
2
Universal Health Coverage and Occupational Health and Safety Issues for the Informal Workforce
This chapter includes presentations from the workshop that provided an overview of the scope and challenges of providing universal health coverage and occupational health safety for the informal workforce in low- and middle-income countries (LMICs).
THE INFORMAL WORKFORCE
Marty Chen, Harvard University and WIEGO Network
Marty Chen from Harvard University and the Women in Informal Employment: Globalizing and Organizing (WIEGO) network provided an overview of the informal workforce by introducing definitions and concepts, presenting recent data, explaining some of the common risks and barriers to access, and sharing some illustrative examples. Much of the information Chen offered was based on her experiences and research through the WIEGO network. The WIEGO network consists of membership-based organizations of informal workers, researchers and statisticians, and practitioners from development agencies who seek to increase the voice, visibility, and validity of the working poor, especially women, in the informal economy and thereby enable them to demand an enabling policy environment.
Informal Sector, Informal Employment, and the Informal Economy
Chen provided some context on the interrelated concepts of “informal sector,” “informal employment,” and “informal economy.” Initially the informal sector was thought about in terms of enterprises, and in 1993 the International Conference of Labour Statisticians (ICLS) adopted an enterprise-based definition that refers to employment in unincorporated enterprises that might also be unregistered or small. “Informal employment” is a broader concept that includes not only those who work for informal enterprises, but also those who work for formal enterprises or for households. The concept of informal employment, which was developed with the International Labour Organization (ILO) and adopted by the ICLS in 2003, refers to both self-employment and wage employment without social protection through work, both inside and outside the informal sector. Chen said that the fastest-growing segment of informal employment in many countries is informal wage employment for formal enterprises. “Informal economy” is the broadest of the concepts and refers to the diversified set of economic activities, enterprises, and workers that are not regulated by the state and do not have employment-based social protection as well as the output that they produce.
Chen discussed the characteristics of the two basic categories of workers within informal employment: self-employed and wage workers. Self-employed workers in informal enterprises are part of the informal economy, and they include employers who hire others (less than 5 percent in most countries), workers who operate on their own account, unpaid contributing family workers, and members of informal producer cooperatives. The other basic category is wage workers in informal jobs, which includes informal employees of informal enterprises, informal employees of formal enterprises, and domestic workers without employer contributions. Chen commented that within these official categories, some groups are still left out, such as casual day laborers and industrial outworkers. She suggested that the inclusion of more categories of informal employment, including different types of employees, could improve the data and understanding of the informal workforce. Table 2-1 provides data that have been collected on the averages and ranges of the incidence of informal employment as a percentage of nonagricultural employment within regions. (Chen commented that the next frontier in defining the informal economy will be to define informality in agriculture.) While earlier models had assumed that economies in LMICs would move away from informal employment and toward modern wage employment, Chen said that this shift is not happening in most countries.
TABLE 2-1 Informal Employment as a Percent of Nonagricultural Employment, 2004–2010
| Region | Average | Range | |
| South Asia | 82% | 62% (Sri Lanka) | 84% (India) |
| Sub-Saharan Africa | 66% | 33% (South Africa) | 82% (Mali) |
| East and Southeast Asia | 65% | 42% (Thailand) | 73% (Indonesia) |
| Latin America | 51% | 40% (Uruguay) | 75% (Bolivia) |
| Middle East and North Africa | 45% | 31% (Turkey) | 57% (West Bank and Gaza) |
SOURCES: Marty Chen presentation to workshop, July 29, 2014; data from WIEGO and ILO, 2013.
