
|
WORKSHOP IN BRIEF |
OF THE NATIONAL ACADEMIES Advising the nation • Improving health |
Engineering Optimal Health Care Scheduling: Perspectives for the Nation—Workshop in Brief
On November 21, 2014, the Institute of Medicine’s (IOM’s) Committee on Optimizing Scheduling in Health Care convened a public, one-day workshop titled “Engineering Optimal Health Care Scheduling.” Funded by the Department of Veterans Affairs (VA), the aim of the session was to explore standards for patient access to health care services across the continuum of care to inform the work of the committee and to shape the content of their upcoming consensus report.
As outlined in introductory comments by committee chair Gary Kaplan, CEO of Virginia Mason Health System, the identification and assessment of best practices and standards for wait times in health care require looking at the entire care delivery system as a single and complex entity with many interrelated and dynamic parts. The workshop convened leading authorities on care delivery, operations management, systems engineering, and patient engagement and satisfaction to
- Better understand the current practices and standards in appointment scheduling and reasons for variation;
- Consider optimization strategies and experiences in health care and other industries;
- Discuss the role of patients and family as catalysts for achieving operational excellence in health care;
- Explore the changing mental model for frontline personnel involved with scheduling improvements; and
- Examine the disciplined structure for change and a strategic and scalable approach to continuous improvement.
The workshop included four panels: current best practices, patient experiences and expectations, technical approaches to wait time improvement, and an overview of the day’s discussion. In addition, a working lunch session considered issues in identifying a toolkit for health systems to implement optimal scheduling practices. For each panel, a moderator and several speakers provided framing comments and presentations that then opened to general discussion. This brief summary of the workshop captures the major topics and issues that emerged over the course of the day and is accompanied by a Workshop in Brief specifically targeted to perspectives for the Veterans Health Administration. Statements, recommendations, and opinions expressed are those of individual presenters and participants and are not necessarily endorsed or verified by the Committee on Optimizing Scheduling in Health Care or the IOM, and they should not be construed as reflecting any group consensus.
Current State: Practices, Standards, and Innovation
Throughout the course of the workshop, many presenters and commenters, including Kaplan and Mark Hallett of ThedaCare Center for Healthcare Value, emphasized the importance of addressing this issue from a systems view, focused on the value stream throughout the continuum of care. “Underlying the system changes are the stories that either propel us to new pinnacles or keep us pinned to our current performance,” said Peter Pronovost of Johns Hopkins Medicine.
The observation came from many speakers that the components that drive the scheduling process are dynamic and require continuous monitoring and balancing of the supply and demand on the system.
Our scheduling process actually begins with a single question when we get a patient calling on the phone. That question is: “Would you like to be seen today?” Recognizing that patients have different needs and different behaviors, and in fact, those behaviors, be it speed sensitive or relationship sensitive, aren’t static. They are dynamic. They change based on the situation (Hallett).
David Krier of Cincinnati Children’s Hospital emphasized in his presentation that “from [Cincinnati Children’s] perspective, it is not terribly complicated, but that doesn’t mean it is easy . . . For the most part, we have kept our focus on supply. That is primarily because it was within our sphere of control to do so.” Terra Thompson, also from Cincinnati Children’s Hospital, expanded upon this concept, detailing the processes and measurements that the health system uses to gauge their capacity (see Figure 1). They have found that making the financial and productivity data available to their providers is key.
Continuing the notion of using a systems approach to improve access and wait times, Andrew Gettinger, of the Office of the National Coordinator for Health IT, stated in his presentation that managing outcomes goes beyond managing IT. He outlined the variation in the scheduling systems at the Dartmouth Hitchcock Hospital and Lahey Clinic, explaining that neither system was better, but rather built to produce outcomes specific to their unique environments. “I don’t believe it is about the IT. I believe it is about the operations that implement the IT,” he said. Reflecting on the panel, Steven Lawless of Nemours introduced the distinction between designing a system to be optimal versus efficient. “Efficient could be more of an internal phenomenon; optimal has to be from the customer’s perspective,” said Lawless.
