
2
Measuring and Conceptualizing Elder Abuse
Measuring elder abuse is challenging, as definitions and conceptualizations of what constitutes elder abuse vary across disciplines, sectors, and cultures. The lack of common definitions and conceptualization of elder abuse and the need for common ground to better understand and collect data on elder abuse were raised by several workshop speakers. As workshop speaker Robert Wallace from the University of Iowa commented, “The problem is, if we do not count cases with good definitions, we cannot know how many people there are. If we do not know that, we do not know whether the [intervention] program works.”
Speaker and planning committee member Tara McMullen from the Centers for Medicare & Medicaid Services noted that even across U.S. government agencies, definitions of elder abuse and how it is classified vary. As acknowledged by the Centers for Disease Control and Prevention, “elder abuse has been (1) poorly or imprecisely defined, (2) defined specifically to reflect the unique statutes or conditions present in specific locations (e.g., states, counties, or cities), or (3) defined specifically for research purposes. As a result, a set of universally accepted definitions does not exist” (CDC, 2013).
Although how elder abuse was defined varied, the categories of abuse discussed at the workshop included physical, sexual, emotional, and financial, as well as neglect and self-neglect. Several speakers also raised some culturally specific types of abuse, such as exclusion from participation in cultural activities. In addition to varying definitions and concepts, measuring and ultimately preventing elder abuse is complicated by several other factors that were raised by workshop speakers: the setting and cultural
context in which it occurs; the role of cognitive impairment; unique challenges in terms of neglect and self-neglect; and lack of a common conceptual framework.
SETTINGS
Several speakers noted that there are not only differences in types of abuse, but that it occurs in different settings, primarily differentiating between community and institutional settings. Workshop speakers presented findings from research on elder abuse in both the community and institutions and the implications for each.
Abuse Occurring in the Community
Workshop speaker Ron Acierno from the University of South Carolina presented findings from the National Elder Mistreatment Study, which surveyed community-presiding older adults in the United States. The study found that the rate of elder mistreatment in the community was 10 to 11 percent, not including financial exploitation. Acierno noted that the majority of the violence in the community is domestic violence. He further noted that the participants in this study gave consent to participate, and therefore the rates of dementia among the participants were limited, if at all present. He suggested that because little is known about the effects or remedies for elder abuse within the community, this high rate of mistreatment among community-residing, primarily non-demented, older adults was very concerning.
Several workshop speakers commented on the complexities of elder abuse in the community. The role of family members who may be caregivers and/or abusers, issues of neglect and self-neglect, cultural perceptions of elder abuse within the family, and stigma were all raised as contributors to elder abuse in the community.
Domestic violence in which victims are community-residing older adults has a unique set of challenges from other forms of domestic violence. Administration on Aging Assistant Secretary Kathy Greenlee, a workshop speaker and Forum member, commented that often older adults who are being abused need other services. She asked the audience, “How do you [plan care] for them? Or [do] safety planning? How do you continue to support someone who is a victim of domestic [violence] and is 75 or 85?” These issues need to be addressed in the context of community-residing victims of elder abuse.
Cultural Context
Workshop planning committee co-chair and Forum member XinQi Dong, from the Rush Institute for Healthy Aging, noted that elder abuse in the community setting is further complicated by the sociocultural context. Within the areas of elder abuse research, practice, and policy, he suggested that consideration of culture issues needs to be included to effectively address the needs of the individuals within their communities. Workshop speaker Lori L. Jervis of the University of Oklahoma commented on cultural relativity and the importance of not making assumptions about how types of abuse are perceived within different cultures. For example, she noted that one type of abuse within Native American populations is spiritual abuse. Being denied access to ceremonies that the group finds essential or important and being denied access to a traditional healer when one is sick are examples of what Native American people consider abusive that other populations may not. From her research within the Native American populations, Jervis found that elders see good treatment as a mixture of being taking care of, having one’s needs met, and being respected. (For more information on Native American populations and elder abuse, see Jervis in Part II of this report.)
