
5
Approaches to Developing
Improved Discharge Instructions
The workshop’s final panel featured two presentations on two very specific approaches to providing discharge instructions. Michael Paasche-Orlow, associate professor of medicine at the Boston University School of Medicine, discussed Project RED (Re-Engineered Discharge), a nationally recognized model for reengineering the hospital discharge process to improve the safety and efficiency of transitions of care. Charles Lee, president and founder of Polyglot Systems, Inc., spoke about the values and challenges associated with preparing discharge instructions for patients with limited proficiency in English.
PROJECT RED: REENGINEERING THE DISCHARGE PROCESS1
In his initial comment to the workshop, Michael Paasche-Orlow noted that the issues that had been discussed are relevant to all transitions in the clinical setting when information is being exchanged between a health care provider and a patient. “I hope that as people learn and touch different parts of this elephant, we can share information and really expand together,” he said.
Turning to the subject of his presentation, Project RED, Paasche-Orlow began by describing the series of activities that he and his colleagues went through to develop 11 mutually reinforcing components for discharge
_______________
1This section is based on the presentation by Michael Paasche-Orlow, associate professor of medicine, Boston University School of Medicine, and the statements are not endorsed or verified by the IOM.
instructions that formed a RED Checklist. This checklist, which has been adopted by the National Quality Forum as 1 of the 30 “safe practices,” includes the following components:
- Make appointments for follow-up care.
- Plan for the follow-up of results from pending tests.
- Organize postdischarge services and equipment.
- Identify the correct medicines and plan for patient to obtain those medications.
- Reconcile the discharge plan with national guidelines.
- Teach a written discharge plan the patient can understand.
- Educate the patient about diagnoses and medicines.
- Assess the degree of the patient’s understanding of the plan.
- Expedite transmission of the discharge summary to the primary care physician.
- Provide telephone reinforcement.
- Review appropriate steps for what to do if a problem arises.
After an evaluation and testing phase, including a project to evaluate and expand their thinking about culture competence in the context of Project RED, Paasche-Orlow and his colleagues added a 12th component, which was to ascertain the need for and obtain language assistance.
One challenge that he sees in creating written discharge instructions is dealing with the fact that they are out of date almost from the moment they are created. For example, the discharge instructions may include medication that the patient needs to get after discharge, but perhaps the patient cannot get to the pharmacy to get the prescriptions filled. What happens then? “These things have to be live documents that should be electronically available anywhere the patient goes, on any device,” Paasche-Orlow said. “It is crazy that we are not there already.”
Rather than thinking of them as a form or a piece of paper, discharge instructions should be viewed as a process that represents a significant cultural shift that, in many organizations, takes work to accomplish. The challenge, he explained, is conveying to an organization’s staff that management cares about the work they do with their patients not only when they are within the health care setting but also when they leave. “This is a different type of focus,” said Paasche-Orlow, one that goes from “who is taking the next admission” to a perspective that says, “I value the work that you do in preparation for your patient to go home and succeed.”
As had been mentioned earlier during the workshop, the electronic systems for producing discharge instructions depend on the quality of the data in EHRs, and it is well known that EHRs are full of bad data. For example, a patient’s medication list is often used by the health care provider as a
memory tool to remind him or her that the patient took an antibiotic for an infection 5 years ago. In most systems, though, that outdated information gets dumped in its entirety into the discharge instructions for the simple reason that the medication list in the EHR was not designed to be used to populate a discharge instruction form. Unless someone takes the time to go over the discharge instructions before the health care provider hands those instructions to the patient, and unless the health care provider takes time to review the discharge instructions before talking to the patient about them, the opportunity is ripe for the patient to receive something with little value and for the health care provider to be embarrassed.
Thinking of the care plan as a process instead of a form allows the health care provider to think about every document that goes to the patient in terms of how that document meets an educational agenda, explained Paasche-Orlow. It is important that the health care provider think about how a document will be empowering and activating for a patient and what educational process is required to support that document. Health care systems need to think about what training is necessary for staff and what supervision and monitoring processes are going to be needed for this process to take place. “This really requires that we regard all of the people working in our institutions in a pedagogic role,” said Paasche-Orlow.
