
“Every American should have the opportunity to be as healthy as he or she can be.
Every community should be safe from threats to its health. And all individuals
and families should have a high level of services that protect, promote, and
preserve their health, regardless of who they are or where they live.”
—Trust for America’s Health (TFAH, 2013b)
The above quote from Trust for America’s Health is indicative of the widely shared social and civilizing ethic that people should live in communities1 that maximize opportunities to be healthy2 and minimize preventable misery and suffering from disease. Disasters are by their very nature devastating to communities, often having significant and long-lasting effects on the physical, mental, and social wellbeing of the impacted population that compromise the realization of a healthy community (see Box 1-1). Further, disaster-related effects may be experienced differentially within a community as a result of the disproportionate vulnerability of certain subpopulations (see Box 1-2). Each year the nation experiences approximately 60 presidentially declared major disasters3 and a far greater number that do not receive such a declaration.4 Not only do they result in tragic loss of human life and have devastating health consequences for survivors; they also often require the expenditure of billions of dollars in public, private, and philanthropic funds for recovery (see Figure 1-1). Depending on the nature of the disaster and its impact,
________________
1 Community can be defined in multiple ways—for example, as a population of individuals that share a geographic area, a culture, religious beliefs, or self-defined interests. For communities defined by geographic area, the scale varies from macro (e.g., national level) to hyperlocal (neighborhood or even block level). For the purposes of this report, the term “community” refers to a community of place at the city or county level, unless otherwise indicated.
2 Health, as defined by the World Health Organization (WHO, 1948) is “a state of complete physical, mental, and social wellbeing and not merely the absence of disease or infirmity.”
3 This number was derived from Federal Emergency Management Agency (FEMA) data available at https://www.fema.gov/disasters/grid/year. Major disaster declarations are made by the President of the United States following a request from the governor of an affected state that is submitted through the regional FEMA office.
4 According to estimates from FEMA, less than 10 percent of all disasters in the United States receive a presidential disaster declaration (FEMA, 2010).
BOX 1-1
Disaster Impacts on Health
The impact of a disaster on the health of a community is complex to predict, difficult to measure, and heavily influenced by both health- and nonhealth-related preexisting factors, including
- the level of pre-disaster planning,
- community demographics,
- social and economic conditions,
- community health status,
- community cohesion and cultural practices,
- geography, and
- any history of previous disaster events.
Disasters have direct and indirect impacts on physical and/or mental health that may manifest in the short-, intermediate-, and long-term post-disaster periods. These effects are worse for vulnerable populations in particular. Indirect effects occur through the disruption of access to health-sustaining goods and services and deterioration of living conditions immediately following a disaster and, in some cases, for extended periods of time thereafter. In many cases, disasters exacerbate preexisting health conditions at the individual and community levels.
Impacts on Short-Term Health Outcomes
- Physical and mental trauma and illness: Direct causes of morbidity and mortality vary by disaster type. Examples of physical health impacts include lacerations, punctures, and trauma caused by debris or falling objects; drowning; burns; and infections (epidemics). Accidents after disasters (e.g., during debris removal or reconstruction) are another common cause of physical trauma. While most disaster survivors display remarkable resilience and experience only short periods of shock, some develop immediate symptoms of psychopathology, such as acute stress disorder or posttraumatic stress disorder (PTSD).
- Lack of access to life-sustaining resources and medications: In the early post-disaster period, lack of access to safe food, clean water, shelter, and critical medications may contribute to additional disaster-related morbidity and mortality. Deaths and illnesses may occur from dehydration, consumption of contaminated food or water, exposure to the elements, carbon monoxide poisoning (from incorrect use of heaters and generators), and heatstroke. Loss of power may be catastrophic for those dependent on medical devices powered by electricity, such as individuals undergoing dialysis.
- Impacts from disruption of critical emergency and medical services and infrastructure: During the disaster response phase, the predominant focus is on saving lives through search and rescue operations and the provision of emergency medical care. These critical services may be directly impacted (e.g., by infrastructure loss), or access to the services may be hindered by the disaster’s effects on transportation systems (e.g., responders cannot access certain areas, or community members cannot reach medical facilities). Furthermore, limited resources may necessitate a transition from conventional standards of
strategic planning and resource allocation decisions must be made; public works, roads, homes, and businesses must be rebuilt; and medical services must be provided and care delivery systems restored. The committee that conducted this study explicitly rejected the traditional characterization of disaster recovery as a process that restores a community to pre-disaster conditions. When viewed through a health lens, this formulation is shortsighted given the general state of suboptimal health status that characterizes so many American communities and the associated economic and societal costs. Although the United States spends
care to contingency or crisis standards of care (IOM, 2012a). In such cases, otherwise preventable morbidity (e.g., infection of wounds) and mortality (e.g., victims succumbing to injuries) may occur.
Intermediate- and Long-Term Health Outcomes
- Effects of trauma and chronic stress on behavioral health: The psychosocial impacts of a disaster may not manifest in survivors until weeks, months, or even years later and may include changes in emotional, physical, cognitive, and interpersonal conditions (Landesman, 2005). These effects may be brought on by the trauma of the disaster itself or by secondary causes such as disruption of social networks, bereavement and loss, and chronic stress associated with the challenges of recovery. The effects of chronic stress on health worsen as recovery time increases. In addition to PTSD, depression and anxiety disorders are serious post-disaster mental health sequelae. Trauma and stress also may induce behaviors that negatively impact health, such as substance abuse and other risky behaviors, as well as violence and abuse.
- Effects of physical stress: The physical demands of recovery can have minor (e.g., musculoskeletal strains) and serious (e.g., acute myocardial infarction or heart attack) health effects. Increased incidence of heart attack after a disaster may persist for years and may be associated with chronic stress (Peters et al., 2014).
- Impacts from degraded capacity of or access to health and human services: Following the disaster response phase, increased demand for primary care services can be associated with, for example, the need for chronic disease management and follow-up care for those who sustained acute injuries during or immediately after the disaster. Chronic illnesses are exacerbated by conditions during the early recovery period (lack of nutritious food, impeded access to medications, stress) (Mensah et al., 2005). Preventable morbidity and mortality result when disrupted health systems are unable to meet this secondary surge or when community members cannot access primary care services (Runkle et al., 2012). Disruption of social services that ensure access of vulnerable populations to resources for disease management further contributes to negative health outcomes.
- Exposure to pollutants and degradation of environmental conditions: Disasters can cause a number of environmental public health concerns. For example, sanitation problems can give rise to infectious diseases such as food and waterborne illnesses and skin infections. Exposure to mold and endotoxins associated with microbial growth in water-damaged buildings may exacerbate asthma and contribute to other acute and chronic respiratory disorders. Exposure to pollutants (e.g., industrial chemicals) in water, food, sediment, or air can result in acute toxic effects, development or exacerbation of chronic health conditions (e.g., respiratory disorders), and cancer (Brandt et al., 2006).
- Impacts on social determinants of health: Major disasters impact many of the conditions known collectively as social determinants of health, such as employment opportunities, the quality and affordability of housing, schooling and child care, and transportation access to essential goods and services. Job loss, displacement, and transportation disruption are common after a disaster. Disparities in these social and economic conditions are correlated with health disparities (e.g., rates of malnutrition, obesity-related chronic diseases, infant mortality, and cancer), which are exacerbated by disproportionate effects of disasters on already vulnerable populations (see Box 1-2).
more on health care than does any other country in the world, the health of its citizens is worse than that in many peer nations that spend less, as evidenced by key health status indicators such as lower average life expectancy (see Figure 1-2) and higher incidence of preventable diseases5 (Bradley et al., 2011; NRC
________________
5 In the United States, chronic diseases account for 7 of the 10 leading causes of mortality and affect almost 50 percent of Americans (CDC, 2011). Annual health care spending in the United States has grown to approximately $2.7 trillion, more than 75 percent of which goes to management of preventable chronic diseases (IOM, 2012b; KFF, 2012; RWJF, 2014; TFAH, 2013a).
BOX 1-2
Vulnerable Populations
Vulnerable, or at-risk, populations are, as defined by the U.S. Department of Health and Human Services, those individuals and groups that “[b]efore, during, and after an incident … may have additional needs in one or more of the following functional areas: communication, medical care, maintaining independence, supervision, and transportation. In addition to those individuals specifically recognized as at-risk in the Pandemic and All-Hazards Preparedness Act (i.e., children, senior citizens, and pregnant women), individuals who may need additional response assistance include those who have disabilities, live in institutionalized settings, are from diverse cultures, have limited English proficiency or are non-English speaking, are transportation disadvantaged, have chronic medical disorders, and have pharmacological dependency” (HHS, 2009a, p. 37).