Workshop speaker Elsie Yan from the University of Hong Kong noted that, in Chinese populations, disrespect and being ignored or left out of family gatherings are major forms of elder abuse. In Chinese American populations, psychological abuse is considered worse than physical abuse; disrespect, cursing, and ignoring are seen as worse than hitting or other types of physical abuse. In Korean and Indian populations, older adults tend to have high tolerance for financial abuse, as it is common practice for older people to transfer their property and valuables to their adult children in hopes that they would take care of them as they age. In many cases, that does not happen. (For more information on elder abuse in Asia, see Yan in Part II of this report.)
Consistent with findings presented by other workshop speakers, Jervis noted that within the Native American populations, she has observed that elder abuse occurs most frequently within a family. Workshop speaker Charles Mouton from Meharry Medical College commented on the complexity of family and community relationships in the reporting of elder abuse. In the context of African American families, older adults often want their children nearby, even if they are being abused by them. They often are reluctant to report abuse because they do not want to harm their family’s reputation in the community, or be seen as going against their kin. Jervis and speaker E-Shien Chang from the Rush Institute for Healthy Aging also commented on this issue of family stigma as a barrier to reporting in Native American and Chinese communities, respectively. Often, there
is a perception that what happens in the family should stay in the family, and reporting abuse could embarrass the family in front of the larger community.
Chang noted that there is a unique aspect of the perception of elder abuse within Chinese communities that stems from the Confucian belief in filial piety, which dictates children’s obligatory roles and responsibilities of caregiving to aging parents. Traditionally, filial piety is expected of adult children and there is a high expectation of emotional support. However, modernization has led to more mobility of adult children from rural to urban settings, affecting traditional family structures and intergenerational caregiving. Within Chinese American communities, filial piety is being affected by a shift from the traditional Chinese conception of collectivism towards the Western individualistic tradition. The discrepancy of expectation versus the receipt of the filial piety made predispose older Chinese Americans to consequences of elder abuse. (For more information on elder abuse and Chinese communities, see Chang and Dong in Part II of this report.)
Social Support and the Community
In the context of culture, community and social support play a large role in an older adult’s well-being. Throughout the workshop, low social support, or a lack of social connectedness and connectedness to the community, was mentioned as a risk factor for elder abuse. Acierno and colleagues (2010) found low social support as a risk factor for emotional, physical, and sexual mistreatment, as well as neglect. Mouton noted that, within African American communities, abuse is greater among those who are socially isolated; a lack of familiar social networks puts them at somewhat higher risk for abuse.
The issue of migration combined with social isolation and low social support was discussed by several participants. Yan noted that aging migrants often live in communities without family members in close proximity. Forum member Michael Phillips from Shanghai Jiao Tong University School of Medicine commented that, in mainland China, young people are migrating away from the rural areas and into cities, leaving their aging parents behind. Workshop planning committee member Alexander Kalache from the International Longevity Centre–Brazil suggested that the issue of migration is complex; some individuals migrate because they are in search of work and entrepreneurial opportunities, while others migrate because they are persecuted in their home country. These are quite different experiences and the impacts on social support vary. In situations where a community migrates together, they tend to stay together, have extremely close links, and often look out for each other. He suggested that, in terms of the issue of migration and social support, the location of one’s birth is not
what matters, but rather the density of individuals from the same cultural background who are in one’s community.
Yan mentioned additional factors that are affecting social isolation of older adults: environmental and structural changes to communities. In China, the government is removing older community dwellings and developing new buildings. Through the relocation process, older adults who used to have a very good social network in their communities and buildings are losing their social supports.
Abuse Occurring in Institutions
Workshop speaker Mark Lachs from Weill Medical College of Cornell University presented on elder abuse occurring in nursing home facilities. Although reports of elders being abused by nursing home staff have been sensationalized in the media and used to sway public opinion, close some facilities, and require background checks, Lachs suggested that major forms of violence in long-term care that pose the greatest threat to residents go unaddressed.
