
3
The Current State of Informed Consent in Research and Treatment
The workshop’s second panel included four speakers who together presented a picture of the challenges created by poor informed consent processes. Sara Goldkind, research and clinical bioethics consultant, discussed the impact of these processes on clinical trials and information sharing, and Yael Schenker, assistant professor of medicine at the University of Pittsburgh, spoke about one approach to developing a better informed consent process. Sandra Crouse Quinn, associate dean for academic affairs, professor of family science, and senior associate director of the Center for Health Equity at the University of Maryland, College Park, described strategies for improving the informed consent process to help increase minority participation in clinical trials, and Alicia Fernandez, professor of clinical medicine at the University of California, San Francisco, highlighted the disproportionately negative impact that poor informed consent processes have on the medical treatment that minorities receive. An open discussion followed the four presentations.
THE IMPACT OF A POOR INFORMED CONSENT PROCESS ON CLINICAL TRIALS1
Sara Goldkind
To start her presentation, Sara Goldkind noted that the FDA’s guidance on informed consent, of which she was one of the authors, was published in draft form recently and is available for comment. Goldkind encouraged the workshop attendees to review the draft guidance and provide feedback to the FDA. She also remarked that the draft guidance document addresses some of the issues that this workshop is tackling, particularly those issues related to literacy and numeracy and how to work with research participants who are physically impaired.
To frame the rest of her presentation, Goldkind listed the conclusions she has drawn regarding how to improve the informed consent process. Any approach, she said, must be multipronged, and it must be driven by research on informed consent that produces a sound evidence base. There also needs to be more effort to educate the public and potential research participants about the informed consent process, the benefits of participating in clinical research, and the essential role that the public plays in the research endeavor, she added. In addition, the research community needs to partner more extensively and effectively with patients and disease-based foundations and advocacy groups.
In discussing the basic components of informed consent, Goldkind said that although it is important to disclose adequate information to allow for an informed decision about participating in research and to facilitate comprehension, the crux of informed consent is not just about disclosure or understanding. A good informed consent process should also provide potential participants adequate opportunity to ask questions and consider whether to participate and should ensure that agreeing to participate is completely voluntary. She also noted that many complex learning activities go on in informed consent that impact the quality and success of the consent process. “I think we need to bear that in mind as we think about how to improve informed consent, and in fact, I think we need to have empiric research on all areas of the various components of informed consent. Clearly, we have largely focused on understanding,” said Goldkind.
Another factor that adds to the complexity of studying informed consent is that clinical research itself is diverse, Goldkind explained. Survey research, for example, is different from first-in-human research with a new investigational product. At the same time, study populations are also
_____________
1 This section is based on the presentation by Sara Goldkind, research and clinical bioethics consultant, and the statements are not endorsed or verified by the IOM.
diverse, and research is needed to understand whether that diversity affects the implementation of adequate informed consent and, if so, what those effects can be. The data derived from various components of the informed consent process are also heterogeneous in terms of the setting, the timing of data collection, and the types and quality of the methodology used to study those components. As a result, there is a question of whether findings from specific studies can be generalized to other groups. “Is someone who has gone through multiple clinical trials as part of cancer therapy different from someone who is a novice to the research setting?” asked Goldkind. “I think that we ought to not only bear in mind how complex informed consent is itself, but also how complex are the data that we are acquiring about informed consent.”
She noted that various practical concerns result when informed consent is conducted poorly. For example, failing to describe the nature of the research and the scientific reasons for it could potentially affect recruitment and retention. She noted that researchers need to conduct exit interviews to ascertain why participants withdraw from studies and determine if the informed consent process played a role in that decision and whether there was a disconnect between an individual’s experiences in the study and what was learned through the informed consent process. It would also be useful, she said, to ask people who decline to participate in research for their reasons for doing so. “It would be really interesting to know after they have gone through an informed consent process whether that changed their minds. Did they come to the clinical context thinking they were going to be part of the research? After they went through the informed consent process, did they say ‘this is not for me’ and why? I think there are ways that we can get more information about recruitment and retention.”
Another practical concern is that long and complex forms may inhibit reading and processing, and as an example she cited the terms-of-use agreements that almost everyone skips when installing new software or joining a new website. Certainly, said Goldkind, long and complex forms may increase resource burdens when drafting them and when reviewing them at the IRB level, which in turn could delay start-up times, particularly when multiple sites and multiple IRBs are all editing various aspects of the informed consent documents. She commented that although many people believe that federal regulations are largely to blame for long and complex informed consent documents, she agrees with the prior speakers that this is not the case. She said that these regulations have been in place and have changed little since the 1980s; what has changed is the way these regulations are being interpreted and implemented.
Goldkind reiterated Aldoory’s statement that consent documents do not need to disclose everything that is in the regulations and cited the fact that of the 14 basic pieces of information listed in the regulations, only 8
are required to be disclosed, with the other 6 required only when appropriate and applicable. Moreover, the regulations do state that the informed consent process has to be in language understandable to the research participants. “In the guidance that I mentioned to you, we actually describe that low literacy and low numeracy should be taken into account when you think about what ‘language understandable to the research participants’ means,” said Goldkind.
If long and complex informed consent forms cause confusion and misunderstanding among research participants, that might in turn affect data integrity, said Goldkind. For example, if participants are not following the protocol-driven procedures, outcome data can be negatively impacted, or if they are participating in a phase I safety study but think that they are in a treatment study, they may underreport adverse events.
Goldkind then discussed what she believes are some of the aspirational goals of informed consent. Informed consent should honor self-determination and be thought of as an expression of the principle of autonomy, she said. Informed consent should empower the potential participant to decide whether the risk/benefit ratio is acceptable to that individual and whether it remains acceptable through the research study. “You can think of informed consent as an expression of beneficence and non-malfeasance in that regard,” said Goldkind. Informed consent should also aspire to convey respect for potential participants as true partners and maintain an ongoing dialogue that starts before study initiation and continues after the study ends. She said that she has heard from patients that they are interested in seeing the aggregate data from a study and learning about the conclusions drawn from their study. Maintaining a dialogue after a study is complete is a way of honoring the participants’ role in the study, said Goldkind. Although not a subject for this workshop, another aspirational goal for informed consent should be to protect individuals with diminished autonomy or decreased decisional capacity, Goldkind stated.
She then discussed what she called “sublime concerns.” At the top of her list was that the failure to provide contextual meaning to a research study may degrade the participant’s autonomy and decision-making abilities. The goal, she said, citing an IOM report on health literacy and numeracy (IOM, 2014), is to enable participants to draw meaning from information to make the choices they need to make. Another sublime concern of hers is that informed consent handled poorly fails to engage participants as true partners and may lead to their sense of objectification or “commoditization” that can then promote distrust and anger.
