
Quality of care is at the heart of any health care program, and yet it is defined in different ways and is difficult to measure. It is determined not only by the capabilities of health facilities and health providers but also by many other variables. Even among formal research studies, the variables measured differ from study to study. The following are the attributes of quality of health care listed in Crossing the Quality Chasm: A New Health System for the 21st Century, a report issued by the U.S. Institute of Medicine (IOM, 2001):
• Safe—avoiding injuries to patients from procedures that are intended to help them
• Effective—providing scientific-based services for all who may benefit and refraining from providing services to those not likely to benefit
• Patient-centered—providing care that is respectful of and responsive to individual patient preferences, needs, and values, and ensuring that patient values guide all clinical decisions
• Timely—reducing waiting time and harmful delays for both care receivers and caregivers
• Efficient—avoiding waste, including waste of equipment, supplies, ideas, and energy
• Equitable—providing care that does not vary in quality because of personal reasons such as gender, ethnicity, geographic location, and socioeconomic status.
Even in the most developed countries, however, quality of care as just defined is received by barely more than 50 percent of the patients who actually need it (Hayder and Dowson, 2005).
Information on many aspects of the quality of care is not readily available in Indonesia. In this chapter, we review those variables that affect the quality of care as it is delivered in Indonesia. Using the limited data available, we draw conclusions and offer some technical recommendations. We start with the human resources available and their abilities to meet current needs. We then discuss those programs available for the training of physicians and midwives and for their certification and skill maintenance. In this context, special attention is paid to accreditation and standards of care as determinants of the quality of care in Indonesia.
Human Resources Availability
According to Global Health Facts,1 Indonesia ranks 112 out of 144 countries in number of physicians. Over the period 2005-2010, the physician ratio in Indonesia was 3 per 10,000 population, which was the lowest for the Association of Southeast Asian Nations (ASEAN) region. Indonesia lagged behind Singapore (18 physicians per 10,000), Brunei (14), Vietnam (12), Malaysia (9), and even Myanmar (5). Currently, the Indonesian physician ratio is 4 per 10,000 population (WHO, 2012b).
1Global Health Facts, http://globalhealthfacts.org.
Similarly, the number of specialists, especially pediatricians and obstetricians, remains very limited. At present, the pediatrician ratio is 3 per 100,000 children (≤18 years). The corresponding 2011 pediatrician ratio for the United States was 49 per 100,000 children (≤18 years). In 2009 the number of obstetricians in Indonesia was about 2,600, which was far below the goal of 35,000 proposed by the Ministry of Health (WHO, 2012b).
In 2007 Indonesian midwives numbered 54,000, or about 30 per 100,000 population. However, by 2012 implementation of the village midwifery program described in this chapter had all but quadrupled the number of Indonesian midwives, to 200,000.2
All told, the figures indicate that the number of health care professionals in Indonesia responsible for reducing maternal and neonatal mortality is very limited. Although there is no exact correlation between the number of health care workers and the quality of care (something influenced by many other factors), the number of health care providers plays an important role in determining the overall quality of care.
The impact of the low number of health care professionals is further compounded by their drastically uneven distribution. For example, most specialists work in the larger cities. Indeed, 20-25 percent of all specialists work in Jakarta, which accounts for no more than 4 percent of the total population. Many districts still lack pediatricians, obstetricians, surgeons, and internists—the four specialists most important for reducing maternal and neonatal mortality (Ministry of Health, Data and Information Center, 2011).
Training
Midwives
Prior to 1984, the training of midwives entailed a three-year course of study in a midwifery school, which students entered at the end of junior high school. However, this course was terminated in 1984. No new midwives were trained for five years, until 1989 when the government launched the Midwifery Education Rapid Training Program in response to the international safe motherhood conference in Nairobi (Shiffman, 2003). Entrants to this program were graduates of health programs who had a basic nursing qualification. In 1998 the Rapid Training Program was replaced by the current midwifery schools,3 a three-year program that students enter at the end of their senior year in high school. But even in this program, only 10 of 30 topics in the curriculum emphasize clinical competency. The current workforce is composed of midwives trained in all three programs. However, the relative proportion contributed by the most recent midwifery school program has been increasing over time (Ministry of Health, Data and Information Center, 2011; Ikatan Bidan Indonesia, 2012).
In 2007 the Ministry of Health’s Center for Human Resources Development and the Indonesian Midwives’ Association (Ikatan Bidan Indonesia, IBI) developed a standardized examination system leading to the credential Certified Professional Midwife (CPM). The examination system was intended to define the standards for the CPM credential, describe the certification and examination process and requirements for application, maintain a registry of those individuals who had passed the examination and received certification, and manage the process of recertification or renewal. In addition, the examination system was to work in multiple related arenas to promote and improve the role of midwives in the delivery of maternity care to women and their newborns (Ikatan Bidan Indonesia, 2012; Ministry of Health, Center for Health Education and Training, 2007).
