
3
Emerging Settings for Implementing Family-Focused Preventive Programs
One workshop panel was devoted to presentations on family-focused programs that are being implemented in settings that are emerging as important points of intervention, such as pediatric practices, schools, home visiting settings, and the Web. Such programs included
- Healthy Steps and Advanced Parenting Education in Pediatrics—which are being applied to pediatric care settings;
- Family Check-Up and Familias Unidas—which are being applied to school settings and through home visitation; and
- Autism Navigator®, Triple P Online, and Familias Unidas—which are being offered online.
Representatives from these programs at the workshop described the opportunities and challenges of applying family-focused programs in these settings. Their experiences may offer insights on strategies to successfully bring programs to scale.
Healthy Steps
Healthy Steps is an evidence-based program of primary health care for infants and young children initiated by the Commonwealth Fund in 1995. Healthy Steps focuses on promoting the emotional well-being of infants and young children and preventing mental health concerns. “The
goal was to infuse child development, trauma-informed care, and family support into primary care pediatrics,” said Margot Kaplan-Sanoff from Boston University and National Director of Healthy Steps. She also noted that the program builds on the principles and practices of others, including Strengthening Families, Bright Futures, Fussy Baby, and the American Academy of Pediatrics.
Healthy Steps enhances well-child care by adding a Healthy Steps Specialist to the pediatric practice team. This specialist has an advanced degree in nursing, child life, early childhood mental health, or social work, and provides the continuity of care for families between their scheduled well-child visits. Such continuity of care is especially important in residency-based clinics, where a child can see a different physician with every visit. In such cases, a Healthy Steps Specialist is available to help coordinate care, Kaplan-Sanoff pointed out.
The family sees both their personal Healthy Steps Specialist and their pediatrician at the same time during each well-child visit. The Specialist can also provide a bridge between clinic and home care by making home visits at times when there are predictable developmental concerns, such as at 6 to 9 months when the child’s mobility and separation anxiety increase, and between 15 and 24 months when the child is starting to talk. Additional optional home visits are also offered if needed. Kaplan-Sanoff emphasized, “Home visits are encouraged but optional because our goal is to make sure that parents know how to use primary care and it becomes their point of contact until they are connected to other services in the community.”
The Healthy Steps Specialist provides a number of services for families, including the following:
- Developmental screening for the child and a child development information phone line or texting;
- Screening for family risk factors, including domestic violence, substance abuse, maternal depression, and smoking, as well as protective factors, such as home safety checks;
- Linking and referring to community resources;
- Offering written materials emphasizing prevention;
- Offering parent support groups and educational programs; and
- Supporting early literacy with the Reach Out and Read program.
To become a Healthy Steps site, the practice hires the Healthy Steps Specialist, and the Specialist, pediatricians, residents, and the clinic manager all attend a Healthy Steps Institute training program as well as have a year of technical assistance follow-up. The sites are financially supported by private foundations, federal programs—such as the Health Resources and Services Administration’s Maternal, Infant, and Early Childhood Home
Visiting (MIECHV) program—and/or state funds. There currently are more than 70 Healthy Steps sites in the United States in a variety of settings, including hospital clinics, private practices, community health centers, and residency training programs. To expand further, Healthy Steps is partnering with various groups of professionals and paraprofessionals and offering training to serve as Healthy Steps Specialists for the families in their caseloads. These groups include public health nurses already making home visits in rural settings, doulas used by Native American tribes, and public health educators used in refugee camps.
Positive outcomes from the Healthy Steps program include parents having greater knowledge of infant development, better recognition of appropriate discipline, greater compliance with immunization schedules, and increased satisfaction with their pediatric care—as well as being less likely to disengage from it (Johnston et al., 2004; Minkovitz et al., 2003). A clinical trial of the Healthy Steps program incorporated developmental scientists and enhanced developmental services into pediatric settings during the first 3 years of life. Enrolled children were followed through age 5½, when computer-assisted telephone interviews were conducted with the children’s mothers. The study found sustained treatment effects on a range of outcomes, including that parents were more likely to report child behavioral issues to the clinician; more likely to receive anticipatory guidance; more likely to report children were reading and looking at books more; and less likely to use severe punishment (Minkovitz et al., 2007).
