
Key Messages Identified by Individual Speakers and Participants
- Student competencies for working effectively with communities go beyond the understandably important disciplinary skills. (Velde)
- Community health and public health principles need to be threaded throughout the educational process. (Morton, Siega-Sur)
- Debates can be a pedagogical tool for stimulating critical thinking and improving communication skills of students and trainees. (Newton)
COMPETENCIES FOR WORK IN COMMUNITIES
Beth Velde moderated the session looking at competencies needed by health professional students for working with communities. Although she is an occupational therapist by training, she is currently director of Public Service and Community Relations at East Carolina University (ECU). Her role in this position is to help faculty and students understand how to engage with communities in doing research that helps to solve community-identified problems. Her community experience began in 1972 with community-based learning/teaching and continues today. Fifteen years
ago, she began working with a small community in Tillery, North Carolina, as an occupational therapist, researcher, and as a faculty member at ECU. Tillery is one of the original “40 acres and a mule” communities; Velde was interested in setting up a community-built health and wellness center that was truly driven by the residents and citizens of Tillery.
In her opinion, the student competencies for working effectively with communities goes beyond disciplinary skills, although, she emphasized, disciplinary skills are most definitely important. Velde stated that another competency is for a student to understand the importance of language, for language conveys beliefs and actions. In that regard, students should also understand that names are important, and that people are not patients but rather members of the same health center. As members, the community has control and authority in terms of what happens in their community health center.
She expressed the view that students learn to use the word we rather than I. For example, “We are doing this together,” not “I am doing this for you.” She also emphasized the value of a student education in humility, and that students understand that differences are valued and that they need to be learned about. She emphasized the significance of defining the impact of one’s work not just in terms of medical care but also in terms of environmental health or social justice. She said that a health professional’s work is reciprocal and mutually beneficial, and this work includes educating students in the community.
Velde said that community members taught the students these competencies even before the health professionals began educating students on their professional competencies, because community comes first in a community-built health practice.
Velde’s work drew heavily from the interprofessional educational methodology. The learning was about, with, and from each other as health professionals from different disciplines, as students, and as community members. The interprofessional education (IPE) model was the foundation on which Velde and her colleagues ran their health services.
To set the stage for the session, Velde described that the focus was on engaging with communities and creating positive changes in health. The focus was also on health disparities and health equity. The skills that speakers would discuss in the session would be on the behaviors, techniques, and attitudes that students would likely need for work in communities, including ways of thinking and believing that drive action and influence behavior.
Velde explained the philosophy she and her colleagues modeled in their community-built health clinic, which involved doing what is right, doing it well, and doing it together to create transformational learning for everyone. Velde then introduced the speakers in her session, Jusie Lydia Siega-Sur and
Jennifer Morton, who have developed interesting ways of operationalizing the philosophy.
University of the Philippines, Manila School of Health Sciences
Jusie Lydia Siega-Sur, University of the Philippines, Manila School of Health Sciences1
Jusie Lydia Siega-Sur is an associate professor and dean of the University of the Philippines, Manila (UP) School of Health Sciences (SHS) and an active member of Training for Health Equity Network (THEnet), where she participated in developing a framework for evaluation of social accountability and medical education (THEnet, 2011). She began her presentation by explaining that their program at UP trains health workers to stay in the country—not for export, like so many of the other programs in the country. For many years, training of health workers in the Philippines has used a Western-based, hospital-oriented model, which resulted in their graduates leaving the country. This particularly affected the University of the Philippines College of Medicine, who found that 63 percent of their medical graduates leave the country versus the national medical school average of 50 percent (Bonifacio, 1978; Estrada, 1978). Only 15 percent of the medical school graduates who stayed in the country worked in rural areas. The other remaining medical school graduates located their practices in urban centers (Estrada, 1978). In short, she said, the universities trained their health professionals to take care of the needs of other countries rather than their own people.
Development and Structure of the UP-SHS Program
The greatest challenge, according to Siega-Sur, was how to develop health workers who were not only technically competent but also—and more important—socially competent and firmly committed to serve in the rural communities where they were most needed. The challenge was also to train them with competencies that were suited to their workplace, and eventually to equitably distribute them in different areas of the country, especially in areas of greatest need for health workers. To address these, UP engaged in joint education and health systems planning with academia, the Ministry of Health, and the communities in order to develop an innovative curriculum that would develop this kind of health worker—someone who would address the country’s needs.
Figure 2-1 shows the stepladder curriculum they developed; it is a
_____________
1 The University of the Philippines, Manila School of Health Sciences (UPM-SHS) in Leyte was forced to rebuild its infrastructure, restart its programs, and rebuild the communities it serves after being damaged in 2013 by Typhoon Haiyan (THEnet, 2014).
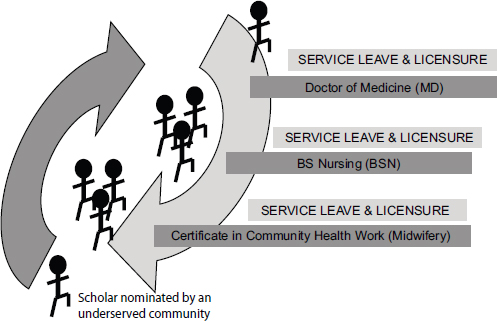
FIGURE 2-1 The stepladder curriculum.
