
4
Self-Report Measures and Symptom Validity Tests
Allegations of disability are sometimes made on the basis of self-report, with few, if any, medical signs or laboratory findings to substantiate such claims. Often in these cases a medical source or consultative examiner may corroborate a claimant’s history and allegations, finding them consistent with a medically determinable impairment that causes a particular level of functional limitation; however, the claim is still based primarily on self-report. Currently, such evidence may be deemed sufficient to grant disability benefits, albeit via a somewhat inconsistent process that varies from one state to another. A more systematic approach to assessing and verifying such claims would improve the consistency and reliability of the determination process in these cases.
To receive benefits, applicants must prove the existence of a medically determinable physical or mental impairment and associated functional limitations that result in an inability to engage in any substantial gainful activity. The U.S. Social Security Administration (SSA) (n.d.-b) defines a medically determinable impairment as
an impairment that results from anatomical, physiological, or psychological abnormalities which can be shown by medically acceptable clinical and laboratory diagnostic techniques … [and] must be established by medical evidence consisting of signs, symptoms, and laboratory findings—not only by the individual’s statement of symptoms.
Following establishment of a medically determinable impairment, the overall degree of functional limitation is evaluated based on the extent to which the applicant’s impairment interferes with his or her “ability to
function independently, appropriately, effectively, and on a sustained basis” (20 CFR § 416.920a). SSA definitions of symptoms, signs, and laboratory findings are provided in Box 4-1.
The current chapter focuses on the potential role of non-cognitive psychological measures, often characterized as self-report measures, in SSA disability determinations. It begins with an examination of potential domains for which psychological self-report measures may provide information to assist in identifying a claimant’s medically determinable impairment and determining the level of functional limitation. Following this, procedures and qualifications for administering tests and interpreting test results are presented. Finally, the chapter concludes with an examination of related symptom validity tests (SVTs).
ASSESSING SELF-REPORT OF SYMPTOMS
For claims based entirely on self-report, it is important to use a systematic method for identifying and documenting a medically determinable impairment and assessing the severity of associated functional limitations. A variety of standardized self-report measures exist that could further systematize SSA’s disability determination process. Before delving into such measures, it is important to briefly address the distinction between self-report of
BOX 4-1
SSA Definitions of Symptoms, Signs, and Laboratory Findings
Symptoms: Your own description of your physical or mental impairment.
Signs: Anatomical, physiological, or psychological abnormalities that can be observed, apart from your statements (symptoms). Signs must be shown by medically acceptable clinical diagnostic techniques. Psychiatric signs are medically demonstrable phenomena that indicate specific psychological abnormalities, e.g., abnormalities of behavior, mood, thought, memory, orientation, development, or perception. They must also be shown by observable facts that can be medically described and evaluated.
Laboratory findings: Anatomical, physiological, or psychological phenomena that can be shown by the use of medically acceptable laboratory diagnostic techniques. Some of these diagnostic techniques include chemical tests, electrophysiological studies (electrocardiogram, electroencephalogram, etc.), roentgenological studies (X-rays), and psychological tests.
SOURCE: 20 CFR § 404.1528.
symptoms and self-report measures. As noted above, SSA defines symptoms as “the claimant’s own description of [his or her] physical or mental impairment, [which] alone are not enough to establish that there is a physical or mental impairment” (20 CFR § 404.1528). In some cases, such as with children, symptoms may be reported by a third party, for example, a parent or a teacher. The committee refers to this as self-report of symptoms. Alternatively, there exist standardized instruments that rely on self-report (for example, of symptoms, behaviors, personality characteristics and/or traits, interests, values, and attitudes) with population-based normative data that allow the examiner to compare an individual’s reported behaviors or symptoms with an appropriate comparison group (e.g., those of the same age group, sex, education level, and/or race/ethnicity). According to SSA regulations, such instruments may be considered medically acceptable laboratory diagnostic techniques, and thus provide signs and laboratory findings that corroborate the claimant’s self-report of symptoms. The committee refers to these instruments as self-report measures.
Among these self-report measures are those that traditionally have been referred to as psychological tests, such as personality, multiscale, or single syndrome inventories and standardized psychiatric diagnostic interviews. These measures generally assess non-cognitive psychological complaints, and are therefore referred to as non-cognitive measures.1 However, it is also important to note that some standardized self-report measures that might be useful to SSA in such cases are not considered psychological tests or measures. Examples may include standardized measures of pain, fatigue, sleep, or adaptive living. Some of these may contain internal validity measures, and indeed may be useful to SSA in the disability determination process; however, these measures are considered outside the scope of the committee and this report. Figure 4-1 delineates between psychological (or non-cognitive) self-report measures and nonpsychological self-report measures.
PSYCHOLOGICAL SELF-REPORT MEASURES AND DISABILITY EVALUATION
As discussed in Chapter 3, psychological assessment generally begins with a referral question followed by a clinical interview, the purpose of which is to explore presenting complaints (self-report of symptoms) and develop an understanding of the case, which may include a history of symptom development and an assessment of current status and impact on daily functioning. From this understanding, the next steps typically include the
_____________
1 Note that when the committee refers to non-cognitive measures, it is referring to standardized psychological self-report measures.
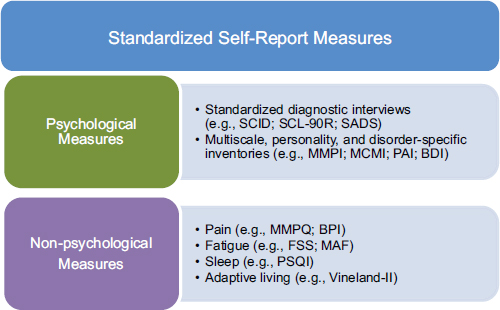
FIGURE 4-1 Psychological versus nonpsychological self-report measures.
