
Key Messages Identified by Individual Speakers and Participants
- More opportunities for meaningful community experiences could provide students with greater insight into the day-today challenges faced by the patients they serve. (Holmboe, Thibault)
- Health providers and others might improve their impact with community interventions by gaining greater understanding of the “insider views.” (Scrimshaw)
- Patient navigators play an important role in engaging communities and bridging cultural and language gaps between patients and providers. (Cooper-Smith, El-Bayoumi, Mabur)
- It is not only about educational designs or the kind of students admitted into health professional programs, but it is also about how the different health professions structure the entire curriculum within a framework of justice and equity for society. (Meleis)
- There is a disconnection when health professionals talk about sending students “into the community,” when in fact health care systems are of the community. (Wolf)
SETTING THE STAGE
Workshop co-chair Susan Scrimshaw, from The Sage Colleges, set the stage for the workshop by reminding participants that the focus of this workshop is on taking health care providers out of the clinic and bringing them into the community. It is in the community where the source of a health problem can be uncovered. Scrimshaw told the story of Richard Carmona, a former surgeon general, who was at a health clinic in the Southwest United States and noticed unusually high rates of carbon monoxide poisoning in children. According to Scrimshaw, youngsters were being left in old trucks with the motor running on cold nights, while their parents dashed into the trading post. The children’s exposure to high levels of carbon monoxide during those brief moments was due to the structure of the old trucks. Carmona discovered this, and so, instead of waiting for unconscious children to be brought to his clinic, he set up a Saturday clinic to fix the old trucks. That is the image of community health that Scrimshaw encouraged participants to internalize during the course of the workshop.
Also in setting the stage, Scrimshaw established a common understanding of some terms that would likely be used throughout the workshop. She began by saying that anthropologists, like herself, spend a lot of time studying culture. As such, there are now roughly 200 definitions of culture. Scrimshaw combined the common elements of these into what is presented in Box 1-1. Scrimshaw emphasized two main points about the elements of the definition. First, individual and group internalizations and expression of their culture are constantly being modified through lived personal experiences; second, much of a health provider’s expression of him- or herself in working with communities is at the unconscious level. The key is to recognize one’s biases in order to provide respect and understanding to individuals of communities in ways that improve communication between the health provider and the community.
BOX 1-1
Definitions of Culture: Common Elements
- Shared ideas, meanings, values
- Socially learned, not genetically transmitted
- Patterns of behavior guided by shared ideas, meanings, values
- Constantly being modified through lived experiences
- Often exists at an unconscious level
SOURCE: Scrimshaw, 2014.
Scrimshaw then provided a definition of community. At the Centers for Disease Control and Prevention (CDC), Scrimshaw and others developed the Guide to Community Preventative Services and spent 1 year trying to define community. In the end, they came up with the following definition: a group of individuals sharing one or more characteristics (place, affinity, culture, network, disease, etc.). The community could be based on geography, although that presents problems (such as individuals who worship in one geographic area and live in another), so it might be a common affinity for a place to which people return frequently. It could also be a group of individuals who are exposed to the same risks, or all have a similar disease or illness.
Another term Scrimshaw defined was health disparities. She did this in order to establish a shared understanding among the workshop participants of what it is. The definition she provided reads as follows: health disparities are differences in rates (likelihood) of disease, severity of disease, or disease outcomes between populations or groups. Some say that health disparities involve measurable differences, but Scrimshaw would add that they also involve preventable differences.
While at the CDC, Scrimshaw and her colleagues developed The Community Guide’s Social Environment and Health Model (see Figure 1-1). An important aspect of its design is that only one item in the figure (“health promotion, disease and injury prevention, and health care”) relates to clinical delivery of care; everything else is in the community. Scrimshaw then pointed to a quote from Health Culture and Community: Case Studies, a book that was published in 1955 by Benjamin Paul, who is often referred to as a founding father of medical anthropology (see Box 1-2).