Informal Workers, Universal Health Coverage, and Occupational Health
Basing her comments on WIEGO’s research, Chen described some of the risks that informal workers face relative to formal workers. Informal workers have greater exposure to health risks due to their living and working environments, less protection against loss of income associated with health risks, and less protection against the costs of health risks because of the lack of employer contributions to health insurance and a limited access to universal coverage. Informal workers also experience more barriers to access. They have less access de jure to health insurance and health services, often because the systems and the schemes are not appropriately designed to take into account the specific realities of informal work (as is detailed by Robert Emrey in his presentation on the elements of universal health care design). Furthermore, informal workers have less access de facto to health insurance and health services, including occupational health services to which they are entitled, due to a lack of knowledge of their entitlements, less ability to negotiate the bureaucracy, and leakages, blockages, and lack of coordination in health insurance and health services.
Table 2-2 illustrates these risks and barriers through three examples: home-based workers, street vendors, and waste pickers. Chen’s research and the research of WIEGO, among others, provide an opportunity to better understand the populations, characteristics, and needs of members of the informal economy and thus how occupational health and safety (OHS) reforms should take into account different places and types of work and how reforms can be sector specific.
TABLE 2-2 Informal Workers’ Occupational Health Risks and Barriers to Health Care
| Occupation | Risks | Barriers |
| Home-based workers |
|
|
| Street vendors |
|
|
| Waste pickers |
|
|
SOURCE: Marty Chen presentation to workshop, July 29, 2014.
UNIVERSAL HEALTH COVERAGE: FRAMEWORKS FOR DISCUSSION
Robert Emrey, U.S. Agency for International Development
To provide an overview of approaches to universal health coverage in LMICs, keynote speaker Robert Emrey from the U.S. Agency for International Development (USAID) introduced several frameworks that currently are being used or explored to achieve universal coverage and discussed their relevance to the inclusion of the informal workforce.
Health Systems Strengthening
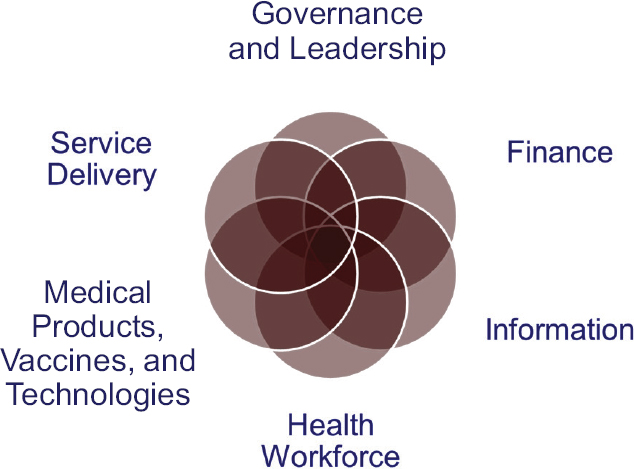
Emrey listed the six items that the World Health Organization (WHO) has identified as the key building blocks of the health system—governance and leadership, finance, service delivery, health workforce, information, and medical products, vaccines, and technology—and elaborated on the relevance of the building blocks to the topic of the workshop. Each block is relevant to both the public sector and the private sector, and each extends beyond the patient–provider relationship to include family members and members of the community. Emrey also commented on the labeling of the six components as building blocks. As blocks, he said, the components are sometimes thought of in terms of a linear stack, which is misleading. Rather, he suggested that the components should be thought of as interconnected and overlapping, as shown in Figure 2-1.
To demonstrate the linkages between the interconnected health system components and universal health coverage, Emrey presented a vision for an action framework that included the health system components from Figure 2-1 as inputs, processes, and outputs, and the objectives of universal health coverage (UHC) as outcomes (see Figure 2-2). The UHC objectives include the three primary objectives of financial protection, essential services, and population coverage as well as a fourth objective added by Emrey—responsiveness. Responsiveness to people’s expectations has been identified by the WHO as an additional objective to which health systems strengthening initiatives should give attention, in particular, to address issues related to stigma and consumer satisfaction. The areas of impact included in the framework are the primary focus areas of the U.S. government’s health programming in LMICs, Emrey said, and they provide context from the U.S. perspective on the ultimate goals of the inputs, outputs, and outcomes for health systems strengthening.