As the community transitions into recovery, vulnerable populations often are the most difficult to reach and/or experience complications and worsening health status as a result of delays in seeking and receiving treatment, provider scarcity and overload, and limited supplies. These populations are at higher risk for negative outcomes after a disaster, including mortality, and may require more time and effort to recover (O’Sullivan et al., 2014).
Although there is no one accepted list of all vulnerable subpopulations, most fall into one or more of the following broad categories that confer vulnerability:
- economic disadvantage;
- language and literacy barriers;
- medical condition or disability (physical, mental, cognitive, or sensory);
- isolation (cultural, geographic [e.g., rural] or social); and
- age (children and the elderly) (CDC, 2010).
Disasters and the conditions left in their wake also may create newly vulnerable populations, thus increasing the scope of the problem during the recovery period. These individuals and families can be difficult to reach and link to services because they have not accessed support services in the past and may be reticent to ask for help. Examples of the newly vulnerable include but are not limited to
- individuals and families previously above the poverty line who may be ineligible for some services because their income level exceeds the cutoff, but who end up destitute as a result of disaster-related costs;
- individuals that develop physical or mental health conditions as a direct or indirect result of the disaster; and
- newly homeless, isolated, or displaced individuals.
Despite clear evidence demonstrating the special needs of vulnerable populations during and after a disaster, these populations continue to be excluded from emergency management planning in some jurisdictions (Sherry and Harkins, 2011). However, recent legislative and judicial proceedings have established some accountability for ensuring that their needs are met. The repercussions of not meeting the needs of at-risk individuals were demonstrated on a national scale after Hurricane Sandy when a federal court found that New York City violated the Americans with Disabilities Act by not adequately protecting the vulnerable disabled population during that disaster (DRA, 2013). This was the first case of its kind in the country, and it has far-reaching implications for emergency planning at the state and local levels. There now is greater focus on vulnerable populations at the federal level as well. The Pandemic and All Hazards Preparedness Act (reauthorized in 2013) requires that the Secretary of Health and Human Services consider the public health and medical needs of at-risk individuals during public health emergencies and, more specifically, “oversee an advisory committee on at-risk persons and disseminate novel and best practices on outreach to and care of the at-risk before, during, and after public health emergencies” (ASTHO, 2012).
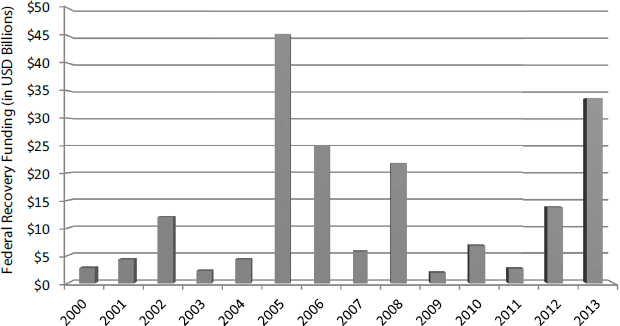
FIGURE 1-1 Federal expenditures on disaster recovery over the past decade.
NOTE: There is no single source for tracking all federal expenditures on recovery assistance. Federal recovery funding estimates in this figure are derived from just three of the largest sources: Federal Emergency Management Agency (FEMA) disaster relief funds, U.S. Department of Housing and Urban Development (HUD) Community Development Block Grant Disaster Recovery funds and Social Services Block Grant Disaster Recovery funds. These estimates are likely underestimates of the total amount of federal recovery assistance from all agencies (Weiss and Weidman, 2013).
SOURCE: Data from CRS (2014) and HUD (2014a).
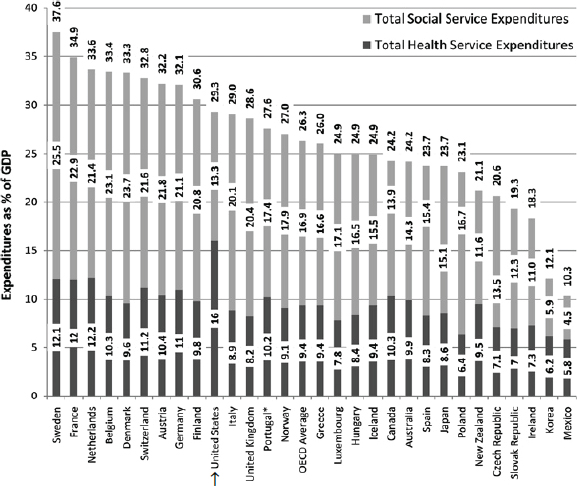
and IOM, 2013; OECD, 2013). In comparison with other nations, expenditures in the United States are disproportionately directed at health care services (see Figure 1-3), despite evidence that a higher ratio of social services to health care spending is significantly associated with better health outcomes (Bradley and Taylor, 2013; Bradley et al., 2011).
It is clear that the process of community planning in the United States has not fully addressed the fundamental elements necessary to protect and enhance health. However, there is growing recognition of the need to leverage the essential health-advancing opportunities presented by the ways in which communities are built and designed; how people live, work, are educated, and play; the social relationships among individuals and the resiliency that results (Aldrich, 2012); and how health and medical care services are organized and financed—all of which, taken together, ultimately determine the health of a community. Several definitions of a healthy community have been advanced, but for the purposes of this report, the committee adopted the following definition proposed by the National Network of Public Health Institutes:
A healthy community is one in which a diverse group of stakeholders collaborate to use their expertise and local knowledge to create a community that is socially and physically conducive to health. Community members are empowered and civically engaged, assuring that all local policies consider health. The community has the capacity to identify, address, and evaluate their own health concerns on an ongoing basis, using data to guide and benchmark efforts. As a result, a healthy community is safe, economically secure, and environmentally sound, as all residents have equal access to high quality educational and employment opportunities, transportation and housing options, prevention and healthcare services, and healthy food and physical activity opportunities. (HRIA, 2013, p. 24)
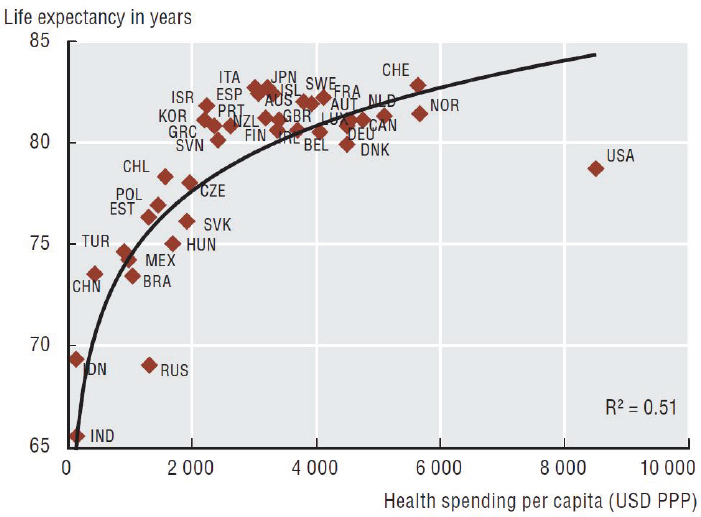
FIGURE 1-2 Average life expectancy as a function of spending on health care.
SOURCE: OECD (2013), Health at a Glance 2013: OECD Indicators, OECD Publishing. http://dx.doi.org/10.1787/health_glance-2013-en.
This definition conveys the concept that a healthy community is one in which the broad array of factors that impact community well-being are addressed, including social, environmental, political, economic, cultural, and health (physical, emotional, and developmental) components. One cannot expect communities to become healthier without understanding the complex interplay among these factors and designing comprehensive strategies to address this complexity. Furthermore, the above definition stresses the importance of a focus on individuals, recognizing that individual and community characteristics reinforce one another. It is the central thesis of this report that optimizing the health of the nation and its communities will require, in large measure, greater attentiveness to the full range of elements that encompass community design and social life and their essential interactions. The process of preparing for disasters and the comprehensive array of immediate and long-term recovery activities represent a continuum of opportunities that, if leveraged thoughtfully, can advance the long-term goal of creating healthy communities.
