
Public health’s mission is to ensure those conditions necessary for people to be healthy (IOM, 1988). The public health sector is unique in that its three core functions—assessment, policy development, and assurance (see Box 5-1)—are the foundation for a community’s capability to address human needs, including those related to disasters. Because these functions cut across all other recovery domains (e.g., housing, transportation, health care delivery), successful recovery requires that the public health sector galvanize and lead an interdisciplinary, team-based approach to the continual assessment of health status and needs, the development and prioritization of plans and policies for addressing those needs, and the assurance of access to essential health services throughout the continuum of disaster response and recovery.
Given that components of the public health recovery mission cut across all other sectors, public health is integral to all of the committee’s recommendations (as noted throughout this chapter) and is woven throughout this report. However, this chapter outlines specific tasks for the public health sector to support
BOX 5-1
Core Public Health Functions
Assessment—regularly and systematically collecting, assembling, analyzing, and making available information on the community’s health, including health status, health needs, and causes of health problems.
Policy Development—facilitating evidence-based decision making in matters that impact public health and mobilizing the community in the development of public health policy that meets local needs.
Assurance—assurance that the full complement of services necessary to protect the public’s health are accessible to all members of the community, either by providing such services directly, or encouraging other public or private entities to do so, using regulatory requirements when necessary.
SOURCE: IOM, 1988.
implementation of the committee’s recommendations, and it describes the capabilities and resources that empower public health in the recovery process both pre- and post-disaster. In developing this guidance, the committee identified a number of key recovery strategies, which serve as cross-cutting themes throughout the chapter and apply to multiple pre- and post-disaster activities. Use of these strategies will facilitate the integration of health improvement into recovery planning before and after a disaster:
- Leverage existing relationships and networks (e.g., coalitions, collaboratives) to integrate public health and other community partners into recovery planning.
- Identify opportunities for alignment between ongoing public health improvement processes (e.g., accreditation prerequisites of community health assessments and community health improvement plans) and recovery planning.
- Educate nonhealth sectors and the community on why health is integral to recovery and how recovery activities impact health outcomes.
- Use and expand health technology infrastructure for data collection and analysis to facilitate data sharing, evidence-based decision making, and continual evaluation of progress toward an optimally healthy community.
The chapter concludes with a checklist of key activities that the public health sector needs to perform during pre-event planning, short-term recovery, and intermediate- to long-term recovery.
PUBLIC HEALTH IN THE CONTEXT OF A HEALTHY COMMUNITY
The public health sector has a central role to play in the realization of a healthy community. (Elements of a healthy community are detailed in Chapter 2, Box 2-2.) The process of creating healthier communities is not linear and has no end point; it is a continuous cycle (see Figure 5-1). Public health agencies and nongovernmental organizations protect and promote the health of individuals and communities through direct provision of health services, regulatory roles, education and advocacy efforts, sharing of health information to inform decision making, and creating and leveraging community partnerships. Through such measures (which are discussed in more detail throughout this chapter), the public health sector can spur within a community what the Robert Wood Johnson Foundation (RWJF) calls a culture of health. A culture of health encompasses a broader vision of what it means to be healthy, extending beyond health care to include work, family, and community life. According to RWJF, the characteristics of an American culture of health include
- “good health flourishes across geographic, demographic and social sectors;
- attaining the best health possible is valued by our entire society;
- individuals and families have the means and the opportunity to make choices that lead to the healthiest lives possible;
- business, government, individuals, and organizations work together to foster healthy communities and lifestyles;
- everyone has access to affordable, quality health care because it is essential to maintain, or reclaim, health;
- no one is excluded;
- health care is efficient and equitable;
- the economy is less burdened by excessive and unwarranted health care spending;
- the health of the population guides public and private decision-making; [and]
- Americans understand that we are all in this together” (RWJF, 2014, p. 5).
As discussed in Chapter 2, a healthy community is a prepared and resilient community. Planning for health improvement, recovery, and disaster response during steady-state periods should be concurrent,
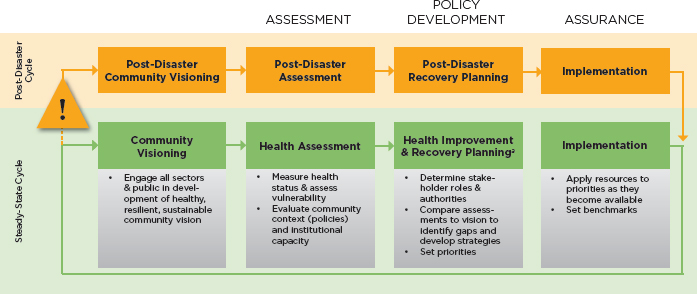
NOTE: This figure can assist public health agencies in articulating roles in and the cyclical nature of planning for health improvement and disaster recovery and encouraging pre-disaster recovery planning as a best practice.
a Disaster response planning also occurs during this phase and should be integrated with the recovery planning process to ensure integration across the emergency management phases and coordination of efforts and funding.
as illustrated in Figure 5-1. As discussed in Chapter 3, integration of health improvement and recovery planning ensures that a clear vision for a healthy, resilient, and sustainable community (and priorities for achieving that vision) is in place before a disaster to drive recovery activities. It should be noted that delineations between the phases in the cycle depicted in Figure 5-1 are not black and white, and various sectors engaged in these processes may be involved in different activities at any given time. Activities within sectors also may vary.
A disaster, which can occur in the community at any point in the steady-state health improvement cycle, initiates an event-specific cycle (detour) that mirrors the pre-disaster process, with cyclical phases of visioning, assessment, planning, and implementation. The diasater cycle persists until such time as the community transitions to a “new normal.” This process can take years or even decades. The public health functions described in the following sections are a part of this phased approach to healthy community planning.
DISASTER-RELATED PUBLIC HEALTH CHALLENGES
As discussed in Chapter 2, a healthy community is contingent upon the optimal functioning and integration of the full spectrum of community and health services on which people depend to survive and thrive. A disaster can disrupt these systems directly through short-term impacts such as damage to health care facilities and indirectly through impacts such as destruction of other critical physical infrastructure (e.g., utilities, transportation, housing) and deterioration of the capacity of essential health and social services to meet a surge in post-disaster human needs. In the long term, a community’s health may be impacted directly by an exodus of health care professionals (Berggren and Curiel, 2006; Rudowitz et al., 2006) or indirectly by unintended consequences of recovery decisions (e.g., unaddressed blight that deteriorates neighborhoods and is associated with increased crime).
After a disaster, the public health sector faces challenges well beyond the initial response phase because not only must it galvanize a multisectoral recovery effort to address long-term health needs, it must do so while also remaining focused on carrying out the core day-to-day functions of fostering good health, offering protection from unsafe or hazardous conditions, preventing disease, and disseminating credible health information. Lessons from the aftermath of the terrorist events of September 11, 2001, demonstrate the importance of balancing the crisis response and routine public health functions (Klitzman and Freudenberg, 2003). A public health system overburdened by existing health disparities before a public health emergency may be the least well equipped to maintain this balance (Runkle et al., 2012). Prior to Hurricane Katrina, for example, one quarter of the New Orleans population lived below the poverty level, and one in five were uninsured. The devastating and long-lasting aftereffects of the hurricane resulted in an overwhelming load on an already overburdened health system (Center for Disaster Philanthropy, 2012). A public health system that is just barely able to support a population on a day-to-day basis will be overwhelmed after a disaster strikes, weakening the recovery process for the overall health system, which in turn will hinder recovery for the community. The trajectory of recovery will depend not only on the characteristics of the disaster but also on the pre-event health (physical, behavioral) and social well-being of the population and the extent of pre-disaster preparation for response and recovery (Chandra et al., 2011). Thus, improving the health of communities is not just an ethical imperative; it must be viewed as a matter of national security and supported accordingly (HHS, 2009). Resilience to all manner of hazards depends not only on robust health systems but also on a robust population (Morton and Lurie, 2013).
The restoration of services and infrastructure, although critical and often regarded as full recovery, is not an end point in itself. The committee holds that within the tragedy of a disaster lies a unique opportunity for a community to reenvision itself through the lens of a healthy community. By leveraging new funding sources, partnerships, and technologies and redirecting existing funding streams, the process of recovery can be exploited to address previously identified gaps in a community, strengthen and expand existing programs and partnerships, and engage the community in a process of envisioning and building a better post-disaster future. Existing recovery guidance for the public health sector (discussed later in this chapter) focuses on the restoration of public health (as well as health care and behavioral health1) systems and mitigation of damage from future incidents. Greater recognition is needed of the broader public health responsibilities related to the building of healthier communities, including the social and physical environments, after disasters.
PUBLIC HEALTH SECTOR ORGANIZATION AND RESOURCES
The public health system comprises numerous governmental and nongovernmental organizations, working collectively to create conditions in which people can be healthy (IOM, 2003) (see Figure 5-2). In the disaster context, public health cuts across all other sectors because the ultimate goal for all preparedness, response, and recovery activities is the protection and betterment of the health and well-being of people (NBSB, 2014).
The Federal Public Health Enterprise2
The U.S. Department of Health and Human Services (HHS) is the main federal department tasked with protecting and improving the nation’s health, and all agencies within it have roles in assuring public health through preparedness, response, and recovery activities. The Assistant Secretary for Preparedness and Response (ASPR) is responsible for coordinating, on behalf of the HHS Secretary, the HHS response activities under Emergency Support Function (ESF) #8 of the National Response Framework (Public Health
________________
1 For the purposes of this report, the term “behavioral health” encompasses “the interconnected psychological, emotional, cognitive, developmental, and social influences on behavior, mental health and substance abuse” (HHS, 2014a, p. 4).
2 A broader synopsis of legislation and federal policy related to disaster recovery and health security can be found in Appendix A.

FIGURE 5-2 Key stakeholders in a healthy community.
and Medical Services), as well as recovery activities under the Health and Social Services Recovery Support Function (RSF) of the National Disaster Recovery Framework (NDRF), which is described in more detail in Chapter 3. Core mission areas for ESF #8 and the Health and Social Services RSF are listed in Box 5-2. Within these mission areas, public health activities include assessing the impact of the disaster; restoring the capacity of systems to meet post-disaster needs; ensuring the well-being of vulnerable populations, such as people with disabilities and the elderly; and providing the public with appropriate and accessible information. Although this report focuses primarily on recovery, it is important to recognize the need for integration across the two frameworks and the associated operational activities. Successful recovery will depend in part on the effectiveness of response activities.
In addition to its federal coordinating role for disaster response and recovery activities, HHS helps state, local, tribal, and territorial public health and health care organizations carry out strategic planning for preparedness, response, and recovery through grant funding (cooperative agreements). Public Health Emergency Preparedness (PHEP) cooperative agreement and Hospital Preparedness Program (HPP) funds are distributed on an annual basis by the Centers for Disease Control and Prevention (CDC) and ASPR, respectively, to all 50 states, 4 major metropolitan areas, and a handful of U.S. territories. These agencies have developed aligned sets of public health and health care preparedness capabilities (see Table 5-1) to guide the use of grant funds and prepare grantees to carry out the ESF and RSF functions described above (ASPR, 2012; CDC, 2011). This alignment of programs has enabled better coordination of the use of funds for preparedness activities at the state and local levels. The PHEP cooperative agreement funds preparedness activities aimed at cultivating emergency-ready, flexible, and adaptable public health departments. The Community Recovery capability is intended to help community partners “plan and advocate for the rebuilding of public health, medical, and mental/behavioral health systems to at least a level of functioning comparable to pre-incident levels, and improved levels where possible” (CDC, 2011, p. 10)
BOX 5-2
Core Mission Areas for Health-Related Emergency and Recovery Support Functions
Core mission areas under the Public Health and Medical Services Emergency Support Function (ESF #8)a
- Assessment of public health/medical needs
- Health surveillance
- Medical care personnel
- Health/medical/veterinary equipment and supplies
- Patient evacuation
- Patient care
- Safety and security of drugs, biologics, and medical devices
- Blood and blood products
- Food safety and security
- Agriculture safety and security
- All-hazard public health and medical consultation, technical assistance, and support
- Behavioral health care
- Public health and medical information
- Vector control
- Potable water/wastewater and solid waste disposal
- Mass fatality management, victim identification, and decontaminating remains
- Veterinary medical support
Core mission areas under the Health and Social Services Recovery Support Functionb
- Public health
- Health care services
- Behavioral health
- Environmental health
- Food safety and medical products
- Responders’ long-term health
- Social services
- Referral to case management
- Children in disasters
SOURCES:
a Excerpted from FEMA, 2008, p. 1-2.
b ASPR, 2015.
(see Box 5-3). Recovery involves identifying and monitoring recovery needs, coordinating recovery operations, and implementing corrective actions to mitigate damages from future incidents.
The CDC, whose mission is to protect America from health, safety, and security threats, is in a unique position to support a healthy community approach to disaster recovery. In addition to its support for preparedness activities through the PHEP cooperative agreement, the CDC has a number of programmatic activities and grants focused on advancing healthy and safe communities that could be leveraged after a disaster. As is the case for many other governmental and professional organizations involved in both preparedness and healthy community development, however, the two efforts are poorly connected. An important opportunity is being missed to expand and leverage the PHEP guidance on recovery capabilities to encourage grantees to incorporate a healthy community vision into recovery planning before and after disasters.
Although community health improvement is a key CDC programmatic area, it is important to note that many other departments across the federal government support the development of healthier communities. The Partnership for Sustainable Communities, for example, which promotes and coordinates improvements in transportation, housing, and land use, is a joint project of the U.S. Department of Housing and
| PHEP Capabilitiesa | HPP Capabilitiesb |
| Community preparedness | Health care system preparedness |
| Community recovery | Health care system recovery |
| Emergency operations coordination | Emergency operations coordination |
| Emergency public information and warning | |
| Fatality management | Fatality management |
| Information sharing | Information sharing |
| Mass care | |
| Medical countermeasure dispensing | |
| Medical material management and distribution | |
| Medical surge | Medical surge |
| Non-pharmaceutical interventions | |
| Public health laboratory testing | |
| Public health surveillance and epidemiological investigation | |
| Responder safety and health | Responder safety and health |
| Volunteer management | Volunteer management |
a CDC, 2011.
b ASPR, 2012.
