCC tiers 2, 3, or 4, depending on local agreements. The RMCC is linked to the MAC/Local EOC and is intended to provide regional health and medical information in those communities; it functions at MSCC tiers 2-4. ASPR = Assistant Secretary for Preparedness and Response (Department of Health and Human Services); CDC = Centers for Disease Control and Prevention; CSC = crisis standards of care; EOC = emergency operations center; HCC = health care coalition; HCF = health care facility; HHS = Department of Health and Human Services; MAC = Medical Advisory Committee; RDMAC = Regional Disaster Medical Advisory Committee; RMCC = Regional Medical Coordination Center; SDMAC = State Disaster Medical Advisory Committee.
SOURCE: Adapted from IOM, 2012, p. 1-44.
understand the situation of the other entities before moving to a different level of response along the continuum of care. As a disaster unfolds, the facilitation of access to additional vetted information will likely come from federal, state, tribal, and local government authorities. But this will happen only if preincident planning regarding the approach to CSC implementation has taken place. Otherwise, access to information is likely to be ad hoc and may obscure a complete assessment of the situation at hand. State and local governments are the most important entities in helping to support such planning. They serve as the conduit from agencies and health care organizations at the local level to state-level authorities, as well as from the state to their respective federal partners. Horizontal and vertical integration (within and across tiers) of the planning effort is critical to the success of CSC planning, particularly as it relates to achieving situational awareness based on preidentified indicators of the transition from conventional surge response toward contingency and crisis response. The data points being evaluated in one corner of the state, resulting in decisions taken regarding the access to potentially scarce resources and the delivery of care, should be the same as those being reviewed and acted on in other areas of the state or adjoining states. Not to do so, or to plan for such coordination, goes against one of the fundamental recommendations of the IOM CSC effort, namely, the
importance of achieving intrastate and interstate coordination (IOM, 2009). Instead of using the MSCC framework and creating another response framework, some states may have existing regional and state infrastructures for inclusive trauma/EMS advisory councils/committees; the points made above about the importance of including all response partners and ensuring horizontal and vertical integration within and across tiers apply equally regardless of the specific framework used.
In addition to responders at the state, local, health care coalition, and health care organization levels, other responders may come from federal National Disaster Medical System (NDMS) teams (ASPR, 2012b). Box 1-3 explores the role of NDMS responders, including disaster medical assistance teams.
BOX 1-3
Role of National Disaster Medical System (NDMS) Responders
Large-scale disaster incidents that require the use of federal resources, including the deployment of NDMS response teams, are likely to be the types of incidents in which the delivery of care may shift, at some point, across the conventional to contingency to crisis surge response continuum. NDMS is composed of four types of teams: Disaster Medical Assistance Team (DMAT), Disaster Mortuary Operational Response Team (DMORT), International Medical Surgical Response Team (IMSURT), and National Veterinary Response Team (NVRT). It is incumbent on federal responders, including those who comprise the NDMS response teams, to understand the context in which they are being asked to deliver health and medical services. Under disaster response conditions, it is likely that the care being delivered falls in the categories of contingency (functionally equivalent) or even crisis care. Establishing tent-based or alternate care site response capabilities in hospital parking lots, for example, can never equate to the degree of care offered in an intact health care facility. Yet, it can provide functionally equivalent care, using a no-frills approach to basic medical care delivery. Under more catastrophic conditions, where only select patient care needs can be met under such circumstances, it is likely that more sophisticated diagnostic capabilities and treatment options are simply not going to be available. Surgical services provided under “battlefield” conditions would be examples by which the federal response teams are providing care under crisis standards. Having to do so, in and of itself, is suggestive of a community-wide “indicator” that the health care infrastructure remains disrupted, save for the establishment and use of these federal resources. Diagnostic capabilities, treatment modalities, documentation of services, and even the types and levels of providers who attend to specific medical needs may all be significantly different than what would be the conventional approach to health care needs in the non-affected state.
Lessons from Hurricane Katrina and the Port au Prince Earthquake
An exploration of the ethical underpinnings related to catastrophic disaster response is an important adjunct to the preparation of health care professionals who take on the responsibilities of joining the NDMS response system. This includes understanding the criteria related to scarce resource allocation, as well as the processes by which triage decisions are taken. Deciding who gets what level of care, when not all patients can be treated equally, are some of the hard lessons learned from the response of NDMS teams to Hurricane Katrina and the Haiti earthquake (Klein et al., 2008; Merin et al., 2010). Are resources that are available to the NDMS responders adequate to meet patient needs? Would their application to few patients potentially compromise their ability to provide
Indicators and Triggers in the PHEP and HPP Capabilities and in the Overall CSC Planning Process
Both the CDC PHEP and the ASPR HPP cooperative agreements specifically call for the development of CSC plans, including indicators (ASPR, 2012a, 2013b; CDC, 2011). Completion of the tables in this toolkit will help users develop appropriate protocol and plans in accordance with the national guidance set forth in the HPP and PHEP documents. Box 1-4 outlines the primary capabilities, functions, and plans that
care for many others who might benefit more? These and related questions are also important considerations in response to complex humanitarian emergencies outside of the United States, where the existing standards of care are fundamentally different from those at home, and the medical and cultural expectations are likely to be very different. It is particularly important to recognize that response to such incidents abroad must come with a longer commitment to support the recovery and rebuilding in the affected countries (Subbarao et al., 2010).
Response teams should coordinate their efforts with the local emergency management agencies, and ensure that as federal assets, they are coordinating the application of their resources in accordance with local needs. In addition, given the dynamic nature of such incidents, it is incumbent on response teams to maintain good communications in the disaster zone, as well as back to the command and control oversight teams that accompany their deployment. Given availability of resources and patient care requirements, it is clear that decisions taken one day, for example, with respect to categorization of patients by triage category, may change. The patients categorized in the “expectant” category during the operations conducted at the New Orleans Louis Armstrong Airport shifted over time as more resources became available and patients’ conditions changed (Klein et al., 2008). Health care providers who are engaged in such missions must recognize the responsibilities that accompany these deployments, the nature of shifting conditions, and the manner by which they make these decisions, grounded in ethical considerations and the rule of law.