SOURCE: Reproduced from BMJ Quality and Safety, Bradley, E. H., B. R. Elkins, J. Herrin, and B. Elbel, 20, p. 828, 2011 with permission from BMJ Publishing Group Ltd.
This report was commissioned by the Office of the Assistant Secretary for Preparedness and Response (ASPR) within the U.S. Department of Health and Human Services (HHS), the Office of Lead Hazard Control and Healthy Homes within the U.S. Department of Housing and Urban Development (HUD), the Veterans Health Administration within the U.S. Department of Veterans Affairs, and the Robert Wood Johnson Foundation. Initiation of this study was spurred by concerns that too often, absent from discussions on recovery is the critical importance of health—including the roles of the health (public health, medical, and social services) and nonhealth sectors in ensuring that health considerations are incorporated into recovery decision making and activities. In the field of disaster and emergency management, the United States has made substantial progress in the preparedness and response arena, but the prevailing approach to recovery remains ad hoc and fragmented (Fossett, 2013). Additionally, guidance on recovery frequently focuses on the restoration of previously extant physical or economic systems within a community; little information is available to aid communities in developing post-disaster recovery approaches that address the physical, social, and economic dimensions of community life with the deliberate intent of improving health and promoting overall well-being.
Communities that have been through a disaster represent a cohort of “learning laboratories.” The
An ad hoc committee will conduct a study and issue a report on how to improve the short-, intermediate-, and long-term health outcomes and public health impact for individuals in a community of place (as contrasted with communities of faith, identity, etc.). The committee will investigate and identify key activities that impact health and public health outcomes in a community of place recovering from a disaster, and develop recommendations for their implementation. In doing so, the committee will consider the determinants of health and how various activities could leverage those determinants to improve health in the post-disaster setting, including the needs of at-risk populations.
The committee will do this by identifying (based in part on a literature review of domestic and international disasters) and recommending a series of recovery practices and novel programs most likely to impact overall community public health and contribute to resiliency for future incidents in the short-, intermediate-, and long-term period during disaster response and following incident stabilization. Specifically the committee will:
- Examine existing guidance and frameworks, peer-reviewed literature, and case studies from post-disaster response and recovery operations;
- – Characterize and identify key determinants of pre- and post-disaster public health, medical, and social services that may serve as indicators for the affected population’s long-term recovery, from various perspectives amongst the different levels of government and nongovernment actors generally located within a community of place;
- – Ascertain which other sectors are responsible for, or have the organizational interest and capacity for, directly affecting the identified determinants, and identify opportunities for collaborative engagement or support amongst those sectors;
- Identify practical guidance for recovery practices and programs for each sector that will benefit community post-disaster health and public health outcomes in the short-, intermediate-, and long-term.
- – Consider how community needs may be integrated into health recovery efforts.
- – Consider any key determinants, differences, and similarities in recovery between rural and urban communities; among household-income strata; among single-family, low-rise multifamily, and high-rise multifamily housing, among households receiving government assistance and unassisted households, etc.
- – Consider how long-term gains for health may be achieved through investments in community, housing, and other non-traditional health infrastructures.
- Identify areas of research that should be explored to answer key questions about where to direct resources before, during, and after an event occurs.
collective body of knowledge stemming from those experiences represents an invaluable resource for recovering communities and the local officials who must make difficult decisions in the face of uncertainty, armed only with the best information available. There is an ethical and moral obligation for lessons learned from past disasters to be made available to guide those decisions and for leaders at all levels to act on them (CommonHealth ACTION, 2007). Recognizing the need for better dissemination of the knowledge and evidence from past disaster recovery experiences both in the United States and abroad to enable communities to build capacity and to support more informed decision making, the sponsors of this study requested that the Institute of Medicine (IOM) convene a committee to develop guidance and recommendations on how local and national leaders can mitigate disaster-related health impacts and
optimize the use of resources—which inevitably must be spent in rebuilding—to pursue more proactively, deliberately, and thoughtfully the goal of creating communities that are healthier and more resilient. The full charge to the committee is presented in Box 1-3.
APPROACH TO ADDRESSING THE CHARGE
Disasters are variable: they come in many forms, from many causes, with different magnitudes of severity, and they trigger different levels of response and recovery effort. They also are context-specific—an event may rise to the level of disaster in one community but not another. Desiring this report to be of maximum utility to decision makers at all levels, the committee decided not to use a set of specific scenarios as the basis of its approach but chose to look at disasters more generally as events causing a community’s status to deteriorate at a level that exceeds its capacity to remedy without outside assistance (see Box 1-4 for the complete definition of a disaster adopted by the committee). Given this broad definition, the committee recognizes that no one set of guidance and recommendations could apply to every disaster scenario. For example, guidance related to behavioral health may be applicable following a pandemic, but guidance on healthy approaches to reconstruction of physical infrastructure may not. The committee’s objective was to provide a set of recommendations for key stakeholders that could be tailored for relevance to local realities and the scale of an incident and would be of practical use during pre-disaster planning and postdisaster recovery to facilitate the building of healthier communities. Local adaptation, innovation, and initiative will be key to success.
For the purposes of this report, the committee adopted the following definition from the United Nations International Strategy for Disaster Reduction:
Disaster: A serious disruption of the functioning of a community or a society involving widespread human, material, economic or environmental losses and impacts, which exceeds the ability of the affected community or society to cope using its own resources.
Comment: Disasters are often described as a result of the combination of: the exposure to a hazard; the conditions of vulnerability that are present; and insufficient capacity or measures to reduce or cope with the potential negative consequences. Disaster impacts may include loss of life, injury, disease and other negative effects on human physical, mental and social well-being, together with damage to property, destruction of assets, loss of services, social and economic disruption and environmental degradation. (UNISDR, 2009)
It should be noted that a hazardous event that results in a disaster declaration also can be declared separately as a public health emergency “when its health consequences have the potential to overwhelm routine community capabilities to address them” (Nelson et al., 2007, p. S9). Such hazardous events might include an infectious disease outbreak; natural disaster; or chemical, biological, or nuclear event (HHS, 2015b). Public health emergency declarations are made by the Secretary of Health and Human Services and enable the Secretary to take measures to respond to the emergency and support states and local communities.
Consistent with the committee’s charge, the language of this report focuses largely on health; socioeconomic components often are discussed as mechanisms for improving health outcomes. However, the committee recognizes that in a healthy community, broader community well-being is the real objective. In a sense, the nation cannot seek health improvements after a disaster without addressing the other aspects of well-being for its people. This report provides a new perspective on the special relationships between healthy communities and recovery from disasters. The study also is about knowledge transfer, blending fields of professionalism and expertise that have not been united before. Given the breadth of scope and the complexity of the subject matter, the committee expects that this initial product will prompt further work, providing the opportunity for deeper analysis and greater elucidation of the influences and relationships that can advance the nation’s sophistication in dealing with disaster recovery, one critical aspect of which is health. This is more than a call for further research, however; it is a recognition that synergies of many sorts are probable when a community’s socioeconomic systems undergo adjustment after a disaster, aided by the infusion of new resources and potentially by surge staffing and outside expertise. Going forward from this initial inquiry oriented to the role of health in post-disaster recovery, it will be time to take advantage of research, knowledge, and best practices focused on achieving more holistic community well-being, thereby linking the full range of socioeconomic endeavors for a more inclusive scope of postdisaster recovery.
The audiences for the committee’s guidance and recommendations and the report as a whole include
- state, local, tribal, and territorial6 elected and public officials who typically hold leadership roles in emergency management and strategic planning (i.e., governors, mayors, city managers and council members, emergency managers, disaster recovery coordinators);
- state, local, tribal, and territorial public health officials;
- infrastructure support professionals, such as those responsible for urban and regional planning, housing, transportation, and public works;
- federal agency stakeholders;
- health care delivery professionals and organizational leaders;
- social services professionals;
- community support (including faith-based) organizations and nongovernmental organizations;
- schools and education sector leaders;
- private-sector stakeholders; and
- empowered community members.
The committee’s approach was four-pronged. First, we developed a shared vision of a healthy community and defined the elements necessary to realize it. Next, we identified the various ways in which disasters impact health in the short-, intermediate-, and long-term periods following an event. We then examined the opportunities and resources existing uniquely in a post-disaster environment that are relevant to the elements necessary to achieving a healthy community. Finally, we explored the processes and mechanisms that determine how the relevant resources are deployed. Specifically, we examined
- the availability of post-disaster resources,
________________
6 Throughout this report, the phrase “state and local” is used for the purposes of brevity but should be inferred to include tribal and territorial leaders.