Urban Development (HUD), the U.S. Environmental Protection Agency (EPA), and the U.S. Department of Transportation (DOT). Through the Partnership, which was formalized in 2009, these departments are working together to align policies, funding opportunities, and technical assistance to “better serve American communities” (DOT et al., 2014, p. 2). As discussed in Chapter 2, health and sustainability are closely interconnected, and sustainability initiatives often yield co-benefits to health. Thus, many of the activities supported by the Partnership and its component departments individually (e.g., mixed-use development, affordable housing initiatives, and protection of open green space) are relevant to post-disaster efforts to build healthier communities. In fact, the committee noted that in the post-disaster context, EPA and the other members of the Partnership are leading these efforts under the banner of sustainability and smart growth, facilitated through a 2010 memorandum of agreement between the Federal Emergency Management Agency (FEMA) and EPA (DHS and EPA, 2010). The committee found little evidence of CDC involvement in post-disaster recovery sustainability initiatives led by Partnership agencies. Given the opportunities for the CDC noted above, the committee believes the agency’s increased engagement in Partnership efforts to support post-disaster recovery could (1) help ensure that health considerations are explicitly included in recovery-related sustainability initiatives, (2) avoid separate and potentially duplicative activities across government agencies, and (3) encourage public health professionals at the state and local levels to expand recovery responsibilities beyond the restoration of public health services and participate in a more comprehensive discussion on building healthier post-disaster communities.
State and Local Health Departments
State, local, tribal, and territorial health departments are the backbone of the public health system (IOM, 2003). They are responsible for conducting epidemiology and surveillance activities to prevent
Under the Public Health Preparedness Capabilities: National Standards for State and Local Planning, funding allocated for the Community Recovery capability should be focused on enabling the following three critical functions, each of which specifies several tasks and planning resource elements:
Function 1—Identify and monitor public health, medical, and mental/behavioral health system recovery needs.
Task 1: In collaboration with jurisdictional partners, document short-term and long-term health system delivery priorities and goals.
Task 2: Identify the services that can be provided by the public health agency and by community and faith-based partners that were identified prior to the incident as well as by new community partners that may arise during the incident response.
Task 3: Activate plans previously created with neighboring jurisdictions to provide identified services that the jurisdiction does not have the ability to provide during and after an incident.
Task 4: In conjunction with healthcare organizations (e.g., healthcare facilities and public and private community providers) and based upon recovery operations, determine the community’s health service priorities and goals that are the responsibility of public health.
Function 2—Coordinate community public health, medical, and mental/behavioral health system recovery operations.
Task 1: Participate with the recovery lead jurisdictional agencies (e.g., emergency management and social services) to ensure that the jurisdiction can provide health services needed to recover from a physical or mental/behavioral injury, illness, or exposure sustained as a result of the incident, with particular attention to the functional needs of at-risk persons (e.g., those displaced from their usual residence).
Task 2: In conjunction with jurisdictional government and community partners, inform the community of the availability of mental/behavioral, psychological first aid, and medical services within the community, with par-
epidemics and the spread of disease, preventing injuries, providing laboratory services, protecting against environmental hazards, promoting healthy behavior, ensuring quality and accessible health services, and responding to disasters and assisting in community recovery. Although public health agencies are ubiquitous across the nation, health departments vary greatly from jurisdiction to jurisdiction in
- governance3 and organizational structure;
- size relative to the population; and
- roles, responsibilities, and authorities (NACCHO, 2014a).
In addition to variation across jurisdictions, responsibilities and authorities at the state and local levels may vary as well. For example, state public health agencies may have more responsibility than their local-level counterparts related to ensuring access to health care. This variability in responsibilities and governance among state and local public health agencies must be taken into consideration in national-level planning efforts and policy development as it will translate to variable roles and authorities, as well as
________________
3 Some local health departments are local or regional units of the state health department (i.e., centralized), others are agencies of the local government, and still others are governed by both state and local authorities (called shared governance, accounting for 6 percent of states) (NACCHO, 2014a).
ticular attention to how these services affect the functional needs of at-risk persons (including but not limited to children, elderly, their caregivers, the disabled, or individuals with limited economic resources).
Task 3: Notify the community via community partners of the health agency’s plans for restoration of impacted public health, medical, and mental/behavioral health services.
Task 4: Solicit community input via community partners regarding health service recovery needs during and after the acute phase of the incident.
Task 5: Partner with public health, medical, and mental/behavioral health professionals and other social networks (e.g., faith-based, volunteer organizations, support groups, and professional organizations) from within and outside the jurisdiction, as applicable to the incident, to educate their constituents regarding applicable health interventions being recommended by public health.
Task 6: In conjunction with jurisdictional government and community partners, inform the community of the availability of any disaster or community case management services being offered that provide assistance for community members impacted by the incident.
Function 3—Implement corrective actions to mitigate damages from future incidents.
Task 1: In conjunction with jurisdictional government and community partners, conduct post-incident assessment and planning as part of the after action report process that affects short- and long-term recovery for those corrective actions that are within the control and purview of jurisdictional public health, including the mitigation of damages from future incidents.
Task 2: Collaborate with sector leaders to facilitate collection of community feedback to determine corrective actions.
Task 3: Implement corrective actions for items that are within the scope or control of public health to affect short- and long-term recovery, including the mitigation of damages from future incidents.
Task 4: Facilitate and advocate for collaborations among government agencies and community partners so that these agencies can fulfill their respective roles in completing the corrective actions to protect the health of the public.
SOURCE: Excerpted from CDC, 2011.
access to resources, in disaster preparedness, response, and recovery. As a result, the committee’s recommendations and guidance (like other national-level guidance materials) will have to be considered in the local context. In all cases, strong relationships with elected officials are critical to ensure funding and political support for health-related policies.
Although public health involvement in pre- and post-disaster community planning for recovery presents a new challenge for the sector, it should be recognized that many of the essential capabilities required for successful recovery are already in place in communities. These capabilities within different jurisdictions may vary, as well as the availability of resources needed for full implementation. Nevertheless, the committee has identified alignments among activities requisite for public health accreditation, performance of the ten essential public health services,4 and the development of plans and procedures recommended under HHS preparedness guidance (PHEP and HPP) and FEMA recovery guidance (NDRF) that may be exploited to achieve recovery goals (see Table 5-2 for illustrative examples of potential alignments).
Unfortunately, the ability of state and local health agencies to carry out essential public health
________________
4 Following a 1988 report of the Institute of Medicine (IOM, 1988) that defined the 3 core public health functions (assessment, policy development, and assurance), the 10 essential public health services were developed as a framework for public health activities that all communities should undertake. These 10 essential services are generally accepted as minimum functions for health departments and serve as the foundation for the National Public Health Performance Standards (CDC, 2014b; NACCHO, 2011).
| 10 Essential Public Health Servicesa | Public Health Accreditation Board Standardsb | Associated Disaster Preparedness and Recovery Functionsc |
|
1 Monitor health status to identify and solve community health problems |
Conduct and disseminate assessments focused on population health status and public health issues facing the community |
Pre-disaster community health assessment to inform recovery planning (vulnerabilities, unmet needs)
|
|
2 Diagnose and investigate health problems and health hazards in the community |
Investigate health problems and environmental public health hazards to protect the community |
Post-disaster assessment of disaster impact on health and medical needs (including environmental health hazards)
|
|
3 Inform, educate, and empower people about health issues |
Inform and educate about public health issues and functions |
Public messaging (health and safety risks, access to resources); health literacy as it relates to recovery; management of expectations
|
|
4 Mobilize community partnerships and action to identify and solve health problems |
Engage with the community to identify and address health problems |
Community partner engagement in health aspects of recovery
|
| 10 Essential Public Health Servicesa | Public Health Accreditation Board Standardsb | Associated Disaster Preparedness and Recovery Functionsc |
|
5 Develop policies and plans that support individual and community health efforts |
Develop public health policies and plans |
Participation in recovery planning to ensure that short- and long-term population health needs are considered
|
|
6 Enforce laws and regulations that protect health and ensure safety |
Enforce public health laws |
Advocate for changes to codes that improve resiliency
|
|
7 Link people to needed personal health services and assure the provision of health care when otherwise unavailable |
Promote strategies to improve access to health care |
Support for clinical care sector recovery to ensure population access to needed health care providers
|
|
8 Assure a competent public and personal health care workforce |
Maintain a competent public health workforce |
Expansion of workforce capacity as needed to meet community recovery needs
|
|
9 Evaluate effectiveness, accessibility, and quality of personal and population-based health services |
Evaluate and continuously improve processes, programs, and interventions |
Continual assessment of health status and progress toward recovery goals to inform planning and develop and share lessons learned
|
|
10 Research for new insights and innovative solutions to health problems |
Contribute to and apply the evidence base of public health |
|
NOTE: This table can assist public health agencies in identifying existing departmental assets for recovery.
a CDC, 2014b.
b PHAB, 2013.
c CDC, 2011; FEMA, 2011.
functions—including ensuring the health of communities and preparing for disasters and other hazards—is compromised by continuing budget cuts and the resultant loss of workforce capacity. Local health departments have lost 44,000 jobs since 2008. In 2012, almost half of all local health departments cut health services, and emergency preparedness was among the areas most affected (NACCHO, 2013). These cuts in staff, programming, and funding mean that local health departments are less able to provide essential services, whether in steady-state times or during and after a disaster. During a large-scale disaster, public health departments need to be able to leverage the entire agency workforce to meet surge needs. During Hurricane Katrina, for example, personnel as varied as mosquito control sprayers, restaurant inspectors, and staff of the Special Supplemental Nutrition Program for Women, Infants, and Children (WIC) were tapped for the disaster response efforts (Shah, 2014). When health departments lose staff—from any part of the department—it affects their ability to effectively respond to disasters.
Public Health Partners for Healthier Post-Disaster Communities
As depicted in Figure 5-2, a number of organizations are included in broad descriptions of the public health system because of their demonstrated influence on population health outcomes, although some, such as planning and community development organizations, would not traditionally consider themselves part of the public health sector. Both in normal times and after a disaster, public health agencies can act as integrators, leveraging partnerships with health and traditionally nonhealth sectors to drive improvements in health at the individual and community levels. However, the success of the public health sector in disaster recovery depends heavily on pre-planning, knowledge of pre-disaster community demographics and health status, and knowledge of and partnerships with other governmental and nongovernmental sectors to ensure alignment of priorities and activities. Public health needs to have effective relationships in place with other governmental and nongovernmental stakeholders across sectors (e.g., housing, behavioral health, transportation, education) before a disaster to ensure that the actions that each sector takes during recovery not only will accomplish that sector’s primary function but also will advance improved health outcomes and a healthier post-disaster community. As described in Chapter 2, this type of approach has been termed Health in All Policies (HiAP), which is described as “a collaborative approach to improving the health of all people by incorporating health considerations into decision-making across sectors and policy areas” (Rudolph et al., 2013, p. 5). The development of cross-sector collaborations to support HiAP will depend on an understanding among other sectors of the assets public health can bring to the table (see Box 5-4).
Health Care Providers
The interface between public health agencies and health care providers at the state and local levels is variable. Governmental public health agencies can act in a direct health care delivery role, sometimes running various care delivery systems such as public hospitals, nursing homes, psychiatric and substance abuse centers, rehabilitation hospitals, provider networks, and community health centers. More often, public health agencies with care delivery roles are gap fillers in the community, assisting those in need in accessing services. For example, the public health department may run clinics for the homeless or uninsured. The state or local public health agency may also be the regulatory entity in a given jurisdiction, with authority extending to facilities, health care provider licensing, and other responsibilities.
This close connection between public health and health care delivery systems has myriad implications for pre- and post-disaster public health activities. Disasters place heightened demands on health care services, demands that can also strain public health agencies with health care responsibilities (the role of the health care delivery system in disaster recovery is discussed in depth in Chapter 6). Working to facilitate the restoration of the health care delivery system should be one of the primary responsibilities of public health after a disaster (ASTHO, 2007). Public health agencies may collaborate with health care delivery partners through
In building cross-sector collaboratives for health improvement planning before and after disasters, stakeholders need to be aware of the assets that the public health sector brings to the table. Relevant public health areas of expertise identified by the committee include
- early childhood development;
- data analysis, including use of geographic information systems;
- social network analysis;
- public health and health care economics;
- clinical—chronic and acute disease states;
- epidemiology;
- policy and legislative actions;
- health education;
- preventive medicine;
- public health– and health care–related legal issues;
- ethical issues;
- lead poisoning;
- continuous quality improvement;
- oral health;
- vital statistics;
- immunizations; and
- special-needs populations.
- risk and threat assessments, both community-wide and for specific facilities;
- evaluation of overall community health status;
- evaluation and identification of at-risk/vulnerable populations;
- evaluation of services needed and identification of mechanisms for filling gaps;
- assessment of local capabilities to fulfill ESF #8 responsibilities;
- engagement of the health care system, ideally through local health care coalitions5 (discussed further in Chapter 6), in healthy community planning, disaster response, and optimal healthy community recovery; and
- collaboration with behavioral health/substance abuse service providers and social services providers.
The federal government has taken steps to promote alignment between preparedness planning conducted by public health and health care systems by jointly awarding PHEP and HPP grants. The goals of this alignment are to promote cross-sector planning, training, and exercising as well as to reduce the administrative burden for grant recipients. This cooperation between sectors can make disaster planning more efficient and the health system more robust and resilient in the face of a disaster. The Patient Protection and Affordable Care Act6 (ACA) is facilitating increased alignment between the two sectors,
________________
5 Health care coalitions consist of a collaborative network of health care organizations and their respective public and private sector response partners within a defined region. They serve as a multi-agency coordinating group that assists emergency management and Emergency Support Function (ESF) #8 with preparedness, response, recovery, and mitigation activities related to health care organization disaster operations (ASPR, 2012).
6 The Patient Protection and Affordable Care Act, Public Law 111-148, 111th Cong., H.R.3590 (March 23, 2010).
particularly with regard to the use of population-level data from health information systems to improve surveillance and service delivery (IOM, 2014). Moreover, the ACA requirement that nonprofit hospitals conduct community health needs assessments motivates collaborative efforts with public health agencies that are also conducting such assessments.
Behavioral Health and Social Services Providers
Disasters can cause or exacerbate behavioral health issues, and social services providers can become overwhelmed by the increased need for their services after a disaster. Public health is a natural partner to these sectors because the client populations served by behavioral health and social services correspond closely to the key populations at risk for adverse health outcomes after a disaster (White, 2014). Consequently, collaboration between public health and these sectors can vastly improve the health and well-being of affected individuals and communities after a disaster. In Galveston, Texas, for example, a preexisting and ongoing coalition of the Galveston County Health District, the Gulf Coast Center (the regional mental health authority), and local social services providers proved invaluable when Hurricane Ike struck. After the hurricane, the coalition sprang into action using already-proven methods such as telepsychiatry and mobile crisis response teams to reconnect clients with services, meet mental health needs, and simultaneously help clients apply for needed federal assistance (UTMB, 2011). By collaborating before a disaster strikes, public health, behavioral health, and social services providers can improve the care provided to individuals, share resources, and reduce the burden on individual sectors and organizations.