Advanced Parenting Education in Pediatrics
Advanced Parenting Education in Pediatrics (APEP) is a parent training intervention carried out in a network of 11 pediatric primary care offices serving an economically, ethnically, and educationally diverse population in the Boston, Massachusetts, area that is focused on preventing oppositional defiance disorder (ODD) or attention deficit and hyperactivity disorder (ADHD) in high-risk toddlers. As Ellen Perrin from Tufts Medical Center pointed out in her presentation, it is well known that toddlers with early disruptive behavior are at risk for developing ODD and ADHD later in childhood. If those children can be identified early, their behaviors are responsive to changes in parenting. Pediatrics is an ideal setting to provide an intervention aimed at improving the behavior of toddlers because pediatricians see children and families frequently, have a long-term supportive relationship with them, and focus on prevention in general, Perrin pointed out.
APEP developed a screening checklist for disruptive child behavior that parents fill out for their children attending 2- and 3-year well-child visits. The checklist was based on longitudinal data indicating early predictors of
such behavior. Children with the predictors were then eligible for sessions in a parent education group that takes place in their pediatricians’ practice settings. These educational sessions were based on The Incredible Years® (IY) curriculum and were co-led by practice staff trained in the program. This staff included nurses, nurse practitioners, social workers, pediatricians, and administrators.
An initial study of APEP found that only 41 percent of eligible parents agree to enroll in the program (Perrin et al., 2014). This low enrollment rate was probably due, in large part, to a rather burdensome research demand, Perrin noted. The controlled study documented a significant improvement in child and parent behavior 1 year after the educational intervention. Both participating parents and pediatricians responded favorably and enthusiastically to the program with almost all the parents wanting the groups to continue at the end of 10 weeks, and the pediatricians wanting to make the program a regular part of what their practices offered, Perrin reported. “This replicates findings that were found by others when these groups were done with parents of older children in a mental health setting,” Perrin concluded. “So what we found is that it is feasible to run parenting groups in pediatric practices. Parents are happy, pediatricians are happy, and space was rarely a problem. And pediatric staff with some mental health or nursing background and IY training can run the groups with fidelity,” she added.
The $10,000 start-up costs for the program were used to buy the appropriate IY materials and training for two leaders, but each session ended up costing only about $26 per family. Perrin added that even this modest cost after start-up was difficult to get reimbursed. In addition, most practices are not sufficiently big or have wide enough age ranges to have enough parents of 2- or 3-year-olds fill a group in a timely fashion. To counter this limitation, Perrin suggested making it available to eligible children between the ages of 2 and 6.
Opportunities and Challenges
Margot Kaplan-Sanoff described advantages to providing family-focused programs to promote children’s mental, emotional, and behavioral health within pediatric settings. She pointed out that pediatric primary care can be a powerful point of entry into services for families with infants and young children because it offers a window of opportunity for families to learn about their child and themselves as parents. Healthy Steps has enjoyed a high recruitment and retention rate in part because it was implemented in pediatric settings, Kaplan-Sanoff noted. Primary care is accessible being universal, affordable with new health insurance coverage, and offered around the clock with same-day care for sick children. Perhaps more im-
portantly, according to Kaplan-Sanoff, care given in a pediatric setting is nonstigmatizing because everyone with a child goes to a pediatrician or family doctor, not just those with problems. Healthy Steps does not require a referral, but instead is offered as standard of care for every family. Perrin concurred with Kaplan-Sanoff that an advantage of pediatric settings is that they are accessible and more inviting than stigmatizing.
Pediatricians have high credibility and, therefore, can be good agents for validating good parenting practices, Kaplan-Sanoff noted, as most parents tend to trust their pediatrician. Primary care is also a setting in which the well-being of both parents and children may be addressed, and one of the best ways to help children is to help their parents, she said. Now that modern medicine has done an effective job curing many of the ills of children, there is a new focus in pediatrics on developmental and behavioral concerns in which parents may play a significant role. In addition, the birth of a child can be a motivating factor for parents wanting to change behaviors, such as smoking or substance abuse, that affect not only their own health but the health of their children, she added.