There are several areas, said Goldkind, where further research is needed in order to improve the informed consent process. Studies have shown, for example, that research participants have a limited understanding of aspects of research after standard informed consent and that interventions
to improve understanding are not effective or are of limited or inconsistent effectiveness. One review of 42 trials of consent processes (Flory and Emanuel, 2004) found that person-to-person interactions, especially those involving extended discussion interventions, may be more consistently effective than approaches using multimedia, test/feedback, or enhanced forms at improving understanding.
Goldkind noted, too, that it is essential for the field to conduct evidence-based research on informed consent interventions. She acknowledged that quality data are challenging to obtain and that it is necessary to assess whether the results from disparate study populations can be generalized and to ensure that the tools used to measure understanding and participant satisfaction are valid and of high quality. Given the complexities of studying informed consent, Goldkind said the field ought to think about nesting informed consent studies within clinical research. “What I mean by that is if you are doing a cardiovascular study, can you build in an informed consent study as an ancillary study to that research so that you actually have real-world data on informed consent rather than simulating certain informed consent projects?” Goldkind explained.
Additional research is also needed to understand what participants want and need to know, she said. Goldkind cited research by Deborah Schrag, from the Dana-Farber Cancer Institute, showing that participants in clinical trials of palliative chemotherapy did not want the informed consent organized by drug but rather by regimen. They wanted to know how chemotherapy was going to affect them: Would they be able to drive? Would they have to be hospitalized? What would they be given to combat nausea? They also wanted to hear real patient voices as part of the informed consent process. Schrag and her colleagues have compiled a booklet with pictures and quotes from real patients that they are now going to test in their population. “I thought that was a really interesting way of thinking beyond the informed consent document,” said Goldkind.
Along similar lines, the NCI revised its informed consent template for late-phase clinical trials based on expert input from a wide range of stakeholders, including physicians and nurses, IRB members and industry representatives, the FDA, lawyers and ethicists, and patient advocates. One of the results of the NCI’s studies was that shortening and simplifying its document had little impact on satisfaction among a group of colorectal cancer survivors. The NCI also found that people who were familiar with clinical trials were more inclined to want to be part of clinical research. Goldkind said that this finding goes back to one of her earlier points that educating people regarding what clinical research is about on a larger, community-wide basis could provide a contextual framework for people to understand information given to them within the informed consent process.
With regard to going beyond the informed consent form, it is important
that the entire process educating individuals rather than simply informs them, Goldkind said. Understanding informed consent is a continuous process rather than a single event, and informed consent must reflect the diversity of research, meaning that one approach to the informed consent process may not be suitable for all types of research. It is also important, Goldkind said, to recognize the role that the larger community, such as patient advocacy groups, community-based advisory boards, and disease-specific foundations, can play in improving the informed consent process beyond improving the actual consent document. She also suggested that the field should reach out to other disciplines and co-opt successful research tools from the social-behavioral and decisional sciences, successful teaching techniques from educators, and effective communication skills.
Goldkind concluded her talk by describing the challenges of discussing information sharing in the informed consent process. It will be important, she said, to conduct research that can identify what people want to know about how data will be shared, what will be disclosed when data are pooled and shared across multiple sites, and how their biospecimens will be used. Questions that she said need answering with regard to data sharing include the following:
- What does privacy mean in today’s highly matrixed and technologically sophisticated world?
- How would the public weigh protection of individual privacy against the utilitarian benefits to public health that could come from future use of linked datasets and/or biospecimens?
- How should differing national concerns and sensitivities be bridged?
- Ultimately, what is the optimal manner to present this information in an informed consent process?
She ended her comments by stating, “I want to emphasize the need for public dialogue and for education coupled with evidence-based research on informed consent.”
FACILITATING INFORMED DECISION MAKING DURING THE CONSENT PROCESS: STRATEGIES FOR INCREASING MINORITY PARTICIPATION IN CLINICAL TRIALS2
Sandra Crouse Quinn
University of Maryland
Sandra Crouse Quinn started her presentation by asking how many of the workshop participants had ever heard somebody say, “I am going to consent the subjects.” Her point in asking that question was to show the power differential that is inherent in the informed consent process and to begin the discussion of how that power differential might affect how members of racial and ethnic minorities might react in the context of the informed consent process. She also noted that, although research has been showing that racial and ethnic minorities are increasingly willing to participate in research, they still are not in fact participating. “How can we look at informed consent to help address that?” Quinn asked, adding that she particularly wanted to focus on the conversation part of the process rather than on the document.
She said that research shows that there is poor recall and understanding of information presented during the informed consent process and that there is a lack of knowledge, particularly among racial and ethnic minorities, about research and research terms. When the consent process is done well, these challenges can be overcome, and trust can be built between researcher and participant, but when done poorly, mistrust can be reinforced by the consent process.
In an effort to improve this situation, Quinn and her colleagues conducted a survey of 347 investigators, research staff, and IRB members whose racial and ethnic identity included Caucasian, African American, Latino, Asian, and Native American researchers (Butler et al., 2013). On average, these investigators had 14 years of research experience and were nearly 47 years old. They also conducted a national phone survey of adults in African American and Latino communities (see Table 3-1). They asked researchers such questions as “What methods do you use during the informed consent process?” “How do you assess understanding?” and “What generally do members of the public know about research terms and the purpose of informed consent?” They asked community members such
_____________
2 This section is based on the presentation by Sandra Crouse Quinn, associate dean for academic affairs, professor of family science, and senior associate director of the Center for Health Equity at the University of Maryland, College Park, and the statements are not endorsed or verified by the IOM.
TABLE 3-1 Demographic Distribution of Participants in a National Phone Survey About Informed Consent
| Demographics (Total n = 2,455) | Latinos (n = 1,264) | African Americans (n = 1,191) |
| Gender (females) | 63% | 68% |
| Age (mean and SD) | 47.1 (17.4) | 54.3 (16.9) |
| Education (college or above) | 45% | 56% |
| Marital status (married or living with a partner) | 63% | 50% |
| Employment | ||
|
• Full-time |
37% | 31% |
|
• Retired |
18% | 35% |
| Health insurance | 74% | 82% |
| Income | ||
|
• <$36,000 |
56% | 56% |
|
• $36,000–$76,000 |
27% | 27% |
|
• >$76,000 |
18% | 17% |
NOTE: SD = standard deviation.
SOURCE: Quinn, 2014.
questions as “How would you like to learn about the consent process?” and “What strategies do you use to increase understanding, and what methods might be helpful for you to understand the informed consent document?”