Response to Hurricane Sandy
In the week after the storm severely impacted the metropolitan New York and New Jersey region, causing the displacement of many hundreds of patients from hospitals and nursing homes that had to be evacuated due to rising flood waters and loss of electricity (Carcamo, 2012), the NDMS response was in full swing. Fourteen DMATS, two teams of U.S. Public Health Service commissioned corps officers, and seven Federal Medical Stations were deployed to the region. One of the Federal Medical Stations was established to serve as a medical shelter, in the attempts to keep patients from seeking care at already overburdened hospitals. The DMATs, with their caches of medical supplies and pharmaceuticals, were deployed across the metro region to provide care in established medical shelters and, in certain cases, to augment hospital staff (ASPR, 2012c). These resources allowed contingency care to be maintained in areas that otherwise might have been faced with a health care crisis situation due to the infrastructure damage.
BOX 1-4
Alignment with Public Health Preparedness and Healthcare Preparedness Capabilities
Public Health Preparedness Capabilities: National Standards for State and Local Planning (2011)
Capability 10: Medical Surge, Function 1. Assess the nature and scope of the incident
• Task 3: At the time of an incident, provide health-related data to healthcare organizations or healthcare coalitions that will assist the healthcare organizations or healthcare coalitions in activating their pre-existing plans to maximize scarce resources and prepare for any necessary shifts into and out of conventional, contingency, and crisis standards of care.
• P5: (Priority) Written plans should include processes (e.g., MOUs or other written agreements) to work in conjunction with emergency management, healthcare organizations, coalitions, and other partners to develop written strategies that clearly define the processes and indicators as to when the jurisdiction’s healthcare organizations and healthcare coalitions transition into and out of conventional, contingency, and crisis standards of care. Jurisdiction should utilize the risk assessment to build jurisdiction-specific strategies and triggers.
Other relevant capabilities:
Capability 1: Community Preparedness
Capability 3: Emergency Operations Coordination
Capability 4: Emergency Public Information and Warning
Capability 6: Information Sharing
Capability 13: Public Health Surveillance and Epidemiological Investigation
Capability 14: Responder Safety and Health
Healthcare Preparedness Capabilities: National Guidance for Healthcare System Preparedness (2012)
Capability 10: Medical Surge, Function 3: Assist healthcare organizations with surge capacity and capability
• P3. Assist healthcare organizations maximize surge capacity: The state and healthcare coalitions, in coordination with healthcare organizations, emergency management, ESF-8, relevant response partners and stakeholders, develop, refine, and sustain a plan to maximize surge capacity for medical surge incidents. This plan may include but is not limited to the following elements:
are addressed by this toolkit. However, the discussions prompted by this toolkit cover a broader set of areas, including information sharing, partnership development, systems coordination, and medical surge planning. Therefore, Box 1-4 also lists other HPP and PHEP capabilities that will be augmented through the toolkit discussions.
As described in the 2012 report, the third step in the CSC planning process should be the identification of indicators and triggers. For communities that are in the early stages of the CSC planning process, the use
o Surge Assessment:
◆ Pre-incident assessment of normal operating capacity for healthcare organizations within the healthcare delivery area
◆ Pre-incident estimate of surge casualties (i.e., medical casualties, mental/behavioral health casualties)
◆ Pre-incident assessment of available resources to address surge estimates
◆ Development of surge capacity indicators that would trigger different aspects of the medical surge plan (e.g., surge in place strategies; early discharge, cancelled elective surgeries; augmented personnel; extra shifts, volunteers; established alternate care sites or activated mobile units; requested mutual aid)
◆ Processes to immediately identify an increase in medical surge status during an incident (e.g., medical, mental/behavioral health, concerned individuals)
Capability 10: Medical Surge, Function 4: Develop crisis standards of care guidance
• Task 2: Identify the guidelines for crisis standards of care, including the effective allocation of scarce resources
• Resource Elements: Plans (P)
o P1: State crisis standards of care guidance
o P2: Indicators for crisis standards of care
o P3: Legal protections for healthcare practitioners and institutions
o P4: Provide guidance for crisis standards of care implementation processes
o P5: Provide guidance for the management of scarce resources
Other relevant capabilities:
Capability 1: Healthcare System Preparedness
Capability 3: Emergency Operations Coordination
Capability 6: Information Sharing
Hospital Preparedness Program (HPP) Measure Manual: Implementation Guidance for the HPP Program Measures (2013)
Capability Roadmap for Medical Surge
• Indicator #1: The awardee has posted its approved crisis standards of care plan on the ASPR Communities of Interest SharePoint Site.
SOURCES: ASPR, 2012a, 2013b; CDC, 2011.
of this toolkit, and the exploration of community, regional, and state-derived indicators, triggers, and the process by which actions are then taken, would be an excellent place to start this important work.
The 2012 report also highlighted the “milestones” for CSC planning. The establishment of indicators and triggers most easily fits within the fourth milestone: Developing a state health and medical approach to CSC planning that can be adopted at the regional/local level by existing health care coalitions, emergency response systems (including the Regional Disaster Medical Advisory Committee), and health care providers (IOM, 2012, p. 1-5).
This suggests that the discussion of indicators and triggers should be started relatively early in the CSC planning process, particularly as it provides much of the needed detail about what it means to transition away from conventional response and toward the delivery of health care that occurs in the contingency arena, or in worst cases, under crisis conditions.
Specialized Surge Capabilities
Pediatric and burn mass casualty incidents are presented as examples that require planning for specific surge capabilities in order to ensure the best possible patient care outcomes. (Table 1-2 outlines considerations.)
