
6
Protection and Prevention Strategies
This chapter addresses the portion of the committee’s statement of task concerning the effectiveness of protection devices and equipment and sports regulations for the prevention of concussions. The chapter begins with an overview of research on the effectiveness of protective equipment for the prevention and mitigation of sports-related concussions in youth. The committee’s information gathering for this section included the commissioning of a paper that reviews the published literature on the ability of helmets to reduce the risk of sports-related concussions in youth (Duma et al., 2013). The chapter then discusses the roles of sports rules, concussion education initiatives, and state concussion legislation in concussion awareness and prevention. The chapter concludes with the committee’s findings for this portion of its charge.
There is debate around the words “prevention” and “reduction” relative to concussions in youth sports (Duma et al., 2013). All activity involves some risk of injury. Although it may be impossible to prevent all sports-related concussions in youth, measures can be taken to reduce the risk of these injuries. Similarly, in modern medicine, although preventive measures such as screening examinations and prophylactic use of medications will not avert all disease in all individuals, such measures can decrease the risk for disease.
Helmets and Other Headgear
Helmets are designed to mitigate the likelihood of head injuries from an impact to the head by dissipating and distributing the energy of impact
and protecting the head from penetration. Early helmets were designed to prevent such injuries as skull fractures as well as moderate to severe brain injuries such as focal contusions and hemorrhages. The typical helmet has a comfort liner, an impact energy attenuating liner, a restraint system, and a shell. Some helmets, such as those used in motor sport, bicycling, and alpine skiing, are designed to attenuate a single impact. Once one of these single-impact helmets has sustained an impact, it must be replaced. Other helmets, such as those used in ice hockey, football, and lacrosse, are designed to withstand multiple impacts over a season of games and practices (Hoshizake and Brien, 2004). Part of the difference between single-impact helmets and multiple-impact helmets lies in the materials used. For example, multiple-impact helmets, such as those for hockey and football, use materials that do not permanently deform but rather compress and return to their original dimensions. Inner shells can be made of vinyl nitrile or expanded polypropylene, and outer shells use lightweight plastics and composites for durability and protection. Single-impact helmets contain materials that are frangible and deform or fracture permanently upon impact as part of their energy management strategy.
Helmet design involves a series of trade-offs between optimal safety and parameters such as the thickness and other characteristics of the attenuation material, the size and mass of the helmet, comfort, and acceptability. A primary goal of the attenuation layer is to decrease the peak deceleration and to increase the time duration over which the deceleration occurs; this can be achieved by a thicker or more compliant layer of material which improves the energy management by reducing the peak linear deceleration upon impact. However, better energy management via an increased thickness results in a large helmet that may be unacceptable from a style, agility, or visibility standpoint. A helmet with increased mass would have reduced linear head acceleration for a given force; however, it may actually increase the rotational acceleration generated from an impact because there would be an increased radius over which the forces are acting.
Review of the Biomechanics of Concussion
In order to determine if helmet design can indeed be protective against concussion, one must first understand what mechanical events lead to concussions and then determine whether the helmet can mitigate those mechanical forces. The key biomechanical principles that define the mechanics of concussion were discussed in detail in Chapter 2 and are only briefly reviewed here. Local brain tissue deformation (i.e., strain) has been shown to cause brain injury as defined by loss of consciousness, white matter injury, hemorrhage, cell death, or some combination of these (Cater et al., 2006; Elkin and Morrison, 2007; LaPlaca et al., 2005; Margulies and Coats,
2013; Monson et al., 2003; Raghupathi and Margulies, 2002; Raghupathi et al., 2004). If the magnitude or rate of tissue strain is high, local tissue damage occurs. The threshold for the amount of strain required to cause a concussion is unknown, as is whether that threshold varies by age, direction, or individual biological and physiological characteristics. Researchers have developed computational models designed to calculate the distortion of brain tissue that results from global head kinematics such as the acceleration or velocity associated with head impacts in sports (e.g., Kleiven, 2007; Post et al., 2011, 2012; Takhounts et al., 2003), but the thresholds used in these studies are not directly applicable to youth concussions as they are often extrapolated from adult human or animal data. Furthermore, the computational models required to make this translation are hampered by a lack of the pediatric-specific brain and skull data needed to ensure that the model adequately mimics a real child.
There are several key mechanical factors that influence brain strain that need to be considered when examining the potential concussion-reducing effect of helmets. These include (1) head-impact versus non-head-impact scenarios, (2) rotational versus linear acceleration, and (3) centroidal versus non-centroidal impacts. Because a concussion is a diffuse injury rather than a focal one, the primary difference between an impact directly to the head and an impact to the body that accelerates or decelerates the head is the overall magnitude of the acceleration. Impacts directly to the head raise the risk of focal injuries such as skull fractures and brain contusions, but they have also been shown to result in head accelerations of greater magnitude (Kimpara and Iwamoto, 2012). Work by Ommaya and colleagues in the 1960s and 1970s demonstrated that loading via direct head impact resulted in unconsciousness at lower input severities (Ommaya and Gennarelli, 1974; Ommaya et al., 1971), and studies of diffuse axonal injury, a severe form of diffuse brain injury, have reported that an impact is likely necessary to decelerate the head quickly enough to cause such injury (Yoganandan et al., 2009). Impacts to the body, which occur frequently in such contact sports as football and ice hockey, can induce a whiplash-like movement of the head which may be able to generate high enough accelerations to cause injury without subsequent head impact, but the impact velocity to the body must be high. A more common concussion-causing scenario occurs when an impact to the body (i.e., person to person) causes the head to hit some other surface (i.e., boards in hockey or the playing surface in football).
An impact to the head can result in both linear and rotational accelerations. These two types of acceleration can at times be very strongly correlated (Newman et al., 1999; Pellman et al., 2003; Viano et al., 2012b), but this is often not the case.
The centricity of the impact—that is, whether the impact is directed through the center of mass of the head (centroid) or not—is critical to un-
derstanding the role of rotational versus linear acceleration in concussion mechanics. Post and colleagues (2011, 2012) conducted an experimental and computational study of centroidal and non-centroidal impacts to a helmeted head. In those impacts directed through the center of mass of the head (centroidal impacts), linear acceleration had a strong correlation with rotational acceleration. For non-centroidal impacts (those not directed through the center of mass) the relationship between linear and rotational acceleration was weak. Furthermore, in those non-centroidal impacts rotational acceleration correlated strongly with brain tissue injury metrics such as strain (correlation=0.638) and stress (correlation=0.677), while linear acceleration did not (correlation=–0.238). These findings were replicated in a study of impacts on equestrian helmets (Forero Rueda et al., 2011) and in simulations of National Football League (NFL) concussion cases (Kleiven, 2007). Walsh and colleagues (2011) also reported that linear and rotational acceleration were only moderately correlated especially in non-centroidal impacts.
Chapter 2 highlighted several animal studies that examined the independent role of linear and rotational acceleration in producing concussions. This research suggested that those scenarios in which the head was allowed to rotate resulted in a greater likelihood of concussion and that a pure linear motion of the head was unlikely to produce such injuries (Hardy et al., 2001; King et al., 2003; Ommaya and Gennarelli, 1974; Ommaya et al., 1971).
These laboratory animal studies with controlled loading conditions examined the influence of linear or rotational accelerations on brain injury risk independently. In sports, however, the vast majority of impacts to the head result in a combination of both linear and rotational motions; it is unlikely to have either purely linear or purely rotational acceleration. Recent head impact data collected in athletes on the playing field using helmet-based sensors, such as the Head Impact Telemetry (HIT) system (see Beckwith et al., 2012; Rowson et al., 2009), initially focused on the role of linear acceleration in concussion risk. From these studies it has been proposed that reducing linear acceleration would lead to reductions in concussion risk (Funk et al., 2012; Rowson and Duma, 2011). However, such conclusions are influenced by important design limitations in how these systems collect and process data. For example, the HIT system does not directly measure rotational acceleration or velocity but rather estimates it from linear acceleration using geometrical assumptions. As a result, the rotational kinematic measures provided by the HIT system have less accuracy than its linear measures do (Allison et al., 2013; Jadischke et al., 2013). In the case of head motions that may have both rotational and linear components, researchers would ideally use independent measures of linear and rotational acceleration (e.g., Camarillo et al., 2013) in order
to evaluate which of these types of movements are associated with greater concussion risk.
When interpreting data on the safety benefits of helmets or other protective devices, it is important to realize that a particular reduction in either linear or rotational acceleration does not necessarily correspond to a similar reduction in concussion risk. Injury risk curves describe the probability of injury given a specific mechanical input—that is, the risk of concussion given a particular rotational acceleration. This relationship is not linear but rather sigmoid (s-shaped), often in the form of a Weibull distribution or some other cumulative distribution function (see Figure 6-1). As a result, a 25 percent reduction in acceleration, for example, could actually correspond to a very small decrease in the probability of injury if the values of acceleration lie in the early lower left region of the curve. On the other hand, if the 25 percent acceleration reduction is along the steep portion of
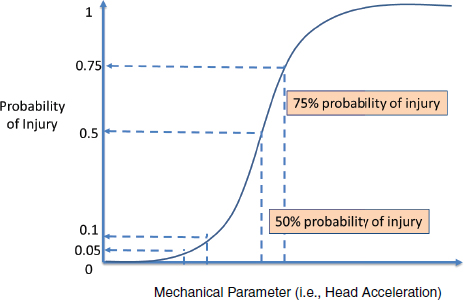
FIGURE 6-1 Injury risk curve relating a mechanical parameter such as head acceleration to the probability of injury. Note that a given reduction in the mechanical parameter does not correspond to an equivalent reduction in injury risk due to the sigmoidal shape of the curve. If the reduction in the mechanical parameter is on the left side of the curve, the corresponding reduction in injury risk is rather small (10 percent to 5 percent in the example above). In contrast, if the reduction in the mechanical parameter is in the steep portion of the curve, the actual injury risk reduction could be rather large (75 percent to 50 percent in the example above).
the risk curve, the corresponding reduction in concussion risk may actually be much greater than 25 percent.
Other research attempted to quantify the relationship between head kinematics and concussion risk using injury risk curves. The initial attempts proposed quantitative relationships between concussion risk and linear acceleration; for example, Pellman and colleagues (2003) used reconstructions of impacts in the NFL, and Rowson and Duma (2011) used collegiate data collected with the HIT system. These efforts focused on linear kinematic measures and thus did not include an evaluation of the influence of rotational kinematics on injury risk. Other researchers have developed injury risk curves that incorporate rotational acceleration or velocity; however, these studies are limited by small sample sizes, particularly of the uninjured (Zhang et al., 2004), include estimates of rotational kinematics that have substantial measurement error and incorporate a generic approximation of concussion underreporting (Rowson et al., 2012). More recently, Rowson and Duma (2013) developed a promising concussion risk curve that includes a combination of linear and rotational acceleration; however, this study non-randomly reclassified players who reported no injury to the injured group thus biasing the relationship between acceleration and injury outcome in a way that makes interpretation difficult. None of the risk curves in the literature comprehensively account for parameters such as impact direction, previous concussion history, or other biological or physiological parameters, all of which likely influence the quantitative relationship. Most importantly, all of the existing risk curves are based on data from collegiate or professional football and cannot be directly applied to children and adolescents.
Evidence That Helmets Have the Potential to Mitigate Concussion Risk
Biomechanical evidence Based on the preceding discussion of the mechanics of concussion, devices that reduce both linear acceleration and rotational acceleration or velocity of the head have the potential to reduce the risk of concussion (Benson et al., 2009, 2013). Reductions in linear acceleration with particular helmet designs may help mitigate skull fractures and other focal brain injuries and likely contribute to some reduction in concussion risk. However, due to the decoupling of linear and rotational acceleration under certain impact conditions as described above, reductions of linear acceleration alone do not necessarily translate into a reduced concussion risk in most impact conditions.
There is some evidence, however, that helmets can indeed reduce rotational acceleration. By comparing the impacts of a bare anthropomorphic test device (ATD) head to one fitted with a football helmet, it has been shown that helmets reduce rotational acceleration by approximately 30
percent (Viano and Halstead, 2012). In a follow-up study, Viano described generic changes in football helmet design that led to decreases in rotational acceleration, suggesting that there are aspects of helmet design that can be modified to reduce the angular motion of the head (Viano et al., 2012b). Post and colleagues (2011) studied different hockey helmet designs through physical testing and a computational model. The helmets demonstrated variability in rotational acceleration which corresponded to variations in brain injury metrics such as maximum principal strain and Von Mises stress.1 Some helmet designs that passed all relevant standards currently based on linear acceleration produced relatively high brain injury metrics (strain) as a result of the angular motion (Post et al., 2011). A similar effect has been observed in speed skating and bicycle helmets (Karton et al., 2012). Rousseau and colleagues (2009) evaluated two different liner materials (vinyl nitrile and expanded polypropylene foam) in hockey helmets and found that while the resulting linear accelerations of the head were similar for the two materials, they differed in the rotational accelerations produced.
In an effort to reduce rotational energy in helmet impacts, several companies have developed a novel helmet design in which a lubricated flexible membrane is placed either on the outside of the helmet or on the inside between the head and the padding. The fundamental idea underlying this new helmet design is the addition of a low-friction layer between the head and the padding that will reduce the rotational acceleration transmitted to the head. Its benefits vary by impact direction. This design concept has been applied, for example, under the MIPS (Multi-directional Impact Protection System) name for equestrian, alpine skiing, snowboarding, and cycling helmets2 and under the Suspend-Tech name by Bauer for hockey helmets. Recently, Hansen and colleagues described the development of such a system in bicycle helmets that was shown to reduce rotational acceleration in oblique impacts by 34 percent (Hansen et al., 2013). While this design approach is promising and suggests that the characteristics of a helmet can be manipulated to reduce rotational acceleration, until an appropriate injury threshold for concussion can be developed that is age- and direction-specific, it will not be clear what levels of rotational acceleration are acceptable and therefore it will remain impossible to quantify the influence of these design changes on actual concussion risk.
In addition to helmets, several other protective devices have emerged that claim to reduce concussion risk. Soccer head gear is a primary example.
____________________________________
1Maximum principal strain refers to the maximum value of elongation or stretch along one of the principal axes of strain. Von Mises stress refers to an equivalent stress (force/area) and is used to determine if the stress state would result in failure of the material. These two metrics are used separately or together in brain injury mechanics to assess whether a brain will sustain injury under a certain set of loading conditions.
2See http://mipshelmet.com/find-a-helmet (accessed October 7, 2013).
