
Key Messages Identified by Individual Speakers and Participants
- When, how, and by whom an innovation is introduced and promoted could ultimately determine the fate of that innovation. (Newton)
- For an innovation to be spread and scaled, it is important to work with the partner to contextualize the innovation to the local environment and population; however, financial constraints can impede scale-up and spread of programs and models regardless of their value to a community. (Hinkle)
- Engagement of leadership can facilitate the spread and scale-up of interventions. (Hinkle, Wageman)
- Technology cannot be a substitute for the simple foundation of engaging people and asking them what they need and what works for them. (Barclay)
- A way to fix broken health systems in cities around the United States is to align engagement with data and systems redesign. (Brenner)
In setting the stage for more in-depth discussions on spreading and scaling up models of community-based health professional education, Forum member and workshop planning committee co-chair Warren Newton from the American Board of Family Medicine first noted that different disciplines
use different terminology for community-based health professional education (HPE). For the purposes of the workshop, Newton requested that spread be considered “expansion across professions” and scale-up would be considered “geographic spread” or “increasing the numbers and size of a previously formed program or model.” He admitted there would be overlap in terminology depending on one’s discipline, but he requested the participants to think about all the multiple dimensions of spread and scale-up as he defined the terms.
Newton then commented on the classic article by Kerr White and colleagues (1961) titled The Ecology of Medical Care (see Figure 3-1), repeated by Larry Green and colleagues in 2001. In it, White described the best available empirical evidence about what happens to individuals who experience illness. Of the 1,000 persons who get ill, 750 will have a symptom, 250 will see a physician, 9 will go into the hospital, and 1 will go into a tertiary care center. The question White raised is why so much of health professional education is located in tertiary care settings, which is the smallest box seen in the lower-right corner of Figure 3-1. The patients who get to these academic settings are systematically very different—demographically, socially,
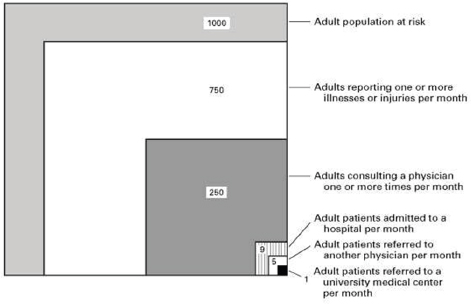
FIGURE 3-1 Monthly prevalence estimates of illness in the community and the roles of physicians, hospitals, and university medical centers in the provision of medical care (adults 16 years of age and over).
SOURCE: White et al., 1961, as presented by Newton on May 1, 2014.
and clinically—from those who stay in community settings—and students’ experience of health care can become skewed.
There have been many changes in both society and health care since the early 1960s. Newton stated that the data are still relevant today in the United States. He stated that Larry Green and others found virtually no change in the numbers in 2001. Fifty years after the original report, health professions education is still heavily weighted toward university hospitals.
Newton then asked the workshop participants—who represent multiple professions and educational associations from around the world—how to move the health professional educational system out of the lower-right boxes of Figure 3-1 into the larger boxes, where students will work with patients in the community and professional settings in which the vast majority of the population experiences health care.
The third point Newton made addressed the application of research on the dissemination of innovation to new educational models. For this, he drew upon the classic work of Rogers in 1962 from his book Diffusion of Innovations. In it, Rogers described the natural history of adoption as a normal bell-shaped curve with innovators representing about 3 percent of the population in the left tail, the majority of the adopters (68 percent) in the center of the curve, and the 16 percent who are slow to adopt are in the right tail (Rogers, 1962). To Newton, most of the health professions’ and educators’ model curricula the Forum members have discussed represents the outstanding innovators and early adopters. Therefore, a key question for this workshop for him was how to spread adoption beyond the innovators and early adopters. To him, this means explicitly addressing how to spread across professions, within institutions, and across geographic regions. In addition, this would mean addressing the various levers that can support this change—starting with education and institutional initiatives, but including licensure/accreditation, incentives, changes in payment for clinical and educational work, and public policy.
Newton then asked: What determines the rate of adoption? There is rich literature on the science of dissemination, he said, but a first step is considering the characteristics of a specific innovation. First, he noted that the more complex the innovation, the slower its diffusion. IPE, for example, is quite complex. Second, he explained that all innovations come with benefits and costs that can have positive or negative impacts on the innovators, the learners, the institutions, and the wider health system—in the short and long term. This complexity means that making the case for educational innovation, both operationally and fiscally, is often challenging. Third, Newton stated that the key issue is the adopters’ perception of the innovation. With respect to innovations in education, what do stakeholders—the payers, the institutions, the accrediting organizations, and the public—think about these innovations? Fourth, he mentioned the importance of timing.
When, how, and by whom an innovation is introduced and promoted could ultimately determine the fate of that innovation. Marketers have been thinking about this for a long time, and Newton believes this thinking would benefit the workshop as participants considered the conditions and interventions necessary to help spread and scale up innovations in health professional education. He believes the time is right for major innovations in education. With careful attention to the design, promotion/incentives, timing of (re)introduction of tools and models for the education of health professionals, and changes in licensure/accreditation processes, more educators may adopt innovations. This adoption, described in the workshop as the spread and scale-up of health professional educational innovations, was the focus of the remaining presentations at the workshop.
