
3
Public Health Surge Capacity and Community Resilience
Highlights and Main Points Made by Individual Speakers and Participants1
- Alternative triage services such as the Nurse Triage Line used in Minnesota in 2009 during the H1N1 outbreak can prevent large numbers of in-patient visits and potentially reduce exposure for many residents and hospital patients. (DeVries)
- To reduce the clinical surge burden on hospitals, communities can provide alternative care and medical needs shelters, as well as increase training and use of community paramedicine, and incorporate better coordination and integration of Emergency Support Function (ESF)-6 and ESF-8, prior to and during a disaster. (Davis)
- Including regional partners such as the Administration for Children and Families’ regional administrators and pharmacists in planning efforts can help to keep people out of health care facilities and reduce the surge burden. (Adams, Meier)
- Encouraging social cohesion can drive community resilience, and creating an evidence base to inform academia, policy makers, and community organizers can gain support for the methods used. By mapping the methodology used in various cities, neighborhood leaders can leverage successes of individual communities and build linkages across jurisdictions. (Aldrich, Schor)
- Linking ESF-8 and ESF-6 at all levels in a response can reduce the reliance on emergency departments and clinical services. (Meier)
- Tying funding incentives from the Office of the Assistant Secretary for Preparedness and Response and the Centers for Disease Control and Prevention to regional and cross-sector engagement in their agreements can better integrate various sectors at the local level. (McClendon, Shah)
________________
1This list is the rapporteurs’ summary of the main points made by individual speakers and participants, and does not reflect any consensus among workshop participants.
Large-scale disasters affect more than just individual health care facilities; they permeate the entire fabric of communities, demanding resources across sectors and jurisdictions. Having scalable and flexible public health surge capacity, in concert with community and social services, can help to alleviate the surge burden on clinical health care facilities throughout a multi-community region. “Surge capacity” can involve area hospitals, as well as alternative care sites and other medically capable shelters specially set up during a disaster to divert people away from overcrowded emergency departments. This chapter examines the opportunities for public health services and other community services to coordinate across a region and keep hospitals and health centers from overcrowding, as well as ideas for better planning across sectors related to vulnerable populations. A region with robust public health surge capacity during steady state times can also become more resilient in the face of disasters. Participants in this section discuss possibilities for achieving this goal by addressing social determinants of health2 and enhancing themes of social capital and cohesion within communities.
REDUCING CLINICAL SURGE THROUGH PUBLIC HEALTH AND COMMUNITY SERVICES
Alleviating burdens on emergency departments and trauma care centers within a region is often a goal for communities in the hours and days following large-scale disasters. This was also the motivation behind several disaster-related initiatives across the country discussed in the following paragraphs. These initiatives, all organized through authorities outside of hospitals and health care centers—from Minnesota to New Jersey to Texas—included a nurse triage line (NTL), Alternative Care Sites, Extended Treatment Areas, and oxygen strike teams.
Nurse Triage Line
Aaron DeVries, medical director of the Infectious Disease Division at the Minnesota Department of Health (MDH), described their experience during the H1N1 pandemic in 2009 to improve access to medical
________________
2The World Health Organization defines social determinants of health as the conditions in which people are born, grow, live, work, and age. These circumstances are shaped by the distribution of money, power, and resources at global, national, and local levels. See more at http://www.who.int/social_determinants/en (accessed December 9, 2014).
care and reduce surge on health care facilities in the state during the outbreak. During the spring and summer of 2009, many Minnesota hospitals and clinics experienced large numbers of ill people seeking care, including those with influenza symptoms and the worried-well. In addition, access to H1N1 antiviral treatment became increasingly problematic. Therefore, MDH leaders created partnerships with existing nurse triage telephone lines operating in the state to create a coordinated statewide nurse triage line that could target high-risk groups across counties and recommend care and treatment where necessary. The Centers for Disease Control and Prevention (CDC) is also exploring other alternate delivery systems for antiviral medications during severe influenza pandemics as well as clear strategies to communicate accurate messages to the public (IOM, 2012b).