- the processes by which resources are mobilized to meet the immediate and long-term demands of a disaster,
- the elements that affect prioritization for the use of resources, and
- the broad range of expertise that must come together.
In this regard, we examined in some detail the availability and flow of financial assistance resources that are mobilized from federal, state, local, private, and philanthropic sources. To support these efforts, we commissioned a paper describing the sources of recovery funding and the pathways for disseminating those resources to localities (see Appendix B). We reviewed the appropriate federal statutes and executive agency authorizing documents and developed case studies from recent experiences with disaster recovery, both domestically and abroad; these case studies are presented throughout the report. Additional information was gathered from a review of the peer-reviewed and grey literature, as well as interviews with key stakeholders from federal, state, and local agencies; elected officials with firsthand experience in disaster recovery; human services organizations; and academic researchers (agendas from the seven public meetings held for this study are available in Appendix G).
A notable challenge for the committee was the paucity of published research and findings connecting recovery practices and approaches with health or social well-being outcomes. Further, as a result of the length of the recovery period and the inevitable delays associated with research and publication, the scientific literature that is available generally pertains to events that occurred nearly a decade ago (Hurricane Katrina) or more. Lessons learned from Hurricane Katrina and legislation subsequent to that disaster (the Post-Katrina Emergency Management Reform Act7) substantially altered the nation’s approach to all aspects of emergency management, including recovery. However, research on more recent disasters is still under way, and available information is primarily anecdotal in nature. Collecting this kind of information in a systematic way requires extensive interviewing, which the committee did not have sufficient time or resources to conduct. Instead, we relied on invited testimony from decision makers representing multiple sectors (e.g., emergency management, public health, city management) whose communities had recently been struck by a disaster.
The following guiding principles informed the committee’s guidance for recovery and its recommendations:
- Because most communities do not enjoy optimal health prior to a disaster, a crisis presents important opportunities to rebuild to a more optimal state of health post-recovery that should not be squandered.
- The guidance and recommendations of this committee should build on successful planning infrastructures and collaborative frameworks to promote an integrated recovery approach, rather than reinventing wheels.
- They should enhance flexibility and innovation at the local level and facilitate local community buy-in.
- They should focus on people, optimizing the opportunities for each person to achieve maximum health.
- They should encourage and facilitate collaboration across administrative, bureaucratic, political, and professional discipline boundaries because the actions of each of these sectors will impact health, either positively or negatively.
- They should recognize the value of nonmonetary resources such as social and cultural capital, community resiliency, leadership, community dynamics, and volunteerism.
________________
7 Post-Katrina Emergency Management Reform Act of 2006, 109th Cong., S.3721 (October 4, 2006).
- They should emphasize the importance of pre-disaster planning and capacity building.
- They should recognize that pre-disaster planning and post-disaster recovery are part of an ongoing cyclical process of community improvement involving assessment, planning, and implementation.
DISASTER RECOVERY IN THE CONTEXT OF COMPREHENSIVE RISK MANAGEMENT
Disaster recovery is “the phase of the emergency management cycle that begins with stabilization of the incident and ends when the community has recovered from the disaster’s impacts” (i.e., achieves a new normal) (Lindell et al., 2006, p. 313). The Federal Emergency Management Agency (FEMA) defines recovery as “those capabilities necessary to assist communities affected by an incident to recover effectively, including, but not limited to, rebuilding infrastructure systems; providing adequate interim and long-term housing for survivors; restoring health, social, and community services; promoting economic development; and restoring natural and cultural resources” (FEMA, 2011, p. 81). The recovery process often is broken down into a series of phases that are not discrete, but represent a continuum of activities (see Figure 1-4). Although this taxonomy is useful for the purposes of discussion, it must be recognized that there will be considerable overlap between phases and that different communities will move through phases at different paces depending on the nature of the disaster-related damage and the capacity within the community. The phases are as follows:
- Pre-disaster preparedness—The phase of the disaster management cycle prior to a disaster focused on mitigation, response and recovery planning, and capacity and resilience building (not part of the recovery process itself, but ongoing).
- Short-term recovery—The phase of recovery that entails addressing health and safety needs beyond rescue; assessing the scope of damages and needs; restoring basic infrastructure; and mobilizing recovery organizations and resources, including restarting and/or restoring essential services. The short-term recovery phase should begin immediately after a disaster, running parallel to response activities.
- Intermediate recovery—The phase of recovery that involves returning individuals, families, critical infrastructure, and essential government or commercial services to a functional, if not pre-disaster, state.
- Long-term recovery—The phase of recovery that includes complete redevelopment and revitalization of the impacted area; rebuilding or relocation of damaged or destroyed social, economic, natural, and built environments; and the transition to self-sufficiency, sustainability, and resilience. Long-term recovery may continue for months or years after the event.
A crucial element of Figure 1-4 is the explicit inclusion of the pre-disaster planning phase, which includes planning for recovery. In the United States, pre-event preparedness has been focused heavily on preparation for the response phase (Leonard and Howitt, 2010). A more comprehensive approach to managing disaster risks requires that the United States expand its focus beyond crisis management to consider the longer-term aspects of recovery, as well as prevention and mitigation efforts that should be undertaken well in advance of any disaster (Leonard and Howitt, 2010). Within a comprehensive risk management framework, there are three stages during which actions can be taken to preserve—and ideally, to improve—social welfare (inclusive of health) following a disaster:
- Prior to a disaster, prevention and mitigation efforts are aimed at eliminating or reducing the probability that a hazardous event will occur or reducing the harm caused should a disaster take place. In addition, interventions undertaken in advance of an event such as pre-event response planning and building of recovery infrastructure limit damage from disasters that do occur and accelerate the recovery process.
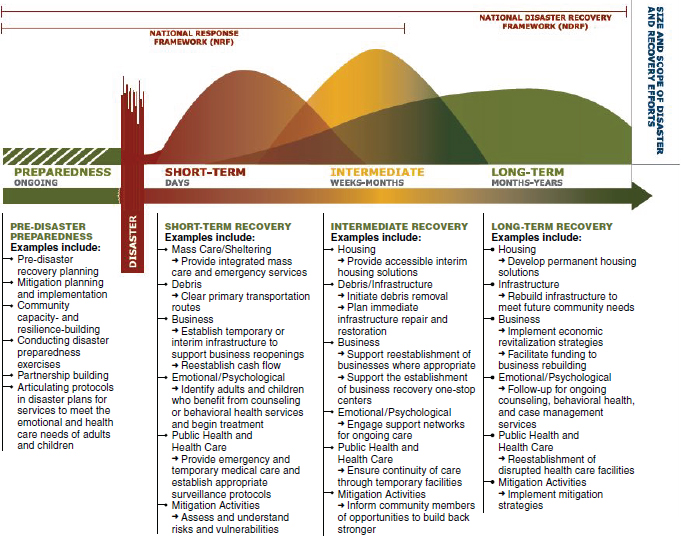
FIGURE 1-4 The recovery continuum: Description of activities by phase.
SOURCE: FEMA, 2011.
- During and immediately after a disaster, crisis management is aimed at limiting damage.
- After a disaster, recovery efforts are aimed at restoring social welfare quickly, and if undertaken thoughtfully, at improving it beyond pre-disaster levels (Leonard and Howitt, 2010).