The mission just described was not fully accomplished until passage of National Education Law No. 20/2003, which established the National Education System in 2005-2006. In doing so, the law transferred responsibility for health education, including the midwifery schools, from the Ministry of Health to the
2Ikatan Bidan Indonesia (Indonesian Midwives' Association), http://www.bidanindonesia.org.
3Postsecondary schools.
Ministry of Education. The resulting 15-fold increase (from 50 to 750) in midwifery schools from 2006 to 2011, combined with the different perceptions in the two ministries of a certification-based platform and a competency-based platform, led to confusion about the skills and experience expected of a certified midwife and in the definition of a skilled birth attendant (Ministry of Health, 2007).
Concurrently, the membership of IBI increased from about 50,000 in 2006 to about 200,000 in 2012. However, IBI’s internal validation procedures revealed the inadequate knowledge, skills, and clinical experience of many of the new members. IBI concluded that the management and quality of learning in the program that lead to the CPM credential are stagnant or deteriorating. The internal review evaluated the multiple educational routes of entry, including apprenticeship, private midwifery schools, and college and university-based midwifery programs. So far, these findings have elicited no response from the Ministry of Education and local health authorities (Ministry of Health, Directorate General of Medical Services, 2011; Ikatan Bidan lndonesia, 2012; AusAid-PMPK Gama-HOGSI, 2012). Subsequently, the Indonesian Competency Assessment Board examined fresh graduates of midwifery schools and permanent or contract staff (PTT) midwives and reported their competency levels as substandard (Ministry of Health, Center for Health Resources Development, 2011).
Because competency is a primary prerequisite for health personnel working in the health delivery system, midwifery schools must supplement their curricula with in-service training either before or soon after the graduation of their students. Some midwifery schools collaborate with the National Clinical Training Network for Indonesia (Jaringan Nasional Pelatihan Klinis, JNPK)—the clinical training institution endorsed by the Ministry of Health since 1998—to improve health provider performance in Indonesia (JNPK, 2012).
In-service training for students of midwifery schools has not lacked internal and external critics. Sources of internal resistance have been the midwifery academy instructors and the Indonesian Midwives’ Association itself. Although the controversy has not been resolved, there is agreement that clinical training does provide a valuable opportunity to improve professional competency, standards of care, and practice with real clients (JNPK, 2010).
Both public and private sector midwives have the right to engage in private practice, and most do so after formal working hours (Ministry of Health, 2010b).
Nurses
The midwife certification process might benefit from linkage to the nurse certification model. Before 1979, nursing schools recruited junior high school graduates for admission, but after 2000 the nursing schools recruited only secondary school graduates. Although the curriculum for nurses includes basic delivery care, a graduate is not authorized to assist in labor or delivery. Ministry of Health Decree No. 369/Menkes/III/2007 and Decree No. 1464/Menkes/X/2010, which authorize a midwife to assist in labor, including management of early complications, and in family planning, do not apply to nurses. Even if a nurse has earned a master’s degree in maternity care, he or she does not have authority to assist in labor or delivery. This situation is unusual because this authority is not related to competency, as is common for other health professionals. Overall, it serves not only to limit effective utilization of health resources, but also to generate unproductive and unfair competition among health professionals. For example, midwives usually use the JNPK for improving their basic competencies, but this service is not available to nurses. They may use the JNPK only if they lack basic competencies for conducting government maternal, newborn, and child health programs (such as neonatal resuscitation skills) that might not have been included in their study (JNPK, 2012; Ministry of Health, 2010b).
Midwifery education is integrated into the nursing program in most countries. In some countries such as Bangladesh and Sri Lanka, midwifery education is offered to those who have already completed a diploma in nursing. Only a few countries, such as Indonesia and Myanmar, offer a separate program in midwifery training (Ikatan Bidan Indonesia, 2012). As in most countries in Asia, midwifery schools in Indonesia can integrate nursing and midwifery education, or they can run the schools separately.
In Indonesia, nurses are considered competent in neonatal care only when it is connected to the Ministry of Health program and training. In basic delivery care, the delivery and neonatal resuscitation caregiver is the midwife. The midwife could have learned neonatal resuscitation in a midwifery school and trained to be competent in the anatomic model in basic delivery care or basic emergency neonatal care with the JNPK (JNPK, 2010, 2012; Ikatan Bidan Indonesia, 2012).