DeVries explained the development of the Minnesota-wide integrated NTL, called the Minnesota Flu Line (see Figure 3-1), which began at the suggestion of an infectious disease physician at a Minnesota children’s hospital during the pandemic. Because many different nurse

FIGURE 3-1 Listing of the Minnesota health systems making up the state’s nurse triage line during the H1N1 outbreak in 2009.
SOURCE: DeVries presentation, July 24, 2014.
triage lines already operated independently by private health care systems within the state, an integrated NTL seemed to be the most effective approach and quickest to operationalize to meet the health care surge. The objectives of the NTL were
- Decrease public confusion by providing accurate information—consistent messaging, and assistance, including use of antiviral medications;
- Decrease the spread of disease by reducing the volume of sick individuals gathering in health care settings;
- Reduce medical surge on health care facilities to ensure that other priority medical needs would continue to be met; and
- Meet the needs of uninsured or underinsured patients and those without easy access to health care.
The NTL provided rapid evaluation, targeting of high-risk groups, recommendation to level of care (home versus clinic versus emergency room), and prescription of antiviral drug by a nurse practitioner if home care is advised. The integrated NTL was a public–private partnership between the MDH and 14 Minnesota health care systems that already operated their own NTLs. DeVries said gathering all of these different organizations in one room was a challenge because they typically saw themselves as competitors and were initially wary of sharing what they thought was “proprietary” information. Having the state as the coordinator and finding the “decision makers” in each organization quickly was critical to keeping the effort moving. All the private partners agreed to coordinate NTL services through a single toll-free number and a standard protocol, which included prescription treatment if necessary. At the designated local pharmacy, if the patient had insurance and there was no market interruption in the supply, a treatment course of oseltamivir was dispensed, and insurance was billed. If the patient was uninsured or underinsured, oseltamivir from pre-positioned state cache antivirals was dispensed at no cost to the patient or with an option of a low-cost fee (Spaulding et. al, 2012). From design to implementation, the integrated NTL took slightly more than 1 month to take shape and began operations in October 2009.
DeVries stated that more than 27,000 individuals from 86 counties called the Minnesota Flu Line during the epidemic, with the highest call volumes from rural, northern Minnesota counties. MDH officials estimated that approximately 11,000 in-person health care encounters may have been pre-
vented by the Minnesota Flu Line (Spaulding et al., 2012), which means possible additional exposures from those individuals seeking in-person care may have been prevented as well. However, because this system was built quickly and created solely for the purpose of clinical triage, there were challenges and gaps in data collection. DeVries said they did not have time to design reporting systems based on this capability but that for future endeavors they hope to gather real-time caller demographics, geo-location, and outcome of patients in order to give even more information to public health officials and state health care partners during a pandemic emergency.
Medical Needs Shelters, Alternative Care Sites, and Extended Treatment Areas
Monique Davis of the Hudson County, New Jersey, Regional Health Commission presented their experiences in integrating public health and human services to increase surge capacity. The integration represented the linkage of Emergency Support Function (ESF)-6 (mass care) with ESF-8 (public health). The presentation focused on medical needs shelters, alternative care sites, and extended treatment areas—sites that are designed to handle surge capacity when hospitals and emergency departments are inundated. Sites with these capabilities were used in New Jersey during Superstorm Sandy. As background, Davis noted that New Jersey has a population of 8.1 million, divided among five public health regions. The state has 75 hospitals and some 21,000 hospital beds, most of which are located in the northeast and central eastern regions of the state. Hudson County was deeply affected by Superstorm Sandy, with all but 1 of the 12 municipalities in the county bordered by some body of water. Every one of the communities experienced power outages of some duration, she commented. Hudson County was still sheltering 17 days after the storm primarily due to lack of power. She explained that the storm left five of six hospitals out of service in Hudson County.
Medical Needs Shelters
Superstorm Sandy emphasized that dedicated medical needs shelters were imperative. Hospitals faced an onslaught of patients who simply needed an outlet to plug in medical equipment or to obtain oxygen support. General population shelters were not properly staffed to assist those whose medical needs required some clinical oversight, but were not
acutely ill and warranted hospitalization. During and immediately following Superstorm Sandy, the lack of medical needs shelters—or similar capabilities at general emergency shelters—led to hospital surges, overwhelming emergency departments.