In discussing some of the results, Quinn said that the phone surveys revealed that two-thirds of the community members understand the terms “confidentiality” and “anonymous” but that the level of understanding drops from there. When they compared the methods the researchers used to elicit the preferences of the community members, they found that some methods, such as taking home information, one-on-one discussions, having a family member or friend present, and holding multiple meetings, were closely matched. However, whereas researchers were less inclined to talk with the participants, hold group discussions, and use new methods such as video and interactive games, participants were much more likely to prefer these methods. “Community members wanted more meetings and more opportunities to talk about the consent process,” said Quinn. They wanted to talk with other participants or potential participants in group discussions, and they saw videos as potentially helpful (see Figure 3-1). On the other hand, community members did not find it particularly useful to have the consent form read to them, a practice that was common among researchers. Quinn noted that many of the community members’ prefer-
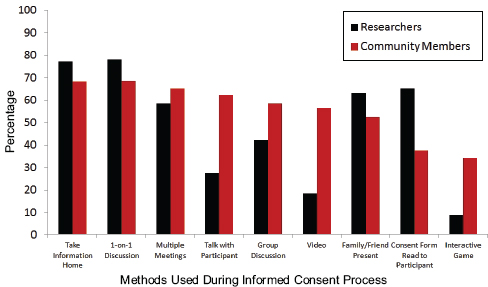
FIGURE 3-1 Comparison of researchers’ methods to community member preferences.
SOURCE: Quinn, 2014.
ences coincided with what the literature says are the most effective means of conveying the information needed to make an informed consent decision.
Regarding the format of the consent form and how content was delivered, 97 percent of researchers said they used plain language, a finding that Quinn called into question, given the state of most informed consent documents and the research showing that informed consent documents are written at a relatively high grade level. Fewer than 20 percent of researchers used a summary at the end of these complex documents, but a majority of the community members said that a summary would be helpful (see Figure 3-2).
In this study, Quinn and her colleagues also asked researchers how they assess understanding. Some 52 percent of the researchers asked open-ended questions of the potential participants, and nearly the same number had participants sign and initial every page, which Quinn said has never been shown to be an effective means of assessing understanding. Nearly 40 percent used teach-back methods, and about 10 percent used an independent monitor or some form of questionnaire. One disturbing finding was that 32 percent of the researchers did not assess understanding at all.
Summarizing these findings, Quinn said that what is known about informed consent is that participants may have incomplete comprehension of information delivered during the informed consent process and that there
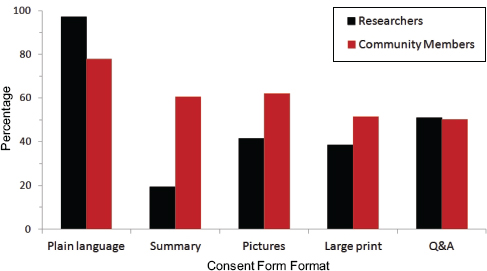
FIGURE 3-2 Comparison of formatting approaches that researchers use and community members’ preferences.
SOURCE: Quinn, 2014.
are discrepancies between researchers’ practices and community members’ preferences in both learning about a study and in the informed consent document. She added that it is clear that researchers’ assessment of participant comprehension is limited and sometimes inadequate and that there are issues with the use of plain language in the informed consent document. She then made two recommendations. First, she said, it is imperative to increase comprehension using methods that research has shown to work, such as one-on-one discussion, multiple meetings, and plain language, and then to make it a standard practice to assess understanding. Second, it is important to increase satisfaction using such methods as one-on-one discussions, multiple meetings, pictures, and summaries. “Our team firmly believes that recruitment and the informed consent process are the beginning of a relationship, and if we begin that relationship in a way that fosters trust and understanding and dialogue, we believe that will ultimately play out in a successful completion of that research subject,” said Quinn. “Increasing satisfaction will help us to build that trust at the beginning.”
She then described the Building Trust research initiative that she and her colleagues have been conducting and the Web-based interaction educational program that they have developed as a resource for researchers and their community partners. On the basis of the data collected, Quinn’s team is creating three curricula, two of which are largely complete. One curriculum is aimed at researchers and staff, and it answers such questions as the following:
- How do you recruit?
- How do you address the history of race and distrust and research abuses?
- How do you address issues that are more complex even when we adhere to the guidelines, even when we do everything right?
- How do we think about complicated ethics?
- How do we have critical conversations in our own research teams about race and ethnicity and recruitment?
- How do we retain people, and how do we build community partnerships?
The second curriculum is for researchers and community organizations to use to explain what research is to their community members. “What we are saying is that it is time for a broader educational component about informed consent that doesn’t wait until the person arrives in your clinic ready to potentially participate in the study, but really helps them to understand it,” said Quinn. This curriculum aims to explain why community members should participate in research and how their participation makes a difference, particularly in the context of health disparities, she explained.
She then showed parts of the Web-based version of this second curriculum, which comprises three components: the importance of research, informed decision making, and the ways community members can be involved with researchers. Each component has video and audio materials, didactic material, questions for discussion, and resources that community members can download for later use. The informed decision-making component, for example, starts by addressing a set of myths and facts about research and informed consent (http://www.buildingtrustumd.org/unit/informed-decision-making/do-you-know). It then addresses the lessons that were learned from the past, particularly from some of the abuses that occurred and the precautions that have since been put into place to protect participants in research studies. The curriculum then answers questions about why community members should participate in research and what informed consent is, including a glossary of terms and the 10 key elements of the informed consent process and the means to identify them. The curriculum then provides a list (which can be downloaded and printed) of 10 key questions to ask a researcher before agreeing to join any study (http://www.buildingtrustumd.org/unit/informed-decision-making/knowledge-ispower). The questions are as follows:
- What is the main purpose of the study?
- What will I be asked to do during the study?
- How will I benefit from participating in this study?
- What are the possible risks?
- How will the results be shared?
- How will my personal information be kept confidential?
- How long is the study going to last?
- Are there any reimbursements or incentives offered?
- Who is funding the study?
- What are the credentials of the researcher and the researcher’s institution?
In conclusion, Quinn said that she and her colleagues believe that a several-pronged process is essential to overcoming underrepresentation of minorities in clinical research and that the informed consent process can be one of those prongs. “There is a broader educational effort that is important, and then there are the specific components of improving informed consent when somebody comes in to talk about participation,” said Quinn. “Those are critical to building trust and to creating a more educated participant.”