TABLE 1-2
Surge Considerations for Pediatric and Burn Care
| Pediatric | Burn | ||
| Stabilization | Pediatric equipment, including guides for weight-based equipment selection and drug dosing (liquid medications), and appropriately trained providers must be available at all emergency departments to stabilize patients, with emphasis on those <8 years of age. | Basic dressings, analgesia, fluid support, and airway management should be available at all emergency departments. Providers should be trained in initial stabilization and management of burn victims in order to avoid critical errors in resuscitation. | |
| Surge capacity | Specific spaces that are safe and appropriate for pediatric care must be identified, as well as the requisite equipment and staff with pediatric expertise necessary for appropriate care. Increased staffing ratios are required to safely care for children. Strategies for adaptation of equipment or medications in adults may not be applicable to the pediatric population. Specific support and safety issues must be addressed—a pediatric safe area, nutrition (including infant formula), psychological support, etc. Non-pediatric hospitals may have to provide inpatient care for pediatric patients during epidemic or mass casualty incidents. | Major burn patients require large amounts of intravenous fluids and narcotic analgesia. Burn unit beds are in critically short supply in the United States and in mass casualty incidents non-burn unit hospitals may have to manage burn victims for at least the first few days. Will need tiered triage to transport those most likely to benefit from care at a burn center over time. | |
| Tracking | Reunification of children with their caregivers is a critical focus of pediatric planning. Policies and processes need to be in place prior to an incident. Information on transfers must be easily shared between organizations to facilitate this process. | Information on number of victims, condition, and transfers must be easily shared among organizations to facilitate appropriate transfers and reunification, especially when regional transfers are required. | |
| Coordination | Incident demand must be balanced across coalition facilities that provide (or can provide) pediatric care and other networks of children’s hospitals. Pediatric subject matter experts or pediatric health care coalitions should be integrated into the transfer framework to provide input on appropriate destinations and use of available beds for specific patients. | Incident demand must be balanced across coalition facilities that provide (or can provide) burn care and burn center networks. Subject matter experts should be integrated into the transfer framework to provide input on appropriate destinations and use of available beds for specific patients so debridement and interventions can be appropriately timed. | |
| Consultation | Must be available for hospitals that have to manage pediatric patients that do not normally do so. Telemedicine, telephone, and other methods of consultation are imperative, and these may need to be set up with national pediatric centers or with pediatric health care coalitions if the local/regional centers of expertise are too overwhelmed to provide such support. | Must be available for hospitals that have to manage burn patients that do not normally do so. Telemedicine, telephone, and other methods of consultation are imperative—and these may need to be set up with national burn centers if the local/regional centers of expertise are too overwhelmed to provide such support. | |
| Transportation | Pediatric patients may have specific transport needs (bassinets, car seats, other safety restraints, appropriate pediatric-sized equipment for en-route care, e.g., IV pumps). | Burn patients need to be protected against hypothermia during transport, and adequate analgesia, fluids, and airway equipment are required for safe transfer. | |
In each case—managing pediatric patients or managing burn patients—specific resources, including knowledgeable and experienced health care providers, may not be readily available to provide care. However, planning for common approaches to regional training and response frameworks may be used to meet the needs of very different incidents (for additional consideration, see, for example, Appendix D in IOM, 2012, which outlines resource challenges by disaster type, and NCIPC, 2007, which discusses surge capacity for a terrorist bombing).
Resource shortages associated with specialized capabilities, such as pediatric and burn care, are more likely to occur in a non-catastrophic incident. Higher tiers in the MSCC framework may have to be activated for lower numbers of victims, compared to nonspecialized capabilities (Barbera and Macintyre, 2007, 2009). These types of examples may, therefore, provide insight into how care changes and how transitions across the continuum of care should be considered, as every health care facility must plan to initially receive these types of patients (see AAP et al., 2009, and Kearns, 2011).
IMPLEMENTATION OF THE DISASTER RESPONSE FRAMEWORK
The 2012 report outlines a process for decision making during a disaster, providing a systems approach to help health care organizations determine whether health care delivery can remain at the conventional level, or whether contingency and/or crisis care should be implemented (see Figure 1-4). The “planning A” cycle is based on the well-honed concept used as part of an emergency management system known as the “planning P” (FEMA, 2008a). This is a combination of management by objectives that relies on the development of specific strategies and the tactics needed to support those strategies, with a time phase element included to ensure that progress and improvements in the response to any given incident are being noted, and when they are not, allows for midcourse adjustments and a shift in strategies and tactics. This would occur within the context of an incident command system that is compatible with the National Incident Management System (NIMS), such as the Hospital Incident Command System (HICS) (EMSA, 2007; FEMA, 2013).
This graphical depiction highlights the dynamic qualities of any given incident, regardless of whether it is one that develops slowly over time, or a sudden onset, no-notice incident. The transition from conventional to contingency response occurs with the crossing of the resource shortage threshold. A shortage in any given resource—both material and personnel items (supplies, equipment, pharmaceuticals) and humans (health care providers)—may result in this threshold being crossed. At this point, strategies and tactics can be employed to attempt to move back toward the delivery of care under conventional conditions. These strategies include conservation, substitution, adaptation, and even reuse of certain resources.9
At some point, however, with severe and sustained shortages of key resources, the ability to deliver medical care services under contingency conditions will be compromised. The goal should be for these adaptations to move care back toward conventional. However, if the situation worsens, extension of these adaptive strategies may be required. At this point, the strategies of conservation, substitution, adaptation, and reuse of resources are extended to the point that they no longer ensure functionally equivalent care.
____________________
9 A recent comparative effectiveness review of strategies for managing and allocating resources during mass casualty incidents categorizes strategies as follows: reduce or manage less urgent demand for health care services, optimize use of existing resources, augment existing resources, and crisis standards of care (Timbie et al., 2012, 2013).
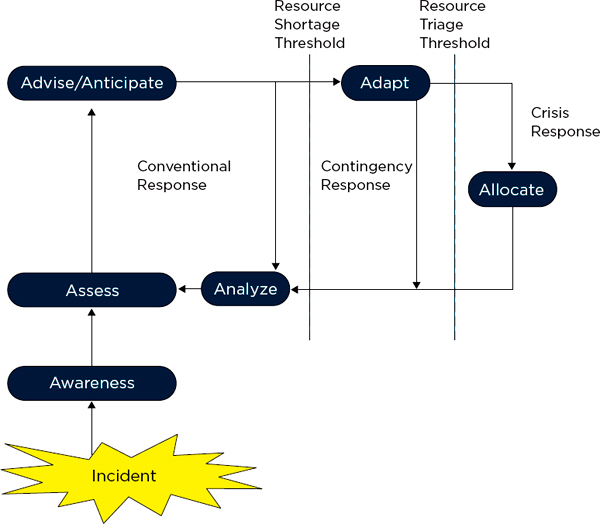
FIGURE 1-4
Implementation of the Surge Response Framework: Conventional, contingency, and crisis response cycle.