The purpose of a medical needs shelter, as Davis explained, is to provide short-term supportive medical care during a disaster when the evacuees are displaced from their homes and cannot be accommodated in the general population shelter due to medical needs. The medical needs shelter can be located in a general population shelter or be freestanding. The ESF-6, which includes mass care, emergency assistance, human services, and temporary housing, is led by the American Red Cross and the Federal Emergency Management Agency (FEMA) and supported by human services. ESF-6 closely coordinates with ESF-8 for staffing and to make sure medical needs are met. ESF-8 personnel conduct environmental assessment of the shelter to ensure that there are the proper number of bathrooms, hot running water, showering facilities and toileting, and food that is served at the proper temperature. Davis explained that public health also has a role in disease surveillance. In the wake of Superstorm Sandy there was a norovirus outbreak in one of the shelters caused by contaminated food. Also involved in the operation of a medical needs shelter is the Salvation Army, and Volunteers Active in Disaster (VOAD).
While they might seem an easy fix in concept, staffing of medical needs shelters can be problematic. Consequently, family members who are caregivers are encouraged to stay and continue their role at the medical needs shelters. Although it tends to break up families, with noncaregiving family members sent to general population shelters, it is crucial to have help at the medical needs shelters, Davis said. Furthermore, Davis’s organization is working with schools of nursing and home care health agency programs to contribute to staffing of medical needs shelters in lieu of using registered nurses for tasks that can be handled by lesser-trained professionals. For staffing issues and any other issue of concern, Davis noted that her county set up a Special Needs Advisory Group to ensure input from the special needs community.
Alternative Care Sites and Extended Treatment Areas
Another common approach to decompress emergency departments is by standing up alternative care sites and extended treatment areas. In New Jersey, planning for these sites began 2 years before Superstorm Sandy, Davis noted. An alternative care site is a community-based loca-
tion that is owned or operated by an entity other than the health care facility to which lower acuity health care patients may be directed for treatment. They are community-based sites—such as a school or community center—converted to provide patient care during a medical surge. When up and running during Superstorm Sandy, Medical Reserve Corps (MRC) volunteers staffed the alternative care sites. Extended treatment areas are similar in intent—to siphon nonemergency patients away from the emergency department—but are places established by a health care facility, typically on a site they own. For example, they can be located in tents constructed in the parking lot belonging to a hospital or in mobile vans, rehab hospitals, or triage sites set up by emergency medical services (EMS). Both extended treatment areas and alternate care sites are scalable in size for the numbers of beds, medical supplies, and equipment needed. They can be adjusted based on available resources or the nature of the medical surge emergency.
As mentioned previously with medical needs shelters, staffing of these alternate sites is also a key issue, because hospitals are not expected to staff them. Davis said potential sources of staff can include the MRC volunteers, Emergency System for Advance Registration of Volunteer Health Professionals (ESAR-VHP), and volunteers with the Red Cross and other private philanthropic organizations. Additionally, ensuring the staff members recruited to work these alternative care sites are trained appropriately has also proven challenging. During Superstorm Sandy, many nurses in the MRC turned out to be school-based nurses who needed training to take care of a common patient presentation, such as a diabetic patient who needed wound care. In the case of New Jersey, the state assumed responsibility for their training, but this is not always the case across the country, and could present complicated issues in a multi-state, regional disaster with volunteers crossing borders to respond. A main concern that continues to arise during and between disasters across the country is liability for the MRC volunteers and other professionals working at alternative sites. In some states, they are covered by significant state tort protections, but in other states they are not. If a staff member is assigned to work at an alternative site on behalf of a hospital, then the usual source of malpractice applies. While states and volunteer agencies work to address liability concerns and best recruiting strategies, spending time during the planning process to answer some of these questions can contribute to a lesser burdened emergency department and a community with potentially greater capacity to care for residents in a large-scale disaster.