SOURCE: Adapted from Siega-Sur, 2014.
community-based and competency-based curriculum that trains the midwife, the nurse, and the physician in one continuous and sequential curriculum. Students are recruited from underserved communities, who nominate the scholars and support them through the program. The entry point of the curriculum is the Certificate in Community Health Work (Midwifery). Students may, however, exit the program at various levels as a functional category of health worker in the health care system. They may also likewise reenter the program at any point at a later time, depending on community’s needs.
Between program levels, there is a built-in “service leave,” when students are required to return to the community that nominated and sponsored them and render health and community development services based in those areas. Service leave is also a requirement for licensure.
Siega-Sur described how the school developed the competencies based on local needs of the community. In many communities in the Philippines, she said, there is only a midwife or a nurse to provide care; therefore, when structuring their curriculum, UP felt the ability of health professionals to multitask was paramount in their education. Students would need to know how to deliver babies, assume multiple tasks, make decisions, and provide
the necessary care within their competence in the absence of other health worker categories. That was an important component that became part of the stepladder curriculum. Drafting of curriculum also had to take into consideration the rules and regulations of midwifery practice, nursing practice, and medical practice in the Philippines.
The Five-Star Health Professional
Siega-Sur then described the five competency areas for what UP-SHS calls the “five-star health professional.” The five competency areas are threaded throughout the curriculum of midwifery, nursing, and medicine—each building on the previous level. The primary area is the education and training students receive as health care providers, either as midwives, nurses, or physicians. The second is training to become community organizers and mobilizers so students become competent in organizing their communities for health action. A third area involves training to be health service and program managers so students can run programs and services in their communities and can supervise health and auxiliary personnel in their communities. The fourth is skills development in research, and the fifth is learning how to be trainers and educators.
Siega-Sur gave an example of how the competencies are woven through various levels of the curriculum. Midwives are taught how to care for babies, children, and childbearing women. At the nursing level, they learn to care for clients with medical or surgical problems, psychiatric problems, and a variety of other health problems. At the medical level, they are taught the knowledge and skills of a clinician. Each element of the program builds on the other components, so graduates who complete the entire program possess the skills and knowledge of a nurse, a midwife, and a physician. Siega-Sur said that, in effect, one has the equivalent of an entire health team rolled into one person. This form of education that emphasizes the different professions learning together gives students a greater understanding and appreciation of the roles and contributions of each of the other health personnel in the team (see Table 2-1).
Skill Sets Taught to Students
Siega-Sur then described the skill sets that are taught to students. As noted in Figure 2-2, the star displays the skill sets taught to students, and the small circles at the edge of the star represent the five competency areas described earlier, which are health care provider, community organizer and mobilizer, health service and program manager, researcher, and trainer/educator. Threaded into all of these competency areas are four main skill sets—communication, advocacy, cultural competence, and decision making.
TABLE 2-1 Skills Learned and Components of the UP-SHS Program
| Certificate or Degree | Skills Learned and Components |
| MD |
|
| BS Nursing |
|
| CHW (Midwifery) |
|
NOTE: BHS/BHC = Barangay Health Station/Barangay Health Center; CHDP = community health development program; MCH = maternal and child health; MHDP = Municipal Health Development Plan; M/S = medical-surgical.
SOURCE: Siega-Sur, 2014.
At the university, it is believed that students should be taught how to communicate and have a dialogue with a community, and be taught advocacy skills so they can be their community’s advocates. Another skill set, cultural competence, is important. One reason is that in the Philippines sometimes treatment is associated with the cause of the disease; for example, if a “supernatural cause” is perceived, then the individual would go to a traditional healer for guidance. Siega-Sur said that understanding the culture is extremely important for any health professional working with communities. Decision making and the development of values—such as equity, service orientation, compassion, commitment, and social accountability—are other key components in all of these skills.
The teaching of values is another important component of the curriculum provided at the University of Philippines. Siega-Sur emphasized that this is critical to the retention of graduates in the country, as economic values often cause graduates from the Philippines to leave the country to seek employment abroad. To get the graduates to stay in the country and serve
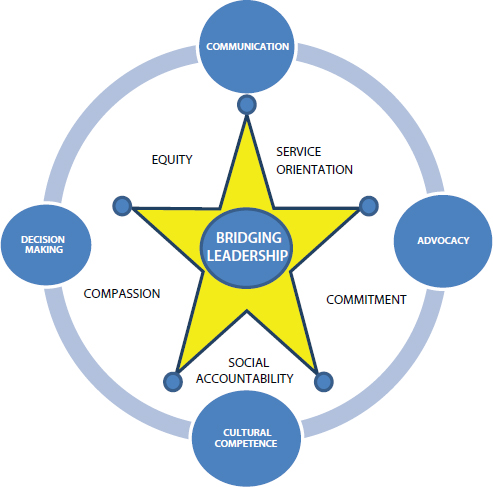
FIGURE 2-2 Skill sets taught through UP-SHS curriculum.
SOURCE: Siega-Sur, 2014.
in the Philippines, the UP-SHS curriculum has a very strong service orientation in their students’ training. There is much dialogue about compassion, equity, social accountability, and commitment to serve the communities that nominated them to train as health workers.
The Bridging Leadership Framework
In recent years, the UP-SHS used the Bridging Leadership Framework as the platform for the development of leadership competencies in their students (Siega-Sur, 2014, adapted from Asian Institute of Management, n.d. See Appendix F for the original figure.). Leadership is seen by UP-SHS as a core competency that health workers must possess to achieve health out-
comes. The Bridging Leadership Framework draws upon the center of the six building blocks for health by the World Health Organization (WHO), which is leadership and governance. The belief is that if able to develop skills of leadership and governance then the health professional will be able to coordinate all the other four WHO building blocks of health. UP-SHS deemed the Bridging Leadership Framework as most appropriate for considering the complexity of problems that cannot be addressed by only one sector. The framework has three components: ownership, co-ownership, and co-creation (see Figure 2-3). Siega-Sur then described the qualities of a bridging leader within each of these three components.
