
3
Concussion Recognition, Diagnosis, and Acute Management
One of the first challenges in responding to sports-related concussions is to recognize that a player may have sustained a concussion and therefore should be removed from the activity for further evaluation. As discussed in Chapter 1, although previous generations of athletes were encouraged to “shake it off” and return to play, current guidelines (Halstead et al., 2010; Harmon et al., 2013; McCrory et al., 2013b) and most state laws (NCSL, 2013) require athletes to be removed from competition or practice if a concussion is suspected so that a more formal evaluation can be completed. In this chapter, the committee responds to the portions of its charge concerning cognitive, affective, and behavioral changes that can occur during the acute phase of concussion; hospital- and non-hospital-based diagnostic tools; and the treatment and management of sports concussion. The chapter provides an overview of concussion screening and diagnosis, including sideline assessments at the time of injury, subsequent clinical evaluation, and the use of evaluation tools such as symptom checklists, and neuropsychological testing. The chapter also reviews the signs and symptoms of concussions and various considerations pertaining to the acute management of concussion, including the reintegration of concussed individuals into academic and athletic activities.
The assessment of an injured player is facilitated by the presence of a certified athletic trainer, team physician, or other health care provider at the venue (e.g., field, gymnasium, or rink) where the injury occurred. How-
ever, the vast majority of young athletes practice and play in circumstances where trained personnel are not routinely available to make sideline injury assessments, and the responsibility for determining whether to remove an athlete from play falls on coaches, parents, players, and, perhaps, officials. A further impediment to identification is that symptoms may not become apparent for several hours after injury, and one result of this is that a large number of concussions are not identified until 24 hours or more after the injury (Duhaime et al., 2012; McCrory et al., 2013b). The Centers for Disease Control and Prevention (CDC) Heads Up campaign is designed to educate coaches, parents, and athletes about the prevention and recognition of and response to concussions (CDC, 2012a). A central feature of the campaign is the dissemination of information about the signs and symptoms of concussion (see Table 3-1) along with the message that players suspected of having sustained a concussion should be removed from play for the remainder of the day, referred to a health care provider for evaluation, and not permitted to return to play until they have been cleared by a health professional trained in concussion diagnosis and management (CDC, 2012a).
The sideline evaluation of a player’s symptoms may be complicated by the tendency of athletes to underreport their symptoms (Anderson et al., 2013; Dziemianowicz et al., 2012; McCrea et al., 2004). A 2004 study
TABLE 3-1 Signs and Symptoms of Concussions Relevant to Sideline Assessment
| Signs Observed | Symptoms Reported by Athlete | |
|
|
|
SOURCE: Based on CDC, 2012b.
of high school football players found that 41 percent of subjects reported not wanting to leave the game as their reason for not reporting a possible concussion, and 66 percent said they did not report their symptoms because they did not think their injury was serious enough to warrant medical attention (McCrea et al., 2004).1 In a 2012 survey of high school football players, a majority indicated that it was “okay” to play with a concussion and said that they would “play through any injury to win a game,” despite being knowledgeable about the symptoms and dangers of concussions (Anderson et al., 2013; see also Coyne, 2013; Kroshus et al., 2013; Register-Mihalik et al., 2013a,c; Torres et al., 2013). In addition, concussion signs and symptoms may develop and evolve over time, particularly within the first hours following injury (Duhaime et al., 2012; McCrory et al., 2013b). The mantra for laypersons faced with a potentially concussed athlete is “when in doubt, sit them out”: If a player has received “a bump, blow, or jolt to the head or body” and exhibits or reports one or more of the signs or symptoms of concussion, the player may have sustained a concussion (CDC, 2012a).
Appropriately trained personnel have a number of tools available for use in the initial assessment of an individual for a possible concussion (see, e.g., Table 3-2; Appendix C). The Standardized Assessment of Concussion (SAC) and the Sport Concussion Assessment Tool (SCAT) 3 or Child SCAT3 were developed for the sideline evaluation of potentially concussed athletes. The Military Acute Concussion Evaluation (MACE) is a screening tool used to assess service members involved in a potentially concussive event. Such tools as well as balance tests (see Table 3-2) may be used either by trained responders as part of an acute sideline or in-field assessment or by health care providers during subsequent clinical evaluation. It is important to note, however, that because of the natural evolution of concussions, not all concussed athletes will be identified at the time of (presumed) injury even when personnel trained in concussion recognition are present (McCrory et al., 2013b). Duhaime and colleagues (2012) found that 50 percent of a sample of collegiate athletes who sustained a diagnosed concussion (with athletic trainers present for all games and practices) did not experience an “immediate or near immediate” onset of symptoms.
____________________________________
1The reasons for athletes not reporting concussion were not mutually exclusive. The subjects were asked to select all that applied.
TABLE 3-2 Sideline Concussion Screening Tools
| Test | Function Assessed | Baseline Needed |
| Glasgow Coma Scale (GCS) | Degree of brain impairment | No |
| (Teasdale and Jennett, 1974) | ||
| Standardized Assessment of Concussion (SAC) (McCrea, 2001; McCrea et al., 1998, 2000) |
Memory and attention processes | Recommended |
| Sport Concussion Assessment Tool (SCAT) 3 and Child SCAT3 (McCrory et al., 2013a,c) |
Compilation of: GCS, SAC, BESS, symptom checklist, and neck evaluation | Recommended |
| Military Acute Concussion Evaluation (MACE) (DVBIC, 2012) |
Compilation of event history, symptom checklist, modified SAC, neurological screening | |
| Balance Error Scoring System (BESS) (Riemann et al., 1999) |
Central integration of vestibular, visual, and somatosensory information | Normative data available but baseline recommended |
| Sensory Organization Test (SOT) (Neurocom, 2013) |
Central integration of vestibular, visual, and somatosensory information | |
| King-Devick Test (Galetta et al., 2011) |
Saccadic eye movements | Recommended |
| Clinical reaction time (RTclin) (Eckner et al., 2010, 2013) |
Reaction time | Yes |
Concussion Diagnosis
Given the absence of a diagnostic test or biomarker for concussion, the current cornerstone of concussion diagnosis is confirming the presence of a constellation of signs and symptoms after an individual has experienced a hit to the head or body. Symptoms are self-reported by the athlete, often using a symptom scale. Reliance on an athlete’s self-report of symptoms as a fundamental part of diagnosing a concussion is complicated by the subjective nature of the assessment and by the possibility of an athlete underreporting the symptoms (Anderson et al., 2013; Dziemianowicz et al., 2012; McCrea et al., 2004). Using multiple evaluation tools, such as symptom
scales and checklists, balance testing, and neurocognitive assessments, may increase the sensitivity and specificity of concussion identification (Broglio et al., 2007b; Guskiewicz and Register-Mihalik, 2011; Harmon et al., 2013; Register-Mihalik et al., 2013b), and this is the current preferred method of diagnosing a concussion, although existing evidence is insufficient to determine the best combination of measures (Giza et al., 2013).
Traditional neuroimaging techniques, such as standard computed tomography (CT) and magnetic resonance imaging (MRI) (see Box 3-1), are
A number of imaging techniques have evolved for measuring the structure, function, and connectivity of the developing human brain in vivo. The most commonly used techniques, which are briefly described below, vary in invasiveness (i.e., requirement of radioactive isotope, intravenous injection, or concentrated radiation).
Computed Tomography (CT) uses focused X-rays together with computer imaging technology to make three-dimensional pictures of the head and can detect skull fracture, hemorrhage, and swelling.
Diffusion tensor imaging (DTI) noninvasively measures axonal microstructure based on diffusion of water molecules that are impeded by the orientation, myelination, and regularity of fibers. The most common measures include water diffusion (mean diffusivity) and the directionality and strength of the diffusion (fractional anisotropy).
Functional magnetic resonance imaging (fMRI) noninvasively measures changes in blood oxygenation in the brain that are assumed to reflect changes in neural activity. Activity is measured either while the individual is performing a task (task-based fMRI) to link brain activity with cognitive performance or while at rest (resting state fMRI) to examine synchronous activity across brain regions.
Magnetic resonance imaging (MRI) uses a magnetic field and pulses of radio wave energy to perturb water molecules in the brain to generate images of different types of brain tissue. This noninvasive technique is used to measure regional and whole brain volume and to identify brain lesions and bleeds.
Magnetic resonance spectroscopy (MRS) uses signals from water molecules to measure concentrations of metabolites noninvasively.
Single-photon emission computed (SPECT) and positron emission tomography (PET) measure cerebral metabolism and blood flow using intravenous injections of radioactive isotopes to construct pictures of functional processes of the brain, including glucose metabolism and blood flow.
used to rule out more severe head and brain injuries, such as skull fractures and intracranial hemorrhages, as well as cerebral swelling that would require surgical intervention (Giza et al., 2013; McCrory et al., 2013b; Suskauer and Huisman, 2009). Because of its accessibility in the emergency room, CT is the most commonly used imaging technique for clinical assessment of head trauma (Belanger et al., 2007; Toledo et al., 2012). CT exposes the individual to radiation, which is an important consideration when evaluating youth. The American Academy of Neurology has recently recommended that CT not be used to evaluate suspected sports-related concussion in the absence of signs or symptoms of more serious traumatic brain injury (TBI) (Giza et al., 2013). Although MRIs avoid the use of ionizing radiation, instead using a magnetic field and pulses of radio wave energy to image different types of brain and body tissue, they too are of little diagnostic value for concussions per se, because structural imaging results are normal in concussions that are uncomplicated by skull fracture or hematoma.
Newer imaging techniques (see Box 3-1), such as magnetic resonance spectroscopy, positron emission tomography, single-photon emission computed tomography, functional magnetic resonance imaging, and diffusion tensor imaging—which all can be used to track metabolic, blood flow, and axonal changes—build on animal work and clinical outcome measures in mild traumatic brain injury (mTBI). Although such techniques may be useful in the future for assessing sports-related concussions, at present they have not been validated for clinical use (Cubon et al., 2011; DiFiori and Giza, 2010; Jantzen et al., 2004; Koerte et al., 2012; Lovell et al., 2007; Vagnozzi et al., 2010; Virji-Babul et al., 2013).
Signs and Symptoms
The signs and symptoms of concussion reported within 1 to 7 days post injury (see Table 3-3) typically fall into four categories—physical (somatic), cognitive, emotional (affective), and sleep—and patients will experience one or more symptoms from one or more categories. A study of high school athletes found that female athletes reported more somatic symptoms (drowsiness and sensitivity to noise) while their male counterparts reported more cognitive symptoms (amnesia and confusion/disorientation), although the number of symptoms reported did not differ by sex (Frommer et al., 2011). Kontos and colleagues (2012) have reported a revised factor structure—cognitive-migraine-fatigue, affective, somatic, and sleep. In their study, high school athletes reported lower levels of the sleep symptom factor than did college athletes, and female athletes reported higher levels of the affective symptom factor than did their male counterparts. There were no age or sex differences for the other factors, and the interaction between age and sex
TABLE 3-3 Concussion Symptoms by Category
| Somatic | Cognitive | Emotional | Sleep |
|
|
|
|
SOURCE: CDC, 2013.
was not significant (Kontos et al., 2012). It should be noted that the symptoms reported differently by males and females in the Frommer study fell within a single factor in the structure presented by Kontos and colleagues.
Clinical Assessment
Because concussions can affect several aspects of brain function, a battery of tests is needed to assess and monitor a concussion. Relying on any one type of test for the ongoing monitoring of a concussed athlete and for making the decision to clear the athlete for activity risks an incomplete picture because the functions covered by each test recover at different rates (Ellemberg et al., 2009; Guskiewicz, 2011; Guskiewicz and Register-Mihalik, 2011).
A comprehensive concussion assessment includes symptom scores, objective measures of postural stability (Hunt et al., 2009), and cognitive testing as is often done with neuropsychological testing. Broglio and colleagues (2007b) found that a complete battery of tests, including assessment of neurocognitive functioning, self-reported symptom assessments, and postural control evaluation, was more sensitive to concussions than was each test individually. The sensitivity of the complete battery ranged from 89 to 96 percent, with the tests detecting no impairment in the other 4 to 11 percent of athletes diagnosed with concussion.
Register-Mihalik and colleagues (2013b) used a healthy sample of college football players to establish reliable change confidence intervals for common clinical concussion measures and applied the reliable change parameters to a sample of concussed players examined before and after
injury. Outcome measures included symptom severity scores, Automated Neuropsychological Assessment Metrics (ANAM) computerized neuropsychological battery throughput scores, and SOT composite scores. Concussed athletes (n=132) were assessed within 5 days of injury. Based on the percentage of athletes with reliable change scores below or above various confidence interval cutoffs (80 percent, 90 percent, 95 percent), they calculated sensitivity and specificity based on the percent of cases that declined by more than the reliable change metric. At all three confidence intervals, individual tests and total battery scores exceeded 90 percent specificity, indicating that when there was either no change or an improvement, it was predictive of the athlete not having a concussion. On the other hand, a decline in the scores was not predictive of having a concussion. Although having at least one score decline across the entire battery improved sensitivity, the sensitivity was still at 50 percent. The authors emphasize the importance of using a total battery in the assessment of concussion. In this particular battery, score declines did not predict concussions any better than chance.
Symptom Assessment
An athlete who has had a concussion often will complete a postconcussion symptom scale at each visit with his or her health care provider. These self-reports of symptoms not only provide information pertinent to concussion diagnosis but also serve as the foundation of monitoring recovery and decision making about the individual’s return to school and physical activity. A variety of symptom checklists are available and are usually completed by the athlete with each symptom graded using a Likert scale (e.g., 0 is “not experiencing” and 6 is “most severe”), although a few use a “yes/no” classification (Valovich McLeod and Leach, 2012). The variety and psychometric properties of several commonly used symptom scales and checklists are discussed later in the chapter (see also Appendix C).
Balance Testing
The dizziness and balance disturbances reported following an impact to the head or body may result from disruption of the central integration of vestibular, visual, and somatosensory information. Postural instability has been seen in patients following mild, moderate, and severe TBI (Geurts et al., 1996), while Guskiewicz (2001) found balance disturbances in college athletes within 2 days following a concussion. Other researchers have corroborated these results, and the equilibrium of the athlete is now objectively tested as a part of an acute concussion evaluation (Cavanaugh et al., 2005; Covassin et al., 2012a; McCrea et al., 2003; Register-Mihalik et al., 2008) carried out using a tool such as the BESS or SOT, described in Appendix C.
Neuropsychological Testing
Neuropsychological testing has become commonplace in the evaluation of concussed athletes. Traditionally neuropsychological tests have not been used to make diagnoses but rather to characterize cognitive function, testing memory, speed, and processing time. Although neuropsychological tests are able to detect cognitive changes in injured athletes, these tests are also sensitive to state effects which might include the symptoms associated with the injury (Fazio et al., 2007). A study by Van Kampen and colleagues (2006) demonstrated that neuropsychological testing improves diagnostic accuracy, particularly in ruling out a concussion if the test results are normal or typical relative to an appropriate individual or group norm (baseline). However, questions have been raised about whether the presence of ongoing cognitive deficits in the absence of symptoms actually predicts any risk for youth in terms of recurrent injury or long-term functional deficits or, conversely, whether the resolution of cognitive deficits on neuropsychological testing is helpful in predicting when it is safe for an athlete to return to full physical activity (Kirkwood et al., 2009). A full discussion of the use of neuropsychological testing in concussion diagnosis and management appears later in the chapter.
Electroencephalography
The electroencephalogram (EEG) provides a reading of the electrical activity on the scalp, which originates within the neurons (gray matter) that make up the surface of the brain. Quantitative EEG (QEEG) techniques record this EEG activity from large arrays of electrodes on the scalp and are effective in detecting changes in brain electrical processing following concussion (Gosselin et al., 2009) as well as after behavior deficits have disappeared (McCrea et al., 2010; Prichep et al., 2013). McCrea and colleagues (2010) compared performance and QEEG measures on 28 high school and college athletes who experienced sports-related concussions with those recorded from 28 matched, uninjured controls. All underwent pre-season baseline testing on QEEG measures as well as on measures of concussive symptoms, postural stability, and cognitive functioning. Controls were matched to injured players based on their baseline tests. Clinical testing and QEEG were performed on the day of injury and were repeated 8 days and 45 days after injury. Although both groups performed identically prior to injury, after injury the concussion group differed significantly from controls, exhibiting more severe levels of post-concussion behavior symptoms through day 3. Importantly, QEEG measures continued to show increasingly larger differences through day 8 even though no behavioral differences occurred after day 3, suggesting that abnormalities in brain
function continued to increase for at least a week following injury, despite the absence of behavior impairments. Barr and colleagues (2012) reported similar results through 45 days post injury. QEEG was also much more effective in predicting when concussed athletes would be ready to return to play. Prichep and colleagues (2013) used a QEEG discriminant function algorithm based on frontal electrode sites to create a TBI Index of brain function that discriminated between those with mild (n=51) and those with moderate concussions (n=14) at 8 days and 45 days post injury. Only the QEEG index predicted return to play before 14 days post injury versus after 14 days post injury. Accuracy was 80 percent in both cases. Such results suggest that QEEG techniques could provide a more effective means to identify athletes with impairments following concussion and to predict when they might more safely return to play.
The event-related potential (ERP) is a portion of the continuous EEG signal, but it differs from the EEG in that the ERP is time-locked to the onset of a discrete stimulus. Upon onset, the EEG desynchronizes and produces an electrical waveform composed of a series of positive and negative voltage fluctuations that can differ in their amplitude (in μV, or millionths of a volt) and latency (in milliseconds). Under most conditions, the ERP continues for approximately 500 to 1,200 milliseconds before it returns to the baseline EEG signal (Molfese et al., 2001). Researchers report numerous instances in which information obtained using ERPs converges with functional findings from fMRI, magnetoencephalography, near-infrared and PET techniques. The advantage of the ERP measure over most other imaging techniques is that it provides very rapid temporal information about the order in which different neural and cognitive processes occur. As Broglio and colleagues (2011) note, this tool has been successful in identifying relationships between brain-behavior measures in concussed versus nonconcussed athletes. The most studied of the ERP components is the P300 or P3b component. Baillargeon and colleagues (2012) reported that this component is reliably smaller in children, adolescents, and adults who have experienced a concussion than in individuals who do not have a concussion. Importantly, as in the case of QEEG, ERP studies show that such differences may continue even after other indications of concussive injury—such as behavior tests and somatic complaints—suggest recovery, indicating that persistent abnormalities in the P3b could reflect suboptimal compensation in concussed athletes. Thériault and colleagues (2009) suggest that if such effects persist, they may indicate that a concussed athlete is at increased risk for future concussions. Subsequent concussions also appear to alter brain responses. Thériault and colleagues (2011) identified impairments of working memory storage capacity that correlated with athletes’ history of concussions. Gosselin and colleagues (2012a) also recorded visual ERPs during a working memory task from 44 patients identified as having mTBI
(7 to 8 months post injury) and 40 control volunteers matched for age (19 to 41 years of age) and sex. They reported that the smaller amplitude ERPs correlated with slower reaction times and poorer working memory. Importantly, results did not differ for the type of injury (e.g., sports concussion versus motor vehicle).
There is some consensus in the literature that both QEEG and ERP procedures can detect differences in performance and neural responses in concussed versus non-concussed student athletes in high school and college even when behavior measures fail to do so. However, these findings are true for a relatively small set of tasks that assess a limited array of cognitive abilities. Use of a broader range of tasks that measure different aspects of cognitive processes is necessary to provide a comprehensive view of behaviors most likely affected and those more likely spared by concussion.
Serum Biomarkers
After a brain injury, proteins may leak from damaged cells into the cerebrospinal fluid, then cross the blood-brain barrier to enter into the bloodstream. Although research on serum brain biomarkers in adults with severe TBI dates back to the 1970s, research on serum biomarkers for milder TBI and in children has emerged in the last 15 years, and the literature on biomarkers for mTBI or concussion in the pediatric population is very limited (Berger and Zuckerbraun, 2012). Potential roles for serum biomarkers in the diagnosis and management of sports-related head injury include (1) distinguishing individuals with a concussion from those with non-concussion head injury; (2) identifying individuals who may have a skull fracture or more severe intracranial injury (e.g., intracranial hemorrhage, cerebral swelling); and (3) identifying those individuals who may be at risk for a prolonged recovery (Berger and Zuckerbraun, 2012). Three biomarkers in particular have emerged from the mTBI literature: S100B, neuron-specific enolase (NSE), and cleaved tau protein (CTP) (Berger and Zuckerbraun, 2012; Finnoff et al., 2011).
S100B is a protein that is found in the brain and also in cartilage and skin. It originates in the glial cells, and plays a role in neuronal proliferation, differentiation, regeneration, and apoptosis (Geyer et al., 2009). Geyer and colleagues (2009) examined S100B levels in 148 children ages 6 months to 15 years of age with either head injury alone or head injury accompanied by symptoms of mTBI. They found that S100B did not readily discriminate between the two groups. Other studies have found elevated S100B levels in uninjured adult marathon runners, adult ice hockey players, adult boxers, and adult basketball players, which suggests that S100B is increased by extracranial release due to exercise (Hasselblatt et al., 2004; Otto et al., 2000; Stålnacke et al., 2003), which may limit its usefulness as a biomarker
for identifying sports-related concussion. In addition, the normal level of S100B varies with age and is particularly high in children under 2 years of age, indicating the need for age-specific normative values. S100B also has a short half-life, so the time a blood sample is obtained after injury is important (Berger and Zuckerbraun, 2012). All of these factors can lead to inadequate and confusing results, which limit the current utility of serum biomarkers (Filippidis et al., 2010).
S100B may have a role in the identification of individuals who require further assessment (e.g., neuroimaging) for intracranial injury. Adult studies have shown that S100B may be useful for identifying individuals with head injury who do not have intracranial injury thereby preventing unnecessary imaging procedures (Berger and Zuckerbraun, 2012). Castellani and colleagues (2009) studied 109 children and adolescents (0 to 18 years of age) diagnosed with mTBI who underwent CT. They found that normal S100B levels predicted the absence of intracranial injury and skull fracture with 100 percent accuracy. Another study of 152 children under 18 years of age with closed head trauma found higher levels of S100B in children with intracranial injury than in those without (Bechtel et al., 2009). However, the study included some patients with more severe TBI and was not designed to maximize sensitivity; the study demonstrated only a 90 percent negative predictive value for intracranial injury (Berger and Zuckerbraun, 2012).