Planning for At-Risk Populations
Teresa Ehnert, bureau chief of Public Health Emergency Preparedness of the Arizona Department of Health Services, spoke about the progress made by the state of Arizona in ensuring that public shelters can accommodate at-risk populations. The conceptual footing for the state’s efforts was established in 2010, with a planning exercise called Arizona Partners in Preparedness. One of the five strategic priorities created by the planning exercise was “to sustain and develop programs for at-risk population preparedness.”3 Within this priority, planners came up with four strategic objectives: (1) strengthen preparedness planning with access and functional needs stakeholders; (2) integrate behavioral health, public health, and health care system response capabilities; (3) engage and establish partnerships with non-English speaking/limited English proficiency stakeholders; and (4) implement strategies for communicating with geographically isolated populations.
To achieve these strategic objectives, Arizona has found it essential to forge community partnerships, especially between emergency management and disability groups such as the Arizona Center for Disability Law and the Arizona Independent Living Council. One example of progress is that Arizona routinely incorporates deaf and hard of hearing individuals into standard hospital decontamination exercises.
Under its new strategic framework arising from the 2010 planning exercise, Ehnert explained, Arizona is trying to break the historical paradigm that designated functional needs populations as “special” or “vulnerable.” That paradigm left people with special needs being served by shelters that were “separate and unequal.” Arizona’s new goal is to ensure equality by integrating the planning for people with functional needs and mainstream populations (see Figure 3-2). Under this approach, all Arizona shelters have become completely accessible for people with functional needs; in contrast to Davis’s approaches of Medical Needs Shelters in New Jersey, Arizona no longer sponsors special health care or medical needs shelters. The integrated approach incorporates all types of functional needs, including physical, sensory, cognitive, and multiple medical needs. Shelters now routinely provide equipment that is used for
________________
3The four other strategic priorities were to (1) improve community resilience through cross-sector collaboration; (2) maximize public health and health care system response capabilities; (3) expand regional health care coalitions; and (4) integrate information-sharing systems and protocols.
activities of daily living: power wheelchairs, audio input/output electronic devices, text devices, and video telephones.
The state also has conducted an exercise planning for a common consequence of floods and fire, namely extended power outages. From the exercises the state learned a lot about equipping all shelters with sufficient battery power to meet the needs of people with functional needs. Shelters have a durable medical equipment cache that allows people with basic medical needs to stay in general population shelters, keeps families/caregivers together, and reduces the need for medical surge. The state also has numerous ongoing projects with disability partners to further its goal of integrating at-risk populations with mainstream shelter populations and it vigorously works with tribes to ensure their members with functional needs are accommodated.
As shown by these two examples, there is not one right answer to ensuring capable response to residents with functional needs or complex medical needs. However, working across regions and states prior to a disaster—shown by both Ehnert and Davis—can aid in planning so state and local health authorities know what systems to expect if their residents need to cross jurisdictional lines for shelter assistance.
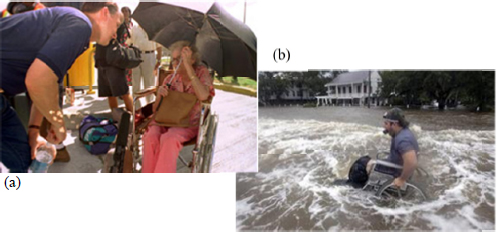
FIGURE 3-2 Examples of at-risk populations that may require extra planning considerations in a disaster.
SOURCES: (a) FEMA photo, September 15, 1995; (b) Ehnert presentation, March 26, 2014.
