
Strengthening the Financing of Maternal and Neonatal Health
As earlier chapters have pointed out, understanding the epidemiological and social dimensions of Indonesia’s maternal and neonatal health (MNH) problem and choosing the right interventions are critical steps in accelerating progress on reducing maternal and newborn mortality in that country. 1 Indonesia also needs to strengthen the capacities of its health system to finance, effectively purchase, and deliver the requisite services to those who need them. This effort includes removing the barriers to effective use of the system, such as those related to financial cost.
This chapter reviews the evidence on how Indonesia finances its MNH services today and recommends steps to strengthen financing for better MNH outcomes. Overall, it calls for Indonesia’s public spending on MNH to rise in order to achieve the desired goals. However, it also points out that impediments to the effective use of the available funds in the current complex and highly variable financing system could be reduced to achieve better outcomes, even in the absence of additional funds. It notes as well that the information available for monitoring financing and ensuring accountability for positive change needs to be strengthened as part of future efforts to improve MNH financing.
Data Sources and Methods
Various data sources were identified for this chapter on the financing arrangements for and expenditures on maternal and neonatal health in Indonesia. The evidence collected was assessed for relevance and quality. The sources included:
• government budget and expenditure accounts;
• relevant household survey results such as those from the Indonesia Demographic and Health Survey (IDHS) and national household health and expenditure surveys;
• available studies and analysis of MNH expenditures such as reproductive health subaccounts;
• provincial- and district-level health accounting studies; and
• other studies and reports deemed relevant.
A variety of publicly available reports, documents, published articles, and presentations from January 2005 to August 2012 were also collected as part of this review project. The data sources were reviewed in August and September 2012.
In assessing Indonesia’s MNH spending, we used as a reference point the definition of “MNH expenditure” in the World Health Organization’s “Guidelines for RMNCH-GET: A Reproductive, Maternal, Newborn, and Child Health Government Expenditure (and Budget) Tool” (WHO, 2011: 53-54). This definition includes all expenditures associated with prenatal and postnatal care and delivery. Prenatal and
1This chapter is based on a background paper by Hasbullah and Brooks (2012) prepared for the U.S. National Academy of Sciences-Indonesian Academy of Sciences joint working group.
postnatal care includes the provision of micronutrients and food supplements to mothers before, during, and after pregnancy. Postnatal care refers to services rendered up to six weeks after delivery for the mother and 28 days after birth for routine care of the infant. Delivery includes emergency obstetric care to deal with complications and transport for emergency obstetric care.
No primary data were collected for this review project. All reviewed data sources associated with MNH financing and expenditure, in addition to the relevant national and district health expenditure, are listed in the references.
Total Health Expenditure
Indonesia’s total health expenditure is relatively low compared with that of other East and Southeast Asia countries. Indonesia spent 3 percent of its gross domestic product (GDP) on health in 2010; by contrast, the regional (East Asia and Pacific) average was 7 percent, and the global average was 10 percent (World Bank, 2012). In 2010 Indonesia spent US$18 billion on health care, almost all (99 percent) of which came from domestic funding sources (WHO, 2012). From 1995 to 2010, both government and household out-of-pocket spending on health increased (Figure 7-1). Of the total health expenditure of $77 per capita in 2010, the government accounted for 49 percent and household out-of-pocket spending for 38 percent (WHO, 2012). The remainder came mostly from other private sources.
Government health spending in Indonesia accelerated substantially during the 2000s with the introduction of several new initiatives in health insurance and decentralized financing. During the same time, household out-of-pocket spending also continued to increase.
Complex Financial Flows in Government Financing of Health Care
The flow of government health resources is a complicated process in Indonesia as shown in Figure 7-2. This complexity is only exacerbated by Indonesia’s strong decentralization policies, which result in substantial resource transfers directly to districts.
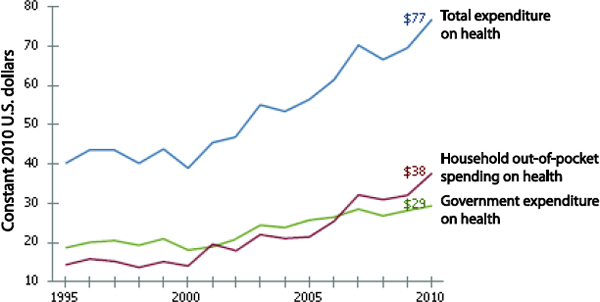
FIGURE 7-1 Per Capita Expenditure on Health: Indonesia, 1995-2010 (constant 2010 U.S. dollars). SOURCE: WHO (2012).
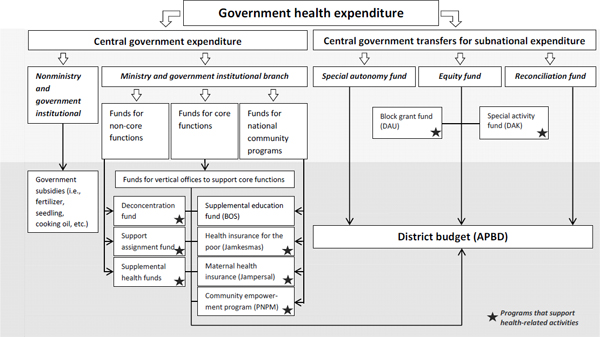
FIGURE 7-2 Overview of Government Health Resource Flows. NOTE: Core functions are foreign affairs, defense, security, justice, financial affairs, and religion. SOURCE: Center for Health Services Management, Faculty of Medicine, University of Gadjah Mada, http://manajemen-jaminankesehatan.net/index.php/80-sumber-dana/154-alur-belanja-apbn-ke-daerah.