Understanding the role that soccer headgear plays in impacts to the head involves understanding the nature of differences between impacts with hard surfaces, such as other players, goal posts, or the ground, and impacts with the compliant surface of the ball (Niedfeldt, 2011; Spiotta et al., 2012). In an impact between the more compliant ball and a noncompliant head, the ball will deform and absorb the energy of the impact, thus reducing the peak acceleration and increasing the duration of the impact. Headgear has the potential to change the duration of the impact and lower the peak linear acceleration during heading only if it is at least as compliant as the ball and it does not compress fully. Once it compresses fully, it loses its ability to attenuate or reduce the energy transferred to the head. Current headgear compresses fully and rather easily upon impact.
The efficacy of soccer headgear in reducing head acceleration has been tested in the laboratory. Withnall and colleagues (2005) conducted volunteer testing of heading and observed that, because of the amount of ball deformation that occurs during the impact, the linear acceleration of the head did not vary with the use of head gear. When these researchers mimicked head-to-head contact using two ATD headforms, because the head form is not deformable the headgear provided an overall 33 percent reduction in both linear acceleration and a metric that included both linear and rotational acceleration. Their findings likely apply to impacts with other solid objects as well, such as an opponent’s elbow, the ground, or the goal post. The findings were confirmed by Naunheim and colleagues (2003), who observed no effect of headgear on impacts from heading but noted attenuation of the impact via the headgear in higher-speed impacts with a noncompliant surface.
Epidemiologic evidence Epidemiological evidence that helmets mitigate concussion primarily comes from the bicycle helmet literature. In a review of five case-control studies from the literature, Thompson and colleagues (2000) concluded that bicycle helmets reduce the risk of head injury (defined as any injury to the brain or skull) by 69 percent, the risk of brain injury by 69 percent, and the risk of more serious brain injury (a score of 3 or more as measured by the Abbreviated Injury Scale score, or AIS) (see AAAM, 1998) by 74 percent as compared with control groups consisting of individuals who visited emergency departments after bicycle accidents in which they were not wearing helmets. Furthermore, when they used a control population of all cyclists who crashed, they documented even stronger benefits (85 percent reduction of head injury, 88 percent reduction in brain injury). Although these studies do not specifically separate out concussion injuries, approximately 70 percent of the brain injury subgroup in the study sustained injuries of an AIS 2 level, most of which were likely concussions. The studies they reviewed did not focus exclusively on children, but about
two-thirds of the population studied were children and adolescents. One of the studies (Thompson et al., 1996) found no effect of age on the effectiveness of the helmet in preventing head injury but suggested that there was a trend that the helmet’s effectiveness in preventing brain injury decreased with increasing age.
In the sports environment, by contrast, the epidemiological evidence of helmet effectiveness in preventing concussions is not as strong. Collins and colleagues (2006) demonstrated that newer football helmet technology in high school athletes resulted in a 31 percent decrease in the relative risk of concussion compared to older helmet designs, suggesting that some aspects of helmet design can help mitigate concussion. However, the absolute decrease in risk in this study was only 2 percent (7.6 percent versus 5.3 percent), suggesting that these findings were not very robust. In equestrian sports, the use of protective riding helmets has been associated with a fivefold reduction in head injury (Havlik, 2010), and similar benefits have been documented in some studies of skiing and snowboarding helmets (Hagel et al., 2005; Mueller et al., 2008; Sulheim et al., 2006); however, these studies have not specifically looked at concussions.
The most substantial line of research has been in the evaluation of protective headgear in the sport of rugby, where results have been conflicting. In an early study of 16 “under 15” rugby teams, McIntosh and McCrory (2001) found no difference in concussion rates with headgear usage; however, this study suffered from selection bias because the use of headgear was not randomized (McIntosh and McCrory, 2001). Players could chose to wear or not wear headgear, and it is possible that players’ perceived risks influenced their decision. A later study involving male rugby players of ages 12 to 19 corrected this flaw by randomizing participants to standard headgear, modified headgear (made from a thicker and denser foam than standard headgear), or no headgear. There was a nonsignificant trend toward wearers of the modified headgear, who have a lower likelihood of missing a game due to concussion, than toward wearers of the standard headgear; however, the subjects in this study showed poor compliance with the headgear use, and there was limited control for such confounding variables as player position and previous concussion history (McIntosh et al., 2009; Navarro, 2011). Kemp and colleagues (2008) prospectively enrolled a cohort of adult rugby players and documented a 57 percent reduction in concussion risk with the use of headgear. Those researchers used a symptom-based definition of concussion which was broader than the definition used by McIntosh and colleagues (2009). In prospective studies, Hollis and colleagues (2009) found that male nonprofessional rugby players (n=3,207) who self-reported that they always wear headgear during games were less likely to sustain a mild traumatic brain injury (mTBI) over one playing season (incidence rate ratio = 0.57; 95% confidence interval [CI],
0.40-0.82). Conversely, in a cohort study of both adult and adolescent male and female rugby players (n=304), Marshall and colleagues (2005) found that rugby headgear had no protective effect on concussions.
In soccer the only formal epidemiological evaluation of headgear in the literature was conducted by Delaney and colleagues (2008), who reported that among Canadian male and female soccer players ages 12 to 17 (n=278) those who did not use headgear were 2.6 times more likely to sustain a concussion than those who did. However, there are important methodological limitations to this study that bias its conclusions. The most important of these is the fact that the use of protective headgear was not randomized so that the headgear may have been used by those who felt they were at risk due to their style of play or occurrence of previous concussions. Furthermore, the outcomes were all obtained via self-report using unvalidated tools (Delaney et al., 2008; Navarro, 2011).
In sum, epidemiological evidence that helmets and other protective devices actually reduce the risk of concussions is lacking. Carefully controlled epidemiological studies are needed to further evaluate these devices’ potential for protection.
Helmet Standards
Organizations such as the National Operating Committee on Standards for Athletic Equipment (NOCSAE) and ASTM International (formerly the American Society for Testing and Materials) have developed helmet standards that specify test protocols and quantitative impact criteria such as the Head Injury Criterion or the Severity Index (see Gadd, 1966; Versace, 1971). These standards are performance standards and do not specify materials or design. They are often sport-specific, and some have different tolerance thresholds for youth helmets than for adult helmets. Such standards were developed initially to prevent skull fracture, and at their core they remain true to that mission today. Many of the standards include a drop test of the helmet with a humanoid headform at specified impact locations and velocities and require that the headform experience linear acceleration below a prescribed threshold known to cause fracture. None of these standards incorporate a measure of rotational acceleration, nor do they include a test protocol that would probe the ability of the helmet to mitigate rotational forces that, as described above, have been shown to cause concussion.
There is considerable controversy among experts on the relevance of these test standards for concussion prevention. There are advocates of this testing methodology who claim that reductions in linear acceleration lead to reductions in angular acceleration and therefore holding helmets to a linear acceleration–based standard decreases the risk of concussions (Rowson and
Duma, 2011). There are others who point out that, as highlighted above, linear and rotational acceleration are not always correlated—particularly in the oblique and non-centroidal impacts that occur often on the playing field—and that any helmet standard or rating system that relies solely on reducing linear acceleration will be limited (Forero Rueda et al., 2011; Halldin et al., 2001; McIntosh et al., 2011).
In addition to testing standards for helmets, helmet rating systems have also begun to emerge. One is the STAR rating system, developed by engineers at Virginia Tech. It is a quantitative metric for rating football helmets that combines concussion injury risk and a theoretical distribution of head impact exposure by impact direction and severity with a helmet’s linear acceleration response from NOCSAE-like drop tests at various impact locations and drop heights (Rowson and Duma, 2011).
The STAR system is theoretically grounded and represents an intriguing approach to how the injury mitigation properties of a helmet could be assessed. However, the rating system contains several assumptions that limit its generalizability. These include (1) estimates of an average number of head impacts per player per season and a distribution of impact direction based on collegiate data; (2) use of a NOCSAE-like drop test which limits the injury risk curve to linear acceleration alone; (3) a concussion risk curve that does not incorporate injury sensitivity to impact direction which has been shown to be an important parameter in head injury thresholds (Gennarelli et al., 1987; Hodgson et al., 1983; Kleiven, 2003; Margulies et al., 1990); and (4) the use of concussion incidence rates derived from college data to weight the injury and non-injury data including a factor of 50 percent applied universally to the data to account for underreporting.
Because the assumptions outlined above are based on collegiate data, the STAR rating system as currently defined cannot be directly utilized to rate helmets for pre-college-age youth. In order to extend the rating systems like the STAR system to younger populations, the following pediatric-specific data would need to be collected: (1) the number of head impacts and the distribution of impact location per season, (2) the distribution of impact severity by impact location, and (3) an injury risk curve for concussion. These data should be acquired using measurement systems that reliably assess impact direction and impact severity and include both linear and rotational motions. It is important that the rating system incorporate the measurement error of these systems perhaps as a confidence range for injury risk. For example, the measurement error associated with the HIT system, which has been used to generate the data for the current STAR system and is being used to collect pediatric-specific data, has recently been reported to be higher than previously published (Allison et al., 2013; Jadischke et al., 2013). Furthermore, it is likely that several of these data sets will need to be created across the pediatric age range—a rating system for high school
helmets is likely not the same as one for youth football helmets. It would also be important that a rating system consider how to incorporate such parameters as helmet fit, helmet condition, and individual variations in style of play or concussion risk and history that are likely to also influence the probability of injury.
In sum, helmet rating systems have the potential to provide useful information to guide consumer decision making. The STAR system is based upon sound principles but is limited by the data available to develop concussion risk curves and thresholds. Through collection of data that could replace some of the assumptions outlined above, its value for widespread application would be increased.
Advances in helmet test standards that incorporate new methods and new injury criteria that evaluate protection in both linear and rotational loading modes are needed before real progress can be made on this issue. NOCSAE, to offer one example, has research under way to develop such test protocols, but the limiting factor may be having sufficiently robust, age-dependent concussion tolerance criteria with which to interpret the results of such tests.
Mouthguards
A mouthguard is a protective device for the mouth that fits over the teeth and gums in order to prevent or reduce the severity of dental and maxillofacial injuries. Research indicates that properly fitted mouthguards reduce the incidence of dental and maxillofacial injuries in sports (Barbic et al., 2005; Daneshvar et al., 2011; Knapik et al., 2007; Labella et al., 2002; Marshall et al., 2005; McNutt et al., 1989; Viano et al., 2012a). One meta-analysis of studies comparing mouthguard users and nonusers showed that the overall risk of orofacial injury is 1.6 to 1.9 times greater when a mouthguard is not worn than when a mouthguard is worn (Knapik et al., 2007). Mouthguards are mandated in several youth contact sports. Both the National Collegiate Athletic Association (NCAA) and the National Federation of State High School Associations (NFHS) require the use of mouthguards in football, ice hockey, field hockey, and lacrosse (Knapik et al., 2007; NFHS, 2011). Some states have passed legislation requiring the use of mouthguards by youth in certain sports. The American Dental Association, although it has no formal authority over youth sports, recommends that individuals who participate in contact sports as well as those who participate in several non-contact sports such as gymnastics, skiing, and track and field, wear a properly fitted mouthguard during practice and competition to prevent dental injuries (ADA, 2004).
There are three broad categories of mouthguards: stock, boil-and-bite, and custom-fitted. Stock mouthguards come ready to wear. Boil-and-bite
mouthguards are made of a thermoplastic material that is softened in boiling water and then formed to fit over the teeth as it cools. Both stock and boil-and-bite mouthguards are relatively inexpensive and may be purchased at sporting goods outlets. Custom-fitted mouthguards are made by a dental professional. They are more expensive, but these mouthguards offer the best fit because they are made using a mold of the athlete’s mouth. The majority of all mouthguards worn by nonprofessional athletes are of the boil-and-bite type (Barbic et al., 2005; Wisniewski et al., 2004). Some research indicates that custom-fitted mouthguards are better for preventing dental and maxillofacial injuries than are other types of mouthguards (Bemelmanns and Pfeiffer, 2001; Finch et al., 2005; Hoffman et al., 1999).
It has been speculated that mouthguards may reduce the risk of concussions caused by impact to the jaw by positioning the jaw to absorb some of the forces that would otherwise be transferred through the base of the skull to the brain (Knapik et al., 2007; Takeda et al., 2005). One biomechanical study found that when hits to the mandibular undersurface of a mechanical skull were applied, the presence of a mouthguard significantly (p < .01) decreased surface distortions related to deformation or fractures to the mandibular bone (by 54.7 percent) and significantly decreased linear acceleration of the head (by 18.5 percent) compared to when a mouthguard was not in place. Nonetheless, the authors of this study acknowledged that further well-designed research is needed on the relationship between mouthguards and concussion risk. Another group of researchers, who worked with a cadaver model, found that having a mouthguard in place reduced by 50 percent the amplitude of bone deformation and intracranial pressure that followed a hit to the chin (Hickey et al., 1967). As noted by McCrory (2001), however, this research does not translate well to live humans because of differences in the compliance of cadaveric and live human tissue, among other reasons.
Several epidemiologic studies have assessed the differences in concussion incidence between users and nonusers of mouthguards as well as between users of custom-made and non-custom-made mouthguards. On the whole, the available research suggests no significant difference in the risk of concussion for athletes who wear mouthguards and those who do not (Benson et al., 2009; Labella et al., 2002). One of the larger, more well-designed studies followed 50 men’s NCAA Division I basketball teams over one season and found no significant differences between mouthguard users and nonusers in rates of concussions (0.35 versus 0.55) (Labella et al., 2002). Furthermore, there is no evidence that custom-made mouthguards offer any more protection against concussion than other types of mouthguards. One large prospective study collected data for 87 NCAA Division I-A football teams over a 15-week period. Over the course of all the games and practices, 369 physician-verified concussions were reported.
No statistical difference was observed in either concussion incidence or concussion severity between players who wore custom-made mouthguards and those who wore non-custom-made mouthguards (Wisniewski et al., 2004). Another small longitudinal study evaluated concussion incidence among 28 high school football players before and after implementation of a customized mandibular orthotic. The mean self-reported incidence of concussion/mTBI for the two seasons prior to the use of the orthotic was 2.1 ± 1.4 events per player, which amounted to 59 concussions/mTBIs. Following the implementation of the orthotic, three concussions/mTBIs were reported over three seasons; the number of concussive events per player fell to 0.11 ± 0.31 with an odds ratio (OR) of 38.33 (95% CI, 8.2-178.6) (Singh et al., 2009). This finding was significant but limited by the small sample size and the fact that 23 of the 28 players had a previous history of concussion, suggesting the possibility of self-selection bias. Player compliance with the orthotics was not reported (Navarro, 2011; Singh et al., 2009).