The basic emergency obstetric and newborn care (BEmONC) concept is not included in the curriculum of the school of nursing or of the midwifery academies. It is a Ministry of Health program, and the nurse or midwife must attend a BEmONC training program to have this competency. At a BEmONC health center, the health care team consists of a general practitioner, a midwife, and a nurse. But they do not have equal roles in providing services because the birth attendant must be the midwife while the nurse serves as the provider of neonatal resuscitation (Ikatan Bidan Indonesia, 2012).
General Practitioners
In Indonesia, senior high school graduates must attend a five-year or 10-semester course of study to attain a degree as a medical doctor. These requirements were expanded in 2011 to include completion of a one-year internship before qualifying for licensure as a general practitioner (Konsil Kedokteran Indonesia, 2005).
Although the system has gradually been improved, the qualifications of the current graduates are not on a par with those associated with the medical education system before 1979. The 1995 list of medical doctor competencies has been reduced in both number and competency level required. In 1995 the level of skills needed to manage a normal delivery was “competency level.” In 2010 it was reduced to “acquisition level.” This level is lower than that required for professional midwives, who must be “competent” to attend a normal delivery (Konsil Kedokteran Indonesia, 2005; Ikatan Dokter Indonesia, 2007).
The mandatory postgraduate internships and lower grade of competencies required reflect a distortion of the learning process for medical students. A medical faculty considers the completion of a one-semester unit equal to one level of competency. This assumption is incorrect, however, because the topic in a curriculum relates only to the theoretical aspect, whereas competency in a skill requires a psychomotor aspect that builds only after practice and frequent repetition of a procedure related to several topics in the curricula (Konsil Kedokteran Indonesia, 2005; Ikatan Dokter Indonesia, 2007; JNPK, 2010). Some medical faculty graduates improve their competency through in-service training for subdistrict deployment, self-preparation, or participation in an obstetrics-gynecology (ob-gyn) specialist training program. The clinical training provides more opportunities for intensive coaching and practice with real obstetric patients, which is not possible in the medical education setting. Thus many general practitioners do not appear to have as much experience or skill in managing labor as a midwife (Ministry of Health, 2010a).
Specialists in Obstetrics and Gynecology
In Indonesia, to become a specialist in obstetrics and gynecology a graduate of a medical faculty must complete 10 semesters or five years of training. Before 2008, ob-gyn training was conducted in nine different training centers with no standard curriculum. In 2009 the Directorate General of Medical Services in the Ministry of Health asked the Indonesian College of Obstetrics and Gynecology (Kolegium Obstetri Ginekologi) to standardize the curricula and create modules in order to improve learning efficacy, budgeting efficiency, and timely graduation of trainees. From 2010 to 2012, 80 ob-gyn’s were produced each year by 15 training centers (Kolegium Obstetri Ginekologi, 2009).
The specialist training program is conducted by the Indonesian College of Obstetrics and Gynecology, which uses a competency-based training principle. The Competency-based Education Program for Medical Specialists (PPDSBK) was launched with an eye toward reducing the number of district hospitals without specialists. The Directorate General of Medical Services and the Indonesian Medical College deploy the fifth-semester resident ob-gyn’s, pediatricians, and anesthetists (those considered to have ade-
quate competencies to perform comprehensive emergency obstetric and newborn care, CEmONC) to remote district hospitals without waiting for them to graduate. This step is taken to avoid the administrative complications associated with employing graduates of specialist training centers. After six months of fulfilling this mandatory duty, the residents return to the training centers and complete their specialist training program (Kolegium Obstetri Ginekologi, 2009; Ministry of Health, Directorate General of Medical Services, 2009).
Although the standardization of curricula, basic clinical competencies, training modules, and preparation of classroom preceptors and clinical instructors were completed in 2007, only 3 of the 15 training centers have applied the learning standard appropriately. As of 2012, seven centers were approaching 80 percent of the standard, and five centers were below 80 percent. The average number of annual baby deliveries in each center was 2,500, or six to seven deliveries per day for all trainees. That figure is considered too low for developing clinical skills or achieving a level of competency (Kolegium Obstetri Ginekologi, 2012).
Pediatricians
Fifteen public medical schools offer pediatric training in Indonesia. Very similar to obstetric and gynecological training, pediatric training is competence-based, and the curriculum is developed and continually revised by the Indonesian College of Pediatrics (Kolegium Ilmu Kesehatan Anak). The training spans nine semesters, or 4.5 years. At the University of Indonesia, the first six months are dedicated to courses in research methods, statistics, evidence-based medicine, general pharmacology, and philosophy of science. The residents then begin clinical work, which includes a two- to three-month rotation among 15 subspecialties or divisions. The longest rotations are in the outpatient clinic and in perinatology (Kolegium Ilmu Kesehatan Anak, 2009).