But there are also unique challenges in delivering a program in a primary pediatric setting, including the lack of time busy practitioners have for training and office visits. Kaplan-Sanoff emphasized that the program should never get in the way of the flow of a practice. In the case of Healthy Steps, Kaplan-Sanoff noted that pediatricians tend to welcome the program because Healthy Steps Specialists (who may be nurses, social workers, or other types of nonphysician providers) are brought in as part of the care team, which helps to minimize burden on physicians. Providing a program in a medical setting can also pose confidentiality and privacy issues regulated by the Health Insurance Portability and Accountability Act (HIPAA). It can also be problematic if parents are with their child when they meet with the Healthy Steps Specialist and issues come up that need more private intensive discussion between just the Specialist and parent, Sanoff-Kaplan noted. You may have to identify another time to have those conversations, she said.
Dishion agreed that time is one of the biggest challenges in pediatric settings. “Physicians are incredibly busy and are not going to do extra work that they are not billing for, so even having them show up to meetings regarding planning an intervention is challenging,” he said. He added that another challenge is figuring out a billing niche for the services provided in a pediatric setting. “If you don’t have a clear niche, it’s not going to fly because people need to have a billing structure for it. That has to be worked out well in advance. So if we can solve the issue of billing, I think pediatrics is a fantastic setting,” he said.
Later during the discussion, David Hawkins from the University of Washington asked to what extent the American Academy of Pediatrics
(AAP) or other relevant organizations might help develop a business model for applying programs such as Healthy Steps and Family Check-Up in pediatric settings. He noted that pediatric practices that offer these programs should be more attractive to parents and might boost the number of patients in their practice. “It’s good for the practice and good for public health so if we could show a business model to pediatric practices that it is also good for business, we could quickly change how much of these programs are available in our country,” he said. Kaplan-Sanoff agreed and noted that Healthy Steps, when carried out correctly, can actually save physicians time and enable them to see more patients. “There are some practices that would say they are actually able to see more patients and take on a bigger caseload because of the Healthy Steps program,” she said.
Perrin added that the AAP and the American Academy of Child and Adolescent Psychiatry are currently interested in developing more team-based care, which would allow for more creativity in implementing family-focused interventions. Vera Frances Tait from AAP responded that from the AAP’s perspective, “We are always looking for models to make this work and for the business case to make a point both for getting the services that children and families need, but also for proper payment for what is provided, particularly for prevention but also for treatment.” She suggested one way to create and test those models is via Center for Medicare & Medicaid Innovation (CMMI) projects. CMMI projects are evaluated for their use of innovative payment and service delivery models to reduce program expenditures while preserving or enhancing the quality of care in Medicare, Medicaid, and the Children’s Health Insurance Program (CMS, 2014). But of more than 2,000 CMMI current projects, only 11 are focused in pediatrics, she said.
Tom Boat of the University of Cincinnati added that, from his perspective, time is not a major factor impeding pediatricians from applying family-focused programs in their practices, but rather a lack of training on this approach to helping families. “Pediatricians are not so busy that they will not do the right thing, but practitioners in medicine do what they were taught to do and I don’t think we are training pediatricians or nurses or social workers about these programs,” he said.
Dishion agreed and suggested that in addition to health care staff receiving the right training, national associations for school counselors, social workers, and other relevant professionals should have exposure to family-focused prevention programs as part of their training standards. “Training is key,” he said. Perrin added that recently pediatric training has started to include a small amount of training in developmental behavioral pediatrics and noted that side-by-side training was key to having nurse practitioners being used more in pediatric practices. “We need to develop training programs that include pediatricians, social workers, and psychologists that are
all learning side by side what it means to collaborate, because team-based care isn’t going to happen if the training happens in isolation. It will happen if we start putting those programs together.”
Kaplan-Sanoff agreed with Perrin and noted that Healthy Steps is already in a number of residency programs, and South Carolina just used their MIECHV funding to put Healthy Steps in all of their medical school settings. She pointed out that the residents who are exposed to Healthy Steps Specialists as part of their training tend to be more open to learning from them because, unlike their attending physicians, they are not evaluating the residents. “Our residents know much more about mental health because they have seen it naturally infused as part and parcel of the well-child visit,” she said.
Family Check-Up
Family Check-Up (FCU) is a preventive program to help parents address typical challenges that arise with children and adolescents before these challenges become more serious or problematic. The program focuses on high-risk families, where normal challenges are more likely to lead to unfavorable outcomes, such as child conduct problems. FCU uses a parent consultant trained in the program model to meet with families in their homes to assess their family–child dynamics. After that assessment, the consultant provides a feedback session with the parents that uses motivational interviewing principles aimed at evoking change talk in the parent. Following the feedback session, families are provided the right type and amount of intervention based on their need.