NSE is found in neuron cytoplasm as well as in smooth muscle cells, adipose cells, red blood cells, and platelets. Because of the presence of NSE in red blood cells and platelets, hemolysis of blood samples, which is common in pediatric samples, may lead to false positive results when using NSE levels to evaluate mTBI (Berger and Zuckerbraun, 2012). The previously mentioned study by Geyer and colleagues (2009) showed that NSE was insensitive for distinguishing children and adolescents with head injury and symptoms of mTBI from those with head injury only. A study of 50 children and adolescents 0 to 18 years of age with blunt head trauma (not all mTBI) found that NSE levels in the acute phase following injury were neither sensitive nor specific for detecting the presence of intracranial injury; nearly 25 percent of patients identified with intracranial injury following CT scans would have been missed (Fridriksson et al., 2000). The study did not report the negative predictive value of a normal NSE level (Berger and Zuckerbraun, 2012).
Several pediatric TBI studies suggest that high levels of NSE and S100B and myelin-basic protein may be associated with poorer outcome (Bandyopadhyay et al., 2005; Beers et al., 2007; Berger et al., 2007), but none was limited to patients with mTBI (Berger and Zuckerbraun, 2012). CTP is a microtubule-associated protein in axons. No studies were found that looked at CTP use in pediatric concussions, but studies showed that
CTP had no diagnostic or prognostic value with adult mTBI (Bazarian et al., 2006; Finnoff et al., 2011).
There is little research on the use of serum biomarkers in the diagnosis and management of pediatric concussions. Although appropriately sensitive and specific serum biomarkers could be of great diagnostic and prognostic value in sports-related concussion sometime in the future, there currently is no evidence to support their use. There is some evidence, however, to suggest that normal levels of S100B following head injury may predict individuals who do not have intracranial injury.
Symptom Scales and Checklists
Concussion symptom checklists survey a broad range of symptoms that are considered to be pathognomonic of concussion. Of the approximately 20 different symptom scales commonly used to evaluate concussion, 14 are variations of 6 core scales,2 which include symptoms associated with sports-related concussion, although the number of items on each scale varies (Alla et al., 2009; Valovich McLeod and Leach, 2012). A 2009 review of literature pertaining to the psychometric properties of these self-report concussion scales and checklists found that very few of them had been developed systematically or had published psychometric properties (Alla et al., 2009; Valovich McLeod and Leach, 2012). The recent American Academy of Neurology guideline states that “evidence indicates it is likely that [a symptom scale or checklist] will accurately identify concussion in athletes involved in an event during which biomechanical forces were imparted to the head” (Giza et al., 2013, p. 3). The guideline indicates that the sensitivity of such symptom reporting tools ranges from 64 to 89 percent and their specificity ranges from 91 to 100 percent (Giza et al., 2013).
A 2009 literature review of symptom scales used in the pediatric, adolescent, and young adult populations (ages 5 to 22 years) identified one research-based scale and four scales that were in clinical use; psychometric evidence for the scales was assessed for younger children (5 to 12 years) and for adolescents and young adults (13 to 22 years) (Gioia et al., 2009).3 The psychometric evidence relating to symptom scales is stronger for ado-
____________________________________
2The core scales are the Pittsburgh Steelers Post-Concussion scale (17 items), Post-Concussion Symptom Assessment Questionnaire (10 items), Concussion Resolution Index post-concussion questionnaire (15 items), Signs and Symptoms Checklist (34 items), Sport Concussion Assessment Tool (SCAT) post-concussion symptom scale (25 items), and Concussion Symptom Inventory (12 items).
3The research-based scale is the Health and Behavior Inventory; the four clinical scales are the Post-Concussion Symptom Scale, Graded Symptom Checklist/Scale, Rivermead Post-Concussion Symptom Questionnaire, and Post-Concussion Symptom Inventory/Acute Concussion Evaluation (Gioia et al., 2009).
lescents than for younger children, and there is reasonable evidence to support the validity of the scales, although data on their reliability is limited and additional research is needed (Gioia et al., 2009). A more recent review by Janusz and colleagues (2012) discussed the psychometric properties of these same symptom scales as well as of the Concussion Symptom Inventory (CSI) (Randolph et al., 2009) and the Acute Concussion Evaluation (ACE) (Gioia et al., 2008a).
Randolph and colleagues (2009) analyzed a large set of data from three separate projects to develop the 12-item CSI, which is the first empirically derived symptom scale for concussion identification and short-term serial use following a sports-related concussion. The CSI was shown to be as effective as longer symptom inventories, such as the Graded Symptom Checklist, at recognizing concussions.
TABLE 3-4 Measures of Post-Concussion Symptomatology
| Instrument | Age Range (years) | Parent Form |
| Health and Behavior Inventory (HBI) (Ayr et al., 2009) | 8-15 | Yes |
| Acute Concussion Evaluation (ACE) (Gioia and Collins, 2006; Gioia et al., 2008a) | 3-18 | Yes |
| Concussion Symptom Inventory (CSI) (Randolph et al., 2009) | High school–college | No |
| Graded Symptom Checklist/Scale (GSC/GSS) (Mailer et al., 2008; Piland et al., 2006) | ≥13 | No |
The characteristics of the instruments and their psychometric properties are discussed in Appendix C and summarized in Table 3-4.
The Health Behavior Inventory and Post-Concussion Symptom Inventory (PCSI) are the only measures that are well studied in children under the age of 12 and have the advantage of having reports from parents and, in the case of the PCSI, teachers. Studies looking at the concordance of symptoms reported by 8- to 15-year-old patients and their parents found that mean symptom ratings tended to be higher for children as compared to their parents (Ayr et al., 2009; Hajek et al., 2011). Gioia has also found that the self-report of symptoms differs between athletes and their parents, with parent reports demonstrating better diagnostic utility than youth self-report (Gioia, 2013).
| Description | Reliability | Validity |
| 20 items, 4-point Guttman scale 3-factor structure (cognitive, somatic, emotional) (Ayr et al., 2009) | Internal consistency, parent-child correlation, no test-retest reliability | Discriminates head injury from orthopedic injuries; correlates with quality of life, family burden, educational, and social difficulties (Yeates et al., 2012) |
| 22 items, 2-point Guttman scale | Test-retest and interrater reliability | Content validity, relationship to other measures, group discrimination, sensitivity to recovery |
| 12 items, 7-point Guttman scale | No report | Sensitivity and specificity high via receiver operating characteristics (ROCs) curve analysis (Randolph et al., 2009) |
| GSC 16 items; GSS 17-20 items, 7-point Guttman scale 3-factor solution reported (cognitive, somatic, neurobehavioral) (Piland et al., 2006) | Internal consistency, test-retest reliability | Discriminates between patients who suffered blows of lower and higher impact (McCaffrey et al., 2007). Convergent validity with measures of balance, neurocognitive function, headaches (McCrea et al., 2003; Register-Mihalik et al., 2007) |
| Instrument | Age Range (years) | Parent Form |
| Post-Concussion Symptom Scale (PCSS) (Lovell and Collins, 1998) | ≥12 | No |
| Rivermead Post-Concussion Symptoms Questionnaire (RPCSQ) (King et al., 1995) | ≥8 | No |
| Post-Concussion Symptom Inventory (PCSI) (Gioia et al., 2008b, 2009) | 5-18 | Yes, also version for teachers |
SOURCES: Based on Gioia et al., 2009; Janusz et al., 2012; Randolph et al., 2009.
Introduction to Neuropsychological Testing
Neuropsychology is the study of brain-behavior relationships, that is, the ways in which specific neural (brain) structure and activity are reflected in cognitive and physical behavior. The terms “neuropsychological” and “cognitive” are often used interchangeably (as in neuropsychological testing, cognitive testing, and neurocognitive testing). For the purposes of this document, the terms can be understood as equivalent.
Tests such as Trail Making, Paced Auditory Serial Attention Test, Digit
| Description | Reliability | Validity |
| 22 items; in youth ages 13-22, 7-point Guttman scale; 4-factor structure score (cognitive-fatigue-migraine; affective, somatic, and sleep) | Test-retest reliability (prepost season, ICC=0.55; test retest, r=0.65 | Discriminates concussed from non-concussed athletes (Echemendia et al., 2001; Field et al., 2003; Iverson et al., 2003; Lovell et al., 2006; Schatz et al., 2006); greater abnormalities in those with multiple concussions (Collins et al., 1999). Convergent validity: correlates with neurocognitive performance and fMRI changes during working memory tasks (Collins et al., 2003b; Pardini et al., 2010) |
| 16 items, 5-point Guttman scale; no reported factor structure | In adolescents, high internal consistency, low test-retest reliability (Iverson and Gaetz, 2004) | Discriminant validity between concussed and non-concussed youth (Wilde et al., 2008) |
| Age 5-7, 13 items, 3-point Guttman scale Age 8-12, 17 items, 3-point Gutmann scale Age 13-18, 20 items, 7-point Guttman scale Parent, 20 items, 7-point Guttman scale; focus on cognitive, emotional, sleep, and physical domains | Test-retest reliability for self-report; high interrater reliability and internal consistency (Schneider and Gioia, 2007; Vaughan et al., 2008); moderate (r=0.4-0.5) (Gioia et al., 2008b); agreement between reporters in one of two studies (Gioia et al., 2009) | Good predictive and discriminant validity (Diver et al., 2007; Vaughan et al., 2008) |
Symbol Substitution, and Digit Span have long been used in documenting cognitive deficits in TBI. The earlier neuropsychological literature on TBI has documented several specific areas of typical deficit, with processing speed, attention and memory typically showing the most significant deficits. Sports concussions may have the following effects:
- Reduced planning and ability to switch mental set (Barth et al., 1983, 1989, 2000; Rimel et al., 1982)
- Impaired memory and learning (Gronwall and Wrightson, 1981; Guskiewicz et al., 2001; Lovell et al., 2003)
- Reduced attention and ability to process information (Maddocks et al., 1995)
- Slowed reaction times and increased variability in response (Collins et al., 2003b; Makdissi et al., 2001)
Although neuropsychological testing is recognized as a powerful tool for understanding the cognitive effects of brain injury, it has inherent limitations and factors that affect the resulting scores and interpretations.
In 2001, Grindel and colleagues reviewed the existing literature on sports concussions and commented on several important issues that needed to be addressed by the field (Grindel et al., 2001). These included the availability of baseline testing, the validity of the test battery, problems involving repeated testing, interpretation of the test, the costs of testing, the presence of severe or prolonged symptoms, the presence of multiple concussions, age, gender, and perhaps the athlete’s level of play. Many of these issues have been addressed as newer tools and improved analyses have been published. Baseline testing has become prevalent with the advent of Web-based computerized tests; the validity of the tests themselves has been established, although confounding factors such as symptom load, test administration environment, and comorbid conditions continue to plague the field. Reliable change metrics have improved the problems with repeat testing, and the effects of multiple concussions have been recognized and often used as a covariate in group studies.
Randolph and colleagues (2005) reviewed the state of neuropsychological testing in sports-related concussion management and concluded that the (then) existing tests did not meet necessary standards for use. Issues of reliability and validity as well as poor psychometric controls were felt to render testing useless for this specified purpose. They opined that athletic trainers and sports medicine professionals would do just as well using standardized graded checklists.
In 2010, Comper and colleagues published a systematic review of the methodological features of research in sports concussion, focusing on studies that used neuropsychological tests. They concluded that the methodological quality of studies were highly variable (Comper et al., 2010). In a separate paper, they noted that no prospective studies using control groups had been done to validate the use of neuropsychological tests (Hutchison et al., 2011). Prospective studies with controls are difficult to complete, but there are now some studies with control groups and within-subjects designs that use baseline test performance and the amount of change relative to expectation as dependent variables.
In spite of these concerns, the use of neuropsychological testing in sports has proliferated, with ever more computerized batteries coming on
the market, and professional, college, high school, and youth sports teams implementing some form of testing.
Factors Affecting Neuropsychological Testing
The influence of intrinsic and extrinsic factors on neuropsychological test performance has long been studied, and clinicians attempt to minimize the effects of these factors by using standardized procedures and testing environments. McCrory and colleagues (2005) listed a number of individual factors (e.g., genetics, general cognitive level of functioning, gender, ethnicity, mood) and methodological factors (e.g., testing environment, practice and learning effects, administrative expertise) that may influence test outcomes (see Figure 3-1). Other individual factors that may affect test outcomes include learning disabilities, attention deficit hyperactivity disorder, and color blindness. Symptom load as a state factor should also be considered as a factor that affects test performance (McCrory et al., 2005). Score interpretation depends on reliable administration and the proper consideration of all of these factors, some of which are reduced with computerized testing (McCrory et al., 2005).
Using trained test administrators and testing in appropriate environ-
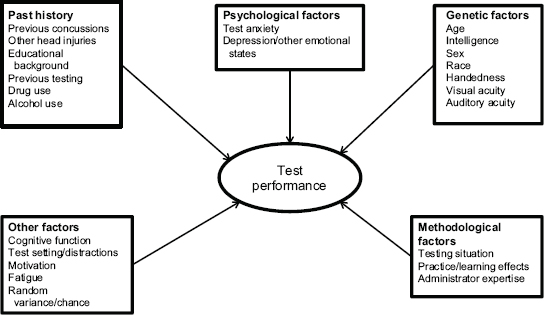
FIGURE 3-1 Factors that impact the results of neuropsychological tests.
SOURCE: McCrory et al., 2005, p. i61. Reproduced with permission from BMJ Group Ltd.
ments are fairly obvious requirements, but there are no data on the actual training or testing environments that are currently in use. Group testing, the way in which most baseline assessments are administered, appears to systematically lower scores compared to individualized administration (Moser et al., 2011).
Age and sex are well-known contributors to score differences in all educational and psychological tests. Test standardization requires validity studies that determine these differences and allow the presentation of separate norms (see AERA et al., 1999). Most published tests, including Immediate Post-Concussion Assessment and Cognitive Testing (ImPACT), CogSport, Concussion Resolution Index (CRI), and Automated Neuropsychological Assessment Metrics, provide age and gender normative standards or references. Unless tests have been shown to be insensitive to gender, they are expected to offer separate scoring parameters.
Higher academic achievement has been linked to higher computerized neuropsychological test scores. One study looked at neuropsychological test scores in more than 300 Division I NCAA schools. Athletes with the highest levels of academic achievement based on the Scholastic Aptitude Test (SAT) had higher scores on the ANAM test battery than did those athletes with lower SAT scores (Brown et al., 2007). Comorbid conditions such as attention deficit hyperactivity disorder, learning disabilities (Collins et al., 1999), and autism also may be reflected in test scores. Some medications can also affect scores, including anti-epileptic drugs and psycho-stimulants (see, e.g., Biederman et al., 2008).
Poor effort is somewhat more difficult to detect and control, but it is a factor that lowers scores. This has been documented in the general TBI literature (Green, 2007; Lange et al., 2010). A major concern in testing for sports-related concussions is the willful lowering of baseline scores in order to establish an easier threshold for “return to baseline” (Pennington, 2013). The ImPACT test has embedded validity indicators to help examiners determine atypically low scores on specific subtests. However, individuals with neurologic or developmental disorders or those who are under acute stress may legitimately score low on these indicators; thus, individual analysis is required before declaring a test invalid. There are also specific tests and profiles within neuropsychological tests that are used to detect poor effort, “malingering,” or suboptimal performance.
Hunt and colleagues (2007) found that 11 percent of their sample of 199 high school athletes exhibited poor effort as indexed by the Dot Counting Test and the Rey 15-Item Test with recognition trial. Statistically significant differences existed between effort groups (p < 0.05) on several of the neuropsychological tests. By comparing a group with unusually low baseline scores versus post-injury scores at 1 week to a group with high baseline scores, Bailey and colleagues (2006) found significantly more improvement
from baseline to post injury for athletes who reported “low motivation” on baseline testing. The authors concluded that low motivation exists and that it does affect test scores. However, Erdal (2012) found that it was difficult for athletes to purposely do poorly on the ImPACT test without tripping the validity indicators embedded in the ImPACT test. Nevertheless, the perceived secondary gain of lowering one’s baseline test score is a concern when using the baseline-testing paradigm. In the case of large-scale baseline testing sessions, it is particularly difficult to know whether low scores are due to intrinsic factors or poor motivation.
In the clinical pediatric population, sleep debt does not appear to interfere with neuropsychological testing, although it is strongly implicated in poor school performance (see Beebe, 2012, for review). Although sleep does not appear to affect laboratory test performances, one small study indicated that the number of hours of sleep the night before baseline testing was related to higher non-sleep symptom scores (i.e., less sleep was related to higher non-sleep symptom totals; see Maerlender and Alt, 2012).
Mood and anxiety have long been known to affect neuropsychological test performance in clinical patients. Bailey and colleagues (2010) and Maerlender and colleagues (2010) presented data demonstrating that mood and anxiety scores on independent measures were related to specific test score patterns on ImPACT and on a paper-and-pencil neuropsychological battery. The Bailey study administered the Personality Assessment Inventory together with the CRI and found that a significant amount of variance in baseline scores was accounted for by mood and anxiety symptom load. Using the symptom scale that is part of the ImPACT battery, Covassin and colleagues (2012b) found that athletes with high levels of depression reported more concussion-like symptoms and had lower ImPACT test scores on baseline tests.4 The ANAM battery has validated a mood scale and demonstrated its relationship to test scores (Johnson et al., 2008). Given the increased use of neuropsychological testing at baseline and post injury, it is important to understand the effect of these factors, and the potential effect of these factors on test results highlights the need for interpretation of the tests by experienced providers. There are several ways in which mood and anxiety can be related to neuropsychological performance in concussed athletes. It could be, for example, that both increased anxiety and decreased performance are the result of the same brain injury, or that the depression and anxiety symptoms are a response to the problems in the cognitive performance, or that depression and anxiety have negatively affected neurocognitive performance. Indeed, there is evidence to support
____________________________________
4High school athletes reported more somatic or migraine symptoms than did college athletes, whereas college athletes reported more emotional and sleep symptoms than did their high school counterparts.
each of these three possibilities (Chen et al., 2007; Pardini et al., 2010). Although most studies of athletes have used older samples and there are no systematic studies in athletes younger than high school age, there is no reason to believe that the state effects of anxiety, mood, or stress would be different in a younger population.
Pain has been shown to affect cognition in some groups of patients. A recent study by Gosselin and colleagues (2012b) compared groups of adolescents with mTBI (n=24, 50 percent of whom had sports-related injuries), non-injured controls (n=16), and athletes with orthopedic injuries (n=29). Levels of pain were the dependent measure and blood oxygen level-dependent activation during working memory task was the outcome. While results were somewhat complicated, the authors interpreted the results as demonstrating that behavioral performance and cerebral function were related to levels of pain.
The validity of neuropsychological tests for interpreting brain-behavior relationships rests on psychometric characteristics, including reliability. The use of the same test multiple times for tracking change or measuring injury (i.e., baseline to post injury) is compromised by several factors, most notably the practice effect of retaking the test. Although multiple forms (using different specific items) can reduce this, the effect of exposure to the procedure (directions, pacing, sequence of tasks) has a greater effect than the likelihood of memorizing specific responses (Heilbronner et al., 2010). To address this issue, several statistical procedures have been developed to account for practice effects, the tendency of scores to “regress to the mean,” and differential pre-injury test scores (for review, see Hinton-Bayre, 2012). The American Academy of Clinical Neuropsychology has issued a position paper that outlines these concerns and discusses the recommended statistical procedures (reliable change indices, regression-based methods) (Bauer et al., 2012; Heilbronner et al., 2010). It recommends that such statistical adjustments be used any time tests are used in a serial fashion.
Neuropsychological Testing and Sports-Related Concussions
Jeffrey Barth and his colleagues are generally credited with originating the use of athletes and teams as a laboratory for studying the nature and outcomes of concussion through sports (the Sports as a Laboratory Assessment Model) and the baseline pre-season testing of athletes with brief neuropsychological batteries for later post-injury comparisons (Barth et al., 1989; Macciocchi et al., 1996). With the growing use of neuropsychological testing in the identification and management of sports-related concussions has come controversy and criticism about the methods and outcomes.
This section considers the following questions concerning neuropsychological assessment in sports-related concussions:
- Can neuropsychological testing assist in the diagnosis of sports-related concussions in youth?
- Does neuropsychological testing have a role in tracking recovery and informing management (e.g., return to school, return to play, return to work)?
- Are computerized tests valid and reliable?
- Does baseline testing improve the utility of neuropsychological testing in the diagnosis and management of sports-related concussion?
Can Neuropsychological Testing Assist in the Diagnosis of Sports-Related Concussions in Youth?
In the context of sports-related concussions, an important distinction must be made between the use of neuropsychological tests for diagnosis and their use for tracking recovery (McCrory et al., 2005). Studies of the ability of neuropsychological tests to provide accurate diagnoses of concussion typically involve tests administered within 72 hours of the injury. They include studies comparing group-level score changes in groups of concussed individuals versus groups of non-concussed individuals and studies looking at individual diagnostic accuracy. However, it should be noted that neuropsychological tests are traditionally not used to make diagnoses, but rather to characterize function. So it is a useful question to ask whether these tests can contribute to diagnosis.
An often unmentioned aspect of concussion research and practice is the variability in identification of concussion and the still-limited knowledge of the biological nature of concussions (i.e., the lack of biomarkers for diagnosis and recovery). Although studies typically rely on the identification of concussions by athletic trainers according to generally accepted standards, the validity of these diagnoses has never been established. In one study, 50 percent of diagnosed concussions were identified more than 24 hours after the incident, and 30 percent of this group had no identifiable biomechanical impacts on the day of the reported injury (based on accelerometer readings in the helmets) (Duhaime et al., 2012). Determinations of the diagnostic efficiency of a test will be affected by the validity of actual diagnoses. Thus variability in this process can produce conflicting or limited results in studies of the predictive ability of any tool.