The following committee recommendations are applicable to this public health priority area:
- Recommendation 8: Develop a National Disaster Behavioral Health Policy. (see Chapter 7)
- Recommendation 9: Develop an Integrated Social Services Recovery Framework. (see Chapter 8)
Emergency Management and Public Safety Entities
Emergency managers and emergency medical services/fire departments have key roles in pre-disaster planning and post-disaster coordination (e.g., evacuation, distribution of medical countermeasures). In recent years, homeland security grant programs such as the Metropolitan Medical Response System and Urban Area Security Initiative programs have been integral in promoting better integration of local emergency management, public health, and medical systems (e.g., health care coalitions). In addition to their responsibilities for ensuring the safety of people and property, law enforcement agencies are also increasingly involved in health care response and recovery planning groups and are often employed in specific roles supporting the public health and health care sectors after a disaster, such as distribution of cached supplies and security for the receipt and movement of medical materials from federal stockpiles. As a critical early component of the community planning process, emergency managers and public safety agencies may partner with public health and health care stakeholders to develop hazard or threat vulnerability analyses.7 These assessments are integral in identifying and prioritizing issues for planners.
During the early recovery period, public safety personnel are key partners in outreach efforts to inform the public on such issues as avoiding health and safety threats and scams. The relationships forged between public health officials and emergency management/public safety entities during preparedness activities related to response planning can be leveraged to ensure that public health is also engaged in recovery planning.
________________
7 Hazard or threat vulnerability analysis is a “systematic approach to identifying all hazards [and threats] that may affect an organization, assessing the risk (probability of hazard or threat occurrence and the consequence for the organization) associated with each hazard [or threat] and analyzing findings to create a prioritized comparison of hazard [and threat] vulnerabilities. The consequence, or vulnerability, is related to both the impact on organizational function and the likely service demands created by hazard [or threat] impact” (HHS, 2007, p. D-6).
Recreational and Natural Resources Organizations
Public health and recreational/natural resources organizations have cross-cutting areas of interest and can be partners in the creation of healthier communities through the development and maintenance of community features that promote active living, such as bike and walking paths, as well as green spaces community members can use to congregate. These kinds of projects (e.g., trails) may fall within the Natural and Cultural Resources RSF of the NDRF, but public health organizations can support their implementation through advocacy efforts and active partnerships between public health and recreational professionals and by providing data to support the strategic placement of resources so as decrease health disparities.
Environmental Health Agencies
Governmental environmental health agencies can be housed within the state or local public health department or may be separate entities. In either case, the two must work in partnership to assess the interrelationships between people and their environment and to foster a safe and healthy environment. Cross-cutting functions include monitoring to identify and mitigate health threats from adulterated food and poor water and air quality, disease vectors, and pests. In partnership with the housing sector, public health and environmental health agencies may also play a role in mitigating health risks (e.g., mold, debris) for recovery workers and homeowners involved in cleaning and reconstruction of housing (see Chapter 10) and other indoor environments. Given the potential negative impacts of disasters on environmental quality (both indoor and outdoor), respective roles and responsibilities of these two sectors, as well as mechanisms for their collaboration, should be discussed as part of pre-disaster planning. A process for joint operations, such as health assessments and risk identification and enforcement, during the response and recovery phases should be in place.
Planning and Community Development Entities
Health concerns are increasingly falling within the purview of urban and regional planning departments (e.g., climate change-related issues) and the public health field has discovered the power of comprehensive plans and other planning tools for altering the physical and social environments that impact health. Partnerships with urban and regional planning agencies are critical to ensuring that a healthy community vision and health improvement priorities are incorporated into the community’s strategic (comprehensive) plan (see Recommendation 1 in Chapter 3). These partnerships can then be leveraged during recovery to ensure that the health implications of planning decisions are considered through such mechanisms as health impact assessments (discussed in Chapter 3).
Partnerships with community development organizations also represent important opportunities to create physical and social environments that better support health and, in particular, to address health equity issues. The community development enterprise is a network of governmental, nongovernmental, and private organizations (e.g., banks, real estate investors) working together to transform impoverished, blighted neighborhoods and improve quality of life and economic security for low- and middle-income individuals by investing in affordable housing and access to community services and amenities (e.g., child care centers, health clinics, grocery stores, charter schools). As with other sectors, public health can offer data to inform these investments and can help promote initiatives that benefit low- and middle-income populations by making explicit links to potential health impacts. Community development agencies often have a key role in disaster recovery as HUD Community Development Block Grants have become a more common vehicle for providing funding for recovery assistance.
According to a RWJF report, collaboration between the health sector and community development organizations is already fairly widespread (Mattessich and Rausch, 2013). In a survey of 661 professionals in health and community development fields, nearly half of the respondents reported successful cross-sector initiatives on such issues as physical activity, access to health care, and promotion of a culture of health
and wellness. However, barriers to the development of these relationships remain. Two-thirds of respondents said that “inadequate funding and resources” was a major barrier, while more than half stated that a “lack of shared vision and common goals” prevented successful cross-sector collaboration (Mattessich and Rausch, 2013). Eighty-six percent of respondents cited an absence of pre-existing relationships and communication with potential partners as a barrier (Mattessich and Rausch, 2013)—perhaps pointing to an opportunity for conveners to promote these collaborations by bringing the health and community development sectors together for recovery planning.
Nongovernmental Organizations and the Business Community
A number of nongovernmental organizations, including community-based nonprofits and academic institutions, play important roles in the public health system, providing health services, training and education, and research capacity, among others. During and after a disaster, nongovernmental organizations and businesses provide invaluable assistance to the community. In the immediate aftermath of a disaster, community organizations that are already integrated into the community can step in to meet immediate needs such as shelter and food (The Alliance for a Just Rebuilding et al., 2014). This local mobilization of resources is particularly important when government is slow to respond or when outside help has not yet arrived. Private businesses assist by ensuring that individuals have access to medications and supplies. CVS Caremark, for example, assisted communities during Hurricane Sandy by setting up mobile pharmacies and delivering prescriptions to stranded customers (CVS Caremark, 2014). Public–private partnerships have enabled Wi-Fi access in shelters and recovery centers to help survivors seek help and connect with their social networks (Morton and Lurie, 2013). This type of collaboration among public health, nongovernmental organizations, and the business community can help reduce disparities in health outcomes following a disaster by accessing difficult-to-reach populations and providing services and supplies to all in need.
Building these partnerships in the pre-disaster phase is critical to ensuring that they are utilized to the fullest extent possible should a disaster occur. In Iowa, for example, the Safeguard Iowa Partnership was created in response to a concern that private-sector businesses wanted to assist during disasters but lacked an organized means for doing so (Beardsley, 2014). The Safeguard Iowa Partnership is an ongoing collaboration between private- and public-sector organizations that leverages community resources by facilitating the donation of private-sector resources and expertise to disaster response and recovery efforts (Beardsley, 2014; FEMA, n.d.). The Safeguard Iowa Partnership played a key role in promoting the sharing of both information and resources following flooding in Iowa in 2008 and again in 2013 (Safeguard Iowa Partnership, 2013).
PRE-DISASTER PUBLIC HEALTH SECTOR PRIORITIES
The best opportunity for improving community health beyond pre-disaster levels following a disaster arises when key elements are in place before a disaster to inform recovery efforts. As indicated during testimony to the committee by one state public health official, “to bring those types of issues up to a community that’s still reeling from a disaster, it would not be well received” (Clements, 2014). Thus, as discussed in Chapter 3, community health improvement goals need to be incorporated into recovery planning prior to a disaster. The key elements that need to be in place for recovery planning include community health assessments, community health improvement plans, and health department strategic plans. These elements are also prerequisites for national accreditation of health departments (PHAB, 2012); however, few communities have linked these existing processes with preparedness activities, even though they can help identify opportunities to build resiliency and improve community health in recovery. Siloing of public health roles and responsibilities, particularly for public health preparedness (Duncan et al., 2007), has impeded integration of community health improvement and recovery planning, resulting in less than optimal health outcomes after disasters.
There are several reasons why it is challenging for communities to make pre-disaster plans that include
opportunities to improve health in the recovery process. First, from a community standpoint, the focus is generally on immediate disaster response and on recovery as a means of returning to normalcy. Recovery as a means of creating a healthier community is a years-long process that for some communities is too far down the road to be a focus (Shah, 2014). Second, federal funding for disaster preparedness does not make long-term community health improvement a priority. The PHEP guidance on the Community Recovery capability, for example, has three foci: identify the recovery needs of health systems, coordinate recovery of these systems, and mitigate damages from future incidents. As James Blumenstock, the chief program officer for public health practice at the Association of State and Territorial Health Officials (ASTHO), pointed out, what is missing is an emphasis on making the community better and healthier in the recovery process (Blumenstock, 2014). Finally, public health professionals may not be engaged in pre-disaster recovery planning; thus, their perspective on long-term recovery is not reflected in the recovery plans.
The committee identified four key pre-disaster priorities in which the public health sector should be engaged to support implementation of the recommendations in this report and to ensure better short- and long-term health outcomes after a disaster:
- Conduct community health assessments.
- Engage community stakeholders in pre-disaster community health improvement and recovery planning.
- Ensure that public health community programs and services are integrated into healthy community and disaster recovery planning processes.
- Leverage pre-disaster preparedness activities in recovery planning.
The following discussion of the operational aspects of these activities, along with some best practices and other examples, is not exhaustive but is intended to be generalizable across a multitude of environments. In each case, there are opportunities to capitalize on traditional, preexisting public health programs, relationships, and resources.
Conduct Community Health Assessments
As discussed in earlier chapters, to optimally leverage disaster recovery-related opportunities to build healthier communities, health improvement goals must be integrated into pre-disaster recovery plans. The health improvement planning process should be informed by an assessment of community health status and needs. Monitoring of population health status is an essential public health function (see Table 5-2); public health departments continually collect, analyze, interpret, and report on community health needs and indicators. Commonly collected surveillance data include disease prevalence as well as individual and community risk factors and gaps in health care delivery (Salinsky, 2010). This type of information is incorporated into the community health assessment (sometimes called a community health needs assessment)—“a systematic examination of the health status indicators for a given population that is used to identify key problems and assets in a community” (PHAB, 2011, p. 8) (see also the discussion of community health assessments in Chapter 3). Assessment data can be used to prioritize interventions and provide a baseline against which change can be measured (Barnett, 2012).
Conducting community health assessments is one of the Public Health Accreditation Board’s prerequisites for accreditation (PHAB, 2013). Nonprofit hospitals, under provisions of the ACA, are now required by the Internal Revenue Service to perform these assessments as well (IRS, 2013). A collaboration between these hospitals and their state and local health departments is desirable in completing these assessments so as to identify the most comprehensive data sets and the elements necessary to improve the health of the community (NACCHO, 2012). Community health assessments have traditionally been separate from assessments related to disaster planning, which have historically focused on ensuring that ESF #8 functions are in place. This separation is due in part to compartmentalization of public health services.
A number of tools are available to guide a community health assessment (and the subsequent commu-
nity health improvement planning process). Examples include Mobilizing for Action through Planning and Partnerships (MAPP) and the Community Commons Community Health Needs Assessment Toolkit. MAPP, a framework designed by the National Association of City and County Health Officials (NACCHO), uses a six-phase process (organizing, visioning, assessments, strategic issues, goals/strategies, and action cycle) that focuses on community engagement and participation throughout (NACCHO, 2014b). For each phase, MAPP resources available on the NACCHO website8 suggest recommended participants and describe each step in that phase. The Community Health Needs Assessment Toolkit is an online tool that brings publicly available data together in one place so users can find and compare data on health indicators within and across communities (Community Commons, 2014a). Users can create printable maps or reports on the indicators and communities they have chosen, or they can run a report on their community that includes preselected indicators (Community Commons, 2014b). The toolkit pulls data from numerous sources, including the CDC, Healthy People 2020, and the Health Resources and Services Administration (Community Commons, 2014a).
Disaster recovery necessitates a process of decision making regarding the use of scarce resources. In the competition for resources, entities that can present a strong position using convincing data and arguments stand to benefit (Smith, 2011). Health assessment data that public health officials are already collecting and analyzing can inform decision making during pre- and post-disaster recovery planning by providing pre-disaster baseline information on health status and identifying gaps in services, communities at risk, and strengths and resources in the community. Public health can use these data to help focus recovery efforts on at-risk populations and “winnable battles” that have a large impact on health and known, effective solutions (CDC, 2014c). Public health professionals have skills in data collection and analysis that can be valuable assets during recovery planning efforts. One of public health’s core capabilities is data collection from multiple sources, including but not limited to health care providers, statistics on chronic disease, vital statistics (births, deaths, causes of death), information on utilization of programs such as Medicaid and WIC, community surveys, and geographic information systems. Public health professionals have experience in analyzing these data and creating reports, or in providing data to various organizations and agencies for purposes of research, grant making, and community and state decision making.
Interdisciplinary relationships established during broad stakeholder engagement in community health assessments or through data sharing arrangements (e.g., between public health and community-based organizations that require data for grant applications) also are valuable assets that can be leveraged during recovery planning. In many jurisdictions, however, public health’s data collection and relationship building currently are not being carried out with disaster recovery in mind. As a result, opportunities to use these data and relationships to make a strong case for investing in healthier communities are being missed.
Engage Community Stakeholders in Pre-Disaster Community Health Improvement and Recovery Planning
Based on the pre-disaster community health assessment, a community health improvement plan should be developed. A community health improvement plan is a “long-term, systematic effort to address public health problems on the basis of the results of community health assessment activities and the community health improvement process” (PHAB, 2011, p. 8). Through a broad-based community stakeholder consensus-building process, agreement should be reached on the elements of a healthy community and the strategies for achieving this goal. Integrating these strategies into the community health improvement plan creates a road map for closing the gap between the current health assessment and the optimal healthy community. The development of a community health improvement plan utilizes many of the essential capabilities of the public health sector: mobilizing community partnerships; developing plans and policies that aid health improvement efforts; and educating and empowering the community with respect to health issues.
________________
8 Information on the MAPP process is available at http://www.naccho.org/topics/infrastructure/mapp/framework/index.cfm (accessed April 10, 2015).