The WIPSS Brain-Pad mouthguard is a two-layered boil-and-bite mouthguard that fits over the upper and lower teeth. It is designed to minimize acceleration forces more than other mouthguards by maintaining a space at the temporomandibular joint (Barbic et al., 2005). At one time the packaging for a version of this mouthguard developed for youth stated that it could reduce the risk of concussions from lower jaw impacts (U.S. Senate Committee on Commerce, Science, and Transportation, 2011). A multicenter, cluster-randomized trial involving 614 male football players and male and female rugby players at universities in Ontario, Canada, found no significant difference in the number of concussions observed between athletes who wore the WIPPS Brain-Pad mouthguard and athletes in the control group who continued to use their mouthguard of choice. There were 22 and 21 concussions in the intervention and in the control group, respectively (Barbic et al., 2005).
Mihalik and colleagues (2007) investigated possible differences in neurocognitive and symptomatic impairments in youth athletes who were concussed while wearing a mouthguard versus those who were concussed while not wearing a mouthguard. Baseline neurocognitive testing was performed before the start of the season using Immediate Post-Concussion Assessment and Cognitive Testing (ImPACT) (see Chapter 3 for a discussion of ImPACT). Among the 152 male and 28 female athletes who sustained a concussion, no significant differences with respect to mouthguard use were observed in neurocognitive deficits for verbal memory, visual memory, visual motor speed, reaction time, or symptom status upon follow-up assessment with ImPACT. Athletes had significantly lower neurocognitive test scores and higher symptom scores following a concussion regardless of mouthguard use (Mihalik et al., 2007).
In summary, over the past decade, although manufacturers have made
claims regarding the protective features of mouthguards to reduce or eliminate concussions, the vast majority of studies have consistently failed to link the use of mouthguards to lowered concussion risk (Barbic et al., 2005; Benson et al., 2009; Knapik et al., 2007; Labella et al., 2002; Mihalik et al., 2007; Navarro, 2011; Viano et al., 2012a; Wisniewski et al., 2004).
Ice Hockey Face Shields, Visors, and Cages
A face shield in ice hockey is a protective device made of impact-resistant plastic that is attached to a player’s helmet in order to lessen the risk of injury to the face. Full-face shields cover the entire face, and half-face shields (or visors) cover the upper half of the face. Cages, an alternative to the full face shield, cover the entire face and are usually made of metal. NFHS rules mandate full facial protection for high school ice hockey players, and USA Hockey requires facial protection in all age classifications below adult (NFHS, 2013; USA Hockey, 2013). NCAA rules require college-level ice hockey players to wear full facial protection that has met standards set by the Hockey Equipment Certification Council (NCAA, 2012).
Facial protection has been shown to reduce the incidence of ocular, facial, and dental injuries in ice hockey (Asplund et al., 2009; Hendrickson et al., 2008; LaPrade et al., 1995; Stuart et al., 2002). It has been hypothesized that facial protection may also reduce the incidence and severity of head injury in ice hockey by decreasing head acceleration after an impact (Lemair and Pearsall, 2007). One biomechanical study using a surrogate headform showed substantially reduced peak linear acceleration during blunt impacts when facial protection, in combination with a helmet, was in place, with cages showing lower peak acceleration than with visors (Lemair and Pearsall, 2007). However, there is no evidence from epidemiologic research that facial protection reduces concussions in ice hockey. An analysis of injury data from the National Hockey League (NHL) (n=787), which does not require players to wear facial protection, found that athletes wearing visors were no less likely to experience concussions than were those not wearing any facial protection (Stevens et al., 2006).3 In addition, studies of college and amateur ice hockey players show no significant difference in the occurrence of concussion between ice hockey players who wear half-face protection versus those who wear full-face protection (Apslund et al., 2009; Benson et al., 1999, 2002; Stuart et al., 2002). One study of university ice hockey players who were followed over one season showed that, although there was no significant difference in the overall risk of sustaining a con-
____________________________________
3Beginning in the 2013-2014 season, the NHL began to grandfather in the mandatory use of visors for new players. Facial protection continues to be optional for athletes who are not new to the league (NHL, 2013).
cussion for players wearing visors (n=323) compared with those wearing full-face protection (n=319), athletes sustaining concussions while wearing visors missed significantly more practices and games per concussion than those sustaining concussions while wearing full-face protection (4.07 sessions; 95% CI, 3.48 to 4.74 versus 1.71 sessions; 95% CI, 1.32 to 2.18) (Benson et al., 2002).
Marketing of Protective Equipment
There are concerns that the makers of sports protective equipment have taken advantage of growing concussion awareness by making unsubstantiated claims that certain products can reduce concussion risk. For example, as discussed at a 2011 hearing on concussions and the marketing of sports equipment before the U.S. Senate Committee on Commerce, Science, and Transportation, packaging and online advertising for particular devices (e.g., mouthguards and soccer headbands) designed specifically for youth athletes have included language that may be construed to mean that the product reduces concussion risk or else they have made explicit claims of reduced concussion risk with use of the product (U.S. Senate Committee on Commerce, Science, and Transportation, 2011). In order to avoid a false sense of security, it is important that athletes, parents, and coaches be aware of—and that marketers of sports equipment accurately convey—the limitations of protective equipment as it relates to concussions. Until a universally accepted injury risk curve for concussions is established, as well as associated variants with age and perhaps direction, claims of reduced concussion risk with protective devices will not be based on fundamentally sound science.
Risk Compensation
One unintended consequence of wearing helmets and other protective devices is that the athlete may be emboldened by the increased protection to take additional risks, thus mitigating any benefits of the protective device. This phenomenon, termed “risk compensation,” has been studied extensively in the safety literature; for an excellent review of the topic, the reader is directed to Hedlund (2000), who summarizes the theory and research in this field. The theory of risk compensation is based on the idea that every individual has an acceptable level of risk. If a protective device lowers that risk, the individual’s actions will change (i.e., become more risky) in such a way as to re-equilibrate the risk to the maximum acceptable level. Hedlund suggests that there are four factors that influence risk compensation: visibility (“Do I know there has been a safety change?”); effect (“How does the safety change affect me?”); motivation (“What influences
my safety behavior?”); and control (“How much control do I have of my behavior?”). Two examples of risk compensation in Hedlund’s review are drivers with antilock brakes driving faster and braking harder than those without antilock brakes and loggers working more quickly and more carelessly once protective equipment was required (Hedlund, 2000). It certainly appears that the four factors described above come into play in the area of sports and protective equipment: The use of protective equipment has high visibility; it may appear to adversely affect a person’s ability to play at a high level; a person may not be motivated to wear such devices if the person does not perceive a risk; and an individual may sometimes have no control over the use of the protective equipment (i.e., it is required). Hagel and Meeuwisse (2004) summarized the issues of risk compensation in sports and provided several examples: the increase in tackling drill fatalities in football in the 1950s and 1960s after the introduction of mandatory hard shell helmets, an increase in injury rates associated with the introduction of soft core baseballs, and increased helmet usage in fatally injured skiers versus the uninjured skiing population.
There has been limited exploration of the role that risk compensation may play in concussions. Tierney and colleagues (2008) studied both men and women soccer players in a controlled soccer heading scenario both with and without headgear and observed that women attacked the balls more forcefully while wearing headgear. This could be attributed to risk compensation or simply to the perception by the women players that they needed to strike the ball harder to reach the target. In a survey of attitudes and beliefs around protective equipment, two-thirds of adolescent rugby players reported increased confidence and an ability to play harder when wearing headgear (Finch et al., 2001). In a convenience sample of recreational ice hockey players using facial protection (n=152), 69 percent reported that they felt they could play more aggressively with the protection (Woods et al., 2007).
Risk compensation studies are difficult to conduct and analyze because the effects are typically evaluated over a population rather than via individual differences in behavior before and after institution of a safety change. As a result, they must control for other behavioral variations of the populations studied. Still, future work in protective devices in sport must evaluate these potential unintended consequences as policy and equipment changes intended to reduce risk are considered.
Playing Surfaces
Playgrounds are a major source of injury for children. From 2001 through 2008 there were an estimated 1,786,608 emergency department (ED)–treated injuries associated with playground equipment, of which
30,578 (2 percent) were concussions. (The actual number of playground-related injuries, including concussions, is likely much higher, given that many such injuries are not treated in an ED.) The greatest share of playground injuries of all types (44 percent) involved falls from, into, or onto equipment, followed by injuries involving equipment breakage, tip over, or poor design or assembly (23 percent) (CPSC, 2009). To reduce the likelihood of head injuries on playgrounds, it is important to consider the impact-attenuating properties of the surfacing under and around the playground equipment (CPSC, 2010). The Consumer Product Safety Commission (CPSC) and ASTM International have developed guidelines for playground surfacing. The most recent CPSC handbook for public playgrounds states that playground equipment should not be placed over asphalt, concrete, dirt, grass, or carpet not tested to ASTM F1292. ASTM standard F1292 provides a “critical height” rating for playground surfaces that approximates the fall height below which a life-threatening head injury would not be expected to occur. The rating assigned to a given surface should be greater than or equal to the fall height of the highest piece of equipment on the playground. Preferred surfacing includes unitary surfaces (rubber tiles, mats) tested to ASTM F1292; loose fill materials (pea gravel, sand, wood mulch not treated with chemical preservative, and wood chips) maintained at a minimum depth of 9 inches; or shredded or rubber mulch maintained at a minimum depth of 6 inches (CPSC, 2010).4 Recent nationwide data on the safety conditions of playgrounds are not available. A 2004 survey of 3,000 school, childcare, and park playgrounds in the United States resulted in overall grade of B– for fall surfacing and, within this category, a grade of F for appropriate depth of loose fill materials (National Program for Playground Safety, 2004). There currently are no national safety standards for outdoor play equipment. A few states mandate compliance with the CPSC guidelines.
One organized sport for which the impact-attenuating properties of the playing surface are particularly important is cheerleading. Concussions and other closed-head injuries account for 4 to 6 percent of all cheerleading injuries (Labella and Mjaanes, 2012). Although concussion rates in cheerleading (0.06 per 1,000 exposures) are low compared with other sports, from 1998 to 2008 concussion rates in cheerleading increased by 26 percent each year, which was a greater rate of increase than for any other sport played by female youth at the high school and college levels. This increase is thought to have been due to the increasing difficulty of stunts (Labella and Mjaanes,
____________________________________
4The recommendations for protective surfacing do not apply to equipment that requires a child to be standing or sitting at ground level, such as sandboxes, playhouses, activity walls at ground level, and any other equipment that children use when their feet remain in contact with the ground surface (CPSC, 2010).
2012; Shields and Smith, 2009a). Falls and stunts that involve interaction with the surface (e.g., tumbling) account for a sizable share of all injuries in cheerleading (Marar et al., 2012; Schulz et al., 2004; Shields and Smith, 2009a). The potential for concussions and other injuries can be minimized by increasing the shock-absorbing capacity of the surface on which cheerleaders practice and perform (Shields and Smith, 2009b).
Daneshvar and colleagues (2011) noted that the momentum transfer and impact associated with collisions increases as the speed of athletes increases. Because the surface on which an athlete plays affects his or her speed, it may also influence the incidence of concussions. Synthetic surfaces are generally harder and result in faster speeds than on natural ones. Artificial turfs (e.g., AstroTurf), which do not require sunlight and regular maintenance, were introduced in the 1960s following the construction of indoor football stadiums. These turfs were made of a hard plastic material and are believed to have led to an increase in injuries, particularly musculoskeletal injuries, among football players. Beginning in 2000 synthetic turfs designed to mimic the properties of natural grass while reducing friction and impact forces were developed and deployed (Williams, 2007). A few epidemiologic studies have evaluated whether athletes sustain more injuries when playing on the newer artificial turfs than when playing on natural grass. Findings have varied across studies and injury type (Dragoo et al., 2012; Fuller et al., 2007; Guskiewicz et al., 2000; Meyers, 2010; Meyers and Barnhill, 2004). An analysis of NCAA Injury Surveillance System data for soccer showed that the three most common injuries on artificial turf for men (ankle lateral ligament complex tear, hamstring tear, concussion) and for women (ankle lateral ligament complex tear, concussion, and anterior cruciate ligament tear) were the same as the most common injuries on grass, but the incidence of head and neck injuries, including concussions, was significantly (p < .01) higher on artificial turf than on grass for men (4.31/1,000 player hours [95% CI, 3.03-6.13] on artificial turf versus 2.37/1,000 player hours [95% CI, 1.86-3.02] on natural grass) (Fuller et al., 2007). Meanwhile, a study of college football players showed no significant variation in the incidence of head trauma by field type (Meyers, 2010), and another study found that football players experienced more concussions on natural grass than on artificial turf (Meyers and Barnhill, 2004). In summary, the evidence is inconclusive as to whether concussion risks are higher on synthetic than on natural turf.
The rules of play are the foundation of safe conduct in sports because they set expectations for behavior and define infractions. As noted in the 2013 American Medical Society for Sports Medicine position statement
on concussion in sports, promoting fair play encourages respect for opponents and emphasizes safety precautions for athletes (Harmon et al., 2013). Enforcement of the rules by coaches and officials and adherence to rules by players may help to reduce the incidence and severity of sports-related concussions in youth (Cusimano et al., 2013; Harmon et al., 2013; Lincoln et al., 2013; Roberts et al., 1996; Yard et al., 2008). In a 2008 study of athletes in 100 U.S. high schools, 25 percent of the concussions reported were related to illegal play activity as determined by a referee or disciplinary committee (Collins et al., 2008). In contact and collision sports in particular, a shift toward a greater emphasis on player safety will require education and a change in expectations on the part of coaches, officials, and athletes as well as of parents and fans (Harmon et al., 2013).
Some research has been conducted on the relationship between the rules for specific sports and concussion risk. Body checking in ice hockey is a tactic in which a defensive player uses his or her body to legally separate a puck carrier from the puck. Body checks must be done with the trunk of the body (hips and shoulders) and must be above the opponent’s knees and below the neck. Although legal body checking is a necessary skill at more advanced levels of play, safety can be jeopardized when players do not have the skills to check in the correct way (USA Hockey, 2009). Body checking is a leading cause of injury in general and of concussion in particular in youth ice hockey (Cusimano et al., 2011; Emery and Meeuwisse, 2006; Emery et al., 2010a; MacPherson et al., 2006; McIntosh and McCrory, 2005). Research from Canada that studied youth ages 10 to 15 in ice hockey leagues in which body checking was permitted and those where it was not found that body checking was associated with an increased risk of concussions (Emery et al., 2010b; MacPherson et al., 2006). In a study comparing rates of concussion in male ice hockey players before and after a Hockey Canada rule change that lowered the legal age of body checking from 11 to 9, the odds of an ED visit due to a body checking–related concussion increased significantly for “Atom” division players (i.e., those 10 and 11 years old). There were four reported concussions prior to rule change and 22 after the rule change (OR 10.08, 95% CI, 2.35-43.29) (Cusimano et al., 2011). These findings support policies that prohibit body checking for younger ice hockey players as a means of reducing the risk of concussions and other injuries. Recognizing that the youngest ice hockey players may not be prepared for body checking in competitive play, USA Hockey delayed the legal age for body checking from 12 to 14 starting with the 2011-2012 season. In older youth for whom body checking is permitted, USA Hockey requires officials to penalize players who engage in illegal body checking, such as checking another player from behind or for the purpose of intimidation (USA Hockey, 2011, 2013).