Legally, the authority of the central and provincial governments to regulate and even monitor district-level expenditures is quite limited. As a result, to an unknown degree districts may allocate funds earmarked for MNH to other purposes and vice versa.
As illustrated in Figure 7-2, the national government’s health spending is split into two main pathways: direct central government expenditure and transfers for subnational expenditures. For the direct central government expenditure, health resources can flow through two main funding channels: (1) ministries and other government institutions and (2) other channels. Those that flow through the second category are mainly used to finance subsidies on basic goods and are not related to maternal and neonatal health.
Funds that flow through ministries and other government institutions can be further divided into funds for core functions, noncore functions, and national community programs. Funds for core functions support the administrative structures of government, such as those of the Ministry of Health (MoH), which in part indirectly support MNH services as well.
For the noncore functions funding channel, the central government has three categories of financing that can be used to support the direct and indirect costs of various health programs, including MNH at the provincial and district levels:
• Deconcentration fund (Dekon). Grants from the Ministry of Health used for central government-sponsored activities. District proposals that utilize these funds are approved at the provincial level.
• Support assignment fund (Tugas Pembantuan). Fund flows directed to district hospitals for physical assets, infrastructure, and equipment. The allocation and use of these funds are approved by the central Ministry of Health.
• Assistance Fund for Operational Costs at Health Center Level (Bantuan Operasional Kesehatan, BOK). Supplemental resources directed to community health centers (puskesmas) for health protection and promotional activities. These funds, which are allocated by the Ministry of Health, cannot be used to support personnel costs.
The other relevant central government funding channel, “funds for national community programs” (Mendanai Program Nasional Kewenangan Bersama), provides health resources to the district through several social assistance programs:
• Health insurance for the poor (Jamkesmas). This insurance provides free primary health care services for the poor, including maternity care, at community health centers (puskesmas) and inpatient services in hospital wards (third-class). Funds are approved by the Ministry of Health.
• Maternal health insurance (Jampersal). This insurance finances antenatal, postnatal, and family planning services for all pregnant women not covered by any insurance scheme at community health centers and hospitals. It also finances services at private facilities that have a memorandum of understanding (MoU) with the district health office. Funds are approved by the Ministry of Health.
• National Program for Community Empowerment (PNPM). These central government grants are used for community empowerment activities such as building and rebuilding village sanitation units and community health posts and constructing and reconstructing roads. Community proposals for these funds are approved by the district administration.
A separate channel of national funding is that transferred directly to district budgets (Anggaran Pendapatan dan Belanja Daetah, APBD) as funding support. As part of these transfers, two channels of central government financing are used to support various health programs, including MNH, at the district level:
• Block grant fund (dana alokasi umum, DAU). Grants from the central government to district governments to pay primarily civil servants’ salaries (e.g., doctors, nurses) and activities approved by the district parliament.
• Special activity fund (dana alokasi khusus, DAK). Specific sectoral grants from the central government that can be used for construction, rehabilitation, and equipment for primary care facilities.
Districts receive other fiscal transfers from the central government as well, and they have considerable discretion in how they use these funds. For example, in recent years district-based health insurance schemes (Jamkesda) have received greater attention; they may be funding MNH-related expenditures.
In addition to the funding sources just described, districts have their own directly raised and controlled revenue sources. This includes local taxes (pajak) and excise taxes and fees on natural resources. Districts may choose to allocate some of these funds to MNH-related activities. In addition, districts earn revenues directly from the user fees and other revenues received at district hospitals and health centers, some of which could be financed from transfers from the central government for health insurance. This latter flow is important for MNH because the districts have an incentive to collect revenue from users of government health facilities and health insurance schemes. The degree to which such revenue is “recycled” for MNH is unknown.
Overall, then, maternal and neonatal health care in Indonesia is characterized by fiscal complexity and limited information. It is known, however, that multiple channels of central and local funding can and do support MNH. Districts have substantial autonomy in deciding what to spend on specific health activities as well as incentives to increase their own revenue from some of these activities. It is hard to say with any precision how much is actually spent and from what sources. The discussion that follows on district health accounts provides further details.
Ministry of Health Financing of MNH Services
In 2010 Indonesia’s Ministry of Health had a budget of Rp 23.8 trillion (US$2.6 billion or about $12 per capita). Of those funds, 71 percent was allocated to patient services, comprising social health insurance, 30.4 percent; medical services, 29.4 percent; public health services, 6.7 percent; and pharmacy and medical supplies, 4.4 percent (Ministry of Finance, 2011). It is likely that both the patient services and nonpatient services categories of the MoH budget contribute to MNH services in an accounting sense, including both direct and indirect costs. For example, the MoH budget allocated to patient services, totaling US$1.8 billion, includes MNH expenditures such as the cost of deliveries and prenatal and postnatal care. The national budget does not provide a detailed function or service-level breakdown to allow a full accounting. Nor has a specific MNH “subaccounts” analysis been undertaken to provide such a breakdown.
What is important to understand is that MNH services are funded through different departments and programs under the overall ministry. For example, delivery services might be funded through hospital financing (medical services) for hospital-based deliveries or through nonhospital health facilities (public health services) for health center-based deliveries. Budgets for drugs and supplies may support both. Funds from government community social health insurance (Jamkesmas) are linked to maternal health as well. Table 7-1 provides examples of where expenditures associated with MNH activities can be found in the MoH budget.