Given the relatively rapid time-course of concussions, the temporal aspects of the injury are also significant factors in studying the phenomena. Indeed, studies have shown that the closer the assessment was to the time of injury, the more pronounced the effect of the biomechanical force on cognition was (Beckwith et al., 2013a,b; McAllister et al., 2012). Broglio and Puetz (2008) questioned whether comparing athletes who are assessed at different time-points from injury likely invalidates the findings.
As Hutchinson and colleagues (2011) found, the presence of pain can have an effect on test scores. Controlling for diagnosis and time of testing, baseline exposure to the tests, and other factors adds to the complexity of studying concussions at the group and individual levels, particularly in the immediate aftermath of the injury when symptoms are typically high. McCrory and colleagues (2005) also questioned whether the presence of symptoms could preclude accurate (valid) test results. Symptoms may interfere in test performance through any or all attention mechanisms, reducing arousal, orienting, focus, sustaining focus, and so on, or symptoms may make the individual feel too bad to participate (a type of motivational effect). Unfortunately, the actual evidence is limited, as few studies directly test the hypothesis that symptoms (either in total or individually) account for significant variance in test scores.
As a practical matter the test scores may reflect the overall status of the individual, but, because neuropsychological tests are designed to assess brain function, the inclusion of symptom-related error into the test score interferes in the psychometric accuracy of the test. In other words, poor performance on a neuropsychological test because one feels bad may obscure the test’s ability to accurately measure brain function. Studies indirectly point to the correlation of symptoms and test scores (Collins et al., 2003a; Fazio et al., 2007), particularly immediately after injury, when symptoms tend to be highest. Thus, the mediating effect of symptoms on test scores in the immediate aftermath of the injury likely reduces the predictive power of tests alone. The evidence for diagnostic validity and utility comes from group studies and from studies of individual probability. Group studies have employed cross-sectional designs and within-subjects designs using baseline or multiple test points for comparisons. Group studies have been described in two meta-analytic studies (Belanger and Vanderploeg, 2005; Broglio and Puetz, 2008). There was considerable overlap in the groups of studies reviewed in the two analyses, but Broglio and Puetz were interested in the effect of using multimodal assessments, while Belanger and Vanderploeg were focused on neuropsychological assessments only.
Group studies have generally shown that a significant proportion of concussed athletes have neurocognitive decrements compared to controls (or compared to baseline performances) in the initial days following the injury, but scores are back to normal or baseline by 7 days post injury. Belanger and Vanderploeg (2005) analyzed 21 studies from 1994 to 2004. All had multiple assessment points using control groups tested at the same interval. They found significant acute effects (changes in scores reflecting worsening in the first 24 hours after injury) for most cognitive domains (delayed memory: d=1.00; memory acquisition: d=1.03; and global cognitive functioning: d=1.42). However, when analyzed across all studies, no
group residual neuropsychological reductions were found when testing was completed beyond 7 days post injury.
The meta-analysis of Broglio and Puetz (2008) included 39 studies from 1970 to 2006 that met their inclusion criteria: studies of concussed athletes who were evaluated using symptom assessment, balance assessment, or neuropsychological/cognitive assessment. One post-injury assessment had to have been completed within 14 days of injury and compared with a baseline measure or control group. Three types of cognitive assessments were included: the SAC, paper-and-pencil batteries, and computerized batteries. They found significant effects of concussion on all three types of assessments immediately after injury. The type of cognitive assessment was determined to be a moderator effect, as was the time from injury to assessment. The largest effect was for the SAC administered immediately after injury.
The usefulness of tests to diagnose a disease entity (e.g., their ability to detect a person with disease or exclude a person without disease) is usually described by such terms as sensitivity, specificity, positive predictive value, and negative predictive value. These various measures describe how well the tests identify people who actually have the disease (or not) as diagnosed by some gold standard method. Sensitivity (the chance that a person with the disease is correctly identified as having it) and specificity (the chance that a person without the disease is correctly identified as being free of it) are the characteristics most reported for a diagnostic test because they reflect the characteristics of the test and not those of the group tested. However, the users of the test are likely to be more interested in the predictive values (the chance that a person identified by the test as concussed actually had a concussion—positive predictive value—and the chance that a person identified as not having a concussion was actually free of a recent concussion—negative predictive value). The predictive value changes depending on what fraction of the athletes tested truly had a concussion.
Van Kampen and colleagues (2006) tested the diagnostic value of adding neuropsychological testing to assessments of symptom load. One hundred twenty-two athletes diagnosed with concussion and 70 without a recent concussion were compared by looking at their post-injury symptoms and their ImPACT test scores. Concussed athletes were tested 2 days after injury. Ninety-three percent of athletes with a reliable increase in symptoms actually had a concussion—a positive predictive value (PPV) of 93 percent—but 41 percent of those without a reliable increase in symptoms also had a concussion—a negative predictive value (NPV) of 59 percent. When ImPACT was used in the absence of symptom data, 83 percent of
those having at least one abnormal5 neurocognitive test score had a concussion (PPV=83%) and 70 percent of those with no abnormal neurocognitive scores did not have a concussion (NPV=70%). However, when criteria for concussion classification were changed to require at least one abnormal ImPACT test or a reliable increase in symptoms, 81 percent of those who the tests indicated had a concussion actually did (PPV=81%) and 83 percent of those the tests indicated were free of concussion actually were (NPV=83%). These predictive values are based on 64 percent (122 of 192) of the athletes studied having a recent concussion. If the same diagnostic criteria were used to screen every football player after every game (prevalence under 1 percent), more than 97 percent of the athletes the test identified as having a recent concussion actually would be diagnosed in error.
Several other studies have demonstrated a strong diagnostic efficiency for neuropsychological tests. Schatz and colleagues (2006) obtained 82 percent sensitivity and 89 percent specificity comparing ImPACT tests scores (n=72) within 72 hours of injury to scores of non-concussed athletes (n=66). A similar approach was used by this group analyzing ImPACT data of 81 concussed athletes and 81 controls, ages 13 to 21 (Schatz and Sandel, 2013). High sensitivity (91 percent) and adequate specificity (69 percent) were obtained.
Summary Neuropsychological tests have the ability to detect cognitive changes in injured athletes, although cognition as indexed by test scores appears to improve for the vast majority of injuries within 2 weeks. There are mixed results of the diagnostic utility of neuropsychological testing immediately (within 48 hours) after injury, although significant differences between concussed and non-concussed individuals are more often found in group studies. There is general agreement that neuropsychological tests should not be used in isolation for diagnosis; symptom levels are the best predictor of diagnosis (i.e., concussion diagnosis is made based on symptom presentation). Although the presence of symptoms can influence test results, potentially obscuring the accurate measurement of brain function, neuropsychological testing is one of several tools (along with symptom assessment, clinical evaluation, and the like) that may aid in concussion diagnosis. It appears that high scores on neuropsychological tests, indicating good cognitive function, are predictive of not having a concussion.
____________________________________
5Abnormal here means a change from baseline to post-injury score outside the 80 percent confidence interval for reliable change: abnormal reliable change index. This does not necessarily imply clinical abnormality.
Does Neuropsychological Testing Have a Role in Tracking Recovery and Informing Management?
Neuropsychological testing has been used extensively in the rehabilitation setting to document and track cognitive recovery. In the area of sports-related concussions, the standard as promulgated by the Zurich statement and other consensus statements has been that recovery can be said to have taken place when symptoms, cognition, and balance have returned to the athlete’s baseline (or typical) performance (Halstead et al., 2010; Harmon et al., 2013; McCrory et al., 2013b). Using that as the benchmark, studies have generally found neuropsychological testing to be a useful aid in determining when an athlete has recovered enough to return to competition. Although the methodological rigor of the studies varies (Comper et al., 2010), the ability of neuropsychological tests to detect subtle changes in cognitive function is well established.
Several studies have documented persistent declines in post-injury neuropsychological scores even after symptoms have resolved (Broglio et al., 2007a; Iverson et al., 2006; Peterson et al., 2003). These studies found improvements in cognitive scores, balance testing, and symptoms over time, with the cognitive scores taking longer to improve than the balance and symptom scores. Iverson and colleagues (2006) included a reliable change methodology and demonstrated that 37 percent of the concussed athletes continued to have at least two ImPACT composite scores significantly lower than expected after 10 days, even though the symptoms had resolved after 5 days. A more recent study using ANAM found that several subtest scores differentiated mild from moderate concussions on the day of injury but not at 8 days post injury (Prichep et al., 2013).
The two meta-analyses noted above also examined the ability of neuropsychological tests to measure changes in cognitive function through recovery. Belanger and Vanderploeg (2005) found significant improvement between days 7 and 10 for verbal memory retention scores only. Broglio and Puetz (2008) examined how the effects of concussion were manifested in three assessment modalities: the SAC, paper-and-pencil batteries, and computerized batteries. They found significant effects of concussion on the scores of all three assessment modalities immediately after injury as well as reduced but still large effects for the cognitive assessment at 14 days post injury interval. The type of cognitive assessment was determined to be a moderator effect, as was the time from the injury to the assessment. The largest effect was seen for the SAC immediately after injury, with the paper-and-pencil batteries having significantly greater effects than the SAC or computer batteries at 14 days.
Summary There is a long history of neuropsychological tests being used to track recovery from brain injury as they are thought to reflect functional cognitive recovery. Group studies of individuals with sports-related concussions have shown that neuropsychological test scores improve as the time from injury increases. Some studies have found continued cognitive declines on neuropsychological testing, even after individuals’ concussion symptoms have resolved, although other studies show symptoms lasting longer than cognitive declines. The persistence of cognitive declines following symptom resolution in some individuals suggests there may be a role for neuropsychological testing in concussion management, for example, to help inform return-to-play decisions in these cases. Such a role for computerized neuropsychological testing has been criticized, however, on the grounds that there currently is no evidence to show that delaying an individual’s return to full physical activity on the basis of residual neurocognitive deficits actually improves recovery outcomes or reduces the risk of subsequent injury (Kirkwood et al., 2009; Randolph and Kirkwood, 2009).
Are Computerized Tests Valid and Reliable?
All neuropsychological tests require standardized administration and expert interpretation of results. Assuming that these conditions are met, test effectiveness is typically determined by several factors: Is it reliable (does it produce consistent results each time it is administered), is it valid (do the test scores represent the construct of interest, e.g., working memory), and does it measure individuals with respect to the construct of interest (i.e., specific cognitive functions, diagnostic efficiency)? Test developers attempt to show that their tests meet these criteria, but a fourth aspect is also important: Does independent research obtain the same results as the test developers’ research? Computerized test batteries are not unique to sports neuropsychology, but it is important to examine their role in concussions because of how extensively they are used.
A complete neuropsychological assessment of the multiple cognitive functions of an individual can take between 4 and 8 hours (Lezak et al., 2012). Screening tools that focus on functions typically affected by brain injuries were developed to reduce the length of the typical neuropsychological batteries and to focus on identifying acute cognitive dysfunction. Such targeted batteries also made larger-scale testing feasible, which in turn created the opportunity to implement the Sports as a Laboratory Assessment Model (SLAM) for sports-related concussion.
Collie and colleagues (2001) raised concerns about paper-and-pencil testing that centered on interrater reliability issues, the general lack of alternative forms, and the effect of practice in repeat testing. McCrory and colleagues (2005) noted that computerized testing offered advantages such
as standardized and randomized presentation of stimuli, shorter administration time, central data storage, and more sensitive and accurate detection of reaction times. Furthermore, standard paper-and-pencil tests did not typically have normative standards developed specifically for athletes, and computerized tests allowed for easier repeat (serial) testing to track cognitive recovery. Indeed, an entire industry, with its corresponding potential financial conflicts of interest, has developed around providing baseline and serial post-injury testing to thousands of athletes. By 2003, the brief paper-and-pencil test battery was becoming replaced by computerized test batteries such as ImPACT, CogSport, ANAM, and CRI (see, e.g., Cernich et al., 2007; Collie et al., 2003; Collins et al., 2003b; Erlanger et al., 2003).
Between 1999 and 2002 there were 10 studies using paper-and-pencil batteries and only one using computer testing; between 2003 and 2008 there were 8 studies utilizing paper-and-pencil batteries and 15 using computer testing (Comper et al., 2010). Thus, in terms of research, there was a dramatic shift in focus. The shift in research focus also appears to have been mirrored by practice. In 2009, Covassin and colleagues reported that 95 percent of the 266 athletic trainers who participated in a survey said they administered baseline computerized neurocognitive testing to their athletes. However, only 51.9 percent examined the baseline test validity indices. The researchers concluded that the athletic trainers in the study appeared to rely more on symptoms than on neurocognitive test scores when making return-to-play decisions (Covassin et al., 2009). When Meehan and colleagues (2011) reviewed data from the High School RIO™ database of athletic injuries for the 2009-2010 school year (1,056 sports-related concussions), they found that computerized neuropsychological testing was used for 41.2 percent of concussions. Although there are concerns with the use of such testing, it continues to represent a large portion of concussion management activity. At this point, all of the computerized tests have some peer-reviewed research to support their use.
Psychometric tests are judged on their reliability and validity as documented in their manuals and published studies. Reliability is usually assessed as a test-retest correlation or in terms of an intraclass correlation coefficient (ICC). A Pearson correlation can be a valid estimator of interrater reliability (i.e., test-retest reliability), but only when there are meaningful pairings between two and only two raters. A test of internal stability (Chronbach’s alpha) is a test of the function of the number of test items and the average intercorrelation among the items (see Anastasi and Urbina, 1997). These are statistical tests that provide information about the ability of the test to maintain its performance and psychometric characteristics over time.
Evidence to support test interpretation (validity) may come from various forms: evidence based on test content, evidence based on response pro-
cesses, evidence based on internal structure, evidence based on relations to other variables, and evidence based on the consequences of testing. Establishing validity is seen as a long-term process, and no one study can make that determination. Test development practice calls for documentation of some form of reliability and validity (see AERA et al., 1999). All of the major computerized tests have demonstrated some level of reliability and validity. Other aspects of their structure may make them more suitable for some situations than others, and practitioner preference, experience, and knowledge are important factors. It should be noted that the Department of Defense currently uses ANAM to assess post-concussion neurocognitive changes in service members in all branches of the military. Table 3-5 outlines the basic features of several of the currently available computerized tests.
Reliability of computerized tests The ability of a test to perform consistently is important to having confidence in its scores. Table 3-6 lists published reliability studies of several different computerized neuropsychological tests used in concussion management. Several approaches to reliability can be taken: Internal consistency can be measured using Chronbach’s alpha test or one can examine the correlation between half of the items and the other half (split-half reliability). Test-retest reliabilities are used to determine consistency across test administration: a Pearson correlation or an ICC can be calculated. The ICC has become the preferred measure as it is a type of interrater reliability. However, there is no agreement on the minimum ICC value that is considered “acceptable” for computerized neuropsychological tests. Some authors find a minimum correlation of 0.60 to be acceptable (e.g., Baumgartner and Chung, 2001; Weir, 2005), while others employ a higher standard of 0.70 (e.g., Anastasi and Urbina, 2007) and still others may consider 0.80 or 0.90 to be the mark of a good, reproducible automated test.
As Table 3-6 demonstrates, ICCs for different composite scores within tests are quite variable, and low intraclass correlations are frequently found. If there is a trend across tests, it appears to be that speeded tests have better reliability than do tests of other functions such as memory. This may have to do with the inherent nature of computerized tests and the manner in which tasks must be presented in this format.
Reliability studies are quite variable, with some studies demonstrating adequate reliability and some indicating less than adequate reliability. There are many possible reasons for the variability, including different sample sizes, unknown testing conditions, and variable item pools. Most computerized tests produce multiple forms through a quasi-randomization of items. All of the commercial test batteries that were reviewed had some studies indicating acceptable reliability. Tests involving speed appear to be
more reliable than those involving memory or accuracy. This may be due to computer-format constraints. Clinicians and researchers need to be aware of the variability in reliability studies with these tools.
Validity of computerized tests The presentation format of a computer-based test presents different limitations and strengths than those of paper-and-pencil testing. For instance, memory is a complex function and computerized tests of memory are limited to recognition formats. This format limitation may be one reason for the difficulty in isolating specific cognitive functions, as there may be overlap between (for example) processing speed and working memory (Maerlender et al., 2010). However, answering questions about identification and recovery may not require such construct specification.
As the previous sections document, a large number of studies have demonstrated the various aspects of validity of these computerized batteries. Table 3-7 lists published validity studies of several different computerized neuropsychological tests used in concussion management. Concurrent validity (comparing the scores from one test to those from another similar test) and criterion and predictive validity (predicting a criterion such as the diagnosis of concussion) are the most frequently cited methods of establishing validity. Construct validity attempts to establish the underlying cognitive mechanisms that the test is actually measuring (e.g., memory, attention). There is overlap in these types and methods for understanding validity.
Concurrent validity has been demonstrated for each of the batteries when compared with paper-and-pencil neuropsychological tests. Most studies show high correlations with tests thought to measure similar constructs. Only two studies mention the discriminating ability of the tests, that is, whether a particular test shows low correlations with other tests that it should not be highly correlated with. For example, although the ImPACT test has high correlations between the composite scores and similar paper-and-pencil tests (convergent construct validity), the same sample showed high correlations with dissimilar paper-and-pencil measures (Maerlender et al., 2010). On the other hand, Newman and colleagues (2013) found that the new Pediatric ImPACT test showed good discrimination between speed of processing and memory tests. Using a factor-analytic approach, Allen and Gfeller (2011) also demonstrated construct validity for ImPACT. ANAM (Bleiberg et al., 1997, 2000, 2004; Prichep et al., 2013), CogSport (Collie et al., 2003; Makdissi et al., 2010; Moriarity et al., 2012), and CRI (Erlanger et al., 2003) also have been shown to possess various types of validity.