Ownership Siega-Sur said that the first phase involves students developing self-awareness of their values, purpose in life, and leadership capital. They should also have a strong sense of purpose, which is to help their communities. After developing self-awareness, the goal is to develop awareness of the health and societal divides in their communities. This process helps students create a personal vision for themselves.
Co-ownership This personal vision is brought into the next phase, co-ownership. In co-ownership, each of the students develop an ability to engage all the stakeholders from different sectors in creating a shared vision as their collaborative response. They are taught how to do work using processes such as dialogue, multi-stakeholder analysis, and systems thinking to bring the stakeholders together and create a space of trust that promotes discussion and team development. During the community experience, they are given opportunities to engage the stakeholders in the communities they are assigned.
Co-creation When it becomes a shared and common vision of the community, the students are able to move into the last phase of the framework, co-creation. This phase involves developing an empowered citizenry, a transformation of institutions, and a creation of new institutional arrangements to improve health outcomes. In essence, Siega-Sur said, the goal is to train students to think creatively and to network and collaborate with health or nonhealth stakeholders in the community who are in a position to improve health outcomes. For several of their cohorts, Siega-Sur reported successfully bringing down maternal mortality rates as well as infant mortality rates (Zuellig Family Foundation, 2013a,b). She attributes much of this success to training of the local chief executives, most of whom are not doctors.
Required competencies for each phase Competencies required for the first phase of ownership include self-mastery, understanding health challenges,
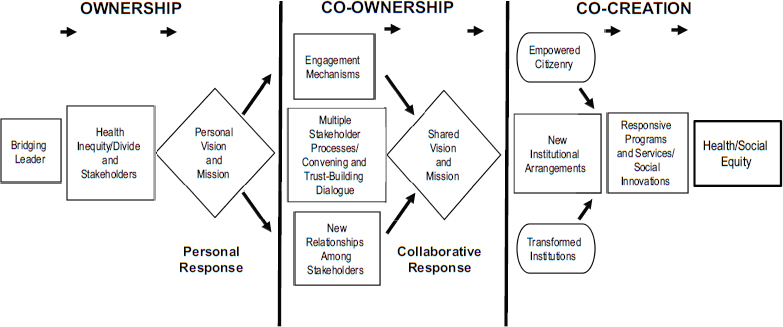
FIGURE 2-3 Bridging leadership framework and process.
NOTE: This figure was adapted from Asian Institute of Management, n.d. See Appendix F for the original figure and description.
SOURCE: Siega-Sur, 2014. Adapted from Asian Institute of Management, n.d.
visioning, change mastery, and resilience mastery. For the co-ownership phase, competencies include visioning, teamwork, clear communication, coaching, and conflict management among health professionals and community members. Co-creation competencies involve creativity, innovation, networking partnership, and resource mobilization.
Community Involvement
The community is very involved with the educational process. To begin, Siega-Sur turns to the Ministry of Health and local government units for input as to which communities should be targeted for student recruitment. Identified community members then participate in selecting their scholar. For their entire community experience, students live with foster families in the community, who are selected by the community members, specifically, the rural health staff and the local leaders. The students’ activities that cover the five competency areas noted in the Five-Star Health Professional diagram (see Figure 2-2) are also decided within the community and carried out with their participation.
The community is also involved with the evaluation of programs and projects that take place in their community. And although students facilitate the evaluation process, communities participate in conducting the actual evaluations of the projects that were implemented while the students resided in each community.
Evaluation
Siega-Sur reported that evaluation is done at two levels. One level assesses student learning, and the second evaluates the effect students have on community health indicators, as established by the Department of Health. Such indicators might include studying whether student placement in the community increased facility-based childbirth or increased the number of deliveries handled by skilled birth attendants.
In addition to those indicators, there are also community-identified indicators that are part of the community health development plan. This plan is a joint effort between the student and the village council, and it includes evaluation indicators the community wants to see achieved by the time the student finishes his or her learning experience in their community.
At the end of their community-based experiential learning opportunity, students conduct a municipal exit assembly. During this event, different sectors of the community, as well as the students and the community representatives, are invited to present the output of the joint efforts of the students and the community that made up the entire community experience.
Key Messages
Siega-Sur shared four key messages from her perspective about the program:
- There is a need to train more health professionals with unique skills to meet the workforce shortage.
- Education of health professionals in the Philippines is best if it is community-based, competency-driven, and interprofessional. While students learn midwifery and nursing separately in the classroom, the training in the communities is interprofessional. Together, medical students, nursing, and midwifery students learn to work as teams in addressing community problems. They are also able to practice supervision. The entire education is community engaged from the beginning; students start in the community much earlier than they do in other schools. According to Siega-Sur, medical students spend 18 months in a community internship, in addition to their community experiences in the midwifery and nursing levels.
- The UP-SHS program emphasizes quality and relevance. The intent is to train the right type of health worker with the right skills for future work in the place where the student will ultimately be employed.
- The interaction and joint planning between academia, the health system, and local governments are necessary to improve health outcomes.