INNOVATIONS
Zohray Talib, who is an assistant professor of medicine and of health policy at George Washington University, moderated the session on spreading and scaling up innovations in community-based HPE. The objective of the session, said Talib, was to discuss methods of improving population health outcomes by identifying and addressing gaps, and by scaling up best practices in community-based experiential learning. She said that the session would also address where along the pipeline from education to practice might efforts be concentrated. To underscore the value of shared learning for scaling up best practices, Talib described the Medical Education Partnership Initiative (MEPI) and her role in the initiative.
MEPI is a $150 million program of the U.S. government that is designed to strengthen the health workforce in Africa. It is completing its 4th year of a 5-year grant. Almost two dozen medical schools in Africa were given funding to achieve three aims: to improve the quality and quantity of health workers, to address the retention of workers in underserved areas, and to improve locally driven research and the research capacity of these institutions.
George Washington University, along with an African counterpart, is part of the MEPI coordinating center that observes and provides assistance and support to the MEPI network. What Talib has observed through her work with the network is that among the MEPI-funded and supported schools all are investing in community-based education to achieve their goals of quality, quantity, and research.
Talib convenes a technical working group on community-based education, whose leaders and members are from the MEPI schools. They discuss what community-based education looks like in different countries and what methodologies, programs, and interventions are successful. These conversations allow the members to determine what community-based education
innovations work and what could be scaled up and spread. Talib stated that the conversation about spreading and scaling up community-based education is a global conversation.
Talib then introduced the two panelists in her session: Scott Hinkle, from the National Board for Certified Counselors, and Ruth Wageman, from ReThink Health.
Mental Health Facilitator Program
Scott Hinkle, National Board for Certified Counselors
Scott Hinkle, from the National Board for Certified Counselors (NBCC), is a nationally certified counselor in clinical mental health and an approved clinical supervisor. He has been a practitioner for 35 years in the areas of community and school mental health. Hinkle currently consults with universities on issues concerning distance education and clinical training, and he is the coauthor of the mental health facilitator program.
Mental Health Facilitator Program
The NBCC Mental Health Facilitator (MHF) Program was started in 2007 and has been taught in 22 countries around the globe. It is administrated by NBCC International, a division of NBCC. It was brought to the United States in January 2013. The program expands mental health service capacity, and it complements existing resources to improve services for communities.
Hinkle used the pyramid in Figure 3-2 to explain the MHF Program. Self-care, the largest slice, is at the bottom of the pyramid. This is followed by mental health services via primary care and informal community care. The next level of the pyramid contains (1) community mental health services, and (2) psychiatric services and general hospitals. The top of the pyramid is long-stay facilities and specialized psychiatric mental health services.
An important part of mental health facilitation is to teach individuals in the community self-care and to train community workers so they can prevent their fellow community members from entering areas higher up on the pyramid. To accomplish this, Hinkle avoids technical terms and sophisticated terminology so the students can understand the teachers. For example, the MHF program uses common terms such as stress, distress, and disorder and being balanced, less-balanced, and off-balanced. The MHF program has also been translated into 10 languages, including Arabic and Swahili. Hinkle noted that the program was taught in Arabic on the Syrian–Jordan border in 2012 to train workers going into refugee camps with high rates of domestic violence and child maltreatment.
Another item Hinkle pointed to in Figure 3-2 is that the program uses a
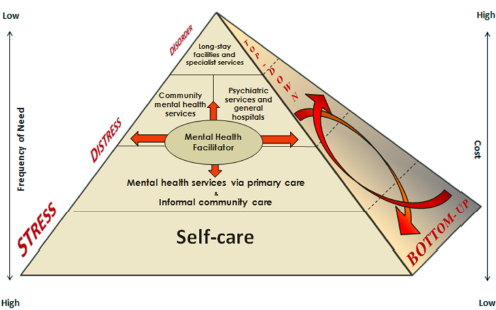
FIGURE 3-2 Modified WHO pyramid framework: mental health facilitator (MHF).
SOURCE: Hinkle, 2014.
bottom-up and a top-down approach to training (or “inside” and “outside” approach, referred to by workshop co-chair Susan Scrimshaw in her opening remarks). Though the work happens in a bottom-up model, Hinkle said that without the country’s top leaders giving sanction and credibility to the program, it will not be successful. Therefore, Hinkle often works with ministers of health and deputy ministers of health to get the program initiated.
Hinkle then addressed the “frequency of need” that is shown on the left side of Figure 3-2. As one moves up the pyramid, interventions change from brief encounters to long-term care placement that would be in the form of asylum care in many developing countries. Though the frequency of need diminishes as one moves up the pyramid, the cost increases (see the right side of Figure 3-2). This means that with more long-term care placements there is less funding available for the other interventions noted lower down in the pyramid.
New Curricula
Educator’s Edition of the MHF program The Educator’s Edition of the MHF program is a new addition to the program that was first piloted in a school district in North Carolina and is being brought to the state of
Montana for the second piloting. Hinkle stated that this program aims to teach all school staff—including teachers, administrators, cafeteria workers, transportation, bus drivers, security, and safety officers—about basic mental health care. It provides training in how to identify people with mental health issues, how to support them, and how to get them referred.
The curriculum also includes information about child abuse, how to recognize it, what to do about it, and whom to contact within the school’s mental health system. Suicide is another topic covered in the training because in the United States the data on suicide among young people are extensive and disturbing. Bullying is also included in the training. The program provides information on classroom management, because as many as 75 percent of schoolteachers indicate that they do not know how to manage behavioral problems and emotional difficulties in their classroom. The course also includes training to help teachers make referrals for appropriate consultation and follow-up. Like the MHF program, the 18 to 20 modules can covered in 24 hours. It can be split into two weekends because, said Hinkle, the material does not need to be given in 4 straight days.