Community Paramedicine
Jolene Whitney of the Utah State Health Department, suggested considering community paramedicine, the field of medicine focused on assisting individuals, families, and communities in attaining optimal health, often following acute or sudden onset of medical or traumatic events—but outside of the hospital setting (Bigham et al., 2013). With worries of physician shortages in coming years, there is an opportunity for EMS professionals to expand their scope of work outside the typical hospital environment. During an IOM workshop in November 2013, Matt Zavadsky of MedStar Mobile described their Mobile Integrated Health Care Program. It trains community paramedics and others to triage patients in their homes and with the help of physicians on the phone, to either treat them or refer them to appropriate services. In addition to receiving care in their home, he noted the benefits to the community by keeping patients out of the emergency department—on a routine basis but also during an emergency:
The Mobile Integrated Health Care program has helped the community by increasing the capacity of the hospital and the health care system, returning thousands of emergency department and inpatient bed hours, in other words, freeing up beds and staff time that were previously used because all 911 calls resulted in transports to the hospital. It has improved collaboration across the health care continuum, and providers in the program work very closely with primary care and emergency department physicians. (IOM, 2014, p. 46)
In a similar example of paramedicine, Lori Upton, recounted her experience with “strike teams” of paramedics in southeast Texas during Hurricane Ike in 2008. One problem frequently encountered in a disaster is the need to refill oxygen tanks for the homebound ill. Those patients call 911, hoping to get their oxygen tanks refilled at the hospital. However, what many do not realize is that hospitals do not possess the capability to refill oxygen cylinders, even when not under duress. Upton’s agency worked with 911 dispatch to create a so-called oxygen-strike team of paramedics whose purpose was to go to homes and refill oxygen from specially-equipped ambulances. If patients were stable, the paramedics conducted the cylinder swap and put patients on a return schedule for as
long as necessary. Upton’s agency also created a plan for homebound patients needing dialysis. They set up a call center where patients could locate the closest operational center and in this way were able to avoid going to the overcrowded emergency department. Though local emergency medical services may already be stretched fielding regular emergency calls, adding coordinated regional ambulances and emergency medical assets during a disaster and expanding the scope of practice of paramedics can help to keep many people out of hospitals— both keeping them safer at home and reducing surge in crowded emergency departments.
The discussions on public health surge capacity and community resilience built off of multiple meetings on both surge management and community engagement. Much of the conversation included how to build sustainable and inclusive health coalitions that can allow for greater resources, communication, and surge capacity when needed. Many of the suggestions by participants and discussion leaders Umair Shah, director of Harris County Public Health and Environmental Services in Texas, and Andrew Stevermer, regional emergency coordinator for the Office of the Assistant Secretary for Preparedness and Response (ASPR), focused on long-term goals of making communities more resilient by addressing social determinants of health, mentioned previously in this chapter. If public health can address those determinants such as housing, transportation, education, access to health care and nutrition, access and functional needs of children, and others prior to a disaster—in addition to fostering stronger community bonds through social capital and cohesion—then communities could become more resilient in disasters and experience less of a clinical surge burden on regional hospitals. In addition, having a framework for broad, cross-sector community risk assessment, allowing better understanding of which areas will be rebuilding and how, could be a crucial linkage to disaster recovery on multiple levels, including funding.
Inclusive Health Coalitions
One of the opportunities discussed to increase services outside the hospital included widening the net for coalition inclusion. Alex Adams of the National Association of Chain Drug Stores commented that there are 120 pharmacy organizations across the country with thousands of
actual pharmacies. Because of their complexities, he said, planning at the local level for them is very challenging, and regional planning would be far more advantageous. He also noted that with the explosion of pharmacies as “minute clinics,” pharmacists are often doing point of care flu/strep testing, and have the ability to provide vaccinations—adding that one in five flu shots is given in a pharmacy. Especially as the emphasis on community and population health from Affordable Care Act (ACA) continues, Adams said pharmacies could be a public health asset in mitigating surge issues in the community, also reducing the burden on hospitals.
In addition to pharmacies, Carolyn Meier, deputy regional administrator for the Administration for Children and Families (ACF), highlighted ACF’s regional emergency management specialists who can serve as liaisons between ESF-6 and ESF-8 in coalitions’ planning efforts to provide services that residents might otherwise seek in a hospital or health care setting (e.g., crisis counseling, mental health services, child reunification and social services for children, help securing or renewing prescription medications, or special needs support). In recent years, some states and local jurisdictions have also been developing Children’s Emergency Task Forces to respond to children’s needs in disasters.4 These are models of community collaboration that include ESF-6 and ESF-8 partners, including pediatricians, 211 call centers, behavioral health, child care providers, schools, public health, VOAD, and local social services. Such regional collaboration could help to further address the access and functional needs of children or other planning, especially for children with no caregivers present in neighborhoods, hospitals, and shelters. Connecting the work of the Children’s Emergency Task Forces with medical and public health coalitions could provide meaningful collaboration for community response and recovery, and reduce the impact on public health systems.