SOURCES: Robert Emrey presentation to workshop, July 29, 2014; USAID Office of the Standard Health Systems Functions; data from WHO, 2007.
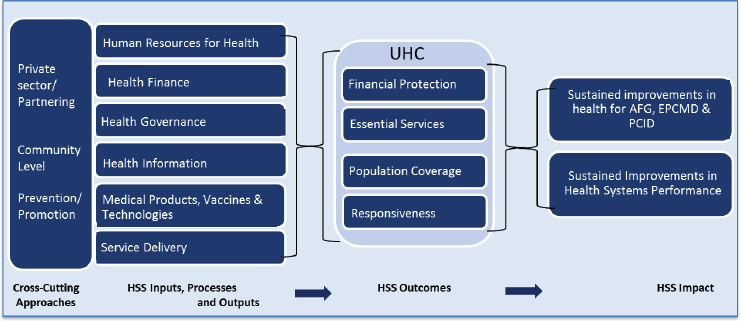
NOTE: AFG = AIDS-free generation; EPCMD = ending preventable child and maternal deaths; HSS = health systems strengthening; PCID = protecting communities against infectious diseases; UHC = universal health coverage.
SOURCES: Robert Emrey presentation to workshop, July 29, 2014; USAID’s Vision: Strengthening Health Systems for Lasting Health Impact 2015 (Draft).
Universal Health Coverage
To frame the discussions on universal health coverage, Emrey displayed a three-dimensional cube that was developed by the WHO and which served as a reference point throughout the workshop discussions (see Figure 2-3). The three sides of the cube represent the three primary objectives of UHC: population coverage, essential package of services, and financial protection.
Currently, the financing situation at the national level for both the formal and informal sector in most countries is divided up into small categories, Emrey said. These arrangements have developed over time according to the politics and the economic situations and the opportunities to move forward in various countries. This process has created systems where coverage is spread into categories that were politically acceptable at the time they were created, and in many cases the financing arrangements have stayed in place for the long term. For example, a health financing arrangement before a national approach to universal coverage is implemented might include within the formal sector a mix of coverage
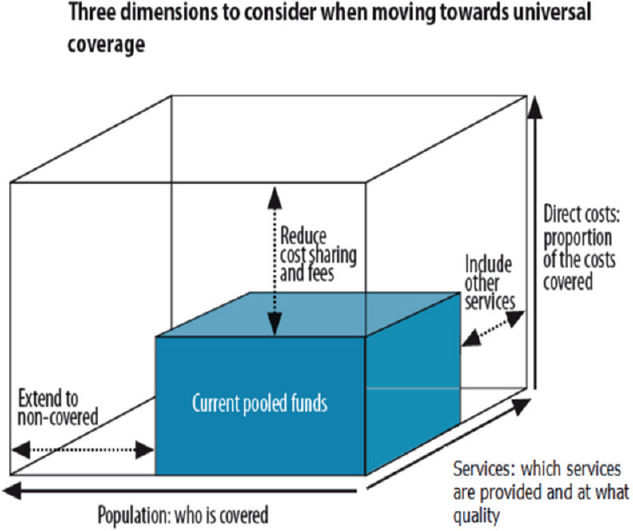
SOURCES: Robert Emrey presentation to workshop, July 29, 2014; WHO, 2015b.
SOURCES: Robert Emrey presentation to workshop, July 29, 2014; Wang et al., 2012.
provided by employers, social security, and through private commercial insurance; and within the informal sector a mix of coverage through user fees, fee exemptions, vouchers, and community-based health insurance or mutual health organizations (Wang et al., 2012). Emrey stressed that reforming, improving, or expanding coverage in a country requires starting from such a base, looking at what is already there, and determining how to move forward.
