
2
Paying for Population Health Improvement: An Overview
In 1997 David Kindig, co-chair of the Roundtable on Population Health Improvement and professor emeritus of population health sciences at the University of Wisconsin School of Medicine and Public Health, wrote that “population health improvement will not be achieved until appropriate financial incentives are designed for this outcome” (Kindig, 1997, p. 174). In his overview of the workshop he said that the statement is still true, but with an additional caveat: in order to improve overall health and to reduce or eliminate health disparities, significant new and reallocated resources of many kinds will be required. Yes, he said, philanthropy and public pilot funds are critical for testing new sources and ideas, but it is essential that partners in all health-promoting government agencies develop and align dependable, long-term revenue streams to fund effective population health efforts. “We cannot do this any other way,” Kindig added.
The first step toward creating dependable and long-term revenue streams for population health will be to reallocate savings from ineffective health care expenditures, Kindig said, “but we will need to go beyond that to expand to ‘health in all policy’ investments as well, especially finding the sweet spots where the core missions of other sectors align with health improvement objectives.” Doing so, he added, will require new evidence regarding the relative cost effectiveness of different investments, but waiting decades to gather that evidence and act is not acceptable. Where the Roundtable can add value to this effort, he said, is to “lead the call for the development of optimal cross-sectoral financial investment or policy
strength benchmarks that are tailored to individual community outcomes and [health] determinants profiles.”
One key issue that population health approaches need to address is determining how much money is needed and where to invest funds for the biggest impact in terms of improving the health of the nation and reducing the enormous health disparities that exist in this country. This is not a new issue, Kindig said, but it is one that has yet to be adequately addressed, in part because the true size of the nation’s health expenditures is masked by the way those costs are calculated. According to national health expenditure accounts, the United States spends about $2.7 trillion on health care and governmental public health (RWJF, 2014), but the true cost of promoting health is greater if the costs of nonmedical determinants are included, Kindig said. Without knowing this total cost, he added, it is difficult to set a figure for what the total health budget should be. The budget should apportion less funding to health care spending, he said, and instead include adequate resources for public health agencies as well as for other sector investments that promote health, such as education, housing, and economic development.
The 2012 IOM report For the Public’s Health: Investing in a Healthier Future recommended that annual governmental public health spending should increase from $11.6 billion to $24 billion, which would at least partially address the $20 billion annual shortfall in governmental public health spending that Trust for America’s Health highlighted in a 2008 report (Trust for America’s Health, 2008). Kindig noted, echoing the previous IOM committee, that the ratio of nonmedical social service spending to medical care spending in Organisation for Economic Co-operation and Development (OECD) countries is 2.0, compared to 0.83 in the United States (Bradley et al., 2010). With regard to the fact that the United States spends more per capita on medical care than other developed nations while having poorer health outcomes, Kindig suggested that the relatively lesser spending on social services in the United States might point to some of the reasons for the relatively poor performance of the United States on health measures. He added that if he were in charge of setting spending on the public’s health, he would take the 20 percent of health care expenditures thought to be ineffective, which is roughly $500 billion, and reallocate $100 billion to provide health insurance for the uninsured, $100 billion to prevention, and $300 billion to social factors, such as education and jobs, that are known to promote health.
Reallocating funds and setting overall budget priorities is just a start, though, because different parts of the country need different types of investment. To offer an example of such differences, Kindig looked at two states that rank highly in terms of health outcomes: North Dakota, at number 9, and Utah, at number 6 (United Health Foundation, 2013).
In North Dakota, the two biggest determinants of health are smoking and binge drinking, while in Utah, a lack of health insurance, failure to graduate from high school, and air quality are the three most important determinants of health. Realizing that such differences also exist at the community level complicates the matter of creating investment profiles that would achieve the biggest return on investment, Kindig said.
What would help set investment profiles, he said, is an analysis of how different patterns of financial investment and health-promoting policy strength over time correlate with the county-by-county disparities in health outcomes seen in the United States (see Figure 2-1). Somewhat surprisingly, the data do not exist to conduct such an analysis. A researcher in Wisconsin, for example, tried to conduct such an analysis by looking at per capita investments in Medicaid, Head Start, and other programs. He found that there was too much variation and too many imperfections in the relevant accounting systems. “That is a huge challenge for us to be able to move forward and dissect out what might really work,” Kindig said. He suggested that the Roundtable could help in developing the means to standardize how investments in programs can be measured or estimated in order to help jurisdictions plan their health budgets and other budgets relavant to health (e.g., early childhood education).
In terms of where new investments will come from, Kindig cited four possible sources of dependable financial support. One source would be from savings in health care and the hospital community benefit requirement expanded by the Affordable Care Act.1 Kindig explained that, contrary to the common perception that community benefit funds go primarily toward charity care, data from the Internal Revenue Service show that 25 percent of these funds go toward uncompensated services provided to patients who are unable to pay, 5 percent is spent on community health improvement, and almost 60 percent, or nearly $40 billion, goes toward Medicaid discounts or other money-losing services.2 Kindig offered his opinion that some, though not all, of the approximately $40 billion, could be marginally redirected in more health-promoting ways.
A second source of support, he said, would be to get more health from what is already being spent in other sectors, including the community development opportunities that other speakers at the workshop would address in a subsequent session. Although governments and foundations will continue to be the third dependable sources of some funding, businesses that understand the business case for public health investments
_________________
1For more information on the community benefit requirement see http://kresge.org/news/kresge-supported-project-provides-easily-accessible-information-about-%E2%80%98community-benefit%E2%80%99-requi (accessed July 11, 2014).
2The exact figure is $37 million.