After an incident occurs, the first priority is to develop situational Awareness, and then to Assess the situation relative to the available resources. The incident commander, along with relevant technical experts and/or the clinical care committee (in a proactive response/longer-term incident) Advises on strategies and Anticipates any resource deficits (and recommends obtaining necessary supplies, staffing, etc.). If a resource is scarce, Adaptive strategies (e.g., conservation, substitution, adaptation, and reuse) should be implemented. In a crisis, a deliberate triage decision to Allocate/reallocate resources may be necessary. In all cases, the response and any strategies should be Analyzed at regular intervals as part of the disaster response planning cycle, and the elements repeated until the incident concludes.
SOURCE: IOM, 2012, p. 1-48.
Supplies, space, and staff have to be employed in a way that presents a risk of a compromised outcome to the patient. Thus, contingency and crisis care may coexist in this area depending on the degree to which the strategies are extended.
Lack of specific treatment resources may require that a health care organization also cross the resource triage threshold. Under these conditions, there are not enough resources available relative to the demand for care, and key resources must be triaged for patients. Reallocation of scarce resources will be needed, based on population-based values (derived from community engagement inputs) and population-based outcomes (based on what limited evidence base may be available to support such decisions) and is inherently located in the crisis portion of the continuum.
In general the space before reaching a resource shortage threshold corresponds to conventional care, the space after crossing that threshold but before reaching the resource triage threshold corresponds to contingency care, and the space after crossing the resource triage threshold corresponds to crisis care. However, the discus-
sion above makes clear that there are gray areas in the resource shortage space, where a combination of contingency and crisis care may be delivered depending on the resources that are scarce and the strategies that are being implemented. For example, depending on the resource that is being reused, the care may be considered functionally equivalent or it may present a risk to patient outcomes. The extent to which staff members are practicing within or beyond their usual or comfortable scope of practice and supervision is another example.
This indicators and triggers toolkit is intended to expand on the concepts described above, including issues such as sources of indicator information, types of triggers and decision making, and what information planners and decision makers can use to make these determinations. These questions are particularly challenging given the dynamic conditions during such incidents, the number of resources and other variables involved in providing care, and the many different potential resource shortages that could occur during the response.
THE NEED TO DEVELOP INDICATORS AND TRIGGERS
The need for the development of indicators and triggers for crisis standards of care has been discussed in a number of studies and reports throughout the past 5 years (Devereaux et al., 2008; IOM, 2009, 2012; Joynt et al., 2010). Recommendations to define and incorporate clear indicators and triggers into preparedness protocols were highlighted in the two IOM reports (IOM, 2009, 2012). Developing indicators and triggers at all levels of the emergency response system, as outlined in Figure 1-2, will help ensure consistency in the implementation of CSC. The identification of specific measurements and predictors throughout the planning process is critical to determining appropriate actions and decision making. In addition, the development and use of indicators and triggers can help support responders’ behavioral health and resilience.
Individuals involved in disaster response should understand what sources of information are available to inform decision making, what authorities they have, and what the plan is for pulling the trigger—who will do it, how, and when. This type of planning needs to be done in advance to allow the necessary dialogue about sources of information, integration, authorities, and processes.
Experience, training, information sharing, and data interpretation are key factors that influence decision making during crises, particularly given the impact of stress, complexity, uncertainty, and time pressure associated with such situations (see Box 1-5). The careful monitoring of indicators is likely an important determinant of successful incident response. As noted by Alberts (2007, p. 19), “focus represents a synthesis of how [a] situation is perceived and understood, including perceptions about the nature of the endeavor (strategies and plans) that are appropriate for the situation.” In the context of crisis response, there should be a focus on the indicators that are used to determine that a transition in care is occurring across the surge continuum. Leaders and decision makers involved in having to make scarce resource allocation decisions require reliable, authenticated, predictive, and actionable data on which they will make important choices during a crisis incident. The development of indicators and triggers can also provide a standard operating procedure for line employees to rely on, although this is only appropriate for certain types of information and decisions, as will be discussed in Chapter 2.
Box 1-6 discusses issues related to the decision to evacuate health care facilities or shelter in place. This decision illustrates the difficulty of decisions made during disasters and the importance of advance planning.
BOX 1-5
Decision Making in Crises
Making reasoned decisions in a stressful situation is one of the most important skills for a first responder. This is true for those in leadership roles such as the incident commander, those managing the National Incident Management System (NIMS) designed response hierarchy support functions, field-based uniformed-services first responders, health professionals, and nontraditional emergency responders. Facing unique and dynamic situational environments and the psychological pressure of adapting well-practiced work routines into novel response sets is very challenging. The adverse impact of personal stress on decision making is well documented.
The literature on decision making associated with crisis situations consistently identifies stress and fatigue as contributing factors having a detrimental effect on the decision-making process (Brecher, 1979; Helmreich and Merritt, 1998; Rosenthal and t’Hart, 1991). Stress primarily has been shown to negatively affect decision making (Keinan, 1987; Kowalski-Trakofler and Vaught, 2003; Staal, 2004). In particular, people consider fewer alternatives and options, rely on prior decisions made in similar situations (even when ineffective), and have the potential to reach an overall state of attentional disorganization. Similar findings were also seen when decisions had to be made within pressing time constraints (Zakay, 1993). In addition, uncertainty and lack of information can lead to misguided and suboptimal decision making (Bell, 1982; Hansson, 1996; Sarter and Schroeder, 2001).
As an incident progresses, the quality of decision making at all leadership and responder levels is threatened. Renaud (2012) recently suggested a straightforward cognitive approach for thinking through chaotic situations before deciding on an action. She suggests a cognitive strategy for accessing the situational demands of the incident, comparing the current event to past experience, identifying what one needs to know, what one does not know, and ultimately what one wants, and can and must do. All of this should occur within the context of the assigned mission goals of what must be accomplished. This process helps keep decision making relevant to the current incident, and decision makers from rushing too quickly to judgment and action based on excessive reliance on past experience.
Extreme events (catastrophic) and adaptive decision making also involves monitoring of the response environment and the changing capabilities of responders to competently carry out their duties over time. Other data (Burkle and Hayden, 2001) on emergency response decision making indicate that decision making in isolation is not effective in
managing unique and rapidly changing large-scale disaster events. Abandoning vertical or stovepipe organizational models for lateral management models improves communication and data acquisition necessary for dynamic decision making. Decision-making capabilities during a large-scale incident are enhanced though preplanning strategies, practicing response plans, and building a response framework that recognizes threats to responder health and sustained response capabilities by integrating responder physical and psychological health care strategies into response protocols (HHS, 2005).