Using accelerometers to monitor linear and rotational head accelera-
tion, Guskiewicz and colleagues examined the biomechanics of legal and illegal plays in youth ice hockey players. Illegal collisions—those involving elbowing, intentional head contact, or high sticking to the head—made up 17 percent of all body collisions. Illegal collisions resulted in slightly higher linear and rotational acceleration (23 g; 1530 rad/s2) than did legal collisions (21 g; 1417 rad/s2). The researchers concluded that athletes and coaches should better conform to game rules and that officials should be more stringent in enforcing and assessing more severe penalties to players who purposefully foul an opponent (Guskiewicz, 2013; Mihalik et al., 2010). It is important to note, however, that these differences are relatively small and their effect on concussion risk is not clear.
Low rates of adherence to fair play policy have been linked to a greater risk of injury in youth soccer (Koutures and Gregory, 2010). Unintentional collisions such as the head-to-head and head-to-elbow contacts that are associated with more aggressive play are frequent mechanisms for concussion in this sport (Boden et al., 1998; Kolodziej et al., 2011).
The responsibilities of officials who preside over sporting events include enforcing game rules, assessing penalties, detecting infractions and signaling other participants and officials when infractions occur, and starting and stopping play when necessary (BLS, 2012). Aside from other players, officials often have the closest view of play and any injuries that occur. Officials therefore have a role to play in both the prevention of sports-related concussions and the identification of players who may have been concussed. At a committee workshop, Jeff Triplette of the National Association of Sports Officials reported that many officials of youth sports have not been educated on the signs and symptoms of concussions, and he noted further that many of them are former athletes from a time when the prevalent mindset was to play through injuries. He also described the sorts of incidents that can lead to a concussion and discussed how enforcement of rules can protect athletes. Triplette noted that greater awareness and reporting of possible concussions in youth sports could be facilitated by
- a requirement that officials and coaches receive concussion training before they can supervise athletic activities;
- education of first responders (i.e., medical personnel) to engage officials in the assessment of injured players;
- the use of video documentation to assess whether officials are enforcing safety rules; and
- the discipline of officials who fail to enforce rules that affect player safety (Triplette, 2013).
In response to concerns about the long-term consequences of repetitive head impacts, several organizations have called for a “hit count” in youth
sports—in other words, a limit on the amount of head contacts a particular player experiences over a given amount of time. This concept, most publicly advanced by the Sports Legacy Institute,5 is similar to the pitch counts that are used in youth baseball to reduce injury to the shoulder and elbow of pitchers. Reflecting concern about the hit count, the NFL and collegiate athletic organizations such as the Ivy League and PAC-12 conference have limited the number of full-contact practices in an effort to reduce the number of head impacts (Council of Ivy League Presidents, 2011, 2012). Similar actions were taken in 2012 by Pop Warner Football, the largest youth football program in the United States. At the high school level there has been no national limit on contact, but some states have taken action. Most notably, Texas passed limits on contact in football practice during the 2013 season (House Bill 887).
Support for such limits is not universal. Some believe that the technology to quantify the number and magnitude of head impacts is not adequately developed and that the science behind setting a specific threshold is not well defined (see discussions earlier in this chapter and in Chapter 2). Furthermore, there is some concern that delaying or reducing contact in practice puts athletes at risk down the road because they have not adequately learned appropriate contact skills at an early age when the ability to acquire skills is at its greatest (Guskiewicz, 2013). These researchers advocate for proper coaching techniques that emphasize fundamentals and the development and enforcement of sport-specific rules to prevent unsafe behavior and to reduce but not eliminate contact.
While the concept of limiting the number of head impacts is fundamentally sound, there is no evidence available at this time to provide a scientific basis for implementing a specific limit on the number of impacts or the magnitude of impacts per week or per season.
Knowledge of concussion signs and symptoms has been found to be deficient in some surveys of youth athletes (Bloodgood et al., 2013; Kaut et al., 2003; Kroshus et al., 2013). Studies of the effectiveness of educational interventions, including workshops and lectures, videos, and other programs, show with some consistency that education can improve concussion knowledge in youth (Bagley et al., 2012; Bramley et al., 2012; Cook et al., 2003; Cusimano et al., 2014; Echlin et al., 2010; Miyashita et al., 2013). In one of the larger studies, students ages 9 to 18 (n=599)—who participated in an education workshop lasting 40 to 60 minutes and featuring interactive demonstrations, discussion, and case studies of
____________________________________
5See http://www.sportslegacy.org/policy/hit-count (accessed January 15, 2014).
athletes—displayed significant improvement in concussion knowledge; specifically, the pre- and post-intervention mean scores on a quiz assessing the recognition of signs and symptoms and appropriate responses after a concussion were 43 and 65 percent, respectively. Furthermore, the proportion of students who passed the quiz (i.e., who answered half of the quiz questions correctly) increased from 34 percent to 80 percent (Bagley et al., 2012). Miyashita and colleagues (2013) found that concussion knowledge scores among 70 male and female college soccer and basketball players improved significantly after the athletes participated in an educational lecture describing concussion basics and a question and answer session. A randomized study involving 67 junior ice hockey players ages 16 to 21 showed that participants who viewed a concussion DVD or interactive computer module had greater increases in concussion knowledge than did controls based on the results of pre- and post-intervention knowledge tests (Echlin et al., 2010). Another randomized study of 267 minor league ice hockey players found that players who viewed an ice hockey safety video on concussion had significant increases in concussion knowledge immediately following the video. However, a reassessment 2 months later revealed that in athletes who had viewed the video concussion knowledge had decreased, suggesting that the effect of the intervention was temporary (Cusimano et al., 2014).
Knowledge, although essential to behavior change, does not necessarily translate into changes in behavior. Various factors—including social, attitudinal, and emotional forces—influence whether and how individuals respond to information. Yet little research has evaluated the effect of concussion education on behavior change in youth. One study found a significant reduction in body checking–related penalties (which in other studies have been linked to concussion risk) as well as improvements in concussion knowledge in 75 youth ice hockey players ages 11 to 12 who viewed a video on the mechanisms, consequences, and prevention of brain and spinal cord injury versus a group of controls (Cook et al., 2003). Another study found no effect of an ice hockey safety video on behavior change among minor league ice hockey players (Cusimano et al., 2014). Although not focused specifically on concussions, an evaluation of the “Bike Smart” program—an eHealth software program using video, animations, and still images to teach bicycle safety behaviors to children—found that elementary-school-age children who participated in the program had significant gains in their recognition of safety rules, helmet placement, and hazard discrimination as compared with children who watched a video about childhood safety. One particularly important result was that children viewing the Bike Smart program more often donned a bike helmet correctly (McLaughlin and
Glang, 2010).6 In a prospective study of 146 NCAA Division 1 ice hockey players from six universities who had received NCAA compliant concussion education, Kroshus and colleagues observed only a small decrease in athletes’ reported intention to continue to play while experiencing concussion symptoms. Because the NCAA mandate states only that institutions provide concussion education, the content and form of delivery (e.g., handout, email, lecture, video) of the education varied across schools. Change in intention to continue to play with a concussion was significantly higher among athletes who reported receiving a lecture (p=0.021) and significantly lower among those who reported receiving concussion information via email (Kroshus et al., 2013).
As discussed earlier in the report, the current culture of sports may discourage athletes from reporting their concussion symptoms and removing themselves from play (Kroshus et al., 2013; Torres et al., 2013). A recent study of high school athletes’ (n=167, age=15.7 ± 1.4) intentions to report sports-related concussions showed that intention to report was associated with perceptions about concussion reporting, perception of important social referents’ beliefs about concussion reporting, and perceived control over concussion reporting. Although reporting intention may not always be an indicator of what an individual’s actual concussion reporting behaviors will be, these findings suggest that future concussion education initiatives should focus on improving attitudes and beliefs about concussions among athletes, coaches, and parents (Register-Mihalik et al., 2013b). Greater athlete knowledge about concussions and more favorable attitude toward reporting possible concussion also was associated with increased reporting prevalence of concussion and “bell-ringer” events in these youth (Register-Mihalik et al., 2013a).
A recent online survey of youth athletes (n=252) showed that younger youth (ages 10 to 13) were significantly more likely to view concussions as a “critical issue” than were older youth (ages 16 to 18 years) (Bloodgood et al., 2013), perhaps indicating that existing concussion educational efforts are reaching younger youth more effectively than older youth.
Especially in youth sports, coaches often preside over athletic events without medical personnel present. It is therefore important that youth coaches have a basic knowledge of concussions. A small number of studies have evaluated the effectiveness of concussion education interventions
____________________________________
6Bicycle crashes are a leading cause of sports- and recreation-related mTBI in youth. Centers for Disease Control and Prevention data from emergency department visits (nonfatal sports- and recreation-related TBI) show that bicycle crashes are the most common cause of concussion among boys 5 to 9 years old and the second most common cause of concussion among boys 10 to 14 and 15 to 19. Bicycle crashes are also the second most common cause of concussion among girls 5 to 9 and the most common cause of concussion among girls 10 to 14 (Gilchrist et al., 2011).
for coaches. The Athletic Concussion Training using Interactive Video Education (ACTive) program was developed to train community coaches of youth ages 10 to 18 about youth sports concussions. Designed using the Health Belief Model (Becker, 1974; Rosenstock et al., 1988) as its conceptual framework, the program offers an interactive video consisting of three modules that cover the prevention, recognition, and management of youth sports concussions using simple graphics and video segments. In one study, 75 coaches (52 males and 23 females) completed the program over the Internet. Post-intervention analysis showed significant overall gains in concussion knowledge compared to baseline among coaches who received the intervention versus coaches in the control group who were sent a link to materials prepared by the Centers for Disease Control and Prevention (CDC) on bicycle and pedestrian safety. The greatest gains were obtained in knowledge about concussion symptoms, followed by general concussion knowledge, knowledge of misperceptions about concussion, perceived self-confidence about taking appropriate action based on scenarios presented, and intention to take action based on the scenarios (Glang et al., 2010). A cross-sectional investigation showed that prior coaching education was predictive of the ability of youth sport coaches (n=157) to recognize concussion signs and symptoms (Valovich-McLeod et al., 2007). In a study involving 20,000 coaches and 4,000 referees of community rugby in New Zealand, Gianotti and colleagues found that a concussion management education program consisting of a film and slide show provided “minimum best practice” for the management of suspected concussions (Gianotti and Hume, 2007). The committee did not identify any studies of the effect of concussion education on changes in coaching behavior, such as the removal of athletes who may have sustained a concussion from play.
Over the past several years, the CDC has developed concussion education materials for a variety of stakeholders. In collaboration with 26 health, sports, and national organizations, the CDC created the “Heads Up: Concussion in Youth Sports” initiative in 2007. The initiative is centered on a toolkit designed to provide coaches, school administrators, athletes, and parents with practical and easy-to-read information on concussions from a reliable source. The toolkit includes fact sheets tailored for coaches, parents, and athletes; a clipboard; a magnet; and a quiz to test concussion knowledge. An online concussion training module for coaches is also available via the campaign’s website7 (CDC, 2009, 2012a).
Despite relatively low response rates, survey assessments of the Heads Up campaign concerning changes in knowledge and attitudes about concussions among youth coaches indicated that after reviewing the Heads Up
____________________________________
7The toolkit materials are available in English and Spanish and may be downloaded from http://www.cdc.gov/concussion/HeadsUp/youth.html (accessed January 15, 2014).
materials the coaches viewed concussions more seriously and were better able to identify athletes who may have had a concussion. Many of the coaches surveyed said that they had learned something new about concussions from the materials and that they would continue to use the materials (Covassin et al., 2012; Sarmiento et al., 2010; Sawyer et al., 2010).
“Heads Up: Brain Injury in Your Practice” is a CDC initiative that provides materials on mTBI and concussion for physicians, including a booklet with information on concussion diagnosis and management, a patient assessment tool, a care plan, concussion prevention fact sheets, a palm card for on-field management, and a CD-ROM with downloadable kit materials and other resources (CDC, 2011).8 An analysis of the effect of the toolkit on concussion knowledge in a random sample of physicians showed no difference in general concussion knowledge between an intervention group who received the materials (183 physicians) and a control group that did not (231 physicians). However, physicians who received the toolkit were significantly less likely to recommend next-day return to play (OR .31, 95% CI, .12-.76) (Chrisman et al., 2011), suggesting that continuing medical education on concussion may improve the management of patients with concussions.
As discussed earlier in the report, youth often experience deficits in concentration and in short-term and working memory after a concussion. These deficits can interfere with school performance and may require school personnel to make academic accommodations. For example, a student who has difficulty concentrating after a concussion may need to be given more time to take tests or to complete assignments. Thus, school personnel need to receive education on the effects that a concussion may have on a student and on his or her school performance, the role of schools in concussion management, and the potential long-term consequences of returning to activity too soon (Sady et al., 2011). The CDC developed a toolkit, the “Heads Up to Schools: Know Your Concussion ABCs,” to aid in the dissemination of concussion information to school personnel who are not directly involved in athletics, such as principals, school counselors, teachers, and school nurses. The toolkit highlights concussion signs, effects, and what schools should watch for when a student returns to school after a concussion. The materials provide a starting point for concussion education for school personnel (CDC, 2012b; Sady et al., 2011). Thus far, there does not appear to have been a peer-reviewed evaluation of the effect of the Heads Up to Schools program on concussion knowledge or on concussion management by schools.