In group studies, neuropsychological test scores have generally not been shown to predict prolonged recovery. Most recently, McCrea and colleagues
TABLE 3-5 Common Computerized Neuropsychological Tests
| Test Name | Age Range | Time to Administer | Functions Assessed | Other |
| Automated Neuropsychological Assessment Metrics (ANAM) 4 Traumatic Brain Injury battery (Eonta et al., 2011; VistaLife Sciences, 2013) | Not given | 20-25 minutes | Simple reaction time, code substitution, procedural reaction time, mathematical processing, matching to sample, code substitution delayed | Demographics, sleep scale, mood scale; pseudorandomized items; embedded effort measure included with the ANAM Performance Report |
| ANAM Sports battery (Cernich et al., 2007; Reeves et al., 2007) | 17-65 | 20-25 minutes | Simple reaction time, code substitution learning, running memory continuous performance task, mathematical processing, delayed matching to sample, code substitution delayed memory test, spatial processing, Sternberg procedure, procedural reaction time | Demographics module, Modified Stanford Sleepiness Scale, pseudorandomized items; “throughput score” is a speed-versus-accuracy measure |
| CNS Vital Signs (CNS Vital Signs, 2013; Gualtieri and Johnson, 2006) | 8-90 | 25-30 minutes (Brief Core battery) | Composite memory, verbal memory, visual memory, psychomotor speed, reaction time, complex attention, cognitive flexibility, processing speed, executive function, simple attention, motor speed | General purpose neuropsychological test developed for drug trials but used in neuropsychiatric clinics; no studies available that assess sports concussions, although materials indicate it is valid and reliable for that purpose; performance validity measure |
| Concussion Vital Signs (CNS Vital Signs, 2013; Concussion Vital Signs, 2013) | 8-90 | 25-30 minutes | Verbal memory, visual memory, psychomotor speed, executive function, cognitive flexibility, continuous performance task correct responses, reaction time | Concussion version of CNS Vital Signs; performance validity measure |
| CogSport/Axon/Computerized Cognitive Assessment Tool (CCAT) (Axon Sports, 2013; Falleti et al., 2006) | Not given | 15-20 minutes | Processing speed, attention, learning, working memory | Basic demographics |
| Concussion Resolution Index (CRI)/ Headminder (Erlanger et al., 2001, 2003) | 13-35 | 25-30 minutes | Processing speed, simple reaction time, complex reaction time | Basic demographics and health history |
| Immediate Post-Concussion Assessment and Cognitive Testing (ImPACT) (ImPACT, 2013) | 12-60 | 20-25 minutes | Composite scores: verbal memory, visual memory, visual-motor speed, reaction time | Background and basic health information; symptoms assessment; calculates post-injury change in reliable change index metrics; has baseline test validity indicators |
| Pediatric ImPACT (Gioia et al., 2013a; Newman et al., 2013) | 5-12 | Symptom scale, response speed, learning and memory accuracy | Validity indicators; regression-based reliable change metrics built in | |
TABLE 3-6 Reliability Studies on Common Neuropsychological Tests
| Test | Study Author | N/population |
| Automated Neuropsychological Assessment Metrics (ANAM) | Segalowitz et al., 2007 | 29 adolescents, age 15 |
| ANAM | Cernich et al., 2007 | Review of previous tests; U.S. Military Academy cadets |
| ANAM4 | Cole et al., 2013a | 50 active duty military, predominantly male (83%); ages 19-59 (mean 34) |
| CogSport | Collie et al., 2003 | 60 healthy youth |
| Subtest | Statistic/Reliability | Test Intervals | Comment |
| Matching to Sample | ICC=.72 r=.72 | 2 times over 1-week interval | |
| Continuous | |||
| Performance | ICC=.65 r=.70 | ||
| Math Processing | ICC=.61 r=.71 | ||
| Code Substitution | ICC=.58 r=.81 | ||
| Simple Reaction | |||
| Time | ICC=.44 r=.48 | ||
| Simple Reaction | |||
| Time 2 | ICC=.47 r=.50 | ||
| Code Substitution | |||
| Delayed | ICC=.68 r=.67 | ||
| Matching to Sample | ICC=.66 | 166 days | |
| Continuous | |||
| Performance | ICC=.58 | ||
| Math Processing | ICC=.87 | ||
| Simple Reaction | |||
| Time | ICC=.38 | ||
| Spatial Processing | ICC=.60 | ||
| Sternberg Memory | ICC=.48 | ||
| Matching to Sample | r=.69; ICC=.67 | 21-42 days | Sample likely is not comparable to youth athletics |
| Procedural Reaction | |||
| Time | r=.62; ICC=.51 | ||
| Math Processing | r=.70; ICC=.70 | ||
| Simple Reaction | |||
| Time | r=.65; ICC=.60 | ||
| Simple Reaction | |||
| Time repeated | r=.41; ICC=.40 | ||
| Code Substitution | |||
| Learning | r=.79; ICC=.79 | ||
| Code Substitution | |||
| Memory | r=.68; ICC=.59 | ||
| speed indices | ICC 1 hr.=.69, 1 week=.90 | 1 hour, 1 week | |
| accuracy indices | ICC 1 hr.=.08, | ||
| 1 week=.51 | |||
| Test | Study Author | N/population |
| CogSport | Straume-Naesheim et al., 2005 | 232 male professional soccer players (Norwegian and Spanish) ages 17-35 |
| Concussion Sentinel (CogSport) | Broglio et al., 2007cb | 73 high school |
| CogSport | Faleti et al., 2006 | 45 adults, ages 18-40 |
| CogState v5.6 | Cole et al., 2013a | 53 active duty military, predominantly male (83%); ages 19-59 (mean 34) |
| Subtest | Statistic/Reliability | Test Intervals | Comment |
| Simple Reaction | Immediate | Sample is somewhat atypical for sports concussion management | |
| Time | ICC=.73 | ||
| Choice Reaction | |||
| Time | ICC=.65 | ||
| Complex Reaction | |||
| Time | ICC=.69 | ||
| Monitoring | ICC=.45 | ||
| 1-back Monitoring | ICC=.71 | ||
| Matching | ICC=.69 | ||
| Learning | ICC=.79 | ||
| Working Memory | ICC 45 days=.65; | T1 to T2: 45 days; | |
| 5 days later=.64 | T2 to T3: 5 days | ||
| Reaction Time | ICC 45 days=.60; | ||
| 5 days later=.55 | |||
| Decision Making | ICC 45 days=.56; | ||
| 5 days later=.63 | |||
| Attention | ICC 45 days=.43; | ||
| 5 days later=.39 | |||
| Matching | ICC 45 days=.23; | ||
| 5 days later=.66 | |||
| Simple Reaction | T1-2, T2-3, T3-4, | T1, T2, T3, T4 at | Model and |
| Time Choice Reaction | T4-5 ICC>.73 | 10-minute intervals, T4-5 at 1 week interval | form of ICC not provided. These ICCs are for the reaction times; very few ICCs were >.60 for accuracy measures |
| Time | T3-4, T4-5 ICC>.71 | ||
| Complex Reaction | |||
| Time | T2-3, T3-4, T4-5 ICC>.64 | ||
| Monitoring | T2-3, T3-4, ICC>.68 | ||
| 1-back Monitoring | T1-2, T2-3, T3-4, T4-5 ICC>.62 | ||
| Matching | T1-2, T2-3, T3-4, T4-5 ICC>.71 | ||
| Incidental Learn | T3-4, T4-5 ICC>.60 | ||
| Associative Learn | T1-2, T2-3, T3-4, T4-5 ICC>.77 | ||
| Detection Speed | r=.77; ICC=.78 | 21-42 days | Sample is atypical for sports-related concussion management |
| Identification Speed | r=.78; ICC=.77 | ||
| One Card Learning | |||
| Accuracy | r=.25; ICC=.22 | ||
| One Back Speed | r=.76; ICC=.74 | ||
| Composite | r=.80; ICC=.79 | ||
| Test | Study Author | N/population |
| Concussion Resolution Index (CRI) | Broglio et al., 2007cb | 73 high school |
| CRI | Erlanger et al., 2003 | 414, ages 13-35 |
| CRI | Erlanger et al., 2002 | 46-49, ages 18-29 |
| Immediate Post-Concussion Assessment and Cognitive Testing (ImPACT) | Iverson et al., 2003 | 29 males and 27 females, average age 17.6 years |
| ImPACT | Elbin et al., 2011 | 369 high school varsity athletes |
| ImPACT | Miller et al., 2007 | 58 Division III college football |
| Subtest | Statistic/Reliability | Test Intervals | Comment |
| Simple Reaction | ICC 45 days =.15; | T1 to T2: 45 days; | |
| Time Error | 5 days later=.03 | T2 to T3: 5 days | |
| Complex Reaction | ICC 45 days=.43; | ||
| Time | 5 days later=.66 | ||
| Complex Reaction | ICC 45 days=.26; | ||
| Time Error | 5 days later=.46 | ||
| Processing Speed | ICC 45 days=.66; | ||
| Index | 5 days later=.58 | ||
| Processing Speed | r=.82 | 2 week | Authors noted that reliabilities for the sample under 18 years were “with a trend of lower reliability scores in the sample under 18 years of age” (pp. 306-307) |
| Simple Reaction | |||
| Time | r=.70 | ||
| Complex Reaction | |||
| Time | r=.68 | ||
| Processing speed factor | r=.78 | Random 1 to 110 days | Practice effects significant for Processing Speed only |
| Response speed factor | r=.80 | ||
| Memory factor | r=.68 | ||
| Attention factor | r=.74 | ||
| Verbal Memory | r=.70 | 1 week | Significant practice effects for Visual-Motor Speed |
| Visual Memory | r=.67 | ||
| Visual-Motor Speed | r=.89 | ||
| Reaction Time | r=.79 | ||
| Verbal Memory | ICC=.62 | 1.2 year | |
| Visual Memory | ICC=.76 | ||
| Visual-Motor Speed | ICC=.85 | ||
| Reaction Time | ICC=.76 | ||
| Significant practice effects for Visual Memory and Visual-Motor Speed composites only | Preseason, mid-season, end of season | Raw scores at each time-point compared | |
| Test | Study Author | N/population |
| ImPACT | Schatz, 2010 | 95 collegiate athletes |
| ImPACT | Broglio et al., 2007cb | 73 high school |
| ImPACT | Schatz and Ferris, 2013 | 25 undergraduates, no concussion history |
| ImPACT | Cole et al., 2013a | 44 active duty military predominantly male (83%); ages 19-59 (mean 34) |
| ImPACT | Register-Mihalik et al., 2012 | 20 high school, 20 college (male=female) |
| Subtest | Statistic/Reliability | Test Intervals | Comment |
| Verbal Memory | ICC=.46 | 2 year | |
| Visual Memory | ICC=.65 | ||
| Visual-Motor Speed | ICC=.74 | ||
| Reaction Time | ICC=.68 | ||
| Verbal Memory | ICC 45 days=.23; 5 days later=.40 | T1 to T2: 45 days; T2 to T3: 5 days | Serial testing of three batteries, one after the other; few expected practice effects |
| Visual Memory | ICC 45 days=.32; 5 days later=.39 | ||
| Visual-Motor Speed | ICC 45 days=.38; 5 days later=.61 | ||
| Reaction Time | ICC 45 days=.39; 5 days later=.51 | ||
| Verbal Memory | ICC=.79; r=.66 | 4 weeks | Has a table comparing ICC and r across five studies Only visual memory showed significant practice effects |
| Visual Memory | ICC=.60; r=.43 | ||
| Visual-Motor Speed | ICC=.88; r=.63 | ||
| Reaction Time | ICC=.77; r=.63 | ||
| Verbal Memory | r=.61; ICC=60 | 21-42 days | All showed improvement from T1 to T2, except RT; sample is atypical for sports-related concussion management |
| Visual Memory | r=.49; ICC=50 | ||
| Visual-Motor Speed | r=.86; ICC=.83 | ||
| Reaction Time | r=.53; ICC=.53 | ||
| Verbal Memory | ICC (T1-T2)=.29; r’s T1-T2, T2-T3, NS; T1-&3 r p=.013 | 3 times each 24 hours apart | Significant practice effect for Visual-Motor Speed only, no age effects |
| Visual Memory | ICC (T1-T2)=.45; T1-T2, T2-T3 r p’s <.002, T1-T3 r p=.023 | ||
| Visual-Motor Speed | ICC (T1-T2)=.71; all r p’s <.001 | ||
| Reaction Time | ICC (T1-T2)=.60; all r p’s <.001 | ||
| Impulse Control | ICC (T1-T2)=.6; all r p’s <.05 | ||
| Test | Study Author | N/population |
| ImPACT | Resch et al., 2013 | 2 groups college n=45, n=46 |
| Pediatric ImPACT | Gioia et al., 2013b | 705, ages 5-12 |
| CNS Vital Signs | Cole et al., 2013a | 39 active duty military, predominantly male (83%); ages 19-59 (mean 34) |
aSame study, different subjects; demographics for overall sample.
bSame study
NOTES: ICC = intraclass correlation coefficient, T = time.
(2013) analyzed data obtained from 570 high school and college athletes with concussions at several time-points after injury. The study divided the athletes into groups in which symptoms had resolved within 7 days (typical) and had lasted more than 7 days (prolonged recovery). Neuropsychological test scores at less than 2 days post injury were not predictive of which recovery group an athlete would be in. This finding was similar to findings in the two meta-analytic studies described previously (Belanger and Vanderploeg, 2005; Broglio and Puetz, 2008). It should be noted that because in 90 percent of concussion cases the individuals recover by the end of 2 weeks (typical), group analyses may obscure the effects in those 10 percent of cases in which scores continue to suggest injury.
| Subtest | Statistic/Reliability | Test Intervals | Comment |
| Verbal Memory | Both Groups, all intervals ICC<.59 | Group 1: T1 to T2=7 days, | Used a one-way random effects model (atypical) |
| Visual Memory | Group 1 ICC.26, .53, .85; Group 2 ICC .52-.55 | T2 to T3=7days, T1 to T3=14 days Group 2: | |
| Visual-Motor Speed | Both Groups, all intervals ICC>.66 | T1 to T2=45 days, T2 to T3=5 days, T1 to T3=50 days | |
| Reaction Time | Group 1 all intervals >.78; Group 2 .57, .49, .71 | ||
| Response speed | r=.97 | ||
| Memory | r=.53; ICC=.54 | 21-42 days | Sample is atypical for sports-related concussion management |
| Verbal Memory | r=.34; ICC=.29 | ||
| Visual Memory | r=.48; ICC=.47 | ||
| Psychomotor Speed | r=.77; ICC=.72 | ||
| Reaction Time | r=.78; ICC=.75 | ||
| Complex Attention | r=.79; ICC=.79 | ||
| Cognitive Flexibility | r=.71; ICC=.62 | ||
| Processing Speed Executive | r=.68; ICC=.63 | ||
| Functioning | r=.73; ICC=.64 | ||
| Neurocognitive Index | r=.76; ICC=.70 | ||
Summary All of the computerized neuropsychological test batteries present some evidence of concurrent validity with traditional paper-and-pencil tests. Direct comparisons between tests provide some strong relationships, typically for the speeded tests rather than the memory tests. Within-battery reliabilities tend to be better for speeded tests as well. The CRI does not include a memory component. CogSport has demonstrated good reliability for working memory speed, but not for accuracy.
The generally poorer performance of “memory” tasks is unfortunate because working memory has long been identified as a significant cognitive function that declines in all forms of TBI; the poorer performance may be a function of the computer presentation of the tests. The trend of speeded
TABLE 3-7 Validity Studies on Common Neuropsychological Tests
| Test | Study Author | Age Range | Subjects (n) |
| Automated Neuropsychological Assessment Metrics (ANAM) | Bleiberg et al., 1997 | 6 concussed, 6 control | |
| ANAM | Bleiberg et al., 2000 | High school, college | 122 high school and college |
| ANAM | Bleiberg et al., 2004 | College | 68 concussed of 729; 18 controls tested at same interval |
| ANAM | Prichep et al., 2013 | 15-23 years | 65 concussed |
| ANAM | Register-Mihalik et al., 2013b | College | 132 concussed |
| ANAM | Woodard et al., 2002 | High school, non-concussed | |
| Type of Validity | Comparisons | Findings |
| Concurrent | ANAM with H-R plus other tests | Too few subjects for meaningful interpretation |
| Concurrent | Trail Making Test Part B, Auditory Consonant Trigrams total score, Paced Auditory Serial Addition test (PASAT), Hopkins Verbal Learning test, Stroop Color-Word test | PASAT r Mathematical Processing=.66; PASAT r with Sternberg Memory=.45; PASAT r with Spatial Processing=.33; Trails B r Matching to Sample=.50 //PASAT & Trails B correlated with Mathematical Processing, Sternberg Memory, Spatial processing, and Matching to Sample |
| Predictive | Test intervals: 0 to 23 hours, 1 to 2 days, 3 to 7 days, and 8 to 14 | <24 hour: Spatial Processing p<.01; Mathematical Processing <.05; 1-2 d Spatial Processing <.05/ no other findings |
| Predictive | Moderate versus severe concussion | At the time of injury, athletes with moderate concussion performed significantly worse than athletes with mild concussion on ANAM Code Substitution-Delayed, Code Substitution, Matching to Sample, Simple Reaction Time and Simple Reaction Time 2 subtests (p<0.05) |
| Predictive | Percent exceeding reliable change index; reliable change index values based on separate healthy sample | Sensitivity at 80%, 90%, and 95% all <15%; specificity >90% |
| Concurrent | Healthy athletes ANAM and paper-and-pencil tests | Significant correlations between individual ANAM scores and Hopkins Verbal Learning test, Controlled Oral Word Association test, Digit Symbol Substitution test, Symbol Search |
| Test | Study Author | Age Range | Subjects (n) |
| CogSport | Collie et al., 2003 | 240 elite Australian rules football players | |
| CogSport/Axon | Makdissi et al., 2010 | 16-35 years, median=22 years | 88 concussed Australian rules football |
| CogSport/ Axon | Moriarity et al., 2012 | Amateur boxers | |
| CogSport | Schatz and Putz, 2006 | 18-23 | 30 college students |
| Immediate Post-Concussion Assessment and Cognitive Testing (ImPACT) | Iverson et al., 2005 | Mean age 17 years | 72 amateur |
| ImPACT | Iverson et al., 2004 | None given | 25 amateur |
| Type of Validity | Comparisons | Findings |
| Concurrent | Trails, Digit Symbol Substitution test; ICCs calculated from z-scores | ICCs stronger for Digit Symbol than Trails; speed scores better than accuracy |
| Predictive | Trails B, Digit Symbol, and CogSport; symptomatic versus asymptomatic at time of testing | Both CogSport and paper-and-pencil showed more reliable change index changes for symptomatic than asymptomatic; significantly more athletes showed reliable change index changes on CogSport than paper- and-pencil for both |
| Predictive | Baseline to post bout | 2 of 96 had low scores but no concussion; not clear what the conclusion was; some took baseline tests in dorm room |
| Concurrent | Significant correlations (p<.05) Simple Reaction Time: no significant r; Complex Reaction Time to ImPACT Reaction Time r=.649; to Trails A r=.544; to Trails B r=.535; Memory to CogSport Learning r=.723 | Complex Reaction Time correlated with paper-and-pencil and ImPACT |
| Concurrent | Tested within 21 days of concussion; correlated with Symbol Digit Modalities | All composites and symptom total significantly correlated with Symbol Digit Modalities |
| Concurrent-construct | Tested within 20 days of injury; Brief Visual Memory test, Trail Making, Symbol Digit Modalities | Symbol Digit Modalities and Brief Visual Memory tests delayed significantly correlated with all 4 ImPACT composites. Both Trails correlated with processing speed |
| Test | Study Author | Age Range | Subjects (n) |
| ImPACT | Schatz et al., 2006 | High school | 72 concussed athletes |
| ImPACT | Schatz and Putz, 2006 | 18-23 | 30 college students |
| ImPACT | Schatz and Sandel, 2013 | High school and college | 81 concussed symptomatic athletes; 37 concussed asymptomatic athletes, ages 13-21 |
| ImPACT | Tsushima et al., 2013 | High school | 26 concussed versus 25 controls |
| ImPACT | Maerlender et al., 2010 | College | 54 non-concussed |
| Type of Validity | Comparisons | Findings |
| Predictive | 72 concussed (within 72 hours of injury) compared to 66 controls | Significant differences between groups on all ImPACT composites and symptoms; 1 discriminant function included Visual Memory, Processing Speed, Impulse Control and symptom total: sensitivity=82%, specificity=89% |
| Concurrent | Significant correlations (p<.05) Complex Reaction Time to Headminder r=.407; to CogSport r=.649; to Trails A r=.641; to Trails B r=.442; to Digit Symbol r=–.455 Memory no significant r Processing Speed to Headminder r=–.373 | Speed tests show correlations with paper-and-pencil and other computer tests; memory tests do not correlate (no memory tests in paper-and-pencil battery) |
| Predictive | 81 concussed evaluated within hours of injury compared to 81 controls’ baseline testing; also compared scores of 37 symptomatic athletes to asymptomatic athletes to 37 matched controls | Symptomatic athletes: Sensitivity=.75; specificity=.89; PPP=.91, NPP=.69; Asymptomatic: Sensitivity, Specificity, PPP, NPP=.97 (only 2 cases were misclassified) Sample was well characterized and clean (no learning disability, attention deficit hyperactivity disorder) |
| Criterion | Score comparisons at 6 days | No difference in test scores at 6 days, significant difference in symptoms; authors felt it replicated previous findings of no test score difference at 7 days (6) Very small n, no control for baseline, so amount of actual change may be obscured |
| Convergent, concurrent, construct | ImPACT to paper-and-pencil and to in-scanner behavioral tests | High correlations between similar measures for all 4 composites |
| Test | Study Author | Age Range | Subjects (n) |
| ImPACT | Maerlender et al., 2013 | College | 54 non-concussed (same sample as 2010 study) |
| ImPACT | Allen and Gfeller, 2011 | College | 100 non-concussed |
| Pediatric ImPACT | Newman et al., 2013 | 5-12 years | 164 concussed |
| Pediatric ImPACT | Gioia et al., 2013a | 5-12 years, <7 days post concussion | 22 ages 5-7, 67 ages 8-12 |
| Concussion Resolution Index (CRI) | Erlanger et al., 2003 | 13-35 years | 414 |
| Type of Validity | Comparisons | Findings |
| Discriminant, concurrent, construct | ImPACT to paper-and-pencil and to in-scanner behavioral tests | Poor discriminant validity for 3 or 4 composites–high correlations with dissimilar paper-and-pencil measures, except for reaction time |
| Construct | Factor analysis of ImPACT and paper-and-pencil battery | Five ImPACT factors accounted for 69 percent of variance; significant correlations between ImPACT composites and paper- and-pencil tests (except impulse control) |
| Concurrent, construct | Tested an average of 12 days from injury; correlations with paper-and-pencil and fluency tests | Response Speed Composite r: Digit Span, forward and backward, Auditory Consonant Trigrams, Symbol Digit memory; Response Speed Composite was more strongly associated with traditional speed measures than it was with the Learning and Memory Composite, indicating relative independence of the Response Speed and Learning and Memory Accuracy |
| Criterion, predictive | Response speed and symptoms by age | Response speed and symptoms together correctly classified by age |
| Concurrent | CRI factors correlated with paper-and-pencil tests (Processing Speed, Simple Reaction Time, Complex Reaction Time) | Symbol Digit Modalities and Grooved pegs (bilateral) correlated with all three factors; Trails A correlated with Simple and Complex Reaction Time; Trails B and Stroop interference correlated with Processing Speed; Digit Symbol (WAIS-III) correlated with Simple Reaction Time |
| Test | Study Author | Age Range | Subjects (n) |
| CRI | Erlanger et al., 2002 | 18-87 years | 66 out of a larger sample |
| CRI/Head-minder | Schatz and Putz, 2006 | 18-23 | 30 college students |
NOTES: ICC = intraclass correlation coefficient, NPP = negative predictive power, PPP = positive predictive power.
tests showing better performance than the accuracy measures may be reflecting the strengths of the computerized platform.
Does Baseline Testing Improve the Utility of Neuropsychological Testing in the Diagnosis and Management of Sports-Related Concussion?
Baseline testing has become commonplace and often is considered an invaluable part of sports concussion management as it allows for more accurate interpretation of post-injury scores (McCrory et al., 2005). In 2011, Congress mandated that the Department of Defense develop and implement a comprehensive policy on consistent neurological cognitive assessments of service members before and after deployment (P.L. 111-383, sec. 722). The Department of Defense now mandates pre-deployment baseline testing to be performed on all service members within 12 months of their deployment (DoD, 2013). Comparing a post-injury score to an individual’s baseline allows a comparison that controls for many of the individual factors that can affect test performance, and several papers have called for its (continued) use (Barth et al., 1989; Gardner et al., 2012; Hinton-Bayre et al., 1997,
| Type of Validity | Comparisons | Findings |
| Concurrent | 4 factors identified (Response Speed, Processing Speed, Memory, Attention) and correlated with paper-and-pencil tests | Symbol Digit Modalities correlated with all four factors; Symbol Search and Digit Span correlated with Response Speed, Processing Speed, Reaction Time; Bushke Selective Reminding correlated with Response Speed, Memory, Attention; Trails A and B correlated with Response Speed |
| Concurrent | Significant correlations (p<.05) Simple Reaction Time to Trails A r=.428; to Digit Symbol r=–.526 Complex Reaction Time no significant r Processing Speed to Trails B r=.601; to Digit Symbol r=–.610; to ImPACT r=–.373 | Simple Reaction Time and processing speed correlate with paper-and-pencil and ImPACT |
1999; Lovell and Collins, 1998). Only a few empirical studies have examined the potential benefit of using baseline test scores instead of comparing post-injury scores to normative standards. Baseline testing is costly and, as indicated previously, is not without its logistical and administration problems, which can sometimes lead to questionable results. Furthermore, the use of baseline testing automatically presumes repeat testing; with that, appropriate statistical procedures are needed for interpreting results (Heilbronner et al., 2010; McCrory et al., 2005). Test scores are known to “regress to the mean” after multiple exposures, practice effects can inflate scores, and baseline scores on the extremes of the distribution will have different effects with repeat testing. Although having different “forms” of a test (different items) reduces the test taker’s ability to memorize responses, the test procedures are the same, so practice increases test familiarity, which can enhance performance.