To be successful, health improvement planning needs to move beyond the health sector. Public health stakeholders should participate in broader strategic community planning for healthy places to live, work, learn, and play. As discussed in Chapter 2, integration of health improvement plans with a community’s comprehensive plan and recovery plan can better ensure uptake and resourcing of public health goals before and after a disaster (see Recommendation 1 in Chapter 3). Table 5-3 shows steps public health stakeholders can take to ensure that health considerations are incorporated into the comprehensive planning process (APA, 2006).
At the same time, the development of cross-sector partnerships, including public-private partnerships and partnerships with local planning, transportation, and housing departments and others, is critical since the public health sector typically does not design or build a community’s physical environment. Thus, a Health in All Policies approach is well suited to steady-state community planning and disaster recovery planning alike. In fact, recovery can accelerate the adoption of HiAP (Stevenson et al., 2014). A case study on how the disaster recovery process has enabled public health leadership in Canterbury, New Zealand, to “leapfrog” to an enduring HiAP approach is presented in Chapter 2 (see Box 2-10). However, as noted in the testimony of James Blumenstock, although current ASTHO educational materials and position statements on HiAP are relevant to post-disaster recovery, “there is absolutely no reference to post-disaster recovery as an opportunity or an issue or a circumstance where Health in All Policies needs to apply. No examples, no case studies, no verbiage basically linking the two” (Blumenstock, 2014). This is a gap that professional public health organizations (governmental and nongovernmental) need to address in the near term. Doing so will require a significant continued effort to educate health sector and nonhealth sector stakeholders, including the general public, on the value of HiAP and such tools as health impact assessments. This upfront investment can pay off in the event of a disaster. As discussed in the Galveston Health in All Policies case study in Chapter 2 (see Box 2-11), the time required to conduct such health literacy efforts after a disaster can significantly delay progress toward the building of healthier and more resilient and sustainable communities (Nolen, 2014).
The incorporation of health improvement goals from the health improvement plan into the recovery plan should be guided by an advisory committee for the Health and Social Services RSF (see Box 5-5). This advisory committee should have clear roles within the overarching organizational structure for recovery decision making, consistent with the principles of the NDRF. Public health officials should be heavily involved in the process, and individuals familiar with local community health programs and activities should be represented on the committee. The advisory committee may or may not have the same composition as the group leading a community health improvement planning process but should, in collaboration with emergency management and urban and regional planning agency officials, identify opportunities to advance toward a healthier and more resilient community should a disaster strike.
The following committee recommendations are applicable to this public health priority area:
- Recommendation 1: Develop a Healthy Community Vision for Disaster Recovery. (see Chapter 3)
- Recommendation 2: Integrate Health Considerations into Recovery Decision Making Through the National Disaster Recovery Framework. (see Chapter 3)
- Recommendation 3: Facilitate the Engagement of the Whole Community in Disaster Recovery Through Simplified and Accessible Information and Training. (see Chapter 3)
The programs and services that are the foundational care functions of public health—for example, creation of programs for prevention and education, disease control measures for outbreaks, immunizations, and direct health care provision and referrals to services—all are critical tools for health protection and promotion during post-disaster recovery. After disasters, demand for public health organizations to carry out these routine health functions surges concurrently with new responsibilities related to emergency
TABLE 5-3 Public Health Roles in the Comprehensive Planning Process
| Comprehensive Plan Action | Public Health Agency Role |
|
Step 1: Visioning and Goal Setting |
|
|
|
|
Step 2: Data Collection and Needs Assessment |
|
|
|
|
Step 3: Drafting the Plan |
|
|
|
|
Step 4: Adoption and Implementation |
|
|
|
|
Step 5: Revise Development Regulations and Evaluate Plan Performance |
|
|
|
SOURCE: Copyright 2006 by the American Planning Association. Reprinted by permission.
BOX 5-5
Promising Practice: Recovery Support Function Advisory Committees
Recovery Support Functions under the National Disaster Recovery Framework are designed to support and supplement local disaster recovery efforts. These local efforts can be strengthened by the creation of local advisory committees. The Health and Social Services advisory committee should be charged with collaborating with emergency management and planning agency officials on the integration of the community health improvement plan into disaster recovery planning. The advisory committee should identify opportunities to improve the overall health status of the community after a disaster. It should exercise flexibility and responsiveness to input from an ongoing assessment process, adjust the recovery plan accordingly, and continuously gauge movement toward implementation of the elements essential for improved community health. The opportunities identified by the advisory committee need to be integrated into the recovery plan framework for the community to advance toward a healthier and more resilient community should a disaster strike.
These types of advisory committees are already in development in some communities. Florida’s Hillsborough County has created a Post-Disaster Redevelopment Plan (PDRP) to guide long-term recovery. Eight voluntary Technical Advisory Committees (TACs) on such topics as environmental restoration, housing recovery, and health and social services form the backbone of the PDRP. The TACs coordinate on issues that overlap. The Health and Social Services TAC focuses on meeting the health, social services, and public safety needs of the population after a disaster, and ensuring a smooth transition from short-term recovery to long-term redevelopment. Examples of organizations that may serve on the Health and Social Services TAC include the health department, the school district, health care providers, the Red Cross, and advocates for homeless or disabled residents (Hillsborough County Government, 2010). Similarly, in Fairfax County, Virginia, the Pre-Disaster Recovery Plan includes a provision for the establishment of subcommittees that would advise on areas of subject-matter expertise, such as housing or community services, should a disaster occur. These subcommittees might meet on an ongoing or ad hoc basis, and could coordinate regional issues or provide a venue for public input on recovery. They might include residents of the county as well as outside experts from academia, government, or nongovernmental organizations (Fairfax County, 2012).
operations (Klitzman and Freudenberg, 2003). Inability to meet this increased demand for ongoing public health services will have adverse effects on population-level health outcomes; therefore, strengthening these programs before a disaster will pay dividends should such an event occur.
As discussed earlier in this chapter, the community-based programs and services of the public health sector (e.g., health care delivery clinics, immunizations, nutrition and food services, wellness programs, home care, education programs) vary greatly by community depending on needs, authorities, and resources. These existing programs and services provide an interface to the community and can be leveraged to identify gaps and populations at risk and to educate and mobilize the community to develop a vision for health. Relationships with community partners involved in public health programs (e.g., social services, behavioral health) can be used to integrate these groups into disaster recovery planning.
The following committee recommendation is applicable to this public health priority area:
- Recommendation 4: Enhance and Leverage Social Networks in Community Health Improvement and Recovery Planning. (see Chapter 3)
Leverage Pre-Disaster Preparedness Activities in Recovery Planning
Much public health pre-disaster planning takes place under the guidance of the PHEP cooperative agreement, administered by the CDC. PHEP funding is provided to state public health departments (with a few exceptions) to help communities become more resilient and better prepared to respond to disasters. The CDC releases guidance on how PHEP awardees should use the funding (CDC, 2011). The 15 public health preparedness capabilities are split into two tiers. Tier 1, the highest-priority activities, includes Community Preparedness, Public Health Surveillance and Epidemiological Investigation, and Public Health Laboratory Testing. Tier 2 includes Medical Surge, Fatality Management, and Community Recovery (CDC, 2011). This prioritization—with Community Recovery in the bottom tier—demonstrates the lack of emphasis on disaster recovery during preparedness planning. Further, not only is Community Recovery a low priority, it is also currently defined in terms of systems recovery rather than overall community health: “the ability to collaborate with community partners … for the rebuilding of public health, medical, and mental/behavioral health systems to at least a level of functioning comparable to pre-incident levels, and improved levels where possible” (CDC, 2011, p.10).
The lack of emphasis on recovery is further demonstrated in data on actual preparedness activities carried out by PHEP awardees. More than one-third of grantees (37 percent) reported that they had not undertaken any kind of activities related to the Community Recovery capability. Fewer than half (45 percent) had begun the process of recovery planning but were in early stages of identifying community partners or holding training meetings.9 Recovery—particularly long-term recovery—is simply not a priority for many public health officials during disaster preparedness planning. As the President of the International Association of Emergency Managers, Bruce Lockwood, emphasized, “We were allowed to bullet vote at the public health advisory meeting as to which capabilities were our priorities. Where do you think recovery ended up? It is at the bottom of the list” (Lockwood, 2014).
PHEP funding offers an opportunity to support integration of health into recovery planning both horizontally (across sectors) and vertically. Despite the lack of emphasis on recovery in PHEP grant-related activities, myriad other preparedness efforts are directly linked to the recovery process and can be leveraged for that purpose. Some examples are described below.
Community preparedness (PHEP Capability 1) encompasses cross-disciplinary processes that include the development of plans, training exercises, and participation in coalitions. These activities are where relationships are built and agencies are exposed to each other’s capabilities and challenges. Under the Community Recovery function, PHEP guidance encourages the development of community partnerships in order to identify the health system needs after a disaster and to coordinate the provision of services and health systems recovery. However, partnerships developed for community preparedness purposes can and should be utilized in recovery planning as well (see the example in Box 5-6).
Enhancement of the information-sharing environment (PHEP Capabilities 3 and 6) includes public information and warning as well as information sharing among agencies. Exploiting preexisting channels of communication can accelerate recovery planning at any stage. Having technology and data systems in place that allow for patient monitoring at a time when basic infrastructure may be compromised may prove critical, especially for vulnerable populations (Zucker, 2014). Based on experiences during Hurricane Sandy, for example, New York State accelerated development of its eFINDS system, a patient tracking system that had been initiated before the disaster and uses barcodes on wristbands to track patients evacuated from state-regulated and state-run medical and adult care facilities (Zucker, 2014). Electronic health records also may be lifesaving, providing up-to-date information on medications, such as those for older adults and people with psychiatric disorders, as well as information on individuals who may have mobility issues or may be homebound. Systems that allow for quick and systemic identification of those requiring medical devices and specialized equipment and treatment may also be critical. Although there may be concerns regarding Health Insurance Portability and Accountability Act (HIPAA) protections, a
________________
9 E-mail communication, C. Singleton, Centers for Disease Control and Prevention, to A. Downey, Institute of Medicine, regarding a request for information on PHEP recovery capability, October 6, 2014.
BOX 5-6
Los Angeles County Community Disaster Resilience Project
The Los Angeles County Community Disaster Resilience (LACCDR) project is intended to promote community resilience in the event of a disaster. The project defines community resilience as “the capacity of the community as a whole to prepare for, respond to, and recover from adverse events and unanticipated crises that threaten the health of all” (LACCDR, 2014; Plough et al., 2013). To foster community resilience, public and private community-based organizations work together in preparedness, response, and recovery planning activities, seeking to focus disaster planning not solely on individual preparedness but more broadly on community preparedness and social connections. The project’s message is that community resilience is about “transforming disaster planning and response from just ‘me’ to include ‘we’” (LACCDR, 2014). The project is a collaborative venture supported by the Centers for Disease Control and Prevention (CDC), the National Institute of Mental Health, and the Robert Wood Johnson Foundation. The project is an outgrowth of awareness that the absence of sustainable engagement with community organizations hampered recovery from Hurricane Katrina, the H1N1 pandemic of 2009, and Hurricane Sandy and explained the disparities between communities that recovered successfully and those that did not (Plough et al., 2013).
One of the LACCDR project’s first activities was to survey health department staff and community organizations to identify barriers to and facilitators of resilience building. The survey revealed that minimal time was devoted to community resilience and emergency preparedness, even though many populations in the community stood to benefit from such efforts (Chandra et al., 2013). Building upon the results of this sur-vey, the project is undertaking the following five activities: (1) improving the community engagement skills of Los Angeles County health department staff to enable them to build sustainable multisector community partnerships; (2) developing a best practices and resilience curriculum for engagement of county health department staff with community organizations; (3) creating a resilience toolkit for use by community organizations in building coalitions that increase community preparedness; (4) developing a countywide media campaign around the theme of “Just Be Ready” in order to encourage social connectivity (i.e., “Know your neighbors. Plan together. Be ready.”); and (5) identifying metrics for gauging whether the LACCDR project has successfully achieved community resilience, including a social network analysis tool called “PARTNER” that measures and monitors collaboration among people and organizations (Plough et al., 2013).
2014 bulletin from HHS’s Office for Civil Rights, HIPAA Privacy in Emergency Situations, notes that “the HIPAA Privacy Rule protects the privacy of patients’ health information (protected health information) but is balanced to ensure that appropriate uses and disclosures of the information still may be made when necessary to treat a patient, to protect the nation’s public health, and for other critical purposes” (HHS, 2014b, p. 1). According to the bulletin, the Privacy Rule allows for disclosure of protected health information to a public health authority (federal, state, or local) as necessary to carry out its public health mission. For example, Medicare claims data recently were used in an emergency preparedness drill to identify locations of individuals who rely on electricity-dependent medical equipment, a key vulnerable population. The data were securely transmitted to the local health department. The success of this model depends on having appropriate protocols and privacy protections in place in advance of a disaster, as well as on local capabilities to receive and manage the data for preparedness purposes (DeSalvo et al., 2014).
Emergency operations center operations and surge (medical, fatality, mass care, volunteers) management (PHEP Capabilities 3, 5, 7, 9, 10) require evaluation and coordination of resources (including human resources) both vertically and horizontally. The knowledge and relationships built in developing
these capabilities form the basis for initiating recovery planning discussions. An example of pre-disaster surge preparedness is the development of local and regional Medical Reserve Corps (MRCs), disaster medical assistance teams (DMATs), and other medical teams to be deployed in the immediate aftermath of a disaster. In many cases, a disaster prompts a generous outpouring of volunteerism from the medical community across the country. The MRC and DMAT models give volunteer health professionals access to specific disaster-related training and provide pre-event credentialing, both of which are equally important to response and recovery efforts.
Additional activities pivotal to public health pre-disaster planning take place under the guidance of the HPP, which, as noted earlier, is administered by ASPR within HHS. These activities, detailed in Chapter 6, require engagement of state and local public health agencies in planning, training, and exercise events with partners from the health care delivery sector, often in the context of health care coalitions.
THE CONTINUUM OF POST-DISASTER PUBLIC HEALTH RESPONSE AND RECOVERY PRIORITIES
Early recovery and response operations need to begin concurrently (ASTHO, 2007), and in fact, the effectiveness of the response to a disaster can significantly impact the trajectory of recovery. The most pressing issues typically facing a community during and immediately following a disaster are ensuring the immediate safety and security of those present and the continuity of essential services. Coordination among stakeholders during this period should occur through ongoing operation of an incident command system that allows for active participation in public health recovery activities by social services agencies, behavioral health agencies, volunteer organizations, the medical examiner/coroner, mass sheltering organizations, and businesses and organizations regulated by the public health department. Steps necessary to ensure safety and continuity of services are discussed in the following sections. As circumstances change during response and then throughout recovery, however, opportunities to invest in changes that will strengthen resiliency and add those elements of a healthy community that may previously have been absent ought to be actively pursued.