Crew resource management (CRM) training, principles of human factors, and the use of checklists are also valuable resources to potentially enhance decision making in disasters. CRM was developed as a training resource to decrease error through the use of behavioral countermeasures that address human factors that can lead to error. Recognizing the influence of stress, fatigue, and other situational and individual factors on cognitive processes (WHO, 2009), CRM is not meant to eliminate human error, but rather to encourage appropriate error management and safety (Helmreich et al., 1999). Strategies to promote teamwork, communication, situational awareness, interpersonal skills, leadership, and decision making are addressed in this predominantly simulation-based training (Flin et al., 2002). The use of checklists has also been discussed in great detail, particularly in aviation and more recently in the medical context, as a means to inform and guide decision making. Checklists, when used properly, can manage error, reduce risk, increase patient safety, and serve as quality control (Walker et al., 2012; Winters et al., 2009). However, each of these resources has limitations that must be considered. Findings from several studies revealed predominantly positive results regarding the effectiveness of CRM on attitudes, reactions, and learning, yet mixed results on behavior (O’Connor et al., 2008; Salas et al., 2006). Although checklists have been found to be beneficial tools, it is important to note that they must be considered within the context of the overall system; the environment, technology, and human error can ultimately influence outcomes (Degani and Wiener, 1993; Mauro et al., 2012). Therefore, it is particularly important for decision makers to consider additional approaches and strategies based on the situation at hand.
Key points: Stress adversely impacts decision making at all levels; there are strategies that can help enhance decision making; planning and practicing facilitates better decisions as long as this does not cause decision makers to reduce the ability to consider novel and innovative approaches.
BOX 1-6
Making the Decision: Evacuation Versus Shelter in Place
Given the complexities involved in conducting partial and full-scale health care facility evacuations, particularly under the duress of an emergency incident, both the decision taken “to stay” and the calculus applied “to go” is fraught with risk. Choosing to move patients and staff ahead of an impending storm can be a very difficult maneuver to execute, may result in increased morbidity and mortality to patients, and introduces a heightened risk associated with the movement of patients, whether by air or ground transportation. In 2005, 23 nursing home patients were killed in a bus fire after being evacuated from a facility in Houston in preparation for the arrival of Hurricane Rita (NTSB, 2007). When it arrived, Houston was spared the brunt of the storm’s effects. On the other hand, choosing to shelter patients and staff in place, to hunker down and let the storm pass or conditions stabilize, may be equally risky, as evidenced most recently by the infrastructure failures in two lower Manhattan hospitals during Hurricane Sandy, prompting spontaneous decisions to evacuate at the height of the storm, and soon thereafter (Fink, 2012). It could be said, then, that the decisions taken around whether to evacuate versus sheltering in place can amount to no better than a Pyrrhic victory.
The decision-making process to either shelter in place or evacuate a health care facility in response to a disaster incident, both sudden onset (earthquake) and anticipated (hurricane), requires assessing a number of interrelated variables and determining the risk related to each one taken independently, and then together (Downey et al., 2013a,b; Sexton et al., 2007; Sternberg et al., 2004; Zaenger et al., 2010):
• Impact: How much time is available to make a decision? How severe is the storm expected to be? What is its projected path? Will critical utilities or access to the facility likely be compromised? If a decision to evacuate is deferred, will a later decision to evacuate carry an increased safety risk?
• Infrastructure: Does the health care facility have specific vulnerabilities related to infrastructure support and storm resiliency? Are there sufficient staffing and resources to support extended operations under duress? Are alternate locations available to send patients? Are means available to get patients out of harm’s way, if necessary? Are there any plans by the utilities to cut power or gas supply to the impacted area after the storm to prevent injury and fires?
• Incident specific: Preparedness efforts must take into account the known variables, as well as the rapid assessment and integration of event-specific variables that develop during the incident, and must be flexible enough to be able to adapt to changing circumstances. These may include the ability of emergency medical services (EMS) to support evacuation operations, and other community and facility factors. Radiation and the presence of hazardous materials also impacts decision making.
In July 2006, the Government Accountability Office report on this issue found that hospitals and nursing home facility administrative leaders noted that they considered evacuation a decision of “last resort,” and that their emergency plans were primarily designed to shelter in place (GAO, 2006). Moreover, it highlighted the issue that despite some jurisdictional calls for “mandatory evacuation,” some health care organizations may not be capable of complying with the requested actions given the lack of suitable transportation and the staff to accompany patients. At the same time, few hospitals would choose to evacuate on their own, without a formal governmental recommendation/order to do so due to the anticipated impact on business operations (Schultz et al., 2003). Making matters worse, the loss of communications infrastructure can significantly impede decision making in real time, as conditions change and a stay-or-go decision must
be made. Despite health care organization accreditation processes that include written plans for evacuation, this is a skill that is rarely, if ever, tested given the logistical challenges faced with doing so, and the exorbitant expense that would be incurred to take on a full-scale exercise (see Femino et al., 2013; Jen et al., 2009).
Once a commitment is made to evacuate, immediate follow-on decisions are required (Zane et al., 2010):
• Is the evacuation to be partial or complete? Plans must be made to ensure the scalability of these efforts, recognizing that conditions resulting in the movement of some patients may ultimately require the evacuation of all patients. A subset of high-technology dependent patients (e.g., ventilator dependent, intra-aortic balloon pump) may be at such elevated risk from a move that unless the facility clearly cannot continue operations, a shelter-in-place strategy may be most appropriate for them.
• If a partial evacuation is warranted, should remaining patients be moved to more accessible areas of the hospital, in order to facilitate their rapid evacuation, should the necessity arise based on changing conditions?
• Are the most critically ill, resource-dependent patients triaged to be moved first, or are they the last to be moved?
• In the absence of specialized equipment used to help facilitate the evacuation of patients, can an evacuation plan still be carried out?
• How are destination hospitals selected and how is acceptance of patients arranged?
• What staging areas and evacuation process will be used (designated stairwells vs. elevators, mechanisms of movement, etc.)?
• What paperwork/chart information will be sent with the patients?
• What transportation resources are available, and in what time frame? Will they continue to be available as the event continues/progresses?
Many of these secondary decisions can be managed in stepwise fashion, but in all cases, the decision makers will have to convey expectations to the patient units (except in the case of a catastrophic impact on the facility when each unit must recognize the immediate safety risk and proceed with relocation of patients to a safe area). Staff, patients, and, whenever appropriate, patient families must be kept apprised of the choices contemplated and selected.