Indonesia has been compiling a national health account (NHA) since 2004 (see, for example, Soewondo, Nadjib, and Soeharno, 2009). The NHA is a financial tracking system and accountability tool that provides the evidence needed to monitor trends in health spending for all sectors (public and private), health care activities, providers, diseases, population groups, and regions of a country. A standard methodology allows the complex tracking of a country’s health expenditures (WHO, World Bank, and USAID, 2003). Furthermore, subanalyses of the NHA allow one to track specific health programs, or so-
called subaccounts. Subaccounts associated with HIV, child health, and reproductive health provide detailed financial analysis in these specific areas.
The latest Indonesian national health account contains expenditure data up to 2010. It contains an HIV subaccount, but focuses mainly on sources of funding. As of September 2012, Indonesia did not have a reproductive, maternal, newborn, and child health (RMNCH) subaccount to track MNH-related expenditures, which would allow full measurement of MoH expenditures related to MNH.
Financing of MNH Health Insurance Programs
Indonesia’s current health insurance programs are summarized in Table 7-2. It is estimated that they cover less than half of the population, according to the figures available for this report. (However, the government of Indonesia is seeking to achieve “universal health coverage” by 2014, and so these figures may be changing.) The largest of these is the community health insurance program (Jaminan Kesehatan Masyarakat, Jamkesmas) targeting the poor.
In 2004 Indonesia created a platform for expanding health insurance coverage with the introduction of the Askeskin (Asuransi Kesehatan Keluarga Miskin) program, designed to increase access for the poor. The tax-financed targeted scheme for the poor and near-poor provided capitation payments to community health centers (puskesmas) and a fee-for-service health insurance scheme in third-class hospitals. In 2008 the program was expanded to include 76 million people under the current Jamkesmas program.
Since the introduction of Jamkesmas, district governments have also established complementary community-based health insurance schemes for the near-poor (Jaminan Kesehatan Daerah, Jamkesda) that provide basic health coverage for those who do not have Jamkesmas. With the lack of coordinated regulations and responsibilities between central and local governments, Jamkesda schemes have increased considerably over the last few years; an estimated 27 million households were covered through this insurance program in 2012 (World Bank, 2012). However, these schemes vary considerably in terms of the population groups they cover, benefit packages offered, member contributions, and the ways in which they are managed and organized.
| Budget, Ministry of Health, 2010—$2.6 billion |
| Social health insurance—$0.79 billion |
| • Social health insurance for the poor (Jamkesmas)—funding provided for MNH services such as antenatal, delivery, and postnatal care for pregnant women |
| Medical services—$0.76 billion |
| • Payment for health staff and facilities that provide MNH services in hospitals |
| Human resource development and training—$0.29 billion |
| • Training for health workers who provide MNH services |
| Secretary general—$0.28 billion |
| • Indirect costs for policy analysis and support |
| Public Health Service—$0.17 billion |
| • Immunization programs for newborn babies |
| • Nonhospital clinical services for deliveries, newborns |
| Center for Disease Control and Environmental Health—$0.16 billion |
| • Research and surveillance relevant to MNH |
| Pharmacy and medical supplies—$0.11 billion |
| • Drugs, medical supplies, and equipment related to MNH |
| Health Research Center—$0.03 billion |
| • Evaluation of MNH funding initiatives such as the BOK program |
| Inspector general—$0.01 billion |
| • Indirect costs associated with accountability of funding |
SOURCE: Ministry of Finance (2011).
TABLE 7-2 Health Insurance Programs: Indonesia, 2013
| Program | Model | Population | Coverage (Susenas) | Ambulatory services | Inpatient services | Maternity benefits |
| Askes | Social health insurance | Civil servants and their dependents, military | 14 million (2007) | Public only | Public only | Yes |
| Jamsostek | Social health insurance | Private formal sector employees and their dependents | 4.1 million (2009) | Public or private | Public or private | Yes |
| Jamkesmas | Social health insurance | Identified poor and near poor | 76.4 million (2009) | Mostly public | Mostly public | Yes |
| JPKM | Managed-care model | Informal sector, civil servants, military for their uncovered dependents | 0.5 million (2009) | Mostly public | Mostly public | Yes |
| Jamkesda | Various community-based health insurance schemes | Informal sector | 27 million (2010) | Public only | Usually not covered | Yes |
| Private health insurance | Private voluntary health insurance | Private formal sector employees and their dependents | 6.6 million (2006) | Private | Private | Yes |
NOTE: JPKM = Jaminan Pemliharaan Kesehatan Masyarakat.
SOURCE: Rokx et al. (2009).
As Table 7-2 shows, all of these schemes cover maternity care to some degree, although for some schemes this care may be limited to exemption from user charges in public facilities. To further improve the maternal health care situation and help achieve Millennium Development Goal 5 in Indonesia, the government launched a maternity coverage scheme (Jaminan Persalinan, Jampersal) in January 2011. Jampersal is directed at all pregnant women who are not covered by any insurance schemes. Services covered by Jampersal include antenatal care, delivery, postnatal care, and family planning. These services are offered in health centers and hospitals, both public and private, that have a memorandum of understanding with the district health office.