Some jurisdictions may require an emergency declaration to assist with various aspects of response and recovery. In some cases, the use of certain stockpiles or procedures or even funding may be tied to the issuance of an emergency declaration. Such declarations may be made at various levels of government, making available resources held at that level for emergency use. A presidential declaration is necessary to activate federal reimbursement funding for specific emergencies covered under the Stafford Act (see Chapter 4).
Post-disaster response and early recovery priorities for public health include
- participating in a shared communication effort;
- conducting impact assessments of the community’s health and medical needs;
- reestablishing critical public health infrastructure;
- delivering public health services to meet post-disaster needs of the community; and
- providing support to impacted health care delivery systems.
There are also a number of priorities for which efforts may be initiated in the short-term post-disaster period but will extend into long-term recovery. These include
- facilitating health-informed recovery decision making through data;
- engaging in health-informed community rebuilding and redevelopment planning; and
- sharing lessons learned with other communities to improve disaster recovery planning.
EARLY POST-DISASTER PUBLIC HEALTH RECOVERY PRIORITIES
Participating in a Shared Communication Effort
During disaster response and recovery, clear and bidirectional communication within and across sectors and with the public is critical to providing needed health-related information and preventing further illness or injury. Coordination of communication efforts across sectors should be conducted within the structure of a joint information system. Emergency management officials often lead shared communication efforts, but the joint information system should include spokespersons from all major agencies to make it possible to develop, maintain, and disseminate a coordinated message; manage media inquiries and press conferences; and ensure that early and accurate information is provided to the public. The joint information system may or may not have a formal physical location but must provide capabilities for message review, conference calls, and secure communications between agencies. As the event unfolds and the transition from response to recovery begins, the communication methods used must be sustainable throughout.
When communicating with the public, the health sector (including public health, health care, behavioral health) and social services providers should focus on messaging, education, and outreach. Communication about the health risks of a disaster and how to prevent further injury and illness can be accomplished through such channels as press releases, interviews with experts, and news conferences. Disaster-related communications should be written and designed to ensure that the general public can comprehend the basic health information necessary to make appropriate health-related decisions.
The use and monitoring of social media during disaster response and recovery are increasingly important functions for public health agencies. The use of preestablished social media outlets to provide messaging to followers (e.g., Facebook and Twitter) is now a common vehicle for communication. Monitoring social media is critical to identify trends and discredit false rumors that can be detrimental to successful response and recovery activities or even pose a danger to the public and responders (Knearl, 2014).
In addition to social media and more traditional media venues, public health officials should consider using community partners to help reach the public, especially vulnerable populations. A best practice is to identify in advance of a disaster those community partners that serve vulnerable populations, faith-based groups, and other culturally unique populations. These partners can serve as agents of the public health entity, providing a trusted source of information and visible leaders who can translate public health messaging in linguistically and culturally appropriate ways using their unique access to their constituents. In King County, Washington, for example, public health officials learned to use community partners to reach out to immigrant populations after a storm-related power outage in 2006 resulted in eight carbon monoxide poisoning fatalities and scores of hospital admissions when people used grills indoors for heat. In a similar outage in 2012, when public health officials used communication channels suggested by their community partners—including flyers in multiple languages and robo-calls from a mosque—carbon monoxide poisoning was reduced by 90 percent and caused no fatalities (NRC, 2012).
Within the health sector, a well-designed health information technology recovery plan can help ensure continued access to health information such as vital records, immunization records, and medical histories. Information-sharing systems can help health care systems share resources and manage capacity; the Hospital Available Beds for Emergencies and Disasters (HAvBED) system, for example, tracks available hospital beds in real time to facilitate management of a surge in patients during a large-scale disaster (AHRQ, 2005). Likewise, the CDC’s Health Alert Network can keep public health practitioners and clinicians up to date on ongoing or emerging threats to public health (CDC, 2014a).
Conducting Impact Assessments on the Community’s Health and Medical Needs
A critical post-disaster task for the public health sector is to conduct an assessment of the immediate health and medical needs of the impacted community. This process needs to be rapid, flexible, and data driven, with a focus on actively seeking opportunities to strengthen community resiliency and health.
The information gathered, along with any relevant pre-disaster assessment data (e.g., from a community health assessment), is then used to inform planning efforts and forms the basis for resource and funding requests. As indicated in Figure 5-1 presented earlier, assessment is part of a continuous feedback loop. A multidisciplinary task force (such as the advisory committee discussed previously in Box 5-5) should be responsible for recommending course corrections based on the most recent data gathered through the ongoing assessment process throughout recovery.
The following committee recommendation is applicable to this public health priority:
- Recommendation 5: Establish Pathways by Which Health Information Can Inform Recovery Decision Making. (see Chapter 3)
Reestablishing Critical Public Health Infrastructure
In the aftermath of a disaster that compromises public health capabilities, it is critical for services to be restored as soon as possible, even in a degraded mode (e.g., paper rather than computerized forms). To this end, it is important to have a robust continuity of operations plan and/or continuity of government plan with pre-identified mission-essential functions, alternative work sites, vendors and suppliers, and backup systems. Such a plan should, when possible, identify primary, secondary, and tertiary alternative locations that include at a minimum sanitation facilities, parking, adequate work and rest spaces, and backup electricity/phones/computers. Emergency procurement procedures should be identified to enable the agency to obtain the necessary goods and services. The agency succession process should be activated if needed to ensure that key leadership roles are filled. Access to vital records is imperative during the immediate response to a disaster and during recovery. Methods of operation for a vital records agency may be severely degraded in a disaster, requiring the development of plans for keeping records intact and secure and for distributing and collecting information in a degraded mode when necessary.
Once an agency has identified its emergency needs related to reconstitution and recovery, numerous sources of human capital can be called upon to increase workforce capacity. These sources include federal or state assistance (such as the Emergency Management Assistance Compact), temporary employees, volunteers, the Medical Reserve Corps, and contracted employees or agencies. Recent legislative changes under the reauthorization of the Pandemic and All Hazards Preparedness Act (PAHPA)10 have mitigated some of the legal and logistical barriers that previously impeded deployment of local public health personnel funded through federal grants for alternative functions during a disaster. If licensed personnel, certified personnel, or those with special skills are used to augment public health recovery resources, care should be taken to verify their credentials and skills before deployment. Disaster response plans should include provisions for the licensing and certification of incoming volunteer resources in two categories: those that are planned and those that are spontaneous.
Delivering Public Health Services to Meet Post-Disaster Needs of the Community
In addition to the essential services provided during steady-state times, a number of services must be ensured by the public health sector in the aftermath of a disaster. These services are described below.
Environmental Services
In a post-disaster community, ensuring the safety of food and water is a critical function of public health. If a disaster involves flooding or power outages, there is the risk that food and water supplies will be contaminated or spoiled. Mass feeding operations, such as at shelters, must be inspected for proper
________________
10 Pandemic and All-Hazards Preparedness Reauthorization Act of 2013, Public Law 113-5, 113th Cong., H.R.307 (March 13, 2013).
food handling and storage to prevent the spread of foodborne illness. To monitor the safety of food and water, public health laboratories must have the capacity to test samples and obtain results reasonably quickly. Public health agencies should take appropriate actions to protect the public when contamination is suspected, and they should coordinate their food and water safety efforts with media outreach to ensure the confidence of the public. Disaster impact assessments should address potential releases of toxins, radiation, or other hazards into the environment (both indoors and outdoors). Public health agencies should work with municipal and private water and sewer systems and environmental protection agencies to ensure environmental health.
Fatality Management
Public health involvement in fatality management will vary by jurisdiction. Typical public health support for fatality management may include providing or coordinating the receipt of supplies, as well as facilitating federal efforts such as the disaster mortuary operational response team (DMORT). Public health agencies may also be involved in the coordination of assets and processes for identification, storage, embalming, and interment of remains. Public health laboratories may be needed for these efforts. Usually, public health coordinates with the local medical examiner or coroner and the local emergency management agency on mass fatality issues. Agencies should be well versed in their roles as assigned by their local fatality management plan.
Access and Functional Needs Populations
In all post-disaster efforts, public health should consider individuals with access and functional needs and the community-based agencies that serve them. Individuals with access and functional needs include but are not limited to people with disabilities that affect their ability to function independently without assistance, women in late stages of pregnancy, children and the elderly, non-English speakers, and people needing special medical equipment (FEMA, 2010). All planning for recovery operations should take into account these populations, and public health should consider taking a lead role in coordinating volunteer and advocacy groups to ensure that recovery efforts are meeting their needs. For example, public health should be part of a multisector task force on interim and temporary housing to ensure that access needs are addressed.
Providing Support to Impacted Health Care Delivery Systems
Working with other community stakeholders (e.g., emergency management), public health agencies can facilitate the recovery of a jurisdiction’s health care system through a variety of activities. Most jurisdictions have mutual aid plans that can be implemented automatically to ensure emergency medical coverage. Depending on the nature of the event, these plans may be disrupted or hindered. When the resources needed outweigh those available, a public health agency may be asked to assist in augmenting those resources. Volunteers in the local Medical Reserve Corps or registered through the Emergency System for Advance Registration of Volunteer Health Professionals (ESAR-VHP; discussed further in Chapter 6) can be mobilized to support these efforts. Interstate and federal assistance can also be requested, such as implementation of the National Disaster Medical System to facilitate patient transport to other areas; deployment of DMAT, DMORT, and federal medical station teams; and other critical resources. Advance planning, combined with training and exercising of plans on a regular basis, is essential. An adequate health operations center should be identified and equipped for long-term continuous operations in support of health care system recovery, and health care coalition leadership should be integrated into the public health incident command system. Past disaster experience has demonstrated that health care coalitions are critical to bridging the gap between public health and the medical community (Clements, 2014).
Public health agencies may also be asked to coordinate transitions to and from contingency or crisis
standards of health care delivery to ensure the most comprehensive care for the greatest number of people. Such measures may be required in inpatient and outpatient settings and other environments, such as coordination of additional health care personnel to establish a shelter-based clinic and pharmacy. The effects of a disaster on the community may create a need to change EMS or dispatch protocols temporarily to facilitate care or to require a modification of transportation patterns for health responders.
Changes to licensing or certification requirements and suspension or modification of protocols, rules, or even certain laws may be necessary to coordinate the restoration of a health care system. For example, communities may decide to recognize medical credentials of out-of-state volunteer providers to meet a surge in care delivery needs. Ideally, systems for verifying credentials (e.g., ESAR-VHP) should be developed in advance of a disaster. Some changes also may need to be made in nonmedical areas (such as spending and personnel rules). Public health agencies should anticipate in advance and plan for situations that may require this type of response and determine the best way to obtain the necessary legal permissions.
Public health should work with appropriate authorities to assess damaged health care facilities in accordance with priorities based on the community’s needs. Rapid mobilization of public health department staff to conduct reviews of medical facility plans and surveys of facilities can expedite the process of reopening facilities to the public. Some normal facility requirements may be temporarily waived to facilitate bringing a given building back to operational status.
After a disaster, the emphasis is on immediate response and short-term recovery—getting things back to normal. While these restoration efforts are critical to meeting the most immediate needs of the community, they may well fall short of moving the community closer to a consensus-derived vision of a health community. During its efforts to engage the public health sector in discussions about recovery, the committee noted a lack of focus on long-term recovery concerns. Public health officials agreed that long-term health improvement opportunities were of interest to them but not a priority because of their strong mission focus on disaster response and early recovery and the scarcity of resources and funding for existing public health programs. As described by one public health director: “As soon as the waters recede or there’s no more disease going around or we’ve administered all the vaccine, it’s really [about getting] back to business as usual. We really don’t have a plan or a thought about what are we going to do now long term in assessing the community” (Beardsley, 2014). Yet despite the challenges involved in long-term recovery, previous events have shown that long-term disaster recovery presents an opportunity for public health officials to facilitate the development of healthier and more resilient and sustainable communities. The sections below describe how the public health sector can engage in long-term recovery efforts and help inform decision makers and the community at large about how they can exploit this opportunity.
Facilitating Health-Informed Recovery Decision Making Through Data
Long-term recovery requires a commitment on the part of the community to continually assess itself and identify the best uses for recovery resources and funding. Public health agencies are positioned to be among the main providers of data and analysis on health-related issues. Through preexisting community health assessments and public health-related data sets, new disaster needs assessments, disaster-related research projects, and health impact assessments targeting community rebuilding projects, public health stakeholders can promote a HiAP approach to long-term recovery. (See Chapter 2 for a discussion of this approach.) Continual outreach to and education of decision makers and the community at large must occur during this process to ensure buy-in. A cyclical process of continual assessment, analysis, planning, and evaluation of early outcomes, such as that depicted earlier in Figure 5-1, is a best practice.
The following committee recommendations are applicable to this public health priority area:
- Recommendation 5: Establish Pathways by Which Health Information Can Inform Recovery Decision Making. (see Chapter 3)
- Recommendation 7: Ensure a Ready Health Information Technology Infrastructure. (see Chapter 6)
Engaging in Health-Informed Community Rebuilding and Redevelopment Planning
Based on impact and damage assessments, public health leadership should work with elected and public officials, as well as leaders from relevant nonhealth sectors (e.g., housing, transportation), to identify opportunities for integrating some or all of the goals and objectives of the community health improvement plan with long-term community recovery efforts. Familiarity with and support for these goals and objectives prior to a disaster will greatly facilitate their implementation. Success can still be achieved even when this integration has not been done in advance (see Box 5-7 for an example from New Orleans in the wake of Hurricane Katrina), although the task will most likely be more challenging and take significantly longer. Public health can assist community decision makers in the use of a HiAP approach—for example,
BOX 5-7
New Orleans After Hurricane Katrina: A New Approach to Public Health
New Orleans has been honored with the inaugural 2013 Robert Wood Johnson Foundation Culture of Health Prize for its progress in transforming community health. The award honors New Orleans’ exemplary community partnerships, which are encouraging its citizens to live healthier lives (RWJF, 2013).