As is the case for emergency response, disaster recovery is facilitated if communities anticipate the most significant recovery demands and plan for them in advance (Rubin, 1991; Rubin et al., 1985). The committee recognizes that the extent to which a community should undertake disaster recovery planning needs to be based on a comprehensive analysis of risks. Minimally, however, communities should ensure that a vision is in place and organizational arrangements have been laid out that will enable a coordinated approach to recovery planning. Pre-event recovery planning allows communities to think carefully about the obstacles that will be encountered during recovery, when there will be great pressure to act quickly, and, importantly, to identify opportunities to approach redevelopment in ways that enhance the health, resilience, and sustainability of the community. Pre-event recovery planning should be used to
BOX 1-5
Emergency Managers as Risk Management Practitioners
The following, extracted from the report Principles of Emergency Management, identifies some of the principles of emergency management that relate to the role of emergency managers as practitioners of risk management:
Emergency managers generally employ risk management principles such as hazard identification and risk analysis to identify priorities, allocate resources and use resources effectively.... Setting policy and programmatic priorities is therefore based upon measured levels of risk to lives, property, and the environment. The National Fire Protection Association (NFPA) 1600 states that emergency management programs should identify and monitor hazards, the likelihood of their occurrence, and the vulnerability to those hazards of people, property, the environment, and the emergency program itself. The Emergency Management Accreditation Program (EMAP) Standard echoes this requirement for public sector emergency management programs.... Emergency managers are seldom in a position to direct the activities of the many agencies and organizations involved in emergency management. In most cases, the people in charge of these organizations are senior to the emergency manager, have direct line authority from the senior official, or are autonomous. Each stakeholder brings to the planning process their own authorities, legal mandates, culture and operating missions. The principle of coordination requires that the emergency manager, or other actors responsible for risk management and increasing resilience, gain agreement among these disparate agencies as to a common purpose, and then ensure that their independent activities help to achieve this common purpose.
SOURCE: Excerpted from NRC, 2012, p. 31.
- build relationships among stakeholders and plan and exercise administrative structures for decision making so that coordination and collaboration both horizontally (across sectors) and vertically (across levels of government) are enhanced during recovery (discussed further in Chapter 3);
- develop strategies and identify needed resources for addressing critical issues likely to arise early in the recovery phase that can impede the progress of recovery and impact health/quality of life for survivors (e.g., get children back into schools and daycare, address mental health needs);
- identify opportunities to build resilience, mitigate hazards, address unmet needs, promote health during long-term recovery, and deal with expected barriers to seizing these opportunities (e.g., controversial issues such as private property rights); and
- identify and adopt a shared vision developed as part of ongoing community strategic planning.
Finally, although disaster management is a primary function of emergency managers, a comprehensive approach to managing disaster risks will require the engagement of the whole community (see Box 1-5).
THE CURRENT POLICY CONTEXT FOR HEALTH-FOCUSED RECOVERY: WHY NOW?
This report was developed in the context of the convergence of two shifting policy landscapes: (1) a disaster policy environment that increasingly reflects a growing emphasis on incorporating health considerations into resilience building and recovery efforts, and (2) a shift in the U.S. approach to population health to support greater emphasis on prevention. It is the committee’s belief that this convergence, while still evolving, is bringing unprecedented attention to the interconnectedness of health, resilience, and sustainability, thereby creating a social and policy context that will support the call for a healthy community
approach to disaster recovery that is the central theme of this report. Brief descriptions of key domestic and international policies in these two areas are provided below.
The Changing Disaster Policy Landscape
The increasing focus on the health implications of disasters, in terms of both challenges and opportunities, can be seen in a number of domestic and international disaster-related policies, including the National Health Security Strategy; domestic preparedness and disaster recovery policy, including the National Preparedness System and the recent National Disaster Recovery Framework; international disaster risk reduction policy; and climate change policy. Each of these is described briefly below; a more comprehensive description of recovery-related legislation and policies can be found in Appendix A.
The National Health Security Strategy
The Pandemic and All-Hazards Preparedness Act8 of 2006 called for the development of a National Health Security Strategy (NHSS),9 the first version of which was released by ASPR in December 2009. The second version, released in 2015, presents a vision for the nation’s health security to guide action over the next 4 years (HHS, 2015a).10 The new NHSS defines and will support five strategic objectives:
- Build and sustain healthy, resilient communities.
- Enhance the national capability to produce and effectively use both medical countermeasures and non-pharmaceutical interventions.
- Ensure comprehensive health situational awareness to support decision making before incidents and during response and recovery operations.
- Enhance the integration and effectiveness of the public health, health care, and emergency management systems.
- Strengthen global health security (HHS, 2015a).
Unlike the original NHSS, which identified health recovery as an independent objective, the new version integrates recovery into each of the above strategic objectives. Of particular interest to this committee is the increased focus on building community health resilience—“the ability of a community to use its assets to strengthen public health and healthcare systems and to improve the community’s physical, behavioral, and social health to withstand, adapt to, and recover from adversity” (HHS, 2015a, p. 10)—and acknowledgment of the multisector nature of this important endeavor. Key priorities for community health resilience include (1) encouraging social connectedness; (2) enhancing coordination of health and human services; and (3) building a culture of resilience through physical, behavioral, and social health, as well as leveraging health and community systems and increasing access to information and training to empower individuals to assist their communities after incidents (HHS, 2015a). The committee notes that these are all themes that run throughout this report.
Domestic Preparedness and Disaster Recovery Policy
Domestic disaster policy is framed by the architecture of the National Preparedness System, which outlines the process by which the whole community works toward achieving the National Preparedness Goal—“a secure and resilient nation with the capabilities required across the whole community to prevent,
________________
8 Pandemic and All-Hazards Preparedness Act, Public Law 109-417, 109th Cong., S.3678 (December 19, 2006).
9 As defined by the NHSS, national health security is “a state in which the Nation and its people are prepared for, protected from, and resilient in the face of health threats or incidents with potentially negative health consequences” (HHS, 2009b, p. 3).
10 HHS is required to submit an updated version of the NHSS every 4 years.
protect against, mitigate, respond to, and recover from the threats and hazards that pose the greatest risk” (FEMA, 2014, p. 1). The National Planning Frameworks,11 which are part of the National Preparedness System, establish the strategy and doctrine for building, sustaining, and delivering the core capabilities identified in the National Preparedness Goal. They describe the roles, responsibilities, and coordinating structures for the whole community—individuals, nongovernmental entities, the private sector, and governments at all levels. Of particular relevance to this report is the National Disaster Recovery Framework (NDRF), released in 2011, which serves as a guide to facilitate recovery at the community level (FEMA, 2011). Health and social services are featured prominently in the NDRF as one of six recovery support functions12 with a mission of helping locally led recovery efforts restore and improve public health, health care, and social services networks, thereby promoting community resilience, health, independence, and well-being. The NDRF is discussed in more detail in Chapter 3.
The growing national focus on disaster recovery has been accompanied by increasing integration of sustainability and resilience agendas into recovery efforts, with significant implications for health. A 2010 memorandum of agreement between FEMA and the U.S. Environmental Protection Agency’s Office of Sustainability was developed to identify and leverage opportunities to incorporate sustainability and smart growth principles into long-term disaster recovery and hazard mitigation activities (DHS and EPA, 2010). Additionally, HUD has become a major player in disaster recovery as its Community Development Block Grant (CDBG) program has increasingly been used as a vehicle for funding post-disaster redevelopment, either through reprogramming of previously awarded funds or through supplemental appropriations from Congress. The CDBG program, with its focus on helping low- and moderate-income individuals, has historically addressed affordable housing, community development, and employment opportunities, all of which are social factors that influence health (HUD, 2014b). As discussed in more depth later in this report, requirements and guidance associated with recent supplemental appropriations for disaster recovery (i.e., CDBG-Disaster Recovery [DR] funds for Hurricane Sandy recovery) are being used to promote broader goals of community resilience and sustainability. Further, in 2014, President Obama announced the National Disaster Resilience Competition, which offers communities that have recently experienced a natural disaster the opportunity to compete for funds that would enable them to rebuild in ways that would increase resilience to future disasters (White House Office of the Press Secretary, 2014). Although the funds for this competition came from a one-time supplemental appropriation, it is spurring a national conversation about resilience and sustainability that may lead to further investment and legislation supporting resilience and sustainability at all levels, ultimately yielding benefits for health as well.
International Disaster Risk Reduction Policy
Internationally, greater emphasis on incorporating health considerations into resilience building and recovery is evident in recent efforts surrounding the second Hyogo Framework for Action (HFA-2), titled “Building the Resilience of Nations and Communities to Disasters” (Burkle et al., 2014). The first Hyogo Framework for Action (HFA-1) came about in 2005 at the request of the United Nations General Assembly and served as a 10-year international disaster risk reduction plan (UNISDR, 2015a). Disaster risk reduction refers to the “concept and practice of reducing disaster risks through systematic efforts to analyse and reduce the causal factors of disasters,” such as by minimizing hazard exposure, reducing the vulnerability of people and property, and improving preparedness (UNISDR, 2015b). Investment in disaster risk reduction stems from the recognition that a disaster is a consequence of the choices societies make for their populations and environments (e.g., how they grow food, where and how they build homes, what
________________
11 There are five National Planning Frameworks—one for each of the core mission areas under the National Preparedness System, which are Prevention, Protection, Mitigation, Response, and Recovery (FEMA, 2014).