Schmidt and colleagues (2012) analyzed retrospective data for 1,060 collegiate athletes with baseline neuropsychological test (ANAM), balance, and symptom checklist results. The study used reliable-change methodology for the baseline comparisons and difference from mean baseline score
for the normative comparison. An analysis of variance comparing the number of correct identifications between methods found that the baseline comparison was significantly better (fewer misidentifications) for a reaction time score, and the normative comparison was better for a mathematical reasoning score. The authors noted that individual differences in baseline performance on math processing may have caused the high rate of misidentifications. This is a drawback of the reliable-change method as opposed to a regression-based method. No other significant neuropsychological score disagreements were observed, nor were there any score disagreements for postural control or symptom severity.
Summary Baseline testing has been called for and recommended for many years. It was a cornerstone of Barth’s original SLAM model and has been seen as an answer to the limitations of normative comparisons for detecting clinical change. However, very few studies have specifically examined the value of baseline testing, and establishing the validity of baseline testing is difficult. The consensus statement from the Fourth International Conference on Concussion in Sport held in Zurich has taken the lack of evidence for baseline testing as an indication that baseline testing should not be required (McCrory et al., 2013b). Baseline testing is a common practice in schools and programs for many sports (Covassin et al., 2009), and it has a theoretical foundation. On the other hand, there are drawbacks to conducting large-scale baseline assessments; as Moser and colleagues (2011) have pointed out, group testing has its disadvantages. In addition, baseline testing is expensive and time-consuming, and there is the question of whether the use of baseline testing in concussion management actually reduces risks of recurrent injury or long-term functional deficits.
Randolph and Kirkwood (2009) provided a comprehensive review of the evidence to that date regarding the use of different strategies in sports concussion management. They acknowledged that few prospective studies had been done regarding risks and means for minimizing them. Their review of the literature on football concussions (as the paradigmatic sport) noted potential risks of death or permanent disability, delayed recovery, same-season repeat concussion, and the late-life consequences of multiple concussions. They observed that catastrophic outcomes associated with sports-related concussion are extremely rare, and less serious short-term adverse outcomes also are rare and generally transient. In addition, they argued that current management strategies, including baseline testing, did not modify these risks. The same group followed up with a critique of baseline testing specifically. They argued that the utility of using baseline tests rests on the function (real-world) outcomes derived from the procedure. They note:
The primary justification for the baseline method is that it helps to ensure that athletes are fully recovered from a concussion and are therefore “safe” to [return to play]. At present, however, little to no empirical evidence is available to demonstrate that such testing actually reduces any known risk associated with concussive injury. (Kirkwood et al., 2009, p. 1410)
The 2013 position statement of the American Medical Society for Sports Medicine states that most concussions can be managed appropriately without neuropsychological testing and also notes the lack of evidence that use of baseline testing in the clinical management of concussions improves short- or long-term outcomes (Harmon et al., 2013).
Summary
Neuropsychological testing has been an important element of clinical practice in traumatic brain injury research and practice for many years. Its adoption into the sports concussion field is thus based on a considerable history. The temporal aspects of concussions, together with the potential consequences of improper behavior management, create the need for effective and efficient tools with strong psychometric foundations. However, these demands create challenges for tests and test interpretations. Furthermore, changes in knowledge and the development of newer tools have led to the need for more sophisticated analytic procedures and more nuanced interpretations. Although the quality of the studies varies, the tests reviewed here have some level of validity; reliability is even more variable, however, and users must be aware of the limitations that these studies imply. Even though computerized neuropsychological tests are easy to obtain and administer, the many factors that affect test interpretation along with the need for technical expertise in understanding test scores as they relate to individual cases together make it important that neuropsychologists or other professionals with training and expertise in neuropsychological testing and concussion management provide test interpretation.
Research on the effectiveness of neuropsychological tests in the identification and management of sports concussions is mixed. Some studies are challenged by the difficulty in establishing solid diagnostic criteria of what a concussion is, by confusion between statistical and clinical significance, by inappropriate analyses of multiple exposures to tests, and by questionable control of state-related and intrinsic subject factors. The universal “screening” approach of using baseline tests may be a significant improvement, but there are very few data on that issue, and it is not clear how one could determine if one approach is “better” than another (i.e., comparing post injury to one’s own baseline or to normative standards).
Neuropsychological test scores appear to reflect the presence of a
concussion, although, again, the complexity and associated factors make interpretation more difficult than it might seem on the surface. Neuropsychological testing may be of use in tracking recovery, although studies are emerging that question the presence of ongoing cognitive dysfunction when test results appear to be back to normal or baseline. The use of computerized batteries has allowed for easier test administration, but at the cost of what appears to be a loss of some specificity; that is, tests may be valid indicators of concussion in a broad sense, but they are less useful for saying what cognitive functions are actually affected. Although baseline testing is a common practice, studies provide mixed (and limited) evidence concerning the utility and cost-effectiveness of such testing.
The time-course of the effects of a concussive blow or blows appears to take place on the order of minutes, hours, and days. Within the period of recovery, the brain is thought to be vulnerable to further injury, which can be more severe and may complicate recovery (Cantu, 1998; Cantu and Voy, 1995; Eisenberg et al., 2013; McCrory and Berkovic, 1998; Saunders and Harbaugh, 1984). Thus, although the initial injury may be mild, acute management is still needed to protect the individual from more significant harm.
In 80 to 90 percent of high-school- and college-age patients, concussion symptoms resolve within 2 weeks without any overt intervention (McClincy et al., 2006; McCrea et al., 2004, 2013). McCrea and colleagues (2013) examined 570 high school and college athletes with concussions6 and 166 non-concussed athlete controls. Only 10 percent of the concussed athletes (n=57) took longer than 7 days to recover. In an earlier study, McCrea and colleagues (2004) reported on the recovery from concussions in 94 concussed college football players and 56 non-concussed controls. On average the athletes reverted to baseline by day 7, and there were no symptomatic or functional differences between the two groups by 3 months. This study also found that neuropsychological recovery tended to lag 2 to 3 days behind symptomatic recovery. McClincy and colleagues (2006) documented symptom and ImPACT test scores at baseline and at 2, 7, and 14 days post injury in 104 concussed high school and college athletes. They found significant differences in symptom and ImPACT scores through 7 days post injury, although the magnitude of differences dropped over time. There was no significant difference between symptom scores at baseline and at 14 days post injury. In addition, at day 14, only the verbal memory composite
____________________________________
6Of the injuries, 60.5 percent were in high school athletes, and 39.5 percent were in college athletes.
score of the ImPACT test was significantly different from baseline, although this suggests that at least some areas of neuropsychological recovery may persist in asymptomatic individuals. However, no adjustments for baseline scores or repeat testing were made. Makdissi and colleagues (2010) reported on the natural history of concussion in Australia elite junior and senior football players. The mean time to return to play was 4.8 days, with 18 percent showing symptoms for more than 7 days. Again, computerized neuropsychological testing revealed that abnormalities in neurocognitive performance persisted for 2 to 3 days after the athletes no longer were asymptomatic.
In a study comparing concussion recovery times of high school and college athletes through 7 days post injury, Field and colleagues (2003) found that high school athletes recovered more slowly within the first week after injury, but there was no difference in performance by 7 days in most areas tested. Unlike their college counterparts, high school athletes with a concussion still exhibited a significant decrease in memory performance at 7 days compared with controls (Field et al., 2003).
There is no body of literature on sports-related concussion recovery times for younger children (5 to 12 years). Eisenberg and colleagues (2013) found that concussion symptoms in children 11 to 13 years old presenting to the emergency department (ED) resolved more quickly than in those age 13 and older. It is important to note that the sample in the Eisenberg study was drawn from patients presenting to the ED with acute concussions, raising the possibility that participants may have experienced a more severe injury or a higher initial symptom load than did individuals with acute concussion who do not seek care in an ED. Almost 64 percent of those included in the study sustained their concussions playing sports, 22 percent experienced loss of consciousness, and 43 percent experienced amnesia.
In most studies, the majority of youth adjust well after an mTBI, but in studies that had a non-head-injury control group and good sample retention, around 10 to 13 percent were still symptomatic at 3 months and 1 year after the injury (Barlow et al., 2010; McCrea et al., 2013; Yeates et al., 2009, 2012). Chapter 4 includes recovery curves for reported symptoms, postural stability, and cognitive function (see Figures 4-1, 4-2, and 4-3).
In the acute phase of concussion management, in addition to symptom resolution, the goals include protecting the brain from additional injury and stress, avoiding potential long-term cognitive sequelae of repeated injury, and avoiding the risk of second impact syndrome. The current consensus statements put forth by the international Concussion in Sport Group (McCrory et al., 2013b), the American Medical Society for Sports Medicine (Harmon et al., 2012), the American Academy of Pediatrics (Halstead et al., 2010), and the American Academy of Neurology (Giza et al., 2013) state that athletes who sustain a concussion should not return to play on
the same day as the injury. There is evidence that high school and college athletes may have a delayed onset in symptoms and demonstrate post-injury neuropsychological deficits that may not be apparent on the sideline of an athletic event, and therefore the athletes would benefit from immediate removal from play for their protection (Collins et al., 1999, 2003b; Duhaime et al., 2012; Guskiewicz et al., 2003; Lovell et al., 2003; McCrea et al., 2003). This suggests that same-day return would place that athlete at higher risk for adverse outcomes.
During the acute phase, clinical management strategies to limit physical and cognitive activity are emphasized. The more aggressive medical management of symptoms typically does not begin until 2 to 4 weeks post injury, when an athlete may be said to be experiencing prolonged recovery (see Chapter 4).
Physical Rest
Consensus opinion holds that athletes who have sustained a concussion should refrain from aerobic exercise, sport-specific training, and competition until symptoms resolve (Giza et al., 2013; Halstead et al., 2010; Harmon et al., 2013; McCrory et al., 2013b). Two issues underlie this consensus recommendation. First, concussed athletes are usually instructed to avoid any activity that will increase their heart rate, as this may worsen symptoms and potentially increase recovery time. Second, a premature return to contact or collision activities may increase the risk of repeat injury (Cantu, 1998; Cantu and Voy, 1995; Guskiewicz et al., 2003; McCrory and Berkovic, 1998; Saunders and Harbaugh, 1984). There is evidence in animals that additional concussive injury within a certain period of vulnerability following the initial injury has an additive effect (see Chapter 5). The period of vulnerability may be related to metabolic depression in the brain following the initial injury, but it is not yet known what the time frame is for this vulnerable period, how it varies across ages ranges, and how best to measure it.
Physical rest can range from bed rest to simply refraining from full contact athletic activity. It is important to distinguish between potentially concussive activities (e.g., contact sports or activities that carry a risk of head or body impact) and noncontact physical activity, which may or may not exacerbate symptoms.
Cognitive Rest
Cognitive rest is also recommended for the initial period following a concussion (Halstead et al., 2010; Harmon et al., 2013; McCrory et al., 2013b), although what cognitive rest entails has not been well defined, and
its efficacy in promoting recovery has not been fully determined. Generally, cognitive rest is achieved by eliminating or decreasing activities that require concentration, including schoolwork (McCrory et al., 2009, 2013b) and mental stimulation, as these may exacerbate symptoms and prolong recovery. However, there is a suggestion in the literature that 1 to 2 weeks away from school and schoolwork may place students at academic risk (Allensworth and Easton, 2007).
Evidence for Physical and Cognitive Rest
There is limited evidence about the effects of physical and cognitive rest in youth recovering from sports-related concussion, although it is widely accepted that concussion symptoms are aggravated by both physical and mental exertion (Kissik and Johnston, 2005), and, as previously mentioned, there is evidence of a period of vulnerability during which the brain is more susceptible to secondary injury and during which it is prudent to avoid activities that may lead to additional impacts. In a prospective, nonrandomized study of 635 high school and college athletes with concussion, McCrea and colleagues (2009) found that the more time that elapsed between an athlete’s injury and return to play, the less likely the athlete was to have a repeat concussion during the same season. In addition to the adverse effects of concussion on physical and cognitive function in the acute post-concussion period, there is evidence that the brain is recovering from metabolic changes, as described in Chapter 2. Physical and cognitive activities may increase energy demands on an already overtaxed system. Evidence from a study of voluntary exercise in rats suggests that an initial period of physical and cognitive rest is therapeutic after concussive injury (Griesbach et al., 2004). A retrospective cohort study of 95 high school athletes found that individuals engaging in high levels of activity (school and full athletic participation) after a concussion did not perform as well on neurocognitive testing as those with moderate levels of activity (school and moderate physical activity—light jogging, mowing the lawn) (Majerske et al., 2008). In another study, high school and college athletes who completed at least 1 week of cognitive and physical rest after injury showed significant improvement on concussion symptom scale ratings and neurocognitive scores, even when rest was prescribed weeks or months following a concussion (Moser et al., 2012).
Other studies, however, suggest little or no beneficial effect of physical rest on length of recovery. The same study by McCrea and colleagues (2009) found no difference in concussion outcomes at 45 and 90 days post injury between athletes who returned to play while symptomatic or immediately following symptom resolution and those who observed at least a 1- to 7-day wait following symptom resolution before returning to play.
Another study showed that rest (defined as no mental or physical exertion, but continued activities of daily living) as a treatment for mTBI was ineffective (see Willer and Leddy, 2006). A randomized human trial of patients presenting to the ED with mTBI showed that complete bed rest for 6 days after presentation was ineffective in reducing symptoms at 2 weeks and 6 months post injury (de Kruijk et al., 2002).
The expert consensus opinion is that an individualized treatment plan including physical and cognitive rest is beneficial for recovery from concussion, although current research is insufficient to identify the level and duration of physical and cognitive rest needed to promote recovery. Randomized controlled trials or other appropriately designed studies on the management of concussion in youth are needed in order to develop empirically based clinical guidelines; this includes studies to determine the efficacy of physical and cognitive rest following concussion and the optimal level and duration of rest.7
Return to Physical Activity
The return of an individual to physical activity following a concussion is typically governed by his or her symptom load. Consensus opinion (McCrory et al., 2013b) and practice guidelines (Giza et al., 2013; Halstead et al., 2010; Harmon et al., 2013) state that individuals who have sustained a concussion should avoid physical activity during the acute phase of recovery until they are symptom-free at rest and without medication (see also Buzzini and Guskiewicz, 2006; Canadian Academy of Sport Medicine Concussion Committee, 2000; Herring et al., 2011; Hunt and Asplund, 2010; Kutcher and Eckner, 2010; Lee, 2006; Moser et al., 2007; Poirier, 2003; Purcell and Canadian Paediatric Society, 2012; Putukian et al., 2009). Before returning to activity, individuals should also be back to either their own baseline or the appropriate population norm with regard to neuropsychological/cognitive functioning (McCrory et al., 2013b). When this is measured or obtained by computerized testing, it is important that interpreting providers consider reliable change in test scores rather than exclusively focusing on the numbered scores or percentile scores.
The Department of Defense requires that all deployed service members who are diagnosed with their first concussion observe a mandatory minimum 24-hour recovery period, which may be extended on the basis of
____________________________________
7The report reflects information that was available at the time it went to press. A prospective study of the effect of cognitive activity level on the duration of symptoms following sports-related concussions in 335 youth ages 8 to 23 years subsequently was published in January 2014 (Brown et al., 2014).
subsequent clinical evaluation (DoD, 2012).8 Similar concussion management policies are being developed for concussed service members in the non-deployed setting as well (Tsao, 2013).
During the period when the patient denies symptoms but when metabolic changes presumably are still in effect, symptoms may be induced by rigorous exercise. Therefore, team physicians and athletic trainers may use exercise as a “symptom stress test” to determine whether a player is ready to return to play. Furthermore, evidence that the resolution of neurocognitive impairment following concussion may take longer than the resolution of physical symptoms (Broglio et al., 2007a; Iverson et al., 2006; Peterson et al., 2003; Sandel et al., 2012) and that moderate exercise may induce cognitive declines in athletes who are asymptomatic and have returned to neurocognitive baseline following concussion (McGrath et al., 2013) highlight the importance of appropriately managing an individual’s return to physical activity.
Once individuals are symptom-free, it is frequently recommended that they follow a graded return-to-play protocol (see Table 3-8), progression through which is governed in part by recurrence of symptoms (Canadian Academy of Sport Medicine Concussion Committee, 2000; Halstead et al., 2010; Herring et al., 2011; McCrory et al., 2013b). The protocol calls for individuals to proceed to the next level if they remain asymptomatic at the current stage. If concussion symptoms reappear, the athlete should revert back to the previous asymptomatic stage and resume the progression after 24 hours (Canadian Academy of Sport Medicine Concussion Committee, 2000). The Department of Defense is also in the process of developing a gradual return-to-duty guideline (personal communication with Jack W. Tsao, October 8, 2013).
However, aside from evidence supporting refraining from activities that risk additional injury or re-injury during the temporally undefined “window of cerebral vulnerability” following a concussion, there is little empirical evidence to support the timing of return to physical activity or the use of graded approaches for doing so.
Return to Cognitive Activity
The resumption of cognitive activity, including returning to school, is a primary concern for the majority of the age groups under consideration in this report. Individualized academic adjustments are often needed and are
____________________________________
8Service members who receive a second concussion diagnosis within 12 months are not returned to full duty for 7 days following symptom resolution (DoD, 2012). Individuals who sustain 3 or more concussions within 12 months are required to undergo a “recurrent concussion evaluation,” which is used in determining return-to-duty status (DoD, 2012).
TABLE 3-8 Graded Return-to-Play Protocol
| Step | Rehabilitation Stage | Functional Exercise at Each Stage of Rehabilitation | Objective of Each Stage |
| 1 | No activity | Complete cognitive and physical rest. | Recovery |
| 2 | Light aerobic exercise | Walking, swimming, or stationary cycling, keeping intensity <70% maximum predicted heart rate. No resistance training. | Increase heart rate |
| 3 | Sport-specific activity | Skating drills in ice hockey, running drills in soccer. No head impact activities. | Add movement |
| 4 | Non-contact training drills | Progression to more complex training drills, e.g., passing drills in football and ice hockey. May start load progressive resistance training. | Exercise, coordination, and cognitive |
| 5 | Full contact practice Following medical clearance, participate in normal training activities. | Restore confidence and assess functional skills by coaching staff | |
| 6 | Return to play Normal game play. | ||
SOURCE: Based on Canadian Academy of Sport Medicine Concussion Committee, 2000.
guided by the individual’s experience of symptoms (Halstead et al., 2010; McCrory et al., 2013b). Some students may be unable to participate in full days of school or work, may need a reduced amount of classwork and homework, or may require additional time to take tests and accomplish other tasks (McGrath, 2010; Popoli et al., 2013; Sady et al., 2011). It is also important to note that students who are limited should specifically not be allowed to participate in physical education classes.
Evidence that the resolution of neurocognitive impairment following concussion may take longer than the resolution of physical symptoms (see, e.g., McClincy et al., 2006) highlights the importance of appropriately managing the return to cognitive activity. Academic work demands focus, memory, processing speeds, and concentration, which are the processes that are affected by a concussion (McCrory et al., 2004). In addition, cognitive
stress may elicit or exacerbate concussive symptoms. Indeed, at 1 month post injury, individuals noted more symptoms with cognitive stress than with physical stress (Gioia et al., 2010). The ImPACT test has a post-test symptom checklist that in effect documents the effect of mental exertion on neurocognitive testing.
Although the majority of concussions resolve within 2 weeks, missing school for even a portion of that time can be detrimental to student performance. Assuming a standard school year of approximately 180 days, a 2-week absence for concussion translates into missing 5 percent of the school year. Minimizing time lost from school without compromising the recovery and academic performance of a student recovering from concussion is a challenge. Allensworth and Easton (2007) found that only 63 percent of students in the Chicago school system who missed 5 to 9 days of school in 1 year graduated in 4 years, compared to 87 percent of students who missed less than 1 week. As is the case with a return to physical activity, however, there is little evidence to support protocols for returning students to school following a concussion.
Nationally there are currently two categories of accommodations for disabled students, including those with TBI: the individualized educational plan (IEP) and the 504 plan. The details of each vary by state. In general, IEPs are designed to address long-term cognitive disabilities and ensure that qualified elementary or secondary school students receive individually appropriate specialized instruction, including modified curricula, and related services. A 504 plan is designed to accommodate those individuals with a disability under the Americans with Disabilities Act. This refers to specific laws that protect students who need accommodations in order to have a “level playing field” while pursuing the typical school curriculum—for example, ensuring that a blind student is provided with audio or Braille textbooks or a student with severe dyslexia is permitted additional time on timed assessments.
Although a concussed student, with limitations in memory and processing speeds, may qualify for accommodations under a 504 plan, in practice the time it often takes to determine eligibility and implement the plan makes this an impractical approach for meeting the needs of students who recover within the typical 2-week time frame (Popoli et al., 2013). In addition, a parental request for academic accommodations via a 504 plan or IEP obligates the school to act upon the request, which poses real costs to the school district, both financial and in terms of staff time. Because most concussions resolve within a few weeks, short-term school-based accommodations often can be arranged without the need for a 504 plan (Popoli et al., 2013). Longer-term accommodations may be considered in cases when concussive symptoms persist much longer (e.g., 3 months or more).
Several states, including Arizona (Barrow Concussion Network, 2013), Maine (Maine Department of Education, 2012), New Jersey (P.L.
2013, Ch. 71 [June 27, 2013]), New York (New York State Department of Education, 2012), and Oregon (Oregon Department of Education, 2010), have implemented formal systems to help educate educators on the effects of concussion and to manage the return of students with concussions to academic activity through the use of concussion management teams or other mechanisms. A number of other states provide links to informational material for parents and educators. A common element of the formal school-based concussion management policies is the inclusion of accommodations to permit a gradual return to academic activity (e.g., a shortened school day or extra time to make up assignments and tests).