One of the lessons he and his colleagues learned during the testing and evaluation phase of Project RED was that it is critical to ferret out jargon. For example, everyone on a patient’s care team knows what a discharge plan is, but patients relate better when it is called a care plan. Another lesson, Paasche-Orlow said, was the need for a new position, the nurse discharge advocate, who takes responsibility for interacting with the care team, reconciling the medication list, scheduling appointments, facilitating the checklist, and ensuring that the care plan meets national guidelines. The nurse discharge advocate also teaches the care plan and makes sure that the patient understands the details of the plan. The nurse discharge advocate’s role is reinforced by the pharmacy staff, a member of whom makes a follow-up phone call 72 hours after discharge that reinforces the care plan and reviews medications.
Following medication instructions is often one of the biggest challenges for newly discharged patients, and the Project RED care plan goes to great lengths to present medication information as clearly as possible. The medication section of the RED care plan breaks down patients’ medications according to the time of day they need to take a particular prescription and uses a graphically simple chart format that tells patients why they are taking a specific drug and how many pills to take at each time of the day (see Figure 5-1). The section that lists patients’ upcoming appointments also makes use of a simple color-coded chart format that is organized by date and includes the health care provider’s contact information, location, and
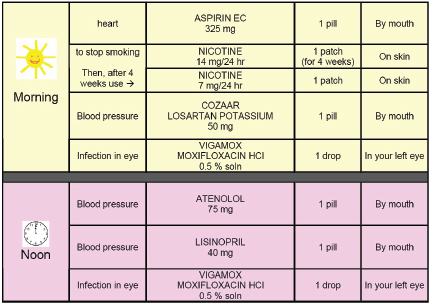
FIGURE 5-1 Patient medication schedule.
SOURCE: As presented by Paasche-Orlow, 2014.
the reason for the visit. This section is followed by one in which patients can develop an agenda and write down questions for each health care provider at these future appointments.
In his closing remarks, Paasche-Orlow briefly reviewed the results of a randomized controlled trial that he and his colleagues ran to test whether the RED intervention was any better than usual care. The data from this randomized controlled trial of 749 patients showed marked improvements, with a 33 percent reduction in the number of emergency visits and readmissions in the group that received the RED intervention.
DISCHARGE INSTRUCTIONS: PATIENT VALUES AND CHALLENGES2
The mission of Polyglot Systems is to develop practical, affordable multi-language technology solutions to improve access to health care and reduce disparities for underserved patients and those with limited profi-
_______________
2This section is based on the presentation by Charles Lee, president and founder of Polyglot Systems, Inc., and the statements are not endorsed or verified by the IOM.
ciency in English. “What we are trying to do is to develop technology-based, scalable solutions to simplify instructions for patients to reduce common avoidable mistakes. The communication areas we currently focus on include reducing medication errors, improving medication adherence, and effective transitions of care,” explained Charles Lee, who founded the company in 2001.
His approach is to consider health literacy as a personal skill for gathering, understanding, and then acting on appropriate health information. He mitigates people’s low health literacy by consolidating relevant information in a way that enables them to focus on key messages, and by removing clutter and reducing noise. Improving understanding requires getting the reading level to one that is appropriate for most patients and using each patient’s preferred language. “Why are we gathering a patient’s language preference if we are not going to give them instructions in that language?” he asked. Improving understanding also requires the use of visual aids to reinforce written concepts and the use of font sizes that the elderly and visually impaired can actually read. Lee agreed with Paasche-Orlow that patient discharge is a process, not just a form, and it is essential then that the discharge instructions include specific actionable items presented in a way that is both personalized and encourages dialogue with the health care provider.
As illustrations of how Polyglot Systems is tackling these problems, Lee discussed three examples of the company’s work. The medication summary (see Figure 5-2) is organized by time of day in an easy-to-read chart format. The summary that Lee presented was written in Spanish, but the Polyglot system is currently capable of generating the summary in 19 different languages. The summaries contain QR codes that the patient can scan to view video demonstrations, narrated in the patient’s language, of complex medications. In the example Lee presented, scanning the QR code took the patient to a website that demonstrated in Spanish how to use a prescribed inhaler. A pilot study of this “Meducation calendar” showed that it reduced medication nonadherence by 56 percent over the first 90 days, compared to a baseline measurement taken prior to using this module (Zullig et al., 2014).