Other individuals highlighted the potential of the entire EMS community, in addition to the previously mentioned “community paramedics,” as health professionals who could augment a community response in emergencies. Especially in the initial and mitigation phases of public health surge responses, EMS providers at all levels could add to needed staffing demands. Including non-traditional partners in coalitions who
________________
4Examples of these task forces can be found in an ACF document on guidelines for development. See http://www.acf.hhs.gov/sites/default/files/ohsepr/childrens_task_force_development_web.pdf (accessed March 19, 2015).
are already patched into the regions can help to reduce clinical surge demands as well as foster a more holistic response and recovery.
Social Capital and Cohesion
Daniel Aldrich, an associate professor of political science at Purdue University, delivered an overview of social capital and cohesion, a concept that refers to knowing one’s neighbors, volunteering in the community, and having ties to one’s locality or region through participation in civic groups, parent/school groups, houses of worship, and other neighborhood organizations. Previous experiences have shown that communities that have high levels of social connectedness (often referred to as social capital or social cohesion) display resilience that serves them well in post-disaster recovery (Aldrich and Sawada, 2015).
Aldrich introduced himself as a victim of Hurricane Katrina who lost his home, his possessions, and his job. About 6 months after Katrina, he and a colleague conducted a house-to-house survey of 1,000 New Orleans residents to determine factors associated with rebuilding. To their surprise, rebuilding was not correlated with less water depth (2 feet versus 15 feet), more resources (insurance and savings), lower population density (offers more routes of evacuation), and fewer deaths. Instead, he found that rebuilding occurred in clusters, and it was correlated with residents having social ties to the community (see Figure 3-3). One example of is from one small New Orleans community, the village of L’est. When residents returned to their homes they found there was no electricity and no gas. They alerted the local power company to turn on the gas, fix the transformers, and restore utility lines. Officials told them that to consider such an expensive undertaking, they needed proof that enough people would benefit. Within 3 days the community collected hundreds of signatures on a petition. Residents had succeeded in maintaining contact during the evacuation process through e-mail, websites, phones, and face-to-face contact.
Social Capital Research
Based on subsequent research of four disasters (1923 Tokyo earthquake, 1995 Kobe earthquake, 2004 Indian Ocean tsunami, and 2005 Hurricane Katrina), Aldrich found that three types of social connections were associated with recovery and resilience: bonding social capital (cohesion within social networks, e.g., ethnicities and religions); bridging
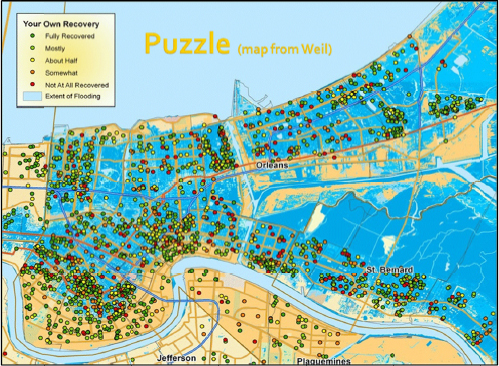
FIGURE 3-3 Perceived recovery after Hurricane Katrina (yellow and white areas are between 1 and 2 feet; darker blue areas are up to 13 feet of water).
SOURCE: Aldrich presentation, March 26, 2014.
social capital (linkages across different social networks through institutions, schools, and sports clubs, among other venues); and linking social capital (connections between citizens and government and elected officials who hold positions of authority and power) (see Figure 3-4).
Aldrich also reported the types of costs associated with rebuilding: psychological, financial, and opportunity costs. If people are strongly connected to their community in terms of sense of place and engagement, they want to rebuild regardless of costs. For example, he and his colleagues found that in Japan people who lived within 1 kilometer of the shore in Sendai wanted to rebuild. Aldrich suggested that policy makers encourage four activities to build trust and community ties:
- Encourage people to get to know their neighbors;
- Hold social events to begin strengthening ties across neighborhoods;
- Have people meet on a regular basis on any topic; and
- Incentivize volunteering by paying them in local currency that can be used only in locally owned stores.