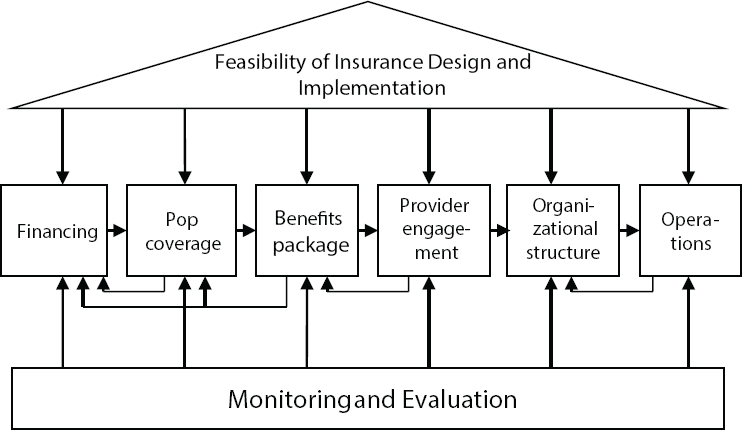
Emrey commented that the process of developing a UHC scheme in a country will occur in the middle of an ongoing dialogue about the opportunities to redesign and improve the current system. Approaching UHC is not a linear process, but rather very cyclical. With this context, Emrey said that, when approaching the development of a UHC scheme at the national level, it is helpful to consider the design elements that make up the system and how they interact and contribute to the overall system (see Figure 2-4). He presented the individual elements and the potential barriers within each element for the inclusion of the informal workforce.
Feasibility of Insurance Design and Implementation
Emrey said that a national conversation about UHC should start with establishing an understanding of the financing arrangements that are in place, the situational politics, and where there are gaps. It is important
early on to find the gaps, to have conversations about the availability of existing financing arrangements, and to look at the way in which the insurance arrangements, if there are any, and the fees and other finances work their way through the system as it currently stands in a given country. Small and poorer countries often need different kinds of health services than bigger or richer countries, but the same set of issues applies across national contexts and is an important part of the conversation about the feasibility of redesign within any given country. Ultimately, to determine this feasibility Emrey suggested that policy makers and other stakeholders from the legislature, executive branch, private sector, and civil society be brought together for a conversation about what is possible. Tools have been developed to assess the feasibility, including political mapping tools, health accounts and service access datasets, and community cohesion assessment tools (see Box 2-1 for examples of existing tools).
During his discussion of the feasibility of insurance design and implementation, Emrey noted some potential barriers for the inclusion of the informal workforce: Major stakeholders may not be aligned with the informal workforce or even aware of it; the informal workforce may not accurately be captured in the statistical systems and studies of a given country; and the beliefs and behaviors of the informal workforce may not be clear.
Financing
Emrey listed three objectives of financing and insurance arrangement: (1) to create health insurance systems that will efficiently pool the losses associated with health risks so that in return for a premium (or tax), beneficiaries are protected from those losses if the insured risk occurs; (2) to ensure that risks of loss are spread and shared among many individuals; and (3) to find ways to create large pools of people to protect the stability of the health insurance scheme (Wang et al., 2011). To facilitate the financing process, Emrey suggested the following steps:
- Study the effectiveness of health insurance models that the country is currently using to finance health care.
- Examine other options for financing mechanisms for addressing the need for more resources, more efficient collection systems, more efficient purchasing systems, and involving other stakeholders, such as the private sector and informal workforce.
- Identify the political, social, and implementation considerations.
Emrey cautioned that the success of these steps depends on the availability of good data; otherwise the process can be misled. Two poten-
tial barriers to the inclusion of the informal workforce in the financing arrangements are not being organized or recognized as a population able to participate in a scheme and having poor—or nonexistent—data on the informal workforce for use in informing financing decisions.