12 The six recovery support functions are (1) Community Planning and Capacity Building, (2) Economic, (3) Health and Social Services, (4) Housing, (5) Infrastructure Systems, and (6) Natural and Cultural Resources (FEMA, 2011).
kind of government they have, how their financial system works). Every decision and action can make communities more vulnerable to—or more resilient to—disasters.
The United Nations International Strategy for Disaster Reduction (UNISDR) led the implementation of HFA-1, which emphasized ensuring the priority of disaster risk reduction, enhancing early warning, working to build a culture of safety and resilience at all levels, reducing underlying risk factors, and strengthening disaster preparedness for effective response (UNISDR, 2005). The original HFA, however, failed to identify health as a priority in disaster risk reduction and management. Since 2005, there has been widespread recognition of and emphasis on the need to make community health, resilience, and well-being, beyond just saving lives, an explicit focus. UNISDR recently reviewed HFA-1 and consulted on the development of HFA-2, a post-2015 framework for disaster risk reduction. At the Third World Conference on Disaster Risk Reduction, which took place in March 2015 in Sendai, Japan, conference representatives from U.S. and international organizations developed a post-2015 framework (Burkle et al., 2014; UNISDR, 2015a). The Sendai Framework for Disaster Risk Reduction 2015-2030 outlines the following goal: to “prevent new and reduce existing disaster risk through the implementation of integrated and inclusive economic, structural, legal, social, health, cultural, educational, environmental, technological, political and institutional measures that prevent and reduce hazard exposure and vulnerability to disaster, increase preparedness for response and recovery, and thus strengthen resilience” (WCDRR, 2015, p. 7). Such efforts are part of a growing recognition that disaster response is costly, whereas mitigation and preparedness initiatives, particularly those that address community health and resilience, save money and lives in the long run (Burkle et al., 2014).
The core mission areas of the U.S. National Preparedness System—prevention, protection, mitigation, response, and recovery—are consistent with a comprehensive approach to disaster risk reduction. Nonetheless, alignment of terminology and greater emphasis on addressing social determinants of health and reducing poverty as key strategies for reducing disaster risk could better harmonize U.S. policy with international efforts.
Climate Change Policy
The growing emphasis in the United States and internationally on increasing resilience is particularly important in the context of the emerging threat of climate change and scientists’ predictions on how it may contribute to future disasters. Climate change is expected to lead to higher global temperatures, the secondary effects of which include increased sea levels, reduced snow cover, and changes in rainfall patterns (van Aalst, 2006). Experts project that the global warming observed in the last century will accelerate in the coming decades, likely increasing the frequency and severity of future natural disasters (Schipper and Pelling, 2006). Key determinants of health—water, air, food—are affected by changes in climate. The Fifth Assessment Report of the Intergovernmental Panel on Climate Change states with very high confidence that the health of human populations is sensitive to shifts in weather patterns and other aspects of climate change. This sensitivity is expected to manifest as exacerbations of existing health problems, disproportionately impacting vulnerable populations, such as the poor (O’Brien et al., 2006). With regard to health, the most effective measures for reducing vulnerability in the near term are programs that implement and improve such basic public health functions as providing clean water, sanitation, and essential health care; alleviating poverty; and increasing disaster preparedness capacity (Smith et al., 2014).
Both in the United States and internationally, it is recognized that disaster recovery planning should integrate the projected impacts of climate change with respect to future disasters. The United States has begun to take steps in this direction through President Obama’s Climate Action Plan, released in June 2013. This plan not only commits to reducing U.S. carbon pollution and leading international efforts to combat global climate change but also outlines the importance of preparing the nation for the impacts of climate change by reducing vulnerabilities. Areas of focus within this key pillar include directing agencies to support local climate-resilient investments, working to create resilient and sustainable health care institutions, building on the new flood risk reduction standard for the region affected by Hurricane Sandy, and
piloting strategies in that region to strengthen those communities against future extreme weather (White House Office of the Press Secretary, 2013).
The Changing Health Policy Landscape
This is a time of major change in the organization and financing of health care services, with increased focus on patient-centered medical homes, accountable care organizations, and outcome-based payment methodologies being driven by public- and private-sector initiatives to improve quality while decreasing costs. The Patient Protection and Affordable Care Act13 (ACA) demonstrates clear support from the nation’s top leadership for an approach to health that favors prevention (e.g., health promotion, access to primary care). This changing health policy landscape is an important factor in the opportunities communities have to achieve optimal health through recovery planning and execution. For example, the ACA includes provisions requiring nonprofit hospitals in the United States to conduct a community health needs assessment and adopt an implementation strategy for meeting identified community health needs. This information represents a valuable resource to inform recovery planning.
There is also increasing recognition that health is not just the responsibility of those working in the health sector (public health, medical system). Other examples of a shifting paradigm in population health are the adoption of a health-in-all-policies approach—“a collaborative approach to improving the health of all people by incorporating health considerations into decision-making across sectors and policy areas”—and the increasing use of health impact assessments to inform policy development (Rudolph et al., 2013, p. 5; WHO, 2014).
Despite the advances described above, there is a clear disconnect between the increasing understanding of how the health of communities can be improved through changes in policies, services, and environments and the approaches taken to community redevelopment after a disaster. It is the committee’s premise that the growing prevention-based and all-sectors approach to health needs to be incorporated into disaster planning and recovery efforts.
HOW THIS REPORT IS INTENDED TO BE USED
As detailed earlier, this report is directed at several key audiences. These audiences fall essentially into two groups: those individuals and organizations involved in planning for and carrying out disaster recovery activities (see Figure 1-5) and those involved in planning for and building healthy communities. Through this report, the committee hopes to bring these two stakeholder groups together so that a health lens is applied to disaster recovery planning and the menu of tools and resources for health improvement planners is expanded to include those associated with disaster planning and recovery activities. The committee emphasizes that it does not consider health to be more important than other recovery support functions; in fact, it considers each area as critical to the building of healthy communities. The committee merely asserts that impacts on health outcomes should be one of the many priorities factored into decision making on recovery strategies and allocation of resources.
A particular focus of this report is key leadership involved in disaster recovery activities as they control the processes and resources that are mobilized in the pre- and post-disaster planning process. These leaders include elected officials such as governors, mayors, county and city managers, emergency managers, and disaster recovery coordinators. Following a disaster, pressure for urgent action is intense, and the decisions that must be made are inherently complex. Without prior sensitization, therefore, the longer-term health agenda can too easily be ignored, resulting in missed opportunities. Worse, inadequate attention to critical health protection functions can exacerbate long-standing health challenges or create new ones.
This report also is focused on sensitizing and educating leaders engaged in building healthier communities, who, the committee observed, generally are unaware of the opportunities and mechanisms associated
________________
13 The Patient Protection and Affordable Care Act, Public Law 111-148, 111th Cong., H.R.3590 (March 23, 2010).
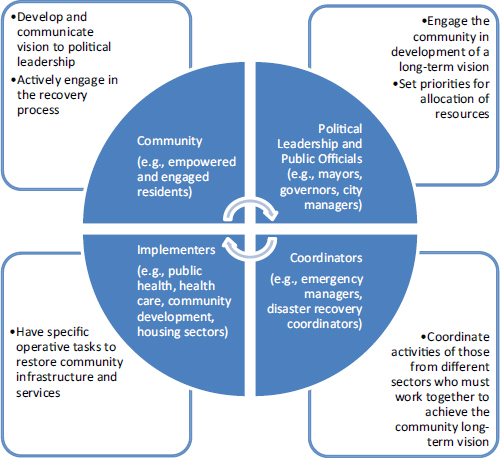
FIGURE 1-5 Key stakeholders in the disaster recovery process.
with disaster recovery. Disasters can catalyze bold changes that would not otherwise have been possible or that would have progressed at a much slower pace. Although there is a growing awareness that the way communities and service delivery systems have been designed has resulted in suboptimal health outcomes, healthy community initiatives often are impeded by a scarcity of resources. By bringing awareness of the opportunities presented during the recovery planning process to advance the goals of those working across multiple sectors to promote community well-being, the committee hopes to elicit their increased engagement in that process—both before and after a disaster.