Residents are trained to treat patients across the divisions under the supervision of staff. The training they receive depends on their level of residency (junior, medium, or senior). Residents at all levels participate in on-call duties, ward rounds, journal clubs, case presentations, and an outpatient clinic for general pediatrics (Kolegium Ilmu Kesehatan Anak, 2009).
Residents are also obliged to undertake a research project and write a formal thesis adhering to strict requirements (proposal development and examination, data collection and management, analysis, pre-seminar presentation, and formal examination). The results are to be published in a national or international journal—one of the requirements of the National Examination Board for pediatrician. Some observers consider this thesis project to be unnecessary because in many countries a formal thesis is an elective topic. In fact, many residents have to prolong their residencies to complete the thesis. Replacing the thesis requirement with a publishable evidence-based case report could reduce the duration and cost of residency, consistent with evidence-based practice (Kolegium Ilmu Kesehatan Anak, 2009).
The curriculum for pediatric training has been implemented in all specialist training programs in the 15 centers, with some modifications for variations among teaching hospitals in qualifications and facilities. For example, pediatric cardiac surgery and postoperative care can only be performed in six centers (with different capacities). Similarly, not all centers have the capacity to perform the molecular biology studies required to manage certain genetic syndromes. Implementation of evidence-based practice is also being employed in some centers.
In the area of neonatal health, residents are considered able to deal with normal and abnormal neonates with problems common in the neonatal period such as prematurity, asphyxia, management of respiratory distress syndrome, and neonatal infection. Pediatricians who are interested in becoming neonatologists can pursue two more years of training in perinatology. Most of them work in teaching hospitals, large district hospitals, and private hospitals.
Currently, some 100 pediatricians and 10 consultants in perinatology are produced each year. Pediatricians interested in a fellowship in neonatology receive six months of intensive training in a large neonatal unit, but this program is currently available only in Jakarta. The number of the fellows is presently
about 12-15 per semester. After completing the program, they are expected to be capable of managing most neonatal problems; however, no formal examination or certification is provided.
Accreditation and Licensing of Hospitals and Health Care Providers
Accreditation, especially of hospitals, has been introduced as a means of maintaining quality of care. The main challenge in measuring the variables determining the quality of care has been the limited resources available to carry out the process. One of the parameters used to judge quality of care is outcome, which, in this context, is measured by the infant mortality rate (IMR) and maternal mortality ratio (MMR). According to the 2012 Indonesia Demographic and Health Survey (IDHS), the reported infant mortality rate in Indonesia was 32 per 1,000 live births, and the maternal mortality ratio was 360 per 100,000 live births.
Indonesia’s accreditation system is run by the Ministry of Health (MoH), and inspections are carried out in all public and private hospitals every three years. The MoH accreditation outline generally compares with that enunciated by the Joint Commission International (JCI), including assessment of patient safety. Some of the private hospitals choose to forgo the MoH accreditation, relying instead on the International Organization for Standardization (ISO) applied by private companies (Ministry of Health, Committee for Hospital Accreditation, 2002). There is no accreditation process for outpatient programs, especially for villages and remote areas, including the village midwifery program.
Hospital accreditation is conducted by KARS, the Hospital Accreditation Commission. KARS accredits both public and private hospitals, but does not regulate the private practices of physicians and midwives. The accreditation commission examines five key hospital activities: management and administration, medical services, emergency services, nursing, and medical records.
According to Indonesia’s health minister, as of 2012 only five of Indonesia’s 1,800 hospitals were accredited internationally, and all five were privately owned. As of the same year, 65-66 percent of the 1,800 hospitals were nationally accredited, and one-third of those were privately owned (Jakarta Globe, 2012).
The Ministry of Health does have a system for registering and licensing health care providers. However, providers only need to fulfill a series of administrative criteria rather than demonstrate the minimum competence required to perform professional work. This system is contributing to significant variation in the quality of care among providers. Since 2007, physicians have had to take a mandatory competency test in order to get their license (Wang et al., 2009). For eligibility for license renewal, physicians are required to earn 250 continuing education units within a five-year period. However, no penalties or sanctions are in place for practicing at substandard levels, although the local health authorities, in collaboration with the Indonesian Medical Association or health professional organizations, can pull the licenses of physicians and midwives for cause (Government of Indonesia, 2004; Ministry of Health, 2010b).