This program was designed as part of an effort to help reduce maternal mortality by reaching out to women who were not already covered for pregnancy and delivery-related services under other insurance schemes, particularly the insurance program Jamkesmas that was initiated in 2008 and aimed at the poor and near-poor,2 as well as older programs serving public sector employees, formal sector workers, and individually purchased schemes aimed mainly at the better-off. Jampersal is intended to be comprehensive, including coverage for health services during pregnancy and delivery as well as postpartum services for mothers (up to 42 days after delivery) and for their newborns (up to 28 days of age). Specific coverage is provided for health checks for pregnant women, aid delivery, childbirth services, postpartum family planning services, and newborn care.3
The program covers basic maternal health services at local health centers (Puskesmas and related local facilities), including services at private health facilities that have cooperation agreements (MCC) with
2Jamkesmas was a follow-on to programs initiated closer to the start of century aimed at providing free or inexpensive health care to Indonesia’s poorest households. These included a system of “poor-cards” issued by local officials and entitling holders to free services and an initial national program (from 2004) known as Askeskin that formalized this process for the poor. A main innovation of Jamkesmas was expansion of coverage to include the near-poor (a total of 76.4 million eligible participants) and the use of national survey data to define and target the potential recipients.
3See http://www.jamsosindonesia.com/prasjsn/jamkesmas/jampersal.
the district Jampersal management teams. Women can also receive more advanced services at the Class III level either indirectly through referral or directly in emergency cases at public and private hospitals having similar district-level cooperation agreements. Financial support is also available at the level of the health center through centrally provided operational funding (BOK program).
In theory, the program should help fill a gap and ensure that nearly all women willing to accept the standards of service provided have access to maternal care. However, although national surveys4 have included questions on access to health insurance, Jampersal has not yet been treated as a separate category, making it difficult to assess any impact.5 And because roughly the poorest third of the population (76.4 million) are supposed to be covered under Jamkesmas, it is not clear how this program by itself will affect the group of women who are most likely to have births at home and under less qualified medical supervision.
There may also be changes in the future stemming from the overall system management consolidation planned under the new government Health Insurance Implementation Board (Badan Penyelenggara Jaminan Social Bidang Kesehatan, BPJS) that will become effective in 2014. Even so, the availability of this kind of social insurance remains a potentially positive motivation for women to seek better care, and it remains one of a multitude of efforts that should be made available to help address the social and economic issues affecting the choices women and communities make about maternal health care.
As for the general extent of coverage itself, a 2009 national household survey reported that 43.6 percent of households had some sort of health insurance (Badan Pusat Statistik, 2010). For households that had health insurance, the different types are shown in Figure 7-3. Urban households had higher percentages of most types of health insurance programs, with the exception of health insurance for the poor, where higher percentages are found for rural households.
As discussed further in the next section, the linkage between what some government-financed insurance schemes cover (in the sense of providing a formal entitlement as part of a benefits package) and what their resources actually finance (i.e., what is actually paid for with health insurance rupiah) is difficult to determine because the largest schemes send their funds to the district administration and do not track the actual benefits received by enrollees. Thus figures on the share of health insurance funds financing MNH services are not available.
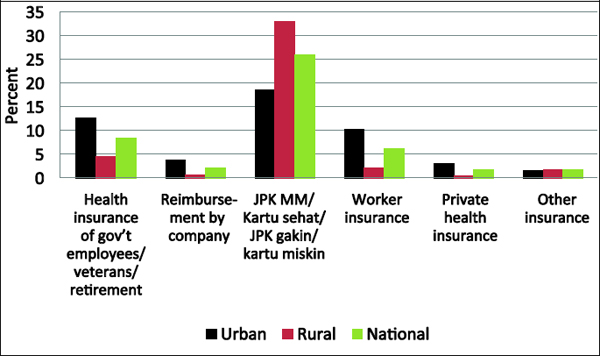
FIGURE 7-3 Percentage of Households with Health Insurance by Type: Indonesia, 2009. SOURCE: Badan Pusat Statistik (2010).
4Notably, the annual National Socio Economic Survey (Susenas).
5A few smaller-scale, largely qualitative evaluation studies are discussed later in the chapter. In addition, the latest (2012) Indonesian Demographic and Health Survey has shown a marked increase in births occurring in health institutions, which may provide at least some grounds for optimism.
District Health Expenditures on MNH Services
Districts are responsible for implementing government-provided health care. However, the complex flow of resources through the intergovernmental financial system and the varying capacities of district governments to generate health revenue on their own and through external revenue sources reportedly result in inequitable, inefficient, and fragmented financing across districts (Rokx et al., 2009).
Tracking the actual use of funds is also difficult. Most intergovernmental funds (such as those provided by the Ministry of Health and Jamkesmas) are passed from the central government to the district as a lump sum budget transfer and not for payment of specific health services. Because the decentralization policies enacted in Law No. 22/1999 and Law No. 32/2004 do not require specific financial reporting, the districts do not report to the central government how resources have been used from the various funding streams. As a result, the central government records only aggregated funding stream transfers without any detailed information on expenditures at the district level. Regulations have been developed by the Ministry of Home Affairs and the Ministry of Finance to achieve more accountability and transparency at the district level. However, the debates continue on the appropriate level of financial reporting that districts should undertake to the central government.
To make up for this lack of data, several studies conducted recently in Indonesia have sought to determine how resources are actually used at the district level (Mahlil, 2009; Gani et al., 2010; Seknas-Fitra, 2012). These studies of district health accounts (DHAs) required detailed work in specific districts to analyze the local expenditure accounts. Consequently, their coverage is limited.
In addition, these studies do not provide the detailed analysis needed to capture the entire government MNH expenditure. All the district health expenditure studies report the maternal and child health (MCH) expenditure and not the maternal and neonatal health expenditure. Any attempts to estimate the MNH expenditure from these data face two significant limitations. First, the MCH expenditure definition includes all health-related expenditure for mothers and children under age 5 and does not break out expenditures related only to maternal and newborn health. Second, the government MCH expenditure reported is usually only for services provided through the “public health” line of the budget, which covers mainly services for health promotion and prevention of illness (such as antenatal care or well-child services) and does not include expenditures on many MNH-related general clinical services in nonhospital facilities or hospital-based services. Thus these figures are a poor proxy for the total MNH expenditure.