The literature on concussion education in medical schools is sparse. In a Canadian survey of medical schools, only 4 of the 14 schools that responded to the survey (out of a total of 17 medical schools) indicated that
____________________________________
8Materials are available for download at http://www.cdc.gov/concussion/headsup/physicians_tool_kit.html (accessed January 15, 2014).
concussion education is included in the curriculum for medical students (Burke et al., 2012). In a study in the United States, practicing pediatric primary care and emergency medicine physicians cited inadequate training on how to provide concussion education as an important barrier to educating families about concussion (Zonfrillo et al., 2012). Furthermore, these doctors demonstrated by their actions that they did not completely understand the cognitive limitations that follow a concussion. While they gave general return-to-activity instructions to more than half of their concussion patients (52 percent of first visits and 53 percent of follow-up visits), they provided instructions about returning to school to far fewer (28 percent first visits, 43 percent on follow-up) (Arbogast et al., 2013). Increasing concussion awareness in the medical community may be accomplished by targeting the medical school and residency curriculums as well as through continuing education through the various academies for board-certified physicians.
Content analyses of social media sites such as Facebook and Twitter show that people use these sites not only to share and discuss news stories about concussions but also to share personal experiences and to seek and offer advice. These content analysis studies highlight the capacity of social media to serve as a broadcast medium for sports concussion information and education (Ahmed et al., 2010; Sullivan et al., 2012).
Washington State House Bill 1824, also known as the Zackery Lystedt law, was signed into law in May 2009 and is widely recognized as the first statewide advocacy effort focused on concussion prevention to formally result in the passage of legislation. As discussed in Chapter 1, most states have since followed suit, which has resulted in a proliferation of laws addressing concussions in youth sports across the United States. In fact, since 2009 all 50 states and the District of Columbia have had bills introduced before their legislatures with language addressing youth concussions. Consideration of these bills has resulted in either codified statute or statewide administrative regulation in 49 states and the District of Columbia. The one exception is Mississippi; concussion legislation was last introduced in the Mississippi legislature in January 2013, but it did not pass through committee (USA Football, 2013).9 Although state concussion laws do not focus on the primary prevention of concussion, they do aim to increase awareness about concussion signs, symptoms, and outcomes and to reduce the risk and consequences of multiple concussions (e.g., second impact syndrome) and potentially to promote quicker recovery (Harvey, 2013).
____________________________________
9See http://legiscan.com/gaits/search?state=MS&keyword=concussion (accessed January 15, 2014).
Requirements of State Concussion Laws10
A committee review of state concussion laws, including review of the text from the laws as well as previously published analyses of these laws, shows that most states require (1) education or training of athletes, coaches, and parents about the nature and risk of concussions in sports, with parents signing a form acknowledging receipt of the information; (2) removal from play of any youth athlete suspected of having sustained a concussion; and (3) clearance for return to play by a licensed health care professional. However, state laws vary somewhat along several important dimensions that may influence the effect that they actually have on concussion prevention, diagnosis, and recovery, such as the extent of education and training required, the expertise of the health care providers who are permitted to clear athletes for return to play, and the entities that are covered by the law.
In most states, coaches are required to receive education on concussion recognition, sequelae, treatment, and return-to-play criteria. However, the extent of education that is required varies widely across states. Laws in some states require that coaches complete formal concussion training at specific time intervals, while laws in other states require that coaches be provided with concussion information materials. For example, as a condition of the issuance and renewal of a coaching permit, Connecticut’s law (Senate Bill 456) mandates that coaches of intramural and interscholastic athletics complete an initial training course on concussions and head injuries prior to coaching and every 5 years thereafter and that coaches review relevant information on concussions and head injuries each year that the course is not required. In contrast, legislation in Illinois (House Bill 200) states that educational materials describing the nature and risk of concussions and head injuries should be made available to school districts in order to educate coaches as well as parents and student athletes.
States also vary on their education and release requirements for parents and youth athletes. Although laws in the majority of states require that parents be provided with concussion education materials, several states do not require parents to read and sign an information sheet describing the nature and risks of concussion as a prerequisite to their children’s participation in sports. Many states’ laws do not require youth athletes themselves to read and sign a concussion information sheet (Tomei et al., 2012). CDC’s Heads Up initiative materials are explicitly mentioned in some state’s laws as the guideline for creating educational materials for parents and athletes.
Some states’ laws identify a specific entity, such as a state agency, to implement training and education provisions, while others are less specific.
____________________________________
10For detailed information on each state’s concussion legislation, please see NCSL, 2013, and Sun, 2013.
State and local boards of education are the governing bodies most commonly cited as responsible for implementation of concussion laws across the country. Interscholastic athletic associations, independently or in collaboration with a board of education, are the organizations next most likely to be identified in legislation as having an implementation role, especially in the education and training of coaches and adult volunteers. Health departments are generally given supportive responsibility, although in Massachusetts, Missouri, New York, and Pennsylvania, the legislative language gives health departments primary responsibility for the development of concussion training. The only example of an academic entity that has been given the lead responsibility for the development of concussion safety training programs is the Sport-Related Traumatic Brain Injury Research Center at the University of North Carolina at Chapel Hill, which leads a coalition that is developing such programs for the state of North Carolina.
Current guidelines for the management of sports-related concussions suggest that athletes who may have sustained a concussion be removed from practice or play (see Giza et al., 2013; Harmon et al., 2013; McCrory et al., 2013). Similarly, laws in the majority of states require that a youth athlete be removed from play when a concussion is suspected. In a handful of states, the laws are more specific, stating that athletes should be removed from play when signs, symptoms, or behaviors consistent with concussion are observed (Tomei et al., 2012). North Carolina’s law (House Bill 792), for example, states that “if a student participating in an interscholastic athletic activity exhibits signs or symptoms consistent with concussion,” he or she should be removed from the activity at that time. Some states’ laws name coaches, officials, or athletic trainers as the parties responsible for removal of an athlete from play, while most say nothing about who has this authority. Texas law specifies that parents and guardians are among the individuals who may call for the removal of a youth athlete from play (House Bill 2038). The removal-from-play requirements of concussion laws highlight the importance of education on signs, symptoms, behaviors, and other indicators (e.g., a hard impact to the head or body) of concussion for coaches, athletes, parents, and others who participate in or attend youth sporting events.
Another way in which states vary considerably is the types of health care providers who can provide clearance for return to play. Laws in several states specify that a licensed health care provider trained in concussion diagnosis and management may provide clearance for athletes to return to play. Other states allow any licensed health care provider to make such decisions, and still others say nothing about who is allowed to evaluate concussions. In states that are more specific about the types of health care providers who may make return-to-play decisions, all allow physicians to evaluate concussions, and many allow physician assistants and nurse prac-
titioners to do so. Some states allow athletic trainers, psychologists with training in neuropsychology, or physical therapists to provide clearance for return to play. Figure 6-2 shows the types of providers who were permitted to clear youth athletes for return to play according to a review of state laws as of December 2012 (Tomei et al., 2012). As these laws are continually being updated, there may have been some shift in states’ provisions regarding the types of providers who may make return-to-play decisions since the review was published.
Although a provider would need experience managing concussions in order to provide clearance for return to play, there is no consensus regarding why a particular health professional should perform this function or whether one type of professional should be preferred over another (Harvey, 2013). A qualitative assessment of concussion laws in Washington state and Massachusetts (discussed in the following section) noted that parents and athletes in rural and low-income communities face greater barriers than do those in other communities to accessing experts in concussion assessment and management services who can provide medical clearance (CDC, 2013). This finding suggests that there is a need for broader concussion education so that more providers can deliver these services and
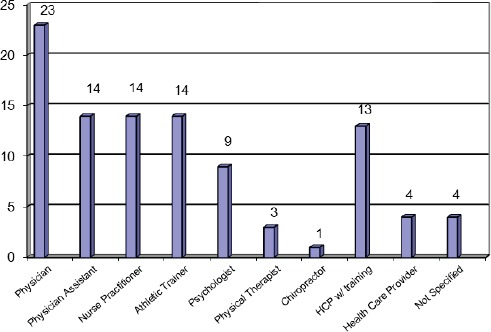
FIGURE 6-2 Bar graph showing the types of health care providers permitted to make return-to-play decisions, according to state laws as of December 2012.
NOTE: HCP = health care provider.
SOURCE: Adapted from Tomei et al., 2012.
also a need for the creation of mechanisms that local providers can use to remotely coordinate with providers with concussion expertise.
States also differ somewhat in the entities that are covered by concussion laws. In the District of Columbia, the law applies to all public, charter, parochial, and private schools, as well as athletic programs sponsored by the Department of Parks and Recreation and nonprofit and for-profit organizations (Athletic Concussions Protection Act of 2011). However, state concussion laws often cover only school athletic teams and include no specific requirements or guidelines for recreational leagues (CDC, 2013). College athletes are not affected by state concussion legislation, which leaves organizations such as the NCAA to implement concussion management policies at this level.
As discussed in Chapter 3, baseline neurocognitive testing may be a useful tool in the evaluation of concussion. Currently, a small number of states (e.g., Pennsylvania and Rhode Island) recommend baseline testing. Other states, such as Massachusetts, have recently introduced legislation to mandate baseline neurocognitive testing for youth athletes.
Implementation and Efficacy of State Concussion Laws
Of the 47 fully enacted and adopted state laws, 39 of them (83 percent) were passed between 2011 and 2013 and are in the early stages of implementation; many of them have already been or are in the process of being amended and revised. No comprehensive evaluation of the implementation and efficacy of these laws or their specific provisions has yet been published. While undertaking such an analysis will be necessary, it will be challenging in the absence of pre-legislation baseline data, especially for those provisions directed at assessing public awareness and professional education.
Investigators at the University of Washington administered a survey to youth soccer parents, coaches, and adult volunteers 1 year after the passage of the Lystedt Law (House Bill 1824) to assess knowledge about concussion and the return-to-play guidelines contained in the legislation (Shenouda et al., 2012). The law specifically requires that athletes, coaches, and parents be educated about concussions and annually sign an information sheet before the start of practice or competition. In Washington State, local boards of education in collaboration with the interscholastic activities association are responsible for developing the educational materials and for the administration of the signed information forms. The law also explicitly states that all youth athletes suspected of sustaining a concussion must be immediately removed from play and receive written medical clearance from a licensed health care provider before returning to play. The survey by Shenouda and colleagues was electronically distributed over 2 consecutive months at the beginning of the 2010 soccer season to a convenience sample
of adults receiving the electronic newsletter of the Washington Youth Soccer association. Of the 391 survey respondents, 63 percent were parents, 20 percent were coaches, and 17 percent were non-coach volunteers. Almost all respondents (>90 percent) had good general knowledge about concussions (e.g., knew that a concussion is a type of traumatic brain injury, that concussions may occur without loss of consciousness, and that identifying and treating a first concussion may prevent further injury). Ninety percent appropriately said that they would elect to delay return to play in the face of a neurologic symptoms scenario. Eighty-five percent were aware that the Lystedt Law requires that a youth athlete be evaluated by a trained professional before he or she can return to play. However, only 73 percent were aware that the return-to-play provisions of the law require written clearance from a licensed health care provider, and 80 percent were unaware that the health care provider could be a volunteer (Shenouda et al., 2012).
Oklahoma’s concussion law (Senate Bill 1700), which was passed in May 2010, requires school districts to work with the Oklahoma Secondary School Activities Association (OSSAA) to develop concussion guidelines and educational materials for coaches, youth athletes, and parents. To reinforce the law, OSSAA worked with the Oklahoma State Department of Health Injury Prevention Service to disseminate CDC Heads Up campaign materials to YMCAs and schools. Thirty-four YMCAs, 958 schools, and 205 martial arts schools received the information. An evaluation of this effort showed that of 163 schools that received the materials and responded to a survey, all reported that they were aware of the law, and 79 percent reported that their schools had strengthened their return-to-play policies in response to the law. All but one school responded that its coaches had been notified about the law and return-to-play guidelines (Langthorn and Wendling, 2012).
An online survey of high school varsity football coaches in Connecticut evaluated the effectiveness of mandatory concussion education for coaches required under the state’s concussion law. The survey included three knowledge questions that were part of the coaching education. Seventy-six of 143 coaches responded to the survey, and most (>70 percent) responded correctly to concussion knowledge questions relating to concussion risk factors and signs and symptoms, and most (>85 percent) also responded correctly to questions about when to remove an athlete from play. Sixty-six percent of the coaches responded that the mandatory concussion education required in the law was “definitely” or “probably” useful, but only half responded that they felt the mandatory concussion education increased their knowledge of concussions. Although the survey had no information about what concussion knowledge these coaches possessed prior to receiving the mandatory coaching education, the authors noted that after the coaches had received the education, the accuracy of their responses to some ques-
tions was lower than in a previous survey of high school football coaches in New England (Guilmette et al., 2007). The low overall response rate (53 percent) for this study was a major limitation, as coaches who responded may have viewed the concussion education more positively or gained more from the education (Trojian and Hoey, 2012).
Because state concussion laws do not always provide guidance on how they should be carried out, implementers are sometimes required to make decisions after the law has passed that can influence the success of the implementation (CDC, 2013). CDC’s National Center for Injury Prevention and Control conducted a case study evaluation of the implementation of legislation in Washington state and Massachusetts, two of the first states to adopt concussion legislation. Using information from interviews with stakeholders at the state level (health departments and statewide Interscholastic Athletic Associations) and at the school level (athletic directors and coaches), the evaluation assessed implementation efforts and related challenges and successes in order to inform implementation in other states (CDC, 2013). The evaluation identified the following factors as important for successful implementation of state concussion laws:
- the involvement of a wide range of stakeholders in the implementation planning process in order to identify various barriers and facilitators to implementation and to improve outreach and education;
- the development of a comprehensive and specific implementation plan early on to support the consistent and complete implementation of the law by the various stakeholders;
- the consideration of a broad approach to injury prevention, such as combining the return-to-play protocols for concussion with those for other sports-related injuries;
- communication with and provision of resources to recreational leagues to whom the state law does not apply by, for example, providing public access to resources developed for entities that are covered under the law;
- continuing education for individuals involved in the diagnosis and management of sports-related concussions to ensure that they stay up to date on the latest science; and
- consideration of the importance of educating teachers about concussions and “return to academics” in order to increase their understanding of the symptoms and management of concussions.
The case study also highlighted the importance of planning ahead to assess the effects of a law. In addition to determining what types of evaluation should be conducted (e.g., evaluations of the implementation or the impact
of the law), it is important to take into account staff time and capacity to conduct the evaluations and also to consider potential sources of additional funding for the evaluations. The data elements needed to respond to the questions of interest also should be considered. Data may be available through existing administrative databases or collected via instruments developed specifically for the evaluation (CDC, 2013).
Although no definitive conclusions can be drawn from the experiences of these states, with similar legislation being broadly implemented across the country there is ample opportunity for impact analysis and evaluation. Ultimately, as educators, advocates, providers, parents, and researchers all learn from one another about what works best in terms of legislation, a set of model provisions may be identified that can then be applied with uniformity, minimizing state-to-state variability and objectively informing policy makers as they move forward in dealing with youth concussions.