Patients and Families as Change Agents: Experiences and Expectations
The need to engage patients and family members in the beginning stages of designing a better scheduling system was raised by several speakers and discussants, both with respect to improving patient satisfaction in current systems as well as achieving optimal systems in the future. Panelists divided their comments to focus on the human factors aspect of scheduling and the patient perspective on wait times.
Sara Czaja from the University of Miami provided an overview of the changing trends in consumer expectations and roles in their care. Cjaza noted that “consumers are expected to be empowered and take a more active role in health self-management. There is an increased use of technology within the health care arena that has expanded the realm of health-related tasks that consumers are expected to or can perform.” Pascale Carayon, University of Wisconsin, continued on this theme, speaking to the multifaceted role of the scheduler. As Carayon put it, “They also have huge social organizational functions. Their role is a lot more than a formal role. There are a lot other informal roles… [and] it is really unclear whether providing different technology is something that is going to reduce or potentially increase visits in the clinic.”
David Andrews noted that from his standpoint as a patient with significant experiences with waits and scheduling, “How much of the issue is the wait, [and] how much is the communication about the wait?” He and several other commenters discussed the importance of turning time spent waiting into valuable time in which information is exchanged between the provider and patient. Ashley Benedict of the VA spoke to the potential value that could be added if IT systems could integrate patient appointment times with clinical needs, to identify and complete work that could be done prior to the patient–physician face-to-face.
The discussions of human factors and patient perspective were synthesized into closing remarks by Kristen Carmen of the American Institutes for Research, who noted that “efficiency and optimization is always from a perspective, purchaser’s perspective, payer’s perspective, patient’s perspective, and provider’s perspective. I think we need to do a much better job of making those differences in perspective or those commonalities in perspectives transparent.”
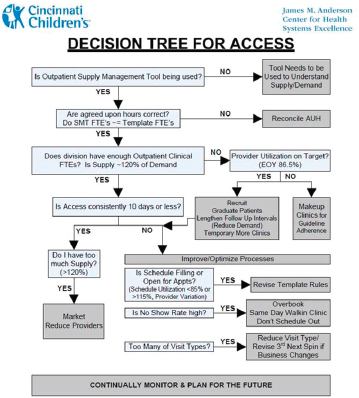
FIGURE 1 Cincinnati Children’s Hospital scheduling algorithm to effectively match supply and demand to improve access to care.
NOTES: AUH = agreed-upon hours; EOY = end of year; FTE = full-time equivalent; SMT = supply management tool.
Copies of this document may be distributed to any organization for the global purpose of improving child health. Examples of approved uses of this document include the following:
- copies may be provided to anyone involved in the organization’s process for developing and implementing improved scheduling and access
- the model may be adopted or adapted for use within the organization, provided that Cincinnati Children’s Hospital Medical Center receives appropriate attribution on all written or electronic documents; and
- copies may be provided to patients and the clinicians who manage their care.
Notification to Cincinnati Children’s at childrens-quality@cchmc.org when this document is being adopted, adapted, implemented, or hyperlinked to by your organization is appreciated. © 2014 Cincinnati Children’s Hospital Medical Center.
SOURCE: Cincinnati Children’s Hospital, as presented by David Krier and Terra Thompson on November 21, 2014.
A Roadmap for the Nation
William Pierskalla of the UCLA Anderson School of Management facilitated a discussion on developing a short-term roadmap for institutions to address scheduling issues and to begin transitioning to an optimal method of scheduling and access to care. He highlighted the major components of the care delivery process: the pre-visit period of scheduling and patient arrival to the care facility, the waiting period prior to connecting with the provider,
and the period in which care services are delivered. He emphasized that improving patient flow through these stages required continuous process improvement rather than addressing issues and increasing resources in each discrete period.