Scrimshaw then discussed what she called the “outsider view” and the “insider view.” These were first articulated in 1954 by linguist Kenneth Pike, and promoted by anthropologists Ward Goodenough and Marvin Harris. But, Scrimshaw said, it was Paul who was key to establishing the “outsider view” and the “insider view” in looking at culture and health. In her remarks, Scrimshaw described the outsider’s view as the health provider’s perspective and the insider’s view as the community’s perspective. The outsider view might be framed by a Western biomedical perspective of the world—such as that a particular disease is caused by a bacterial infection—whereas the insider view might be based on a community’s belief system. For example, in Guatemala, where Scrimshaw worked, one of the community perspectives was that Ascaris (worms) in children were caused by eating sweets and that because all children had worms it was normal and there was nothing one could do about it. In probing the community’s perspective a little further, it turned out that in their view, the worms were agitated by thunder and lightning because they were more common in the rainy season. To the community, this was obvious. Health providers with
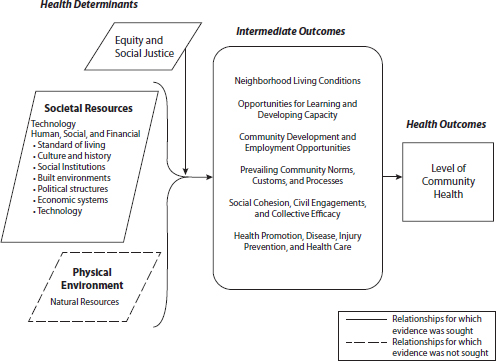
FIGURE 1-1 The Community Guide’s Social Environment and Health Model.
SOURCE: Anderson et al., 2003, as presented by Scrimshaw on May 1, 2014.
BOX 1-2
Excerpt from Health Culture and Community: Case Studies
If you wish to help a community improve its health, you must learn to think like the people of that community. Before asking a group to assume new health habits, it is wise to ascertain the existing habits, how these habits are linked to one another, what functions they perform, and what they mean to those who practice them.
SOURCE: Paul, 1955, p. 1, as presented by Scrimshaw on May 1, 2014.
Western medical training understand the pathology between higher rates of Ascaris infections and more gastrointestinal complications during the rainy season in a Guatemalan village (Warren and Mahmoud, 1977; CDC, 2013a). The key to working with the community to eliminate Ascaris was to say to the parents, “Come and get your children’s worms removed before
the rainy season and the thunder and lightning come.” This is because to the parents, worms were not a problem unless they saw them, and they only saw them when their children had diarrhea and other intestinal problems (CDC, 2013b).
In closing, Scrimshaw reemphasized the concept that health providers working in a community have to always be aware of the outsider and the insider views. A provider’s task, she said, is to understand both perspectives well enough to be able to negotiate the best possible access to health (referring to Figure 1-1).
RESPONSIBILITIES OF AND FOR THE COMMUNITY
Jehan El-Bayoumi, Rodham Institute of George Washington University
Jehan El-Bayoumi of George Washington University opened her remarks by reminiscing on her time as a clerkship director for medical students as well as her 15-year tenure as program director of the Internal Medicine residency. She expressed great dismay when she heard any disparaging comments made by her students about their patients. Their objectification of patients reflected an organizational culture that was perpetuated by the residents who passed on their own negative reflections of patients to the next generation of learners. She noted that, especially at the time, the burden of disease in Washington, DC, was very high. Patients had very complex medical cases of chronic diseases, like HIV/AIDS, diabetes, and end-stage renal disease, along with mental and/or substance use issues overlaid by poverty. She noticed that the disparaging remarks began when these more complex patients entered the hospital, and she realized that the problem was the medical institution, the health providers, and the entire medical community who unwittingly perpetuated the negative behaviors.
Establishment of the Rodham Institute in Washington, DC
El-Bayoumi began the Rodham Institute to shine a light on the dismal health situation in the nation’s capital. El-Bayoumi pointed out that per capita, Washington, DC, is currently number one in HIV, end-stage renal disease, and cancer mortality, noting that pockets in the city have the same HIV rates as Namibia—a shocking statistic that appears to have eluded even the political leaders, she said. Although shocking, this statistic also represents a window into the communities these individuals come from and underscores what is known about the social determinants of health.