It is important to note that state concussion legislation is only one of several policy layers that shape concussion education and management. Sports clubs, school districts, and even individual schools may have their own policies. Health care provider protocols and standing orders also may influence how concussions are managed. Exactly how these various levels of policy will interact remains a question.
The committee offers the following findings concerning protection and prevention strategies aimed at youth concussions:
- There is little evidence that current helmet designs reduce the risk of sports-related concussions in young athletes. However, there is evidence that helmets reduce the risk of other injuries, such as skull fractures, and thus the use of properly fitted helmets should be promoted.
- There is currently no evidence that mouthguards or facial protection, such as face masks worn in ice hockey, reduce concussion risk. These devices are known to reduce the risk of other sports-related injuries—such as those to the eyes, face, mouth, and teeth—and their use is important for this reason.
- The marketing of some protective devices designed for youth athletes, such as mouthguards and soccer head gear, has included statements that these devices reduce concussion risk without sufficient scientific foundation to support such claims.
- Reductions in a specific biomechanical parameter, such as head acceleration, by a particular protective device do not correspond to
-
an equivalent reduction in concussion risk because of the nonlinear relationship between the mechanical input and injury risk.
- Current testing standards and rating systems for protective devices do not incorporate measures of rotational head acceleration or velocity and therefore do not comprehensively evaluate a particular device’s ability to mitigate concussion risk.
- While the concept of limiting the number of head impacts is fundamentally sound, implementing a specific threshold for the number of impacts or for the magnitude of impacts per week or per season is without scientific basis based on the evidence available at this time.
- While additional research across a variety of sports is needed, some studies involving youth ice hockey and soccer players have shown that the enforcement of rules and fair play policies contributes to reductions in the incidence of sports-related injuries, including concussions.
- Research indicates that concussion education programs are effective in improving concussion knowledge, although there is a lack of research concerning the effect of these interventions on behavior. Preliminary evidence suggests a need for additional research to evaluate the effectiveness of educational programs that emphasize improving attitudes and beliefs about concussions among athletes, coaches, and parents in order to improve concussion reporting among youth athletes.
- Most state concussion laws include requirements for concussion education, criteria for removal from play, and standards for health care providers who make return-to-play decisions. There is variation across states in the specific educational requirements for coaches, student athletes, and parents; the qualifications of providers who are permitted to make return-to-play decisions; and the populations to which the legislation applies. Given that most states are in the early stages of implementing these laws, there is so far very little evidence of their efficacy.
AAAM (Association for the Advancement of Automotive Medicine). 1998. The Abbreviated Injury Scale, 1998 revision (AIS-98) Des Plaines, Illinois.
ADA (American Dental Association). 2004. The importance of using mouthguards: Tips for keeping your smile safe. Journal of the American Dental Association 135(7):1061.
Ahmed, O. H., S. J. Sullivan, A. G. Schneiders, and P. McCrory. 2010. iSupport: Do social networking sites have a role to play in concussion awareness? Disability and Rehabilitation 32(22):1877-1883.
Allison, M. A., Y. S. Kang, M. R. Maltese, J. H. Bolte, and K. B. Arbogast. 2013. Validation of a helmet-based system to measure head impact biomechanics in ice hockey. Medicine and Science in Sports and Exercise 46(1):115-123.
Arbogast, K. B., A. D. McGinley, C. L. Master, M. F. Grady, R. L. Robinson, and M. R. Zonfrillo. 2013. Cognitive rest and school-based recommendations following pediatric concussion: The need for primary care support tools. Clinical Pediatrics 52(5):397-402.
Asplund, C., S. Bettcher, and J. Borcher. 2009. Facial protection and head injuries in ice hockey: A systematic review. British Journal of Sports Medicine 43(13):993-999.
Bagley, A. F., D. H. Daneshvar, B. D. Shanker, D. Zurakowski, C. A. d’Hemecourt, C. J. Nowinski, R. C. Cantu, and K. Goulet. 2012. Effectiveness of the SLICE Program for youth concussion education. Clinical Journal of Sport Medicine 22(5):385-389.
Barbic, D., J. Pater, and R. J. Brison. 2005. Comparison of mouth guard designs and concussion prevention in contact sports. Clinical Journal of Sport Medicine 15(5):294-298.
Becker, M. H. 1974. The Health Belief Model and personal health behavior. Health Education Monographs 2:324-473.
Beckwith, J. G., R. M. Greenwald, and J. J. Chu. 2012. Measuring head kinematics in football: Correlation between the head impact telemetry system and Hybrid III headform. Annals of Biomedical Engineering 40(1):237-248.
Bemelmanns, P., and P. Pfeiffer. 2001. Shock absorption capabilities of mouthguards in different types and thicknesses. International Journal of Sports Medicine 22(2):149-153.
Benson, B. W., N. G. H. Mohtadi, M. S. Rose, and W. H. Meeuwisse. 1999. Head and neck injuries among ice hockey players wearing full face shields vs. half face shields. JAMA 292(24):2328-2332.
Benson, B. W., M. S. Rose, and W. H. Meeuwisse. 2002. The impact of face shield use on concussions in ice hockey: A multivariate analysis. British Journal of Sports Medicine 36(1):27-32.
Benson, B. W., G. M. Hamilton, W. H. Meeuwisse, P. McCrory, and J. Dvoøák. 2009. Is protective equipment useful in preventing concussion? A systematic review of the literature. British Journal of Sports Medicine 43(Suppl 1):i56-i57.
Benson, B. W., A. S McIntosh, D. Maddocks, S. A. Herring, M. Raftery, and J. Dvoøák. 2013. What are the most effective risk-reduction strategies in sport concussion? British Journal of Sports Medicine 47(5):321-326.
Bloodgood, B., D. Inokuchi, W. Shawver, K. Olson, R. Hoffman, E. Cohen, K. Sarmiento, and K. Muthuswamy. 2013. Exploration of awareness, knowledge, and perceptions of traumatic brain injury among American youth athletes and their parents. Journal of Adolescent Health 53(1):34–39.
BLS (Bureau of Labor Statistics). 2012. What umpires, referees, and other sports officials do. http://www.bls.gov/ooh/entertainment-and-sports/umpires-referees-and-other-sportsofficials.htm#tab-2 (accessed August 5, 2013).
Boden, B. P., D. T. Kirkendall, and W. E. Garrett. 1998. Concussion incidence in elite college soccer players. American Journal of Sports Medicine 26(2):238-241.
Bramley, H., K. Patrick, E. Lehman, and M. Silvis. 2012. High school soccer players with concussion education are more likely to notify their coach of a suspected concussion. Clinical Pediatrics (Phila) 51(4):332-336.
Burke, M. J., J. Chundamala, and C. H. Tator. 2012. Deficiencies in concussion education for Canadian medical students. Canadian Journal of Neurological Sciences 39(6):763-766.
Camarillo, D. B., P. B. Shull, J. Mattson, R. Shultz, and D. Garza. An instrumented mouthguard for measuring linear and angular head impact kinematics in American football. Annals of Biomedical Engineering 41(9):1939-1949.
Cater, H. L., L. E. Sundstrom, and B. Morrison. 2006. Temporal development of hippocampal cell death is dependent on tissue strain but not strain rate. Journal of Biomechanics 39(15):2810-2818.
CDC (Centers for Disease Control and Prevention). 2009. Heads Up: Concussion in Youth Sports. Activity Report, 2007–2008. Atlanta, GA: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention. http://www.cdc.gov/concussion/pdf/Heads_Up_Activity_Report_Final-a.pdf (accessed August 5, 2013).
CDC. 2011. Heads Up: Brain injury in your practice. http://www.cdc.gov/concussion/headsup/physicians_tool_kit.html (accessed August 5, 2013).
CDC. 2012a. Heads Up: Concussion in youth sports. http://www.cdc.gov/concussion/HeadsUp/youth.html (accessed August 5, 2013).
CDC. 2012b. Heads Up to schools: Know your concussion ABCs. http://www.cdc.gov/concussion/headsup/schools.html#3 (accessed August 5, 2013).
CDC. 2013. Implementing return to play: Learning from the experiences of early implementers. http://www.cdc.gov/concussion/policies/rtp_implementation.html (accessed August 5, 2013).
Chrisman, S. P., M. A. Schiff, and F. P. Rivara. 2011. Physician concussion knowledge and the effect of mailing the CDC’s “Heads Up” toolkit. Clinical Pediatrics (Phila) 50(11):1031-1039.
Collins, C. L., S. K. Fields, and R. D. Comstock. 2008. When the rules of the game are broken: What proportion of high school sports-related injuries are related to illegal activity? Injury Prevention 14(1)34-38.
Collins, M., M. R. Lovell, G. L. Iverson, T. Ide, and J. Maroon. 2006. Examining concussion rates and return to play in high school football players wearing newer helmet technology: A three-year prospective cohort study. Neurosurgery 58(3):275-286.
Cook, D. J., M. D. Cusimano, C. H. Tator, and M. L. Chipman. 2003. Evaluation of the ThinkFirst Canada, Smart Hockey, brain and spinal injury prevention video. Injury Prevention 9(4):361-366.
Council of Ivy League Presidents. 2011. Ivy League presidents approve concussion-curbing measures for football. http://www.ivyleaguesports.com/sports/fball/2011-12/releases/Ivy_League_Presidents_Approve_Concussion-Curbing_Measures_for_Football (accessed August 5, 2013).
Council of Ivy League Presidents. 2012. Ivy League presidents approve concussion recommendations for lacrosse and soccer. http://www.ivyleaguesports.com/information/gen-releases/2012-13/releases/Ivy_League_Presidents_Approve_Concussion_Recommendations_for_Lacrosse_and_Soccer (accessed August 5, 2013).
Covassin, T., R. J. Elbin, and K. Sarmiento. 2012. Educating coaches about concussion in sports: Evaluation of the CDC’s “Heads Up: Concussion in Youth Sports” initiative. Journal of School Health 82(5):233-238.
CPSC (Consumer Product Safety Commission). 2009. Injuries and investigated deaths associated with playground equipment, 2001–2008. http://www.cpsc.gov//PageFiles/108596/playground.pdf (accessed August 5, 2013).
CPSC. 2010. Public Playground Safety Handbook. Bethesda, MD: U.S. Consumer Product Safety Commission. http://www.cpsc.gov//PageFiles/122149/325.pdf (accessed August 5, 2013).
Cusimano, M. D., N. A. Taback, S. R. McFaull, R. Hodgins, T. M. Bekele, and N. Elfeki. 2011. Effect of bodychecking on rate of injuries among minor hockey players. Open Medicine 5(1):E57-E64.
Cusimano, M. D., S. Nastis, and L. Zuccaro. 2013. Effectiveness of interventions to reduce aggression and injuries among ice hockey players: A systematic review. Canadian Medical Association Journal 185(1):E57-E69.
Cusimano, M. D., M. Chipman, P. Donnelly, and M. G. Hutchison. 2014. Effectiveness of an educational video on concussion knowledge in minor league hockey players: A cluster randomized controlled trial. British Journal of Sports Medicine 48(2):141-146.
Daneshvar, D. H., C. M. Baugh, C. J. Nowinski, A. C. McKee, R. A. Stern, and R. C. Cantu. 2011. Helmets and mouth guards: The role of personal equipment in preventing sport-related concussions. Clinics in Sports Medicine 30(1):145-163.
Delaney, J. S., A. Al-Kashmiri, R. Drummond, and J. A. Correa. 2008. The effect of protective headgear on head injuries and concussions in adolescent football (soccer) players. British Journal of Sports Medicine 42(2):110-115.
Dragoo, J. L., H. J. Braun, J. L. Durham, M. R. Chen, and A. H. Harris. 2012. Incidence and risk factors for injuries to the anterior cruciate ligament in National Collegiate Athletic Association football: Data from the 2004–2005 through 2008–2009 National Collegiate Athletic Association Injury Surveillance System. American Journal of Sports Medicine 40(5):990-995.
Duma, S. M., S. Rowson, B. Cobb, A. MacAllister, T. Young, and R. Daniel. 2013. Effectiveness of Helmets in the Reduction of Sports-Related Concussions in Youth. Commissioned Paper. Committee on Sports-Related Concussions in Youth.
Echlin, P. S., A. M. Johnson, S. Riverin, C. H. Tator, R. C. Cantu, M. D. Cusimano, J. E. Taunton, R. E. G. Upshur, C. R. Hall, L. A. Forwell, and E. N. Skopelja. 2010. A prospective study of concussion education in 2 junior ice hockey teams: Implications for sports concussion education. Neurosurgery Focus 29(5):E6.
Elkin, B. S., and B. Morrison. 2007. Region-specific tolerance criteria for the living brain. Stapp Car Crash Journal 51:127-138.
Emery, C. A., and W. H. Meeuwisse. 2006. Injury rates, risk factors, and mechanisms of injury in minor hockey. American Journal of Sports Medicine 34(12):1960-1969.
Emery, C. A., B. Hagel, M. Cecloe, and C. McKay. 2010a. Risk factors for injury and severe injury in youth ice hockey: A systematic review of the literature. Injury Prevention 16(2):113-118.
Emery, C. A., J. Kang, I. Shrier, C. Goulet, B. E. Hagel, B. W. Benson, A. Nettel-Aguirre, J. R. McAllister, G.M. Hamilton, and W. H. Meeuwisse. 2010b. Risk of injury associated with body checking among youth ice hockey players. JAMA 303(22):2265-2272.
Finch, C. F., A. S. McIntosh, and P. McCrory. 2001. What do under 15 year old schoolboy rugby union players think about protective headgear? British Journal of Sports Medicine 35(2):89-94.
Finch, C., R. Braham, A. McIntosh, P. McCrory, and R. Wolfe. 2005. Should football players wear custom fitted mouthguards? Results from a group randomized controlled trial. Injury Prevention 11(4):242-246.
Forero Rueda, M. A., L. Cui, and M. D. Gilchrist. 2011. Finite element modeling of equestrian helmet impacts exposes the need to address rotational kinematics in future helmet designs. Computer Methods in Biomechanics and Biomedical Engineering 14(12):1021-1031.
Fuller, C. W., R. W. Dick, J. Corlette, and R. Schmalz. 2007. Comparison of the incidence, nature and cause of injuries sustained on grass and new generation artificial turf by male and female football players. Part 1: Match injuries. British Journal of Sports Medicine 41(Suppl I):i20-i26.
Funk, J. R., S. Rowson, R. W. Daniel, and S. M. Duma. 2012. Validation of concussion risk curves for collegiate football players derived from HITS data. Annals of Biomedical Engineering 40(1):79-89.