DEVELOPING A BETTER PROCESS FOR INFORMED CONSENT3
Yael Schenker
University of Pittsburgh
The focus of her talk, said Yael Schenker, was to describe practical steps to improve the process of informed consent in the effort to achieve ethical goals (Schenker and Meisel, 2011), and she used a specific case to frame the discussion. This case involved “Mr. L,” a 70-year-old man with end-stage heart failure who was being evaluated for a destination left ventricular assist device (LVAD). An LVAD, explained Schenker, is a complex device consisting of a pump connected to an external computer that does the work of the left ventricle of the heart pumping blood throughout the body. Surgical mortality for LVAD surgery ranges from 5 to 30 percent: it is considered a high-risk procedure. The decision to have a destination LVAD implanted is also a preference-sensitive one, meaning that it involves significant tradeoffs affecting quality and length of life. Schenker emphasized that LVADs are one of many cases where we face challenges in informed consent, and she believes that it is equally important to examine and improve the consent process for less complex and lower-risk procedures.
Schenker drew an analogy between informed consent and scaffolding. Like scaffolding, informed consent performs a basic safety function—
_____________
3 This section is based on the presentation by Yael Schenker, assistant professor of medicine at the University of Pittsburgh, and the statements are not endorsed or verified by the IOM.
protecting patient autonomy and helping ensure that patients have the fundamental right to decide what is done to their bodies. And, like scaffolding, she said, informed consent supports the building of the cathedral; in this case, the cathedral is patient-centered health care. “Informed consent is the platform from which we work to help ensure that patients are involved in medical decisions and that these decisions reflect their values and preferences,” Schenker said.
There are many documented failures of informed consent, according to Schenker, including the failure to achieve adequate patient understanding that can lead to medical errors or the receipt of preference-discordant care. Some commentators have viewed these failures as evidence that the requirements of informed consent are unrealistic or that the concept itself is somehow flawed. Schenker said she does not share this view; rather, she believes that it is possible to improve the process of informed consent, and she cited evidence to support this more optimistic view (Schenker et al., 2011). Data from a systematic review that she conducted with several colleagues demonstrate that relatively simple or straightforward interventions can improve patient comprehension in informed consent (see Figure 3-3). “I would submit that rather than abandon the cathedral, we build a better scaffolding,” said Schenker. “I think that when we look carefully at key
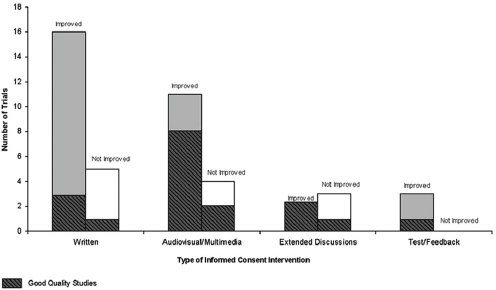
FIGURE 3-3 Review of 44 trials indicating possibility of improving patient comprehension.
SOURCE: Schenker et al., 2010.
steps of the process—the who, when, what, and how of informed consent—we find room for simple improvements.”
The “who” of informed consent is the person obtaining informed consent—traditionally this is the physician performing the procedure. In the case of Mr. L, this would be the cardiothoracic surgeon. Schenker emphasized that it is important for Mr. L and the family to have the opportunity to meet with the surgeon prior to surgery and to ask questions, but she questioned whether the surgeon is the best person to conduct the consent process. The surgeon may, for example, have poor communication skills or have little time to conduct a thorough consent process that leads to meaningful consent, or simply may not enjoy talking with patients. Schenker noted that there are other important members of the clinical team involved in the consent process of a destination LVAD. For example, perhaps the LVAD nurse coordinator, Schenker said, probably knows more about these devices than anyone and has more time to spend at the patient’s bedside.
As of 2013, the Center for Medicare & Medicaid Services (CMS) also requires that a palliative care physician be involved in the consent process for this procedure. “When you think about it, this makes sense because a surgeon knows a lot and thinks about the risks of surgery but may not be the best person to discuss alternatives to surgery,” said Schenker, likening the situation to asking an air conditioning company representative for information about ceiling fans. Palliative care clinicians, in contrast, are trained to discuss alternatives, including the alternative of not pursuing a potentially life-prolonging intervention, to think about and compare outcomes for different options, and to elicit patient values.
Schenker noted that a team-based approach to informed consent requires clearly defined roles. She said that involving members of the team who are not involved in performing the procedure may provide more balanced information, improve patient understanding and help to ensure that informed consent is truly an informed choice that reflects patient values. “I would propose that this approach can also be more efficient if each member of the team is charged with achieving a smaller piece of the consent process at the appropriate time,” she added.
Turning to the “when” of informed consent, Schenker noted that previous speakers at the workshop had addressed the problem of obtaining informed consent immediately prior to a planned procedure. Mr. L, for example, may be too sick at the point of receiving an LVAD to participate meaningfully in the consent process, meaning that a family member (or surrogate) may be required to provide consent. He may also be psychologically committed to the procedure at that point. Commentators have written that informed consent in such a situation constitutes little more than a medical Miranda warning (Meisel and Kuczewski, 1996). In contrast, there are several potential advantages to starting the consent process in advance—
the patient may not be as sick, and multiple information sessions may be possible, for example. For LVAD surgery and other high-risk procedures, starting the process in advance would give the patient more time to prepare, engage, and ask questions, making informed consent an informed choice rather than an acknowledged understanding of a treatment option that has, for all intents and purposes, already been chosen.
Timing does matter, said Schenker, and she illustrated one possible workflow for LVAD surgery (see Figure 3-4). “I think the nature of this workflow will vary depending on the urgency, complexity, and preference-sensitive nature of a procedure,” she said. “When we talk about informed consent as a process, I think it is important that we allow time for this process to occur.”
In discussing the “what” of informed consent, Schenker noted that the current focus of consent discussions and consent forms is on risks. She said that for a high-risk procedure such as LVAD surgery, it is appropriate to discuss these risks in detail. However, an overwhelming focus on risk has several potential downsides. One is that risks are often described in vague terms—“There is a risk of bleeding and infection,” for example—that could apply to a simple blood draw as much as it does to destination LVAD. Laundry lists of risks are also overwhelming. When presented with forms written in fine print, patients will often just skim them, sign them, and hope for the best. Schenker emphasized that a focus on risks in this manner can also be impersonal. “It is not clear to what extent each risk on the laundry list will apply to you,” she explained. “If the risk of surgical mortality is 30 percent, patients may hope that they will be in the 70 percent.”
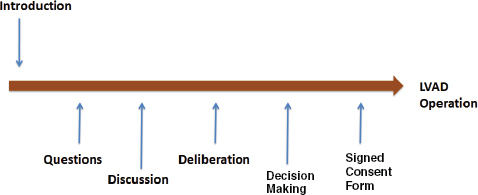
FIGURE 3-4 Possible workflow for conducting meaningful informed consent for a high-risk surgical procedure.
SOURCE: Schenker and Meisel, 2011.