In the 1970s in New York state, there were descriptions of abuse committed by staff and legislation was passed to protect nursing home residents. About 15 or 20 years ago, a small amount of literature began to emerge about residents themselves committing violence against staff. In this research, staff were asked if they had been physically assaulted by their residents. About 50 percent of the staff described being physically assaulted in the course of providing care to residents. There is also literature about rates of staff-to-staff aggression. More recently, research has been being conducted on resident-to-resident aggression. Figure 2-1 is a model Lachs presented to show the types of violence occurring in nursing homes and the actual level of harm (as opposed to the perceived level) to residents.
Lachs commented on staff-to-resident and resident-to-resident violence from his experience. “I have spent tens of thousands of hours in nursing homes as a physician,” he said. “I have never physically seen a staff member strike a resident with my own eyes. Yet every day, I see residents saying bad things or physically striking one another.” In addition, Lachs suggested that resident-to-staff abuse may put residents at risk if poorly trained staff retaliate.
Lachs presented the findings of the study he and his colleagues completed on resident-to-staff aggression. They found that resident-to-staff aggression, including verbal, physical, and sexual aggression, was extremely common, with more than 15 percent of residents exhibiting such aggression within the previous 2-week period. Residents demonstrating resident-to-staff aggression were more likely to be white, require more assistance with activities of daily living, and have affective and behavioral disturbances.
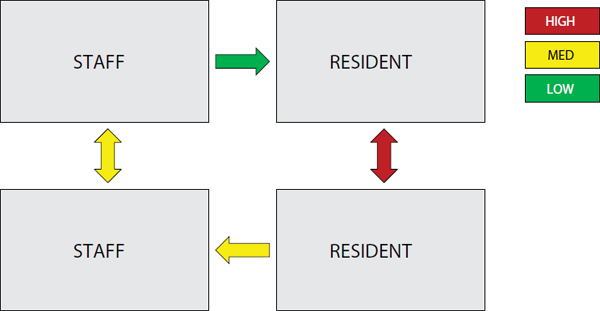
FIGURE 2-1 Actual (versus potential) harm to the largest number of residents.
SOURCE: Lachs, 2013.
Lachs defined resident-to-resident elder mistreatment as “negative and aggressive physical, sexual, or verbal interactions between long-term care residents that would likely be construed as unwelcome by the recipient in a community setting, and that have high potential to cause physical or psychological distress.” In terms of prevalence estimations, measuring resident-to-resident violence is extremely challenging. Lachs noted that for domestic violence, a large amount of the data is collected through self-reporting; however, in nursing home settings, rates of cognitive impairment are so high that self-reporting can result in high levels of false positives and false negatives. Despite the challenges of measuring resident-to-resident aggression within institutions, Lachs suggested that with innovative methods and a research agenda, it can be done. Currently, a National Institute on Aging–funded study of resident-to-resident elder mistreatment in 10 facilities is employing methodology to try to ascertain prevalence rates and identify resident, facility, and contextual correlates. The study is triangulating case findings from multiple sources, including (1) a culturally validated instrument administered to residents and primary certified nursing assistants; (2) incident reports; and (3) “shift coupons,” a novel method adapted for staff identification of resident-to-resident mistreatment in real time.
Workshop speaker Pamela Teaster from the University of Kentucky commented that the evidence so far indicates that abuse occurs more predominantly in the community setting and more dominantly by family and friends than other individuals, but the field still has much to do to understand the nuances of types of abuse. She remarked, “Those types
of individuals who may be the offenders, the abusers, the perpetrators, can also be spouses, can also be other intimate partners, can also be carers, can also be paid, can also be providing volunteer services; all those individuals in community settings or in facility settings can be potential victims and can be potential abusers.”