CHANNELS Project
Jennifer Morton, University of New England
Jennifer Morton is Program Director for the Department of Nursing at the University of New England. She is also a core faculty member for the Interprofessional Education Collaborative at the university, which is located in Maine. With campuses in three separate locations, Morton pointed out her university educates the largest number of health professional students in the State of Maine without the benefit of an academic health center. Because of this, she and her colleagues rely on clinical partnerships to educate their students in their clerkships, preceptorships, and clinical experiences. Although these partnerships pose significant challenges, this setup is actually beneficial for community-based learning.
A cornerstone of the university, according to Morton, is its robust IPE infrastructure and its community-based educational focus that is guided by a public mission. Box 2-1 includes the list of health professions and
BOX 2-1
Health Professions Within the
Westbrook College of Health Professions Campus
- Applied exercise science
- Athletic training
- Dental hygiene
- Nurse anesthesia
- Nursing
- Occupational therapy
- Physical therapy
- Physician assistant
- Social work
Other Colleges: College of Dental Medicine, College of Osteopathic Medicine, College of Pharmacy.
other colleges within the University of New England Westbrook College of Health Professions campus.
In describing how she and her colleagues at the university think about competencies for good work in communities, Morton referred to a project that her university was awarded through the Health Resources and Services Administration (HRSA) 2 years ago. To frame her comments, Morton explained that most residents of Maine are Caucasian, but Maine is also a resettlement area for immigrants and refugees. There are also other vulnerable populations including rural, low-income residents.
The HRSA award was to create an innovative, interprofessional program that would improve health outcomes for immigrant and refugee communities in the Portland, Maine, area.
The resettlement area is a new home to 400 to 450 primary or secondary refugees annually. Also, about 13 percent of the City of Portland, Maine, where Morton has rolled out this initiative, is foreign-born, with English as a second language. The fact that Maine is also a non-Medicaid expansion state, Morton says, causes great confusion among the most vulnerable members of the community.
The program, called CHANNELS (Community, Health, Access, Network, Navigate, Education, Leadership, Service), is based on a model of education for students, training of health professionals, and service to the community (see Figure 2-4 for the program model). Morton provided the context surrounding her fundamental and targeted approach to working
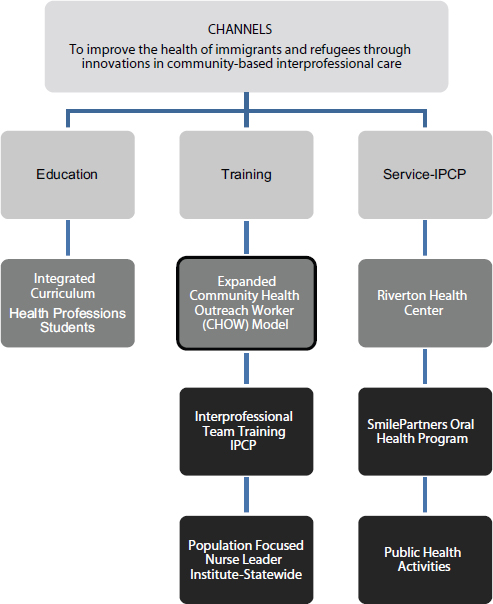
FIGURE 2-4 CHANNELS program model.
NOTE: IPCP = interprofessional collaborative practice.
SOURCE: Adapted from Morton, 2014.
with communities, which uses the best available evidence to inform education and practice. Figure 2-4 shows that the ultimate goal of the project is to improve the health of immigrants and refugees through innovations and community-based interprofessional care.
Educating Students
Morton expressed her dismay that in her experience and historically, universities educate students in community and population health during the final semester of their fourth year. To her, that was too late in the curriculum. She believes that community health and public health principles need to be threaded throughout the educational process and not presented as a stand-alone course. Therefore, in designing their program, Morton and her colleagues elected to integrate population health throughout the students’ education and to teach the more advanced skills for community and population health during the final semester.
In addition to being longitudinal and interprofessional, the program is bicultural and participatory with the community. It is also grounded in cultural sensitivity. Although there are many theories about how to teach it, Morton views cultural sensitivity as an area that is continuously changing and evolving; she said that because of this, no one can ever truly reach full cultural competence, and it is a process that one learns over a lifetime.
The other component of their program integrates what Morton referred to as the 3 Ds, which draws from ideas presented in the nursing literature. The 3 Ds include diversity, health disparities, and social determinants of health. In commenting on diversity, Morton expressed her view that health professions education has a long way to go in creating academic environments that are rich with diversity. This is because academic diversity translates to workforce diversity, and there is a huge deficit in workforce diversity, said Morton. She went on to say that workforce diversity helps to eliminate health disparities (Cohen et al., 2002; LaVeist and Pierre, 2014).
The full interprofessional curriculum that will be implemented in late 2014 is intended to be 6 hours long; the number of hours, like all the pieces of the curriculum, is the result of a compromise among the health professional educators. It includes educational and community-specific competencies, as well as education in cultural humility. The cultural humility education begins with self-reflection and works toward self-awareness, sensitivity, and knowledge as the student matures personally and professionally.
The curriculum is supported by an environment and culture that has multiple opportunities for the students to engage in extracurricular activities. For example, the project runs an event series with invited speakers as well as team-based activities for students that are related to health disparities and social determinants of health. At one event, the program’s community health outreach workers (CHOWs) ran a world café where students from different professions could learn about and from each other. Students learned what the other professions do and how the CHOW is an essential part of the health professional team. The intent of the exercise, according to Morton and her colleagues, was to broaden students’ thinking from in-
terprofessional teams to teams that might include nonhealth professionals, like religious leaders or law enforcement.