The decision to evacuate is not an easy one. By necessity, health care facility evacuations force the adoption of a change in the delivery of health care services along the continuum of care from conventional to contingency to crisis response. The implications of such incidents are not simply focused on the facilities that have to evacuate, but also greatly impact those facilities that receive patient evacuees. It also has a big impact on the surrounding community, as patients often look to hospitals as safe havens and continue to seek medical treatment and care. Moreover, the decision to evacuate a health care facility will always be made with less than the full array of information desired by decision makers. Although never prominently discussed, fiduciary concerns related to the decision to “close the doors” can also figure prominently in the process.
As has been often noted of military decision making under stress, leaders must be careful not to end up fighting the “last war” by using strategies and tools with which they are familiar, but are inappropriate for the current situation. In the case of Hurricane Sandy, the mandatory evacuations ordered the year before for a storm surge that never arrived with Hurricane Irene may have been enough to impart a sense of confidence among health care organization leadership and the belief that all would be fine—a mistake that could have been much more costly. Deciding whether “to stay or go” is not an easy decision to make.
AAP (American Academy of Pediatrics), ACEP (American College of Emergency Physicians), and ENA (Emergency Nurses Association). 2009. Joint policy statement—guidelines for care of children in the emergency department. Pediatrics 124(4):1233-1243. http://aappolicy.aappublications.org/cgi/reprint/pediatrics;124/4/1233.pdf (accessed April 3, 2013).
AHRQ (Agency for Healthcare Research and Quality). 2005. Altered standards of care in mass casualty events: Bioterrorism and other public health emergencies. Rockville, MD: AHRQ. http://archive.ahrq.gov/research/altstand/altstand.pdf (accessed March 11, 2013).
Alberts, D. S. 2007. Agility, focus, and convergence: The future of command and control. The International C2 Journal 1(1):1-30.
ASPR (Assistant Secretary for Preparedness and Response). 2012a. Healthcare preparedness capabilities: National guidance for healthcare system preparedness. Washington, DC: Department of Health and Human Services. http://www.phe.gov/preparedness/planning/hpp/pages/default.aspx (accessed March 29, 2013).
ASPR. 2012b. National Disaster Medical System. Washington, DC: Department of Health and Human Services. http://www.phe.gov/preparedness/responders/ndms/Pages/default.aspx (accessed April 3, 2013).
ASPR. 2012c. Hurricane Sandy—Public health situation updates. Washington, DC: Department of Health and Human Services. http://www.phe.gov/newsroom/Pages/situpdates.aspx (accessed March 11, 2013).
ASPR. 2013a. Public health emergency medical countermeasures enterprise. Washington, DC: Department of Health and Human Services. https://www.phe.gov/Preparedness/mcm/phemce/Pages/default.aspx (accessed March 11, 2013).
ASPR. 2013b. Hospital Preparedness Program (HPP) measure manual: Implementation guidance for the HPP program measures. Washington, DC: Department of Health and Human Services. http://www.phe.gov/Preparedness/planning/evaluation/Documents/hpp-bp2-measuresguide-2013.pdf (accessed June 17, 2013).
Barbera, J. A., and A. G. MacIntyre. 2007. Medical surge capacity and capability: A management system for integrating medical and health resources during large-scale emergencies, 2nd ed. Washington, DC: Department of Health and Human Services. http://www.phe.gov/preparedness/planning/mscc/handbook/documents/mscc080626.pdf (accessed April 3, 2013).
Barbera, J. A., and A. G. MacIntyre. 2009. Medical surge capacity and capability: The healthcare coalition in emergency response and recovery. Washington, DC: Department of Health and Human Services. http://www.phe.gov/preparedness/planning/mscc/documents/mscctier2jan2010.pdf (accessed May 14, 2013).
Bell, D. E. 1982. Regret in decision making under uncertainty. Operations Research 30(5):961-981.
Brecher, M. 1979. State behavior in international crisis. Journal of Conflict Resolution 23(3):446-480.
Burkle, F. M., Jr., and R. Hayden. 2001. The concept of assisted management of large-scale disasters by horizontal organizations. Prehospital Disaster Medicine 16(3):87-96.
Carcamo, C. 2012. Storm forces evacuation of hundreds of New York hospital patients. Los Angeles Times, October 30. http://articles.latimes.com/2012/oct/30/nation/la-na-nn-hurricane-sandy-hospital-evacuations-20121030 (accessed April 16, 2013).
CDC (Centers for Disease Control and Prevention). 2011. Public health preparedness capabilities: National standards for state and local planning. Atlanta, GA: CDC. http://www.cdc.gov/phpr/capabilities (accessed March 29, 2013).
Cibulsky, S. M., and M. A. Kirk. 2010. Summary: Symposium on chemical decontamination of humans, final report. Washington, DC: Department of Homeland Security. http://www.phe.gov/Preparedness/mcm/Documents/summary-chemdecon-20June12.pdf (accessed March 11, 2013).
Degani, A., and E. L. Wiener. 1993. Cockpit checklists: Concepts, design, and use. Human Factors 35(2):28-43.
Devereaux, A. V., J. R. Dichter, M. D. Christian, N. N. Dubler, C. E. Sandrock, J. L. Hick, T. Powell, J. A. Geiling, D. E. Amundson, T. E. Baudendistel, D. A. Braner, M. A. Klein, K. A. Berkowitz, J. R. Curtis, and L. Rubinson. 2008. Definitive care for the critically ill during a disaster: A framework for allocation of scarce resources in mass critical care. From a Task Force for Mass Critical Care summit meeting, January 26-27, 2007, Chicago, IL. Chest 133(Suppl 5):S51-S66.
DHS (Department of Homeland Security). 2011. Homeland Security Advisory Council: Community Resilience Taskforce recommendations. Washington, DC: DHS. http://www.dhs.gov/xlibrary/assets/hsac-community-resilience-task-force-recommendations-072011.pdf (accessed May 3, 2013).
Downey, E. L., K. Andress, and C. H. Schultz. 2013a. Initial management of hospital evacuations caused by Hurricane Rita: A systematic investigation. Prehospital and Disaster Medicine 28(3):257-263.