Some families receive brief tailored parent management training (PMT) that encourages supporting positive behavior in the child, setting healthy limits, and building family relationships. Others may be linked to community treatment resources or the children may undergo cognitive behavioral therapy. “We try to link them to the right resources for the right conditions,” Dishion said, and gave the example of a single mom of three children, who is in recovery from a drug addiction. She might be given recovery support and a relief nursery, where support is provided for her children, in addition to some parent training. “It’s unrealistic to think a brief parent training model is going to be enough for this particular family,” he said.
Several studies showed that when FCU was applied to families participating in the Women, Infants, and Children (WIC) program and in preschools, it reduced problem behavior in children, maternal and child depression, and parents’ use of a coercive parenting style, while it improved children’s school readiness, and parents supporting positive behavior in
their children (Chang et al., 2014; Connell et al., 2008; Dishion et al., 2008, 2014; Shaw et al., 2006, 2009; Smith et al., 2013). Some of these effects lasted at least 5 years. Dishion pointed out that the intervention also reduced parental coercion, but only when the parent consultant gave videotape feedback on their parenting style. Seventy percent of eligible families participated in FCU.
After initial studies indicated the effectiveness of FCU, Dishion and his colleagues started applying the program in public school settings to families with children aged 11 to 19. Long-term behavioral outcomes were gained in this new setting, including reduced antisocial behavior, early drug use, drug abuse, and high-risk sexual behavior. It also reduced depression rates in children and improved parent monitoring of child behavior, conflict in families, and it improved the children’s grades and attendance in high school (Brennan et al., 2013; Caruthers et al., 2014; Connell et al., 2006; Dishion et al., 2002, 2003; Fosco et al., 2014; Stormshak et al., 2010; Van Ryzin and Dishion, 2012; Van Ryzin et al., 2012; Véronneau and Dishion, 2012). One-quarter to one-half of eligible families participated in public school setting FCU.
The FCU team then decided to scale-up the program and apply it to more settings. To do such scale-up, they developed a systemic implementation model (see Figure 3-1). To apply FCU broadly in a home visiting setting for preschoolers, in public schools, and in pediatric settings, the intervention was trimmed to make it more cost and time effective. Assessments were shortened to a half-hour and had Web-based supports, including videotaped sessions with therapists that were uploaded onto a confidential portal. The program was also translated into Spanish. In addition, a brief proactive screening was added to the pediatric program that identified families that needed more support.
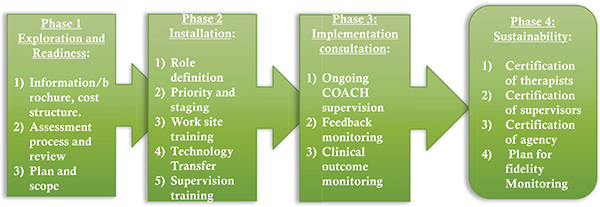
FIGURE 3-1 Overview of Family Check-Up team’s systemic implementation model.
SOURCE: Dishion, 2014.
Researchers are currently implementing FCU’s home visiting program for early childhood in the state of South Carolina, its pediatric version in Phoenix Children’s Hospital, and its school-based program in 42 schools, including about 25 schools in Oregon and 6 schools in Sweden. Three other states have also started applying FCU in their public schools.
Familias Unidas
This prevention program for Hispanic youth aims to prevent and reduce problem behaviors by increasing family functioning and parental monitoring of peer and school activities. It is delivered through family-centered, multi-parent sessions that teach parent and adolescent communication, positive parenting, and parental monitoring of peers. The program tries to place parents in the change agent role in the family, Guillermo Prado from the University of Miami School of Medicine reported. There also is an opportunity for the parent to practice some of the skills they have learned with their adolescents in school settings as well as in the home setting via a more limited set of family home visits.
Studies show Familias Unidas is effective in preventing and reducing a wide array of problem behaviors. It fosters a 40 percent reduction in drug use, a 60 percent increase in condom use, and a 50 percent reduction in alcohol use at the cost of approximately $200 per family (Prado et al., 2007, 2012a,b). Familias Unidas has traditionally been offered in school settings, but is launching a pilot study in four different clinics, including academic centers, pediatric clinics, and community clinics.