There are also interprofessional service learning projects and small grants to support interprofessional research by students. One popular service learning project is run at the community jail. The CHANNELS project (presented in more detail in abstract C.8) has been the inspiration for other creative opportunities for this kind of innovative, interprofessional learning.
Training of Health Professionals
The training arm of the program includes the CHOW model and interprofessional team-based training for interprofessional clinical practice environments. To be sure health professionals are receiving training that draws upon the latest and best available evidence, Morton and her colleagues are reaching out to their community-based partners to help them better understand the principles of a robust interprofessional practice, as their educational competencies dictate.
Morton discovered that much larger investments in resources were required for improving the training side than were required on the educational side of her program. In fact, a relatively small amount of their HRSA grant resources went to the education side. Because many of her community-based partners work in low-resource settings that involve medical homes and Federally Qualified Health Centers (FQHCs), the false belief was that these partners were already proficient in working interprofessionally. Morton realized that understanding how to work effectively as a team or in a collaboration is something that requires active learning of those in practice.
The other piece of information that Morton discovered through the training of health professionals is that public health nursing around the world is very poorly resourced. Maine’s state public health nursing agencies are so underresourced that capacity building was not possible. So, Morton and her colleagues developed a public health nursing institute that provides public health nurses in the field with advanced public health nursing skills, as well as leadership development.
Service to the Community
The interprofessional clinical practice environments of Morton’s program included the rollout of a new health center that was part of an FQHC, an oral health program, and roughly 50 public health activities that have been critical to the work of their program.
One example of a project within the service delivery arm is the Riverton Health Center, a clinic implemented at a housing authority site in the City of Portland that is home to 650 immigrant and refugee families. One of the problems with that housing authority site is that it is on the outskirts of Portland, and so access to health care was very difficult. Therefore, Morton and her colleagues built a community-based clinic that is a satellite of the local community health center. In building the community-based clinic, Morton’s group conducted a formal needs assessment and asked the community members what services they wanted, and even how the clinic should be decorated. They initiated public health activities requested by the communities. For example, many immigrant and refugee female patients were suffering from frequent back pain; therefore, Morton implemented back pain clinics by involving the university’s physical therapy department (both students and community members). Other community requests that were implemented at the clinic included Zumba classes, wellness activities, and cooking classes.
CHANNELS CHOW Model
CHANNELS uses an expanded CHOW model, which Morton believes could translate to any vulnerable population. In this expanded CHOW model, the CHOWs and patient navigators not only educate vulnerable communities in Maine but also educate the university’s students and others at the training sites. They educate about what navigation means and about the importance of understanding culture. Two of the CHOWs who work with Morton, Siyad Ahmed and Malual Mabur, were present at the workshop.
In the expanded model, CHOWs include cultural brokers, patient advocates, medical interpreters, and educators (community, students, providers). The model uses the Institute for Healthcare Improvement’s (IHI’s) Triple Aim not only as a guiding framework but also as an evaluation framework that emphasizes the importance of population outcomes, patient centeredness, and an awareness of costs.2 By instilling these principles into her students early in their academic education, Morton hopes that students will have a sense of systems thinking and a overarching sense of resources and costs.
_____________
2 The Institute for Healthcare Improvement (IHI) Triple Aim is a framework for health system performance involving (1) better patient care, (2) improved population health, and (3) reduced health care costs (IHI, 2014).
Measuring Success
As mentioned previously, CHANNELS uses the IHI’s Triple Aim for their evaluation framework. Morton also reported using both formative and summative assessments to measure progress under the education arm of her program. She and her colleagues are measuring cultural sensitivity as well as attitudes and behaviors across the continuum of interprofessional education to practice. CHANNELS uses Team Strategies and Tools to Enhance Performance and Patient Safety (TeamSTEPPS) for their education and training model for communication, quality, and safety and to measure progress toward and attainment of important interprofessional skills among her students and community health professionals.
For the service side of Morton’s program, she relies heavily upon usage reports, electronic medical records, and satisfaction measured through Consumer Assessment of Healthcare Providers and Systems (CAHPS). Morton noted that one of the difficulties with the CAHPS form is its length, which makes it burdensome for people who speak languages other than English and results in survey fatigue. To avoid this difficulty, the CHANNELS project is also using another tool, the Outcome Rating Scale developed by Miller and colleagues (2003), which is a visual analog scale that contains five items. It has been translated into multiple languages and offers another lens for measuring patient satisfaction.
COMMUNITY-BASED HPE PEDAGOGY: FRAMING FOUNDATIONAL ISSUES THROUGH DEBATE
In keeping with the principle of active learning, Forum member and workshop planning committee co-chair Warren Newton from the American Board of Family Medicine described the pedagogical technique of debating and the benefits of debates as a teaching tool. If done well, debates can stimulate critical thinking and improve communication skills while reinforcing the value of evidence-based reasoning (Hall, 2011; Shaw, 2012). The prior sessions, said Newton, started the discussion about competencies needed for innovation in community-based education. What the debate session is designed to accomplish is to talk about fundamental pedagogical issues, many of which have already come up in previous discussions, and to begin to process how the discussions might get beyond individual innovations or programs possibly within a single profession, and move toward considering how particular innovations might be spread and scaled up in the future. But before one can talk about theoretical spread and scale-up of programs, Newton felt it was important to talk some about the structure of education, which was addressed through the pedagogical technique of debates.
Demonstrating Innovative Pedagogy
Newton has used debates for about 20 years to actively engage his students. He adapted the technique for the workshop to demonstrate how he uses this tool with his students. At the workshop, Newton refereed three 20-minute debates. Each began with a brief introduction of the topic by Newton followed by a vote of all the participants. Box 2-2 shows the topics each debater argued.