Instead of focusing on risks, Schenker proposed that the focus of informed consent discussions should be on outcomes. A focus on outcomes involves thinking about the best-case scenario, the worst-case scenario, and the most likely case scenario for an individual patient (Schwarze et al., 2013). For Mr. L, the best-case scenario may be that he survives the operation and can return home and live independently for another five to seven years. The worst-case scenario may depend on Mr. L’s values: it may be that he dies during the operation, or it may be that he suffers a devastating postsurgical complication, such as a stroke, that leaves him requiring 24-hour care for the rest of his life. Finally, the most likely scenario for Mr. L may be that he survives the surgery and is able to return home but is unlikely to be able to return to activities he previously enjoyed, such as sailing. Once these scenarios are compiled, it is then possible to discuss how these outcomes, and the outcomes for alternative therapies, align with the patient’s goals (see Figure 3-5). “Thinking about outcomes in light of a patient’s goals helps to contextualize risks and may aid patients in making more informed and personal choices,” said Schenker.
Ending with the “how” of informed consent, Schenker spoke about two best communication practices: “ask-tell-ask” and “show, don’t tell.” Ask-tell-ask is a variation of teach-back that has been recommended for use in many types of medical conversations, including discussions with seriously ill patients near the end of life and conversations to engage patients in the self-management of chronic illness (Back et al., 2009; Bodenheimer et al., 2005). Schenker believes that “ask-tell-ask” is also a useful model for informed consent. Ask-tell-ask starts by inviting the patients to share
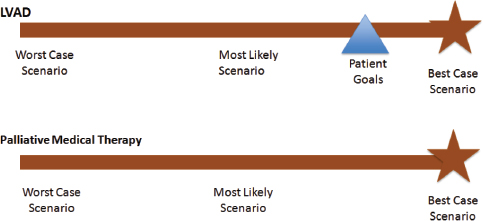
FIGURE 3-5 Aligning patient goals and outcomes.
NOTE: LVAD = left ventricular assist device.
SOURCE: Schwarze et al., 2013.
what they know about a procedure. This approach not only signals the importance of the patient’s involvement but also elicits any potential misunderstandings or misconceptions at the start. The clinician can then use the time more efficiently to fill knowledge gaps and correct misconceptions. The final ask is framed not as a test or a challenge but rather as an opportunity to help the clinician to do a better job of explaining the next time. For example, the clinician may say something like, “I want be sure I have done a good job of explaining things today. Can you tell me what we talked about?”
The “show, don’t tell” approach replaces descriptive text with pictures, videos, and demonstrations. “As I mentioned, LVADs are complex devices requiring lines of fine print to describe. Why not show a picture instead? Postsurgical care and conditions are also complicated. Why not use a video or perhaps even introduce a real patient?” asked Schenker. Evidence supports the idea that pictures or video can help patients envision both treatments and their outcomes (Volandes et al., 2009). Technology can also help engage patients in the informed consent process and connect patients with others who are contemplating or have already received a high-risk procedure, for example through online support groups.
INFORMED CONSENT AND PATIENTS WITH LIMITED ENGLISH PROFICIENCY4
Alicia Fernandez
University of California, San Francisco
Alicia Fernandez began this session’s final presentation by noting that there are no national or multicenter data on how best to overcome language barriers in conducting the treatment-related informed consent process. She also explained that the definition of limited English proficiency comes from the U.S. census, which starts with the question of whether an individual speaks a language other than English at home and, if the answer is yes, then asks if that individual speaks English very well, well, not well, or not at all.
According to the Census Bureau’s American Community Survey, some 60 million people, or 21 percent of the U.S. population, speak a language other than English at home, and of this group, 62 percent speak Spanish and under 5 percent speak Chinese, with all other languages accounting for less than 2 percent of those who speak a language other than English at home. About 24 million people speak English below the “very well”
_____________
4 This section is based on the presentation by Alicia Fernandez, professor of clinical medicine at the University of California, San Francisco, and the statements are not endorsed or verified by the IOM.
proficiency level (see Figure 3-6), and 14 million people—11 million who speak Spanish as their primary language—fall into the “not well” or “not at all” categories, representing a population of American residents who cannot really participate in treatment conversations. Fernandez put this population in perspective by saying that it is larger than the combined populations of Guatemala, Honduras, Nicaragua, and El Salvador, and it gives the United States the world’s third-largest Spanish-speaking population. She also noted that the Hispanic or Latino population in the United States has grown from 6.4 percent in 1980 to 9 percent in 1990, 12 percent in 2000, and 16.3 percent in 2010 (see Figure 3-7). Currently, more than 17 percent of the U.S. population is Hispanic or Latino, and one-quarter of these individuals do not speak English well or at all.
The challenges for achieving meaningful informed consent in the low-English-proficiency population go beyond language. Some 60 percent of this population have less than a high school education—in studies by Fernandez’s group at San Francisco General Hospital, the mean education level for patients with diabetes was third grade, for example—and about 6.6 million individuals with low English proficiency fall below the poverty
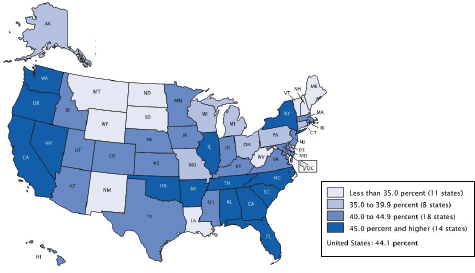
FIGURE 3-6 Percentage of the U.S. population speaking a language other than English at home who spoke English less than “very well,” by state, 2007.
NOTE: Population 5 years and older. For information on confidentiality protection, sampling error, nonsampling error, and definitions, see www.census.gov/acs/www.
SOURCE: Census Bureau, 2007.
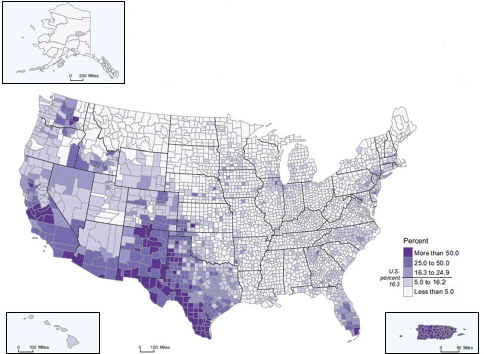
FIGURE 3-7 Hispanic or Latino population as a percentage of total population, by county, 2010.
SOURCE: Census Bureau, 2010.
line. Patients in the low-English-proficiency population are also less acculturated to U.S. health practices, including informed consent practices, and are less likely to question physicians, Fernandez said.