Gadd, C. W. 1966. Use of a weighted-impulse criterion for estimating injury hazard. In Proceedings of the 10th Stapp Car Crash Conference. New York: Society of Automotive Engineers. Pp. 164-174.
Gennarelli, T., L. Thibault, G. Tomei, R. Wiser, D. Graham, and J. Adams. 1987. Directional dependence of axonal brain injury due to centroidal and non-centroidal acceleration. In Proceedings of the 31st Stapp Car Crash Conference. New York: Society of Automotive Engineers.
Gianotti, S., and P. A. Hume. 2007. Concussion sideline management intervention for rugby union leads to reduced concussion claims. NeuroRehabilitation 22(3):181-189.
Gilchrist, J., K. E. Thomas, L. Xu, L. C. McGuire, and V. Coronado. 2011. Nonfatal traumatic brain injuries related to sports and recreation activities among persons ≤19 years—United States, 2001–2009. Morbidity and Mortality Weekly Report 60(39):1337-1342.
Giza, C. C., J. S. Kutcher, S. Ashwal, J. Barth, T. S. D. Getchius, G. A. Gioia, G. S. Gronseth, K. Guskiewicz, S. Mandel, G. Manley, D. B. McKeag, D. J. Thurman, and R. Zafonte. 2013. Summary of evidence-based guideline update: Evaluation and management of concussion in sports. Neurology 80(24):2250-2257.
Glang, A., M. C. Koester, S. Beaver, J. Clay, and K. McLaughlin. 2010. Online training in sports concussion for youth sports coaches. International Journal of Sports Science and Coaching 5(1):1-12.
Guilmette, T. J., L. A. Malia, and M. D. McQuiggan. 2007. Concussion understanding and management among New England high school football coaches. Brain Injury 21(10):1039-1047.
Guskiewicz, K. 2013. The Role of Sports Rules and Training in the Prevention of Sports-Related Concussions in Youth. Presentation before the committee, Washington, DC, February 25.
Guskiewicz, K. M., N. L. Weaver, D. A. Padua, and W. E. Garrett. 2000. Epidemiology of concussion in collegiate and high school football players. American Journal of Sports Medicine 28(5):643-650.
Hagel, B., and W. Meeuwisse. 2004. Risk compensation: A “side effect” of sport injury prevention? Clinical Journal of Sport Medicine 14(4):193-196.
Hagel, B. E., I. B. Pless, C. Goulet, R.W. Platt, and Y. Robitaille. 2005. Effectiveness of helmets in skiers and snowboarders: Case-control and case crossover study. British Medical Journal 330(7486):281-283.
Halldin, P., A. Gilchrist, and N. J. Mills. 2001. A new oblique impact test for motorcycle helmets. International Journal of Crashworthiness 6(1):53-64.
Hansen, K., N. Dau, F. Feist, C. Deck, R. Willinger, S. M. Madey, and M. Bottlang. 2013. Angular Impact Mitigation system for bicycle helmets to reduce head acceleration and risk of traumatic brain injury. Accident Analysis and Prevention 59:109-117.
Hardy, W. N., C. D. Foster, M. J. Mason, K. H. Yang, A. I. King, and S. Tashman. 2001. Investigation of head injury mechanisms using neutral density technology and high-speed biplanar x-ray. Stapp Car Crash Journal 45:337-368.
Harmon, K. G., J. A. Drezner, M. Gammons, K. M. Guskiewicz, M. Halstead, S. A. Herring, J. S. Kutcher, A. Pana, M. Patukian, and W. O. Roberts. 2013. American Medical Society for Sports Medicine position statement: Concussion in sport. British Journal of Sports Medicine 47(1):15-26.
Harvey, H. H. 2013. Reducing traumatic brain injuries in youth sports: Youth sports traumatic injury state laws, January 2009-December 2012. American Journal of Public Health 103(7):1249-1254.
Havlik, H. S. 2010. Equestrian sport-related injuries: A review of current literature. Current Sports Medicine Reports 9(5):299-302.
Hedlund, J. 2000. Risky business: Safety regulations, risk compensation, and individual behavior. Injury Prevention 6(2):82-90.
Hendrickson, C. D., K. Hill, and J. E. Carpenter. 2008. Injuries to the head and face in women’s collegiate field hockey. Clinical Journal of Sport Medicine 18(5):399-402.
Hickey, J., A. Morris, L. Carlson, and T. E. Seward. 1967. The relation of mouth protectors to cranial pressure and deformation. Journal of the American Dental Association 74(4):735-740.
Hodgson, V., L. Thomas, and T. Khali. 1983. The role of impact location in reversible cerebral concussion. In Proceedings of the 27th Stapp Car Crash Conference. New York: Society of Automotive Engineers.
Hoffman, J., G. Alfter, and N. K. Rudolph. 1999. Experimental comparative study of various mouthguards. Endodontics and Dental Traumatology 15(4):157-163.
Hollis, S. J., M. R. Stevenson, A. S. McIntosh, E. A. Shores, M. W. Collins, and C. B. Taylor. 2009. Incidence, risk, and protective factors of mild traumatic brain injury in a cohort of Australian nonprofessional male rugby players. American Journal of Sports Medicine 37(12):2328-2333.
Hoshizake, T. B., and S. E. Brien. 2004. The science and design of head protection in sport. Neurosurgery 55(4):956-967.
Jadischke R., D. C. Viano, N. Dau, A. I. King, and J. McCarthy. 2013. On the accuracy of the Head Impact Telemetry (HIT) System used in football helmets. Journal of Biomechanics 46(13):2310-2315.
Karton, C., P. Rousseau, M. Vassilyadi, and T. B. Hoshizake. 2012. The evaluation of speed skating helmet performance through peak linear acceleration and rotational acceleration. British Journal of Sport Medicine. January 11 [Epub ahead of print.]
Kaut, K. P., R. DePompei, J. Kerr, and J. Congeni. 2003. Reports of head injury and symptom knowledge among college athletes: Implications for assessment and educational intervention. Clinical Journal of Sports Medicine 13(4):213-221.
Kemp, S. P. T., Z. Hudson, J. H. M. Brooks, and C. W. Fuller. 2008. The epidemiology of head injuries in English professional rugby union. Clinical Journal of Sport Medicine 18(3):227-234.
Kimpara, H., and M. Iwamoto. 2012. Mild traumatic brain injury predictors based on angular accelerations during impacts. Annals of Biomechanical Engineering 40(1):114-126.
King, A. I., K. H. Yang, L. Zhang, W. Hardy, and D. C. Viano. 2003. Is head injury caused by linear or angular acceleration? IRCOBI Conference–Lisbon (Portugal). http://snellhelmets.org/docs/articles/hic/King_IRCOBI_2003.pdf (accessed August 5, 2013).
Kleiven, S. 2003. Influence of impact direction on the human head in prediction of subdural hematoma. Journal of Neurotrauma 20(4):365-379.
Kleiven, S. 2007. Predictors of traumatic brain injuries evaluated through accident reconstructions. Stapp Car Crash Journal 51:81-114.
Knapik, J. J., S. W. Marshall, R. B. Lee, S. S. Drakjy, S. B. Jones, T. A. Mitchener, G. G. dela Cruz, and B. H. Jones. 2007. Mouthguards in sport activities. History, physical properties and injury prevention effectiveness. Sports Medicine 37(2)117-144.
Kolodziej, M. A., S. Koblitz, C. Nimsky, and D. Hellwig. 2011. Mechanisms and consequences of head injures in soccer: A study of 451 patients. Neurosurgery Focus 31(5):E1.
Koutures, C. G., and A. J. M. Gregory. 2010. Injuries in youth soccer. Pediatrics 125(2):410-414.
Kroshus, E., D. Daneshvar, C. M. Baugh, C. J. Nowinski, and R. C. Cantu. 2013. NCAA concussion education in ice hockey: An ineffective mandate. British Journal of Sports Medicine 48(2):135-140.
Labella, C. R., and Mjaanes, J. 2012. Cheerleading injuries: Epidemiology and recommendations for prevention. Pediatrics 130(5):966-971.
Labella, C. R., B. W. Smith, and A. Sigurdsson. 2002. Effects of mouthguards on dental injuries and concussions in college basketball. Medicine and Science in Sports and Exercise 34(1):41-44.
Langthorn, L., and T. Wendling. 2012. Young athletes protected by concussion law. Journal of Safety Research 43(4):311-312.
LaPlaca, M. C., D. Kacy Cullen, J. J. McLoughlin, and R. S. Cargill. 2005. High rate shear strain of three-dimensional neural cell cultures: A new in vitro traumatic brain injury model. Journal of Biomechanics 38(5):1093-1105.
LaPrade, R. F., Q. M. Burnett, R. Zarzour, and R. Moss. 1995. The effect of the mandatory use of face masks on facial lacerations and head and neck injuries in ice hockey. A prospective study. American Journal of Sports Medicine 23(6):773-775.
Lemair, M., and D. J. Pearsall. 2007. Evaluation of impact attenuation of facial protectors in ice hockey helmets. Sports Engineering 10(2):65-74.
Lincoln, A. E., S. V. Caswell, J. L. Almquist, R. E. Dunn, and R. Y. Hinton. 2013. Video incident analysis of concussions in boys’ high school lacrosse. American Journal of Sports Medicine 41(4):756-761.
MacPherson, A., L. Rothman, and A. Howard. 2006. Body-checking rules and childhood injuries in ice hockey. Pediatrics 117(2):e143-e147.
Marar, M., N. M. McIIvain, S. K. Fields, and R. D. Comstock. 2012. Epidemiology of concussions among United States high school athletes in 20 sports. American Journal of Sports Medicine 40(4):747-755.
Margulies, S., and B Coats. 2013. Experimental injury biomechanics of the pediatric head and brain. In Pediatric Injury Biomechanics, edited by J. R. Crandall, B. S. Myers, D. F. Meaney, and S. Zellers Schmidtke. New York: Springer. Pp. 157-189.
Margulies, S. S., L. E. Thibault, and T. A. Gennarelli. 1990. Physical model simulations of brain injury in the primate. Journal of Biomechanics 23(8):823-836.
Marshall, S. W., D. P. Loomis, A. E. Waller, D. J. Chalmers, Y. N. Bird, K. L. Quarrie, and M. Feehan. 2005. Evaluation of protective equipment for prevention of injuries in rugby union. International Journal of Epidemiology 34(1):113-118.
McCrory, P. 2001. Do mouthguards prevent concussion? British Journal of Sports Medicine 35(2):81-82.
McCrory, P., W. H. Meeuwisse, M. Aubry, B. Cantu, J. Dvoøák, R. J. Echemendia, L. Engebretsen, K. Johnston, J. S. Kutcher, M. Raftery, A. Sills, B.W. Benson, G. A. Davis, R. G. Ellenbogen, K. Guskiewicz, S. A. Herring, G. L. Iverson, B. D. Jordan, J. Kissick, M. McCrea, A. S. McIntosh, D. Maddocks, M. Makdissi, L. Purcell, M. Putukian, K. Schneider, C. H. Tator, and M. Turner. 2013. Consensus statement on concussion in sport: The 4th International Conference on Concussion in Sport held in Zurich, November 2012. British Journal of Sports Medicine 47(5):250-258.
McIntosh, A. S., and P. McCrory. 2001. Effectiveness of headgear in a pilot study of under 15 rugby union football. British Journal of Sports Medicine 35(3):167-169.
McIntosh, A. S., and P. McCrory. 2005. Preventing head and neck injury. British Journal of Sports Medicine 39(6):314-318.
McIntosh, A. S., P. McCrory, C. F. Finch, J. P. Best, D. J. Chalmers, and R. Wolfe. 2009. Does padded headgear prevent head injury in rugby union football? Medicine and Science in Sports and Exercise 41(2):306-313.
McIntosh, A. S., T. E. Andersen, R. Bahr, R. Greenwald, S. Kleiven, M. Turner, M. Varese, and P. McCrory. 2011. Sports helmets now and in the future. British Journal of Sports Medicine 45(16):1258-1265.
McLaughlin, K. A., and A. Glang. 2010. The effectiveness of a bicycle safety program for improving safety-related knowledge and behavior in young elementary students. Journal of Pediatric Psychology 35(4):343-353.
McNutt, T., S. W. Shannon, J. T. Wright, and R. A. Feinstein. 1989. Oral trauma in adolescent athletes: A study of mouth protectors. Pediatric Dentistry 11(3):209-213.
Meyers, M. C. 2010. Incidence, mechanisms, and severity of game-related college football injuries on FieldTurf versus natural grass: A 3-year prospective study. American Journal of Sports Medicine 38(4):687-697.
Meyers, M. C., and B. S. Barnhill. 2004. Incidence, causes, and severity of high school football injuries on FieldTurf versus natural grass: A 5-year prospective study. American Journal of Sports Medicine 32(7):1626-1638.
Mihalik, J. P., M. A. McCaffrey, E. M. Rivera, J. E. Pardini, K. M. Guskiewicz, M. W. Collins, and M. R. Lovell. 2007. Effectiveness of mouthguards in reducing neurocognitive deficits following sports-related cerebral concussion. Dental Traumatology 23(1):14-20.
Mihalik, J. P., R. M. Greenwald, J. T. Blackburn, R. C. Cantu, S. W. Marshall, and K. M. Guskiewicz. 2010. Effect of infraction type on head impact severity in youth ice hockey. Medicine and Science in Sports and Exercise 42(8):1431-1438.
Miyashita, T. L., W. M. Timpson, M. A. Frye, and G. W. Gloeckner. 2013. The impact of an educational intervention on college athletes’ knowledge of concussions. Clinical Journal of Sport Medicine 23(5):349-353.
Monson, K. L., W. Goldsmith, N. M. Barbaro, and G. T. Manley. 2003. Axial mechanical properties of fresh human cerebral blood vessels. Journal of Biomechanical Engineering 225(2):288-294.
Mueller, B. A., P. Cummings, F. P. Rivara, M. A. Brooks, and R. D. Terasaki. 2008. Injuries of the head, face, and neck in relation to ski helmet use. Epidemiology 19(2):270-276.
National Program for Playground Safety. 2004. State report cards. http://playgroundsafety.org/research/state-report-cards (accessed April 1, 2013).
Naunheim, R. S., A. Ryden, J. Standeven, G. Genin, L. Lewis, P. Thompson, and P. Bayly. 2003. Does soccer headgear attenuate the impact when heading a soccer ball? Academy of Emergency Medicine 10(1):85-90.
Navarro, R. R. 2011. Protective equipment and the prevention of concussion: What is the evidence? Current Sports Medicine Reports 10(1):27-31.