NOTE: BDI = Beck Depression Inventory; BPI = Brief Pain Inventory; FSS = Fatigue Severity Scale; MAF = Multidimensional Assessment of Fatigue; MCMI = Millon Clinical Multiaxial Inventory; MMPI = Minnesota Multiphasic Personality Inventory; MMPQ = McGill-Melzack Pain Questionnaire; PAI = Personality Assessment Inventory; PSQI = Pittsburgh Sleep Quality Index; SADS = Schedule for Affective Disorders and Schizophrenia; SCID = Structured Clinical Interview for DSM Disorders; SCL-90R = Symptom Checklist 90 Revised; Vineland-II = Vineland Adaptive Behavior Scales.
identification of hypotheses to be examined and postulation of methods to assess these hypotheses. The primary goal of such methods is to provide corroborative evidence for the presenting complaints and their integration into case understanding. This may include the longitudinal history (which may provide evidence of internal consistency, such as refractoriness to treatment, chronicity, and severity); objective medical evaluation; direct observation of the claimant; and information from third parties such as family members, employers, and teachers. The use of non-cognitive measures may be another source of corroborative information, with the potential to inform the existence of a medically determinable impairment and/ or functional limitations. Because of the potential for gain associated with disability determinations, a systematic method for assessing the validity of claims based primarily on self-report would prove valuable. In some cases, the use of non-cognitive psychological testing may contribute to achieving these goals.
Areas of Symptom Complaint
In the realm of disability evaluation, the committee identified two primary areas of impairment in which psychological self-report measures may prove beneficial to SSA disability determinations: mental disorders and somatic symptoms disproportionate to demonstrable medical morbidity. Each of these are discussed in turn, followed by a discussion on the ability of psychological self-report measures to provide useful information in confirming a medically determinable impairment and assessing functional capacity in these areas. A variety of non-cognitive measures, such as multiscale personality measures, disorder-specific inventories, and standardized diagnostic interviews, are provided as illustrative examples, and not an endorsement of any specific test.
Mental Disorders
Within its mental health listings, SSA (n.d.-a) identifies nine diagnostic categories (see Chapter 3, Table 1). Of these nine, the committee identified five categories for which non-cognitive measures may provide useful information: (1) schizophrenic, paranoid, and other psychotic disorders; (2) affective disorders; (3) anxiety-related disorders; (4) personality disorders; and (5) somatoform disorders.2Box 4-2 contains the SSA descriptions of each of the first four mental disorders categories.
These categories of mental disorders are well-established psychiatric diagnoses with distinct diagnostic criteria. In clinical settings, diagnosis in these categories often relies on self-report of symptoms, which are then weighed against criteria in the Diagnostic and Statistical Manual of the American Psychiatric Association (DSM-5). However, the method for assessing symptom report may vary, from a simple, unstructured clinical interview to more systematic approaches, such as the use of standardized psychiatric diagnostic schedules and interviews or formal psychological self-report measures. The use of such systematic approaches may help corroborate and validate a patient’s symptom report.
There are also 11 mental disorder diagnostic categories listed by SSA specifically for children. The structure and organization of these categories is parallel to mental disorder listings shown for adults. The categories that contain conditions typically first diagnosed in childhood contain intellectual disability, autistic disorder and other pervasive developmental disorders, and attention deficit hyperactivity disorder. In addition, conduct disorder and oppositional defiant disorder are contained in the SSA listing for personality disorders.
_____________
2 Although somatoform disorders are included in the SSA mental health listings, the committee focuses on these in the next section on disproportionate somatic symptoms, alongside multisystem illnesses and chronic idiopathic pain conditions.
BOX 4-2
SSA Definitions of Relevant Mental Disorders
| Schizophrenic, paranoid, and other psychotic disorders | Characterized by the onset of psychotic features with deterioration from a previous level of functioning. |
| Affective disorders | Characterized by a disturbance of mood, accompanied by a full or a partial manic or depressive syndrome. Mood refers to a prolonged emotion that colors the whole psychic life; it generally involves either depression or elation. |
| Anxiety-related disorders | In these disorders anxiety is either the predominant disturbance or it is experienced if the individual attempts to master symptoms; for example, confronting the dreaded object or situation in a phobic disorder or resisting the obsessions or compulsions in obsessive compulsive disorders. |
| Personality disorders | A personality disorder exists when personality traits are inflexible and maladaptive and cause either significant impairment in social or occupational functioning or subjective distress. Characteristic features are typical of the individual’s long-term functioning and are not limited to discrete episodes of illness. |
SOURCE: SSA, n.d.-a.
Similar to those listed for adults, mental disorders present in childhood are well-established conditions listed in the DSM-5 (American Psychiatric Association, 2013). These conditions are diagnosed in clinical settings based on report of symptoms, often by parents or others who interact with the child (e.g., teachers), as well as behavioral observations and the completion of standardized or systematic approaches, such as questionnaires, tests, and age-appropriate self-report instruments. Many conditions diagnosed in children are reevaluated when a child reaches majority age.
Disproportionate Somatic Symptoms
The committee identified three distinct groups of applicants seeking disability compensation for somatic symptoms unaccompanied by demonstrable
anatomical, biochemical, or physiological abnormalities: somatoform disorders (recently termed somatic symptom disorders in the DSM-5), multisystem illnesses, and chronic idiopathic pain conditions. Brief descriptions of these disorders are provided in Box 4-3.
Somatoform (or somatic symptom) disorders are diagnosable psychiatric disorders with distinct, well-elaborated diagnostic criteria (American Psychiatric Association, 2013); as such, they are among the listed mental disorders that are eligible for SSA disability compensation. These disorders appear to be medical disorders because their clinical presentation is characterized by somatic or physical symptoms, but on further examination they are best understood and treated as psychiatric conditions. They include somatic symptom disorder (formerly termed somatization disorder), hypochondriasis or illness anxiety disorder, and conversion disorder. These diagnoses require clinically significant and persistent bodily symptoms and a substantial degree of associated distress and functional impairment.