El-Bayoumi wondered how it might be possible to help learners continue to pursue the calling that drove them to enter the health professions,
and how to help preserve the enthusiasm that the vast majority of health professional students have when they enter school. El-Bayoumi believes community-based education is the solution. In this way, students become connected with the people they are serving in the environments those people come from. “It is time academic institutions take the responsibility. We need to be accountable to our communities,” she said. Health professional educational organizations need to have a bidirectional bridge so communities do not see the health professionals solely as researchers looking for subjects. Although research is important, she says, it needs to be conducted under an umbrella of trust that is gained when health professionals directly connect with the community they are serving. This is the essence of the Rodham Institute that El-Bayoumi founded in 2013 in honor of Dorothy Rodham, mother of Hillary Clinton, who believed passionately in the power of education to achieve social change.
The Rodham Institute and Community Health Education
In establishing the institute, community, education, and political stakeholders came together and agreed the essence of their work would revolve around creating an action-oriented institute to reduce health disparities in Washington, DC. When asked where to concentrate the efforts of the institute, the stakeholders unanimously agreed to focus on two things: education and food. Although this was somewhat surprising to the health professional educators, it made sense in the context of the community, and it was important that the community members voiced what they would value.
In response, the institute organized a 1-week program during the DC Public Schools’ spring break entitled HELP (Health Education Leadership Program). The event included 45 children from middle and high schools in Prince George’s County that came from low-income households. The facilitators of the event were medical students, undergraduate students, public health students, residents, and faculty. As facilitators, these individuals led small group sessions where the students were asked about health disparities.
The group El-Bayoumi co-led with an undergraduate student dealt with access to green space. She described the impact this session had on the health professional student who learned from the children about the lack of facilities or space for them to exercise. There is no gym at their school, and there is no green space to run or play—they have only asphalt and concrete. El-Bayoumi’s students gained insight into the struggles of those they work with when trying to comply with medical orders to exercise more or to eat more fruits and vegetables, especially when the only stores in the neighborhood sell liquor and tobacco products. In her opinion, that is the way to do applied health disparities education. Instead of the classic
“bench to bedside” training, El-Bayoumi refers to her work as “classroom to community.” El-Bayoumi added that she uses the Association of Black Cardiologists heart health curriculum, which is made up of 12 modules created in conjunction with the National Heart, Lung, and Blood Institute (NHLBI). This curriculum forces learners to apply health literacy concepts so appropriate messages are designed for their target population.
El-Bayoumi reminded the health providers that community health education has been done for decades, especially by medical anthropologists and the international community. She acknowledged the community-focused work of Lisa Fitzpatrick, who trained in public health at the CDC, did her infectious disease training in Denver, Colorado, and is a scientific liaison at National Institutes of Health (NIH). Fitzpatrick is a practicing physician at the United Medical Center in southeast Washington, DC (Fitzpatrick’s presentation is summarized in Box 1-3). According to El-Bayoumi, Fitzpatrick single-handedly created the HIV Red Carpet Program, known as the Care Center; in this program, anyone who tests positive for HIV is immediately scheduled an appointment with Fitzpatrick, with a social worker, and with a patient navigator (the Care Center’s social worker, Marjorie Cooper-Smith, and patient navigator, Daveda Hudson, presented at the workshop). Patients also receive primary care, a dental appointment, and a mental health appointment. If a patient does not come to the follow-up appointment, the patient navigators find out what is going on. If that patient gets admitted, the patient navigators follow him or her into the hospital. This is the type of environment that El-Bayoumi wants the Rodham Institute learners to experience in hopes of counteracting the sorts of negative imprinting she mentioned earlier. El-Bayoumi finished by acknowledging the DC program called Food & Friends.1 The organization runs a meal delivery program that started in 1988 for people living with HIV/AIDS, but now delivers meals to cancer patients and others who are in hospice care. Food & Friends allows learners from the Rodham Institute to accompany them for the meal deliveries. This experience is designed to give students an opportunity to see the living conditions of those for whom they care. It takes 1 day—not weeks of clinical experience—for the learners to gain an insight into the struggles people with illness and disabilities face every day.