After tallying the votes, the two debaters were each given 4 minutes to state their case. One debater was given the task of arguing for a particular position, and the other was given the responsibility of arguing against the position. Neither side was allowed to use PowerPoint slides. Following the two arguments, Newton opened the floor for 8 minutes of discussion to allow the workshop participants an opportunity to comment on either side of the debate. This led to a recount of the votes to see whether the debate and the subsequent discussion had changed any of the participants’ positions. The last step was to allow each debater an opportunity to express their true opinion of the topic.
Newton pointed out that the three selected debate topics do not have a clear right or wrong answer. However, for the purposes of the debate, the debaters and the participants are asked to commit to one side when debating and when voting, respectively. Newton likened this to most academic and leadership roles, in which hard decisions have to be made even though there is no one obviously right answer.
He further noted that this debate is not about winning. There was no rebuttal, and there were no judges. What he looked forward to was see-
BOX 2-2
Debate Topics and Forum Member Debaters
Admission Versus Training:
Rick Kellerman, American Academy of Family Physicians
Sarita Verma, University of Toronto
Longitudinal Versus Block:
Lucinda Maine, American Association of Colleges of Pharmacy
Holly Wise, American Council of Academic Physical Therapy
Virtual Versus Real:
Pam Jeffries, Johns Hopkins University School of Nursing
Eric Holmboe, Accreditation Council for Graduate Medical Education
ing how the group thinking might shift as the discussion over the topic unfolded. In essence, said Newton, the point is enlightenment, not victory.
Debate Number 1: Admission Versus Training
In framing the first debate, Newton expressed the opinion that social accountability of health professional education involves placing health professionals in rural and underserved communities. However, this has been a challenge throughout the world. Newton asked whether it is better to recruit people who want to serve in these settings or whether it is better to educate students to obtain specific competencies that will enable them to practice in low-resource settings. He stated the question to vote on as a proposition noted in Box 2-3.
Below is a summary of the final remarks made by the two debaters, Forum members Rick Kellerman (admissions) and Sarita Verma (training). These comments reflect their feelings about the topic and not the side each was asked to support in the debate.
In the end, Verma and Kellerman agreed that an integrative approach that combines admitting the right students and training them for specific competencies is necessary. Kellerman felt that admissions committees he has worked with do a fairly good job of selecting the right candidates for his medical school, but by the time those same students enter their third year clerkship they do not have the same idealism they entered medical school with. Kellerman reflected upon a comment made during the discussion period when Patricia Hinton Walker from the Uniformed Services University of the Health Sciences brought up the negative, implicit training students receive from the “hidden curriculum.” Kellerman still sees idealism at the end of the second year, but by the third year, much of the hope has been extinguished as the students become acculturated in what can be described as a “toxic environment.”
BOX 2-3
Admission Versus Training Proposition
Health profession and educational institutions should place more emphasis on admissions than in training specific competencies during the educational program.
Vote 1: Those in favor of admissions
Vote 2: Those in favor of training on specific competencies
In her remarks, Verma cautioned against the desire to use admissions for solving all the attitudinal and workforce problems faced by health professions educators. Although important, admissions are not the panacea, she said. This is a complex problem created in part by the complexity of the systems students train under and ultimately must work within.
Debate Number 2: Longitudinal Rotations Versus Block Rotations
Newton set the stage for the second debate by saying that block rotations have frequently been used by health professions educators for clinical training. However, there is a movement for educating health professional students through more longitudinal, integrated curricula. Most of the critics of longitudinal curricula cite practical reasons for not moving forward. With that brief introduction, Newton presented the question as a proposition in Box 2-4.
Following Newton’s introduction, Forum members Lucinda Maine (longitudinal rotations) and Holly Wise (block rotations) presented their arguments before opening the floor up to the workshop participants for comments. After the discussion, Newton gave each of the debaters an opportunity to state how they really felt about the topic.
Lucinda Maine felt that both methods are necessary for educating health professional students. She then reflected on the point made by Mattie Schmidt from the American Academy of Nursing that longitudinal rotations help to provide a more meaningful, continuous, and mutually valuable experience for the student and the educator. She also acknowledged that students often do not know what area of expertise they want to pursue and therefore benefit from the wider range of options offered in the block rotations.
BOX 2-4
Longitudinal Rotations Versus Block Rotations Proposition
Should health professions education of the future promote the use of longitudinal clinical educational experiences to the advantage of patients, learners, sites, and academic programs?
Vote 1: Those in favor of longitudinal education
Vote 2: Those in favor of block rotations
Like Maine, Holly Wise thought a hybrid model was the best way to educate toward the competencies she hoped to see attained by her students and trainees. She also admitted that preparing for this debate was a challenge because in reviewing and collating the literature, she was again reminded of the different vocabularies and terms used across all the professions. This presents challenges for communication as well as comparison of the literature.
Debate Number 3: Virtual Versus Real
The final debate Newton moderated looked at the virtues of simulation and various forms of virtual education compared with an education that uses real-life experiences with patients for educating their health professionals. In setting the stage for the debate, Newton explained that the last decade has seen an explosion of both quantity and complexity of simulations. He asked the participants to consider whether they would put their resources toward simulations or toward real patients. Participants voted on the proposition in Box 2-5.