Several studies have reported that the National Development Planning Agency (Badan Perencanaan Pembangunan Nasional, Bappenas) has recommended an MCH expenditure of Rp 65,000 (about US$7) per capita, although the source of that figure is not clear. All district health expenditure studies discovered in the course of preparing this report present MCH expenditures per capita that fall well below the recommended target, but again these do not include many MCH-related services. It is also not clear whether the recommended figure is intended to include all MCH-related clinical services or only the main promotional and preventive ones.
Mahlil (2009) analyzed district budgets (not actual expenditures) from 2007 to 2009 in 20 districts in five provinces. District budgets allocated 2.8-9.1 percent of their total health budgets to public health activities, with MCH services accounting for 17 percent of those public health budgets. On average, districts allocated Rp 3,250 per capita to the MCH expenditure per capita (5 percent of the Bappenas target), and Siantar was the district with the highest MCH expenditure per capita at Rp 7,400 (11 percent of the Bappenas target). Similar results are found in a study by Seknas-Fitra (National Secretariat—Indonesian Forum for Budget Transparency). This study analyzed district budgets for 2008-2011 in 20 districts in four provinces (Seknas-Fitra, 2012). According to its findings, districts allocated from 7.5 to 13.5 percent of total health budgets to public health programs, with MCH services accounting for about 5 percent of district public health budgets. Districts on average allocated Rp 9,000 per capita (approximately one U.S. dollar) to the MCH expenditure per capita (12 percent of the Bappenas target). The district Aceh Singkil had the highest MCH expenditure per capita at Rp 25,000 (34 percent of the Bappenas target).
Similar findings emerge from the district health account analysis conducted by Gani et al. (2010). The DHA methodology was developed by a team of researchers at the University of Indonesia’s Center
for Health Economics and Policy Analysis (CHEPA), and it follows the methodology developed for the national health account work by the World Health Organization (WHO), World Bank, and U.S. Agency for International Development (Gani et al., 2010). This methodology includes both government and non-government spending. Analysis of DHA data from 21 districts in Nusa Tenggara Timur (NTT) province show the high contribution of government sources of health funding (approximately two-thirds) to NTT province, a relatively poor area. About one-third of total health spending is from private sources, and 86 percent of that is from out-of-pocket spending. Personnel expenditures (28 percent) and drugs (22 percent) make up half of the total district health expenditure. Allocations of funds to MCH programs are minuscule, averaging 1.75 percent of total district health funding. The average MCH expenditure per capita is Rp 7,420, with the highest district, Lembata, spending Rp 25,866 per capita—only 40 percent of the Bappenas target.
The district health account study by Gani et al. (2010) provides several ways in which to understand the uses of health funds at the district level. When DHA data were organized by “program,” three categories were reported: public health, individual health, and capacity building. A separate MCH category was calculated within the public health category, which is the source used to calculate the percentage of health funds allocated to MCH programs. However, the costs associated with MCH services can also be found in other line item categories such as outpatient care, general treatment, and health insurance. As a result, the actual MCH expenditure may be higher than the numbers reported by the DHA because other MCH activities may be found in other line items. Gani et al. (2010) also report district budget allocations and not actual expenditures, which may be lower, or higher, than what was budgeted.
Impact of Government Financing Initiatives on MNH Services
Information on the effectiveness and impact of various MNH funding initiatives in Indonesia is limited because it is very difficult to link specific sources of funding to specific services. Another study by Gani et al. (2011) evaluated in 2011 the Bantuan Operasi Kesehatan (BOK) program in 39 districts in 13 provinces. The BOK program was implemented in 2010 to send supplemental funds from the Ministry of Health directly to puskesmas for the purposes of health protection and promotional activities (nonpersonnel). According to the findings, BOK on average added Rp 74.6 million per puskesmas. About 27 percent of BOK funds (Rp 20.3 million) were allocated to MCH programs, and from this amount the majority (85 percent) of resources for MCH were used for transportation costs (Rp 17.2 million). A pre-post analysis using a linear regression of composite indicators indicated that BOK funds had no impact on MCH performance. The lack of any significant impact on MCH is most likely a result of the implementation issues at the district level stemming from this newly implemented program.
As of August 2012, three studies had evaluated the Jampersal insurance program, which was implemented in January 2011: Trisnantoro, Riyarto, and Tudiono (2011)—from the University of Gajah Mada—in three provinces and six districts; Febriani (2011)—from Johns Hopkins University—in three provinces and six districts; and Rachmawati (2012)—from Health Research and Development (Litbangkes)/Ministry of Health—in seven provinces and 14 districts. The studies are mainly qualitative in nature with several quantitative analyses of utilization data over time. The results indicate a trend toward an increasing number of deliveries at district hospitals, but not at community health centers (puskesmas). Furthermore, the studies suggest limited understanding and awareness of the Jampersal program at the community level. Issues associated with funding were also noted by key informants—for example, the slow disbursement of funds and the overall low level of funds for the Jampersal program. Finally, the studies report concern about the inability of facilities to provide basic maternal services. In a program that tries to increase access to facility-based maternal health services, it is critical to ensure that these services have the personnel and equipment needed to provide good services.