Fernandez listed four options for navigating language barriers: get by with limited language skills and gestures; use untrained interpreters, such as family and untrained staff; hire professional interpreters; and rely on bilingual clinicians. She noted again that there are no national data to answer the question of how the U.S. health care system is actually dealing with this challenge. “We could know, but we don’t know,” is how she characterized the situation. At San Francisco General, which she said has one of the country’s most robust interpreter systems, she and Yael Schenker found that among Chinese- and Spanish-speaking patients with limited English proficiency who received a thoracentesis, paracentesis, or lumbar puncture, only 22 percent had signed a consent form in a language they could read, and only 28 percent had fully documented informed consent that made use of an interpreter (Schenker et al., 2007) (see Table 3-2).
Fernandez said that the biggest factors that drive underuse of skilled
| LEP (n = 74) % | English (n = 74) % | p-value | |
| Procedure note documenting IC discussion, n (%) | 59% | 58% | 0.9 |
| Consent Form—any language, n (%) | 70% | 85% | 0.03 |
| Consent Form—patient’s language, n (%) | 22% | 85% | <0.001 |
| Fully Documented Informed Consent, n (%) | 28% | 53% | 0.003 |
NOTE: IC = informed consent; LEP = low English proficiency.
SOURCE: Schenker et al., 2007.
interpreters, even at a hospital with a well-developed interpreter system, are physician culture, the perception that communication is perhaps not that important, and the time and hassle involved in getting an interpreter. San Francisco General attacked this last problem by installing a bedside system that connects automatically to the hospital’s interpreter corps via phone or video conferencing, she said. Training physicians in interpreter use, combined with making it convenient, increased interpreter use by 30 percent, she noted. However, physicians at San Francisco General report using untrained interpreters frequently, largely because it is convenient and because they are not aware of the evidence on communication errors associated with using family members or untrained staff as interpreters (Diamond et al., 2009).
In contrast, said Fernandez, there is substantial evidence from audiotape studies that professional interpreters provide more accurate information than ad hoc interpreters and that the use of professional interpreters increases patient and physician satisfaction compared to when ad hoc interpreters or no interpreters are used (Karliner et al., 2007; Tschurtz et al., 2011). Nonetheless, there are issues about the use of professional interpreters that bear underscoring, she said. Currently, there is a certification and supply problem, as there are no mandatory national standards for what constitutes appropriate certification for professional interpreters. California, for example, mandates interpreter training, but many states do not. Fernandez explained that the Joint Commission suggests that hospitals have some way of knowing that their interpreters are competent, but it has not established clear standards for doing so.
The quality of interpreters varies across the country, she added, with limited national data on actual interpreter use or availability. One study conducted in Washington State, a state that Fernandez said has paid a great deal of attention to informed consent, used audio recordings in the intensive care unit to check the accuracy of information passed on by professional
interpreters (Pham et al., 2008). A blinded review of the tapes by the investigators found that for every exchange of information, there was a 55 percent chance that an alteration, such as an addition, omission, substitution, or editorialization, would occur. Of these alterations, 75 percent were judged to be of clinical significance, and 93 percent of them were likely to have a negative effect.
For example, in one case a family member asked the doctor, “What we want to know is, after his lungs get better, and when he wakes up, will his brain suffer and affect his ability to recognize people?” What the interpreter said was, “Okay, so she wants to know about the lungs when he wakes up. So about his lungs and what about after, will it not affect him?” The physician replied, “Right now, it is very interesting to us because we don’t understand what the problem is in his lungs.” In another example, the physician said, “I don’t know. This is a very rapidly progressing cancer,” whereas the interpreter said, “He doesn’t know because it started gradually.”
Fernandez said that interpreters themselves believe they need to do a better job. She and Schenker, along with other colleagues, surveyed interpreters regarding end-of-life discussions. Some 85 percent of them—most of whom were experienced and certified—had multiple discussions per week, but only half of the interpreters reported that those discussions usually went well. Eighty percent reported wanting additional training in end-of-life interpreting, and 81 percent thought that physicians needed more training in working with interpreters (Schenker et al., 2012). Fernandez described another study, conducted at Bellevue Hospital Center in New York City, that compared two state-of-the-art interpreter systems and language-relevant bilingual physicians who were seen in the emergency department (Gany et al., 2007). When patients were asked whether they understood the doctor’s explanation of their diagnosis and their medication instructions, fewer than 40 percent of those who received those explanations via either of the interpreter systems understood key points. In contrast, close to 60 percent of those who received their instructions straight from the bilingual physician understood key points (see Table 3-3).
Multiple studies, said Fernandez, have shown that language-discordant care results in lower levels of comprehension, patient satisfaction, and trust in the physician. In a study that she and her colleagues conducted at Kaiser Permanente of Northern California, 35 percent of low-English-proficiency patients with diabetes who were treated by a physician who did not speak Spanish reported a lack of trust, compared to only 16 percent of those treated by a Spanish-speaking physician who reported a lack of trust (Schenker et al., 2010). “Trust is an essential element of any informed consent discussion, as we cannot expect our patients to become physicians and make the choices that we can help them make,” said Fernandez. In addition, 20 percent of the patients who received language-discordant care
TABLE 3-3 Professional Interpreters Versus Bilingual Physicians
| Interpreter System A | Interpreter System B | Language Concordant MD | |
| Understood MD explanation Dx | 35% | 39% | 59% |
| Understood Rx instructions | 33% | 38% | 63% |
NOTE: Dx = diagnosis; MD = physician; Rx = prescription.
SOURCE: Gany et al., 2007.
reported feeling poorly treated because of the language barrier, and 40 percent thought their physician did not show respect when their doctor did not speak their language (see Table 3-4). Unfortunately, she added, “about 30 percent of all of our patients, irrespective of language, believe that we do a poor job of listening to them.”
Bilingual physicians are more likely to be patient centered and elicit their patients’ points of view, Fernandez said. In observational studies comparing bilingual physicians and interpreted discussions, the latter have fewer open-ended questions and less elicitation of questions or values. Data from studies that Fernandez and her colleagues conducted (Fernandez et al., 2011) show that patients with diabetes treated by language-discordant
TABLE 3-4 Suboptimal Communication Resulting from Language-Discordant Care
| English-proficient n = 8,116 | LEP n = 522 | P value | LEP-LC n = 210 | LEP-LD n = 153 | P value | |
| Lack of trust in MD | 26% | 25% | 0.37 | 16% | 35% | <0.0001 |
| Treated poorly because language | 2% | 12% | <0.001 | 9% | 20% | 0.001 |
| MD not showing respect | 28% | 30% | 0.31 | 29% | 39% | 0.04 |
| MD not listening | 33% | 28% | 0.02 | 26% | 32% | 0.24 |
NOTE: LC = language concordant; LD = language discordant; LEP = low English proficiency; MD = physician.
SOURCE: Schenker et al., 2010.
physicians are twice as likely to have poor glycemic control, though they are equally likely to take a cholesterol medication. “We think that as discussions become more complex, the role of language and direct communication takes on more importance,” said Fernandez.