COGNITIVE IMPAIRMENT
As was recognized in discussions about the settings in which abuse occurs, cognitive impairment is a unique challenge in elder abuse. Several speakers commented that, when addressing elder abuse, distinction should be made between cognitive impairment and non-cognitive impairment, as the remedies will be different. Acierno suggested that abuse against non-cognitively impaired older adults is violence against an independent adult by an independent adult, and thus should be perceived as domestic violence. In domestic violence, the intervention is very different than in child abuse, in which a non-independent, non-empowered individual is being abused by an independent, empowered individual.
Recognizing that cognitive impairment is and will be a major problem that has to be addressed in the field of elder abuse, workshop speaker Jason Karlawish from the University of Pennsylvania suggested two important ways in which cognitive impairment and elder abuse intersect. First, cognitive impairment has been recognized as a problem and national attention is being paid to addressing it as a disease-based problem. One of the first signs of cognitive impairment is the inability to manage finances, which also is one of the risk factors for being a victim of elder abuse and exploitation. The more elder abuse awareness and prevention is linked to a disease-based mandate that has policy makers’ attention, such as cognitive impairment, the more progress can be made. Second, Karlawish noted that the field of cognitive impairment deals with biological, pathological, clinical, and ethical issues, including ethical issues on elder abuse.
Phillips commented that, in many developing countries, less than 1 percent of the seriously disabled elderly are in institutions. Thus, while elder abuse often is characterized by the setting, either in the community or in an institution, such a characterization does not necessarily distinguish between those who are cognitively impaired and those who are non-cognitively impaired. Phillips further elaborated that there are levels of cognitive impairment to consider: those who are severely demented and therefore incapable of expressing their own desires, and those who are mildly demented and have some degree of capacity. In addition, within institutions, there are individuals with physical illness who are not necessarily cognitively impaired. Therefore, one way to consider characterizing elder abuse and its remedies could be to think of a matrix with six categories:
the three levels of cognitive impairment and in the setting of either the community or the institutions. Workshop speaker Gil Livingston from the University College of London agreed with this point. She noted that types of elder abuse, whether occurring in the home or in institutions or to someone who is cognitively intact or not, are very different and there will not be a one-size-fits-all solution.
NEGLECT AND SELF-NEGLECT
Speaker and planning committee member Terry Fulmer from Northeastern University stressed that although neglect and self-neglect are often grouped with other forms of elder abuse, there is a need to consistently tease out what is neglect versus abuse because of the unique challenges associated with both neglect and self-neglect. Based on the data she has reviewed, Fulmer conservatively estimated that 4 percent of elders experience neglect; however, she suggested that, based on the difficulties associated with prevalence studies for elder neglect, the rate is likely much higher.
Rather than being defined by the infliction of injury and suffering, neglect is a failure to provide services necessary to maintain physical and mental health. According to the 2003 National Research Council (NRC) report Elder Mistreatment, neglect is defined as “an omission by responsible caregivers that constitutes ‘neglect’ under applicable federal or state law” (NRC, 2003, p. 39). The National Center on Elder Abuse defines neglect as “refusal or failure by those responsible to provide food, shelter, health care or protection for a vulnerable elder” (National Center on Elder Abuse, 2013).
Self-neglect was defined in the 2003 NRC report as “failure of individual to provide essential services for self as result of mental or physical inability” (NRC, 2003, p. 37). Workshop speaker Carmel Dyer from the University of Texas presented a model that she and her colleagues published in 2007 that demonstrates the risk factors for elder self-neglect. As shown in the model, self-neglect begins with neurodegenerative and mental health issues, and then executive dysfunction sets in, followed by impairment in activities of daily living. When coupled with inadequate support services due to lack of capacity for self-care and self-protection, or because of extrinsic issues like poverty access or lack of social support, self-neglect can result. Current research has provided an evidence base for the model.
Workshop speaker Kathleen Quinn from the National Adult Protective Services Association noted that issues of caregiver neglect are often complicated when a spouse is providing the care. For example, she suggested there are situations where a 100-pound, 80-year-old woman with osteoporosis is trying to care for her 175-pound husband who had a stroke. She does
not want to be separated from him, she wants to care for him, she does her best, but she cannot provide the care.