Multisystem illnesses (also termed functional somatic syndromes) share a common, nonspecific symptom pool, that includes fatigue, weakness, lightheadedness, dizziness, sleep difficulties, headache, problems of memory and attention, blurry vision, gastrointestinal complaints (e.g., heartburn,
BOX 4-3
Definitions of Relevant Disorders with Disproportionate Somatic Symptoms
| Somatoform disordersa | Physical symptoms for which there are no demonstrable organic findings or known physiological mechanisms. |
| Multisystem illnessesb | Characterized by multiple, widespread, nonspecific, often diffuse symptoms that involve several different organ systems and anatomical locations, for which no consistent biochemical, anatomical, or physiological abnormality can be demonstrated. Hence the medical and psychiatric status of these conditions remains unclear. |
| Chronic idiopathic pain conditionsc | The only or predominant symptom is bodily pain, most commonly musculoskeletal pain, that is disproportionate to (in completely explained by) tissue injury or disease. |
_____________
a American Psychiatric Association, 2013.
b Barsky and Borus, 1999; Henningsen et al., 2007.
c Vranceanu et al., 2009.
bloating), palpitations, shortness of breath, sore throats, and urinary frequency. Chronic fatigue syndrome, repetitive strain injury, toxic building syndrome, multiple chemical sensitivity, and chronic Lyme disease are among these conditions. Other apparently related illnesses include interstitial cystitis, chronic whiplash (cervical hyperextension), multiple food allergies, and hypoglycemia. These conditions are considered together as a group because they appear to share a number of characteristics: the same individual over time is frequently diagnosed with more than one of these conditions; they share extensive phenomenological overlap and common epidemiological characteristics; there is a higher than expected prevalence of psychiatric comorbidity; and they are marked by a refractoriness to the usual symptomatic medical treatments and standard palliative measures (Barsky and Borus, 1999; Henningsen et al., 2007).
The only or predominant symptom of chronic idiopathic pain disorders is bodily pain, most commonly musculoskeletal pain, that is disproportionate to (incompletely explained by) tissue injury or disease (Vranceanu et al., 2009). These conditions account for a large fraction of all disability payments; musculoskeletal pain accounts for 25 to 35 percent of adult disability claims. Low back pain is one of the most common single sources of disability compensation, but other pain conditions in which pain may be disproportionate to medical findings include fibromyalgia, complex regional pain syndrome, carpal tunnel syndrome, and temporomandibular joint disorder. There is often an acute precipitating injury or illness or procedure, after which the individual experiences chronic, intense, and severe pain that impairs their physical and role functioning.
Confirming the Existence of a Disability
As noted above, a disability determination requires a medically determinable impairment that affects an applicant’s ability to function in a work setting. Such a determination must be confirmed with observable signs and laboratory findings. Included among acceptable laboratory findings are psychological tests (20 CFR § 404.1528).
Standardized non-cognitive measures are developed, interpreted, and evaluated in accordance with psychometrics, the scientific study of tests and measures used to assess variability in behavior and link such variability to psychological phenomena. Psychometrics also considers measurement theory (e.g., classical test theory and item response theory) and its applicability to measures. In evaluating the quality of psychological measures, psychometrics is primarily concerned with test reliability (i.e., consistency) and validity (i.e., accuracy).3 Therefore, standardized psychological self-report
_____________
3 See Chapter 3 for an in-depth discussion on psychometrics.
measures that demonstrate good psychometric properties can provide scientific laboratory findings that corroborate self-report of psychological symptoms.
The systematic use of standardized psychological self-report measures can help identify and document the presence and severity of a medically determinable impairment in each of the areas outlined above. Broad personality and multiscale inventories can provide medical evidence of a wide variety of mental disorders. The most prominent example of such measures is the Minnesota Multiphasic Personality Inventory (MMPI) (Hathaway and McKinley, 1940, 1943), along with more recent editions. The instrument was originally created more than 70 years ago and has been through two normative revisions. The MMPI, MMPI-2 (Butcher et al., 1989), and MMPI-2RF (Ben-Porath et al., 2008) all consist of a self-report inventory of symptoms and personal characteristics. Items are statements for which the test-taker responds in a dichotomous fashion (i.e., True/False) as the content applies to his or her own functioning. The current version of this assessment, the MMPI-2RF, comprises 338 items that are part of 51 different scales and was normed on a U.S. population (n = 2,227) of men and women ages 18–80. Other widely used multiscale inventories include the Millon Clinical Multiaxial Inventory (MCMI-III) (Millon et al., 2009) and the Personality Assessment Inventory (PAI) (Morey, 2007). The MCMI-III is a 175-item test normed largely on individuals seeking psychiatric services. The PAI contains 344 items and was developed on a U.S. normative sample of 1,000 adults matched to the census; additionally, 1,265 patients and 1,051 college students completed the test in the standardization process.
Standardized psychiatric diagnostic schedules, interviews, and inventories may also provide scientific medical findings across a broad range of psychiatric symptoms and diagnoses. The Symptom Check-List 90 Revised (SCL-90R) (Derogatis, 1994), a broad-based measure designed for individuals 13 years and older, contains a list of symptoms commonly associated with psychological difficulties and psychiatric disorders. Written at a sixth-grade level, the test measures nine primary symptom dimensions (i.e., somatization, obsessive-compulsive disorder, interpersonal sensitivity, depression, anxiety, hostility, phobic anxiety, paranoid ideation, and psychoticism), assessing symptom presence and frequency and severity across a 1-week period of time. There is also a 53-item version of the scale, the Brief Symptom Inventory (BSI) (Derogatis and Spencer, 1993). Designed specifically to measure subjective symptom report, the SCL-90R has separate norms for nonpatient adults, adult psychiatric outpatients, adult psychiatric inpatients, and nonpatient adolescents. Some reviewers suggest that this instrument is best used to screen for global psychological distress, as the individual symptom dimensions have not always been identified in studies examining the psychometric properties of the scale. Another broad
symptom inventory, the Patient Health Questionnaire (PHQ) (Spitzer et al., 1999), was developed for use in primary care settings and normed against this population. From the original test, scales to measure symptoms of depression (PHQ-9), anxiety (GAD-7), and somatic symptom severity (PHQ-15) have been constructed, along with a derivate scale, the PHQ-SADS that measures convergence of psychiatric symptoms often seen in primary care patients: depression, anxiety, and somatic complaints.
Many disorder-specific scales, such as the Beck Depression Inventory, second edition (Beck et al., 1996), Hamilton Depression Rating Scale (Hamilton, 1980), Beck Anxiety Inventory (Beck and Steer, 1993), and PTSD (posttraumatic stress disorder) Checklist (Weathers et al., 1994) may also provide medical evidence to corroborate patients’ identification and report of symptoms.