Regarding how to address the challenges regarding individuals with limited English proficiency, who are among the most vulnerable of all patients, Fernandez said that to start, more data are needed on the state of the problem and on what is happening nationwide. There is also a need, she said, for national standards for interpreters and the mandatory use of certified professional interpreters for high-risk treatments and procedures, including high-risk outpatient decisions, such as a decision to start chemotherapy. “I think we could set a minimal standard requiring documented use of an interpreter for hospitalized patients as once a day. Once a day, if you are sick enough to be in the hospital, you should be able to speak to a treating physician.” There should also be a signature line for the interpreters on the informed consent form to enable auditing. Health care systems should also facilitate additional interpreter training as well as training for medical students and residents on the use of professional interpreters. Technology, such as video-mediated interpretation and qualified telephone interpreters, could also be better used to address language barriers.
Several years ago, San Francisco General created state-of-the-art consensus forms in five languages that prompt a physician to call an interpreter. However, a survey of physician behavior conducted 1 year after rolling out these forms found no change despite what Fernandez characterized as “our best efforts at scolding and educating the residents.” Today, the situation has improved, as the most recent survey showed an increase in resident self-reporting of interpreter use for informed consent, though she cautioned that the results of an audit are pending. She believes, though, that it is possible to change physician practice patterns, albeit slowly.
In summary, said Fernandez, many patients—including those proficient in English—have trouble with complex communication. For example, a study of English-speaking patients undergoing angioplasty found that 80 percent believed erroneously that angioplasty would reduce their risk of myocardial infarction and reduce mortality (Rothberg et al., 2010). The physicians, who were also interviewed, did not share that erroneous belief. In Fernandez’s opinion, “Improving care for low-English-proficiency patients and focusing on low-English-proficiency patients will help improve informed consent for all patients.” Accomplishing that task, she added, requires “ongoing commitment from all levels of leadership and from all levels of participation in the health care industry.” She recommended that the roundtable convene a group to focus specifically on the problems of language barriers and to do it for two reasons. “One, it is the right thing to do. People are struggling out there knowing how to best take care of these
patients ethically and legally. Second, if it is not because of these patients, then do it because I think it will improve informed consent for all patients.”
George Isham started the discussion with the comment that when lawyers help their clients with estate planning, they often introduce decision making with respect to their clients’ preferences at the end of life. He wondered whether there is a way to disaggregate the decision-making process by first understanding patients with respect to their values and preferences. “I wonder if we are really thinking about the relationship of these concepts and the systems approach to understanding our patients’ needs and preferences and approaching them with decision-making and then using technology on the provider side to make that information available at the point of care,” said Isham. He then asked Schenker if she and her colleagues were thinking about this type of approach. “Yes, definitely,” she replied. “Informed consent is often the trigger that gets doctors thinking about this.” She added that, in her opinion, there is time to start the consent process in advance for many kinds of procedures. In the case of destination LVAD surgery, for example, heart failure is often a chronic disease, and most of these patients have been seen in the hospital repeatedly, long before the decision is made to implant an LVAD. “We don’t think about bringing some of these things up until the procedure is imminent,” said Schenker. “I think the more we can incorporate these conversations earlier, the better.”
Kim Parson remarked that she was surprised by Goldkind’s statement that dropouts from clinical trials were not interviewed to find out why they withdrew and asked whether there were rules or regulations that would limit such conversations. Goldkind replied that she was not aware of any legal limitations and that she believed that investigators should be encouraged to conduct such interviews as part of doing good research. She also said that not doing so is a missed opportunity and forfeits the ability to collect valuable information. “You don’t know whether it is because they are disgruntled with the study, whether they had adverse events that they are not reporting, or whether they feel like they didn’t get the benefits out of the research that they thought they were going to be getting,” said Goldkind. These data would not only help improve the consent process but also help researchers design better trials and provide better data on the efficacy and safety of the intervention being studied. She did acknowledge that it takes effort to track down trial dropouts because often they simply stop returning to the clinical setting.
Roundtable member Catina O’Leary, president and chief executive officer of Health Literacy Missouri, asked the panelists if the risk level differed between biomedical studies and community studies. “When you talk
to community members as Dr. Quinn’s group has done, you see that many times those community members feel the risk of what they are doing in the moment is as significant as anything else that anybody else would do, even a surgery or other things,” said O’Leary. Quinn commented that in her study of community members, she and her colleagues asked African Americans and Latinos if they would be willing to participate in a range of studies with different levels of risk. What they found was that there was a surprising willingness to participate even as the level of risk rose. The respondents were motivated, she said, by wanting to help future generations, believing that they could make a contribution somehow. She cautioned that “when we focus on risk, we need to be careful that we don’t have preconceived notions about what people are willing to do, and we have to talk about benefits,” said Quinn. “The benefits may be not simply benefits to the individual but benefits to the community or to broader society.”
Goldkind added, citing anecdotal experiences she has had working with disease-based foundations and groups in a number of settings where risk was high, that in some cases it was clear that the people who were going to be enrolled in research were not going to be the beneficiaries of that immediate intervention. “What struck me was how very engaged the groups were and how much input there was in terms of design, the informed consent process, the language used, and the understanding of what risk levels they were willing to tolerate beyond what we actually expected they would [be willing to incur],” said Goldkind. The lesson she learned from these anecdotal experiences is that investigators should not underestimate the power of dialogue and person-to-person exchanges.
Isham then asked if that dialogue should be conducted only when there is something to offer participants in research or if it should happen in the treatment setting, too. “Should we be asking those questions beforehand so that we know how to approach our patients in the first place?” asked Isham. Quinn said that it should happen and that community review boards are a good avenue to engage in those conversations about risks and concerns before studies even get started. She noted that her team was about to submit a paper describing a conceptual model for creating and maintaining openness to research. “We think of this as a long-term relationship,” said Quinn, “and if we are really smart as researchers, we would go back to these communities and [tell them] here is what we found and ask what they think the results mean.”
Wilma Alvarado-Little asked Quinn if she had looked at the generational status of African American and Latino patients to see if that would lend some insight into their responses and reactions. Quinn replied that she and her colleagues are in the process of analyzing data from such a study. Regarding the idea of the medical Miranda warning, Alvarado-Little asked Schenker if patients hear that they have a right to remain silent, and
Schenker replied that informed consent discussions often convey the notion that patients should remain silent. Addressing Fernandez, Alvarado-Little asked if any steps were being taken to address inaccuracies that occur during translation, and Fernandez replied that interpretation is very difficult, particularly in end-of-life discussions because many concepts may not be known and because of nuances that might be lost during translation. She and her colleagues have been working with the California HealthCare Foundation and the California Interpreter Association to create a free online curriculum designed to help interpreters improve their end-of-life conversations. Preliminary data show that interpreters like this curriculum, that they learn from it, and that they are more open to doing palliative care because of it.