Opportunities and Challenges
One of the biggest challenges in implementing FCU in school settings is having enough time allocated to it, according to Dishion. Another challenge has been administrative turnover. “A school adopts FCU and then the principal leaves and there’s no champion of your program at the school level,” he said. But when there is a champion, schools are an excellent setting for delivery of the program, he added. Prado noted that the Patient Protection and Affordable Care Act offers new opportunities to integrating family-centered, evidence-based preventive interventions, such as Familias Unidas, within health care settings. The challenge is to make the programs minimally disruptive and not interfering with physicians’ time in these settings, he added. To increase its reach and sustainability, Familias Unidas has also recently developed and tested an online version of its program (see Online Programs section on next page).
In order to make their family-focused programs more widespread and to help contain costs, some developers have created online versions of them, including Familias Unidas, Autism Navigator®, and the Triple P-Positive Parenting Program. Other programs, such as FCU, use online support for their training and educational sessions.
Familias Unidas Online
Familias Unidas online can be accessed from a variety of electronic devices, including computers, tablets, and smartphones. The online program gives the same number of behavioral sessions as the standard program, but these sessions are comprised of mock groups that are videotaped with a trained interventionist, as well as culturally compatible telenovelas or soap operas. At the end of each session there is a cliff-hanger that makes the participants want to come back, Prado reported.
The online program also offers parents the opportunity to interact with optional interactive exercises “so they feel they are a part of the process, which is something that is so central to our family-based intervention program,” Prado said. Family visits are done online via a setup similar to what Skype offers only with more privacy protections.
In a pilot study of the online version, all 16 parents in a focus group reported they enjoyed watching the intervention and found it entertaining. Parents felt that the intervention helped them better communicate with their adolescents, and about 95 percent claimed they identified with the characters and the situations in the mock group and telenovelas.
Autism Navigator®
Amy Wetherby and colleagues of the Florida State University College of Medicine developed the online program Autism Navigator® to meet the compelling need to provide early home-based autism interventions to the growing number of children being diagnosed with the condition. Many studies by Wetherby and others show autism can be detected as early as 16 to 20 months in children, and that interventions have the greatest impact if they start before 3 years of age, when they can help foster optimal development of the child’s social communication, language, and behavior. But most children are not diagnosed with autism until they enter school. At this time, interventions for children with autism as well as other developmental disabilities are less likely to be effective because it is difficult for children to catch up on low reading and language trajectories. Wetherby noted that a child’s rate of language acquisition is solidified and their learning trajec-
tories already formed by 2 to 3 years of age for language learning, which is positively correlated with IQ (Hart and Risley, 2003; Walker et al., 1994).
Wetherby pointed out that time-intensive (25 hours per week) interventions are often needed for children with autism. This requires supporting caregivers to apply these strategies in everyday activities before the child enters preschool. “We need to improve early detection as well as access to early intervention,” Wetherby emphasized. “Eighty percent of children with developmental delays who will need early intervention and be eligible for special education services when they get to school age are missed and don’t even get identified or receive early intervention,” she added (see U.S. Department of Education, 2012).
Recognizing this, Wetherby and her team developed Autism Navigator®, a Web-based instructional system to aid the early identification and intervention of children with autism and with communication delays. This system has tiered supports and services, including a self-guided digital family tool. Videos embedded in the system show how to identify the early signs of autism and communication delays in the behavior of babies and toddlers. Those signs include delays in ability to share attention and interest, rate of and reason for communicating, developmentally normal inventory of gestures, sounds, play actions, and understanding words and book knowledge (see Figure 3-2) (Caselli et al., 2012; Watt et al., 2006; Wetherby et al.,
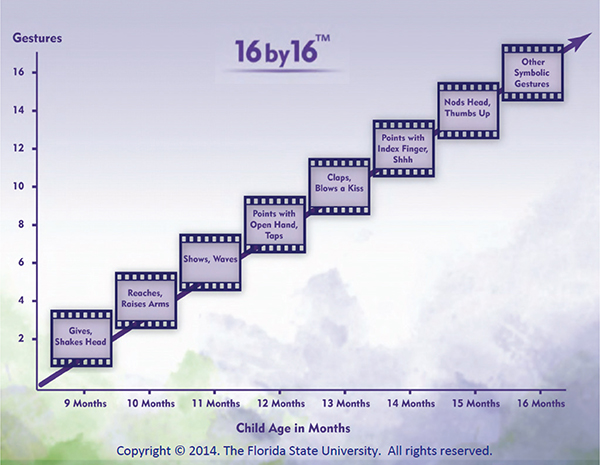
FIGURE 3-2 16 by 16: Gestures commonly observed in children, by age in months. SOURCE: Wetherby, 2014. Copyright 2014 by Florida State University. All rights reserved. Reprinted with permission.