The second example Lee discussed addresses medication safety (see Figure 5-3), and it represents an attempt to take the consumer medication information sheet, which is typically written at a 12th–14th grade reading level and in 6-point font and turn it into something that a patient would read rather than throw away. The result of this project is a medication instruction sheet that is written at a 5th–8th grade reading level and that uses pictograms and other readability tools. These sheets can be generated in one of three font sizes for patients with visual impairments. Each sheet contains a bar code that the user can use at Meducation’s free Internet
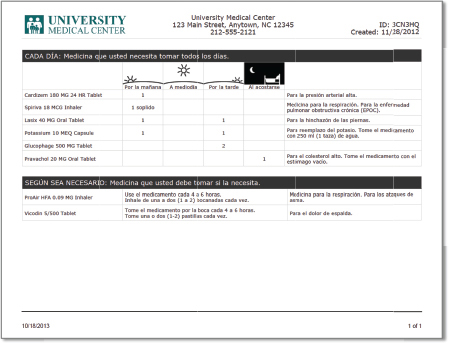
FIGURE 5-2 Medication summary.
SOURCE: Polyglot as presented by Lee, 2014.
portal to view in any of the 19 available languages. “If you receive this in Chinese, but I am the caregiver and prefer to read it in English, I can go to the Web portal and download a copy in English,” explained Lee. The Web portal also includes demonstrations of how to take complex medications. A pilot test of this tool by the University of Connecticut’s John Dempsey Hospital showed that it increased Hospital Consumer Assessment of Healthcare Providers and Systems scores on three medication education measures from the 1st/1st/4th percentiles to the 85th/98th/52nd percentiles.
Lee’s final example described a solution for creating customized discharge instructions using a template-based format. This tool allows the health care provider to select a condition, which then populates the system with a list of associated instructions, personalize the instructions available through dropdown menus to make the instructions relevant to the patient, and then print the instructions in English or the patient’s preferred language. A pilot study involving 94 bilingual patients found that these discharge instructions were considered the best among all the models from the 18 participating sites. One interesting finding from this small pilot
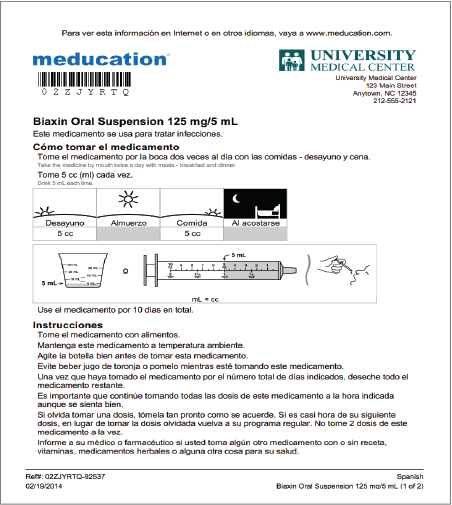
FIGURE 5-3 Medication safety.
SOURCE: Polyglot as presented by Lee.
study was that patients and physicians both preferred by a large margin a format that included both English and the second language in a dual-column format. Physicians preferred the dual-column format because they did not like handing out materials they could not read themselves. Patients preferred the dual-column format because it enabled other English speakers in their household to be able to read the instructions. When asked, patients who received the Meducation discharge instructions described the
organizations that used them as caring, considerate, excellent, helpful, professional, responsible, and thoughtful. “The vast majority of patients felt that by receiving these types of documents, they were not being left alone, which is how they often feel when they get sent home from the hospital,” said Lee.
He noted that one of the challenges to creating these types of documents is that they need to accommodate both science and art. The science part includes research-based best practices, such as the use of the Universal Medication Schedules; appropriate grade reading level; layouts that are visually pleasing and easy to read; and reinforcements of educational messages. The art part has to do with the intangibles—the key points that need to be included for a specific patient and the presentation for that particular patient given his or her cultural and language background. “You have to be careful how you represent different concepts for patients,” said Lee. “For example, how do you represent food? Is it a sandwich, a pizza, or a bowl of rice? That depends on the patient’s background.”