Population Coverage
The basic objectives of population coverage are to reduce inequities and to reach frequently marginalized populations within society. As part of the effort to reach these populations, individuals are often grouped according to their relative ability to contribute as well as their relevant political, social, or cultural characteristics. Emrey stressed the importance
of having well informed, country-specific expertise when designing a system in order to be able to develop insights about the characteristics of the population and the different political, tribal, and cultural patterns of the country. Concerning population coverage for informal sector workers, Emrey said that the barriers may include the proximity of informal sector workers to service providers; the workers’ age, gender, and health status; and the special burden of HIV for informal workers who need both coverage and access to social welfare benefits.
Benefits Package
The benefits package specifies which services are covered and which are not. Developing a benefits package requires understanding the tradeoffs between benefits and available financial resources, analyzing who should pay for the services that have externalities, determining which services should be prioritized, and considering how to integrate these services into the health insurance system (Wang et al., 2012). Emrey said that determining what services should be in the benefits package is an important step in the overall design process which may need to be revisited several times.
Emrey said that there are a number of tools for designing benefits packages. However, the tools can be complicated to use and require projecting and modeling both costs and benefits. To ensure the inclusion of informal workers in the insurance system, Emrey suggested that the benefits package design should consider how to increase the utilization of services among the poor and how to achieve the widespread use of benefits for essential life-saving health interventions.
Provider Engagement
Provider engagement focuses on creating a payment system with incentives for providers and patients to improve quality and equity and to align health insurance policy goals with the choices of providers and with payment methods. Policy considerations may include access, quality, cost containment, inclusion of preventive versus curative care, simplicity, and the prevention of fraudulent behavior. Emrey suggested several important factors to study when addressing provider engagement: the supply of health care providers, options for adequate provider networks, and the mapping of providers to service areas with geographic information system tools. He also suggested the use of franchise models to guide the selection, contracting, and payments for quality services. Potential barriers to the inclusion of the informal workforce related to provider engagement are that providers may not be located near the places of work for
informal sector workers and that trust may be lacking between providers and the informal workforce.
Organizational Structure
Emrey stated that the organizational structure of the insurance system is critically important for aligning all of the system elements into an efficient arrangement that is accountable, transparent, answerable, and controlled. Several core components of the organizational structure include governance and management, provider services, consumer services, actuarial and risk management, clinical standards and quality assurance, and financial management. In terms of barriers for the inclusion of informal workers, Emrey said that governance arrangements and staffing may not be aware of the needs of the informal sector workers and that there are not many options for involving the informal workforce in policy development and management arrangement.
Operations
The operations component is the “back office” part of the system, and the relevant objective when developing an insurance system is to create operational functions that are adaptable, efficient, accountable, and sustainable. Within operations, Emrey identified several key functions: financial processes and management, contract management, marketing, and communications; enrollment and member services; utilization and quality management; premium collections; claims management; and information systems and monitoring. Emrey suggested that there is a promising opportunity to apply e-health and mobile health technologies to accelerate progress and improve the efficiencies of operations. For example, handheld devices, Internet connectivity, and arrangements with information systems are permitting the use of technologies and approaches that would have required huge investments in infrastructure in the past. Emrey said that including informal sector workers may be challenging because of the lack of a secure means for collections of payments and premiums. However, he added that examples like the RSBY smart card in India and M-Pesa in Kenya are demonstrating the potential for innovations to overcome this barrier. In India, the National Health Insurance Scheme, or RSBY, makes payments through a smart card system overseen by a third-party administrator. M-Pesa in Kenya is a cellphone device that serves as a means of transmission of funds and which has been used to arrange health insurance payments and other types of payments within rural and urban areas.
Monitoring and Evaluation
Most insurance arrangements are limited in their monitoring and evaluation mechanisms, Emrey said; however, he emphasized how important investments in monitoring and evaluation are for determining impacts and cyclical improvements, particularly given how complicated the systems are. Concerning existing tools, he said that tools have been developed for monitoring enrollments, reimbursements, financial performance, and the utilization and burden of the financial arrangement. However, Emrey posited it is probably the case in almost every country that the monitoring and evaluation arrangements are not giving attention to the informal sector workers.