2003, 2007). For example, gestures that develop between the ages of 9 to 16 months, such as reaching out with arms, showing, pointing, or waving, predict language 1-2 years later and, therefore, may inform early detection.
If a child has a communication delay, the system offers families a self-guided digital tool with social communication growth charts for children 9 to 24 months of age with tips to support development. If a child is also positively identified as having autism, the system will provide information about the importance of early intervention as well as an online guide for parents that will suggest evidence-based strategies they can use to foster their child’s normal language and behavioral development. Autism Navigator® also has an electronic monitoring system that will enable monthly check-ins through text, phone, or other means, so providers can stay in touch with families using it to help treat their children with autism.
Two courses of Autism Navigator® have been developed. One is for primary care physicians and the other is for early interventionists. Future versions are planned for kindergarten classrooms, Head Start, and other preschool education or child care programs. Autism Navigator® also provides online tools for the public (see Figure 3-3). Wetherby pointed out that because Autism Navigator® relies heavily on embedding interventional strategies in everyday activities, such as caregiving, meals, family chores, or

FIGURE 3-3 Autism Navigator®: Free tools for the public.
SOURCE: Wetherby, 2014.
going to the store, its screening and intervention procedures can be adapted to the everyday activities unique to other cultures. Her team was able to successfully apply the model to the KwaZulu Natal region of South Africa, for example.
Triple P Online
Triple P Online is a comprehensive, eight-module Web-based program that guides parents through Triple P’s core parenting skills (see Chapter 2 for a description of Triple P). Based on Level 4 Standard Triple P, it includes opt-in SMS or email reminders of session goals and strategies (Triple P, 2013). Prinz reported that the Child Protective Services system in Los Angeles County is using the online version of Triple P with the parents in their program.
Opportunities and Challenges
The future of family-focused preventative interventions will include eHealth (delivered via computers) and mHealth (delivered via smartphones or tablets), said Prado. Technology offers a lot of opportunity for increasing the reach of evidence-based programs, although this needs to be balanced with program efficacy. Maximized sustainability is another benefit of online interventions, he said.
The biggest challenges to overcome with online interventions will be engagement and retention. In the pilot study discussed above, Familias Unidas had remarkable engagement and retention for an online program, with 83 percent attending all five sessions that have been given online so far. Seventy-eight percent of families completed family visits online. “All the families that we were able to engage have been retained in the intervention,” Prado said.
During discussion, Bowen noted that many low-income families do not have good access to Web-based programs. Often they do not have computers at home, he said, and even if they have smartphones, they may only be able to use them for a few days until their minutes run out. He also questioned whether online programs such as Autism Navigator® can reach and be effective for parents who are depressed and therefore not likely to engage with their children.
Wetherby responded that some parents’ depression could be child-driven due to the child’s autism or communication delay so the intervention offers a way out of their depression or a way of preventing it. She added that the online tools provided by Autism Navigator® can be used by providers who make home visits to low-income families or families who are at risk. “The technology can train very cost-efficiently the home visitor work-
force that we have for families at risk, so the technology is not only for the families,” she said. She also suggested using funding to make the technology available at home for those low-income families who need it. “Think of the technology as nutrition for our children,” she said.
Brennan, L. M., E. C. Shelleby, D. S. Shaw, F. Gardner, T. J. Dishion, and M. Wilson. 2013. Indirect effects of the Family Check-Up on school-age academic achievement through improvements in parenting in early childhood. Journal of Educational Psychology 105(3):762-773.
Caruthers, A. S., M. J. Van Ryzin, and T. J. Dishion. 2014. Preventing high-risk sexual behavior in early adulthood with family interventions in adolescence: Outcomes and developmental processes. Prevention Science 15(Suppl 1):S59-S69.
Caselli, M. C., P. Rinaldi, S. Stefanini, and V. Volterra. 2012. Early action and gesture “vocabulary” and its relation with word comprehension and production. Child Development 83(2):526-542.