To facilitate maximum utility for the wide array of audiences from various sectors, the report is organized in a modular format so that key operational guidance and recommendations, as well as their supporting background and evidence, are easily accessible. Part I of the report, which includes Chapters 1 through 4, establishes the framework for a healthy community approach to disaster recovery. These chapters define the concept of healthy communities and detail the comprehensive components that are pertinent to their realization. They also describe the financial and other resources that support disaster recovery and the allocation process by which those resources are mobilized. Some of the information presented in this first part of the report will be rudimentary to audiences who are well experienced in the complexities of recovery planning, financing, and governance. However, a key goal of this work is to present this information in a manner that is comprehensible to stakeholders who are not familiar with disaster management but whose engagement is critical to achieving healthy communities. Furthermore,
the committee does not intend for this report to serve as a comprehensive guide to the recovery process and available recovery-related resources. In keeping with its charge, the committee focuses its description on those aspects of the recovery process relevant to the protection and promotion of the health of the affected community.14
The committee’s operational-level guidance for individual sectors is presented in Part II. Chapters 5 through 8 provide guidance and supporting background regarding the opportunities to enhance human recovery through health and social services, including medical, behavioral and public health, and social support services. Chapters 9 and 10 provide guidance and supporting background regarding the opportunities to use place-based strategies15 (i.e., coordinated interventions targeted to specific geographic areas) to rebuild the physical, social, and economic environments in a health-enhancing manner.
The final part of the report contains appendixes that include a detailed description of the federal policy environment influencing disaster recovery (Appendix A), a commissioned paper on financial assistance for recovery (Appendix B), a listing of additional resources (Appendix C), a description of measures and tools for evaluating healthy communities (Appendix D), a summary of the research needs identified throughout the chapters of this report (Appendix E), a key to select terms used to describe primary actors and key partners in Chapters 5 through 10 checklists (Appendix F), meeting agendas (Appendix G), and biographical sketches of the committee members (Appendix H).
Although this report was designed in a modular format with a number of sector-specific chapters, the committee emphasizes its intent that the report not contribute to the all too common problem of siloed engagement. As is noted throughout this report, all sectors have a role in creating communities that maximize the opportunities for their residents to live healthy and fulfilled lives. Accordingly, the reader will observe from time to time across different chapters a redundancy intended to advance an integrated perspective. Further, the committee strongly urges readers to consult not only the chapters specifically related to their own sector or field of practice but also those related to others. Reading the report in this way should provide a more holistic picture of the health-related impacts and opportunities associated with disasters and reveal complementary efforts, shared challenges, and abundant opportunities for synergy. With a strong belief that there is an ethical imperative to use every available opportunity to engage all available resources in the fight for health, the committee concludes that all stakeholders involved in the pre-disaster and immediate- and long-term post-disaster strategic planning process need to be engaged, empowered, and supported in maximizing the opportunities to transform an unfortunate crisis into long-term benefit in the form of healthier communities and individuals. What follows in the subsequent chapters is the committee’s vision and recommendations for how this goal can be achieved.
Aldrich, D. P. 2012. Building resilience: Social capital in post-disaster recovery. Chicago, IL: University of Chicago Press.
ASTHO (Association of State and Territorial Health Officials). 2012. Pandemic and All-Hazards Preparedness Act fact sheet. http://astho.org/Programs/Preparedness/Public-Health-Emergency-Law/Emergency-Authority-andImmunity-Toolkit/Pandemic-and-All-Hazards-Preparedness-Act-Fact-Sheet (accessed October 10, 2014).
Bradley, E. H., and L. A. Taylor. 2013. The American health care paradox: Why spending more is getting us less. New York: Public Affairs.
________________
14 A broader selection of resources is available from FEMA’s Community Recovery Management Toolkit, “a compilation of guidance, case studies, tools, and training to assist local communities in managing long-term recovery following a disaster.” The toolkit can be accessed at http://www.fema.gov/national-disaster-recovery-framework/community-recovery-management-toolkit (accessed October 21, 2014). Additional resources are listed in Appendix C.
15 “Place-based policies leverage investments by focusing resources in targeted places and drawing on the compounding effect of well-coordinated action. Effective place-based policies can influence how rural and metropolitan areas develop, how well they function as places to live, work, operate a business, preserve heritage, and more. Such policies can also streamline otherwise redundant and disconnected programs” (The White House, 2009, p. 1).
Bradley, E. H., B. R. Elkins, J. Herrin, and B. Elbel. 2011. Health and social services expenditures: Associations with health outcomes. BMJ Quality and Safety 20(10):826-831.
Brandt, M., C. Brown, J. Burkhart, N. Burton, J. Cox-Ganser, S. Damon, H. Falk, S. Fridkin, P. Garbe, M. McGeehin, J. Morgan, E. Page, C. Rao, S. Redd, T. Sinks, D. Trout, K. Wallingford, D. Warnock, and D. Weissman. 2006. Mold prevention strategies and possible health effects in the aftermath of hurricanes and major floods. Morbidity and Mortality Weekly Report Recommendations and Reports 55(RR08):1-27.
Burkle, F. M., S. Egawa, A. G. MacIntyre, Y. Otomo, C. W. Beadlin, and J. T. Walsh. 2014. The 2015 Hyogo Framework for Action: Cautious optimism. Disaster Medicine and Public Health Preparedness 8(3):191-192.
CDC (Centers for Disease Control and Prevention). 2010. Public health workbook: To define, locate, and reach special, vulnerable, and at-risk populations in an emergency. Atlanta, GA: CDC.
CDC. 2011. Healthy communities: Preventing chronic disease by activating grassroots change at a glance 2011. http://www.cdc.gov/chronicdisease/resources/publications/aag/healthy_communities.htm (accessed October 10, 2014).
CommonHealth ACTION. 2007. Katrina and social determinants of health: Toward a comprehensive community preparedness approach. http://commonhealthaction.org/PDF/CHA_KatrinaSocialDet.pdf (accessed March 27, 2015).
CRS (Congressional Research Service). 2014. FEMA’s disaster relief fund: Overview and selected issues. Washington, DC: CRS, Library of Congress.
DHS (U.S. Department of Homeland Security), and EPA (U.S. Environmental Protection Agency). 2010. Memorandum of agreement between the Department of Homeland Security (DHS), Federal Emergency Management Agency (FEMA) and the Environmental Protection Agency (EPA). http://www.epa.gov/dced/pdf/2011_0114_fema-epamoa.pdf (accessed March 17, 2015).
DRA (Disability Rights Activists). 2013. Federal judge rules New York City’s inadequate disaster plans discriminate against hundreds of thousands of New Yorkers with disabilities. http://www.dralegal.org/pressroom/pressreleases/federal-judge-rules-new-york-citys-inadequate-disaster-plans-discriminate (accessed March 4, 2015).
FEMA (Federal Emergency Management Agency). 2010. Flood insurance dollars and sense. https://www.fema.gov/news-release/2010/09/29/flood-insurance-dollars-and-sense (accessed February 24, 2015).
FEMA. 2011. National disaster recovery framework. Washington, DC: FEMA.
FEMA. 2014. Overview of the national planning frameworks. Washington, DC: FEMA.
Fossett, J. W. 2013. Let’s stop improvising disaster recovery. http://www.rockinst.org/observations/fossettj/201307-09-Improvising_Disaster_Recovery.aspx (accessed June 5, 2014).
HHS (U.S. Department of Health and Human Services). 2009a. HHS/ASPR/ABC fact sheet on at-risk individuals. http://www.phe.gov/Preparedness/planning/abc/Documents/abc_listening_session.pdf (accessed March 4, 2015).
HHS. 2009b. National health security strategy of the United States of America. Washington, DC: HHS.
HHS. 2015a. National health security strategy and implementation plan: 2015-2018. Washington, DC: HHS.
HHS. 2015b. Public health and social services emergency fund. http://www.hhs.gov/budget/fy2015/fy2015-publichealth-social-services-emergency-budget-justification.pdf (accessed March 17, 2015).
HRIA (Health Resources in Action). 2013. Defining healthy communities. Boston, MA: Health Resources in Action. http://hria.org/uploads/catalogerfiles/defining-healthy-communities/defining_healthy_communities_1113_final_report.pdf (accessed October 21, 2014).
HUD (U.S. Department of Housing and Urban Development). 2014a. CDBG-DR active disaster grants and grantee contact information. https://www.hudexchange.info/cdbg-dr/cdbg-dr-grantee-contact-information (accessed March 31, 2015).