Guidelines
Standards of care in hospitals are usually indicated by the guidelines they follow. Our observation indicates, however, that the guidelines are often not developed and implemented properly. And it is not unusual for guidelines to remain unrevised for a long time. In many situations, health professionals ignore the guidelines, and evidence-based practice is in fact not yet established.
In 2010 the Ministry of Health announced Health Regulation No. 1439 on Standards of Medical Care, which sets forth the National Clinical Practice Guidelines for diseases or conditions that have high prevalence, high risk, high cost, or high variability among patients. These guidelines must be adopted by every hospital in keeping with its capabilities. For example, a Class A hospital may be able to diagnose as well as treat infants with congenital heart disease (CHD). Another hospital of the same rank may be able to diagnose but not treat CHD. It follows that these two Class A hospitals likely subscribe to different clinical practice guidelines for the management of infants with CHD.
The guidelines are usually useful for patients with common characteristics. Deviations arise when a specific characteristic (e.g., allergy to a commonly used antibiotic) prevents the application of regular management. In almost all sets of guidelines, there is a disclaimer stating that the guideline is not a standard of care for every patient with the same diagnosis; rather, it is a recommendation that should be implemented in accordance with the individual patient’s characteristics. The health professional must state the reason he or she could not follow the guideline. However, the National Clinical Practice Guidelines and notifications of deviations from the guidelines have not been properly implemented in Indonesia (Ministry of Health, Directorate General of Medical Services, 2011; AusAid-PMPK Gama-HOGSI, 2012; JNPK, 2012).
Assessing the Factors Affecting Quality of Care Offered by Birth Attendants
Of those women who receive antenatal care in Indonesia, 71 percent will first visit a midwife, 20 percent an ob-gyn, 3 percent a traditional birth attendant (TBA), and 2 percent a general practitioner (Ministry of Health, Data and Information Center, 2011). However, as shown in Figure 5-1, more than 90 percent of births are overseen by midwives and TBAs (Indonesian Basic Health Survey, 2010).
The World Health Organization (WHO) defines a skilled birth attendant (SBA) as an accredited health professional—a midwife, doctor, or nurse—who has been educated and trained to proficiency in the skills needed to manage normal (uncomplicated) pregnancies, childbirth, and the immediate postnatal period, and in the identification, management, and referral of complications in women and newborns. However, only a small fraction of graduates of Indonesian midwifery training programs could meet the WHO definition of an SBA (Ministry of Health, Center for Health Education and Training, 2007; Ministry of Health, 2007; Ministry of Health, Center for Health Resources Development, 2011). In other words, the quality of training they receive is not sufficient to produce qualified midwives who are competent to provide the required midwifery services when they are deployed in community-based maternity clinics or health centers in both rural and urban settings. For example, 28-52 percent of midwives are unable to administer intrapartum care using a partograph (a tool for monitoring the first stage of labor), identify the presenting part of the fetus, estimate fetal weight, actively manage the third stage of labor, measure blood pressure, and provide clean and safe delivery care. They also lack other basic midwifery competencies (JNPK, 2010, 2012).
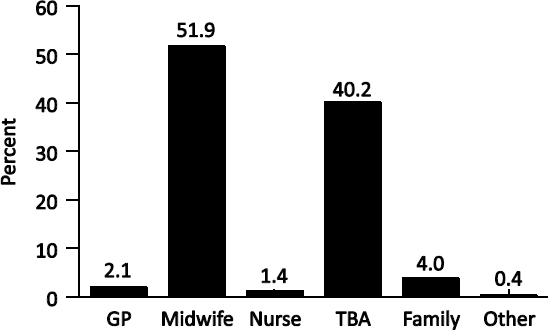
FIGURE 5-1 Birth Attendants at Delivery: Indonesia, 2010. NOTE: GP = general practitioner; TBA = traditional birth attendant. SOURCE: Indonesian Basic Health Survey (Riskesdas), 2010.
The goal of the Bidan di Dasa program was to place midwives in every village. This goal was largely achieved in the mid-1990s, but it could not be sustained despite the rapid growth in the number of midwives—in 2012 there were approximately 200,000, but only 40 percent of villages currently have a midwife. The other midwives moved to nearby urban areas in order to establish private practices while retaining a nominal village presence. The system also still suffers from a questionable quality of service because pre-service training is often weak and lacks opportunities to practice skills (Heywood and Harahap, 2009).
It is therefore not surprising to see some impact on maternal mortality, but not the full impact that might be expected from such a large-scale program. Indonesia has consistently relied on midwives in villages as the primary providers of maternal health services at the community level, whereas referral, promotion of facility-based delivery, and improvements in quality of care, which have a greater impact on maternal mortality, have only recently been placed on the policy agenda (Government of Indonesia, 2004; Ministry of Health, Directorate General of Medical Services, 2009; Ministry of Health, 2010a).