Lisa Fitzpatrick, Daveda Hudson, and Marjorie Cooper-Smith of the Care Center then discussed with the Forum members what they wish health professionals knew (see Boxes 1-3, 1-4, and 1-5).
_____________
1 For more information, visit http://www.foodandfriends.org.
BOX 1-3
What I Wish Health Professionals Knew
Lisa Fitzpatrick, Medical Director of the Care Center
The Care Center, part of United Medical Center, is located in southeast Washington, DC (Ward 8), and is a medical home for persons with infectious diseases—mainly, HIV. The Care Center “offers clinical and social support services that include health education, psychological counseling, patient navigation and referral services, support groups, and medical case management” (United Medical Center, 2014). At the Care Center, 85 percent of its clients receive public insurance (Medicaid or Medicare); 40 percent are unemployed; the vast majority of their clients are African American; 40 percent smoke cigarettes; and many have comorbid conditions (Fitzpatrick, 2014).
Lisa Fitzpatrick, who trained in public health at the Centers for Disease Control and Prevention, began her presentation by listing four policy changes that she would like to see. First, she said that there should be a way for patients to obtain reimbursement for nontraditional providers, such as doctors of pharmacy and physician extenders. Second, she emphasized the importance of data sharing between professionals. Third, she called for the elimination of agency silos. Lastly, she asked that resource allocation be reviewed and that new projects start receiving funding.
Fitzpatrick agreed with El-Bayoumi, saying that from her experience working as a care provider in Washington, DC, the medical system and the health care system are completely disconnected from the community and the people on the ground. She listed three main points that she wish health professionals knew:
DISCUSSION
Individual Forum members and other workshop participants then expressed their views about how they would educate health professionals in order to develop the qualities and skills outlined by the speakers. Individual responses of the members are noted below.
Admission Selection
A comment by one of the speakers on the importance of student community engagement early in their health professional education resonated with Eugene Anderson from the American Dental Educational Association (ADEA). Anderson took the comment a step further; he talked about selecting individuals for health professions that already possess the types of desired experiences and commitment sought by health professions for serving diverse communities.
- When patients come into the medical setting, they are scared. It is up to the health professionals and health workers to welcome patients and put them at ease. For example, one patient at the Care Center was afraid to come in to the medical setting. Fitzpatrick left the hospital and met him at an intersection a few blocks away to talk to him about his health care. He eventually came in to the medical setting, and he now has a long history with the Care Center.
- Though the individualized approach is very labor intensive, it is necessary—particularly for the 1 percent of patients that uses up 50 percent of the health care dollars. Some of the cases described by Daveda Hudson and Marjorie Cooper-Smith (see Boxes 1-4 and 1-5) required a great deal of time and energy from the patient navigators. But this 1 percent of patients requires a high level of individualized care, and Fitzpatrick believes that making resources available to provide that care will ultimately result in cost savings for society through decreased health care expenditures.
- Many patients have low health literacy. A patient once told her that she wanted to wait before her blood pressure was taken because she had just eaten a bag of potato chips; another patient told Fitzpatrick she heard that herpes turns into AIDS. One gentleman told Fitzpatrick that he had never heard of Obamacare or the Affordable Care Act.
She said that with these challenges, it is important to figure out how to adopt tailored approaches for each patient. “These are the realities that we have to deal with and we have to figure out how to close the gaps,” said Fitzpatrick.
In a similar vein, Susan Skochelak with the American Medical Association (AMA) brought up selection criteria that better reflected the values of the community the school seeks to serve. For example, she said, what if admissions committees were reversed so members of the community represented the vast majority of the selection committee rather than faculty? She said that would be a change that could occur in relatively short amount of time and would have the potential to have a significant impact on communities.