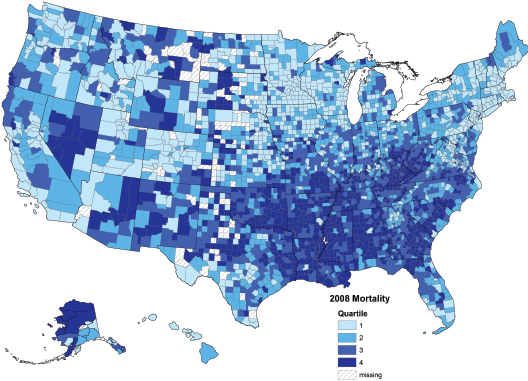
FIGURE 2-1 Age-adjusted mortality by U.S. county.
NOTE: Counties are ranked by the per capita death rate, which is adjusted for the age distribution in each county.
SOURCE: Kindig presentation, 2014.
will also need to be considered as the fourth funding sources. The “sweet spots” for business go beyond health care costs and workforce productivity, Kindig said, and include the ability to attract and retain talent and to build a brand reputation.
The most important factor going forward, he said, will be to make sure that revenue streams are dependable. “We’re talking about one-sixth of the nation’s economy,” he said, “and a voluntary effort is not going to get this done. We need to move beyond grants and short-term appropriations and move to dependable formula sources such as those dedicated to crop subsidies, mortgage interest deductions, or Medicare medical education payments that are not annual grant renewal items.” Kindig also remarked that the medical and public health practice community needs to use its political clout to support investments in other sectors, such as early childhood development, that also benefit public health. “Those are win–win opportunities,” he said, echoing the 2012 IOM report For the Public’s Health: Investing in a Healthier Future. He added that it will be important for governmental public health agencies to examine their own abilities and performance and make sure that they are using existing funds with utmost effectiveness.
The last point that Kindig made was that population health advocates need to move beyond benchmarks based on the determinants of health to benchmarks for effective national and community investments pertinent to health; at present the former benchmarks are better developed, while the latter are not. The field would benefit, he said, from efforts to develop “optimal cross-sectoral financial investment or policy strength benchmarks which are tailored to individual community outcomes and their determinants profiles.” What the nation needs, he added, is a “pay-for-population health performance system, a system that has a coordinated effort across determinants [of health] between the public and private sectors, as well as the financial resources and incentives to make it work.” He closed his comments by offering what he believes to be the key population health question that needs to be answered: “In a resource limited world, what is the optimal national and local per capita investment and policy strength across sectors for improving overall health and reducing disparities?” Answering that question is difficult, but essential.
Robert Kaplan, from the National Institutes of Health, started the discussion by asking Kindig if the Roundtable was looking at metrics to judge the effectiveness of public health spending. Kindig replied that metrics are one of the drivers of the Roundtable and that the Roundtable has found that although there is a great deal of activity in this area, there
may still be opportunities to develop health disparity metrics and metrics for investment targets. Kaplan agreed that there are metrics available, but he said little has been done to implement them.
James Knickman, of the New York State Health Foundation, commented that one problem with many of the available metrics is that they are intended to show progress in the long run, but funding agencies want evidence that actions are working in the short term. As an example, he cited the Medicaid waiver process that enables states to experiment with different ways of reducing Medicaid spending and then receive a portion of the savings to reinvest in other actions that could save additional funds. Although this waiver process is a great idea in theory, those who engage in the process must demonstrate budget neutrality, and one of the metrics that the Centers for Medicare & Medicaid Services (CMS) uses to measure neutrality is the near-term reduction in hospital readmissions. This focus on short-term savings may prevent the implementation of other potentially money-saving ideas because their savings need to be measured over the long term, which does not fit within the CMS timeframe. Having a conversation about the criteria for Medicaid waivers and how to invest funds to support innovation could be valuable, Knickman suggested.
Jeffrey Levi of Trust for America’s Health said that the governmental public health community has a real problem communicating the diversity of interventions that are being used successfully. As an example, he cited the challenge that arises in defending community transformation grant programs because there is no one intervention that all communities are using. He responded to Knickman’s comments by saying that even within the narrow constraints of the CMS savings program, population health initiatives have begun and that being able to reinvest Medicaid savings in social determinants of health, such as housing support, is a promising opportunity.3 He also said there is a need for a thorough and consistent accounting of governmental public health spending, a suggestion that was echoed by Michelle Larkin of the Robert Wood Johnson Foundation. Larkin mentioned that a group of public health experts is currently developing a standardized system to track resources, expenditures, and inputs.
Sanne Magnan of the Institute for Clinical Systems Improvement asked Kindig for his recommendations for improving financial incentives for population health at CMS. Kindig reiterated the idea of reinvesting savings into the social determinants of health and noted the bigger chal-
_________________
3Examples of innovative initiatives include the Michigan Public Health Institute’s Pathways to Better Health (http://innovation.cms.gov/initiatives/Health-Care-Innovation-Awards/Michigan.html [accessed July 11, 2014]) and the Trustees of Dartmouth College’s program named Engaging Patients Through Shared Decision Making: Using Patient and Family Activators to Meet the Triple Aim (http://innovation.cms.gov/initiatives/participant/HealthCare-Innovation-Awards/Trustees-Of-Dartmouth-College.html [accessed July 11, 2014]).
lenge of determining how to reduce health expenditures in general and where to reallocate the savings. George Isham of HealthPartners asked similar questions about how and where to reinvest from health care into social services. Kindig acknowledged that he does not have an answer for the amount of money needed, but he pointed to promising examples of investing in early childhood programs and involvement of the business community. He also noted the challenges that restrictive financial policies pose for moving money from one budget to another.