In the aftermath of Hurricane Katrina, New Orleans made public health and prevention a priority as a critical part of the continuing recovery effort. To advance community health, a cross-sector partnership was developed among New Orleans’ Health Department, businesses, nonprofit organizations, and schools (RWJF, 2013). Prior to Katrina, New Orleans’ approach to health emphasized clinical care over prevention and public health, a common emphasis throughout the nation. New Orleans Health Commissioner Dr. Karen DeSalvo attributes the public health department’s rapid transformation from “broken and outmoded” to a modern public health agency to the city’s use of the Public Health Accreditation Board’s accreditation blueprint (RWJF, 2013). According to DeSalvo, “That is how we’re getting from a place where we were treating the consequences of poor health decisions and the impacts of social determinants of health, and actually move into a place where we’re upstream and we can prevent it, but then work with other sectors” (RWJF, 2013).
DeSalvo stresses that a single department alone cannot solve all the health challenges a community faces. The development of a cross-sector partnership that reflects the various social determinants of health plays a crucial role in advancing community health further and ensuring that health remains an important consideration in every new policy (RWJF, 2013).
Key steps in New Orleans’ transformation included
- reinvesting in the local health system,
- ensuring access to healthy food and opportunities to be physically active, and
- implementing new education models.
While New Orleans has made impressive strides in advancing community health, its new approach to public health and emphasis on prevention remains a “work in progress” (RWJF, 2013). The ongoing nature of this transformation will ensure that New Orleans continues to make progress toward resolving the health challenges caused and brought to light by Hurricane Katrina.
SOURCE: RWJF, 2013.
by conducting health impact assessments—to help them seek opportunities for improved health within their areas of jurisdiction and responsibility. These opportunities may include
- promoting more resilient design of new construction;
- promoting consideration of quality of life in planning for community redesign (e.g., bicycle lines, walking/jogging trails, parks and green spaces, locations of community amenities);
- identifying priority areas for redevelopment based on data showing health disparities;
- implementing strategies designed to retain the health services workforce; and
- promoting access to care as part of action plans.
To facilitate post-disaster health improvement planning, community leaders can activate a health-related advisory committee or subcommittee of the jurisdictional long-term recovery effort (discussed earlier in Box 5-5). Based on the pre-disaster community health assessment and the community health improvement plan, the advisory committee can identify opportunities to implement strategies designed to improve the overall health status of the community. Flexibility and responsiveness will be important to integrate input from the ongoing assessment process, adjust the recovery plan accordingly, and continuously gauge movement toward implementation of the elements essential for improved community health (see Chapter 3 for discussion of measurement tools). This process will help close the gap between the community’s current health status and its agreed-upon criteria for an optimally healthy community, which will likewise be continuously monitored and evaluated for effectiveness (see Figure 5-1).
When opportunities to improve quality of life and public safety are identified, local and state public health agencies should promote efforts to seize these opportunities at the system, policy, and legislative levels. These efforts should cut across nonhealth areas such as housing, land use, and the business community to incorporate health considerations into all governmental decision-making processes. This HiAP approach will enable sustainable strategies to improve community health in the long term. Support from such key partners as local planners, city managers, and school districts will be essential to the success of such efforts. In communities that have established a HiAP approach to decision making prior to a disaster, the event will strengthen the practice and perhaps galvanize support from additional stakeholders. In communities without such an approach, a disaster may open doors for collaboration that have previously been closed and provide a forum for educating the community on the value of considering health in developing community projects.
The following committee recommendations are applicable to this public health priority area:
- Recommendation 6: Leverage Recovery Resources in a Coordinated Manner to Achieve Healthier Post-Disaster Communities. (see Chapter 4)
- Recommendation 10: Design for Healthy Post-Disaster Communities. (see Chapter 9)
- Recommendation 11: Mitigate Against Future Health Hazards. (see Chapter 9)
- Recommendation 12: Ensure Healthy and Affordable Post-Disaster Housing. (see Chapter 10)
Sharing Lessons Learned with Other Communities to Improve Disaster Recovery Planning
After a disaster, a communication strategy should be developed to share lessons learned and opportunities for improvement so other jurisdictions can benefit from experiences with recovery. Local, tribal, territorial, and state health officials should utilize state, regional, and national conferences, workshops, and discipline-specific professional meetings for this purpose and reach out to professional organizations representing traditionally nonhealth sectors to discuss opportunities for improved public health. Increased opportunities to share lessons learned both with other health departments and with other sectors—such as
cross-training, mentorships, cross-disciplinary articles, and urban planning webinars—should be pursued. Examples of mechanisms for sharing lessons learned include but are not limited to
- after-action reports in FEMA’s Lessons Learned Information Sharing System;
- presentations at state and national public health association meetings, including the Public Health Preparedness Summit, the National Healthcare Coalition Conference, and other applicable national emergency management conferences;
- engagement with professional organizations representing traditionally nonhealth sectors, such as the United States Council of Mayors, the National Governors Association, the International City/ County Management Association, the American Planning Association, the International Association of Emergency Managers, and the Council of State Community Development Agencies;
- presentations at conferences of state hospital associations, mental health associations, and other applicable professional associations;
- engagement with philanthropic organizations and foundations regarding the rationale for building resiliency in the face of disasters;
- discussions with intra- and interstate medical system coalitions;
- presentations to emergency management partners at state conferences and meetings;
- leveraging of NACCHO and ASTHO to share lessons learned with other local and state health departments; and
- discussions during PHEP and HPP conference calls and reporting opportunities.
In the process of developing its guidance specific to the public health sector, the committee noted that further research is needed to address the following questions:
- For those with chronic health problems exacerbated by the effects of disasters, what are the stages of exacerbation?
- How can identifying persons that are at highest risk for most rapid deterioration assist in prioritization of limited resources during recovery?
SUMMARY OF FINDINGS AND CONCLUSIONS
Although a disaster causes significant disruption to the status quo, the subsequent recovery period presents a unique opportunity to shift existing funding streams, leverage one-time funding opportunities, and coalesce community stakeholders to build the resiliency of a community intentionally and strategically and to close the gap between the pre-disaster state of health and what the community envisions as an optimally healthy community.
The development of a healthy community requires a solid public health system foundation. The public health enterprise incorporates many activities focused on improving the health of a community. These activities include conduct of a community health assessment and development of community health improvement plan, as required by the national Public Health Accreditation Board. Although communities nationwide are currently engaged in improving their health, their progress to that end is often steady but slow. Disasters can catalyze bold change over a shorter period of time than would otherwise have been possible. However, successful movement toward optimal health—especially in the face of a disaster, which understandably demands attention to the immediate needs of the community—requires strategic use of a comprehensive community health assessment and a community health improvement plan that is fully integrated into the disaster recovery decision-making process. This integration will not occur without the integration of public health into pre- and post-disaster planning for long-term recovery.
PUBLIC HEALTH SECTOR RECOVERY CHECKLIST
The committee has identified four pre-event and eight post-disaster critical recovery priorities for the public health sector that are inextricably linked to strengthening the health, resilience, and sustainability of a community. Action steps for each of these priorities are provided in the following checklist. Although public health leaders will need to adapt these actions to the local context, this guidance provides an indicative set of concerns to be considered during recovery. The checklist illustrates how the following four key recovery strategies, identified as recurring themes at the beginning of this chapter, apply to individual priority areas:
- Leverage existing relationships and networks (e.g., coalitions, collaboratives) to integrate public health and other community partners into recovery planning.
- Identify opportunities for alignment between ongoing public health improvement processes (e.g., accreditation prerequisites of community health assessments and community health improvement plans) and recovery planning.
- Educate nonhealth sectors and the community on why health is integral to recovery and how recovery activities impact health outcomes.
- Use and expand health technology infrastructure for data collection and analysis to facilitate data sharing, evidence-based decision making, and continual evaluation of progress toward an optimally healthy community.
Pre-Event
Priority: Conduct Community Health Assessments
Primary Actors1: State/Local Health Departments2
Key Partners: Social Services Agencies, Health and Medical System Partners, Urban and
Regional Planning Agencies, Emergency Management Agencies
Key Recovery Strategies:
- Leverage existing relationships and networks (e.g., coalitions, collaboratives) to integrate public health and other community partners into recovery planning.
- Use and expand health technology infrastructure for data collection and analysis to facilitate data sharing, evidence-based decision making, and continual evaluation of progress toward an optimally healthy community.
Activities include but are not limited to:
![]() Examine all existing public health data sources and relationships and crosswalk with disaster recovery data needs.
Examine all existing public health data sources and relationships and crosswalk with disaster recovery data needs.
![]() Develop disaster data needs in the pre-disaster environment.
Develop disaster data needs in the pre-disaster environment.
![]() Define how current analyses and reports can support recovery planning; develop new reports for recovery if needed.
Define how current analyses and reports can support recovery planning; develop new reports for recovery if needed.
![]() Create innovative methods for sharing data with disaster recovery planners, political leaders, and the community.
Create innovative methods for sharing data with disaster recovery planners, political leaders, and the community.
![]() Link data to economic opportunities and challenges.
Link data to economic opportunities and challenges.
![]() Utilize existing adjunct technologies such as geographic information systems (GIS) and spatial analysis to articulate findings to broader audiences.
Utilize existing adjunct technologies such as geographic information systems (GIS) and spatial analysis to articulate findings to broader audiences.
![]() Utilize newer vehicles such as social media to share findings with broader audiences and obtain feedback.
Utilize newer vehicles such as social media to share findings with broader audiences and obtain feedback.
![]() Examine opportunities for public health access to electronic medical records from inpatient, outpatient, and prehospital services.
Examine opportunities for public health access to electronic medical records from inpatient, outpatient, and prehospital services.
![]() Proactively engage in health information technology infrastructure planning to connect relevant data sets and develop sharing policies across agencies.
Proactively engage in health information technology infrastructure planning to connect relevant data sets and develop sharing policies across agencies.
--------------------------
Priority: Engage Community Stakeholders in Pre-Disaster Community Health Improvement and Recovery Planning
Primary Actors: State/Local Health Departments
Key Partners: Elected Officials and Community Leaders, Urban and Regional Planning Agencies, Emergency Management Agencies, Community- and Faith-Based Organizations
________________
1 See Appendix F for further description of terms used to describe Primary Actors and Key Partners in this checklist.
2 Throughout this checklist, “State/Local” is used for the purposes of brevity but should be inferred to include tribal and territorial as well.
Pre-Event
Key Recovery Strategies:
- Identify opportunities for alignment between ongoing public health improvement processes (e.g., accreditation prerequisites of community health assessments and community health improvement plans) and recovery planning.
- Leverage existing relationships and networks (e.g., coalitions, collaboratives) to integrate public health and other community partners into recovery planning.
- Educate nonhealth sectors and the community on why health is integral to recovery and how recovery activities impact health outcomes.
Activities include but are not limited to:
![]() Reach out to community, government, and private-sector leaders and create a list of all stakeholder groups, including existing coalitions. Consider maintaining this list within one program for continuity. Existing coalitions may include
Reach out to community, government, and private-sector leaders and create a list of all stakeholder groups, including existing coalitions. Consider maintaining this list within one program for continuity. Existing coalitions may include
- – HIV/Ryan White;
- – those that focus on the elderly, children, and special populations;
- – school/education groups;
- – faith-based groups;
- – health care coalitions;
- – public safety/homeland security; and
- – groups that focus on specific diseases or conditions (e.g., homelessness, poverty, domestic violence).
![]() Assess each group/meeting for the potential to integrate in recovery planning, by either using group time for parallel meetings or soliciting participation in a newly formed recovery coalition.
Assess each group/meeting for the potential to integrate in recovery planning, by either using group time for parallel meetings or soliciting participation in a newly formed recovery coalition.
![]() Evaluate for potential funding streams to facilitate and support groups.
Evaluate for potential funding streams to facilitate and support groups.
![]() Ensure that public health is engaged in recovery planning.
Ensure that public health is engaged in recovery planning.
![]() Engage urban and regional planners and city/county managers in the development of the community health improvement and recovery plans.
Engage urban and regional planners and city/county managers in the development of the community health improvement and recovery plans.
![]() Create materials to educate nonhealth partners on health impacts that should be included in disaster recovery planning and impacts to their sector, as well as the value of a Health in All Policies approach and the cost of failure.
Create materials to educate nonhealth partners on health impacts that should be included in disaster recovery planning and impacts to their sector, as well as the value of a Health in All Policies approach and the cost of failure.
![]() Educate on recovery-related funding and strategies for its future use.
Educate on recovery-related funding and strategies for its future use.
![]() Educate emergency managers and community planners on integrating health improvement into disaster recovery and the importance of engaging those with community health knowledge in pre-disaster recovery planning.
Educate emergency managers and community planners on integrating health improvement into disaster recovery and the importance of engaging those with community health knowledge in pre-disaster recovery planning.
--------------------------
Priority: Ensure That Public Health Community Programs and Services Are Integrated into Healthy Community and Disaster Recovery Planning Processes
Primary Actors: State/Local Health Departments
Key Partners: Elected Officials and Community Leaders, Urban and Regional Planning Agencies, Community- and Faith-Based Organizations, Emergency Management Agencies
Pre-Event
Key Recovery Strategies:
- Leverage existing relationships and networks (e.g., coalitions, collaboratives) to integrate public health and other community partners into recovery planning.
- Identify opportunities for alignment between ongoing public health improvement processes (e.g., accreditation prerequisites of community health assessments and community health improvement plans) and recovery planning.
Activities include but are not limited to:
For external programs and services:
![]() Work with partner agencies to identify gaps and prioritize recovery resources.
Work with partner agencies to identify gaps and prioritize recovery resources.
![]() Identify community-based organizations with capacities that can be used in recovery (e.g., food services, shelters, counseling).
Identify community-based organizations with capacities that can be used in recovery (e.g., food services, shelters, counseling).
![]() Use face-to-face contact with community members to educate on disaster preparedness to improve individual and community resiliency.
Use face-to-face contact with community members to educate on disaster preparedness to improve individual and community resiliency.
![]() Develop post-disaster communications strategies with partner agencies.
Develop post-disaster communications strategies with partner agencies.
For internal programs and services:
![]() Pre-identify essential services to be priorities during recovery and areas in which recovery resources can be used to develop new programs to improve health.
Pre-identify essential services to be priorities during recovery and areas in which recovery resources can be used to develop new programs to improve health.
![]() Identify program areas within public health departments in which alignment exists.
Identify program areas within public health departments in which alignment exists.
![]() Exploit cross-cutting activities for accreditation and public health emergency planning.
Exploit cross-cutting activities for accreditation and public health emergency planning.
![]() Connect program leads with the goal of information and resource sharing and the creation of synergy among programs.