MHF-ASAP! Following his meetings recently with the National Alliance on Mental Illness in Washington, DC, Hinkle and his colleagues condensed their training modules into a 1-day training. Called MHF-ASAP! (as soon as possible), this training educates people in the community about basic information on mental health. This is based on the notion that about 9 out of 10 people can identify someone having a heart attack, but only 3 out of 10 people know when someone is in mental distress, he said. The condensed training modules include an introduction to concepts and skills from the original curriculum. It is for community members who are interested in mental health education but lack time. This is something NBCC would like to see incorporated into more workplaces.
About the MHF Program
Hinkle described the MHF program as using a train-the-trainer model. The program has also been split into three phases: developing the program, implementing the program, and evaluating the program. The MHF program is past the implementation stage of their train-the-trainer stage; it is currently in the evaluation stage and doing outcomes research. A Syracuse University counseling professor is serving as an outside evaluator doing an outcomes study for the MHF program in Malawi and Mexico. The Educator’s Edition evaluation for the state of Montana took place in summer of 2014.
Another characteristic of the MHF Program is “delivery flexibility,” which allows for the information to be applied to low- and middle-income
countries as well as low-resource areas of developed countries such as the United States. It is an independent, stand-alone training. It is also being infused in academic curricula. Recently, the MHF program was introduced into the academic curriculum at the University of Phoenix. NBCC partnered with the university to bring the MHF program into the human services bachelor’s degree program, which has 10,000 enrollees. These students are being trained in mental health facilitation with the hope of creating a large cohort of facilitators that could serve their local communities now and in the future.
Challenges
Hinkle discussed the challenges he faces in scaling up their MHF program. One is the financial constraints. Most of the work is funded through grants that are brought in to support the work of the MHF program. Given the small staff, there is also a human resource capacity constraint, especially since some of the programs, like that in Malawi, have grown very large and now include such innovations as school clubs and plays related to the MHF training. A second challenge is time constraints; Hinkle pointed out that the curriculum took 2 years to develop, in part because of the large number of consulting partners they involved from all areas of mental health. They included experts in psychiatry, psychology, social work, counseling, and psychiatric nursing. Before rolling the project out, Hinkle and his group piloted it twice in Mexico City.
One reason the program is time-consuming for staff is that it is completely contextualized with the local partner. This is a very important step for Hinkle. For example, Hinkle said that in Bhutan, where there are only two psychiatrists (WHO and Ministry of Health Bhutan, 2006), NBCC has established a very robust program. All of the contextualized details must be worked out before NBCC arrives onsite for the actual training. In this way, the first day of the training is directly applicable to the local situations where the education would be applied. On the last day of the training, the students are asked to apply the information they learned.
Another challenge Hinkle faces is striking a balance between maintaining high-quality control while providing flexibility. Hinkle emphasized that NBCC does not want anyone excluded from their program. Based on the tracking of their trainees—the master trainers, the trainers, and the mental health facilitators—on average, the people who get trained do a lot of good in their communities. Given their proven track record, Hinkle believes he and his colleagues have struck the right balance despite many challenges faced in running such a multifaceted mental health training program.
Hinkle stated that the greatest barrier for mental health treatment and education is stigma and discrimination. For example, in the United States,
40 percent of people who have serious, severe mental health conditions do not get treatment, and the main reason for this is stigma (Narrow et al., 2000). Hinkle says that he deals with this barrier in every country where he works.
Enablers to Success
Hinkle stated that the MHF program does not solicit communities to use their program; rather, the communities seek out the program and make the request for the training. In fact, many community partners hear about the MHF program through word of mouth. The training is also flexible and can be applied to a variety of different communities.
In addition, Hinkle said that having the MHF program sanctioned and promoted by the leaders in the country helps their success. He also mentioned that the partner on the ground has an important role of ramping up the program and encouraging members of their community to attend the training.
ReThinking Community Health Workers:
Building Stewardship and Systems Thinking
Ruth Wageman, ReThink Health and Harvard University
Ruth Wageman specializes in the field of organizational behavior, studying and teaching the design and leadership of task-performing teams. Her work at ReThink Health focuses on creating effective multi-stakeholder leadership teams that work in concert to transform regional health systems.
Leadership Teams
A stewardship team is composed of stakeholders in a regional health system who come together to take responsibility for transforming that system to meet the aspirations of its residents. Some groups, working with members of the ReThink Health team, use a computer simulation of a regional health system to test the impact and implications of policies or interventions they could consider implementing. Developers of the model drew from a host of different studies and scenarios when designing the program in an effort to cover the full array of potential outcomes that could result from a given intervention, among them IHI’s Triple Aim (population health, cost of care, quality of care), as well as outcomes such as productivity, access to primary care, and other measures of community well-being
that stakeholders value.1 Using the simulation, stewardship teams can test the effect of many different suites of interventions before committing any public or private funds toward implementation, as well as reach agreement on a shared set of priorities for the system.
Wageman stated that among the benefits of working together in this way are that stewardship teams and other participants in a region gain more understanding of their local health systems and the roles played by others in the community, and they can ask what it would take to be informed agents of change. Wageman sees an important role in the health system for developing the capacity for change leadership among the community professionals who can actually bring about system change.
Stewardship Teams and Systems Thinking
According to Wageman, an increasing number of groups are convening across different institutions to take responsibility not just for their own institutions but for the management of shared resources across the system and leading on behalf of the whole. Wageman calls these leadership clusters “stewardship groups.”