The Brain Injury Association of Pennsylvania (BIAP), with input from the Pennsylvania Department of Education, has developed a model policy to provide guidance for Pennsylvania schools with respect to concussion and mTBI (BIAP, 2013). The BIAP—with additional funding from the Pennsylvania Departments of Health and Education—has developed a program called BrainSTEPS, which offers school districts trained assistance in reintegrating concussed students into school (BIAP, 2013; Brown, 2013). This work in Pennsylvania illustrates the potential for collaboration among government entities (e.g., Departments of Health and Education) and between government and the private sector to develop infrastructures for addressing issues associated with concussion in youth.
The committee identified the following findings on concussion recognition, diagnosis, and management:
- Currently concussion diagnosis is based primarily on symptoms reported by the individual rather than on objective diagnostic markers, which might also serve as objective markers of recovery.
- The signs and symptoms of concussion typically fall into four categories—physical, cognitive, emotional, and sleep—with patients experiencing one or more symptoms from one or more categories.
- The use of multiple evaluation tools, such as symptom scales and checklists, balance testing, and neurocognitive testing, may increase the sensitivity and specificity of concussion identification, although existing evidence is insufficient to determine the best combination of measures.
- Traditional neuroimaging techniques, such as computerized tomography and magnetic resonance imaging, are of little diagnostic value for concussions per se, because structural imaging results are normal in the case of concussions uncomplicated by skull fracture or hematoma.
- Newer imaging techniques, such as magnetic resonance spectroscopy, positron emission tomography, single-photon emission computed tomography, functional magnetic resonance imaging, and diffusion tensor imaging may be useful in the future for assessing sports-related concussions, but at present they have not been validated for clinical use.
- There is some consensus in the literature that both quantitative electroencephalograph and event-related potential procedures can detect differences in performance and neural responses in concussed versus non-concussed student athletes in high school and college even when behavior measures fail. However, these findings are true for a relatively small set of tasks that assess a limited array of cognitive abilities. Use of a broader range of tasks that measure different aspects of cognitive processes is necessary to provide a comprehensive view of behaviors most likely affected and those more likely spared by concussion.
- There is little research on the use of serum biomarkers in pediatric concussion. Although appropriately sensitive and specific serum biomarkers could be of great diagnostic and prognostic value in sports-related concussion, there currently is no evidence to support their use. There is some evidence, however, to suggest that normal levels of S100B following head injury may predict individuals who do not have intracranial injury.
- Neuropsychological testing has a long tradition in measuring cognitive function after traumatic brain injury and is one of several tools (along with symptom assessment, clinical evaluation, and the like) that may aid in the diagnosis and management of concussions in youth. Studies of the effectiveness of these tests to predict diagnosis and track recovery have had mixed results, and the performance of individuals on neuropsychological tests can be influenced by many factors, including effort and the presence of concussion symptoms (e.g., fatigue resulting from sleep disturbance). It appears that high scores on neuropsychological tests, indicating good cognitive function, are predictive of not having a concussion. In group studies these tests have been shown to be useful for tracking cognitive recovery for up to 2 weeks post injury, with a majority of concussions considered to be resolved by that time. There are no data on the effectiveness of monitoring recovery in individuals whose symptoms persist beyond the typical recovery period.
- Reliability studies for computerized neuropsychological tests are quite variable, with some studies demonstrating adequate reliability and some indicating less than adequate reliability. There are many possible reasons for the variability, including different
-
sample sizes, unknown testing conditions, and variable item pools. Most computerized tests produce multiple forms through a quasi-randomization of items. All commercial test batteries reviewed had some studies indicating acceptable reliability.
- Expert consensus opinion is that an individualized treatment plan including physical and cognitive rest is beneficial for recovery from concussion. There is little empirical evidence to indicate the optimal degree and duration of physical rest needed to promote recovery or the best timing and approach for returning to full physical activity, including the use of graded return-to-play protocols. However, there is evidence that the brain is more susceptible to injury while recovering; thus, common sense dictates reducing the risks of a repeat injury. Similarly, there is little evidence regarding the efficacy of cognitive rest following concussion or to inform the best timing and approach for return to cognitive activity following concussion, including protocols for returning students to school.
- Randomized controlled trials or other appropriately designed studies on the management of concussion youth are needed in order to develop empirically based clinical guidelines, including studies to determine the efficacy of physical and cognitive rest following concussion, the optimal period of rest, and the best protocol for returning individuals to full physical activity as well as to inform the development of evidence-based protocols and appropriate accommodations for students returning to school.
AERA (American Educational Research Association), American Psychological Association, and National Council on Measurement in Education. 1999. Standards for Educational and Psychological Testing. Washington, DC: American Educational Research Association.
Alla, S., S. J. Sullivan, L. Hale, and P. McCrory. 2009. Self-report scales/checklists for the measurement of concussion symptoms: A systematic review. British Journal of Sports Medicine 43(suppl 1):i3–i12.
Allen, B. J., and J. D. Gfeller. 2011. The Immediate Post-Concussion Assessment and Cognitive Testing battery and traditional neuropsychological measures: A construct and concurrent validity study. Brain Injury 25(2):179-191.
Allensworth, E. M., and J. Q. Easton. 2007. What Matters for Staying On-Track and Graduating in Chicago Public High Schools: A Close Look at Course Grades, Failures, and Attendance in the Freshman Year. Chicago: University of Chicago, Consortium on Chicago School Research.
Anastasi, A., and S. Urbina, 1997. Psychological Testing, Seventh edition. Upper Saddle River, NJ: Prentice Hall.
Anderson, B. L., W. J. Pomerantz, J. K. Mann, and M. A. Gittelman. 2013. “I can’t miss the big game”: High school (HS) football players’ knowledge and attitudes about concussions. Presented at the Pediatric Academic Societies Annual Meeting, Washington, DC, May 6.
Axon Sports. 2013. Doctor/trainer FAQs. http://www.axonsports.com/index.cfm?pid=88&pageTitle=Doctor/Trainer-FAQs (accessed October 8, 2013).
Ayr, L. K., K. O. Yeates, H. G. Taylor, and M. Browne. 2009. Dimensions of postconcussive symptoms in children with mild traumatic brain injuries. Journal of the International Neuropsychological Society 15(1):19-30.
Bailey, C. M., R. J. Echemendia, and P. A. Arnett. 2006. The impact of motivation on neuropsychological performance in sports-related mild traumatic brain injury. Journal of the International Neuropsycholological Society 12(4):475-484.
Bailey, C. M., H. L. Samples, D. K. Broshek, J. R. Freeman, and J. T. Barth. 2010. The relationship between psychological distress and baseline sports-related concussion testing. Clinical Journal of Sport Medicine 20(4):272-277.
Baillargeon, A., M. Lassonde, S. Leclerc, and D. Ellemberg. 2012. Neuropsychological and neurophysiological assessment of sport concussion in children, adolescents and adults. Brain Injury 26(3):211-220.
Bandyopadhyay, S., H. Hennes, M. H. Gorelick, R. G. Wells, and C. M. Walsh-Kelly. 2005. Serum neuron-specific enolase as a predictor of short-term outcome in children with closed traumatic brain injury. Academic Emergency Medicine 12(8):732-738.
Barlow, K. M., S. Crawford, A. Stevenson, S. S. Sandhu, F. Belanger, D. Dewey. 2010. Epidemiology of postconcussion syndrome in pediatric mild traumatic brain injury. Pediatrics 126(2):e374-e381.
Barr, W. B., L. S. Prichep, R. Chabot, M. R. Powell, and M. McCrea. 2012. Measuring brain electrical activity to track recovery from sport-related concussion. Brain Injury 26(1):58-66.
Barrow Concussion Network. 2013. Barrow Concussion Network. http://www.aiaonline.org/story/uploads/BCN_FAQ_1368640958.pdf (accessed September 23, 2013).
Barth, J. T., S. N. Macciocchi, B. Giordani, R. N. Rimel, J. A. Jane, and T. J. Boll. 1983. Neuropsychological sequelae of minor head injury. Neurosurgery 13(5):529-533.
Barth, J. T., W. M. Alves, T. V. Ryan, S. N. Macciocchi, R. W. Rimel, J. A. Jane, and W. E. Nelson. 1989. Mild head injury in sports: Neuropsychological sequelae and recovery of function. In Mild Head Injury, edited by H. S. Levin, H. M. Eisenberg, and A. L. Benton. New York: Oxford University Press, pp. 257-275.
Barth, J. T., J. R. Freeman, and J. E. Winters. 2000. Management of sports-related concussions. Dental Clinics of North America 44(1):67-83.
Bauer, R. M., G. L. Iverson, A. N. Cernich, L. M. Binder, R. M. Ruff, and R. I. Naugle. 2012. Computerized neuropsychological assessment devices: Joint position paper of the American Academy of Clinical Neuropsychology and the National Academy of Neuropsychology. Archives of Clinical Neuropsychology 27(3):362-373.
Baumgartner, T. A., and H. Chung. 2001. Confidence limits for intraclass reliability coefficients. Measurement in Physical Education and Exercise Science 5(3):179-188.
Bazarian, J. J., F. P. Zemlan, S. Mookerjee, and T. Stigbrand. 2006. Serum S-100B and cleavedtau are poor predictors of long-term outcome after mild traumatic brain injury. Brain Injury 20(7):759-765.
Bechtel, K., S. Frasure, C. Marshall, J. Dziura, and C. Simpson. 2009. Relationship of serum S100B levels and intracranial injury in children with closed head trauma. Pediatrics 124(4):e697-e704.
Beckwith, J. G., R. M. Greenwald, J. J. Chu, J. J. Crisco, S. Rowson, S. M. Duma, S. P. Broglio, T. W. McAllister, K. M. Guskiewicz, J. P. Mihalik, S. Anderson, B. Schnebel, P. G. Brolinson, and M. W. Collins. 2013a. Head impact exposure sustained by football players on days of diagnosed concussion. Medicine and Science in Sports and Exercise 45(4):737-746.
Beckwith, J. G., R. M. Greenwald, J. J. Chu, J. J. Crisco, S. Rowson, S. M. Duma, S. P. Broglio, T. W. McAllister, K. M. Guskiewicz, J. P. Mihalik, S. Anderson, B. Schnebel, P. G. Brolinson, and M. W. Collins. 2013b. Timing of concussion diagnosis is related to head impact exposure prior to injury. Medicine and Science in Sports and Exercise 45(4):747-754.
Beebe, D. W. 2012. A brief primer on sleep for pediatric and child clinical neuropsychologists. Child Neuropsychology 18(4):313-338.
Beers, S. R., R. P. Berger, and P. D. Adelson. 2007. Neurocognitive outcome and serum biomarkers in inflicted versus non-inflicted traumatic brain injury in young children. Journal of Neurotrauma 24(1):97-105.
Belanger, H. G., and R. D. Vanderploeg. 2005. The neuropsychological impact of sports-related concussion: A meta-analysis. Journal of the International Neuropsychological Society 11(4):345-357.
Belanger, H. G., R. D. Vanderploeg, G. Curtiss, and D. L. Warden. 2007. Recent neuroimaging techniques in mild traumatic brain injury. Jounal of Neuropsychiatry and Clinical Neurosciences 19(1):5-20.
Berger, R. P., and N. Zuckerbraun. 2012. Biochemical markers. In Mild Traumatic Brain Injury in Children and Adolescents: From Basic Science to Clinical Management, edited by M. W. Kirkwood and K. O. Yeates. New York: Guilford Press. Pp. 145-161.
Berger, R. P., S. R. Beers, R. Richichi, D. Wiesman, and P. D. Adelson. 2007. Serum biomarker concentrations and outcome after pediatric traumatic brain injury. Journal of Neurotrauma 24(12):1793-1801.
BIAP (Brain Injury Association of Pennsylvania). 2013. BIAPA offers assistance to Pennsylvania schools. http://www.biapa.org/site/apps/nlnet/content2.aspx?c=iuLZJbMMKrH&b=1843921&ct=11590269¬oc=1 (accessed October 7, 2013).
Biederman, J., L. J. Seidman, C. R. Petty, R. Fried, A. E. Doyle, D. R. Cohen, D. C. Kenealy, and S. V. Faraone. 2008. Effects of stimulant medication on neuropsychological functioning in young adults with attention-deficit/hyperactivity disorder. Journal of Clinical Psychiatry 69(7):1150-1156.
Bleiberg, J., W. Garmoe, E. Halpern, D. Reeves, and J. Nadler. 1997. Consistency of within-day and across-day performance after mild brain injury. Neuropsychiatry, Neuropsychology, and Behavioral Neurology 10(4):247-253.
Bleiberg, J., R. L. Kane, D. L. Reeves, W. S. Garmoe, and E. Halpern. 2000. Factor analysis of computerized and traditional tests used in mild brain injury research. Clinical Neuropsycholgist 14(3):287-294.
Bleiberg J., A. Cernich, K. Cameron, W. Sun, K. Peck, J. Ecklund, D. Reeves, J. Uhorchak, M. B. Sparling, and D. L. Warden. 2004. Duration of cognitive impairment after sports concussion. Neurosurgery 54(5):1073-1078; discussion 1078-1080.
Broglio, S. P., and T. W. Puetz. 2008. The effect of sport concussion on neurocognitive function, self-report symptoms and postural control: A meta-analysis. Sports Medicine 38:53-67.
Broglio, S. P., S. N. Macciocchi, and M. S. Ferrara. 2007a. Neurocognitive performance of concussed athletes when symptom free. Journal of Athletic Training 42(4):504-508.
Broglio, S. P., S. N. Macciocchi, and M. S. Ferrara. 2007b. Sensitivity of the concussion assessment battery. Neurosurgery 60(6):1050-1057; discussion 1057-1058.
Broglio, S. P., M. S. Ferrara, S. N. Macciocchi, T. A. Baumgartner, and R. Elliott. 2007c. Test-retest reliability of computerized concussion assessment programs. Journal of Athletic Training 42(4):509-514.
Broglio, S. P., R. D. Moore, and C. H. Hillman. 2011. A history of sport-related concussion on event-related brain potential correlates of cognition. International Journal of Psychophysiology 82(1):16-23.
Brown, B. E. 2013. Concussion: Return to Learning: How Schools Can Accommodate Concussed Youth Athletes & the Role of Schools in Recovery. Presentation before the committee, Washington, DC, February 25.
Brown, C. N., K. M. Guskiewicz, and J. Bleiberg. 2007. Athlete characteristics and outcome scores for computerized neuropsychological assessment: A preliminary analysis. Journal of Athletic Training 42(4):515-523.
Brown, N. J., R. C. Mannix, M. J. O’Brien, D. Gostine, M. W. Collins, and W. P. Meehan III. 2014. Effect of cognitive activity level on duration of post-concussion symptoms. Pediatrics (January 6). [Epub ahead of print.] doi: 10.1542/peds.2013-2125.
Buzzini, S. R., and K. M. Guskiewicz. 2006. Sport-related concussion in the young athlete. Current Opinion in Pediatrics 18(4):376-382.
Canadian Academy of Sport Medicine Concussion Committee. 2000. Guidelines for assessment and management of sport-related concussion. Clinical Journal of Sport Medicine 10(3):209-211.
Cantu, R. C. 1998. Second-impact syndrome. Clinics in Sports Medicine 17(1):37-44.
Cantu, R. C., and R. Voy. 1995. Second impact syndrome a risk in any contact sport. Physician and Sportsmedicine 23(6):27-34.
Castellani, C., P. Bimbashi, E. Ruttenstock, P. Sacherer, T. Stojakovic, and A. M. Weinberg. 2009. Neuroprotein S-100B: A useful parameter in paediatric patients with mild traumatic brain injury? Acta Paediatrica 98(10):1607-1612.
Cavanaugh, J. T., K. M. Guskiewicz, C. Giuliani, S. Marshall, V. Mercer, and N. Stergiou. 2005. Detecting altered postural control after cerebral concussion in athletes with normal postural stability. British Journal of Sports Medicine 39(11): 805-811.
CDC (Centers for Disease Control and Prevention). 2012a. Heads up: Concussion in youth sports. http://www.cdc.gov/concussion/HeadsUp/youth.html (accessed April 3, 2013).
CDC. 2012b. Heads up: Concussion in youth sports. A fact sheet for coaches. http://www.cdc.gov/concussion/pdf/coaches_engl.pdf (accessed October 6, 2013).
CDC. 2013. Injury prevention and control: Traumatic brain injury. Concussion. http://www.cdc.gov/concussion/signs_symptoms.html (accessed September 16, 2013).
Cernich, A., D. Reeves, W. Y. Sun, and J. Bleiberg. 2007. Automated Neuropsychological Assessment Metrics sports medicine battery. Archives of Clinical Neuropsychology 22(1):S101-S114.
Chen, J. K., K. M. Johnston, A. Collie, P. McCrory, and A. Ptito. 2007. A validation of the Post Concussion Symptom Scale in the assessment of complex concussion using cognitive testing and functional MRI. Journal of Neurology, Neurosurgery, and Psychiatry 78(11):1231-1238.
CNS Vital Signs. 2013. CNS Vital Signs. http://www.cnsvs.com (accessed October 7, 2013).
Cole, W. R., J. P. Arrieux, K. Schwab, B. J. Ivins, F. M. Qashu, and S. C. Lewis. 2013. Test-retest reliability of four computerized neurocognitive assessment tools in an active duty military population. Archives of Clinical Neuropsychology (July 12). [Epub ahead of print.]
Collie, A., D. Darby, and P. Maruff. 2001. Computerised cognitive assessment of athletes with sports related head injury. British Journal of Sports Medicine 35(5):297-302.
Collie, A., P. Maruff, M. Makdissi, P. McCrory, M. McStephen, and D. Darby. 2003. CogSport: Reliability and correlation with conventional cognitive tests used in postconcussion medical evaluations. Clinical Journal of Sport Medicine 13(1):28-32.
Collins, M. W., S. H. Grindel, M. R. Lovell, D. E. Dede, D. J. Moser, B. R. Phalin, S. Nogle, M. Wasik, D. Cordry, K. M. Daugherty, S. F. Sears, G. Nicolette, P. Indelicato, and D. B. McKeag. 1999. Relationship between concussion and neuropsychological performance in college football players. JAMA 282(10):964-970.
Collins, M., M. Field, M. Lovell, G. Iverson, K. M. Johnston, J. Maroon, F. H. Fu. 2003a. Relationship between postconcussion headache and neuropsychological test performance in high school athletes. American Journal of Sports Medicine 31(2):168-173.
Collins, M. W., G. L. Iverson, M. R. Lovell, D. B. McKeag, J. Norwig, and J. Maroon. 2003b. On-field predictors of neuropsychological and symptom deficit following sports-related concussion. Clinical Journal of Sport Medicine 13(4):222-229.
Comper, P., M. Hutchison, S. Magrys, L. Mainwaring, and D. Richards. 2010. Evaluating the methodological quality of sports neuropsychology concussion research: A systematic review. Brain Injury 24(11):1257-1271.
Concussion Vital Signs. 2013. Concussion Vital Signs. http://www.concussionvitalsigns.com/About.html (accessed October 7, 2013).
Covassin, T., R. J. Elbin, III, J. L. Stiller-Ostrowski, and A. P. Kontos. 2009. Immediate Post-Concussion Assessment and Cognitive Testing (ImPACT) practices of sports medicine professionals. Journal of Athletic Training 44(6):639-644.
Covassin, T., R. J. Elbin, III, W. Harris, T. Parker, and A. Kontos. 2012a. The role of age and sex in symptoms, neurocognitive performance, and postural stability in athletes after concussion. American Journal of Sports Medicine 40(6):1303-1312.
Covassin, T., R. J. Elbin, III, E. Larson, and A. Kontos. 2012b. Sex and age differences in depression and baseline sport-related concussion neurocognitive performance and symptoms. Clinical Journal of Sport Medicine 22(2):98-104.
Coyne, C. 2103. Experiencing Concussion in Youth Sports: An Athlete’s Perspective. Presentation before the committee, Seattle, WA, April 15.
Cubon, V. A., M. Putukian, C. Boyer, and A. Dettwiler. 2011. A diffusion tensor imaging study on the white matter skeleton in individuals with sports-related concussion. Journal of Neurotrauma 28(2):189-201.
de Kruijk, J. R., P. Leffers, S. Meerhoff, J. Rutten, and A. Twijnstra. 2002. Effectiveness of bed rest after mild traumatic brain injury: A randomised trial of no versus six days of bed rest. Journal of Neurology, Neurosurgery, and Psychiatry 73(2):167-172.
DiFiori, J. P., and C. C. Giza. 2010. New techniques in concussion imaging. Current Sports Medicine Reports 9(1):35-39.
Diver, T., G. Gioia, and S. Anderson. 2007. Discordance of symptom report across clinical and control groups with respect to parent and child. Journal of the International Neuropsychological Society 13(Suppl 1):63. [Poster presentation to the Annual Meeting of the International Neuropsychological Society, Portland, OR.]
DoD (Department of Defense). 2012. Instruction number 6490.11. DoD policy guidance for management of mild traumatic brain injury/concussion in the deployed setting. Issued September 18, 2012. http://www.dtic.mil/whs/directives/corres/pdf/649011p.pdf (accessed September 22, 2013).
DoD. 2013. Instruction number 6490.13. Comprehensive policy on neurocognitive assessments by the military services. Issued June 4, 2013. http://www.dtic.mil/whs/directives/corres/pdf/649013p.pdf (accessed September 21, 2013).
Duhaime, A-C., J. G. Beckwith, A. C. Maerlender, T. W. McAllister, J. J. Crisco, S. M. Duma, P. G. Brolinson, S. Rowson, L. A. Flashman, J. J. Chu, and R. M. Greenwald. 2012. Spectrum of acute clinical characteristics of diagnosed concussions in college athletes wearing instrumented helmets. Journal of Neurosurgery 117(6):1092-1099.
DVBIC (Defense and Veterans Brain Injury Center). 2012. MACE: Military Acute Concussion Evaluation. https://www.jsomonline.org/TBI/MACE_Revised_2012.pdf (accessed October 6, 2013).
Dziemianowicz, M., M. P. Kirschen, B. A. Pukenas, E. Laudano, L. J. Balcer, and S. L. Galetta. 2012. Sports-related concussion testing. Current Neurology and Neuroscience Reports 12(5):547-559.
Echemendia, R. J., M. Putukian, R. S. Mackin, L. Julian, and N. Shoss. 2001. Neuropsychological test performance prior to and following sports-related mild traumatic brain injury. Clinical Journal of Sport Medicine 11(1):23-31.