Connect program leads with the goal of information and resource sharing and the creation of synergy among programs.
![]() Establish strategic plans to leverage activities/resources/contacts.
Establish strategic plans to leverage activities/resources/contacts.
![]() Exploit the opportunity to cross-train public health staff and volunteers and partners.
Exploit the opportunity to cross-train public health staff and volunteers and partners.
![]() Document overlapping areas to show progress toward strategic goals.
Document overlapping areas to show progress toward strategic goals.
![]() Exercise and train for recovery activities.
Exercise and train for recovery activities.
--------------------------
Priority: Leverage Pre-Disaster Preparedness Activities in Recovery Planning
Primary Actors: State/Local Health Departments
Key Partners: Emergency Management Agencies, Health and Medical System Partners, Community- and Faith-Based Organizations
Key Recovery Strategy:
- Identify opportunities for alignment between ongoing public health improvement processes (e.g., accreditation prerequisites of community health assessments and community health improvement plans) and recovery planning.
Pre-Event
Activities include but are not limited to:
![]() Enhance regulatory and accreditation requirements to support more intensive pre-event recovery planning by local and state public health agencies, health care organizations, behavioral health agencies, social services agencies, and local and state emergency management agencies using standard criteria.
Enhance regulatory and accreditation requirements to support more intensive pre-event recovery planning by local and state public health agencies, health care organizations, behavioral health agencies, social services agencies, and local and state emergency management agencies using standard criteria.
![]() Develop health department continuity of operations plans that enable impacted jurisdictions to rapidly overcome damage and engage in recovery efforts by utilizing either local health department staff or public health staff from other jurisdictions.
Develop health department continuity of operations plans that enable impacted jurisdictions to rapidly overcome damage and engage in recovery efforts by utilizing either local health department staff or public health staff from other jurisdictions.
![]() Promote and develop public health rapid assessment teams familiar with local and state emergency response and recovery plans and trained to conduct post-disaster community assessments.
Promote and develop public health rapid assessment teams familiar with local and state emergency response and recovery plans and trained to conduct post-disaster community assessments.
![]() Educate and train medical system and emergency management partners regarding the roles and responsibilities of the public health assessment team during recovery efforts.
Educate and train medical system and emergency management partners regarding the roles and responsibilities of the public health assessment team during recovery efforts.
![]() Routinely train and engage personnel assigned assessment responsibilities in local, regional, state, and national disaster exercises.
Routinely train and engage personnel assigned assessment responsibilities in local, regional, state, and national disaster exercises.
![]() Build in the capacity to identify gaps to be closed to achieve an optimally healthy community.
Build in the capacity to identify gaps to be closed to achieve an optimally healthy community.
Short-Term Recovery
Priority: Participate in a Shared Communication Effort
Primary Actors: State/Local Health Departments, Emergency Management Agencies
Key Partners: Elected Officials and Community Leaders, Health and Medical System Partners, Behavioral Health Authorities
Activities include but are not limited to:
![]() Establish and operate a recovery joint information system staffed with representatives from all engaged sectors.
Establish and operate a recovery joint information system staffed with representatives from all engaged sectors.
![]() Assign health department public information officer(s) to the public health incident command system.
Assign health department public information officer(s) to the public health incident command system.
![]() Engage both internal and external subject matter experts as necessary.
Engage both internal and external subject matter experts as necessary.
![]() Ensure that public health agency information officers participate actively in the jurisdictional joint information center or joint information system.
Ensure that public health agency information officers participate actively in the jurisdictional joint information center or joint information system.
![]() Identify outreach methods and key messages.
Identify outreach methods and key messages.
![]() Integrate health messages with general emergency management messages related to ongoing recovery efforts, focusing on safety and injury prevention and other event-specific public health messages.
Integrate health messages with general emergency management messages related to ongoing recovery efforts, focusing on safety and injury prevention and other event-specific public health messages.
![]() Ensure that communication plans address appropriate risk communication strategies.
Ensure that communication plans address appropriate risk communication strategies.
![]() Engage leaders of community-based organizations in communications to vulnerable or nonmainstream audiences.
Engage leaders of community-based organizations in communications to vulnerable or nonmainstream audiences.
![]() Develop a plan for outreach through and monitoring of social media.
Develop a plan for outreach through and monitoring of social media.
--------------------------
Priority: Conduct Impact Assessments on the Health and Medical Needs of the Community
Primary Actors: State/Local Health Departments
Key Partners: Health and Medical System Partners, Social Services Agencies, Emergency Management Agencies
Key Recovery Strategy:
- Use and expand health technology infrastructure for data collection and analysis to facilitate data sharing, evidence-based decision making, and continual evaluation of progress toward an optimally healthy community.
Activities include but are not limited to:
![]() Deploy public health rapid assessment teams familiar with local and state emergency response and recovery plans and trained to conduct pre- and post-disaster community assessments.
Deploy public health rapid assessment teams familiar with local and state emergency response and recovery plans and trained to conduct pre- and post-disaster community assessments.
![]() Work with health system leaders to assess impacts on health care facilities, emergency medical services, long-term care facilities, and specialty facilities (e.g., dialysis centers).
Work with health system leaders to assess impacts on health care facilities, emergency medical services, long-term care facilities, and specialty facilities (e.g., dialysis centers).
![]() Work with emergency management agencies and applicable volunteer agencies to assess the need and potential duration for mass shelters, including special needs shelters and needs within existing shelter operations.
Work with emergency management agencies and applicable volunteer agencies to assess the need and potential duration for mass shelters, including special needs shelters and needs within existing shelter operations.
Short-Term Recovery
![]() Work with emergency management agencies to assess the need for a public health emergency declaration and provide data to support requests for assistance.
Work with emergency management agencies to assess the need for a public health emergency declaration and provide data to support requests for assistance.
![]() Collect and compile service restoration timelines from key public health and medical system partners.
Collect and compile service restoration timelines from key public health and medical system partners.
![]() Evaluate data, create reports, and communicate findings to responding agencies, stakeholders, and the community at large.
Evaluate data, create reports, and communicate findings to responding agencies, stakeholders, and the community at large.
--------------------------
Priority: Reestablish Critical Public Health Infrastructure
Primary Actors: State/Local Health Departments
Key Partners: Elected Officials and Community Leaders
Activities include but are not limited to:
![]() Reestablish public health department programs based on preestablished (as identified in continuity of operations/continuity of government) departmental service priorities, using temporary service sites if needed.
Reestablish public health department programs based on preestablished (as identified in continuity of operations/continuity of government) departmental service priorities, using temporary service sites if needed.
![]() Develop strategies for increasing workforce capacity to meet surge in needs.
Develop strategies for increasing workforce capacity to meet surge in needs.
![]() Restore access to vital records.
Restore access to vital records.
![]() As reestablishment takes place, identify opportunities and organize activities in a manner that may close the gap between existing conditions, or even the pre-disaster state, and an optimal healthy community.
As reestablishment takes place, identify opportunities and organize activities in a manner that may close the gap between existing conditions, or even the pre-disaster state, and an optimal healthy community.
--------------------------
Priority: Deliver Public Health Services to Meet Post-Disaster Needs of the Community
Primary Actors: State/Local Health Departments
Key Partners: Social Services Agencies, Community- and Faith-Based Organizations
Activities include but are not limited to:
![]() Conduct licensed and unlicensed food vendor inspections (including mass shelters with feeding operations).
Conduct licensed and unlicensed food vendor inspections (including mass shelters with feeding operations).
![]() Focus immunization efforts on responders, victims, and volunteers.
Focus immunization efforts on responders, victims, and volunteers.
![]() Provide behavioral health support.
Provide behavioral health support.
![]() Ensure the availability of services related to functional needs/at-risk populations.
Ensure the availability of services related to functional needs/at-risk populations.
![]() Provide mass shelter support as needed.
Provide mass shelter support as needed.
![]() Provide fatality management support.
Provide fatality management support.
![]() If necessary, issue a public health emergency declaration to assist with debris removal and cleanup.
If necessary, issue a public health emergency declaration to assist with debris removal and cleanup.
Short-Term Recovery
Priority: Provide Support to Impacted Health Care Delivery Systems
Primary Actors: State/Local Health Departments, Health and Medical System Partners
Key Partners: Social Services Agencies, Emergency Management Agencies, Behavioral Health Authorities
Activities include but are not limited to:
![]() Engage health and medical system partners and/or health care coalition members early in the Emergency Support Function (ESF) #8 response and recovery efforts.
Engage health and medical system partners and/or health care coalition members early in the Emergency Support Function (ESF) #8 response and recovery efforts.
![]() Integrate health care coalition leadership within the public health incident command system.
Integrate health care coalition leadership within the public health incident command system.
![]() Establish needed emergency medical treatment capabilities within impacted area.
Establish needed emergency medical treatment capabilities within impacted area.
![]() Mobilize and deploy Medical Reserve Corps or Emergency System for Advance Registration of Volunteer Health Professionals (ESAR-VHP) volunteers to support efforts.
Mobilize and deploy Medical Reserve Corps or Emergency System for Advance Registration of Volunteer Health Professionals (ESAR-VHP) volunteers to support efforts.
![]() Implement strategies designed to retain the health and medical services workforce.
Implement strategies designed to retain the health and medical services workforce.
![]() Coordinate necessary patient transport out of impacted areas.
Coordinate necessary patient transport out of impacted areas.
![]() Engage in a process for wellness checks.
Engage in a process for wellness checks.
![]() Ensure access to and availability of pharmaceuticals, including psychotropics.
Ensure access to and availability of pharmaceuticals, including psychotropics.
![]() Coordinate health care (including behavioral health) resources and volunteers responding to the area.
Coordinate health care (including behavioral health) resources and volunteers responding to the area.
![]() Rapidly mobilize health department staff to expedite reviews of medical facility plans and surveys of facilities to determine readiness to be reopened to the public; reopen minimally damaged facilities.
Rapidly mobilize health department staff to expedite reviews of medical facility plans and surveys of facilities to determine readiness to be reopened to the public; reopen minimally damaged facilities.
![]() Identify opportunities to improve care and the configuration and location of services to best meet the needs of the community.
Identify opportunities to improve care and the configuration and location of services to best meet the needs of the community.
Intermediate- to Long-Term Recovery
Priority: Facilitate Health-Informed Recovery Decision Making Through Data
Primary Actors: State/Local Health Departments
Key Partners: Health and Medical System Partners, Social Services Agencies, Urban and Regional Planning Agencies
Key Recovery Strategies:
- Leverage existing relationships and networks (e.g., coalitions, collaboratives) to integrate public health and other community partners into recovery planning.
- Educate nonhealth sectors and the community on why health is integral to recovery and how recovery activities impact health outcomes.
- Use and expand health technology infrastructure for data collection and analysis to facilitate data sharing, evidence-based decision making, and continual evaluation of progress toward an optimally healthy community.
Activities include but are not limited to:
![]() Ensure ongoing operation of an incident command system that provides for routine assessment of health and medical needs by public health staff working jointly with health, social services, and medical community partners.
Ensure ongoing operation of an incident command system that provides for routine assessment of health and medical needs by public health staff working jointly with health, social services, and medical community partners.
![]() Assess access to mental/behavioral health services, health care services, public health services, and social services.
Assess access to mental/behavioral health services, health care services, public health services, and social services.
--------------------------
Priority: Engage in Community Rebuilding and Redevelopment Planning to Identify Opportunities to Enhance Population Health
Primary Actors: State/Local Health Departments
Key Partners: Emergency Management Agencies, Urban and Regional Planning Agencies, Education System, Transportation Agencies, Housing Agencies
Key Recovery Strategies:
- Leverage existing relationships and networks (e.g., coalitions, collaboratives) to integrate public health and other community partners into recovery planning.
- Educate nonhealth sectors and the community on why health is integral to recovery and how recovery activities impact health outcomes.
Activities include but are not limited to:
![]() Engage community leaders early in the process to encourage their interest in participating in broader community redevelopment processes.
Engage community leaders early in the process to encourage their interest in participating in broader community redevelopment processes.
![]() Educate community leaders, in conjunction with urban and regional planners, on the elements of a resilient and healthy community, the important opportunity to utilize recovery efforts to achieve that goal, and the applicability of such tools as health impact assessments to inform decision making.
Educate community leaders, in conjunction with urban and regional planners, on the elements of a resilient and healthy community, the important opportunity to utilize recovery efforts to achieve that goal, and the applicability of such tools as health impact assessments to inform decision making.
![]() Assist with identifying sources of capital and financing for rebuilding in ways that promote health.
Assist with identifying sources of capital and financing for rebuilding in ways that promote health.
Intermediate- to Long-Term Recovery
![]() Continuously measure progress toward healthy community goals and adapt recovery and health improvement plans accordingly.
Continuously measure progress toward healthy community goals and adapt recovery and health improvement plans accordingly.
![]() Organize and implement a health-related advisory committee or subcommittee of the jurisdictional long-term recovery effort.
Organize and implement a health-related advisory committee or subcommittee of the jurisdictional long-term recovery effort.
![]() Inform and advocate for infrastructure investments that strengthen safety and resilience, such as improved construction standards, safe rooms and storm shelters (where appropriate), underground utilities, and energy-efficient standards/construction.
Inform and advocate for infrastructure investments that strengthen safety and resilience, such as improved construction standards, safe rooms and storm shelters (where appropriate), underground utilities, and energy-efficient standards/construction.
![]() Educate local and state leaders on lessons learned as a result of the disaster and ways to build stronger, more resilient communities.
Educate local and state leaders on lessons learned as a result of the disaster and ways to build stronger, more resilient communities.
--------------------------
Priority: Share Lessons Learned with Other Communities to Improve Post-Disaster Recovery Planning
Primary Actors: State/Local Health Departments, Health and Medical System Partners, Emergency Management Agencies
Key Partners: Community- and Faith-Based Organizations, Elected Officials and Community Leaders
Activities include but are not limited to:
![]() Participate in after-action processes, including analysis of lessons learned and identification of opportunities for improvement.
Participate in after-action processes, including analysis of lessons learned and identification of opportunities for improvement.
![]() Utilize state, regional, and national conferences, workshops, and discipline-specific professional meetings to share lessons learned and opportunities for improvement so that other jurisdictions can benefit from recovery experiences.
Utilize state, regional, and national conferences, workshops, and discipline-specific professional meetings to share lessons learned and opportunities for improvement so that other jurisdictions can benefit from recovery experiences.
![]() Disseminate information regarding opportunities for improved public health to health sector and nonhealth groups, such as the council of mayors, city managers, city councilors, emergency management agencies, and urban and regional planners.