Confirming the diagnosis of disproportionate somatic symptoms may be more difficult, as the first step involves ruling out the presence of demonstrable anatomical, biochemical, or physiological abnormalities as the sole cause for symptom presentation and severity. Note that this does not rule out the existence of such abnormalities, but that reported symptom severity is disproportionate to the diagnosis. Additionally, the lack of a medical explanation does not automatically equal a psychiatric diagnosis (American Psychiatric Association, 2013). There are a variety of self-report questionnaires to assess somatization and somatoform disorders, which examine the number, nature, intensity, persistence, and severity of physical symptoms. These instruments include the PHQ-15, the somatization subscale of the SCL-90R, the Somatic Symptom Inventory (SSI), and the MMPI-2-RF. There are also several structured diagnostic interviews containing modules for diagnosing somatoform disorders, including the Composite International Diagnostic Interview (CIDI) (WHO, 1993), the Structured Clinical Interview for DSM (SCID) (First et al., 2012; Gibbon et al., 1997), the Mini International Neuropsychiatric Interview (MINI) (Sheehan et al., 1998), and the Schedule for Clinical Assessment in Neuropsychiatry (SCAN) (Wing et al., 1990).
There are a great many self-report inventories for assessing the severity, character, location, and chronicity of pain; the nonpsychological nature of such measures place them outside of the committee’s scope. However, there are non-cognitive measures that are used to identify and assess psychological factors related to pain, such as the Pain Patient Profile (P-3) (Tollison and Langley, 1995), which comprises three clinical scales measuring depression, anxiety, and somatization.
The second criterion in disability determinations is the impact of the medically determinable impairment on the applicant’s ability to function in a work setting, what SSA refers to as the Paragraph B criteria. In the realm of mental disorders, SSA currently assesses functioning in four categories:
(1) activities of daily living (ADLs); (2) social functioning; (3) concentration, persistence, or pace; and (4) episodes of decompensation. However, SSA (2010) published a Notice of Proposed Rulemaking (NPRM)4 for its mental disorders listings, which among other changes, would alter the functional categories on which disability determinations would be based, increasing focus on the relation of functioning to the work setting. Proposed functional domains in the NPRM are the abilities to (1) understand, remember, and apply information; (2) interact with others; (3) concentrate, persist, and maintain pace; and (4) manage oneself.5 Definitions of each of these domains are presented in Box 4-4. With SSA’s move in this direction and the greater focus on functional abilities as they relate to work, the committee will examine the relevance of psychological self-report measures to the proposed functional domains.
Although non-cognitive assessments do not provide direct evidence of functional capacity, information obtained from these measures allows for the corroboration of symptoms as presented, which can lead to greater diagnostic accuracy. For example, self-report instruments allow for a standardized method of obtaining information that is normed against other clinical and nonclinical groups, adding to the ability of a clinician to offer accurate diagnoses. In addition, some of these instruments have validity scales, which measure test-taking strategies, as discussed in detail below. Understanding these presentation approaches (i.e., over- or underreporting of symptoms) is helpful in identifying conditions accurately. From obtaining an accurate diagnosis, the ability to generate more accurate prognostic indicators increases and thereby provides greater ability to discern the chronicity of conditions presented.
ADMINISTRATION AND INTERPRETATION OF NON-COGNITIVE PSYCHOLOGICAL MEASURES
One of the most important aspects of administration of non-cognitive measures is selection of the appropriate measures to be administered. That
_____________
4 Public comments are still under review and a final rule has yet to be published as of the publication of this report.
5 These proposed domains align closely with the recommendations of the Mental Cognitive Subcommittee of the Occupational Information Development Advisory Panel (OIDAP), which conceptualized psychological abilities essential to work in four categories: (1) neurocognitive functioning, (2) initiative and persistence, (3) interpersonal functioning, and (4) self-management. Note that with this first category, neurocognitive functioning, the Mental Cognitive Subcommittee’s recommendation goes into greater detail; this will be discussed further in the following chapter, which focuses on cognitive testing. The Mental Cognitive Subcommittee was assembled to advise OIDAP about what psychological abilities of disability applicants should be included in the Content Model and Classification Recommendations made to SSA.
BOX 4-4
SSA Proposed Functional Domains
| Understand, remember, and apply information | The ability to acquire, retain, integrate, access, and use information to perform work activities. You use this mental ability when, for example, you follow instructions, provide explanations, and identify and solve problems. |
| Interact with others | The ability to relate to and work with supervisors, co-workers, and the public. You use this mental ability when, for example, you cooperate, handle conflicts, and respond to requests, suggestions, and criticism. |
| Concentrate, persist, and maintain pace | The ability to focus attention on work activities and to stay on task at a sustained rate. You use this mental ability when, for example, you concentrate, avoid distractions, initiate and complete activities, perform tasks at an appropriate and consistent speed, and sustain an ordinary routine. |
| Manage oneself | The ability to regulate your emotions, control your behavior, and maintain your well-being in a work setting. You use this mental ability when, for example, you cope with your frustration and stress, respond to demands and changes in your environment, protect yourself from harm and exploitation by others, inhibit inappropriate actions, take your medications, and maintain your physical health, hygiene, and grooming. |
SOURCE: SSA, 2010.
is, selection of measures is dependent on examination of the normative data collected with each measure and consideration of the population on which the test was normed. Normative data are typically gathered on generally healthy individuals who are free from significant mental impairments. Data are generally gathered on samples that reflect the broad demographic characteristics of the United States including factors such as age, gender, and educational status. There are some measures that also provide specific comparison data on the basis of race and ethnicity.
As discussed in detail in Chapter 3, the use of psychological testing requires the examiner to follow standardized procedures for the
administration of the tests. Administration instructions for non-cognitive measures are contained in the respective test manuals. Although unique to each test, an overarching concern is the selection of a test for which there have been procedures developed for the characteristics of the person being examined. For example, the majority of non-cognitive measures require that the individual be able to complete a self-report inventory, a task that requires reading and responding to a list of dichotomous (e.g., True/False) or Likert scale items. To complete a task like this, one must have the ability to attend, read, comprehend, and respond to a series of items. For example, the MMPI-2-RF was developed with a fifth-grade reading level, while the MCMI-3 and the PAI both require an eighth-grade reading level. Although some tests have alternative methods of administration (e.g., standardized audio tape administration, computerized administration), ensuring that the examinee is able to understand information at a content level equivalent to the items on the test and has the capacity to attend to and respond to items is generally recommended. In addition, the capacity of the individual to work on an activity with similar characteristics for the development of normative data must be considered. Additionally, consideration of the examinee’s language and administration of a test that has been translated and normed within the language is generally recommended.