Several recent reports from the World Bank (2008a, 2008b, 2010a, 2010b) and Rokx et al. (2009) discuss the effects of the central government’s increased support of MNH funding. Although the central government, recognizing the low level of funding to MNH, has tried to increase maternal health funding
through special programs and resources flows (i.e., BOK, Jampersal), these studies report there is evidence that districts may in turn decrease their own MNH funding allocation, resulting in little overall effect on the MNH expenditure (World Bank, 2010a).
District health funding from the central government is also associated with inefficiencies in financial management and accountability. The central government disburses funds to the district governments through lump sum budget transfers several times each year. However, disbursement is contingent on the submission of financial and programmatic reports by the district governments. Poorly staffed district health administrations or delays in collecting data from the local community health centers (puskesmas) can result in delays in submitting these monthly reports. As a result, funds are often sent late to the field, resulting in low absorption of health resources at the provincial and district levels. When funds are late, districts do not have enough time to spend allocated funds or implement planned programs. For example, Ministry of Health data revealed that West Papua, one of the poorer provinces in Indonesia, spent only 46.3 percent of its allocated health budget in 2006 (World Bank, 2010a). This situation suggests that simply increasing the resources available for MNH services (in budgets, for example) may not be sufficient to achieve rapid improvements in actual spending, especially in more remote areas.
Private Financing of MNH Services
Private financing still accounts for about half of Indonesia’s total health expenditure, and it is likely that this kind of financing is a significant source of overall funding for MNH services. Figure 7-4 is a recent representation of the complexity of private financial flows for health overall.
Although many of these flows are essentially “private to private,” such as when patients pay out of pocket for services from private providers, some of these private resources also flow into the public system in the form of user charges. As noted earlier, these charges can be an important source of revenue for district governments. Out-of-pocket spending also supports those “dual practice” private providers who may also be public sector employees.
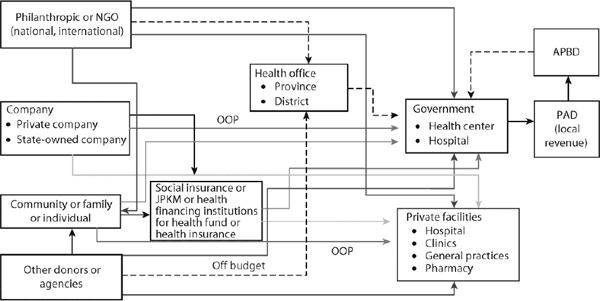
FIGURE 7-4 Overview of Private Health Resource Flows, Indonesia. NOTE: NGO = nongovernmental organization; APBD = regional government budget (Anggaran Pendapatan dan Belanja Daetah); JPKM = public health care insurance (Jaminan Pemeliharaan Kesehatan Masyarakat); OOP = out of pocket; PAD = local-owned revenue (Pendapatan Asli Daetah). SOURCE: Rokx et al. (2009).
For this report, it was not possible to obtain any information on the MNH expenditures of private companies or private insurers, both of which must be included in a comprehensive MNH subaccount. However, attempts were made to assess household out-of-pocket spending on maternal and neonatal health. Unfortunately, it was not possible to obtain the specific breakdowns of household spending that would allow a more detailed analysis. Nor was it possible to obtain information that would illuminate how much of private health spending supports private MNH providers, such as the private maternity hospitals that are widely present in Indonesian towns and cities.
The 2009 National Socio Economic Survey (Badan Pusat Statistik, 2010) indicated that households spent 4.5 percent of the total expenditure on health during the last month, with urban households (4.7 percent) spending a little more than their rural counterparts (4.2 percent).
Several recent national household surveys have collected more detailed information on health expenditures. Unfortunately, it was not possible to obtain from any of them the specifics on the MNH expenditure that are needed to better understand the totals or breakdowns of what households spend on MNH activities. Household spending information associated with major MNH-related health events (e.g., deliveries) are not collected as part of any routine national surveys conducted by the central government. Some limited information of this kind can be found in studies conducted by academic institutions, but these studies have limited geographic coverage.
One such costing study by Quayyum et al. in 2006 looked at the expenditure for different types of obstetric care in three government hospitals in Banten province (Quayyum et al., 2010). The study reported that the expenditure for obstetric care can be a significant financial burden for families (Figure 7-5). About half (51 percent) of women who delivered used an insurance scheme for the poor. However, a sizable proportion of women (41 percent) paid out of pocket. The main conclusion of the study was that insurance schemes for the poor appear to be effective in protecting households from catastrophic expenditure. However, the costing results from this study cannot be generalized because they are based on data from three government hospitals in a province in western Java. Nonetheless, they do provide important information on the approximate cost of obstetric care to families in Indonesia that cannot be found in any of the national household surveys conducted by Indonesia.
In 2007 the Ministry of Health instigated a system of Indonesian Diagnostic Related Groupings (IDRG) that provided parameters for charges at all facilities in order to standardize fees related to maternal health services across provinces and classes of services (Pujiyanto, 2009). For example, the allowable costs of a normal delivery range from US$70 at a Class C hospital to US$154 at a Class A hospital (average = US$112). For a cesarean section, the costs range from US$128 at a Class C hospital to US$282 at a Class A hospital (average = US$205). A comparison of the I-DRG fees set for Class C hospitals (the class of service utilized by the poor) with the household spending data from Quayyum et al. (2010) suggests a gap between the actual price of services and the total amount the government is willing to pay. For example, the reported price of a basic normal delivery is $15 more than what the government is willing to pay for such a delivery. This discrepancy is further highlighted for cesarean sections, where there is a sizable gap of $214 between the government payment and the actual cost of services.