In describing her work with the stewardship groups, Wageman referred to an underlying system diagram map shown in Figure 3-3. She said that this figure can be thought of as a giant meta-analysis of the research literature about the interconnections among a regional health system. Loosely speaking, the upstream drivers of health are at the top left of Figure 3-3, while elements of the health care system are shown to the right.
The schematic diagram of a regional health system illustrates the many interconnections that produce the set of outcomes that the stewardship groups might care about in a health system. No single person could possibly retain all this information or truly understand all of the interrelations, said Wageman. However, by bringing different institutional leaders together who have knowledge of different parts of the system, it is possible to explore a range of ideas.
ReThink Health’s Computer Simulation
ReThink Health uses computer simulation to help groups to explore a range of ideas to transform their health system. For example, a stewardship group might have a set amount of money to invest in transforming their system but very different views about which initiatives would best
_____________
1 The Institute for Healthcare Improvement (IHI) Triple Aim is a framework for health system performance involving (1) better patient care, (2) improved population health, and (3) reduced health care costs (IHI, 2014).
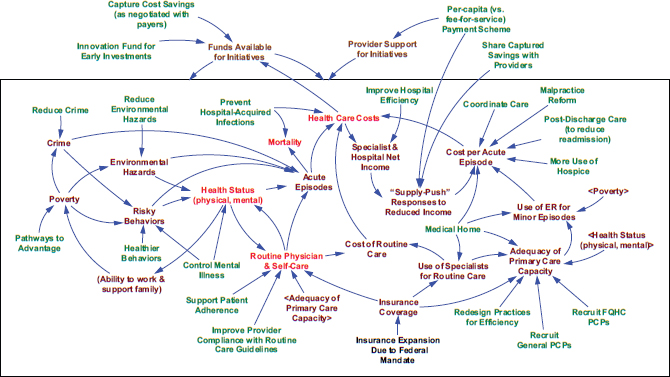
FIGURE 3-3 Schematic diagram of a regional health system.
NOTES: FQHC = federally qualified health center; PCP = primary care provider.
In this diagram, the outcomes are in red text, the interventions are in green text, and the key processes are in brown text. The up-
stream drivers are generally to the left of the diagram, and the downstream initiatives and process are to the right of the document.
The different ways of funding initiatives are at the top of the diagram.
SOURCE: Wageman, 2014. Material original to ReThink Health.
accomplish their goals. The simulation allows the group to test what the effect would be over the course of the next several decades to see what scenarios would enable them to work toward the goals they care about. Some groups that ReThink Health has worked with have tested hundreds of different scenarios, learning from their simulations how different strategies for health system change produce different strengths and weaknesses over time, said Wageman.
For example, one possible challenge that Wageman identified in these theoretical scenarios is that the community runs out of money before producing any significant health improvement outcomes because of the long time lags between project initiation and demonstration of an effect, and because of the need to sustain expensive initiatives for long periods. A stewardship group can then look at investments that might improve the quality of care and reduce some costs in the health system, producing potential savings that might be invested in the program initiatives. Stewardship teams learn and explore by testing suites of initiatives with different timing, sequencing, and degrees of investments. This allows the group to start developing scenarios they might actually be able to accomplish within their local or regional health system.
This exercise engenders a deeper understanding of the various elements of a health system. As the group explores different scenarios, they question why one scenario produced a significant reduction in cost while a fundamentally similar scenario did not. In this way—supporting dialogue with data—Wageman and her colleagues enable stewardship teams to come to agreement on a shared strategy for strengthening their local health system through the suite of tested interventions.
Examples of ReThink Health Stewardship Teams
Wageman provided two examples of groups with whom ReThink Health has worked. The first was located in the upper Connecticut River Valley of Vermont and New Hampshire. That group included leaders from regional businesses, the university, the hospital, the community, and social services. The intent of this group was to invest in community-based population health strategies that would transform their region and become a health system model for the rest of the country.
The other example was the Pueblo Triple Aim Coalition in Pueblo, Colorado. They hoped to simultaneously improve care and population health while lowering costs. They worked with ReThink Health to build a model that would radically improve the state of their health system by better combining and aligning the many different initiatives and programs that were already under way (see Box 3-1).
BOX 3-1
Compelling Scenario for the Future of Pueblo, Colorado
Temporary Innovation Fund = 1 percent of health care spending (i.e., $10M/year for 5 years = $50M)
- Invest in cost-saving initiatives with a stewardship structure for the community to reinvest savings and share a significant fraction of savings with providers.
(invest in coordination of care; invest in postdischarge planning; capture these savings; share these with providers)
- Support self-care and safety net capacity.
(adherence support, safety net recruitment)
- Invest in upstream drivers.
(healthier behaviors, pathways to advantage)
SOURCE: ReThink Health, n.d., as presented by Wageman on May 1, 2014.
Challenges of Spread and Scale-Up
From Wageman’s perspective, one of the challenges to spreading this kind of work to include more leaders is getting leaders in health system organizations to view their role in health system change as one part of their core job responsibilities. Another challenge involves collaborative work. Wageman called for developing the capacity of leaders in the system to establish true system vision, shared stewardship values, and a collective strategy for system transformation.