Educational Design
George Thibault from the Josiah Macy Jr. Foundation discussed the importance of changing the whole model of clinical education so experiences are longitudinal and meaningful in the community. He believes that such experiences would form longer-term relationships with patients, families,
BOX 1-4
What I Wish Health Professionals Knew
Daveda Hudson, Patient Navigator at the Care Center
Daveda Hudson, a patient navigator at the Care Center, told the stories of two patients to illuminate the issues Lisa Fitzpatrick raised. The first involved navigating a young woman who was 19 years old and 5 months pregnant (her fourth pregnancy but third live birth). Hudson tried to get preexisting health information and demographic information from her, but she did not have all of the information needed. At the Care Center, a patient navigator can work with patients from the emergency department to the patients’ homes. Hudson had the opportunity to meet with this patient at her home in order to learn what was keeping her from being actively engaged in her care.
At first, it seemed that the patient was not being medically compliant. She had a history of missed appointments and had accumulated $275 worth of fees because of these. But she began to ask Hudson questions about health forms for her children, and then asked Hudson if she could meet her at her children’s school to help her fill out paperwork for her children. Hudson discovered that her patient had difficulty reading and could not understand her appointment cards, which is why she missed appointments and did not appear to be medically compliant. No other health care providers had noticed this.
Hudson believes there is an automatic assumption that anyone coming to a health clinic can read and understand the information they are provided. However, this is not always the case, and the young woman whom Hudson described is an excellent example of this. With Hudson’s assistance as a patient navigator, the woman is now medically compliant and her babies are healthy.
The second case Hudson described involved a young man she met in the emergency department. He was 22, black, and homosexual. In her role as a navigator, Hudson reaches out to patients weekly to keep them engaged in their care. It took 60 days to convince this young man to come into the hospital because he was afraid and did not want anyone to see him. Hudson would meet with him after work at a convenience store or a public park a few blocks away from the Care Center. Though it took a great deal of prompting and encouragement, Hudson eventually helped him to get ready and mentally prepared to receive health care from Lisa Fitzpatrick.
and the community and would create longer-term relationships between learners and faculty.
Eric Holmboe agreed, having studied standard rotations that occur within internal medicine. He believes they are dysfunctional, and yet many educators assume they are okay, he said. He pointed out that longitudinality is something that accreditation may have impeded because of the process requirements that monitored achievement on the basis of fulfilling a time commitment.
BOX 1-5
What I Wish Health Professionals Knew
Marjorie Cooper-Smith, Social Worker at the Care Center
The key message social worker Marjorie Cooper-Smith wished more health professionals understood is the importance of patient navigation services, particularly for her patients in Ward 8 of Washington, DC. Providers who understand the importance of advocacy and support of patients will connect better with their patients and have greater success with their interventions. To illustrate this point, she told the story of one patient—a 50-year-old African American female—who presented herself to the Care Center with a history of substance abuse and mental illness. She was underweight, frail, depressed, and confused. The patient expressed suicidal ideations and her plans for killing herself. Cooper-Smith and the navigation team spoke gently with the patient, who agreed to walk with them to the emergency room at United Medical Center Hospital, where the navigation team worked with emergency services to stabilize the situation and later get her admitted to the longer-term psychiatric care unit.
After their patient’s release and discharge back into the community, the navigation team again met with her. They discovered she was unable to pay her bills or her rent and she was relapsing into substance abuse. Cooper-Smith believed that there was a possibility the patient was going to be evicted from her home because of her substance use, so her navigation team assisted her with finding resources in the area to help her with her housing situation. Her substance use also affected her ability to adhere to her medication regimen, so the navigation team linked her to a local treatment program. She was reluctant at first, but the navigation team encouraged her until she agreed. The team even picked her up from her home, drove her to the Addiction Prevention and Recovery Administration, waited with her until they were able to see her, and took her to the treatment center.