In summary, the available evidence suggests that people can potentially be charged significantly more than the central government is willing to pay facilities for different types of obstetric care. This gap could have several consequences. Hospitals may be unwilling to accept insurance payments as sufficient for insured patients. Households may have to bear the burden of this difference through out-of-pocket payments, which could discourage even those with health insurance from using higher-level facilities. Facilities may perceive that serving insured patients causes them to “lose” money (reimbursements less than prices), and so they do not encourage access by poor insured patients. It was not possible to find any evidence on the presence or relative strength of these effects.
As health insurance coverage for MNH services expands, it is important that payments are sufficient to ensure the availability of services for the poor and that those covered do not incur substantial additional payments out of pocket, which could discourage the use of essential services.
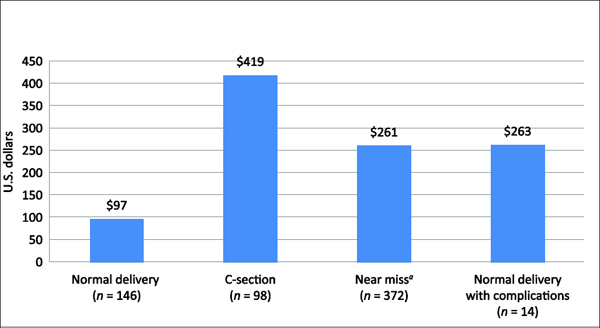
FIGURE 7-5 Mean Expenditure for Different Types of Obstetric Care in Government Hospitals in Banten Province, 2006 (U.S. dollars). a”Near miss” refers to pregnant women with severe life-threatening conditions who nearly die.
SOURCE: Quayyum et al. (2010).
Discussion and Recommendations
Despite major gaps in evidence, the overall picture of MNH financing in Indonesia that does emerge from this report has important implications for future efforts to reduce maternal and newborn mortality.
Spending on health care recently increased, but Indonesia is still spending relatively little, through both government and private sources, on health overall in comparison with other countries. Although spending on MNH services cannot be estimated reliably from the available data, it is likely that it is also quite low and insufficient to achieve the high levels of coverage and quality services needed to lower maternal and newborn mortality rates more rapidly. Unlike in some of its better-performing neighbors such as Sri Lanka and Malaysia, in Indonesia lagging MNH outcomes appear to stem not from inefficient spending but rather from underinvestment and insufficient allocation of resources to address priorities. Indonesia needs to spend more on this priority problem if it wants to see better results quickly.
The government of Indonesia has made significant efforts in recent years to increase its health spending and to focus on spending more on the poor and on priority health needs, which include reducing maternal and newborn mortality and improving maternal and child health. These efforts are evident from the growing government health spending relative to private spending and also from the number of new programs such as Jamkesmas and Jampersal that are intended to increase access to MNH services. However, significant governance and institutional issues are preventing these efforts from being more effective. Also, the gaps in the evidence available indicate that without significant efforts to reform reporting and accountability, it will remain difficult to identify and remedy the bottlenecks to translating increased spending on MNH into better MNH outcomes. Some key findings and recommendations are as follows:
• Indonesia’s complex and decentralized funding mechanisms are a significant impediment to any efforts to mobilize and target government funds to improve MNH-related service delivery in government health facilities. Districts need to set priorities in investment and health care operations and plan more explicitly how to finance these priorities using the existing financial channels. A
district MNH investment and financing plan linked to coverage targets would help provide guidance on financing the government supply of services. District plans should inform the development of national plans and budgets.
• The potential benefits of health insurance plans in increasing access to and use of health services and giving providers the incentive to deliver MNH services are largely lost when these funds are transferred as block grants to districts. Insurance could be much better targeted to increase both demand- and supply-side incentives to expand deliveries at qualified facilities as well as post-delivery follow-up. Insurance funds should be used to finance a payment and purchasing mechanism for MNH services that links eligibility for coverage with a financial entitlement that gives providers the incentive to deliver covered services to those that need them. This mechanism could be operated at the district level, but must have some level of financial accountability to the sources of insurance funds at both the district and national levels.
• In Indonesia, a country of great physical diversity, there are significant disparities in levels of spending on maternal and neonatal health across districts and regions. These disparities are inversely correlated with MNH needs and the likely cost of providing coverage with life-saving services of good quality. Differences in funding allocations across districts may also be related to districts’ willingness to spend on MNH—the poorer, more remote districts may have fewer resources, greater demands across other development sectors, and weaker governance, thereby crippling efforts to ensure effective spending. The financing strategy for MNH should include explicit efforts to direct more resources to areas with greater needs and also assistance to strengthen financial management and monitoring to ensure better use of funds. Mechanisms that give local governments the incentive to deliver on MNH targets and commitments should be developed as part of this strategy.
• The information available on MNH spending levels and the effectiveness of spending is insufficient for monitoring resource flows for MNH and ensuring efficient spending and accountability. Indonesia should develop a functional system for tracking the resources that are allocated and spent on MNH services from the national level down to the district level. This system should integrate data on budgets and expenditures from the different channels of spending, including those at the district level. Resource tracking for MNH should be linked to monitoring of coverage and quality levels and changes, and the monitoring outcomes should be used to develop evidence on program cost and results that can be used to improve program performance.