Benard Dreyer asked Fernandez if there were any data showing the comparative effectiveness of live interpreters and telephone-based interpretation, and Fernandez replied that telephone interpretation is the least effective option. Video interpretations are gaining wider use, and these are more effective, she said. Thanks to technology solutions such as Skype and tablet computers, it should be possible to make use of interpreters with skill in any language and have interpreted conversations in real time wherever the patient is. She said that the private sector needs to step up to make this type of capability broadly available, and she added that “the research is unequivocal that video or in-person are both much better than telephone interpreters.”
In response to a question from Dreyer about whether there are any interventions in the clinical as opposed to the research setting that get people to take more time during the consent process, Schenker replied that it is sometimes difficult to find more time in busy clinical settings. However, she said, the timing of when the patient is engaged in the consent process should change, and we should also think about who is conducting the informed consent process. As an example, she said that a surgeon may rush from one surgery into the preoperative waiting room to start the consent process for the next. “There may be a member of the team who is much more present and able to complete pieces of that process earlier,” said Schenker.
Cindy Brach continued on the theme of bringing in other members of the health care team to conduct pieces of the consent process by asking Schenker if the CMS requirement to bring in a palliative care expert prior to LVAD surgery might raise accusations of death panels. “How do we make sure all of the choices get on the table?” asked Brach. “Who are the right people to talk about those choices?” Schenker replied that, in her experience as a palliative care physician, she and her colleagues are good at taking a patient-centered approach that aims to elicit values and helps patients weigh options. She noted that she has watched the consent process
evolve to become more of a team process where each team member brings something different to the table.
Bernard Rosof voiced the opinion that an important contribution to increased understanding by research participants would be to increase understanding among the research community about excellence in informed consent. Ruth Parker responded that what she hears in the patient-centered community environment is that the focus still needs to be on helping patients and prospective participants better understand the consent process at the community level.
Parker then asked Goldkind if the same informed consent processes will work in the clinical and research settings, given that research studies are mostly about determining safety and efficacy and that informed consent in the clinical setting has more to do with personal liberty and doing no harm. Goldkind replied that she believes that there are some distinct differences between informed consent in the clinical setting and the research setting that have to do with some of the assumptions that are made about motivations behind the consent process. “When clinicians are speaking to their patients about a treatment, the idea is, ‘I am trying to do something good for you. You are my center of focus,’” explained Goldkind. “As a physician who does clinical ethics, I really think it ought to be about taking the medical options and putting them within the patients’ value systems, their medical needs, and their life context.”
Informed consent in the research setting is more about protection that is downstream, Goldkind said. “We should never get to informed consent if we don’t think as a research community, as a researcher investigator, as an IRB, that the research has the right risk/benefit ratio and that the scientific questions that are being asked are critically important,” she continued. “Once that is all in place, there is still the idea that this research is protocol driven. The interventions are not necessarily for the treatment of that individual patient, but to generate scientific knowledge. That shift changes, in my mind, the parity between clinical informed consent and informed consent obtained in the research context.”
Michael Villaire, chief executive officer of the Institute for Healthcare Advancement and a roundtable member, asked whether there are any anecdotes or observations regarding how much value individuals with limited English language capabilities place on the informed consent process as a concept. He noted that his health care nonprofit is signing up people for health insurance who have never had health insurance, and they are so excited to be able to receive medical care now that they do not want to be faced with choices and to digest information, which creates another barrier for the informed consent process. In fact, replied Fernandez, there are data showing that 20 to 30 percent of older patients or patients in vulnerable groups do not want a consumer model of shared decision making—they
want their doctor to decide. Fernandez herself has patients who want her to make the choices and who say they trust her to do so. “I think that is completely valid and should be respected,” she said.
The situation becomes more complicated when trust is broken, however, and Fernandez referred to the fact that most of her residents do not know the story about experiments conducted in Guatemala in which people were intentionally infected with syphilis but that most of her patients—many of whom cannot read—all know that story.5 “What happens when there is no trust or when there isn’t a trusted care relationship or when the patient is sick, and the doctor asks, ‘Chemotherapy or no chemotherapy?’ This is very complicated and cannot be fixed by a form,” she said.
Turning to the role that regulations may or may not play in complicating informed consent forms, Andrew Pleasant, senior director for health literacy and research at the Canyon Ranch Institute and a roundtable member, noted that in his work as a community researcher he interacts with multiple IRBs across the country, and they all apply the existing regulations differently. What he has heard from the presentations is that tailoring situational approaches to the process is missing and very necessary, and he wondered if the regulations should actually require tailoring according to best practices in health literacy. He then asked the panelists if they had some idea of what such regulations would look like. Goldkind responded that it is important to remember that applying regulations uniformly eliminates the ability to have the very flexibility Pleasant wants. “Regulations just can’t be granular enough to cover all of the nuances of different contexts and study populations and scenarios,” said Goldkind, and she cautioned that layering additional requirements on top of those already mandated will only make it harder to incorporate the type of changes that the literature or empirical studies might demonstrate would work best for a specific context.
Fernandez took the opposite view and said that there are areas where more regulation may be beneficial but that empiric data are needed to settle that question. As an example, she said that Washington State regulates what needs to be included in informed consent, but other states do not. The empiric question that needs to be answered is whether people in Washington State understand the same procedure better than someone from western Massachusetts. “I haven’t seen any data, but I suspect they do,” said Fernandez, but the bottom line, she noted, is that the answer is currently unknown.
Isham concluded the discussion by wondering if the process of improving informed consent should start with patients rather than with the process
_____________
5 This research was funded by the U.S. government and conducted in Guatemala from 1946 to 1948. More information is available at http://www.hhs.gov/1946inoculationstudy/factsheet.xhtml (accessed January 29, 2015).
itself and if those who are involved in efforts to improve informed consent should start thinking about the categories of information that patients want. “What are the questions of life or death, function, consequences of the intervention, likelihood of success, potential impact of research? Is it a worthwhile study? Is it a trivial study? Is it a big question? Is it a little question? Is it an early calibration issue or not? Do the answers to these questions make a difference to whether people want to step forward and volunteer or not?” asked Isham. Schenker agreed that the field should take such a patient-centered approach but noted that this is not always seen in the clinical setting. “I think the requirements of informed consent really grew out of a desire to involve and protect patients,” said Schenker. “Unfortunately, I think, given the way the process has been operationalized for many procedures in many different clinical settings, that is not what has happened. To the extent that we can rethink our approach and extend beyond informed consent to informed choice, this would be valuable.”






