Eckner, J. T., J. S. Kutcher, and J. K. Richardson. 2010. Pilot evaluation of a novel clinical test of reaction time in National Collegiate Athletic Association Division I football players. Journal of Athletic Training 45(4):327-332.
Eckner, J. T., J. S. Kutcher, S. P. Broglio, and J. K. Richardson. 2013. Effect of sport-related concussion on clinically measured simple reaction time. British Journal of Sports Medicine. Published online first: January 11, doi:10.1136/bjsports-2012-0915792013.
Eisenberg, M. A., J. Andrea, W. Meehan, and R. Mannix. 2013. Time interval between concussions and symptom duration. Pediatrics 132(1):8-17.
Elbin, R. J., P. Schatz, and T. Covassin. 2011. One-year test-retest reliability of the online version of ImPACT in high school athletes. American Journal of Sports Medicine 39(11):2319-2324.
Ellemberg, D., L. C. Henry, S. N. Macciocchi, K. M. Guskiewicz, and S. P. Broglio. 2009. Advances in sport concussion assessment: From behavioral to brain imaging measures. Journal of Neurotrauma 26(12):2365-2382.
Eonta, S. E., W. Carr, J. J. McArdle, J. M. Kain, C. Tate, N. J. Wesensten, J. N. Norris, T. J. Balkin, and G. H. Kamimori. 2011. Automated Neuropsychological Assessment Metrics: Repeated assessment with two military samples. Aviation, Space, and Environmental Medicine 82(1):34-39.
Erdal, K. 2012. Neuropsychological testing for sports-related concussion: How athletes can sandbag their baseline testing without detection. Archives of Clinical Neuropsychology 27(5):473-479.
Erlanger, D., E. Saliba, J. Barth, J. Almquist, W. Webright, and J. Freeman. 2001. Monitoring resolution of postconcussion symptoms in athletes: Preliminary results of a Web-based neuropsychological test protocol. Journal of Athletic Training 36(3):280-287.
Erlanger, D. M., T. Kaushik, D. Broshek, J. Freeman, D. Feldman, and J. Festa. 2002. Development and validation of a web-based screening tool for monitoring cognitive status. Journal of Head Trauma Rehabilitation 17(5):458-476.
Erlanger, D., D. Feldman, K. Kutner, T. Kaushik, H. Kroger, J. Festa, J. Barth, J. Freeman, and D. Broshek. 2003. Development and validation of a web-based neuropsychological test protocol for sports-related return-to-play decision-making. Archives of Clinical Neuropsychology 18(3):293-316.
Falleti, M. G., P. Maruff, A. Collie, and D. G. Darby. 2006. Practice effects associated with the repeated assessment of cognitive function using the CogState battery at 10-minute, one week and one month test-retest intervals. Journal of Clinical and Experimental Neuropsychology 28(7):1095-1112.
Fazio, V. C., M. R. Lovell, J. E. Pardini, and M. W. Collins. 2007. The relation between post concussion symptoms and neurocognitive performance in concussed athletes. NeuroRehabilitation 22:207-216.
Field, M., M. W. Collins, M. R. Lovell, and J. Maroon. 2003. Does age play a role in recovery form sports-related concussion? A comparison of high school and collegiate athletes. Journal of Pediatrics 142(5):546-553.
Filippidis, A. S., D. C. Papadopoulos, E. Z. Kapsalaki, and K. N. Fountas. 2010. Role of the S100B serum biomarker in the treatment of children suffering from mild traumatic brain injury. Neurosurgical Focus 29(5):E2.
Finnoff, J. T., E. J. Jelsing, and J. Smith. 2011. Biomarkers, genetics, and risk factors for concussion. PM & R 3(10 Suppl 2):S452-S459.
Fridriksson, T., N. Kini, C. Walsh-Kelly, and H. Hennes. 2000. Serum neuron-specific enolase as a predictor of intracranial lesions in children with head trauma: A pilot study. Academic Emergency Medicine 7(7):816-820.
Frommer, L. J., K. K. Gurka, K. M. Cross, C. D. Ingersoll, R. D. Comstock, and S. A. Saliba. 2011. Sex differences in concussion symptoms of high school athletes. Journal of Athletic Training 46(1):76-84.
Galetta, K. M., L. E. Brandes, K. Maki, M. S. Dziemianowicz, E. Laudano, M. Allen, K. Lawler, B. Sennett, D. Wiebe, S. Devick, L. V. Messner, S. L. Galetta, and L. J. Balcer. 2011. The King-Devick test and sports-related concussion: Study of a rapid visual screening tool in a collegiate cohort. Journal of the Neurological Sciences 309(1-2):34-39.
Gardner, A., E. A. Shores, J. Batchelor, and C. A. Honan. 2012. Diagnostic efficiency of ImPACT and CogSport in concussed rugby union players who have not undergone baseline neurocognitive testing. Applied Neuropsychology Adult 19(2):90-97.
Geurts A. C., G. M. Ribbers, J. A. Knoop, and J. van Limbeek. 1996. Identification of static and dynamic postural instability following traumatic brain injury. Archives of Physical Medicine and Rehabilitation 77(7):639-644.
Geyer, C., A. Ulrich, G. Gräfe, B. Stach, and H. Till. 2009. Diagnostic value of S100B and neuron-specific enolase in mild pediatric traumatic brain injury. Journal of Neurosurgery Pediatrics 4:339-344.
Gioia, G. 2013. Perspectives on Management of Students’ Return to School. Presentation before the committee, Washington, DC, February 25.
Gioia, G., and M. Collins. 2006. Acute Concussion Evaluation (ACE): Physician/Clinician Office Version. http://www.cdc.gov/concussion/headsup/pdf/ace-a.pdf (accessed August 23, 2013).
Gioia, G., M. Collins, and P. K. Isquith. 2008a. Improving identification and diagnosis of mild traumatic brain injury with evidence: Psychometric support for the Acute Concussion Evaluation. Journal of Head Trauma Rehabilitation 23(4):230-242.
Gioia, G., J. Janusz, P. Isquith, and D. Vincent. 2008b. Psychometric properties of the parent and teacher Post-Concussion Symptom Inventory (PCSI) for children and adolescents. [Abstract.] Journal of the International Neuropsychologcical Society 14(Suppl 1):204.
Gioia, G. A., J. C. Schneider, C. G. Vaughan, and P. K. Isquith. 2009. Which symptom assessments and approaches are uniquely appropriate for paediatric concussion? British Journal of Sports Medicine 43(Suppl 1):i13-i22.
Gioia, G. A., C. G. Vaughan, J. Reesman, C. McGill, E. McGuire, L. Gathercole, H. Padia, K. Nichols, P. Allen, and C. Wells. 2010. Characterizing post-concussion exertional effects in the child and adolescent. [Abstract.] Journal of the International Neuropsychological Society 16(Suppl 1):178.
Gioia, G., P. Isquith, and C. Vaughan. 2013a. Classification analyses of pediatric concussion assessment battery. [Abstract.] British Journal of Sports Medicine 47(5):e1.
Gioia, G. A., C. G. Vaughan, and P. K. Isquith. 2013b. Professional manual for Pediatric Immediate Post-Concussion Assessment and Cognitive Testing (ImPACT). Odessa, FL: Psychological Assessment Resources.
Giza, C. C., J. S. Kutcher, S. Ashwal, J. Barth, T. S. D. Getchius, G. A. Gioia, G. S. Gronseth, K. Guskiewicz, S. Mandel, G. Manley, D. B. McKeag, D. J. Thurman, and R. Zafonte. 2013. Evidence-Based Guideline Update: Evaluation and Management of Concussion in Sports. Report of the Guideline Development Subcommittee of the American Academy of Neurology. American Academy of Neurology.
Gosselin, N., M. Lassonde, D. Petit, S. Leclerc, V. Mongrain, A. Collie, and J. Montplaisir. 2009. Sleep following sport-related concussions. Sleep Medicine 10(1):35-46.
Gosselin, N., C. Bottari, J. K. Chen, S. C. Huntgeburth, L. De Beaumont, M. Petrides, B. Cheung, and A. Ptito. 2012a. Evaluating the cognitive consequences of mild traumatic brain injury and concussion by using electrophysiology. Neurosurgical Focus 33(6):E7:1-7.
Gosselin, N., J. K. Chen, C. Bottari, M. Petrides, T. Jubault, S. Tinawi, E. de Guise, and A. Ptito. 2012b. The influence of pain on cerebral functioning after mild traumatic brain injury. Journal of Neurotrauma 29(17):2625-2634.
Green, P. 2007. The pervasive influence of effort on neuropsychological tests. Physical Medicine Rehabilitation Clinics of North America 18(1):43-68.
Griesbach, G. S., D. A. Hovda, R. Molteni, A. Wu, and F. Gomez-Pinilla. 2004. Voluntary exercise following traumatic brain injury: Brain-derived neurotrophic factor upregulation and recovery of function. Neuroscience 125(1):129-139.
Grindel, S. H., M. R. Lovell, M. W. Collins. 2001. The assessment of sport-related concussion: The evidence behind neuropsychological testing and management. Clinical Journal of Sport Medicine 11(3):134-143.
Gronwall, D., and P. Wrightson. 1981. Memory and information processing capacity after closed head injury. Journal of Neurology, Neurosurgery, and Psychiatry 44(10):889-895.
Gualtieri, C. T., and L. G. Johnson. 2006. Reliability and validity of a computerized neurocognitive test battery, CNS Vital Signs. Archives of Clinical Neuropsychology 21(7):623-643.
Guskiewicz, K. M. 2001. Postural stability assessment following concussion: One piece of the puzzle. Clinical Journal of Sport Medicine 11(3):182-189.
Guskiewicz, K. M. 2011. Balance assessment in the management of sport-related concussion. Clinics in Sports Medicine 30(1):89-102, ix.
Guskiewicz, K. M., and J. K. Register-Mihalik. 2011. Postconcussive impairment differences across a multifaceted concussion assessment protocol. PM & R 3(10 Suppl 2):S445-S451.
Guskiewicz, K. M., S. E. Ross, and S. W. Marshall. 2001. Postural stability and neuropsychological deficits after concussion in collegiate athletes. Journal of Athletic Training 36(3):263-273.
Guskiewicz, K. M., M. McCrea, S. W. Marshall, R. C. Cantu, C. Randolph, W. Barr, J. A. Onate, and J. P. Kelly. 2003. Cumulative effects associated with recurrent concussion in collegiate football players: The NCAA Concussion Study. JAMA 290(19):2549-2555.
Hajek, C. A., K. O. Yeates, H. G. Taylor, B. Bangert, A. Dietrich, K. E. Nuss, J. Rusin, and M. Wright. 2011. Agreement between parents and children on ratings of postconcussive symptoms following mild traumatic brain injury. Child Neuropsychology 17(1):17-33.
Halstead, M. E., K. D. Walter, and American Academy of Pediatrics, Council on Sports Medicine and Fitness. 2010. Sport-related concussion in children and adolescents. Pediatrics 126(3):597-615.
Harmon, K. G., J. Drezner, M. Gammons, K. Guskiewicz, M. Halstead, S. Herring, J. Kutcher, A. Pana, M. Putukian, W. Roberts, and American Medical Society for Sports Medicine. 2013. American Medical Society for Sports Medicine position statement: Concussion in sport. British Journal of Sports Medicine 47(1):15-26.
Hasselblatt, M., F. C. Mooren, N. von Ahsen, K. Keyvani, A. Fromme, K. Schwarze-Eicker, V. Senner, and W. Paulus. 2004. Serum S100beta increases in marathon runners reflect extracranial release rather than glial damage. Neurology 62(9):1634-1636.
Heilbronner, R. L., J. J. Sweet, D. K. Attix, K. R. Krull, G. K. Henry, and R. P. Hart. 2010. Official position of the American Academy of Clinical Neuropsychology on serial neuropsychological assessments: The utility and challenges of repeat test administrations in clinical and forensic contexts. Clinical Neuropsychologist 24(8):1267-1278.
Herring, S. A., R. C. Cantu, K. M. Guskiewicz, M. Putukian, W. B. Kibler, J. A. Bergfeld, L. A. Boyajian-O’Neill, R. R. Franks, P. A. Indelicato, and the American College of Sports Medicine. 2011. Concussion (mild traumatic brain injury) and the team physician: A consensus statement—2011 update. Medicine and Science in Sports and Exercise 43(12):2412-2422.
Hinton-Bayre, A. D. 2012. Choice of reliable change model can alter decisions regarding neuropsychological impairment after sports-related concussion. Clinical Journal of Sport Medicine 22(2):105-108.
Hinton-Bayre, A. D., G. Geffen, and K. McFarland. 1997. Mild head injury and speed of information processing: A prospective study of professional rugby league players. Journal of Clinical and Experimental Neuropsychology 19(2):275-289.
Hinton-Bayre, A. D., G. M. Geffen, L. B. Geffen, K. A. McFarland, and P. Friis. 1999. Concussion in contact sports: Reliable change indices of impairment and recovery. Journal of Clinical and Experimental Neuropsychology 21(1):70-86.
Hunt, T., and C. Asplund. 2010. Concussion assessment and management. Clinics in Sports Medicine 29(1):5-17.
Hunt, T. N., M. S. Ferrara, L. S. Miller, and S. N. Macciocchi. 2007. The effect of effort on baseline neuropsychological test scores in high school football athletes. Archives of Clinical Neuropsychology 22(5):615-621.
Hunt, T. N., M. S. Ferrara, R. A. Bornstein, and T. A. Baumgartner. 2009. The reliability of the Modified Balance Error Scoring System. Clinical Journal of Sport Medicine 19(6):471-475.
Hutchison, M., P. Comper, L. Mainwaring, and D. Richards. 2011. The influence of musculoskeletal injury on cognition: Implications for concussion research. American Journal of Sports Medicine 39(11):2331-2337.
ImPACT (Immediate Post-Concussion Assessment and Cognitive Testing). 2013. The ImPACT test. http://www.impacttest.com/about/?The-ImPACT-Test-4 (accessed October 8, 2013).
Iverson, G. L., and M. Gaetz. 2004. Practical consideration for interpreting change following brain injury. In Traumatic Brain Injury in Sports: An International Neuropsychological Perspective, edited by M. R. Lovell, R. J. Echemendia, J. T. Barth, and M. W. Collins. Exton, PA: Swets & Zeitlinger. Pp. 323-356.
Iverson, G. L., M. R. Lovell, and M. W. Collins. 2003. Interpreting change in ImPACT following sport concussion. Clinical Neuropsychologist 17(4):460-467.
Iverson, G. L., M. D. Franzen, M. R. Lovell, and M. W. Collins. 2004. Construct validity of impact in athletes with concussions. [Abstract.] Archives of Clinical Neuropsychology 19(7):961-962.
Iverson, G. L., M. R. Lovell, and M. W. Collins. 2005. Validity of ImPACT for measuring processing speed following sports-related concussion. Journal of Clinical and Experimental Neuropsychology 27(6):683-689.
Iverson, G. L., B. L. Brooks, M. W. Collins, and M. R. Lovell. 2006. Tracking neuropsychological recovery following concussion in sport. Brain Injury 20(3):245-252.
Jantzen, K. J., B. Anderson, F. L. Steinberg, and J. A. Kelso. 2004. Prospective functional MR imaging study of mild traumatic brain injury in college football players. American Journal of Neuroradiology 25(5):738-745.
Janusz, J. A., M. D. Sady, and G. A. Gioia. 2012. Postconcussion symptom assessment. In Mild Traumatic Brain Injury in Children and Adolescents: From Basic Science to Clinical Management, edited by M. W. Kirkwood and K. O. Yeates. New York: Guilford Press. Pp. 241-263.
Johnson, D. R., A. S. Vincent, A. E. Johnson, K. Gilliland, and R. E. Schlegel. 2008. Reliability and construct validity of the Automated Neuropsychological Assessment Metrics (ANAM) mood scale. Archives of Clinical Neuropsychology 23(1):73-85.
King, N. S., S. Crawford, F. J. Wenden, N. E. Moss, and D. T. Wade. 1995. The Rivermead Post Concussion Symptoms Questionnaire: A measure of symptoms commonly experienced after head injury and its reliability. Journal of Neurology 242(9):587-592.
Kirkwood, M. W., C. Randolph, and K. O. Yeates. 2009. Returning pediatric athletes to play after concussion: The evidence (or lack thereof) behind baseline neuropsychological testing. Acta Paediatrica 98(9):1409-1411.
Kissick, J., and K. M. Johnston. 2005. Return to play after concussion: Principles and practice. Clinical Journal of Sport Medicine 15(6):426-431.
Koerte, I. K., D. Kaufmann, E. Hartl, S. Bouix, O. Pasternak, M. Kubicki, A. Rauscher, D. K. Li, S. B. Dadachanji, J. A. Taunton, L. A. Forwell, A. M. Johnson, P. S. Echlin, and M. E. Shenton. 2012. A prospective study of physician-observed concussion during a varsity university hockey season: White matter integrity in ice hockey players. Part 3 of 4. Neurosurgical Focus 33(6):E3:1-7.
Kontos, A. P., R. J. Elbin, P. Schatz, T. Covassin, L. Henry, J. Pardini, and M. W. Collins. 2012. A revised factor structure for the Post-Concussion Symptom Scale: Baseline and postconcussion factors. American Journal of Sports Medicine 40(10):2375-2384.
Kroshus, E., D. H. Daneshvar, C. M. Baugh, C. J. Nowinski, and R. C. Cantu. 2013. NCAA concussion education in ice hockey: An ineffective mandate. British Journal of Sports Medicine, in press. doi: 10.1136/bjsports-2013-092498.
Kutcher, J. S., and J. T. Eckner. 2010. At-risk populations in sports-related concussion. Current Sports Medicine Reports 9(1):16-20.
Lange, R. T., G. L. Iverson, B. L. Brooks, and V. L. Rennison. 2010. Influence of poor effort on self-reported symptoms and neurocognitive test performance following mild traumatic brain injury. Journal of Clinical and Experimental Neuropsychology 32(9):961-972.
Lee, M. A. 2006. Adolescent concussions—Management recommendations: A practical approach. Connecticut Medicine 70(6):377-380.
Lezak, M. D., D. B. Howieson, E. D. Bigler, and D. Tranel. 2012. Neuropsychological Assessment, Fifth edition. Oxford University Press.
Lovell, M. R., and M. W. Collins. 1998. Neuropsychological assessment of the college football player. Journal of Head Trauma Rehabilitation 13(2):9-26.
Lovell, M. R., M. W. Collins, G. L. Iverson, M. Field, J. C. Maroon, R. Cantu, K. Podell, J. W. Powell, M. Belza, and F. H. Fu. 2003. Recovery from mild concussion in high school athletes. Journal of Neurosurgery 98(2):296-301.
Lovell, M. R., G. L. Iverson, M. W. Collins, K. Podell, K. M. Johnston, D. Pardini, J. Pardini, J. Norwig, and J. C. Maroon. 2006. Measurement of symptoms following sports-related concussion: Reliability and normative data for the Post-Concussion Scale. Applied Neuropsychology 13(3):166-174.
Lovell, M. R., J. E. Pardini, J. Welling, M. W. Collins, J. Bakal, N. Lazar, R. Roush, W. F. Eddy, and J. T. Becker. 2007. Functional brain abnormalities are related to clinical recovery and time to return-to-play in athletes. Neurosurgery 61(2):352-359.
Macciocchi, S. N., J. T. Barth, W. Alves, R. W. Rimel, and J. A. Jane. 1996. Neuropsychological functioning and recovery after mild head injury in collegiate athletes. Neurosurgery 39(3):510-514.
Maddocks, D. L., G. D. Dicker, and M. M. Saling. 1995. The assessment of orientation following concussion in athletes. Clinical Journal of Sports Medicine 5(1):32-35.
Maerlender, A., and A. Alt. 2012. The effect of sleep the night before on baseline neuropsychological screening and symptom reporting. [Abstract.] Journal of the International Neuropsychological Society 18(Suppl 1):165.
Maerlender, A., L. Flashman, A. Kessler, S. Kumbhani, R. Greenwald, T. Tosteson, and T. McAllister. 2010. Examination of the construct validity of ImPACT™ computerized test, traditional, and experimental neuropsychological measures. Clinical Neuropsychologist 24(8):1309-1325.
Maerlender, A., L. Flashman, A. Kessler, S. Kumbhani, R. Greenwald, T. Tosteson, and T. McAllister. 2013. The discriminant construct validity of ImPACT™: A companion study. Clinical Neuropsychologist 27(2):290-299.
Mailer, B. J., T. C. Valovich-McLeod, and R. C. Bay. 2008. Healthy youth are reliable in reporting symptoms on a graded symptom scale. Journal of Sport Rehabilitation 17(1):11-20.
Maine Department of Education. 2012. Management of concussion and other head injuries model policy. https://www.maine.gov/education/sh/concussion/model-policy.html (accessed September 23, 2013).
Majerske, C. W., J. P. Mihalik, D. Ren, M. W. Collins, C. C. Reddy, M. R. Lovell, and A. K. Wagner. 2008. Concussion in sports: Postconcussive activity levels, symptoms, and neurocognitive performance. Journal of Athletic Training 43(3):265-274.
Makdissi, M., A. Collie, P. Maruff, D. G. Darby, A. Bush, P. McCrory, and K. Bennell. 2001. Computerised cognitive assessment of concussed Australian Rules footballers. British Journal of Sports Medicine 35(5):354-360.
Makdissi, M., D. Darby, P. Maruff, A. Ugoni, P. Brukner, and P. R. McCrory. 2010. Natural history of concussion in sport: Markers of severity and implications for management. American Journal of Sports Medicine 38(3):464-471.
McAllister, T. W., L. A. Flashman, A. Maerlender, R. M. Greenwald, J. G. Beckwith, T. D. Tosteson, J. J. Crisco, P. G. Brolinson, S. M. Duma, A. C. Duhaime, M. R. Grove, J. H. Turco. 2012. Cognitive effects of one season of head impacts in a cohort of collegiate contact sport athletes. Neurology 78(22):1777-1784.