The question of an individual’s right to self-neglect was brought up by several speakers, acknowledging that the decision to self-neglect is related to the right to self-determination. Quinn noted that the Adult Protective Services (APS) code of ethics is based on self-determination, an adults’ right to make their own decisions and refuse intervention if they choose. However, she noted that the question always comes down to “Can they make those decisions?” and then “Who decides?”
Dong asked, “How do we determine the continuity of self-neglect and neglect? Because somebody is living by themselves? Their family is upstairs? At a point where do we determine there is a caregiving responsibility?” He suggested that within certain cultures, such as Chinese culture, there is an assumption of caregiving responsibility on family members regardless if they live in the same house or have moved away. Quinn responded that, in terms of APS, within the United States each state has different definitions for what constitutes neglect. In Illinois, where she worked, the definition is that once somebody undertakes care, they cannot stop providing care in an irresponsible manner. Dyer reported that, based on a survey of APS workers in Houston, they found that APS workers were differentiating between neglect and self-neglect based on whether someone else was living in the house because clinically there is little difference. Fulmer agreed, but stressed that for the purpose of building the evidence and moving the field forward, decisions on definitions need to be made rather than delaying the research.
CONCEPTUALIZING ELDER ABUSE
No overarching theory or conceptual framework exists for elder abuse, and workshop speakers debated the value in developing one and potentially “borrowing” concepts from existing theoretical frameworks.
Workshop speaker Pamela Teaster from the University of Kentucky presented several frameworks that have been applied to elder abuse or have the potential to be applicable to elder abuse; however, she acknowledged that each of them have deficits (see Table 2-1). Rather than suggesting a particular theory to be applied to elder abuse, Teaster proposed several overarching characteristics that any theoretical conceptualization of elder abuse should include transdisciplinarity, global context, community versus institutional setting, levels of cognitive impairment, balancing individual rights with safety, and inclusion of both upstream and downstream issues.
Greenlee suggested that part of the success in the work of domestic violence has been the critical support and training to include law enforcement. Elder abuse is a crime and whatever theoretical framework is developed, it needs to be translatable to law enforcement, prosecutors, and judges so that
TABLE 2-1 Conceptual Frameworks and Perspective on Their Applicability to Elder Abuse
|
|
|
| Framework | Perspective on Applicability to Elder Abuse |
|
|
|
| Ecological Model (Bronfenbrenner, 1979) |
• Originally conceptualized for children • Provides a multilevel, nested systems approach to considering the problem • Highlights the importance of “levels” or layers of thinking • Attaches responsibility/responsivity to micro through macrosystems • Systems are not intersecting, but rather nested • Difficult to measure or consider all of these when conducting research or designing interventions • Idea of time “Chronosystem” is difficult to apply |
| Sociocultural Model (NRC, 2003) |
• Specifically designed to explain elder mistreatment • Like the Ecological Model, considers a variety of contributors to mistreatment • Builds on elders in relationship with others • Considers dynamics of power, exchange, and inequality • Includes outcomes • Issue of the “trusted other” • Does not include self-neglect • Does not address “time” • Needs deeper consideration of characteristics of the abuser |
| Cycle of Violence Theory (Walker, 1979) |
• Derived from the domestic violence literature • Situational and short term • Easily comprehensible to laypersons • Not everyone who commits elder abuse was reared in a home in which violence took place • Could excuse the perpetrator from culpability • Inconsistent support for this theory |
| Lifecourse Perspective (Kuh and Ben-Shlomo, 1997) |
• Provides context for action and intervention • Multiple ways to apply • “Not a theory” conundrum • Misapplication of central tendency • Confounding social change and social forces • Neglects intercohort variability • Confuses time with change • Making choices becomes a “problem” |
|
|
|
SOURCE: Presented by Pamela Teaster, University of Kentucky.
it supports the understanding of elder abuse as a criminal activity. She also commented on the applicability of the public health model to elder abuse. Greenlee noted that as a lawyer by training and as a public servant, she has struggled with applying the public health structure and the categorization of primary, secondary, and tertiary prevention to elder abuse because of ageism. Articulating primary prevention for older people is very hard to do. She posited putting the model on its head with tertiary first and then secondary and then primary, because primary is such a struggle. Greenlee suggested that if a framework can be developed that achieves these objectives, of overcoming ageism and being inclusive of law enforcement, she could work with any structure that is developed.