Although doctors can potentially offer more effective emergency management of complications than midwives, gains in effectiveness are limited if births are in health centers that do not have surgical and blood transfusion capabilities. If high coverage is to be attained, it should not be expected that all normal births would be attended by a doctor because deployment and retention might be more difficult and because of higher salary and training costs. Moreover, some hospitals have been shown to overtreat childbirth and have proven difficult to hold to account. Unnecessary interventions for normal births are likely to be more common in hospitals, as are the costs of care (Campbell and Graham, 2006).
Effects of Location on Quality of Care
In remote areas, a home birth with a skilled attendant may respond to a woman’s demand for home-based care, but home conditions can be extremely variable and inefficient in terms of the skilled attendant’s time and ability to cope with emergencies. The skilled attendant must be able to deal with first-aid for complications with assistance only from the family and to arrange transport for referral when necessary (McDermott et al., 2001). Furthermore, the attendant may not be skilled enough at managing home delivery complications, even when a woman seeks help early. At present, there are more maternal deaths in hospitals than in homes. This difference is attributed to the delays in transport to the hospital of women requiring emergency care. In a home delivery, the decision to transfer and arrange for transport are the responsibility of the midwife and family, and often action is taken too late for financial reasons, clinical errors, or even religious reasons. Hospitals claim that most mothers requiring emergency care arrive at the hospital in terminal condition (Olsen and Jewell, 2009). Most maternal deaths occur during labor, delivery, or the first 24 hours postpartum, and most of the relevant complications cannot be predicted or prevented. Fortunately, individual complications are quite rare, but timely diagnosis and treatment require considerable skills. The critical elements that determine the interventions needed and accessible, and ultimately the outcome, are a woman’s location at delivery, the attendant, and the availability and timeliness of transport (Iskandar, 1997; McDermott et al., 2001).
In Indonesia as a whole, 50 percent of the population lives in urban areas and 50 percent in rural areas.4 However, thirty-six percent of maternal deaths occur in urban areas and 64 percent in rural areas. Forty-two percent of deaths occur in public hospitals, 16 percent in private hospitals, and 30 percent in the home of the mother (UNFPA, 2012). A study of health disparities in access and quality in Indonesia’s five regions has shown that 76 percent of maternal mortality in urban areas occurs in public hospitals and 34 percent in rural areas. In Eastern Indonesia, the disparity occurs because of problems associated with emergency transportation to public hospitals (Olsen and Jewell, 2009).
42010 population census.
Ideally, all women would have immediate access to obstetric care, which would include intrapartum monitoring, as well as early detection and timely referral for complications (Hofmeyr et al., 2009). As noted in Chapter 3, basic emergency obstetric and newborn care comprises a series of interventions, including parenteral antibiotics, oxytocic drugs, anticonvulsants, manual removal of the placenta, postabortion care, forceps or vacuum delivery, and neonatal resuscitation. Comprehensive emergency obstetric and newborn care would add blood transfusion and cesarean section to the list. Staffing for basic emergency obstetric care would include the availability of at least two skilled birth attendants 24 hours a day, seven days a week. A skilled birth attendant should be capable of providing clean and safe delivery and immediate complication management and of recognizing conditions that require CEmONC services (Ministry of Health, Center for Health Education and Training, 2007; Ministry of Health, Directorate General of Medical Services, 2011; JNPK-PPSDM, 2012; JNPK-Dit Yanmed Spesialistik, 2012).
Nationally, of the 1,674 BEmONC health centers, 57.2 percent provide 24-hour services. When viewed regionally, the percentage of 24-hour BEmONC health centers in Eastern Indonesia is close to the national average at 71 percent. This finding suggests that, although these services may be available 24 hours a day, they are difficult to reach, and equipment and drugs are sometimes not accessible. Thus the risk of death remains high. In other words, facilities exist, but access to them may be especially difficult in remote and isolated parts of Indonesia (Olsen and Jewell, 2009).
Nationally, over 50 percent of public hospitals claim to have staff trained and equipped to offer CEmONC services 24 hours a day, seven days a week (Olsen and Jewell, 2009; Ministry of Health, Center for Health Research and Development, 2012). But in 2011, among the CEmONC hospitals, only 35 percent were found to have a complete clinical team available to offer adequate services all day every day. Regionally, there appear to be gaps in CEmONC services among the five regions. The Java-Bali region better fulfills CEmONC criteria than other regions, and hospital maternal mortality ratios and emergency response times are better in the western region than the eastern region (Olsen and Jewell, 2009; Ministry of Health, Directorate General of Medical Services, 2011; Ministry of Health, Center for Health Research and Development, 2012).