SSA requires psychological testing be “individually administered by a qualified specialist,” defining qualified as “currently licensed or certified in the state to administer, score, and interpret psychological tests and have the training and experience to perform the test” (SSA, n.d.-a). It is important to note here, as discussed in Chapter 3, the different qualification levels that may be necessary for administration and interpretation. It is common practice for psychometrists or technicians with specialized training to administer and score psychological tests, under the close supervision and direction of doctoral-level clinical psychologists. Interpretation of testing results requires a higher degree of clinical training than administration alone. Most psychological tests require interpretation by doctoral-level psychologists with a high level of expertise in psychometric test administration and interpretation.6 Threats to the validity of any psychological measure of a self-report nature oblige the test interpreter to understand the test and principles of test construction. In fact, interpreting tests results without such knowledge would violate the ethics code established for the profession of psychology (APA, 2010). Finally, it is important for the person interpreting the test results to address in the assessment report the reliability and validity of test scores and test norms relative to the individual being assessed.
_____________
6 These are commonly referred to as level C tests. Some tests have less stringent qualifications (level B) or no special qualifications (level A) necessary for purchase, administration, and interpretation. See Chapter 3 for additional information on different qualification levels.
ASSESSING THE VALIDITY OF NON-COGNITIVE SYMPTOM REPORT
Because much of psychological assessment relies heavily on self-report, assessing the accuracy of symptomatic complaint, or symptom validity, is critical. Symptom validity may be assessed in a number of ways. For example, an examinee’s self-report may be evaluated alongside data from a number of outside sources, such as behavioral observations, interviews with corroborative sources (e.g., family members, friends, teachers), and review of historical records (e.g., medical, educational, occupational, legal), or a formal analysis of internal data consistency. Symptomatic complaint may also be considered against typical diagnostic considerations, such as onset, symptom presentation, course, and response to treatment (Heilbronner et al., 2009). And, as presented in this chapter, formal non-cognitive psychological testing can provide scientific evidence that may support a patient’s self-report; however, as these measures also rely on self-report, assessing their validity is necessary. For this reason, formal SVTs exist to objectively assess the validity of data obtained during psychological assessment.
The initial step in interpreting results on self-report measures or questionnaires is to examine protocol validity. Multiple threats to validity are possible on most self-report measures. These threats include item responses that are not content based, such as omissions of items, provision of more than one response per item, or random responding. Such response styles may occur for a variety of reasons, for example, limited ability to read and process information, random human error (e.g., mismarking the answer sheet), or confusion or thought disorganization. Alternatively, invalid item responding may be content based, depending on the test-taker’s motivations. While unintentional random response may be due to confusion and thought disorganization, content-based response patterns are thought to be due to defensiveness or other characteristics on the part of the test-taker. Content-based response threats occur when the test-taker intentionally skews his or her approach to responding to items and presents an impression that may or may not be convergent with his or her true characteristics. Such a response style may include exaggeration by intentionally overreporting symptoms, which may occur in settings where there are benefits to being seen as impaired. For this reason, an examination of the measure’s protocol validity scales is often undertaken.
Many of the self-report measures discussed in this chapter contain formal measures of the credibility and consistency of examinee response. These SVTs are measures used to assess whether an examinee is providing an accurate or consistent report of his or her actual symptom experience (Larrabee, 2014). Such tests have recently been distinguished from performance validity tests (PVTs) (Bigler, 2012; Larrabee, 2012; Van Dyke et al.,
2013), which assess whether a test-taker is attempting to perform at a level consistent with his or her actual abilities and generally focus on measures of cognition; such tests will be examined in Chapter 5. SVTs are constructed to assess the accuracy of the test-taker’s responses on non-cognitive measures. Ultimately, such tests provide information on the interpretability and usefulness of results obtained from psychological tests and measures.
SVTs use a variety of approaches to examine response patterns that affect the accuracy of self-report on non-cognitive measures, which generally fall into three broad categories: consistency of response, negative self-presentation, and positive self-presentation. Consistency of response generally refers to whether a test-taker responds in a fixed or a random fashion or answers similar pairs of items in the same way. SVTs assess negative self-presentation in a variety of ways. Often, test-takers are presented with questions about infrequent or unlikely behaviors or symptoms; SVTs look for patterns of overreporting or amplification on these items, as compared to some population (e.g., general, psychiatric for mental complaints, medical patients for somatic complaints). For example, these measures generally contain items to which an individual is asked to respond with respect to concerns or symptoms, such as, “I have difficulty remembering what I had for breakfast” or “I see things around me that others do not see.” There are diagnostic conditions for which an endorsement of either of these individual items would be appropriate. However, many scales use items that are conceptually divergent, minimizing the likelihood of multiple items being endorsed, even if a diagnosis is present. Positive self-presentation is assessed in a similar fashion, but generally examines underreporting or minimization of symptoms or difficulties in an attempt to assert better psychological adjustment. An example of an item in this category might be “I never missed a day of school due to being ill.” While possible, the likelihood of positively endorsing multiple items when the scale consists of low base-rate behaviors is not high.
Scores on SVTs are typically generated by a summation of items and conversion to generate a standardized total score. Total scores are then compared to established cut-off scores, based on normative data on the scale. Norms may be based on nationally representative samples or sub-populations of relevance to the particular patient concern. For example, the MMPI-2-RF contains a validity scale that compares reports of emotional distress and psychiatric illness with psychiatric populations (i.e., Infrequent Psychopathology Responses [Fp-r]) and another that compares reporting of somatic complaints with medical patient populations (i.e., Infrequent Somatic Responses [Fs]). Norms may also include specific diagnostic groups that illuminate particular profiles on the test that may be indicative of a particular diagnosis. Cut-off scores are established to identify the presence of a response set that is either incongruent with known diagnoses or suggestive
of responding employing an alternative response set (e.g., overendorsement of symptoms). Such response sets are commonly seen as invalid and dependent on the test. The scale(s) are interpreted using clinical judgment by the examiner taking into consideration the referral questions, history of the examinee, and context of the evaluation.