To kick off the audience participation portion of the workshop, Pierskalla asked where the roadmap begins. A range of ideas emerged. Both Kaplan and Andrews underscored the need to engage patients at the ground level of transformation. Michael Davies of the VA noted the importance of increased transparency and standardization of acceptable wait times used across the nation, in both public and private sectors. Jackie Griffin of the Department of Defense (DoD) advocated for increased flexibility in hospital operating procedures, and Michael Dinneen of the DoD re-emphasized the need to assess the entire value stream rather than individual parts.
Pierskalla guided the conversation from high-level comments on culture change to focus on the specific measures that health care institutions could implement to affect said change. Several participants considered the incorporation of a measure assessing the linkage between mortality and wait times. Teri Pipe of Arizona State University suggested that measures should focus on the patient and caregiver experience as well as the experiences of inter-professional and interdisciplinary teams in the hospital setting. Patricia Gabow, formerly of Denver Health, described the need to distinguish measures by application, on the individual or system level. Warren Sandberg cautioned against focusing on individual metrics given the complexity of the system, saying that by doing so, “we may actually sub-optimize the system.” Kaplan echoed this sentiment and described the approach at Virginia Mason, in which every employee is required to have a comprehensive understanding of the management system and its basic principles.
Technical Approaches to Wait Time Improvement
Thomas Nolan from the Institute for Healthcare Improvement framed the panel by acknowledging that other industries have had success with implementing technical approaches, using “scheduling as an intervention” to optimize customer satisfaction and reduce waste in systems. The presenters used their experiences working both in health care and other industries to detail the ways in which IT tools can be harnessed to implement systems changes to scheduling processes in the care delivery setting.
Wes Walker of Cerner described innovative health IT tools, such as mobile scheduling platforms and patient portals that are being implemented by individual organizations across the country that view access and scheduling improvement as a key component of achieving high-quality care. As he put it, “[The University of Missouri Health System] put the patient at the center, and they looked at the holistic process with the understanding and the idea that the appointment was a means to an end. The goal was the clinical interaction.”
Speaking from her expertise in operations research, Zelda Zabinsky of the University of Washington provided several anecdotes of the consequences related to a segmented approach to improving patient flow, thus emphasizing the importance of maintaining a systems view when tackling these issues. Determining the specific bottleneck in the system is difficult, said Zabinsky, describing the phenomenon: “You have a big balloon, and you squeeze one place, and it pops out another place.”
Judy Worth, of the Lean Transformations Group, LLC, provided strategies for creating sustainable organizational change across a value stream according to Lean principles (see Figure 2). Reflecting on the implementation of Lean principles in manufacturing operations, Worth highlighted the need to connect these principles to the institution’s broader purpose and goals, as was learned from the Toyota experience.
Several of the discussants raised the issue of an unevenly distributed workflow burden with the implementation of some of these IT tools, and stressed that the tools showing the most promise are those that are collaborative in nature. While agreeing that IT tools are adding value, Michael Harrison, from the Agency for Healthcare Research and Quality, noted, “You can get a really fantastic algorithm that is going to solve a specific problem, but it doesn’t generate capacity among the members of that system to deal with the next thing down the line, whether it is an unintended consequence or something else.”
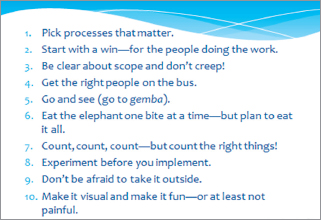
FIGURE 2 The Lean Enterprise Institute’s 10 Strategies for Organizational Change.
NOTE: Gemba = Japanese word for “the real place.”
SOURCE: Judy Worth of the Lean Transformations Group, LLC, as presented on November 21, 2014.
Best Practices for Health Care
Donald Berwick from the Institute for Healthcare Improvement reminded the workshop audience of the charge set by Kaplan at the beginning of the day to inform the committee on the best practices and strategic priorities that could be included in the report recommendations. He opened the final panel with a series of questions: “What did you hear that is cross-cutting and memorable? What are the implications of what we heard today for future steps to take? One of the things I am going to be thinking about and hope our panelists will comment on is: is there any way to accelerate the embrace of the sciences of systems in the kind of care we give?”