Chang, H., D. S. Shaw, T. J. Dishion, F. Gardner, and M. N. Wilson. 2014. Direct and indirect effects of the Family Check-Up on self-regulation from toddlerhood to early school-age. Journal of Abnormal Child Psychology [Epub ahead of print].
CMS (Centers for Medicare & Medicaid Services). 2014. About the CMS Innovation Center. http://innovation.cms.gov/About/index.html (accessed June 7, 2014).
Connell, A. M., T. J. Dishion, and K. D. Deater-Deckard. 2006. Variable- and person-centered approaches to the analysis of early adolescent substance use: Linking peer, family and intervention effects with developmental trajectories. Merrill-Palmer Quarterly 52(3):421-448.
Connell, A., B. M. Bullock, T. J. Dishion, D. Shaw, M. Wilson, and F. Gardner. 2008. Family intervention effects on co-occurring early childhood behavioral and emotional problems: A latent transition analysis approach. Journal of Abnormal Child Psychology 36(8):1211-1225.
Dishion, T. 2014. The Family Check-Up model: An evidence-based approach to promoting child and adolescent behavioral health. Presentation at the workshop on Strategies for Scaling Tested and Effective Family-Focused Preventive Interventions to Promote Children’s Cognitive, Affective, and Behavioral Health, Washington, DC.
Dishion, T. J., K. Kavanagh, A. Schneiger, S. Nelson, and N. K. Kaufman. 2002. Preventing early adolescent substance use: A family-centered strategy for the public middle school. Prevention Science 3(3):191-201.
Dishion, T. J., S. E. Nelson, and K. Kavanagh. 2003. The Family Check-Up with high-risk young adolescents: Preventing early-onset substance use by parent monitoring. Behavior Therapy 34(4):553-571.
Dishion, T. J., D. Shaw, A. Connell, F. Gardner, C. Weaver, and M. Wilson. 2008. The Family Check-Up with high-risk indigent families: Preventing problem behavior by increasing parents’ positive behavior support in early childhood. Child Development 79(5):1395-1414.
Dishion, T. J., L. M. Brennan, D. S. Shaw, A. D. McEachern, M. N. Wilson, and B. Jo. 2014. Prevention of problem behavior through annual family check-ups in early childhood: Intervention effects from home to early elementary school. Journal of Abnormal Child Psychology 42(3):343-354.
Fosco, G. M., M. Van Ryzin, E. A. Stormshak, and T. J. Dishion. 2014. Putting theory to the test: Examining family context, caregiver motivation, and conflict in the Family CheckUp model. Developmental Psychopathology 26(2):305-318.
Hart, B., and T. R. Risley. 2003. The early catastrophe: The 30 million word gap by age 3. Education Review 17(1):4-9.
Johnston, B. D., C. E. Huebner, L. T. Tyll, W. E. Barlow, and R. S. Thompson. 2004. Expanding developmental and behavioral services for newborns in primary care: Effects on parental well-being, practice, and satisfaction. American Journal of Preventive Medicine 26(4):356-366.
Minkovitz, C. S., N. Hughart, D. Strobino, D. Scharfstein, H. Grason, W. Hou, T. Miller, D. Bishai, M. Augustyn, K. T. McLearn, and B. Guyer. 2003. A practice-based intervention to enhance quality of care in the first 3 years of life: The Healthy Steps for Young Children Program. JAMA 290(23):3081-3091.
Minkovitz, C. S., D. Strobino, K. P. Mistry, D. O. Scharfstein, H. Grason, W. Hou, N. Ialongo, and B. Guyer. 2007. Healthy Steps for Young Children: Sustained results at 5½ years. Pediatrics 120(3):e658-e668.
Perrin, E. C., R. C. Sheldrick, J. M. McMenamy, B. S. Henson, and A. S. Carter. 2014. Improving parenting skills for families of young children in pediatric settings: A randomized clinical trial. JAMA Pediatrics 68(1):16-24.
Prado, G., H. Pantin, E. Briones, S. J. Schwartz, D. Feaster, S. Huang, S. Sullivan, M. I. Tapia, E. Sabillon, B. Lopez, and J. Szapocznik. 2007. A randomized controlled trial of a parent-centered intervention in preventing substance use and HIV risk behaviors in Hispanic adolescents. Journal of Consulting and Clinical Psychology 75(6):914-926.