Some interventions are possible only in a CEmONC facility such as cesarean section and blood transfusions. However, other actions also can save many maternal and newborn lives if birth attendants are properly trained. It is important to ensure that life-threatening complications, particularly antepartum bleeding, which can be managed only by a CEmONC facility, are recognized early and referred before complications develop.
Technical Recommendations: Improving Quality of Care
In the implementation of a health program, priority should be given to preventing maternal deaths from direct obstetric causes and unsafe procedures. Training should emphasize rapid recognition of a high-risk pregnancy and labor, resuscitation and stabilization, timely and optimum referral, proper emergency responses and treatment, and effective post-treatment care in BEmONC or CEmONC facilities. Reporting practices should enable further studies of maternal death.
The following five technical recommendations pertain specifically to improving the quality of care. They are independent of this report’s general recommendations (see Chapter 8), and many of them can be implemented by the service organizations themselves.
1. Improve training quality within the certification system. Pre-service training and in-service competency-based workshops should be long enough and of sufficient quality to allow trainees to exhibit their knowledge and competency in essential skills, especially for emergency lifesaving. In other steps, (1) have professional organizations or other third parties conduct regular licensing and competency-based certification at prespecified intervals; (2) build regular supervision and mentoring into the program from inception, and train supervisors in motivational and support strategies (avoid punitive approaches); (3) design and incorporate integrated, pervasive
monitoring and evaluation processes into routine program implementation; and (4) carry out analysis and reporting across the full spectrum of implementation, from staff recruitment to health outcomes.
2. Give health care providers clear responsibilities and assignments. Although the Ministry of Health decree might be used as a legal foundation, the ministry itself must clearly set forth the scope of work for skilled birth attendants, including delegation of authority to perform lifesaving functions and assurance that additional duties do not distract from the mission of maternal and neonatal care. A formal community participation strategy should engage the community in the monitoring and evaluation of services.
3. Change the national education system from a certification-based system to a competency-based system. It should ensure that graduates have the skills needed to fulfill WHO’s definition of a skilled birth attendant. The system should include comprehensive strategic planning for creating and utilizing birth plans and nursing and midwifery services, and should involve all the relevant stakeholders in government, civil society, service delivery, and educational and professional organizations. Policies must focus on regulating practitioners, standardizing educational programs, providing support for nursing and midwifery, and promoting research within and outside the health sector to address significant gaps in policy development (WHO, 2012a).
4. Shift home-based deliveries to institution-based deliveries, attended by WHO-defined SBAs. All women should have immediate, full-time access to emergency care. The midwifery workforce should be capable of consistently meeting established standards of care and the expectations of the public. Strategies can draw on evidence-based recommendations and technical support to enhance midwives’ skills mix, performance, and mobility. National Human Resources in Health plans must cover the costs of nursing and midwifery personnel at every level, manage migration, and remain consistent with approaches to internal and interprofessional task sharing.
5. Reduce the inequity in the distribution of specialists and skilled birth attendants. Planning must take into account local health needs, the current state of health services, the provider mix, the available resources, and the local production and training capacity for health providers.
References
AusAid-PMPK Gama-HOGSI. 2012. Monitoring and Evaluation of Sister Hospital Program in Nusa Tenggara Timur Provinces. Yogyakarta.
Campbell, O. M., and W. J. Graham. 2006. Strategies for reducing maternal mortality: Getting on with what works. Lancet 368:1284-1299.
Government of Indonesia. 2004. Medical Practice Law No. 29/2004. Jakarta.
Hayder, A. A., and L. Dowson. 2005. Defining standards of care in the developing world: The intersection of international research ethics and health systems analysis. Developing World Bioethics 5(2):142-152.
Heywood, P., and N. P. Harahap. 2009. Human resources for health at the district level in Indonesia: The smoke and mirrors of decentralization. Human Resources for Health 7:6.
Hofmeyr, G. Justus, Rachel A. Haws, Staffan Bergström, Anne C.C. Lee, Pius Okong, Gary L. Darmstadt, Luke C. Mullany, Eh Kalu Shwe Oo, and Joy E. Lawn, 2009. Obstetric care in low-resource settings: What, who, and how to overcome challenges to scale up? International Journal of Gynecology and Obstetrics 107:S21-S45.
Ikatan Bidan Indonesia (Indonesian Midwives' Association). 2012. 50th IBI Anniversary. Yogyakarta. Available at http://www.bidanindonesia.org/index.asp?lang=en&part=2011020001.