Maureen Bisognano of the Institute for Healthcare Improvement re-emphasized the need to redesign the care delivery system around the user, patients and caregivers. Christine Sinsky of the American Medical Association highlighted the discussion points surrounding balancing supply and demand from a systems view. Robert Dittus of Vanderbilt University reviewed the players and resources that health care organizations need in order to fully implement systems engineering methods. He advocated for more coordination among health care teams, and for redefining these teams to include industrial engineers, mathematicians, and most importantly, patients as equal contributors. Additionally, he spoke to the variation across the care continuum and recommended that systems be flexible, saying, “If your scheduling system doesn’t acknowledge the different settings that can be utilized, you are not going to have the right system.”
Kaplan closed the session by inviting the audience to view the workshop as a call to action. “We need to create a movement,” he said. “I think the trump card is really the patients and how we galvanize our communities around what is reasonable to expect from the health care system, and then, how do we make sure that we use the systems engineering approaches as well as the many other things that we have talked about to make that happen.” ![]()
DISCLAIMER: This workshop in brief has been prepared by Elizabeth Johnston and Katherine Burns, rapporteurs, as a factual summary of what occurred at the meeting. The statements made are those of the authors or individual meeting participants and do not necessarily represent the views of all meeting participants, the planning committee, or the National Academies.
REVIEWERS: To ensure that it meets institutional standards for quality and objectivity, this workshop in brief was reviewed by Brian Denton, University of Michigan; Michael Dinneen, U.S. Department of Defense; and Robert Dittus, Vanderbilt University Medical Center. Chelsea Frakes, Institute of Medicine, served as review coordinator.
SPONSORS: This workshop was supported by the Department of Veterans Affairs/Veterans Health Administration.
For additional information regarding the workshop, visit http://www.iom.edu/optimizingscheduling.
Copyright 2015 by the National Academy of Sciences. All rights reserved.
|
WORKSHOP IN BRIEF |
OF THE NATIONAL ACADEMIES Advising the nation • Improving health |
On November 21, 2014, the Institute of Medicine’s (IOM’s) Committee on Optimizing Scheduling in Health Care convened a public, one-day workshop titled “Engineering Optimal Health Care Scheduling.” Funded by the Department of Veterans Affairs (VA), the aim of the session was to explore appropriate standards for access, triage, and scheduling of health care services across the continuum of care to inform the work of the committee and to shape the content of their forthcoming consensus report.
As outlined in introductory comments by committee chair Gary Kaplan, CEO of Virginia Mason Health System, the workshop convened leading authorities on care delivery, operations management, systems engineering, and patient engagement and satisfaction. Kaplan discussed the potential role that systems engineering could play in driving improvement in health care. “How do we better bring together the systems engineering principles that have been so effective in so many industries and yet have gotten only very little traction in health care?” he asked. He said that applying systems thinking and intelligently deploying measurement and analysis could be transformative for the health care system by unlocking new potential pathways for change.
The workshop included four panels: current best practices, patient experiences and expectations, technical approaches to wait time improvement, and an overview of the day’s discussion. In addition, a working lunch session considered issues in identifying a toolkit for health systems to implement optimal scheduling practices. For each panel, a moderator and several speakers provided framing comments and presentations that then opened to general discussion.
This brief summary of the workshop captures the major topics and issues discussed over the course of the day that are most applicable to the Veterans Health Administration, and it is accompanied by a Workshop in Brief targeted at perspectives for the broader U.S. health care system. Statements, recommendations, and opinions expressed are those of individual presenters and participants and are not necessarily endorsed or verified by the Committee on Optimizing Scheduling in Health Care or the IOM, and they should not be construed as reflecting any group consensus.
Current VA Practices and Standards in Appointment Scheduling
Peter Pronovost of Johns Hopkins Medicine introduced the session on current practices and standards, saying that the controversy regarding VA wait times for available appointments brought to light needless suffering and the disrespect associated with poor management of scheduling and resources at the VA and in the health care system nationally. This session was an opportunity, he said, to hear stories told by organizations that were able to make meaningful improvements in this area. “Underlying the system changes are the stories that either propel us to new pinnacles or keep us pinned to our current performance,” he said.