Again Newton asked the debaters, Forum members Pam Jeffries (virtual education) and Eric Holmboe (real patients), to explain how they really feel about the issue. Like the presenters before them, Jeffries and Holmboe viewed the issue from both sides. For Jeffries, the big question is when to introduce simulations and when the ideal time is to move learners into the clinical setting using real clients. Jeffries firmly believes in providing as many virtual experiences as possible before students are sent to take care of real patients. In her experience, if students are not educated in how to deal with people, especially when children are involved, families want the students to leave because their presence creates an awkward situation.
Jeffries then reiterated her view that first should be mastery of the competency using virtual or simulated experiences, and next should be the
BOX 2-5
Virtual Versus Real Proposition
Should a priority of health professions education be the development of robust simulations that can be used to train and assess the variety and complexity of behaviors necessary to implement the Triple Aim?
Vote 1: Those in favor of virtual education
Vote 2: Those in favor of educating with real patients
opportunity to train with patients and families in real-life situations. Eric Holmboe agreed, saying that the evidence is growing that initial health professional training should start in the simulation lab and work up to practice delivery training. A good example of this is the study by Barsuk et al. (2009) from Northwestern University in Chicago, he said. In this study, researchers found that simulated learning of central venous catheter insertion increased residents’ skills with the procedure and later showed a decrease in complications when the students placed catheters in actual patients.
Despite the benefits of virtual and simulated education, Holmboe does worry when simulation becomes a substitution for real work where training in a clinical environment is too difficult to set up and monitor. But he also cautioned against what was brought up previously in the workshop about the objectification of patients and people. With simulation, patients become the object instead of the subject, he said. Simulation is just not the same as a longitudinal relationship with people and patients.
This is something Holmboe struggled with while researching his position for the debate. It is difficult to argue against technology in today’s educational environment, said Holmboe. Simulated training for certain skills have great potential to benefiting patients; if the goal is a competency-based education where skills are mastered, that is an excellent structure. However, if the goal is to produce health workers with experience in working with people, educators may want to rethink the structure.
His final remark involved the cost of high-fidelity simulation. There are a lot of things that can be done using low technology that can be very effective. For example, said Holmboe, learning to use a snare on the end of a colonoscope can be done with rubber rings on pegs.
Jeffries built on Holmboe’s remark, reminding the audience that although simulations have exploded in roughly the past 5 years, they have been around since Resusci Anne, a training manikin developed by Laerdal in 1960. Also, she said, simulations are not about the mannequin or the technology, but rather about the pedagogy; the key is faculty development. Faculty need training on how to teach and assess learning using simulations, which in turn will improve the quality of the education.
Global View
In addition to the individual views expressed by the debaters on the three debate topics, a number of the Global Forum members and workshop participants also contributed their personal perspectives. These were part of an open dialogue about the various points made by the debaters. They are found in Tables 2-2, 2-3, and 2-4, and are separated by the debate topic.
TABLE 2-2 Perspectives of Individual Participants: Debate on Admission Versus Training
| Name | Country of Origin | Viewpoint |
| Jan De Maeseneer | Belgium | My idea is that although both admissions and training are important, the most critical element for producing graduates who are competent to work with and in communities is the way the health care system is structured. If the system supports family physicians earning 8 times—or in some countries 15 times—less than a cardiac surgeon, then all the positive attributes at the time of admission or transferred during the training will be overruled by the economic incentives. |
| Marietjie de Villiers | South Africa | We have changed our admission criteria in South Africa to allow for a broader representative sample of students. When students graduate, it does not matter where they come from or what color they are. They are the same. In this regard, it is the training that is the essential element, so the admissions can be flexible in bringing in a diverse student body with less regard to strict academic achievement as an admission criterion. |
| Bjorg Palsdottir | Belgium | I would not want to choose between the two. Around the world, the pool of health professional students in higher education tends to be drawn from similar economic and social backgrounds. By setting admission criteria throughout the world that is based primarily on academic standards, there is a loss of richness and learning that can be brought from other cultures and communities. I think this begins with establishing admission criteria that look at the whole person and take other criteria than academic scoring into perspective. |
TABLE 2-3 Perspectives of Individual Participants: Debate on Longitudinal Versus Block
| Name | Country of Origin | Viewpoint |
| Jusie Lydia Siega-Sur | Philippines | In my opinion, deciding whether an experience should be block or longitudinal depends on the objectives of the student learning. The block system would probably be more appropriate for learning clinical skills, but for community-based education, perhaps the longitudinal approach would be better. Doing block rotations in the community could result in making the community fit into the university’s academic objectives rather than fitting students into the dynamics of the community. |
| Maria Tassone | Canada | We in Canada are experimenting with what has been traditionally longitudinal and moving more toward a rotational design, but within the same system, within the same site. I am wondering if the best curricular design for community-based education is both longitudinal and rotational and not one or the other. |
TABLE 2-4 Perspectives of Individual Participants: Debate on Simulated Versus Real
| Name | Country of Origin | Viewpoint |
| Jan De Maeseneer | Belgium | From a Western perspective, we can afford simulation technology, which can be quite expensive. When working in Africa, simulation is often not an option because those universities cannot afford the equipment. I think that on a world scale, such differences in economic status might shift one’s thinking about the value of high-technology simulations. |