Wagemen also described some of the barriers to scaling up this kind of work to more locations. First, scale-up is extremely labor-intensive work for those engaged in leading change in their own systems. Second, it is relatively difficult to entice leaders to work outside of their own home regions where their constituencies are located. When leaders do share their lessons learned, there is often a view that such lessons are not applicable to other contexts. Wageman admits some truth to that view that context-specific lessons are valuable and that lessons learned from one location would have to be applied in extremely context-sensitive ways to the new location. But despite this perspective, the most frequently asked questions by these leadership groups are “Who else has gone through this before us?” and “Can we talk to them?” In her opinion, a lot of learning happens when leaders
from different regions are connected directly. This connection provides new stewardship teams the opportunity to ask specific questions to those who have faced similar challenges. Wageman believes that such learning networks can be formed by using virtual connections. These networks will enable the development of stewardship capacities and enhance the work that regional leaders are doing to draw upon the power of shared leadership for overcoming challenges to building stronger, community-based health systems.
Enablers of Success
Wageman identified what in her opinion are the key approaches to developing stewardship capacities. These include
- Innovative action-research (systematic learning from theory-guided interventions) and place-based experiments;
- Evidence-based frameworks and guides for action;
- Real-time ongoing coaching and support of stewardship activities;
- A learning community of groups tackling the presented challenges that is convened across contexts for mutual challenge, support, and learning; and
- A learning community of people who teach, support, and coach these groups.
She also stated that a critical factor to success is a shared sense that the moment is now. There is a sense of urgency, and leaders are committed to finding solutions together, she said.
TECHNOLOGY AND INNOVATIONS IN COMMUNITY-BASED HPE
Forum and workshop planning committee member Gillian Barclay started the session by challenging the notion of technology as the driver for better care, improved population health outcomes, and better value for care. It is about people, she said. Technology cannot be a substitute for the simple foundation of engaging people and asking them what they need and what works for them. That is what a system of health and health care can be built upon to meet the needs of the people based on what they themselves say works for them.
After health system players understand the needs of the people, then it is appropriate to look at the usefulness of technology for improving the practice of health care—including how professions practice and interact—and how to improve health outcomes. With those few introductory comments,
Barclay then introduced the two speakers whose remarks are summarized below.
Camden Coalition of Healthcare Providers
Jeffery Brenner, Camden Coalition of Healthcare Providers
Jeffery Brenner is a family physician who has worked in Camden, New Jersey, for the past 15 years. He began his work in Camden by opening a practice that provided full-spectrum family health services to a largely Hispanic Medicaid population. After recognizing the need for a new way for hospital providers and community residents to collaborate, he founded the Camden Coalition of Healthcare Providers and has served as its executive director since 2003.
The City of Camden, New Jersey, and Its Heath System
Brenner described the city of Camden in his opening comments. It is a densely packed urban environment with rampant poverty and high crime, making it one of the most dangerous cities in the United States. And despite taking up only 9 square miles, it is home to three emergency rooms and two hospitals—one of which is a large academic health center.
After 4 years as a solo practitioner in Camden, Brenner put in motion a membership nonprofit that was the start of the Camden Coalition of Healthcare Providers. The vision for the coalition was to be the first city in the country to bend the cost curve and improve quality. To accomplish this, Brenner and his colleagues set up a board involving community voices from three local hospitals, federally qualified health centers, a variety of specialty and primary care practices, and patient representatives. An advantage to this membership structure is the strong sense of ownership by its members, but, as Brenner soon discovered, it also creates a somewhat chaotic organization and a tremendous amount of work.
Soon after incorporating, the coalition had to operationalize their vision; over time, they came to the realization that they would not focus on public health or primary prevention (keeping healthy people healthy). They would also not address secondary prevention (keeping people with mild versions of chronic illnesses healthy). Instead, the Camden Coalition elected to focus exclusively on tertiary prevention that would help patients recover from harmful medical events, rehabilitate, and then reintegrate back into society. This group, Brenner said, had the greatest potential for savings; with constrained public budgets, this represented the best way for the group to improve the system in a sustainable way.
According to Brenner, the health systems in Camden and other cities around the United States are broken, and a way to fix them is to align en-
gagement with data and systems redesign. He then addressed each of these three pieces for fixing the system individually. Engagement, he said, would not be looked at using conventional health professional educational tools and jargon but would include such unconventional elements as motivational interviewing, harm reduction, change management, community organizing, and coalition building. From Brenner’s perspective, these methods also help to break down hierarchies, owing to their facilitative framework. The data piece would similarly be unconventional, looking more at the outliers than the averages and more at segmentation than stratification and using more real-time surveillance data than predictive modeling. For the last piece, redesign, Brenner expressed the view that it is a systems engineering concept that looks more like a flow chart. Each box in the chart redefines who does what and how they do it within the context of the health care system. Brenner thinks of redesign as moving from “craft and guild operations” to “assembly lines.” This often involves task-shifting delegation.
Brenner reiterated his three necessary elements for fixing the health care problems in Camden as engagement, data, and redesign. According to him, it is easy to accomplish one of these things, and sometimes two, but achieving all three is extraordinarily difficult. This is what the Camden Coalition set out to do.
Understanding System Costs
Much of their work at the Camden Coalition was driven from what Brenner calls a homegrown database that was built with claims data from the three local hospitals. When Brenner and his colleagues assembled the database, they ended up with roughly 12 years of claims data from the hospitals. These included all the identifiers, such as name, address, date of birth, date of admission, and charge receipts. These were downloaded into two $50 hard drives with open source encryption and password protection, and the data were analyzed with a desktop computer and Microsoft Access.