Throughout the first panel discussion, speakers discussed the challenges, limitations, and opportunities for the VA in its efforts to improve scheduling. Mike Davies of the VA noted that the VA faces a variety of technical challenges. “The VA’s information system is 30 years old,” he said, and the VA has been asked to measure individual
patient waiting times, which is a complex and sophisticated function. David Krier of Cincinnati Children’s Hospital noted that the VA currently measures wait times, in the context of an appointment visit cycle time, as the time between when registration ends and when a clinician begins to document in the electronic record. As a result, he said, the VA has not yet been able to monitor how long patients wait in the exam room, or more generally, how much time may be wasted once a clinical encounter begins. He acknowledged that this challenge exists in the private sector as well. “I think that is what our biggest struggle is,” said Krier.
Patients and Families as Catalysts for Achieving Operational Excellence in Health Care
The second panel of the day focused on the perspectives, needs, and roles of patients in optimizing scheduling. Matt Puglisi, a veteran now working at Aptima, Inc., provided background on some of the specific challenges the VA faces in meeting patients’ expectations for timely care. “The VA system was not consciously designed,” he said, instead growing over time, beginning with the Civil War, in reaction to post-war needs for expanded health care resources for veterans. He noted that categorization and associated eligibility requirements for veterans contribute significantly to the complexity of connecting veterans with needed health care services at the VA. “The eligibility for an individual veteran depends. Did you serve during the war? Do you have a service-connected disability? How bad is that disability? That affects what care can be provided by the VA.” These decisions about eligibility are further complicated when patients are also eligible for Medicare and/or Medicaid or have private insurance.
Several commenters, including Ashley Benedict from the VA and Pascale Carayon from the University of Wisconsin, also discussed the significance of variations in patients’ perceptions of wait times. “The idea of perceived versus actual wait is not the same for every patient,” said Benedict. Additionally, Benedict noted a need for balancing measures for people’s perceptions. “From the IT component, if we could predict what patients needed and their appointments coming up, and I could get my lab work done, that might not be a waiting time for me because there is a value-added activity that is happening between now and being seen in my actual appointment.” Carayon and Puglisi discussed some of the potential limitations of measuring time alone in assessing waits, noting that measures of perceived wait times or of patients’ satisfaction with wait times could add critical additional meaning. “You may find that by talking a little to patients if you can spare the time, they may be able to withstand longer wait times and be as or more satisfied,” said Puglisi.
Optimization Strategies and Experiences in Health Care
Mark Hallett from ThedaCare Center for Healthcare Value discussed patient-centered scheduling and the practices to improve capacity of their system:
Our scheduling process actually begins with a single question when we get a patient calling on the phone. That question is: “Would you like to be seen today?” Recognizing that patients have different needs and different behaviors, and in fact, those behaviors, be it speed sensitive or relationship sensitive, aren’t static. They are dynamic.
The presenters from Cincinnati Children’s Hospital, Krier and Terra Thompson, acknowledged the similarities between their home organization and that of Hallett’s as adopters of systems-thinking to transform their systems and achieve high quality results. Yet they also cautioned that even once a system is optimized and performing at its peak capacity, it is still extremely complex and fragile and thus challenging to sustain. As a strategy for maintaining performance, Thompson highlighted the importance of leadership at various levels, stating the need to ensure that clinical leadership at the division level is engaged and aware of their role in the optimization strategies for the system (see Figure 1).
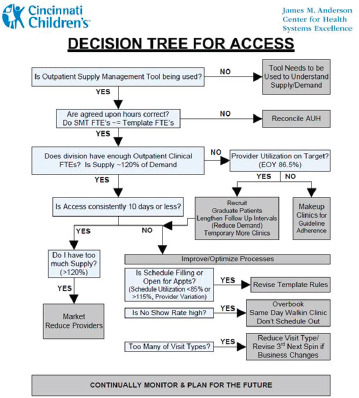
FIGURE 1 Cincinnati Children’s Hospital scheduling algorithm to effectively match supply and demand to improve access to care.