HUD. 2014b. Community Development Block Grant Disaster Recovery program. https://www.hudexchange.info/cdbg-dr (accessed March 23, 2015).
IOM (Institute of Medicine). 2012a. Crisis standards of care: A systems framework for catastrophic disaster response. Washington, DC: The National Academies Press.
IOM. 2012b. For the public’s health: Investing in a healthier future. Washington, DC: The National Academies Press.
KFF (The Henry J. Kaiser Family Foundation). 2012. Health care costs: A primer. http://kff.org/health-costs/issue-brief/health-care-costs-a-primer (accessed October 9, 2014).
Landesman, L. Y. 2005. Public health management of disasters: The practice guide. Washington, DC: American Public Health Association.
Leonard, H. B., and A. M. Howitt. 2010. Acting in time against disasters: A comprehensive risk-management framework. In Learning from catastrophes: Strategies for reaction and response, edited by H. Kunreather and M. Useem. Upper Saddle River, NJ: Wharton School Publishing. Pp. 18-40.
Lindell, M. K., W. C. Nicholson, C. S. Prater, and R. W. Perry. 2006. Fundamentals of Emergency Management. Washington, DC: FEMA.
Mensah, G. A., A. H. Mokdad, S. F. Posner, E. Reed, E. J. Simoes, M. M. Engelgua, and Chronic Diseases and Vulnerable Populations in Natural Disasters Working Group. 2005. When chronic conditions become acute: Prevention and control of chronic disease and adverse health outcomes during natural disasters. Preventing Chronic Disease 2(A04).
Nelson, C., N. Lurie, J. Wasserman, and S. Zakowski. 2007. Conceptualizing and defining public health emergency preparedness. American Journal of Public Health 97(Suppl. 1):S9-S11.
NRC (National Research Council). 2012. Disaster resilience: A national imperative. Washington, DC: The National Academies Press.
NRC and IOM. 2013. U.S. health in international perspective: Shorter lives, poorer health. Edited by S. H. Woolf and L. Aron. Washington, DC: The National Academies Press.
O’Brien, G., P. O’Keefe, J. Rose, and B. Wisner. 2006. Climate change and disaster management. Disasters 30(1):64-80. OECD. 2013. Health at a glance 2013: OECD indicators. http://www.oecd-ilibrary.org/docserver/download/8113161e.pdf?expires=1426695435&id=id&accname=guest&checksum=0897D47D81D49EBEA66A34DE4EBC02CF (accessed October 9, 2014).
O’Sullivan, T. L., C. E. Kuziemsky, W. Corneil, L. Lemyre, and Z. Franco. 2014. The EnRiCH Community Resilience Framework for High-Risk Populations. PLoS Currents Disasters Oct 2. Edition 1.
Peters, M. N., J. C. Moscona, M. J. Katz, K. B. Deandrade, H. C. Quevedo, S. Tiwari, A. R. Burchett, T. A. Turnage, K. Y. Singh, E. N. Fomunung, S. Srivastav, P. Delafontaine, and A. M. Irimpen. 2014. Natural disasters and myocardial infarction: The six years after hurricane Katrina. Mayo Clinic Proceedings 89(4):472-477.
Rubin, C. B. 1991. Recovery from disaster. In Emergency management: Principles and practice for local governments. Washington, DC: International City Management Association, Municipal Management Series. Pp. 224-259.
Rubin, C. B., M. D. Saperstein, and D. G. Barbee. 1985. Community recovery from a major natural disaster. Monograph No. 41. Boulder, CO: Program on Environment and Behavior, Institute of Behavioral Science, University of Colorado.
Rudolph, L., J. Caplan, K. Ben-Moshe, and L. Dillon. 2013. Health in All Policies: A guide for state and local governments. Washington, DC, and Oakland, CA: American Public Health Association and Public Health Institute. http://www.phi.org/uploads/files/Health_in_All_Policies-A_Guide_for_State_and_Local_Governments.pdf (accessed November 18, 2014).
Runkle, J. D., A. Brock-Martin, W. Karmaus, and E. R. Svendsen. 2012. Secondary surge capacity: A framework for understanding long-term access to primary care for medically vulnerable populations in disaster recovery. American Journal of Public Health 102(12):e24-e32.
RWJF (Robert Wood Johnson Foundation). 2014. Time to act: Investing in the health of our children and communities. Princeton, NJ: RWJF. http://www.rwjf.org/content/dam/farm/reports/reports/2014/rwjf409002 (accessed October 9, 2014).
Schipper, L., and M. Pelling. 2006. Disaster risk, climate change and international development: Scope for, and challenges to, integration. Disasters 30(1):19-38.
Sherry, N., and A. Harkins. 2011. Leveling the emergency preparedness playing field. Journal of Emergency Management 9(6):11-16.
Smith, K. R., A. Woodward, D. Campbell-Lendrum, D. D. Chadee, Y. Honda, Q. Liu, J. M. Olwoch, B. Revich, and R. Sauerborn. 2014. Human health: Impacts, adaptation, and co-benefits. In Climate change 2014: Impacts, adaptation, and vulnerability. Part A: Global and sectoral aspects. Contribution of working group II to the fifth assessment report of the intergovernmental panel on climate change, edited by C. B. Field, V. R. Barros, D. J. Dokken, K. J. Mach, M. D. Mastrandrea, T. E. Bilir, M. Chatterjee, K. L. Ebi, Y. O. Estrada, R. C. Genova, B. Girma, E. S. Kissel, A. N. Levy, S. MacCracken, P. R. Mastrandrea, and L. L. White. Cambridge, United Kingdom and New York: Cambridge University Press. Pp. 709-754.
TFAH (Trust for America’s Health). 2013a. A healthier America 2013: Strategies to move from sick care to health care in the next four years. Washington, DC: TFAH.
TFAH. 2013b. Our vision for a healthier America. http://healthyamericans.org/assets/files/VisionHealthierAmerica.pdf (accessed October 9, 2014).
UNISDR (United Nations International Strategy for Disaster Reduction). 2005. Summary of the Hyogo framework for action 2005-2015: Building the resilience of nations and communities to disasters (Hyogo framework). Geneva, Switzerland: UNISDR.
UNISDR. 2009. Terminology. http://www.unisdr.org/we/inform/terminology (accessed February 27, 2015).
UNISDR. 2015a. Post-2015 framework for disaster risk reduction. http://www.unisdr.org/we/coordinate/hfa-post2015 (accessed February 13, 2015).
UNISDR. 2015b. What is disaster risk reduction? http://www.unisdr.org/who-we-are/what-is-drr (accessed March 17, 2015).
van Aalst, M. K. 2006. The impacts of climate change on the risk of natural disasters. Disasters 30(1):5-18.
WCDRR (World Conference on Disaster Risk Reduction). 2015. Sendai framework for disaster risk reduction 2015-2030. http://www.wcdrr.org/uploads/Sendai_Framework_for_Disaster_Risk_Reduction_2015-2030.pdf (accessed March 23, 2015).
Weiss, D. J., and J. Weidman. 2013. Disastrous spending: Federal disaster-relief expenditures rise amid more extreme weather. Center for American Progress. https://cdn.americanprogress.org/wp-content/uploads/2013/04/WeissDisasterSpending-1.pdf (accessed March 22, 2015).
The White House. 2009. Developing effective place-based policies for the FY 2011 budget. http://www.whitehouse.gov/sites/default/files/omb/assets/memoranda_fy2009/m09-28.pdf (accessed March 4, 2015).
White House Office of the Press Secretary. 2013. Fact sheet: President Obama’s climate action plan. https://www.whitehouse.gov/the-press-office/2013/06/25/fact-sheet-president-obama-s-climate-action-plan (accessed February 27, 2015).
White House Office of the Press Secretary. 2014. Fact sheet: National disaster resilience competition. https://www.whitehouse.gov/the-press-office/2014/06/14/fact-sheet-national-disaster-resilience-competition (accessed March 17, 2015).
WHO (World Health Organization). 1948. Preamble to the constitution of the World Health Organization. Geneva, Switzerland: WHO.
WHO. 2014. Health Impact Assessment (HIA). http://www.who.int/hia/en (accessed March 25, 2014).
This page intentionally left blank.
