Types of SVTs
Many SVTs are scales within larger personality or multiscale inventories assessing test-taker response styles used in completing the battery. These scales may be designed as such and embedded or later derived from existing items and scales based on typical response patterns, including those of specific populations. For example, each of the personality measures discussed earlier in this chapter (i.e., MMPI-2-RF, MCMI-III, and PAI) contains validity scales that examine consistency of response, negative self-presentation, and positive self-presentation to varying degrees. Box 4-5 lists the negative self-presentation SVTs included in each of these measures.
Though fewer in number, stand-alone SVTs also exist to assess potential exaggeration or feigning of psychological and neuropsychological symptoms. These include a number of structured interviews, such as the Structured Interview of Reported Symptoms (Rogers et al., 1992), the Structured Inventory of Malingered Symptomatology (Widows and Smith, 2005), and the Miller Forensic Assessment of Symptom Test (Miller, 2001). Like the embedded/derived measures, these SVTs examine accuracy of symptom report in a variety of ways. As this is their sole purpose, they are often used in conjunction with other measures that do not contain tests of validity. Box 4-6 lists the scales related to negative self-presentation in stand-alone SVTs.
Symptom Validity and the Disability Determination Process
When an applicant’s medical record is based primarily on self-report, assessment of symptom validity helps the evaluator assess the accuracy of an individual’s self-report of behavior, experiences, or symptoms. For this reason, it is important to include an assessment of symptom validity in the medical evidence of record. Such assessment may include the analysis of internal data consistency, examination of corroborative evidence, and formal SVTs.
There has been strong advocacy for the assessment of symptom validity—including the use of SVTs when administering non-cognitive measures—in forensic contexts in which examinees may be more likely to exaggerate symptoms. Organizations such as the Association for Scientific Advancement in Psychological Injury and Law (ASAPIL) (Bush et al.,
BOX 4-5
Embedded/Derived SVTs for Negative Self-Presentation
| MMPI-2-RFa | |
| Infrequent Responses (F-r) | Overreporting across psychological, cognitive, and somatic dimensions (as compared with general population) |
| Infrequent Psychopathology Responses (Fp-r) | Overreporting of emotional distress and psychiatric illness (as compared with psychiatric populations) |
| Infrequent Somatic Responses (Fs) | Overreporting of somatic complaints (as compared with medical patient populations) |
| Symptom Validity (FBS-r) | Overreporting of somatic and cognitive complaints |
| Response Bias (RBS) | Overreporting of memory complaints |
| Henry-Heilbronner Indexb | Physical symptom exaggeration (empirically derived from existing scales; for use with personal injury litigants and disability claimants) |
| Malingered Mood Disorder Scalec | Exaggeration of emotional disturbance (empirically derived from existing scales; for use with personal injury litigants and disability claimants) |
| MCMI-IIId | |
| Validity (V) | Improbable symptoms; may measure confusion, difficulties reading and understanding items, or responding in a random fashion |
| Disclosure (X) | Acknowledgment of difficulties and willingness to present with symptoms |
| Debasement (Z) | Tendency to present symptoms in an accentuated fashion |
| PAIe | |
| Infrequency (INF) | Statistically unlikely response patterns in items that have low rates of endorsement and high rates of endorsement |
| Negative Impression (NIM) | Rare symptoms and those that are not reported by many respondents |
| Malingering Index (MAL) | Unlikely patterns; features that are more likely to be found in persons simulating mental disorders than in clinical patients |
| Rogers Discriminant Function (RDF) | A statistically determined method that distinguishes simulators from those who were responding honestly |
_____________
a Ben-Porath et al., 2008.
b Henry et al., 2013.
c Henry et al., 2008.
d Millon et al., 2009.
e Morey, 2007.
BOX 4-6
Stand-Alone SVTs for Negative Self-Presentation
The 172-item Structured Interview of Reported Symptoms (SIRS-2)a evaluates feigning of psychiatric symptoms and deliberate distortions (e.g., exaggeration of symptom severity) in the self-report of symptoms. The inventory comprises a number of scales that produce information on how the examinee may distort his or her symptoms:
- Rare Symptoms (RS)
- Symptom Combinations (SC)
- Improbable and Absurd Symptoms (IA)
- Blatant Symptoms (BL)
- Subtle Symptoms (SU)
- Selectivity of Symptoms (SEL)
- Severity of Symptoms (SEV)
- Reported versus Observed symptoms (RO)
The 75-item Structured Inventory of Malingered Symptomatology (SIMS)b is a true/false screening instrument that assesses for both malingered psychopathology and neuropsychological symptoms. The inventory comprises five scale domains as well as an overall score for probable malingering (i.e., total score):
- Psychosis (P)
- Neurologic Impairment (NI)
- Amnestic Disorders (AM)
- Low Intelligence (LI)
- Affective Disorders (AF)
The 25-item Miller Forensic Assessment of Symptoms Test (M-FAST)c is a screening interview used to provide preliminary information regarding the possibility that an examinee is feigning psychopathology. The interview comprises seven scales corresponding to response styles and strategies related to feigning:
- Reported Versus Observed Symptoms
- Extreme Symptomatology
- Rare Combinations
- Unusual Hallucinations
- Unusual Symptom Course
- Negative Image
- Suggestibility
_____________
a Rogers et al., 1992.
b Widows and Smith, 2005.
c Miller, 2001.
2014), the American Academy of Clinical Neuropsychology (AACN) (Heilbronner et al., 2009), and the National Academy of Neuropsychology (NAN) (Bush et al., 2005) recommend the assessment of validity of self-report through a multimethod approach. This may include examination of consistency among self-report, test data, real-world activities, and historical records and administration of multiple SVTs throughout the evaluation. When there exists consistent evidence of invalid responding, AACN recommends that results of the inventory not be interpreted and data from other instruments without validity scales not be relied upon (Heilbronner et al., 2009, p. 1102). ASAPIL recommends reporting such concerns without “assumptions regarding examinee goals which underlie the production of invalid results” (Bush et al., 2014, p. 202). All three organizations recommend that other factors, such as culture, language, and functional limitations, also be considered when assessing validity.