McCaffrey, M. A., J. P. Mihalik, D. H. Crowell, E. W. Shields, and K. M. Guskiewicz. 2007. Measurement of head impacts in collegiate football players: Clinical measures of concussion after high- and low-magnitude impacts. Neurosurgery 61(6):1236-1243.
McClincy, M. P., M. R. Lovell, J. Pardini, M. W. Collins, and M. K. Spore. 2006. Recovery from sports concussion in high school and collegiate athletes. Brain Injury 20(1):33-39.
McCrea, M. 2001. Standardized mental status testing on the sideline after sport-related concussion. Journal of Athletic Training 36(3):274-279.
McCrea, M., J. P. Kelly, C. Randolph, J. Kluge, E. Bartolic, G. Finn, and B. Baxter. 1998. Standardized Assessment of Concussion (SAC): On-site mental status evaluation of the athlete. Journal of Head Trauma Rehabilitation 13(2):27-35.
McCrea, M., J. P. Kelly, and C. Randolph. 2000. Standardized Assessment of Concussion (SAC): Manual for Administration, Scoring and Interpretation, Second edition. Waukesha, WI: CNS Inc.
McCrea, M., K. M. Guskiewicz, S. W. Marshall, W. Barr, C. Randolph, R. C. Cantu, J. A. Onate, J. Yang, and J. P. Kelly. 2003. Acute effects and recovery time following concussion in collegiate football players: The NCAA Concussion Study. JAMA 290(19):2556-2563.
McCrea, M., T. Hammeke, G. Olsen, P. Leo, K. Guskiewicz. 2004. Unreported concussion in high school football players: Implications for prevention. Clinical Journal of Sport Medicine 14(1):13-17.
McCrea, M., K. Guskiewicz, C. Randolph, W. B. Barr, T. A. Hammeke, S. W. Marshall, and J. P. Kelly. 2009. Effects of a symptom-free waiting period on clinical outcome and risk of reinjury after sport-related concussion. Neurosurgery 65(5):876-882; discussion 882-883.
McCrea, M., L. Prichep, M. Powell, R. Chabot, W. Barr. 2010. Acute effects and recovery after sport-related concussion: A neurocognitive and quantitative brain electrical activity study. Journal of Head Trauma Rehabilitation 25(4):283-292.
McCrea, M., K. Guskiewicz, C. Randolph, W. B. Barr, T. A. Hammeke, S. W. Marshall, M. R. Powell, K. Woo Ahn, Y. Wang, and J. P. Kelly. 2013. Incidence, clinical course, and predictors of prolonged recovery time following sport-related concussion in high school and college athletes. Journal of the Inernational Neuropsychological Society 19(1):22-33.
McCrory, P. R., and S. F. Berkovic. 1998. Second impact syndrome. Neurology 50(3):677-683.
McCrory, P., A. Collie, V. Anderson, and G. Davis. 2004. Can we manage sport related concussion in children the same as in adults? British Journal of Sports Medicine 38(5):516-519.
McCrory, P., M. Makdissi, G. Davis, and A. Collie. 2005. Value of neuropsychological testing after head injuries in football. British Journal of Sports Medicine 39(Suppl 1):i58-i63.
McCrory, P., W. Meeuwisse, K. Johnston, J. Dvoøák, M. Aubry, M. Molloy, and R. Cantu. 2009. Consensus statement on concussion in sport: The 3rd International Conference on Concussion in Sport held in Zurich, November 2008. British Journal of Sports Medicine 43(Suppl 1):i76-i84.
McCrory, P., W. H. Meeuwisse, M. Aubry, B. Cantu, J. Dvoøák, R. J. Echemendia, L. Engebretsen, K. Johnston, J. S. Kutcher, M. Raftery, A. Sills, B. W. Benson, G. A. Davis, R. G. Ellenbogen, K. Guskiewicz, S. A. Herring, G. L. Iverson, B. D. Jordan, J. Kissick, M. McCrea, A. S. McIntosh, D. Maddocks, M. Makdissi, L. Purcell, M. Putukian, K. Schneider, C. H. Tator, and M. Turner. 2013a. Child-SCAT3. British Journal of Sports Medicine 47(5):263-266.
McCrory, P., W. H. Meeuwisse, M. Aubry, B. Cantu, J. Dvoøák, R. J. Echemendia, L. Engebretsen, K. Johnston, J. S. Kutcher, M. Raftery, A. Sills, B. W. Benson, G. A. Davis, R. G. Ellenbogen, K. Guskiewicz, S. A. Herring, G. L. Iverson, B. D. Jordan, J. Kissick, M. McCrea, A. S. McIntosh, D. Maddocks, M. Makdissi, L. Purcell, M. Putukian, K. Schneider, C. H. Tator, and M. Turner. 2013b. Consensus statement on concussion in sport: The 4th International Conference on Concussion in Sport held in Zurich, November 2012. British Journal of Sports Medicine 47(5):250-258.
McCrory, P., W. H. Meeuwisse, M. Aubry, B. Cantu, J. Dvoøák, R. J. Echemendia, L. Engebretsen, K. Johnston, J. S. Kutcher, M. Raftery, A. Sills, B. W. Benson, G. A. Davis, R. G. Ellenbogen, K. Guskiewicz, S. A. Herring, G. L. Iverson, B. D. Jordan, J. Kissick, M. McCrea, A. S. McIntosh, D. Maddocks, M. Makdissi, L. Purcell, M. Putukian, K. Schneider, C. H. Tator, and M. Turner. 2013c. SCAT3. British Journal of Sports Medicine 47(5):259-262.
McGrath, N. 2010. Supporting the student-athlete’s return to the classroom after a sport-related concussion. Journal of Athletic Training 45(5):492-498.
McGrath, N., W. M. Dinn, M. W. Collins, M. R. Lovell, R. J. Elbin, and A. P. Kontos. 2013. Post-exertion neurocognitive test failure among student-athletes following concussion. Brain Injury 27(1):103-113.
Meehan, W. P., III, P. d’Hemecourt, C. L. Collins, and R. D. Comstock. 2011. Assessment and management of sport-related concussions in United States high schools. American Journal of Sports Medicine 39(11):2304-2310.
Miller, J. R., G. J. Adamson, M. M. Pink, and J. C. Sweet. 2007. Comparison of preseason, midseason, and postseason neurocognitive scores in uninjured collegiate football players. American Journal of Sports Medicine 35(8):1284-1288.
Molfese, D. L., V. J. Molfese, and S. Kelly. 2001. The use of brain electrophysiology techniques to study language: A basic guide for the beginning consumer of electrophysiology information. Learning Disabilities Quarterly 24(3):177-188.
Moriarity, J. M., R. H. Pietrzak, J. S. Kutcher, M. H. Clausen, K. McAward, and D. G. Darby. 2012. Unrecognised ringside concussive injury in amateur boxers. British Journal of Sports Medicine 46(14):1011-1015.
Moser, R. S., G. L. Iverson, R. J. Echemendia, M. R. Lovell, P. Schatz, F. M. Webbe, R. M. Ruff, J. T. Barth, and National Academy of Neuropsychology Policy and Planning Committee: D. K. Broshek, S. S. Bush, S. P. Koffler, C. R. Reynolds, and C. H. Silver. 2007. Neuropsychological evaluation in the diagnosis and management of sports-related concussion. Archives of Clinical Neuropsychology 22(8):909-916.
Moser, R. S., P. Schatz, K. Neidzwski, and S. D. Ott. 2011. Group versus individual administration affects baseline neurocognitive test performance. American Journal of Sports Medicine 39(11):2325-2330.
Moser, R. S., C. Glatts, and P. Schatz. 2012. Efficacy of immediate and delayed cognitive and physical rest for treatment of sports-related concussion. Journal of Pediatrics 161(5):922-926.
NCSL (National Conference of State Legislatures). 2013. Traumatic Brain Injury Legislation. http://www.ncsl.org/issues-research/health/traumatic-brain-injury-legislation.aspx (accessed March 28, 2013).
Neurocom. 2013. Sensory organizing test. http://resourcesonbalance.com/neurocom/protocols/sensoryImpairment/SOT.aspx (accessed September 23, 2013).
New York State Department of Education. 2012. Guidelines for concussion management in the school setting. http://www.p12.nysed.gov/sss/schoolhealth/ConcussionManageGuidelines.pdf (accessed September 23, 2013).
Newman, J. B., J. H. Reesman, C. G. Vaughan, and G. A. Gioia. 2013. Assessment of processing speed in children with mild TBI: A “first look” at the validity of pediatric ImPACT. Clinical Neuropsychologist 27(5):779-793.
Oregon Department of Education. 2010. Max’s law: Concussion management implementation guide for school administrators. http://www.ode.state.or.us/teachlearn/subjects/pe/ocampguide.pdf (accessed September 23, 2013).
Otto, M., S. Holthusen, E. Bahn, N. Söhnchen, J. Wiltfang, R. Geese, A. Fischer, and C. D. Reimers. 2000. Boxing and running lead to a rise in serum levels of S-100B protein. International Journal of Sports Medicine 21(8):551-555.
Pardini, J. E., D. A. Pardini, J. T. Becker, K. L. Dunfee, W. F. Eddy, M. R. Lovell, and J. S. Welling. 2010. Postconcussive symptoms are associated with compensatory cortical recruitment during a working memory task. Neurosurgery 67(4):1020-1027; discussion 1027-1028.
Pennington, B. 2013. Flubbing a baseline test on purpose is often futile. New York Times (May 6):D7. http://www.nytimes.com/2013/05/06/sports/sandbagging-first-concussion-test-probably-wont-help-later.html?_r=0 (accessed July 17, 2013).
Peterson, C. L., M. S. Ferrara, M. Mrazik, S. Piland, and R. Elliott. 2003. Evaluation of neuropsychological domain scores and postural stability following cerebral concussion in sports. Clinical Journal of Sport Medicine 13(4):230-237.
Piland, S. G., R. W. Motl, K. M. Guskiewicz, M. McCrea, and M. S. Ferrara. 2006. Structural validity of a self-report concussion-related symptom scale. Medicine and Science in Sports and Exercise 38(1):27-32.
Poirier, M. P. 2003. Concussions: Assessment, management, and recommendations for return to activity. Clinical Pediatric Emergency Medicine 4(3):179-185.
Popoli, D. M., T. G. Burns, W. P. Meehan, III, and A. Reisner. 2013. CHOA concussion consensus: Establishing a uniform policy for academic accommodations. Clinical Pediatrics (August 19). [Epub ahead of print.]
Prichep, L. S., M. McCrea, W. Barr, M. Powell, and R. J. Chabot. 2013. Time course of clinical and electrophysiological recovery after sport-related concussion. Journal of Head Trauma Rehabilitation 28(4):266-273.
Purcell, L. K., and Canadian Paediatric Society, Healthy Active Living and Sports Medicine Committee. 2012. Evaluation and management of children and adolescents with sports-related concussion. Paediatrics & Child Health 17(1):36-37.
Putukian, M., M. Aubry, and P. McCrory. 2009. Return to play after sports concussion in elite and non-elite athletes? British Journal of Sports Medicine 43(Suppl 1):i28-i31.
Randolph, C., and M. W. Kirkwood. 2009. What are the real risks of sport-related concussion, and are they modifiable? Journal of the International Neuropsychological Society 15 15(4):512-520.
Randolph, C., M. McCrea, and W. B. Barr. 2005. Is neuropsychological testing useful in the management of sport-related concussion? Journal of Athletic Training 40(3):139-152.
Randolph, C., S. Mills, W. B. Barr, M. McCrea, K. M. Guskiewicz, T. A. Hammeke, and J. P. Kelly. 2009. Concussion Symptom Inventory: An empirically-derived scale for monitoring resolution of symptoms following sports-related concussion. Archives of Clinical Neuropsychology 24(3):219-229.
Reeves, D. L., K. P. Winter, J. Bleiberg, and R. L. Kane. 2007. ANAM® genogram: Historical perspectives, description, and current endeavors. Archives of Clinical Neuropsychology 22(Suppl 1):S15-S37.
Register-Mihalik, J., K. M. Guskiewicz, J. D. Mann, and E. W. Shields. 2007. The effects of headache on clinical measures of neurocognitive function. Clinical Journal of Sport Medicine 17(4):282-288.
Register-Mihalik, J. K., J. P. Mihalik, and K. M. Guskiewicz. 2008. Balance deficits after sports-related concussion in individuals reporting posttraumatic headache. Neurosurgery 63(1):76-80; discussion 80-82.
Register-Mihalik J. K., D. L. Kontos, K. M. Guskiewicz, J. P. Mihalik, R. Conder, and E. W. Shields. 2012. Age-related differences and reliability on computerized and paper-and-pencil neurocognitive assessment batteries. Journal of Athletic Training 47(3):297-305.
Register-Mihalik, J. K., K. M. Guskiewicz, T. C. Valovich McLeod, L. A. Linnan, F. O. Mueller, and S. W. Marshall. 2013a. Knowledge, attitude, and concussion-reporting behaviors among high school athletes: A preliminary study. Journal of Athletic Training 48(5):645-653.
Register-Mihalik, J. K., K. M. Guskiewicz, J. P. Mihalik, J. D. Schmidt, Z. Y. Kerr, and M. McCrea. 2013b. Reliable change, sensitivity, and specificity of a multidimensional concussion assessment battery: Implications for caution in clinical practice. Journal of Head Trauma Rehabilitation 28(4):274-283.
Register-Mihalik, J. K., L. A. Linnan, S. W. Marshall, T. C. Valovich McLeod, F. O. Mueller, and K. M. Guskiewicz. 2013c. Using theory to understand high school aged athletes’ intentions to report sport-related concussion: Implications for concussion education initiatives. Brain Injury 27(7-8):878-886.
Resch, J., A. Driscoll, N. McCaffrey, C. Brown, M. S. Ferrara, S. Macciocchi, T. Baumgartner, and K. Walpert. 2013. ImPACT test-retest reliability: Reliably unreliable? Journal of Athletic Training 48(4):506-511.
Riemann, B. L., K. M. Guskiewicz, and E. Shields. 1999. Relationship between clinical and forceplate measures of postural stability. Journal of Sport Rehabilitation 8(2):71-82.
Rimel, R. W., B. Giordani, J. T. Barth, and J. A. Jane. 1982. Moderate head injury: Completing the clinical spectrum of brain trauma. Neurosurgery 11(3):344-351.
Sady, M. D., C. G. Vaughan, and G. A. Gioia. 2011. School and the concussed youth: Recommendations for concussion education and management. Physical Medicine and Rehabilitation Clinics of North America 22(4):701-719.
Sandel, N. K., M. R. Lovell, N. Kegel, M. W. Collins, and A. P. Kontos. 2012. The relationship of symptoms and neurocognitive performance to perceived recovery from sports-related concussion among adolescent athletes. Applied Neuropsychology: Child 2(1):64-99.
Saunders, R. L., and R. E. Harbaugh.1984. Second impact in catastrophic contact-sports head trauma. JAMA 252(4):538-539.
Schatz, P. 2010. Long-term test-retest reliability of baseline cognitive assessments using ImPACT. American Journal of Sports Medicine 38(1):47-53.
Schatz, P., and C. S. Ferris. 2013. One-month test-retest reliability of the ImPACT test battery. Archives of Clinical Neuropsychology 28(5):499-504.
Schatz, P., and B. O. Putz. 2006. Cross-validation of measures used for computer-based assessment of concussion. Applied Neuropsychology 13(3):151-159.
Schatz, P., and N. Sandel. 2013. Sensitivity and specificity of the online version of ImPACT in high school and collegiate athletes. American Journal of Sports Medicine 41(2):321-326.
Schatz, P., J. Pardini, M. R. Lovell, M. W. Collins, and K. Podell. 2006. Sensitivity and specificity of the ImPACT Test Battery for concussion in athletes. Archives of Clinical Neuropsychology 21(1):91-99.
Schmidt, J. D., J. K. Register-Mihalik, J. P. Mihalik, Z. Y. Kerr, and K. M. Guskiewicz. 2012. Identifying impairments after concussion: Normative data versus individualized baselines. Medicine & Science in Sports & Exercise 44(9):1621-1628.
Schneider, J., and G. Gioia. 2007. Psychometric properties of the Post-Concussion Symptom Inventory (PCSI) in school age children. [Abstract.] Developmental Neurorehabilitation 10(4):282.
Segalowitz, S., P. Mahaney, D. Santesso, L. MacGregor, J. Dywan, and B. Willer. 2007. Retest reliability in adolescents of a computerized neuropsychological battery used to assess recovery from concussion. NeuroRehabilitation 22(3):243-251.
Stålnacke, B. M., Y. Tegner, and P. Sojka. 2003. Playing ice hockey and basketball increases serum levels of S100B in elite players: A pilot study. Clinical Journal of Sport Medicine 13:292-302.
Straume-Naesheim, T. M., T. E. Andersen, and R. Bahr. 2005. Reproducibility of computer based neuropsychological testing among Norwegian elite football players. British Journal of Sports Medicine 39(Suppl 1):i64-i69.
Suskauer, S. J., and T. A. Huisman. 2009. Neuroimaging in pediatric traumatic brain injury: Current and future predictors of functional outcome. Developmental Disabilities Research Review 15(2):117-123.
Teasdale, G., and B. Jennett. 1974. Assessment of coma and impaired consciousness: A practical scale. Lancet 2(7872):81-84.
Thériault, M., L. De Beaumont, N. Gosselin, M. Filipinni, and M. Lassonde. 2009. Electrophysiological abnormalities in well functioning multiple concussed athletes. Brain Injury 23(11):899-906.
Thériault, M., L. De Beaumont, S. Tremblay, M. Lassonde, and P. Jolicoeur. 2011. Cumulative effects of concussions in athletes revealed by electrophysiological abnormalities on visual working memory. Journal of Clinical and Experimental Neuropsychology 33(1):30-41.
Toledo, E., A. Lebel, L. Becerra, A. Minster, C. Linnman, N. Maleki, D. W. Dodick, and D. Borsook. 2012. The young brain and concussion: Imaging as a biomarker for diagnosis and prognosis. Neuroscience and Biobehavioral Review 3(6):1510-1531.
Torres, D. M., K. M. Galetta, H. W. Phillips, E. M. S. Dziemianowicz, J. A. Wilson, E. S. Dorman, E. Laudano, S. L. Galetta, and L. J. Balcer. 2013. Sports-related concussion: Anonymous survey of a collegiate cohort. Neurology Clinical Practice 3(4):279-283.
Tsao, J. W. 2013. Navy and Marine Corps TBI Efforts. Presentation before the committee, Washington, DC, February 25.
Tsushima, W. T., N. Shirakawa, and O. Geling. 2013. Neurocognitive functioning and symptom reporting of high school athletes following a single concussion. Applied Neuropsychology: Child 2(1):13-16.
Vagnozzi, R., S. Signoretti, L. Cristofori, F. Alessandrini, R. Floris, E. Isgro, A. Ria, S. Marziale, G. Zoccatelli, B. Tavazzi, F. Del Bolgia, R. Sorge, S. P. Broglio, T. K. McIntosh, and G. Lazzarino. 2010. Assessment of metabolic brain damage and recovery following mild traumatic brain injury: A multicentre, proton magnetic resonance spectroscopic study in concussed patients. Brain 133(11):3232-3242.
Valovich McLeod, T. C., and C. Leach. 2012. Psychometric properties of self-report concussion scales and checklists. Journal of Athletic Training 47(2):221-223.
Van Kampen, D. A., M. R. Lovell, J. E. Pardini, M. W. Collins, and F. H. Fu. 2006. The “value added” of neurocognitive testing after sports-related concussion. American Journal of Sports Medicine 34(10):1630-1635.
Vaughan, C., G. A. Gioia, and D. Vincent. 2008. Initial examination of self-reported postconcussion symptoms in normal and mTBI children ages 5 to 12. [Abstract.] Journal of the International Neuropsychological Society 14(Suppl 1):207.
Virji-Babul, N., M. R. Borich, N. Makan, T. Moore, K. Frew, C. A. Emery, and L. A. Boyd. 2013. Diffusion tensor imaging of sports-related concussion in adolescents. Pediatric Neurology 48(1):24-29.
VistaLifeSciences. 2013. ANAM4 FAQs. http://www.vistalifesciences.com/anam-faq.html (accessed September 23, 2013).
Weir, J. P. 2005. Quantifying test-retest reliability using the intraclass correlation coefficient and the SEM. Journal of Strength and Conditioning Research 19(1):231-240.
Wilde, E. A., S. R. McCauley, J. V. Hunter, E. D. Bigler, Z. Chu, Z. J. Wang, G. R. Hanten, M. Troyanskaya, R. Yallampalli, X. Li, J. Chia, and H. S. Levin. 2008. Diffusion tensor imaging of acute mild traumatic brain injury in adolescents. Neurology 70(12):948-955.
Willer, B., and J. J. Leddy. 2006. Management of concussion and post-concussion syndrome. Current Treatment Options in Neurology 8(5):415-426.
Woodard, J., C. Marker, F. Tabanico, S. Miller, E. Corsett, L. Cox, F. Gould, and J. Bleiberg. 2002. A validation study of the Automated Neuropsychological Assessment Metrics (ANAM) in non-concussed high school players. [Abstract.] Journal of the International Neuropsychological Society 8(2):175.
Yeates, K. O., H. G. Taylor, J. Rusin, B. Bangert, A. Dietrich, K. Nuss, M. Wright, D. S. Nagin, and B. L. Jones. 2009. Longitudinal trajectories of postconcussive symptoms in children with mild traumatic brain injuries and their relationship to acute clinical status. Pediatrics 123(3):735-743.
Yeates, K. O., E. Kaizar, J. Rusin, B. Bangert, A. Dietrich, K. Nuss, M. Wright, and H. G. Taylor. 2012. Reliable change in postconcussive symptoms and its functional consequences among children with mild traumatic brain injury. Archives of Pediatrics and Adolescent Medicine 166(7):615-622.


















































