Prado, G., H. Pantin, S. Huang, D. Cordova, M. I. Tapia, M. Velazquez, M. Calfee, S. Malcolm, M. Arzon, J. Villamar, G. L. Jiminez, N. Cano, C. H. Brown, and Y. Estrada. 2012a. Effects of a family intervention in reducing HIV risk behaviors among high-risk Hispanic adolescents: A randomized controlled trial. Archives of Pediatric & Adolescent Medicine 166(2):127-133.
Prado, G., D. Cordova, S. Huang, Y. Estrada, A. Rosen, G. A. Bacio, L. Jiminez, H. Pantin, C. H. Brown, M. R. Valazquez, J. Villamar, D. Freitas, M. I. Tapia, and K. McCollister. 2012b. The efficacy of Familias Unidas on drug and alcohol outcomes for Hispanic delinquent youth: Main effects and interaction effects by parental stress and support. Drug and Alcohol Dependence 125(Suppl 1):S18-S25.
Shaw, D. S., T. J. Dishion, L. Supplee, F. Gardner, and K. Arnds. 2006. Randomized trial of a family-centered approach to prevention of early conduct problems: 2-year effects of the family check-up in early childhood. Journal of Consulting and Clinical Psychology 74(1):1-9.
Shaw, D. S., A. Connell, T. J. Dishion, M. N. Wilson, and F. Gardner. 2009. Improvements in maternal depression as a mediator of intervention effects on early childhood problem behavior. Developmental Psychopathology 21(2):417-439.
Smith, J. D., T. J. Dishion, D. S. Shaw, and M. N. Wilson. 2013. Indirect effects of fidelity to the family check-up on changes in parenting and early childhood problem behaviors. Journal of Consulting and Clinical Psychology 81(6):962-974.
Stormshak, E. A., G. M. Fosco, and T. J. Dishion. 2010. Implementing interventions with families in schools to increase youth school engagement: The Family Check-Up model. School Mental Health 2(2):82-92.
Triple P. 2013. Triple P goes online. http://helpingfamilieschange.org/wp-content/uploads/2013/03/Turner-HFCC-2013-Online-Triple-P-Workshop.pdf (accessed June 5, 2014).
U.S. Department of Education. 2012. The 31st Annual Report to Congress on the Implementation of the Individuals with Disabilities Education Act. Washington, DC: U.S. Department of Education.
Van Ryzin, M. J., and T. J. Dishion. 2012. The impact of a family-centered intervention on the ecology of adolescent antisocial behavior: Modeling developmental sequelae and trajectories during adolescence. Development and Psychopathology 24:1139-1155.
Van Ryzin, M. J., E. A. Stormshak, and T. J. Dishion. 2012. Engaging parents in the Family Check-Up in middle schools: Longitudinal effects through the transition to high school. Journal of Adolescent Health 50(6):627-633.
Véronneau, M. H., and T. J. Dishion. 2010. Predicting change in early adolescent problem behavior in the middle school years: A mesosystemic perspective on parenting and peer experiences. Journal of Abnormal Child Psychology 38(8):1125-1137.
Walker, D., C. Greenwood, B. Hart, and J. Carta. 1994. Prediction of school outcomes based on early language production and socioeconomic factors. Child Development 65(2):606-621.
Watt, N., A. Wetherby, and S. Shumway. 2006. Prelinguistic predictors of language outcome at three years of age. Journal of Speech, Language, and Hearing Research 49(6):1224-1237.
Wetherby, A. 2014. Engaging families of children with developmental disabilities in early detection, early intervention, and prevention. Presentation at the workshop on Strategies for Scaling Tested and Effective Family-Focused Preventive Interventions to Promote Children’s Cognitive, Affective, and Behavioral Health, Washington, DC.
Wetherby, A., H. Goldstein, J. Cleary, L. Allen, and K. Kublin. 2003. Early identification of children with communication delays: Concurrent and predictive validity of the CSBS Developmental Profile. Infants & Young Children 16(2):161-174.
Wetherby, A. M., N. Watt, L. Morgan, and S. Shumway. 2007. Social communication profiles of children with autism spectrum disorders late in the second year of life. Journal of Autism and Developmental Disorders 37(5):960-975.
