Through analysis of the data, Brenner was able to see the majority of the costs of patients being admitted to the hospitals for a given length of hospital stay. But instead of focusing on the center of the bell-shaped curve, Brenner was interested in the outliers—what he called the “long messy tail of data.” According to Brenner, it is the nonlinear segment of the data that, if carefully analyzed, could provide valuable information about what is right and wrong within the Camden health system. In describing the “long tail,” Brenner described one patient who visited every city emergency department hospital for a total of 113 visits in 1 year and another patient who went 324 times in 5 years. In addition, 1 percent of the patients, said Brenner, represented 30 percent of the community’s health costs that came
to a total of $650 million over 5 years, mostly drawn from public funds (Brenner and Highsmith, 2011).
In an attempt to better understand the systems dynamics, Brenner and his colleagues sought out these high users of the health system to hear from them where the system was failing them. What they at the coalition realized is that by providing better, more coordinated care to the small number of “superusers,” it was possible to improve the quality of care while simultaneously decreasing costs by reducing the number of emergency room visits and inpatient stays.
Health Information Exchange (HIE)
Brenner said that much of this health system coordination was and is accomplished through collaborative data sharing known as the Camden Health Information Exchange (HIE). This is a database that provides real-time information about patients to the 50 coalition staff as well as the patients’ providers. The information includes
- Admissions, discharge, and transfer transactions;
- Laboratory results;
- Radiology reports;
- Medication reconciliation; and
- Discharge summaries (Camden Coalition of Healthcare Providers, 2014a).
He said that the HIE is used to identify patients with complex medical and often social conditions who could benefit from focused interventions provided by the coalition’s care management teams. Brenner said that patients enrolled in the care management program often have difficulty in navigating the health system and become the overusers of the hospital and its emergency care. Criteria for admission into the program involve diagnosis of two or more chronic conditions and treatments involving at least five different medications. Once identified, these patients are registered in the program coordinated by the care management team that assists the patient in navigating the complex health care system. The teams include registered nurses, licensed practical nurses, and health coaches, as well as social work support and/or case workers. Patients are kept in the program until they are medically and socially stable. The patient is then transitioned to the health coach, who provides ongoing support (Camden Coalition of Healthcare Providers, 2014b).
The program, said Brenner, reduces health care costs by avoiding preventable readmissions to the hospital for those patients who are socially stable but medically complex and at risk for overuse of the emergency
department. Patients in this program learn to properly use available medical services, despite possible language barriers and/or low literacy, which are frequent causes for difficulty in navigating health systems and the inappropriate use of services. After learning how to manage their own care, patients are then directed to the their primary care physicians for management of their chronic medical conditions. (Camden Coalition of Healthcare Providers, 2014c).
Camden Coalition Workforce
Health coaches Brenner describes the workforce at the coalition as “homegrown,” just like his data system. The coalition currently uses 10 AmeriCorps volunteers each year. These are college-educated young people, all of whom will be going to medical school, nursing school, or social work schools following their experience in Camden. The volunteers are trained to become health coaches. Following their training, volunteers are paired with the coalition’s nurses and social workers and are sent into the community as the frontline of the coalition’s intervention. Brenner emphasized the value of delegation in this and other instances throughout their care coordination process.
Population health fellows Also on the coalition’s team are two population health fellows that have been supported by the Aetna Foundation for 2 years. These are board-certified family doctors who spend a year with the Camden Coalition to analyze data related to the superuser group. Brenner described it as a “hot spotting” fellowship, in which fellows are presented with an ambiguous problem to figure out by using data and other available resources. They gradually learn to align engagement, data, and redesign to solve the problem. Brenner enjoys watching as the fellows’ knowledge of health systems redesign and unconventional data mining grow and develop. In his opinion, there are not enough clinical champions for population health that have the sorts of creative problem solving that are developed during this fellowship. It is going to be an important, new category of people to expand, he said.
Workforce Challenges
Brenner closed by sharing with the participants some of the enormous workforce challenges he faces in Camden. For example, the community health worker (CHW) model that is built for primary prevention and secondary prevention would not fit with the highly complicated, often end-stage patients with whom they work. Because CHWs are not accustomed
to dealing with or seeing terminally ill patients, their first reaction is to send the patient to the emergency room—which brings the sickest patients back in to the hospital.
To avoid this scenario, Brenner and his colleagues have instead retrained and retasked medical assistants (MAs) and licensed practical nurses (LPNs) for this work. What he has found is that people who have spent many years in medical offices as an MA or an LPN are not shocked by the look or condition of terminally ill people. Also, they are not intimidated by doctors or the overall health care system, so they can carefully and appropriately navigate the best care for their patient.
The other workforce challenge Brenner expressed was a lack of informaticists—people who work creatively with data—in health care. Biostatistics and epidemiology are inadequate training for the sorts of skills required for the creative problem solving they do at the coalition. This sort of work, said Brenner, requires more data generalists than data specialists. He needs people who can use multiple different tools, such as Microsoft Access and visualization software, and who can then be capable of explaining what was uncovered in the data set orally or using a self-developed slide presentation. These skills are better suited to a generalist, said Brenner—not a specialist.
Cross-Site Learning
Brenner and his colleagues spent considerable time working through how to implement a superuser program and build financial sustainability. With funding through the Robert Wood Johnson Foundation and the Center for Medicare & Medicaid Innovations, Brenner and his colleagues are able to provide technical assistance to roughly 15 sites across the country that are attempting to emulate the success of the Camden Coalition. And although Brenner is most committed to helping the City of Camden, he recognizes the importance of state and national work. What he and many others have discovered is that you cannot fix health care without reaching outside of your local community.