Another challenge is to sell health literacy to EHR vendors who today are preoccupied with meaningful use certification. “They don’t view health literacy as a high priority,” said Lee, who added that EHR vendors have reported to him that the market is not asking for these types of products. “That is something we have to work on,” he said. There are some positive indicators, though, Lee noted, particularly associated with accountable care organizations and patient-centered medical homes that receive payments on the basis of health outcomes. A key to making inroads, he added, is that these types of tools will have to be integrated into the current workflow. “We need to promote an environment of sharing and sustaining these types of tools and to develop plug-and-play interoperability that makes integrating these types of low-literacy tools easier,” said Lee. He added in closing that “we need to stop hoping that patients are going to figure this out by themselves and give them instructions that will get them engaged—instructions that they can actually read, understand, and then act on.”
During the ensuing discussion, Cindy Brach asked Lee if he had any ideas on how to overcome the market forces that seem to be stymieing adoption of tools for creating better discharge instructions. Lee said that pharmacies might be a good target given that they deal directly with consumers. Paasche-Orlow added that patient satisfaction could be an important lever given that 30 percent of a value-based purchasing score will be based on satisfaction scores. He agreed that pharmacies could be a good leverage point. It was noted that it would be a good idea to bring Walgreens and CVS to a future roundtable workshop.
George Isham said he appreciated the medication instruction sheet with the four-times-a-day regimen for taking medicines. But, he asked, what happens when medications change? How can this medication sheet become a living tool? Also, is there any integration of these instructions with how patients or their family members actually manage the counting out of tablets for each period? Paasche-Orlow responded that a number of issues are involved in trying to turn this into a living tool. For example, the data have to be able to flow and to go to all of a patient’s providers. Another problem is that because patients have to pay different out-of-pocket amounts for medications, depending on their insurance coverage, some of them may not fill the prescriptions because of cost. Although there are great difficulties with relying too heavily on information technology, that is how we are going to be able to address these issues, he said.
Benard Dreyer asked Paasche-Orlow what was known about which of the listed 12 steps for reinforcing components for discharge instructions were most important. Paasche-Orlow said the answer is unknown because they did not have a way to differentiate the relative effects of the different components. There is a change in the length of the process, moving from an 8-minute-per-discharge conversation with patients to 45 to 50 minutes of conversation, education, and confirmation of comprehension. And, he said, the follow-up telephone call appears important because about half the time even those individuals who received the full intervention still had something related to medication that needed to be dealt with in the call. It is interesting to note, he said, that about 30 percent of the prescriptions written were still not filled at the time of the follow-up call, a number that shows that there is great need for improvement.
Wilma Alvarado-Little asked Lee what thoughts or ideas he has about adding languages, even languages with less diffusion, as the demographics of the United States change. Lee responded that the development of forms in different languages is market driven. Those with limited English proficiency are the ones first focused on. For example, there are many German speakers in the United States, but they tend to speak English very well. The population of Chinatown, however, which is somewhat isolated from the rest of the city, and the Hmong population have more of an issue with understanding the English language. Once a form has been developed for a particular customer, it becomes instantly available for every other customer, he said.
Given the complex issues involved in pain relief medication and the potential for abuse or unintentional habituation of pain medications, Isham asked, how does one deal with those challenges in discharge instructions for a low literacy population and those with limited English proficiency? Lee responded that it is very complicated and that there is a big difference between unintentional habituation and intentional misuse. Paasche-Orlow
agreed. He cited Massachusetts as an example of a state that has a system any provider can log onto in order to see a patient’s history of dispensing of opiates, but this does not address the issue of a patient going across state lines to get medications. Acetaminophen is particularly difficult because not only do prescription products contain the drug but also so do many over-the-counter products. In the end, he said, one has to talk with one’s patients because there is only so much a discharge form or an electronic system can do. One must ask oneself whether the patient is a person who is at risk for diversion or for under management of his medications and proceed accordingly.