NCAA (National Collegiate Athletic Association). 2012. NCAA 2012-13 and 2013-14 Rules and Interpretations. http://www.ncaapublications.com/productdownloads/IH14.pdf (accessed October 9, 2013).
NCSL (National Conference of State Legislatures). 2013. Traumatic brain injury legislation. http://www.ncsl.org/issues-research/health/traumatic-brain-injury-legislation.aspx (accessed March 28, 2013).
Newman, J. A., M. C. Beusenberg, E. Fournier, N. Shewchenko, C. Withnall, A. I. King, K. Yang, L. Zhang, J. McElhaney, L. Thibault, and G. McGinnes. 1999. A new biomechanical assessment of mild traumatic brain injury: Part 1: Methodology. In International Research Council on Biomechanics of Injury. Pp. 17-36.
NFHS (National Federation of State High School Associations). 2011. Position statement and recommendations for mouthguard use in sports. http://www.nfhs.org/search.aspx?searchtext=mouthguard (accessed August 5, 2013).
NFHS. 2013. NFHS rules changes affecting risk, 1982–2013. www.nfhs.org/WorkArea/DownloadAsset.aspx?id=5760 (accessed September 6, 2013).
NHL (National Hockey League). 2013. NHL, NHLPA agree on mandatory visors. http://www.nhl.com/ice/news.htm?id=672983#&navid=nhl-search (accessed September 16, 2013).
Niedfeldt, M. W. 2011. Head injuries, heading, and the use of headgear in soccer. Current Sports Medicine Reports 10(6):324-329.
Ommaya, A. K., and T. A. Gennarelli. 1974. Cerebral concussion and traumatic unconsciousness. Correlation of experimental and clinical observations of blunt head injuries. Brain 97(4):633-654.
Ommaya, A. K., R. L. Grubb, and R. A. Naumann. 1971. Coup and contre-coup injury: Observations on the mechanics of visible brain injuries in the rhesus monkey. Journal of Neurosurgery 35(5):503-516.
Pellman, E. J., D. C. Viano, A. M. Tucker, I. R. Casson, and J. F. Waeckerle. 2003. Concussion in professional football: Reconstruction of game impacts and injuries. Neurosurgery 53(4):799-812.
Post, A., A. Oeur, B. Hoshisake, and M. D. Gilchrist. 2011. Examination of the relationship between peak linear and angular accelerations to brain deformation metrics in hockey helmet impacts. Computer Methods in Biomechanics and Biomedical Engineering 16(5):511-519.
Post, A., A. Oeur, B. Hoshisake, and M. D. Gilchrist. 2012. The influence of centric and non-centric impacts to American football helmets on the correlation between commonly used metrics in brain injury research. IRCOBI Conference Proceedings. http://ircobi.org/downloads/irc12/pdf_files/52.pdf (accessed August 5, 2013).
Raghupathi, R., and S. S. Margulies. 2002. Traumatic axonal injury after closed head injury in the neonatal pig. Journal of Neurotrauma 19(7):843-853.
Raghupathi, R., M. F. Mehr, M. A. Helfaer, and S. S. Margulies. 2004. Traumatic axonal injury is exacerbated following repetitive closed head injury in the neonatal pig. Journal of Neurotrauma 21(3):307-316.
Register-Mihalik, J. K., K. M. Guskiewicz, T. C. McLeod, L. A. Linnan, F. O. Mueller, and S. W. Marshall. 2013a. Knowledge, attitude, and concussion-reporting behaviors among high school athletes: A preliminary study. Journal of Athletic Training 48(5):645-653.
Register-Mihalik, J. K., L. A. Linnan, S. W. Marshall, T. C. McLeod, F. O. Meuller, and K. M. Guskiewicz. 2013b. Using theory to understand high school aged athletes’ intentions to report sport-related concussion: Implications for concussion education initiatives. Brain Injury 27(7-8):878-886.
Roberts, W. O., J. D. Brust, B. Leonard, and B. J. Hebert. 1996. Fair-play rules and injury reduction in ice hockey. Archives of Pediatric and Adolescent Medicine 150(2):140-145.
Rosenstock, I. M., V. J. Strecher, and M. H. Becker. 1988. Social Learning Theory and the Health Belief Model. Health Education Quarterly 15(2):175-183.
Rousseau, P., A. Post, and T. B. Hoshizaki. 2009. The effects of impact management materials in ice hockey helmets on head injury criteria. Journal of Sports Engineering and Technology 223(4):159-165.
Rowson, S., and S. Duma. 2011. Development of the STAR evaluation system for football helmets: Integrating player head impact exposure and risk of concussion. Annals of Biomedical Engineering 39(8):2130-2140.
Rowson, S., and S. Duma. 2013. Brain injury prediction: Assessing the combined probability of concussion using linear and rotational head acceleration. Annals of Biomechanical Engineering 41(5):873-882.
Rowson, S., G. Brolinson, M. Goforth, D. Dietter, and S. Duma. 2009. Linear and angular head acceleration measurements in collegiate football. Journal of Biomechanical Engineering 131(6):061016 doi:10.1115/1.3130454.
Rowson, S., S. M. Duma, J. G. Beckwith, J. J. Chu, R. M. Greenwald, J. J. Crisco, P. G. Brolinson, A. C. Duhaime, T. W. McAllister, and A. C. Maerlender. 2012. Rotational head kinematics in football impacts: An injury risk function for concussion. Annals of Biomedical Engineering 40(1):1-13.
Sady, M. D., C. G. Vaughan, and G. A. Gioia. 2011. School and the concussed youth: Recommendations for concussion education and management. Physical Medicine and Rehabilitation Clinics of North America 22(4):701-719.
Sarmiento, K., J. Mitchko, C. Klein, and S. Wong. 2010. Evaluation of the Centers for Disease Control and Prevention’s concussion initiative for high school coaches: “Heads Up: Concussion in High School Sports.” Journal of School Health 80(3):112-118.
Sawyer, R. J., M. Hamdallah, D. White, M. Pruzan, J. Mitchko, and M. Huitric. 2010. High school coaches’ assessments, intentions to sue, and use of a concussion prevention toolkit: Centers for Disease Control and Prevention’s Heads Up: Concussion in high school sports. Health Promotion Practice 11(1):34-43.
Schulz, M. R., S. W. Marshall, J. Yang, F. O. Mueller, N. L. Weaver, and J. M. Bowling. 2004. A prospective cohort study of injury incidence and risk factors in North Carolina high school competitive cheerleaders. American Journal of Sports Medicine 32(2):396-405.
Shenouda, C., P. Hendrickson, K. Davenport, J. Barber, and K. R. Bell. 2012. The effects of concussion legislation one year later—What have we learned: A descriptive pilot survey of youth soccer player associates. Physical Medicine and Rehabilitation 4(6):427-435.
Shields, B. J., and G. A. Smith. 2009a. Cheerleading-related injuries in the United States: A prospective surveillance study. Journal of Athletic Training 44(6):567-577.
Shields, B. J., and G. A. Smith. 2009b. The potential for brain injury on selected surfaces used by cheerleaders. Journal of Athletic Training 46(6):595-602.
Singh, G. D., G. J. Maher, and R. R. Padilla. 2009. Customized mandibular orthotics in the prevention of concussion/mild traumatic brain injury in football players: A preliminary study. Dental Traumatology 25(5):515-521.
Spiotta, A. M., A. J. Bartsch, and E. C. Benzel. 2012. Heading in soccer: Dangerous play? Neurosurgery 70(1):1-11.
Stevens, S. T., M. Lassonde, L. deBeaumont, and J. P. Keenan. 2006. The effect of visors on head and facial injury in National Hockey League players. Journal of Science and Medicine in Sport 9(3):238-242.
Stuart, M. J., A. M. Smith, S. A. Malo–Ortiguera, T. L. Fischer, and D.R. Larson. 2002. A comparison of facial protection and the incidence of head, neck, and facial injuries in Junior A hockey players. A function of individual playing time. American Journal of Sports Medicine 30(1):39-44.
Sulheim, S., I. Holme, A. Ekeland, and R. Bahr. 2006. Helmet use and risk of head injuries in alpine skiers and snowboarders. JAMA 295(8):919-924.
Sullivan, S. J., A. G. Schneiders, C. Cheang, E. Kitto, H. Lee, J. Redhead, S. Ward, O. H. Ahmed, and P. R. McCrory. 2012.What’s happening? A content analysis of concussion-related traffic on Twitter. British Journal of Sports Medicine 46(4):258-263.
Sun, J. F. 2013. See where your state stands on concussion law. http://usafootball.com/news/featured-articles/see-where-your-state-stands-concussion-law (accessed July 17, 2013).
Takeda, T., K. Ishigami, S. Hoshina, T. Ogawa, J. Handa, K. Nakajima, A. Shimada, T. Nakajima, and C. W. Regner. 2005. Can mouthguards prevent mandibular bone fractures and concussions? A laboratory study with an artificial skull model. Dental Traumatology 21(3):134-140.
Takhounts, E. G., R. H. Eppinger, J. Q. Campbell, R. E. Tannous, E. D. Power, and L. S. Shook. 2003. On the development of the SIMon Finite Element Head Model. Stapp Car Crash Journal 47:107-133.
Thompson, D. C., F. P. Rivara, and R. S. Thompson. 1996. Effectiveness of bicycle safety helmets in preventing head injuries: A case-control study. JAMA 276(24):1968-1973.
Thompson, D. C., F. Rivara, and R. Thompson. 2000. Helmets for preventing head and facial injuries in bicyclists. Cochrane Database of Systematic Reviews 2:CD001855.
Tierney, R. T., M. Higgins, S. V. Caswell, J. Brady, K. McHardy, J. B. Driban, and K. Darvish. 2008. Sex differences in head acceleration during heading while wearing soccer headgear. Journal of Athletic Training 43(6):578-584.
Tomei, K. L., C. Doe, C. J. Prestigiacomo, and C. D. Gandhi. 2012. Comparative analysis of state-level concussion legislation and review of current practices in concussion. Neurosurgery Focus 33(6):E11.
Torres, D. M., K. M. Galetta, H. W. Phillips, et al. 2013. Sports-related concussion: Anonymous survey of a collegiate cohort. Neurology Clinical Practice 3(4):279-287.
Triplette, J. 2013. Perspectives of Families, Coaches, and Officials. Presentation at the IOM Committee on Sports-Related Concussions in Youth Workshop, February 25. Washington, DC.
Trojian, T. H., and P. R. Hoey. 2012. Connecticut high school football coaches and concussion law CT PA 10–62. Connecticut Medicine 76(8):495-498.
U.S. Senate Committee on Commerce, Science, and Transportation. 2011. Concussions and the marketing of sports equipment. http://www.gpo.gov/fdsys/pkg/CHRG-112shrg73514/pdf/CHRG-112shrg73514.pdf (accessed September 6, 2013).
USA Football. 2013. See where your state stands on concussion law. http://usafootball.com/news/featured-articles/see-where-your-state-stands-concussion-law (accessed August 7, 2013).
USA Hockey. 2009. Checking the right way for youth hockey. http://www.usahockey.com/uploadedFiles/USAHockey/Menu_Coaches/Menu_Coaching_Materials/Menu_Checking_materials/Checking%20Manual_FINAL.pdf (accessed August 5, 2013).
USA Hockey. 2011. 2011–2013 Official Rules of Ice Hockey. http://www.usahockey.com/uploadedFiles/USAHockey/Menu_Officials/Menu_RulesEquipment/2011%20-%2013%20Rulebook.pdf (accessed August 5, 2013).
USA Hockey. 2013. 2013–2017 Official Rules of Ice Hockey. http://wwa.usahockey.com/uploadedFiles/USAHockey/Menu_Officials/Menu_RulesEquipment/2013-17%20USAH%20Rulebook.pdf (accessed September 6, 2013).
Valovich-McLeod, T., C. Schwartz, R.C. Bay, and R. Curtis. 2007. Sport-related concussion misunderstandings among youth coaches. Clinical Journal of Sport Medicine 17(2):140-142.
Versace, J. 1971. A review of the severity index. In Proceedings of the 15th Stapp Car Crash Conference. New York: Society of Automotive Engineers. Pp. 771-796.
Viano, D. C., and D. Halstead. 2012. Change in size and impact performance of football helmets from the 1970s to 2010. Annals of Biomechanical Engineering 40(1):175-184.
Viano, D. C., C. Withnall, and M. Wonnacott. 2012a. Effect of mouthguards on head responses and mandible forces in football helmet impacts. Annals of Biomedical Engineering 40(1):47-69.
Viano, D. C., C. Withnall, and D. Halstead. 2012b. Impact performance of modern football helmets. Annals of Biomedical Engineering 40(1):160-174.
Walsh, E. S., P. Rousseau, and T. B. Hoshizaki. 2011. The influence of impact location and angle on the dynamic response of the Hybrid III headform. Sports Engineering 13(3):135-143.
Williams, J. H. 2007. How safe are the new artificial turf fields? http://filebox.vt.edu/users/jhwms/SOS/Turf%20Field%20Research.pdf (accessed August 5, 2013).
Wisniewski, J. F., K. Guskiewicz, M. Trope, and A. Sigurdsson. 2004. Incidence of cerebral concussions associated with type of mouthguard used in college football. Dental Traumatology 20(3):143-149.
Withnall, C., N. Shewchenko, M. Wonnacott, and J. Dvoøák. 2005. Effectiveness of headgear in football. British Journal of Sports Medicine 39(Suppl 1):40-48.
Woods, S. E., E. Zabat, M. Daggy, J. Diehl, A. Engel, and R. Okragly. 2007. Face protection in recreational hockey players. Family Medicine 39(7):473-476.
Yard, E. E., M. J. Schroeder, S. K. Fields, C. L. Collins, and R. D. Comstock. 2008. The epidemiology of United States high school soccer injuries, 2005–2007. Sports Medicine 36(10):1930-1937.
Yoganandan, N., T. A. Gennarelli, J. Zhang, F. A. Pintar, E. Takhounts, and S. A. Ridella. 2009. Association of contact loading in diffuse axonal injuries from motor vehicle crashes. Journal of Trauma 66(2):309-315.
Zhang, L., K. H. Yang, and A. I. King. 2004. A proposed injury threshold for mild traumatic brain injury. Journal of Biomechanical Engineering 126(2):226-236.
Zonfrillo, M. R., C. L. Master, M. F. Grady, F. K. Winston, J. M. Callahan, and K. B. Arbogast. 2012. Pediatric providers’ self-reported knowledge, practices, and attitudes about concussion. Pediatrics 130(6):1120-1125.













