Telemedicine in Rural Alaska
Sarah Freeman, Alaska Native Tribal Health Consortium
Sarah Freeman is the Telehealth Program Development Director for the Alaska Federal Health Care Access Network (AFHCAN) department at the Alaska Native Tribal Health Consortium. Her role is to help develop the clinical programs and processes to deliver health care to rural areas via telehealth technologies. Freeman is a pharmacist by training and
had a diverse health care background prior to settling into telemedicine. She has worked in tribal and private sectors as well as in university and rural settings.
The Need for Telemedicine
In 1999, the AFHCAN was created to improve health care access across the state of Alaska. The program was developed because patients are not physically located near their health providers. Freeman showed Figure 3-4 to illustrate the relative size of Alaska, which is often depicted on maps as being much smaller than its actual dimensions. In the Alaska Tribal System, there are six regional hospitals that serve various regions across the state, said Freeman, and most of these are very small, sometimes with only 5 to 10 beds.
The largest tribal hospital is in Anchorage, but given Alaska’s enormous size, its harsh weather conditions, and the lack of road systems in the majority of the state, travel into Anchorage for health care is extremely time-consuming, expensive, and challenging. According to Freeman, flights to Anchorage are expensive and cumbersome (often involving multiple stops on small planes with intermittent flight schedules or boat rides), and the trip is disruptive to patients’ lives.
The Alaska Tribal Health System is a voluntary association serving
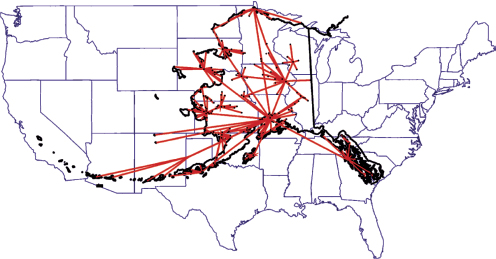
FIGURE 3-4 The Alaska Native Health Care System referral pattern. Same scale
comparison: Alaska area to lower 48 states.
SOURCE: Freeman, 2014.
roughly 130,000 Alaska Native American Indian patients from more than 30 tribes across the state. Seventy percent of those patients live in small rural villages with an average size of 350 residents.
The Alaska Tribal Health System
According to Freeman, most of these communities have no on-site primary care physician or midlevel provider, and 59 percent of the entire state’s residents reside in medically underserved areas (Ferguson et al., 2009).
Local level At the village level, there are 180 small village health centers that employ about 550 community health aide/practitioners (CHAPs). The health aides are typically residents of the community and are hired by their specific tribal health organization to be the hands-on caregivers for their area. This helps foster trust and cultural understanding between the community members and the health worker. The CHAPs are physician extenders, they work out of very small clinics, and they have access to fairly extensive technological tools. The health aides go through a series of four 4-week courses where they are trained in Anchorage in basic health care delivery. They also receive an electronic health care manual, accessible through iPads, that is a guide for triaging patients and providing care. Freeman stated that the Alaska Tribal Health System also has behavioral health aides and dental health aides that work with community members. These individuals are typically stationed in the Alaska Tribal Health System hubs of their spoke-and-hub model.
Alaska referral system The Alaska Native Medical Center (ANMC), located in Anchorage, is the tertiary care and the specialty care provider for the entire state. They use a hub-and-spoke system for referrals. Each of the black dots in Figure 3-4 identifies one of the villages served by the ANMC where the referrals originate. Referrals are first sent to a primary care hub. If the patient requires care beyond what the primary hub can provide, then the patient is referred to ANMC for care. On average, this costs $900 for one plane ticket, which does not include lodging or the price of an escort. Not uncommonly, this is a 3-day journey for a 20-minute visit. As Freeman pointed out, this is an inefficient system creating huge barriers to access care for the patients.
Telemedicine and the Alaska Federal Health Care Access Network
About 13 years ago, AFHCAN was tasked with creating a means of providing access to care for patients living in rural Alaska. Owing to the
poor telecommunications connectivity in Alaska at that time, said Freeman, video teleconferencing with real-time interactions between patients and providers was not a viable option (videoconferencing on a larger scale is now possible because of bandwidth expansion in Alaska within the past couple of years). Instead, the group developed a store-and-forward telemedicine software and hardware system that required less stable connections.
This store-and-forward telemedicine system is still widely used today. The technology involves capturing patient data through various peripheral medical equipment—such as an electrocardiogram, an otoscope, or a stethoscope—and securely transmitting the information to a primary care provider or one of the specialty providers for review. CHAPs are trained to capture clinical data using this equipment. The primary care provider evaluates the patient based on the clinical data received from the community health aide. Based on the data, the provider then decides whether to treat the patient or refer the patient to a specialist. Either way, the patient does not have to travel to Anchorage to physically see the provider. It is what Freeman called asynchronous telemedicine care.
Using the example of a child requiring a cochlear implant, Freeman remarked that in the past the child and his or her family may have had to physically move to Anchorage because of the frequency of the follow-up needed with the ear, nose, and throat specialist. But with the store-and-forward system, an image of the ear can be quickly taken and sent to the specialist in Anchorage without having to remove the child from his or her community. Freeman explained that ear infections and other auditory complications are common in the Alaskan population, so this technology has significantly improved the quality of life of Alaskan families. The technology is used well beyond ear, nose, and throat cases; according to Freeman, there are more than 35,000 cases sent per year through their telemedicine system across Alaska. Both primary care and specialty care services are delivered through this model of care.