| John Finnegan | United States-Australia | I would very much disagree that one cannot bring the community into simulation. In fact, we have seen quite the opposite with numerous efforts bringing the conditions of a community into a simulated program (http://www.cdc.gov/flu/pandemic-resources/tools/communityflu. htm [accessed July 30, 2014]; http://3dqld.org/ background [accessed July 30, 2014]; http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2431099 [accessed July 30, 2014]). One example is the Island that is run by the University of Queensland in Australia (https://escholarship.org/uc/item/2q0740hv [accessed July 30, 2014]). |
| Dirk Hagemeister | South Africa | I think we need to balance simulation with real-life experiential learning. While I want students to learn procedures not on another human being but on a plastic body, I fear greater depersonalization of people and patients as health workers mentally remove themselves from situations. In my opinion, the very ontological experience of dealing with another human body is something that a simulation will not be able to reproduce. That experience takes place in many different forms and shapes within the context of human conversation. |
| Bjorg Palsdottir | Belgium | I want to emphasize the need for partnering with communities throughout the entire educational process so communities co-own the education of their health professionals. In this way, communities will guide educators through pedagogical decisions like whether a curriculum should be virtual or real. |
| Name | Country of Origin | Viewpoint |
| Frederic Schwartz | United States | My feeling is that virtual education is easy to undertake poorly and difficult to do well. As the associate dean of osteopathic medicine in Arizona, [I know that] our group has the advantage of training at community health centers around the country; however, such training is inherently uneven with regard to student experiences. The use of simulation technology to be able to bridge some of those gaps is important if done in a way that does not dehumanize. Our hope is that our students will not remember whether their learning was on a simulated patient or a real patient because the experience is the same. |
| Zohray Talib | United States-Africa | Thinking more globally, if low-fidelity simulation is included in the discussion, then I think it is possible to improve the quality and the quantity of graduates. For example, in Ethiopia many of the health professional class sizes have doubled, tripled, or quadrupled in size, so it is not uncommon for 20 students to gather around one patient bed. If training takes place at only one center, it is possible for students to graduate without having ever laid hands on a patient. Low-technology simulation skills labs provide hands-on training opportunities in order to scale up the number of health workers produced. |
| Maria Tassone | Canada | I would agree with the important role for simulation, but I think there is an opportunity to be more thoughtful about the role that simulation plays. Despite huge investments in simulated technologies, many of the simulation centers are not fully used in part because of the time required for technical training of facilitators to support the simulations. |
| I think there is much to be learned from simulation, particularly for briefing and debriefing that brings simulated experiences into real environments rather than restricting such briefings to simulated environments. As such, I would promote greater strategic thinking about how simulation is used and how it can be leveraged to transform the curriculum, and make the hidden curriculum much more explicit through the best practices of simulation. | ||
REFERENCES
Asian Institute of Management TeaM Energy Center for Bridging Leadership. n.d. Bridging leadership framework. Makati City, Philippines. http://bridgingleadership.aim.edu/about/ the-center (accessed September 24, 2014).
Barsuk, J. H., W. C. McGaghie, E. R. Cohen, J. S. Balachandran, and D. B. Wayne. 2009. Use of simulation-based mastery learning to improve the quality of central venous catheter placement in a medical intensive care unit. Journal of Hospital Medicine 4(7):397-403.
Bonifacio, A. 1978. The Institute of Health Sciences: A strategy for health manpower development. Proceedings of the 32nd World Medical Assembly. Manila, 1978. Pp. 43-54.
Cohen, J. J., B. A. Gabriel, and C. Terrell. 2002. The case for diversity in the health care workforce. Health Affairs 21:90-102.
Estrada, H. A. 1978. The realities of Philippine medical education. Proceedings of the 32nd World Medical Assembly, Manila, 1978. Pp. 17-24.
Hall, D. 2011. Debate: Innovative teaching to enhance critical thinking and communication skills in healthcare professionals. The Internet Journal of Allied Health Sciences and Practice 9(3). http://ijahsp.nova.edu (accessed February 26, 2015).
IHI (Institute for Healthcare Improvement). 2014. The IHI Triple Aim. http://www.ihi.org/offerings/Initiatives/TripleAIM/Pages/default.aspx (accessed July 3, 2014).
LaVeist, T. A., and G. Pierre. 2014. Integrating the 3Ds—social determinants, health disparities, and health-care workforce diversity. Public Health Reports-US 129(Suppl 2):9-14.
Miller, S. D., B. L. Duncan, J. Brown, J. A. Sparks, and D. A. Claud. 2003. The outcome rating scale: A preliminary study of the reliability, validity, and feasibility of a brief visual analog measure. Journal of Brief Therapy 2:91-100.
Morton, J. 2014. Competencies for work in communities. Presented at the IOM workshop: Scaling up best practices in community-based health professional education. Washington, DC, May 1.
Shaw, J. A. 2012. Using small group debates to actively engage students in an introductory microbiology course. Journal of Microbiology and Biology Education 13(2):155-160.
Siega-Sur, J. L. 2014. Competencies for work in communities. Presented at the IOM workshop: Scaling up best practices in community-based health professional education. Washington, DC, May 1.
THEnet (The Training for Health Equity Network). 2011. THEnet’s Social Accountability Evaluation Framework, version 1. Monograph I (1 ed.). The Training for Health Equity Network.
THEnet. 2014. THEnet website. http://thenetcommunity.org (accessed July 30, 2014).
Zuellig Family Foundation. 2013a. Bridging leadership: Part one. http://zuelligfoundation.org/index.php?option=com_content&view=article&id=281:bl-partone&catid=18&Itemid=238 (accessed September 2, 2014).
Zuellig Family Foundation. 2013b. Bridging leadership: Part two. http://zuelligfoundation.org/index.php?option=com_content&view=article&id=280:bl-parttwo&catid=18&Itemid=238 (accessed September 2, 2014).
This page intentionally left blank.




