Several workshop speakers noted the contagious nature of elder abuse, both within a setting and across the lifespan.1 Lachs spoke of cultures of violence and suggested that the ecological model, which considers factors at the individual, family, community, and societal levels and how they influence each other, could be a useful model for elder abuse. He added that the ecologic model of violence has been recognized as valid and highly suitable for developing intervention. Several speakers noted that many victims of elder abuse experienced other forms of violence earlier in life (Dong, 2013). Considering earlier exposures to violence, the lifecourse perspective could be a valuable framework for conceptualizing elder abuse. Workshop planning committee and Forum co-chair Jacquelyn Campbell suggested that some frameworks are useful for prevention by identifying risk factors, while others are useful for developing interventions.
ISSUES WITH PREVALENCE STUDIES
Livingston pointed out that the problem of knowing who to ask about elder abuse makes measuring difficult. Some researchers ask older adults themselves, while others rely on third-party assessments by family members or professionals, or data from APS or the police. Lachs raised the difficulty of getting prevalence estimates for neglect because through typical modes of collecting prevalence data—including screening in health care settings—individuals, particularly those with cognitive impairments, are largely excluded. He suggested a need for global mapping and novel high-risk methodology to get community-based prevalence estimates. Wallace stressed the need to look at multiple sources to get a better picture of what is going on in the community and suggested a need for multiple modes of
_____________________
1 For more information, see Dong, X. 2012. Elder abuse and the contagion of violence, Discussion Paper, Institute of Medicine, Washington, DC. http://iom.edu/Global/Perspectives/2012/ElderAbuse.aspx (accessed October 14, 2013).
data collection, as prevalence surveys by themselves are important but not sufficient.
Key Messages Raised by Individual Speakers
• There is a high prevalence of elder abuse in community-residing elders, primarily domestic violence (Acierno, Teaster).
• Conceptualizations and definitions of elder abuse need to be culturally relevant (Chang, Dong, Jervis, Mouton, Yan).
• The distinction between elder neglect and self-neglect often is not easy to determine and is defined differently by institutions and by communities (Dyer, Fulmer, Quinn).
• No overarching conceptual framework for elder abuse exists (Teaster).
REFERENCES
Acierno, R., M. A. Hernandez, A. B. Amstadter, H. S. Resnick, K. Steve, W. Muzzy, and D. G. Kilpatrick. 2010. Prevalence and correlates of emotional, physical, sexual, and financial abuse and potential neglect in the United States: The National Elder Mistreatment Study. American Journal of Public Health 100(2):292-297.
Bronfenbrenner, U. 1979. The ecology of human development: Experiments by nature and design. Cambridge, MA: Harvard University Press.
CDC (Centers for Disease Control and Prevention). 2013. Elder abuse: Definitions. http://www.cdc.gov/violenceprevention/elderabuse/definitions.html (accessed September 13, 2013).
Dong, X. 2013. The pine report. Chicago, IL: Rush Institute for Health Aging, Rush University Medical Center.
Kuh, D., and Y. Ben-Shlomo. 1997. A life course approach to chronic disease epidemiology. New York: Oxford Univeristy Press.
National Center on Elder Abuse. 2013. Types of abuse. http://www.ncea.aoa.gov/FAQ/Type_Abuse (accessed April 15, 2013).
NRC (National Research Council). 2003. Elder mistreatment: Abuse, neglect, and exploitation in an aging America. Washington, DC: The National Academies Press.
Walker, L. 1979. The battered woman. New York: Harper and Row.