Downey, E. L., K. Andress, and C. H. Schultz. 2013b. External factors impacting hospital evacuation caused by Hurricane Rita: The role of situational awareness. Prehospital and Disaster Medicine 28(3):264-271.
EMSA (California Emergency Medical Services Authority). 2007. Disaster Medical Services Division—Hospital Incident Command System (HICS). http://www.emsa.ca.gov/hics (accessed March 11, 2013).
FEMA (Federal Emergency Management Agency). 2008a. Incident command system training: Review material. Washington, DC: FEMA. http://training.fema.gov/EMIWeb/IS/ICSResource/assets/reviewMaterials.pdf (accessed March 11, 2013).
FEMA. 2008b. Emergency support function annexes: Introduction. Washington, DC: FEMA. http://www.fema.gov/pdf/emergency/nrf/nrf-esf-intro.pdf (accessed April 3, 2013).
FEMA. 2010. Developing and maintaining emergency operations plans: Comprehensive preparedness guide (CPG) 101, Version 2.0. Washington, DC: FEMA. http://www.fema.gov/pdf/about/divisions/npd/CPG_101_V2.pdf (accessed May 14, 2013).
FEMA. 2011. A whole community approach to emergency management principles, themes, and pathways for action. FDOC 104-008-1. Washington, DC: FEMA. http://www.fema.gov/library/viewRecord.do?id=4941 (accessed March 11, 2013).
FEMA. 2013. National Incident Management System (NIMS). Washington, DC: FEMA. http://www.fema.gov/emergency/nims (accessed March 11, 2013).
Femino, M., S. Young, and V. C. Smith. 2013. Hospital-based emergency preparedness: Evacuation of the neonatal intensive care unit—the smallest and most vulnerable population. Pediatric Emergency Care 29(1):107-113.
Fink, S. 2012. In hurricane’s wake, decisions not to evacuate hospitals raise questions. http://www.propublica.org/article/in-hurricanes-wake-decisions-not-to-evacuate-hospitals-raise-questions (accessed April 3, 2013).
Flin, R., P. O’Connor, and K. Mearns. 2002. Crew resource management: Improving team work in high reliability industries. Team Performance Management 8(3-4):68-78.
GAO (Government Accountability Office). 2006. Disaster preparedness: Limitations in federal evacuation assistance for health facilities should be addressed. GAO-06-826. Washington, DC: GAO. http://www.gao.gov/new.items/d06826.pdf (accessed April 3, 2013).
GAO. 2008. States are planning for medical surge, but could benefit from shared guidance for allocating scarce medical resources. GAO-08-668. Washington, DC: GAO. http://www.gao.gov/new.items/d08668.pdf (accessed March 11, 2013).
Hansson, S. O. 1996. Decision making under great uncertainty. Philosophy of the Social Sciences 26(3):369-386.
Helmreich, R. L., and A. C. Merritt. 1998. Culture at work: National, organisational and professional influences. Aldershot, Hampshire, England: Ashgate.
Helmreich, R. L., A. C. Merritt, and J. A. Wilhelm. 1999. The evolution of crew resource management training in commercial aviation. International Journal of Aviation Psychology 9(1):19-32.
HHS (Department of Health and Human Services). 2005. Pandemic Influenza Plan Supplement 11. www.hhs.gov/pandemic flu/plan/pdf/S11.pdf (accessed April 8, 2013).
Hick, J. L., J. A. Barbera, and G. D. Kelen. 2009. Refining surge capacity: Conventional, contingency, and crisis capacity. Disaster Medicine and Public Health Preparedness 3(Suppl 2):S59-S67.
IOM (Institute of Medicine). 2009. Guidance for establishing crisis standards of care for use in disaster situations: A letter report. Washington, DC: The National Academies Press. http://www.nap.edu/catalog.php?record_id=12749 (accessed April 3, 2013).
IOM. 2010. Crisis standards of care: Summary of a workshop series. Washington, DC: The National Academies Press. http://www.nap.edu/catalog.php?record_id=12787 (accessed April 3, 2013).
IOM. 2012. Crisis standards of care: A systems framework for catastrophic disaster response. Washington, DC: The National Academies Press. http://www.nap.edu/openbook.php?record_id=13351 (accessed April 3, 2013).
Jen, H. C., S. B. Shew, J. B. Atkinson, J. T. Rosenthal, and J. R. Hiatt. 2009. Creation of inpatient capacity during a major hospital relocation: Lessons for disaster planning. Archives of Surgery 144(9):859-864.
Joynt, G. M., S. Loo, B. L. Taylor, G. Margalit, M. D. Christian, C. Sandrock, M. Danis, Y. Leoniv, and C. L. Sprung. 2010. Coordination and collaboration with interface units. Journal of Intensive Care Medicine 36(Suppl 1):S21-S31.
Kearns, R. D. 2011. Burn surge capacity in the south: What is the capacity of burn centers within the American Burn Association southern region to absorb significant numbers of burn injured patients during a medical disaster? Medical University of South Carolina: ProQuest Dissertations and Theses.
Keinan, G. 1987. Decision making under stress: Scanning of alternatives under controllable and uncontrollable threats. Journal of Personality and Social Psychology 52(3):639-644.
Klein, K. R., P. E. Pepe, F. M. Burkle, N. E. Nagel, and R. E. Swienton. 2008. Evolving need for alternative triage management in public health emergencies: A Hurricane Katrina case study. Disaster Medicine and Public Health Medicine 2(Suppl 1):S40-S44.
Kowalski-Trakofler, K. M., and C. Vaught. 2003. Judgment and decision making under stress: An overview for emergency managers. International Journal of Emergency Management 1(3):278-289.
Mauro, R., A. Degani, L. Loukopoulos, and I. Barshi. 2012. The operational context of procedures and checklists in commercial aviation. Proceedings of the Human Factors and Ergonomics Society Annual Meeting 56(1):758-762.
Merin, O., N. Ash, G. Levy, M. J. Schwaber, and Y. Kriess. 2010. The Israeli field hospital in Haiti: Ethical dilemmas in early disaster response. New England Journal of Medicine 362(11):e38.
NCIPC (National Center for Injury Prevention and Control). 2007. In a moment’s notice: Surge capacity for terrorist bombings. Atlanta, GA: CDC. http://emergency.cdc.gov/masscasualties/pdf/surgecapacity.pdf (accessed June 5, 2013).