Ikatan Dokter Indonesia (Indonesian Medical Association). 2007. Indonesian General Practitioner College, Basic Competencies and Post-graduate Internships. Jakarta.
IOM (Institute of Medicine). 2001. Crossing the Quality Chasm: A New Health System for the 21st Century. Washington, DC: National Academies Press.
Iskandar, M. B. 1997. Health and Mortality (1997) in Indonesia. Assessment: Population and Human Resources. Australian National University and Institute of Southeast Asian Studies, Canberra and Singapore.
Jakarta Globe. 2012. Only 5 Indonesian hospitals internationally accredited: Minister. February 15. Available at http://www.thejakartaglobe.com/archive/only-5-indonesian-hospitals-internationally-accredited-minister/498295/.
JNPK (Jaringan Nasional Pelatihan Klinis, National Clinical Training Network). 2010. Report on Post-training Qualification and Service Delivery Point Accreditation. Jakarta.
______. 2012. Indonesia’s Clinical Training Annual Report. Congress of the Indonesian Society of Obstetricians and Gynecologists, Denpasar, July.
JNPK (Jaringan Nasional Pelatihan Klinis, National Clinical Training Network)-Dit Yanmed Spesialistik. 2012. Comprehensive Emergency Obstetrics and Neonatal Care—Curricula and Modules for Health Professionals. Jakarta.
JNPK (Jaringan Nasional Pelatihan Klinis, National Clinical Training Network)-PPSDM. 2012. Basic Emergency Obstetrics and Neonatal Care—Curricula and Modules for Health Professionals. Jakarta.
Kolegium Ilmu Kesehatan Anak (Indonesian College of Pediatrics). 2009. Standard Curricula for Competency-Based Education for Pediatrics Specialists. MKKI-IDAI-Dit Yanmed Spesialistik, Jakarta.
Kolegium Obstetri Ginekologi (Indonesian College of Obstetrics and Gynecology). 2009. Standard Curricula for Competency-based Education for Ob-Gyn Specialists. MKKI-POGI-Dit Yanmed Spesialistik, Jakarta.
______. 2012. Annual Graduation Report 2011. Denpasar.
Konsil Kedokteran Indonesia. 2005. Indonesian Core Curricula of Medical Education. Jakarta.
McDermott, J., et al. 2001. Two models of in-service training to improve midwifery skills: How well do they work? Journal of Midwifery and Women’s Health 46:217-225.
Ministry of Health. 2007. MoH Decree No. 369/Menkes/III/2007—Midwife Standard Definition. Jakarta.
______. 2010a. Basic Health Research. Jakarta.
______. 2010b. MoH Decree No. 1464/Menkes/X/2010—License and Clinical Practice of Midwife. Jakarta.
Ministry of Health, Center for Health Education and Training. 2007. Midwifery School Training Curricula and Modules. Jakarta.
Ministry of Health, Center for Health Research and Development. 2012. Health Facility Research. Jakarta.
Ministry of Health, Center for Health Resources Development. 2011. Midwives Basic Competency and Performance Assessment Results. Indonesian Competency Assessment Board, Jakarta.
Ministry of Health, Committee for Hospital Accreditation. 2002. Hospital Accreditation System and Assessment Instruments. Jakarta.
Ministry of Health, Data and Information Center. 2011. Indonesian Health Profile Data. Jakarta.
Ministry of Health, Directorate General of Medical Services. 2009. PPDSBK Program for Accelerating Medical Specialists to Achieve MDG 2015 Targets. Jakarta.
______. 2011. Indonesia’s CEmONC Program Report 2007-2011. Jakarta.
Olsen, O., and D. Jewell. 2009. Home versus hospital birth. Cochrane Library, January 21.
Shiffman, J. 2003. Generating political will for safe motherhood in Indonesia. Social Science and Medicine 56:1197-1207.
UNFPA (United Nations Population Fund). 2012. Kajian Determinan Kematian Maternal di Lima Region di Indonesia,
Wang, Hong, Mark McEuen, Lucy Mize, Cindi Cisek, and Andrew Barraclough. 2009. Private Sector Health in Indonesia: A Desk Review. Bethesda, MD: Health Systems 20/20 project, Abt Associates Inc., February.
WHO (World Health Organization). 2012a. Enhancing Nursing and Midwifery Capacity to Contribute to the Prevention, Treatment and Management of Noncommunicable Diseases. WHO, Geneva.
WHO (World Health Organization). 2012b. World Health Statistics 2012. Available at http://www.who.int/gho/publications/world_health_statistics/2012/en/index.html.