Although administration of self-report measures is foundational in the field of psychology, requiring administration of SVTs in all disability claims is not a position with unequivocal supporting evidence. Administration of SVTs as part of the psychological evaluation battery can be helpful; however, interpretation of SVT data in the context of the non-cognitive testing must be undertaken carefully. Any SVT result can only be interpreted in an individual’s personal context, including psychological/emotional history, level of intellectual functioning, and other factors that may affect responding. This is true for all testing and the interpretation of test results. Particular attention must be paid to the limitations of the normative and validation data available for each SVT. As such, a simple inter-individual interpretation of SVT results is not acceptable or valid. Additionally, as discussed in Chapter 3, a qualified test user is responsible for all aspects of appropriate test use; this includes understanding the normative and validation data, potential limitations, and appropriate interpretation of any SVT, whether embedded or stand-alone. Evidence of inconsistent self-report based on SVTs is cause for concern with regard to self-reported symptoms; however, it does not provide information about whether or not the individual is, in fact, disabled. As such, failure on SVTs alone is insufficient grounds for denying a disability claim.
The challenge is in determining how best to proceed when one or more SVTs indicate overreporting of symptoms on self-report measures. In such cases, self-report measures administered during the evaluation will likely yield little meaningful information; additional information will therefore be required to assess the applicant’s allegation of disability. Additionally, because SVTs are used to help assess the validity of an individual’s responses on standardized non-cognitive psychological measures, the administration of SVTs outside of that assessment cannot provide information about the validity of evidence already in the medical evidence record.
USE OF NON-COGNITIVE MEASURES WITH SPECIFIC POPULATIONS
As suggested above, there are a number of allegations that may warrant the administration of non-cognitive tests. Such allegations generally fall in two broad categories: mental disorders and disorders with somatic complaints that are disproportionate to demonstrable medical morbidity. Mental disorders include schizophrenic, paranoid, and other psychotic disorders; affective disorders; anxiety-related disorders; and personality disorders. It is important to note that some of these conditions may also include cognitive complaints, in which case cognitive testing (discussed in Chapter 5) may be more appropriate. Disorders with somatic complaints that are disproportionate to demonstrable medical morbidity include somatoform disorders, multisystem illnesses (e.g., chronic fatigue syndrome, repetitive strain injury, chronic Lyme disease), and chronic idiopathic pain conditions (e.g., fibromyalgia, carpal tunnel syndrome).
The committee concludes that the use of standardized non-cognitive psychological measures is essential to the determination of all cases in which an applicant’s allegation of non-cognitive functional impairment meets three requirements:
- The applicant alleges a mental disorder (i.e., schizophrenic, paranoid, and other psychotic disorders; affective disorders; anxiety-related disorders; and personality disorders) unaccompanied by cognitive complaints or a disorder with somatic symptoms that are disproportionate to demonstrable medical morbidity (i.e., somatoform disorders, multisystem illnesses, and chronic idiopathic pain conditions).
- The presence and severity of impairment and associated functional limitations are based largely on applicant self-report.
- Objective medical evidence or longitudinal medical records sufficient to make a disability determination do not accompany the claim.
As noted above, when cognitive complaints accompany the applicant’s allegations, cognitive testing may prove more appropriate. The committee also recognizes that some chronic conditions may generate potentially disabling, non-cognitive functional impairments but may not be accompanied by objective medical evidence (i.e., medical signs and/or laboratory or test results that constitute clear evidence of a significant mental disorder and related functional impairment of sufficient severity to make a disability determination). In such cases, the evidence provided by longitudinal medical records (i.e., a documented history of a significant mental disorder or
a chronic condition such as chronic idiopathic pain or multisystem illnesses and related functional impairment of sufficient severity and duration to make a disability determination) may be sufficient to substantiate the allegation.
When the medical evidence of record primarily relies on self-report of symptoms, a statement regarding the validity of results obtained in the assessment is essential. As noted above, a variety of methods for objectively assessing validity exist that go beyond the clinical opinion of the examiner. In addition to analysis of the results of SVTs administered at the time of the testing and analysis of internal data consistency, evidence could include a pattern of test results that is inconsistent with the alleged condition, observed behavior, documented history, and the like. It is important to note that a finding of inconsistency between the test results and the areas specified is more informative than a finding of consistency would be. Determination of the method or methods used to assess validity is best left to the discretion of a qualified evaluator.
American Psychiatric Association. 2013. The diagnostic and statistical manual of mental disorders: DSM-5. Washington, DC: American Psychiatric Association.
APA (American Psychological Association). 2010. Ethical principles of psychologists and code of conduct. http://www.apa.org/ethics/code (accessed March 9, 2015).
Barsky, A. J., and J. F. Borus. 1999. Functional somatic syndromes. Annals of Internal Medicine 130(11):12.
Beck, A., and R. Steer. 1993. Beck Anxiety Inventory manual. San Antonio, TX: Harcourt Brace & Company.
Beck, A. T., R. Steer, and G. Brown. 1996. Beck Depression Inventory. 2nd ed. San Antonio, TX: The Psychological Corporation.
Ben-Porath, Y. S., A. Tellegen, and N. Pearson. 2008. MMPI-2-RF: Manual for administration, scoring, and interpretation. Minneapolis, MN: University of Minnesota Press.
Bigler, E. D. 2012. Symptom validity testing, effort, and neuropsychological assessment. Journal of the International Neuropsychological Society 18(4):632-642.
Bush, S. S., R. M. Ruff, A. I. Tröster, J. T. Barth, S. P. Koffler, N. H. Pliskin, C. R. Reynolds, and C. H. Silver. 2005. Symptom validity assessment: Practice issues and medical necessity. NAN policy and planning committee. Archives of Clinical Neuropsychology 20(4):419-426.