After being in treatment for several months, she visited the Care Center; she had gained weight, she had new glasses and new dentures, and she had a new wig. She returned as a completely new person, and she stayed in the program for some time. Cooper-Smith said that it is important for health professionals to realize that even though patients come into a health care setting for medical care, there may be additional stressors in their lives that are barriers to receiving care and being healthy.
Cooper-Smith then discussed a case that involved a 45-year-old African American male who was diagnosed with diabetes and taking a number of medications when he came to the Care Center. In reviewing his medications, the navigation team quickly realized that one of the medications he was taking was for high blood pressure; the patient was not aware that he had these conditions, and thought that all of his medications were for his diabetes. This case illustrated Cooper-Smith’s second point, which is that it is important for individuals to be given some sort of documentation—such as a pamphlet, a referral, or a website—from their doctor’s office so patients are aware of their diagnoses and understand the medications they are taking.
Representing the Accreditation Council of Graduate Medical Education (ACGME), Holmboe described the difficult balancing act between monitoring the educational process and structure requirements, and determining whether the desired outcomes are being obtained—outcomes that might include such values as those described previously by the other Forum members. ACGME is now focusing predominantly on outcomes with the Next Accreditation System; they describe the necessary milestones a student should meet upon completion of a program, and they depend on programs to revise the process and curricular elements to help the students get to that point (ACGME, 2014).
Maria Tassone from the University of Toronto and the Canadian collaborative commented on nontraditional ways of educating health professionals that go beyond the clinical preceptorship or clinical rotation model. One example is the University of Toronto Health Mentor Program, modeled after the program at Thomas Jefferson University (University of Toronto Center for Interprofessional Education, 2011). In this model, interprofessional groups of students go out into the community without preceptors to spend time with people who are living with chronic illness and chronic conditions. The students return from these community experiences and debrief with faculty about the encounter. According to Tassone, this model alleviates the need for clinical preceptors and the challenges associated with trying to identify robust community experiences that are meaningful and interprofessional. Another nontraditional example Tassone described is the student-run clinic. In particular, the IMAGINE Clinic Toronto (Interprofessional Medical and Allied Groups for Improving Neighborhood Environments), an interprofessional student-led clinic, is an opportunity for students to engage in health education and health literacy beyond the clinical preceptorship model.2
Role Models
Building on the discussion of longitudinality, Afaf Meleis of the University of Pennsylvania School of Nursing thought the question for faculty and other educators was how to impart a value system to all health care students—a value system about the social mission and making a difference in patients’ lives. She asked, how might social justice and an equity framework be infused into health professionals’ curricula and how might it be operationalized and modeled by faculty? Ideally, she said, the modeling would demonstrate team members working together in equal partnership with a full understanding of each other’s perspective. According to Meleis, it is not only about educational designs or the kind of students admitted
_____________
2 For more information, visit http://imagine.uoftmeds.com.
into health professional programs, but it is also about how the different health professions structure the entire curriculum within a framework of justice and equity for society.
Carol Aschenbrener, who represents the Association of American Medical Colleges (AAMC), echoed the desire for strong role models that demonstrate social accountability and for deans and health system directors to take responsibility for instilling social accountability into their students. Unless this message comes from leadership with a passion, she said, changes in curriculum are not likely.
Global Health Education
Malual Mabur is a health promotion specialist and community health outreach worker with the City of Portland, Maine, but is originally from Sudan. He pointed out the important role patient navigators play in engaging communities and bridging cultural and language gaps between patients and providers. For example, where he works, there is a large immigrant population. Many providers he works with have never seen an immigrant patient from Africa or Iraq, but, he said, this is the new reality; “Maine is not just a white state anymore . . . global health is coming toward your own town,” he said. The community health outreach workers help students and providers learn how to work with immigrant patients. Mabur stated that community health outreach workers like himself are helping students gain an interprofessional understanding of cultures different from their own. He is helping students to learn together about the importance of cultural literacy and cultural humility to the people and communities they serve.