To sum up his remarks, Emrey said that within the efforts to achieve UHC, involving different groups that are currently working with informal sector workers as well as private sector stakeholders is an opportunity to incubate new ideas in order to make better progress and overcome barriers to achieving UHC.
UNIVERSAL HEALTH COVERAGE AND THE INFORMAL WORKFORCE
Peter Berman, Harvard School of Public Health
Peter Berman from Harvard University provided an overview of the evolving definition of UHC since it has entered into the global political discourse, the challenges with how it is defined, and implications for including informal sector workers. Berman said that the initial discussions about UHC were broad and aspirational. The World Health Assembly in 2005 stated that a health system that provides universal health coverage would guarantee everyone access to all necessary services while providing protection against financial risk (WHA58.33, 2005).1 Berman acknowledged that no health system in the world achieves this goal today; still, he said, it is a notable goal that all should work to achieve. This kind of a health system would produce the highest attainable outcomes that a health system can achieve—top performances in terms of health output and status as well as financial protection. Berman said that since its entry into the global discourse, the definition of universal health coverage has been modified to be less aspirational and less broad. He used the following definition from the United Nations General Assembly resolution as an example:
___________________
1 World Health Organization Document WHA58/2005/REC/1. 58th World Health Assembly Decisions and Resolutions (accessed May 10, 2015).
Universal health coverage implies that all people have access, without discrimination, to nationally determined sets of the needed promotive, preventive, curative and rehabilitative basic health services and essential, safe, affordable, effective and quality medicines, while ensuring that the use of these services does not expose the users to financial hardship, with a special emphasis on the poor, vulnerable and marginalized segments of the population.2
To illuminate the challenges related to the definition of UHC as it has evolved within the global discourse, Berman pointed to some areas where there is debate about how it is interpreted. For example, it is not clear if access refers to the use or receipt of services; how basic versus necessary services are determined; or if an entitlement to benefits is the same as coverage. UHC has been defined in a complete sense, but how does one characterize or compare different positions on the road to UHC in terms of the coverage of some services but not others, the coverage of some population groups but not others, or the different degrees of financial protection?
In grappling with some of these issues that emerge within the definition, Berman recommended several areas to consider within each country context when addressing the inclusion of informal workers:
- What kind of “coverage” (e.g., services, financial protection) is currently available, and to whom (e.g., informal sector)?
- For instance, if government guarantees comprehensive free services, what is actually provided?
- Employers may provide financial coverage, but, again, what is actually provided?
- What should be the strategy for reducing missing coverage or expanding coverage to priority populations?
- Should government financing and delivery be strengthened?
- Should insurance coverage be expanded? Should it be expanded as a substitute or a complement?
Designing the right strategies for a particular country requires a sound diagnosis of the situation and the causes of gaps, a willingness to honestly assess the potential for remedies to address gaps, and developing capacity and learning from the experiences of others.
Berman listed a number of risks in the movement toward UHC:
___________________
2 United Nations General Assembly Document A/67/L.36, Global Health and Foreign Policy (accessed May 10, 2015).
- Unfunded entitlements
- Duplicative schemes competing for scarce funds (financing) or scarce delivery inputs (e.g., human resources)
- Multiple tiers of coverage entitlement (e.g., civil servants, formal sector workers, and the informal sector) fragment risk pools and are difficult to integrate.
UNIVERSAL HEALTH COVERAGE, INFORMALITY, AND WORKERS’ HEALTH
Ivan Ivanov, World Health Organization
Ivan Ivanov from the WHO expanded on some challenges in the inclusion of the informal workforce within the objectives of UHC and on specific OHS needs for the population.