In Aldrich’s view, social connections across affected communities are what drive the process of recovery. The physical infrastructure itself will never be completely secure. There is no way of guaranteeing any bridge or any levy will hold, but social cohesion, in contrast from experience and data, is what drives resilience. Promoting social cohesion, said Aldrich, should be part of the job description of city officials and emergency managers. Ideally such efforts should be undertaken before a disaster—as a component of resilience-building initiatives, and can be either top-down or bottom-up approaches. Some cities have already started programs with this goal in mind, such as the Neighborhood Empowerment Network (NEN) in San Francisco.5 Although NEN is a
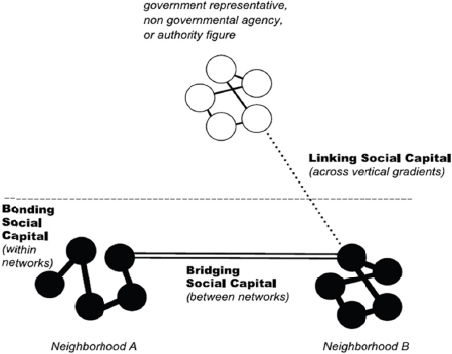
FIGURE 3-4 Theoretical approach to social capital and cohesion.
SOURCE: Aldrich presentation, March 26, 2014.
________________
5For more on the Neighborhood Empowerment Network, see http://empowersf.org (accessed January 29, 2015).
collaborative of several organizations to advance resilience at the community level, it is sponsored by the San Francisco Department of Emergency Management. Having this type of grassroots encouragement and support from the local government can help communities band together to build more resilience into their social bonds and physical infrastructure to better prepare for disasters.
HIGHLIGHTED OPPORTUNITIES FOR OPERATIONAL CHANGES
During various discussions on these issues throughout the meetings, individual participants voiced suggestions for potential changes ranging from the local level up to the national level, in order to better accommodate some of the needs highlighted:
- Ken Schor, director of the National Center for Disaster Medicine and Public Health, remarked on the need to create an evidence base about social cohesion’s effects to mitigate disasters and build resilience. He said community members need to have access to the evidence to inform academia, policy makers, and community organizers and gain their support for the methods. By mapping the methodology used in various cities, neighborhood leaders can leverage successes of individual communities and build linkages across jurisdictions.
- Several speakers voiced the need to build ownership of resilience from within the neighborhood or community to strengthen capacity at the community level. Aldrich argued that communities should be flexibly engaged in developing shared goals and plans for disaster recovery, which also creates a sense of empowerment at the community level, and strengthens ties within and outside the community.
- Facilitation of regional information sharing regarding at-risk individuals could be accomplished by enhancing mechanisms across entities in the same region, said Suzet McKinney, deputy commissioner of the Chicago Department of Public Health. Identification of at-risk populations is often challenging, and shared information from the health care system across state or county lines could help better prepare the distribution of regional assets and capabilities. This could be facilitated by CDC’s Division of
-
State and Local Readiness within the Office of Public Health Preparedness and Response, assisted by the Division for At-Risk Individuals, Behavioral Health, and Community Resilience in ASPR.
- To reduce reliance on emergency departments, several speakers, including Meier, noted that human services and public health could be better integrated in a response, for example, by linking ESF-6 (mass care, emergency assistance, housing and human services) and ESF-8 (public health and medical) at all levels to leverage resources, avoid duplication, and increase situational awareness across communities.
- Several speakers suggested that because disaster funding is currently siloed from the federal level, better integration at the local level could be promoted through funding being contingent on cross-sector engagement. Bruce Clements, preparedness director for the Texas Department of State Health Services, saw a need for a broader, crosscutting risk assessment instead of making risk assessment requirements for multiple communities and sectors based on specific funding. Shah suggested possibly tying ASPR and CDC funding incentives to regional and cross-sector engagement in the agreements to better integrate various sectors at the local level.
This page intentionally left blank.


