Liana Orsolini with Bon Secours Health System added to Marbur’s comments, emphasizing the value of a global health education in order to better serve the populations that are increasingly making up the array of cultures in the United States. Afaf Meleis also reminded workshop participants of the importance of exposing learners to the rest of the world, and to avoid egocentrism, that is, thinking only about one’s own country for health professional education.
Anticipating Future Needs
According to John Finnegan, representative from the Association of Schools and Programs of Public Health (ASPPH), the critical issue is how to plan for a health system that is not yet created and how to train health professionals in a rapidly changing world. In his view, tying things back to the community is an old idea that came out of the 19th century, and it deserves to be tried again in the 21st century using current principles and circumstances.
Karen Wolf, representing the National Academies of Practice, noticed a paradigm shift from health professionals talking about practicing on communities to now talking about practicing in communities. Wolf’s desire is for there to be a shift to talking about practicing of the community. In her view, there is a disconnection when health professionals talk about sending students “into the community,” when in fact health care systems are of the community. And until educators, health professionals, and policy makers start talking about health and educational institutions as being of the community, she believes the United States as a nation will continue to have problems with its health professions education.
Susan Scrimshaw highlighted some of the points of the discussion. First, she said, keep in mind the notion that health professional students are being prepared for a world that no longer exists. Second, she emphasized the importance of modeling desirable behaviors so students have positive role models to emulate. Third, she returned to the idea of insider/outsider perspectives, which she described at the beginning of the workshop. She said that up to now at the workshop, most discussions have taken place from the outsider perspective (not as people of the community, but as people who want to do the right thing with the community). The critical component, according to Scrimshaw, is learning how to get that insider perspective. She finds that taking learners deeply into the community can provide the connection she described. This might happen through home visits with patients, or possibly by attending community meetings—not as the authority, but as somebody who is listening as a concerned member of the community. She asked how education systems (that include accreditation and licensure) could give emerging health professionals the experience of being in and with the community—learning to listen to the values expressed by members of those communities.
REFERENCES
ACGME (Accreditation Council of Graduate Medical Education). 2014. Next accreditation system (NAS). http://www.acgme.org/acgmeweb/tabid/435/ProgramandInstitutionalAccreditation/NextAccreditationSystem.aspx (accessed July 31, 2014).
Anderson, L. M., S. C. Scrimshaw, M. T. Fullilove, J. E. Fielding, and the Task Force on Community Preventive Services. 2003. The community guide’s model for linking the social environment to health. American Journal of Preventive Medicine 24(3):12-20.
CDC (Centers for Disease Control and Prevention). 2013a. Parasites—Ascariasis: Epidemiology & risk factors. http://www.cdc.gov/parasites/ascariasis/epi.html (accessed July 30, 2014).
CDC. 2013b. Parasites—Soil-transmitted helminths (STHS). http://www.cdc.gov/parasites/sth (accessed July 30, 2014).
Fitzpatrick, L. 2014. Establishing a framework: What I wish the health professional knew. Presented at the IOM workshop: Scaling up best practices in community-based health professional education. Washington, DC, May 1.
Paul, B. D., ed. 1955. Health, culture, and community: Case studies of public reactions to health programs. New York: Russell Sage Foundation.
Scrimshaw, S. 2014. Establishing a framework. Presented at the IOM workshop: Scaling up best practices in community-based health professional education. Washington, DC, May 1.
United Medical Center. 2014. Our services: The Care Center. http://www.united-medicalcenter.com/services/the-care-center.html (accessed July 30, 2014).
University of Toronto Center for Interprofessional Education. 2011. Transformation through collaboration: Inaugural report, 2009-2011. Toronto, Ontario: University of Toronto Center for Interprofessional Education.
Warren, K. S., and A. A. F. Mahmoud. 1977. Algorithms in the diagnosis and management of exotic diseases. Xxii. Ascariasis and toxocariasis. Journal of Infectious Diseases 135(5):868-872.
This page intentionally left blank.
