NTSB (National Transportation Safety Board). 2007. Motorcoach fire on Interstate 45 during Hurricane Rita evacuation near Wilmar, Texas, September 23, 2005. Highway Accident Report NTSB/HAR-07/01. Washington, DC: NTSB. http://www.ntsb.gov/doclib/reports/2007/HAR0701.pdf (accessed April 12, 2012).
O’Connor, P., J. Campbell, J. Newon, J. Melton, E. Salas, and K. Wilson. 2008. Crew resource management training effectiveness: A meta-analysis and some critical needs. International Journal of Aviation Psychology 18(4):353-368.
Ohio Hospital Association and Ohio Department of Health. 2011. Ohio medical coordination plan. Columbus: Ohio Hospital Association and Ohio Department of Health.
ORISE (Oak Ridge Institute for Science and Education). 2013a. Public health discussion guide for pandemic influenza planning. http://www.cdc.gov/phpr/healthcare/documents/Discussion_Guide_for_Public_Health.pdf (accessed May 15, 2013).
ORISE. 2013b. Hospital discussion guide for pandemic influenza planning. http://www.cdc.gov/phpr/healthcare/documents/Discussion_Guide_for_Hospitals.pdf (accessed May 15, 2013).
ORISE. 2013c. Emergency management discussion guide for pandemic influenza planning. http://www.cdc.gov/phpr/healthcare/documents/Discussion_Guide_for_Emergency_Management.pdf (accessed May 15, 2013).
Phillips, S. J., and A. Knebel, eds. 2007. Mass medical care with scarce resources: A community planning guide. Rockville, MD: AHRQ. http://archive.ahrq.gov/research/mce/mceguide.pdf (accessed June 10, 2013).
Powell, T., K. C. Christ, and G. S. Birkhead. 2008. Allocation of ventilators in a public health disaster. Disaster Medicine and Public Health Preparedness 2(1):20-26.
Renaud, C. 2012. The missing piece of NIMS: Teaching incident commanders how to function in the edge of chaos. Homeland Security Affairs Article 8. http://www.hsaj.org/?article=8.1.8 (accessed April 22, 2013).
Rosenthal, U., and P. t’Hart. 1991. Experts and decision makers in crisis situations. Knowledge: Creation, Diffusion, Utilization 12(4):350-372.
Salas, E., K. A. Wilson, C. S. Burke, and D. C. Wightman. 2006. Does crew resource management training work? An update, an extension, and some critical needs. Human Factors 48(2):392-412.
Sarter, N. B., and B. Schroeder. 2001. Supporting decision making and action selection under time pressure and uncertainty: The case of in-flight icing. Human Factors 43(4):573-583.
Schultz, C. H., K. L. Koenig, and R. J. Lewis. 2003. Implications of hospital evacuation after the Northridge, California, earthquake. New England Journal of Medicine 348(14):1349-1355.
Sexton, K. H., L. M. Alperin, and J. D. Stobo. 2007. Lessons from Hurricane Rita: The University of Texas Medical Branch Hospital’s evacuation. Academic Medicine 82(8):792-796.
Staal, M. A. 2004. Stress, cognition, and human performance: A literature review and conceptual framework. Hanover, MD: National Aeronautics and Space Administration. http://human-factors.arc.nasa.gov/flightcognition/Publications/IH_054_Staal.pdf (accessed February 11, 2013).
State of Michigan. 2013. Michigan Emergency Department Syndromic Surveillance System. Lansing, MI: Department of Community Health. http://www.michigan.gov/mdch/0,4612,7-132-2945_5104_31274-107091--,00.html (accessed April 12, 2013).
Sternberg, E., G. C. Lee, and D. Huard. 2004. Counting crises: US hospital evacuations, 1971-1999. Prehospital Disaster Medicine 19(2):150-157.
Subbarao, I., M. K. Wynia, and F. M. Burkle. 2010. The elephant in the room: Collaboration and competition among relief organizations during high-profile disasters. Journal of Clinical Ethics 21(4):328-334.
Timbie, J. W., J. S. Ringel, D. S. Fox, D. A. Waxman, F. Pillemer, C. Carey, M. Moore, V. Karir, T. J. Johnson, N. Iyer, J. Hu, R. Shanman, J. W. Larkin, M. Timmer, A. Motala, T. R. Perry, S. Newberry, and A. L. Kellermann. 2012. Allocation of scarce resources during mass casualty events. Rockville, MD: AHRQ. http://www.ncbi.nlm.nih.gov/books/NBK98854/pdf/TOC.pdf (accessed June 6, 2013).
Timbie, J. W., J. S. Ringel, D. S. Fox, F. Pillemer, D. A. Waxman, M. Moore, C. K. Hansen, A. R. Knebel, R. Riccardi, and A. L. Kellermann. 2013. Systematic review of strategies to manage and allocate scarce resources during mass casualty events. Annals of Emergency Medicine 61(6):677-689.
Walker, I. A., S. Reshamwalla, and I. H. Wilson. 2012. Surgical safety checklists: Do they improve outcomes? British Journal of Anesthesia 109(1):47-54.
Winters, B. D., A. P. Gurses, H. Lehmann, J. B. Sexton, C. J. Rampersad, and P. J. Pronovost. 2009. Clinical review: Checklists—translating evidence into practice. Critical Care 13(6):210-219.
WHO (World Health Organization). 2009. Human factors in patient safety: Review of topics and tools. Geneva, Switzerland: WHO. http://www.who.int/patientsafety/research/methods_measures/human_factors/human_factors_review.pdf (accessed May 20, 2013).
Zaenger, D., N. Efrat, R. R. Riccio, and K. Sanders. 2010. Shelter-in-place versus evacuation decision making: A systematic approach for healthcare facilities. Risk, Hazards & Crisis in Public Policy 1(3):19-33.
Zakay, D. 1993. The impact of time perception processes on decision making under time stress. In Time pressure and stress in human judgment and decision making, edited by O. Svenson and J. Maule. New York: Plenum. Pp. 59-72.
Zane, R., P. Biddinger, A. Hassol, T. Rich, J. Gerber, and J. DeAngelis. 2010. Hospital evacuation decision guide. Rockville, MD: AHRQ. http://archive.ahrq.gov/prep/hospevacguide (accessed April 3, 2013).






