NOTES: AUH = agreed-upon hours; EOY = end of year; FTE = full-time equivalent; SMT = supply management tool.
Copies of this document may be distributed to any organization for the global purpose of improving child health. Examples of approved uses of this document include the following:
- copies may be provided to anyone involved in the organization’s process for developing and implementing improved scheduling and access
- the model may be adopted or adapted for use within the organization, provided that Cincinnati Children’s Hospital Medical Center receives appropriate attribution on all written or electronic documents; and
- copies may be provided to patients and the clinicians who manage their care.
Notification to Cincinnati Children’s at childrens-quality@cchmc.org when this document is being adopted, adapted, implemented, or hyperlinked to by your organization is appreciated. © 2014 Cincinnati Children’s Hospital Medical Center.
SOURCE: Cincinnati Children’s Hospital, as presented by David Krier and Terra Thompson on November 21, 2014.
Several speakers and commenters, including Patty Gabow (Denver Health), Krier, and Hallett, also discussed centralized scheduling as a necessary precondition for achieving a meaningful reduction in wait times, while ensuring that high-quality clinical decision making is applied in triage. Krier said that he would support separating scheduling and triage functions, such that scheduling becomes centralized and triage functions move closer to clinicians.
Andrew Gettinger of the Office of the National Coordinator for Health IT spoke of the operational details that contribute to optimizing scheduling, such as open access to appointment times and appointment pre-approvals. In discussing the ability to enhance capacity using advanced IT tools, such as virtual visits, Christine Sinsky of the American Medical Association cautioned that “they are an enhancement, but they are not necessarily the solution.”
Identifying a Structure for Change
In the closing session on common themes and best practices, participants including Davies, Pronovost, and Donald Berwick, Institute for Healthcare Improvement, commented on potential approaches to both improving scheduling at the VA and ensuring that scheduling is well managed throughout the care system. Berwick identified “two different voices in the room”—(1) the conversation focused specifically on the challenges surrounding scheduling mechanics and immediate strategies for improvement, and (2) the conversation focused on broader organizational changes possible by implementing and embracing systems engineering techniques.
Davies and Berwick discussed the potential benefits of identifying baselines and benchmarks for scheduling and wait-time performance, as a tool for both understanding the causes and consequences of wait times and for monitoring progress as interventions are undertaken at the VA. Davies said:
In the context of all of these forward thinking, clearly exciting and relevant comments, I would just ask you to think about the question of how do we ensure some floor, some standards, something that is a little deeper that would have given us some predictive [indicator] that this was going to happen.
Several discussants, including Benedict and Robert Dittus, Vanderbilt University, emphasized the importance of ensuring that systems engineering approaches are incorporated into the care delivery setting. Kaplan closed the session by reminding the audience that this issue is a national challenge. “We need to create a movement,” he said. “I think the trump card is really the patients and how we galvanize our communities around what is reasonable to expect from the health care system, and then, how do we make sure that we use the systems engineering approaches as well as the many other things that we have talked about to make that happen.” ![]()
DISCLAIMER: This workshop in brief has been prepared by Katherine Burns, Elizabeth Johnston, and Elizabeth Malphrus, rapporteurs, as a factual summary of what occurred at the meeting. The statements made are those of the authors or individual meeting participants and do not necessarily represent the views of all meeting participants, the planning committee, or the National Academies.
REVIEWERS: To ensure that it meets institutional standards for quality and objectivity, this workshop in brief was reviewed by Mark Hallett, ThedaCare; Christine Sinsky, American Medical Association; William W. Stead, Vanderbilt University; and Catherine Tantau, Tantau & Associates. Chelsea Frakes, Institute of Medicine, served as review coordinator.
SPONSORS: This workshop was supported by the Department of Veterans Affairs/Veterans Health Administration.
For additional information regarding the workshop, visit http://www.iom.edu/optimizingscheduling.
Copyright 2015 by the National Academy of Sciences.