Bush, S. S., R. L. Heilbronner, and R. M. Ruff. 2014. Psychological assessment of symptom and performance validity, response bias, and malingering: Official position of the Association for Scientific Advancement in Psychological Injury and Law. Psychological Injury and Law 7(3):197-205.
Butcher, J. N., W. Dahlstrom, J. Graham, A. Tellegen, and B. Kaemmer. 1989. MMPI-2: Manual for administration and scoring. Minneapolis, MN: University of Minnesota Press.
Derogatis, L. 1994. SCL-90-R: Symptom Checklist-90-R. Minneapolis, MN: Pearson.
Derogatis, L. R., and P. Spencer. 1993. Brief Symptom Inventory: BSI. Minneapolis, MN: Pearson.
First, M. B., R. L. Spitzer, M. Gibbon, and J. B. Williams. 2012. Structured Clinical Interview for DSM-IV axis I disorders (SCID-I), clinician version, administration booklet. Arlington, VA: American Psychiatric Publishing.
Gibbon, M., R. L. Spitzer, and M. B. First. 1997. User’s guide for the Structured Clinical Interview for DSM-IV axis II personality disorders: SCID-II. Arlington, VA: American Psychiatric Publishing.
Hamilton, M. 1980. Rating depressive patients. Journal of Clinical Psychiatry 41(12):21-24.
Hathaway, S. R., and J. C. McKinley. 1940. A multiphasic personality schedule (Minnesota): I. Construction of the schedule. Journal of Psychology 10:249-254.
Hathaway, S. R., and J. C. McKinley. 1943. Manual for the Minnesota Multiphasic Personality Inventory. New York: The Psychological Corporation.
Heilbronner, R. L., J. J. Sweet, J. E. Morgan, G. J. Larrabee, S. R. Millis, and Conference participants. 2009. American Academy of Clinical Neuropsychology consensus conference statement on the neuropsychological assessment of effort, response bias, and malingering. The Clinical Neuropsychologist 23(7):1093-1129.
Henningsen, P., S. Zipfel, and W. Herzog. 2007. Management of functional somatic syndromes. Lancet 369(9565):946-955.
Henry, G. K., R. L. Heilbronner, W. Mittenberg, C. Enders, and D. M. Roberts. 2008. Empirical derivation of a new MMPI-2 scale for identifying probable malingering in personal injury litigants and disability claimants: The 15-item Malingered Mood Disorder Scale (MMDS). The Clinical Neuropsychologist 22(1):158-168.
Henry, G. K., R. L. Heilbronner, J. Algina, and Y. Kaya. 2013. Derivation of the MMPI-2-RF Henry-Heilbronner Index-r (HHI-r) scale. The Clinical Neuropsychologist 27(3):509-515.
Larrabee, G. J. 2012. Performance validity and symptom validity in neuropsychological assessment. Journal of the International Neuropsychological Society 18(4):625-630.
Larrabee, G. J. 2014. Performance and Symptom Validity. Presentation to IOM Committee on Psychological Testing, Including Validity Testing, for Social Security Administration, June 25, 2014, Washington, DC.
Miller, H. A. 2001. M-FAST: Miller forensic assessment of symptoms test professional manual. Odessa, FL: Psychological Assessment Resources.
Millon, T., C. Millon, R. D. Davis, and S. Grossman. 2009. Millon Clinical Multiaxial Inventory-III (MCMI-III) manual. San Antonio, TX: Pearson/PsychCorp.
Morey, L. C. 2007. Personality Assessment Inventory. Odessa, FL: Psychological Assessment Resources.
Rogers, R., R. M. Bagby, and S. E. Dickens. 1992. Structured Interview of Reported Symptoms: Professional manual. Odessa, FL: Psychological Assessment Resources.
Sheehan, D., Y. Lecrubier, K. Sheehan, P. Amorim, J. Janavs, E. Weiller, T. Hergueta, R. Baker, and G. Dunbar. 1998. The Mini-International Neuropsychiatric Interview (MINI): The development and validation of a structured diagnostic psychiatric interview for DSM-IV and ICD-10. Journal of Clinical Psychiatry 59(20):22-33.
Spitzer, R. L., K. Kroenke, J. B. Williams, and P. H. Q. P. C. S. Group. 1999. Validation and utility of a self-report version of PRIME-MD: The PHQ primary care study. JAMA 282(18):1737-1744.
SSA (Social Security Administration). 2010. Revised medical criteria for evaluating mental disorders. Federal Register 75(160):34.
SSA. n.d.-a. Disability evaluation under social security—Part III: Listing of impairments—Adult listings (Part A)—section 12.00 mental disorders. http://www.ssa.gov/disability/professionals/bluebook/12.00-MentalDisorders-Adult.htm (accessed November 14, 2014).
SSA. n.d.-b. Disability evaluation under Social Security: Part I—general information. http://www.ssa.gov/disability/professionals/bluebook/general-info.htm (accessed November 14, 2014).
Tollison, D., and J. Langley. 1995. Pain Patient Profile manual. Minneapolis, MN: National Computer Systems.
Van Dyke, S. A., S. R. Millis, B. N. Axelrod, and R. A. Hanks. 2013. Assessing effort: Differentiating performance and symptom validity. The Clinical Neuropsychologist 27(8): 1234-1246.
Vranceanu, A., A. Barsky, and D. Ring. 2009. Psychosocial aspects of diabling musculoskeletal pain. Journal of Bone and Joint Surgery 91(8):2014-2018.
Weathers, F., B. Litz, D. Herman, J. Huska, and T. Keane. 1994. The PTSD checklist-civilian version (PCL-C). Boston, MA: National Center for PTSD.
WHO (World Health Organization). 1993. Composite International Diagnostic Interview (CIDI): Interviewer’s manual. Geneva, Switzerland: WHO.
Widows, M. R., and G. P. Smith. 2005. Structured Inventory of Malingered Symptomatology: Professional manual. Lutz, FL: Psychological Assessment Resources.
Wing, J. K., T. Babor, T. Brugha, J. Burke, J. Cooper, R. Giel, A. Jablenski, D. Regier, and N. Sartorius. 1990. SCAN: Schedules for Clinical Assessment in Neuropsychiatry. Archives of General Psychiatry 47(6):589-593.
