• The aggregated data indicate that the private sector plays a significant role in both the financing and delivery of health care in Indonesia. It is likely that a large part of MNH expenditures are financed by out-of-pocket payments, even though health insurance coverage is expanding. MNH services are provided widely on a private basis, including through midwives and physicians in private practice as well as private maternity hospitals (rumah sakit bersalin). It was not possible to obtain sufficient evidence on the financing and costs of private MNH services. In developing policies to accelerate the achievement of MNH outcomes, Indonesia should consider how to better engage private providers to contribute to increasing coverage with quality services. Such a step could involve channeling some financing to private maternity hospitals where these would increase access to safe delivery services equivalent to that provided by comprehensive emergency obstetric and newborn care (CEmONC) facilities or where government and private facilities could share the costs of essential inputs such as blood banks, anesthesia services, and specialist obstetric care.
Currently, Indonesia’s health financing policies are not sufficiently well designed and focused to support national strategies to rapidly improve MNH outcomes. It is recommended that enhanced national efforts include provisions for additional spending, better use of purchasing and payment methods to improve spending efficiency, and more and better information on planning, monitoring, and accountability, including around the role of the private sector. A strong health financing component should be built into national policies going forward.
References
Badan Pusat Statistik (Statistics Indonesia). 2010. Susenas (National Socio Economic Survey). Jakarta.
Febriani, Esty. 2011. Laporan Hasil Kajian Pelaksanaan Program Jampersal di 6 Kabupaten. Johns Hopkins University Center for Communication Programs, Jakarta. Available at http://www.kesehatanibu.depkes.go.id/wpcontent/uploads/downloads/2012/08/Hasil-Studi-Jampersal-2011_Esty-Febriani.pdf.
Gani, A., et al. 2010. The Methodology of DHA: A Guide Book for Those Implementing the DHA in Indonesia. 3rd ed. Jakarta: CHEPA (with AusAID funding support).
Gani, A., Pujiyanto, D. Dunlop, A. Hajaraeni, Mundiharno, T. Tachmanand, and H. Wahyu. 2011. Laporan Hasil Studi: Pengembangan Sistem Monitoring dan Evaluasi Biyaya Operasi Kesehatan (BOK). University of Indonesia School of Public Health, Depok.
Hasbullah R., and M. Brooks. 2012. Review of maternal and neonatal health (MNH) expenditure in Indonesia. Background paper prepared for U.S. National Academy of Sciences/Indonesian Academy of Sciences Joint Committee on Reduction of Maternal and Neonatal Mortality in Indonesia. Jakarta, October.
Mahlil, R. 2009. Analisi Anggaran Kesehatan Ibu, Bayi Baru Lahir, dan Anak Belita (KIBBLA) di Daerah Binaan HSP 2007-2009. University of Indonesia School of Public Health, Depok.
Ministry of Finance (Mentri Keuangan Indonesia). 2011. Profil Anggaran Kesehatan Kementrian Kesehatan. Jakarta.
Pujiyanto. 2009. Pengalaman Pembayaran Klim Askeskin Vs INA-DRG. In Sakit, Pemiskinan dan MDGs, H. Thabrany, ed. Jakarta: Kompas.
Quayyum, Z., M. Nadjib, T. Ensor, and P. K. Sucahya. 2010. Expenditure on obstetric care and the protective effect of insurance on the poor: Lessons from two Indonesian districts. Health Policy and Planning 25:237-247.
Rachmawati, T. 2012. Studi Evaluatif Implementasi Jampersal di 14 Kabupaten. Center for Health Research, Ministry of Health, Jakarta.
Rokx, C., G. Schieber, P. Harimurti, A. Tandon, and A. Somanathan. 2009. Health Financing in Indonesia: A Roadmap for Reform. Washington, DC: World Bank.
Seknas-Fitra (National Secretariat-Indonesian Forum for Budget Transparency). 2012. Laporan Analisis Anggaran Daerah 2011: Temuan-temuan Hasil Studi Pengelolaan Anggaran di 20 Kabupaten/Kota Partisipan Program KINERJA. KINERJA/RTI, Jakarta.
Soewondo, P., M. Nadjib, and R. Soeharno. 2009. The Indonesian National Health Accounts: Year 2003-2004. University of Indonesia School of Public Health, Jakarta.
Trisnantoro, L., S. Riyarto, and Tudiono. 2011. Monitoring Pelaksanaan Kebijakan BOK dan Jampersal di DIY, Papua dan NTT. Center for Health Services Management, University of Gadjah Mada Faculty of Medicine, Yogyakarta.
World Bank. 2008a. Indonesia Quarterly Economic Update: Battening Down the Hatches. Jakarta: World Bank.
______. 2008b. Investing in Indonesia’s Health: Challenges and Opportunities for Future Public Spending. Washington, DC: World Bank.
______. 2010a. “… And then she died.” Indonesia Maternal Health Assessment. Jakarta: World Bank.
______. 2010b. Indonesia Health Sector Review—Accelerating Improvement in Maternal Health: Why Reform Is Needed. Washington, DC: World Bank, UKAid.
______. 2012. Protecting Poor and Vulnerable Households in Indonesia. Jakarta: World Bank.
WHO (World Health Organization). 2011. Guidelines for RMNCH-GET: A Reproductive, Maternal, Newborn, and Child Health Government Expenditure (and Budget) Tracking Tool. Working document. Geneva.
______. 2012. WHO Health System Financing Country Profile: Indonesia 2010. National Health Accounts Database. Available at http://apps.who.int/nha/database/StandardReport.aspx.
WHO (World Health Organization), World Bank, and USAID (U.S. Agency for International Development. 2003. A Guide to Producing National Health Accounts with Special Application to Low and Middle Income Countries. Geneva: WHO.
This page intentionally left blank.
