Disseminate information regarding opportunities for improved public health to health sector and nonhealth groups, such as the council of mayors, city managers, city councilors, emergency management agencies, and urban and regional planners.
AHRQ (Agency for Healthcare Research and Quality). 2005. National Hospital Available Beds for Emergencies and Disasters (HAvBED) system: Final report. AHRQ Publication No. 05-0103. Rockville, MD: AHRQ.
The Alliance for a Just Rebuilding, ALIGN, Community Development Project at the Urban Justice Center, Community Voices Heard, Faith in New York, Families United for Racial and Economic Equality, Good Old Lower East Side, Red Hook Initiative, and New York Communities for Change. 2014. Weathering the storm: Rebuilding a more resilient New York City Housing Authority post-Sandy. http://www.rebuildajustny.org/wp-content/uploads/2014/03/Weathering_The_Storm.pdf (accessed October 20, 2014).
APA (American Planning Association). 2006. Integrating planning and public health (PAS 539/540). APA Planning Advisory Service. Washington, DC: APA.
ASPR (Office of the Assistant Secretary for Preparedness and Response). 2012. Healthcare preparedness capabilities: National guidance for healthcare system preparedness. Washington, DC: HHS.
ASPR. 2015. Core mission areas. http://www.phe.gov/about/oem/recovery/Pages/rsf-core.aspx (accessed February 26, 2015).
ASTHO (Association of State and Territorial Health Officials). 2007. Disaster recovery for public health. http://www.astho.org/programs/preparedness/disaster-recovery-for-public-health (accessed November 18, 2014).
Barnett, K. 2012. Best practices for community health needs assessment and implementation strategy development: A review of scientific methods, current practices, and future potential. In Report of proceedings from a public forum and interviews of experts. http://www.phi.org/uploads/application/files/dz9vh55o3bb2x56lcrzyel83fwfu3mvu24oqqvn5z6qaeiw2u4.pdf (accessed August 25, 2014).
Beardsley, D. 2014. Session I: Public health, panel discussion. Paper presented at IOM Committee on Post-Disaster Recovery of a Community’s Public Health, Medical, and Social Services: Meeting Two, February 3, Washington, DC.
Berggren, R. E., and T. J. Curiel. 2006. After the storm—health care infrastructure in post-Katrina New Orleans. New England Journal of Medicine 354(15):1549-1552.
Blumenstock, J. 2014. Coordination among state and local government agencies. Paper presented at IOM Committee on Post-Disaster Recovery of a Community’s Public Health, Medical, and Social Services: Meeting Three, April 28-29, Washington, DC.
CDC (Centers for Disease Control and Prevention). 2011. Public health preparedness capabilities: National standards for state and local planning. Washington, DC: HHS.
CDC. 2014a. Health Alert Network (HAN). http://www.bt.cdc.gov/han (accessed November 18, 2014).
CDC. 2014b. The public health system and the 10 essential public health services. http://www.cdc.gov/nphpsp/essentialservices.html (accessed February 6, 2014).
CDC. 2014c. Winnable battles. http://www.cdc.gov/winnablebattles (accessed November 18, 2014).
Center for Disaster Philanthropy. 2012. The impact of disasters on public health. http://disasterphilanthropy.org/the-impact-of-disasters-on-public-health (accessed November 26, 2014).
Chandra, A., J. Acosta, S. Howard, L. Uscher-Pines, M. Williams, D. Yeung, J. Garnett, and L. S. Meredith. 2011. Building community resilience to disasters: A way forward to enhance national health security. http://www.sciencedirect.com/science/article/pii/S0277953612005953 (accessed November 18, 2014).
Chandra, A., M. Williams, A. Plough, A. Stayton, K. B. Wells, M. Horta, and J. Tang. 2013. Getting actionable about community resilience: The Los Angeles County Community Disaster Resilience Project. American Journal of Public Health 103(7):1181-1189.
Clements, B. 2014. Public health and community recovery: Texas’ experience. Paper presented at IOM Committee on Post-Disaster Recovery of a Community’s Public Health, Medical, and Social Services: Meeting Two, February 3, Washington, DC.
Community Commons. 2014a. Community Health Needs Assessment (CHNA). http://assessment.communitycommons.org/chna/About.aspx (accessed November 18, 2014).
Community Commons. 2014b. Indicator data list. http://assessment.communitycommons.org/CHNA/Datalist.aspx (accessed November 18, 2014).
CVS Caremark. 2014. CVS disaster relief. http://info.cvscaremark.com/newsroom/featured-topics/disaster-relief (accessed November 18, 2014).
DeSalvo, K., N. Lurie, K. Finne, C. Worrall, A. Bogdanov, A. Dinkler, S. Babcock, and J. Kelman. 2014. Using Medicare data to identify individuals who are electricity dependent to improve disaster preparedness and response. American Journal of Public Health 104(7):1160-1164.
DHS (U.S. Department of Homeland Security) and EPA (U.S. Environmental Protection Agency). 2010. Memorandum of agreement between the Department of Homeland Security (DHS), Federal Emergency Management Agency (FEMA) and the Environmental Protection Agency (EPA). http://www.epa.gov/dced/pdf/2011_0114_fema-epamoa.pdf (accessed November 18, 2014).
DOT (U.S. Department of Transportation), EPA (U.S. Environmental Protection Agency), and HUD (U.S. Department of Housing and Urban Development). 2014. Partnership for sustainable communities: Five years of learning from communities and coordinating federal investments. Washington, DC: DOT, EPA, and HUD.
Duncan, W. J., P. M. Ginter, A. C. Rucks, M. S. Wingate, and L. C. McCormick. 2007. Organizing emergency preparedness within United States public health departments. Public Health 121(4):241-250.
Fairfax County. 2012. Fairfax County pre-disaster recovery plan. http://www.fairfaxcounty.gov/oem/pdrp/pdrpcomplete-doc-march2012.pdf (accessed November 18, 2014).
FEMA (Federal Emergency Management Agency). 2008. Emergency support function #8—public health and medical services annex. http://www.fema.gov/media-library-data/20130726-1825-25045-8027/emergency_support_function_8_public_health___medical_services_annex_2008.pdf (accessed February 26, 2015).
FEMA. 2010. Guidance on planning for integration of functional needs support services in general population shelters. Washington, DC: DHS.
FEMA. 2011. National disaster recovery framework. Washington, DC: FEMA.
FEMA. n.d. State partnership—Safeguard Iowa Partnership. http://www.fema.gov/pdf/privatesector/ia_ppp.pdf (accessed November 18, 2014).
HHS (U.S. Department of Health and Human Services). 2007. Medical surge capacity and capability: A management system for integrating medical and health resources during large-scale emergencies. http://www.phe.gov/preparedness/planning/mscc/handbook/documents/mscc080626.pdf (accessed March 24, 2015).
HHS. 2009. National health security strategy of the United States of America. Washington, DC: HHS.
HHS. 2014a. HHS disaster behavioral health concept of operations. http://www.phe.gov/Preparedness/planning/abc/Documents/dbh-conops-2014.pdf (accessed October 21, 2014).
HHS. 2014b. HIPAA privacy in emergency situations. Washington, DC: HHS.
Hillsborough County Government. 2010. Post-disaster redevelopment plan. http://www.hillsboroughcounty.org/index.aspx?nid=1795 (accessed November 18, 2014).
IOM (Institute of Medicine). 1988. The future of public health. Washington, DC: National Academy Press.
IOM. 2003. The future of the public’s health in the 21st century. Washington, DC: The National Academies Press.
IOM. 2014. The impacts of the Affordable Care Act on preparedness resources and programs: Workshop summary. Washington, DC: The National Academies Press.
IRS (Internal Revenue Service). 2013. IRB 2013-21. http://www.irs.gov/irb/2013-21_IRB/ar09.html (accessed December 1, 2014).
Klitzman, S., and N. Freudenberg. 2003. Implications of the World Trade Center attack for the public health and health care infrastructures. American Journal of Public Health 93(3):400-406.
Knearl, E. 2014. Role of public information in health systems recovery. Paper presented at IOM Committee on Post-Disaster Recovery of a Community’s Public Health, Medical, and Social Services: Meeting Three, April 28-29, Washington, DC.
LACCDR (Los Angeles County Community Disaster Resilience). 2014. What is community resilience? http://www.laresilience.org (accessed August 26, 2014).
Lockwood, B. 2014. Coordination among state and local government agencies. Paper presented at IOM Committee on Post-Disaster Recovery of a Community’s Public Health, Medical, and Social Services: Meeting Three, April 28-29, Washington, DC.
Mattessich, P. W., and E. J. Rausch. 2013. Collaboration to build healthier communities: A report for the Robert Wood Johnson Foundation Commission to Build a Healthier America. http://www.rwjf.org/content/dam/farm/reports/surveys_and_polls/2013/rwjf406479 (accessed November 18, 2014).
Morton, M. J., and N. Lurie. 2013. Community resilience and public health practice. American Journal of Public Health 103(7):1158-1160.
NACCHO (National Association of County and City Health Officials). 2011. National public health performance standards: Local implementation guide version 3.0. http://www.naccho.org/topics/infrastructure/NPHPSP/loader.cfm?csModule=security/getfile&pageid=256555 (accessed March 2, 2015).
NACCHO. 2012. Role of local health departments in community health needs assessments. http://naccho.org/advocacy/positions/upload/12-05-Role-of-LHDs-in-CHNA.pdf (accessed November 18, 2014).
NACCHO. 2013. Local health department job losses and program cuts: Findings from the 2013 profile study. http://www.naccho.org/topics/infrastructure/lhdbudget/upload/Survey-Findings-Brief-8-13-13-3.pdf (accessed November 18, 2014).
NACCHO. 2014a. 2013 national profile of local health departments. http://www.naccho.org/topics/infrastructure/profile/upload/2013-National-Profile-of-Local-Health-Departments-report.pdf (accessed November 5, 2014).
NACCHO. 2014b. MAPP framework. http://www.naccho.org/topics/infrastructure/mapp/framework/index.cfm (accessed November 18, 2014).
NBSB (National Biodefense Science Board). 2014. Community health resilience report. Washington, DC: NBSB.
Nolen, A. 2014. A health in all policies approach to disaster recovery: Lessons from Galveston. Paper presented at IOM Committee on Post-Disaster Recovery of a Community’s Public Health, Medical, and Social Services: Meeting Four, June 13, Washington, DC.
NRC (National Research Council). 2012. Disaster resilience: A national imperative. Washington, DC: The National Academies Press.
PHAB (Public Health Accreditation Board). 2011. Acronyms and glossary of terms. http://www.phaboard.org/wpcontent/uploads/PHAB-Acronyms-and-Glossary-of-Terms-Version-1.0.pdf (accessed November 18, 2014).
PHAB. 2012. National public health department accreditation prerequisites. http://www.phaboard.org/wp-content/uploads/PrerequisitesJuly-2012.pdf (accessed November 18, 2014).
PHAB. 2013. Standards & measures. http://www.phaboard.org/wp-content/uploads/SM-Version-1.5-Board-adoptedFINAL-01-24-2014.docx.pdf (accessed November 18, 2014).
Plough, A., J. E. Fielding, A. Chandra, M. Williams, D. Eisenman, K. B. Wells, G. Y. Law, S. Fogleman, and A. Magaña. 2013. Building community disaster resilience: Perspectives from a large urban county department of public health. American Journal of Public Health 103(7):1190-1197.
Rudolph, L., J. Caplan, K. Ben-Moshe, and L. Dillon. 2013. Health in all policies: A guide for state and local governments. http://www.phi.org/uploads/files/Health_in_All_Policies-A_Guide_for_State_and_Local_Governments.pdf (accessed November 18, 2014).
Rudowitz, R., D. Rowland, and A. Shartzer. 2006. Health care in New Orleans before and after Hurricane Katrina. Health Affairs 25(5):w393-w406.
Runkle, J. D., A. Brock-Martin, W. Karmaus, and E. R. Svendsen. 2012. Secondary surge capacity: A framework for understanding long-term access to primary care for medically vulnerable populations in disaster recovery. American Journal of Public Health 102(12):e24-e32.
RWJF (Robert Wood Johnson Foundation). 2013. New Orleans, Louisiana: 2013 RWJF culture of health prize. http://www.rwjf.org/en/about-rwjf/newsroom/newsroom-content/2013/02/new-orleans--louisiana--2013-roadmaps-tohealth-prize.html (accessed November 18, 2014).
RWJF. 2014. Building a culture of health: 2014 President’s message. http://www.rwjf.org/content/dam/files/rwjf-webfiles/Annual_Message/2014_RWJF_AnnualMessage_final.pdf (accessed April 5, 2014).
Safeguard Iowa Partnership. 2013. 2013 annual report. https://safeguardiowa.wildapricot.org/Resources/Documents/Annual%20Meeting/2013/2013%20SIP%20ANNUAL%20REPORT.pdf (accessed November 18, 2014).
Salinsky, E. 2010. Governmental public health: An overview of state and local public health agencies. National Health Policy Forum, background paper no. 77. http://www.nhpf.org/library/background-papers/BP77_GovPublicHealth_08-18-2010.pdf (accessed March 2, 2015).
Shah, U. 2014. Coordination among state and local government agencies. Paper presented at IOM Committee on Post-Disaster Recovery of a Community’s Public Health, Medical, and Social Services: Meeting Three, April 28-29, Washington, DC.
Smith, G. 2011. Planning for post-disaster recovery: A review of the United States disaster assistance framework. Fairfax, VA: Public Entity Risk Institute.
Stevenson, A., A. Humphrey, and S. Brinsdon. 2014. A health in all policies response to disaster recovery. Perspectives in Public Health 134(3):125-126.
UTMB (University of Texas Medical Branch at Galveston). 2011. Mental health continuum of care program. http://www.utmbhpla.org/doc/Page.asp?PageID=DOC000725 (accessed November 18, 2014).
White, J. 2014. Post-disaster social services and health outcomes in recovery. Paper presented at IOM Committee on Post-Disaster Recovery of a Community’s Public Health, Medical, and Social Services: Meeting Two, February 3, Washington, DC.
Zucker, H. 2014. Post-disaster recovery: New York State Department of Health experience with Superstorm Sandy. Paper presented at IOM Committee on Post-Disaster Recovery of a Community’s Public Health, Medical, and Social Services: Meeting Two, February 3, Washington, DC.












