Training the Health Workforce
Freeman stated that training community health aides on how to use store-and-forward equipment is essential for the system to function properly. The equipment was designed to be very user-friendly; for example, it has a touch screen that is color coded for simplicity. Health aides are trained on how to use the equipment, and information technology staff are trained on how to service their own equipment.
The technology that the consulting providers in Anchorage use for receiving information from health aides is also designed for simplicity. The Web-based software has the feel of Microsoft Outlook, so it is familiar to the provider and is easy to use to access and respond to cases.
According to Freeman, the Alaska Tribal Health System tends to have a large turnover rate in staff. With more than 1,500 users of the telemedicine system, this represents a significant effort by Freeman and her colleagues to keep up with the large number of new trainees. But despite the high turnover, Freeman feels this model has been working well in Alaska. The evidence is that it is now deployed in 13 different countries around the world, and domestically it is used in at least 17 states besides Alaska.
Challenges
One of the challenges that Freeman noted is working with multiple health organizations to provide consistent care across the state. The consortium works with more than 30 different tribal health organizations, and Freeman believes the collaboration between these sites has been improving significantly over the 8.5 years she has been with Alaska Native Tribal Health Consortium. She believes that part of this improvement is driven by a culture shift of organizations thinking more as a health system rather than as single entities.
Another challenge that AFHCAN faces is that many community health aides leave their jobs because of burnout. They are the only persons in their communities who are seeing all of the health care issues of the community, including serious traumas. They essentially need to be available 24 hours per day, 7 days per week. Health aide work can be very difficult at times as the community health aide may be treating a family member or friend. Freeman also noted that with increased telehealth resources to assist the community health aides remotely, it is easier for them to provide services to their community and burnout may be mitigated.
Occasionally, community health aides may choose to live in more urban areas; after experiencing training there, they elect to stay instead of returning to their communities. However, Freeman stated that this is a rare problem and that the community health aides in training make a commitment to their communities to return after training.
Distance Learning
Freeman’s final remarks involved leveraging technology for advancing the education and skills of the health aides as well as the providers. Freeman commented that with the expanded bandwidth, it is now possible to offer live videoconferences not only for patient visits but also for training. This is an active area of engagement for Freeman and her colleagues because it is a way of educating and updating Alaskan providers residing in more rural areas.
One method they use to facilitate knowledge transfer between provid-
ers is to link physicians on a video teleconference. In one model being used today, an HIV physician specialist can conference with the primary care doctor during the virtual patient visit. This helps provide real-time guidance in how to manage the patient’s care, which is particularly important because HIV is not a common disease to treat in rural Alaska. In this same visit, a pharmacist and health educator or nurse can be part of a conference call to help support all the needs of the patient in one visit. This is an excellent way to communicate the care plan across the multidisciplinary team.
Freeman said that this model is effective for a number of different specialties, including pain management, pediatric subspecialties, and other services.
REFERENCES
Brenner, J., and N. Highsmith. 2011. An ACO is born in Camden, but can it flourish in Medicaid? In Health Affairs Blog. http://healthaffairs.org/blog/2011/06/23/an-aco-isborn-in-camden-but-can-it-flourish-in-medicaid (accessed July 31, 2014).
Camden Coalition of Healthcare Providers. 2014a. Camden health information exchange. http://www.camdenhealth.org/programs/health-information-exchange (accessed July 31, 2014).
Camden Coalition of Healthcare Providers. 2014b. What is a care management team. http://www.camdenhealth.org/what-is-a-care-management-team (accessed July 31, 2014).
Camden Coalition of Healthcare Providers. 2014c. What is the care transitions team. http://www.camdenhealth.org/what-is-the-care-transitions-team (accessed July 31, 2014).
Ferguson, A. S., J. Kokesh, C. Patricoski, P. Hofstetter, and N. Hogge. 2009. Impact of store- and-forward telehealth in Alaska: A seven-year retrospective. Anchorage: Alaska Native Tribal Health Consortium.
Freeman, S. 2014. Technology and innovations in community-based HPE. Presented at the IOM workshop: Scaling up best practices in community-based health professional education. Washington, DC, May 1.
Hinkle, S. 2014. Spreading community-based innovations. Presented at the IOM workshop: Scaling up best practices in community-based health professional education. Washington, DC, May 1.
IHI (Institute for Healthcare Improvement). 2014. The IHI Triple Aim. http://www.ihi.org/offerings/Initiatives/TripleAIM/Pages/default.aspx (accessed July 3, 2014).
Narrow, W. E., D. A. Regier, G. Norquist, D. S. Rae, C. Kennedy, and B. Arons. 2000. Mental health service use by Americans with severe mental illnesses. Social Psychiatry and Psychiatric Epidemiology 35(4):147-155.
ReThink Health. n.d. Setting strategy: Pueblo, CO. http://www.rethinkhealth.org/case-studies/setting-strategy (accessed September 29, 2014).
Rogers, E. M. 1962. Diffusion of innovations. First ed. New York: Free Press.
Wageman, R. 2014. Spreading community-based innovations. Presented at the IOM workshop: Scaling up best practices in community-based health professional education. Washington, DC, May 1.
White, K. L., T. F. Williams, and B. G. Greenberg. 1961. The ecology of medical care. New England Journal of Medicine 265(18):885-892.
WHO (World Health Organization) and Ministry of Health Bhutan. 2006. WHO-AIMS report on mental health system in Bhutan. Thimphu, Bhutan: World Health Organization.
