While the primary objectives of UHC are to reduce the gap between the need for and the use of services, to ensure that the quality of health services is such that they improve the health of those receiving the services, and to provide financial risk protection, Ivanov emphasized that UHC is also about prevention and about the poor and vulnerable populations. UHC relates not only to primary care but also to secondary and tertiary care. It is not only a package of essential health services, but it is about needed services based on demographic and health status conditions as well as the expectations of the covered populations. It is not only about curative care, but also includes prevention, promotion, rehabilitation, and palliative care. It is not only about essential medicines, but it is also about health technologies. It is not about specific population groups, it is for all, including formal and informal workers and the poor and vulnerable.
Ivanov provided some comments specifically about UHC governance and the informal workforce. While the governance of UHC for informal workers should be held to the same standards and accountability as the formal sector, Ivanov said, the formal sector is typically better organized and able to lobby more effectively for arrangements that explicitly apply to it. This can result in separate governance systems, including separate information systems and management arrangements, for the formal and informal sectors. There are documented cases of formal sector organizations being reluctant to extend benefits to the informal sector and to extend the pools of health financing to members from the informal sector.
Ivanov suggested that a primary problem facing the informal sector is that countries lack the fiscal capacity and ability to collect taxes from the informal sector, which limits the capacity and resources that countries have to meet the needs of the informal sector. Other problems and challenges related to the informal sector reflect past policy choices
and implementation failures, such as the attachment to contributory based entitlements, fragmented pooling systems that reinforce underlying social differences and constrain redistribution, weak purchasing from general budget revenues according to bureaucratic line item practices, and unclear and poorly communicated entitlements. Because of these historical arrangements, Ivanov suggested that inclusion of the informal workforce will require distinguishing between the problems that have been inherited and those problems that arise from the financial mechanisms and schemes that can be changed. Ivanov said that UHC will likely be one of the targets for the Sustainable Development Goals, thus the topic is attracting significant political attention. However, in many countries redressing the past inequalities within the health system is a challenge.
In including informal sector workers as a recognized population with unique needs and services, it will be important to understand the burden of occupational health risks. Ivanov suggested that occupational risks are
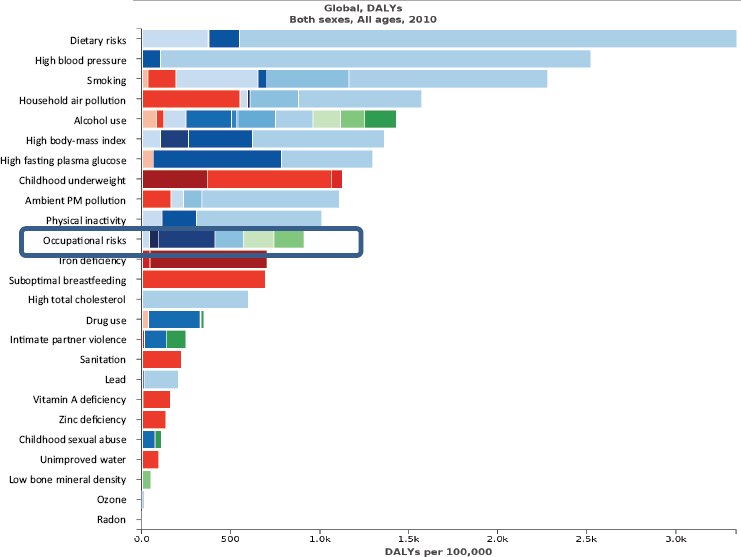
NOTE: DALY = disability-adjusted life year; PM = particulate matter.
SOURCES: Ivan Ivanov presentation to workshop, July 29, 2014; data from IHME Global Burden of Disease 2010.
sufficient to justify special action on the health of workers in the context of UHC. Occupational risks are among the 10 top risks that determine the burden of disease and disability worldwide (see Figure 2-5) and lead to the deaths of about 2.3 million people every year and cost more than 60 million disability-adjusted life years annually. Furthermore, much of this burden falls during the most productive part of people’s lives, in the age interval between 30 and 39 years of age (see Figure 2-6), leading to an enormous impact on productivity. Occupational risk costs to society amount to an annual financial loss of approximately 4 percent of gross domestic product.
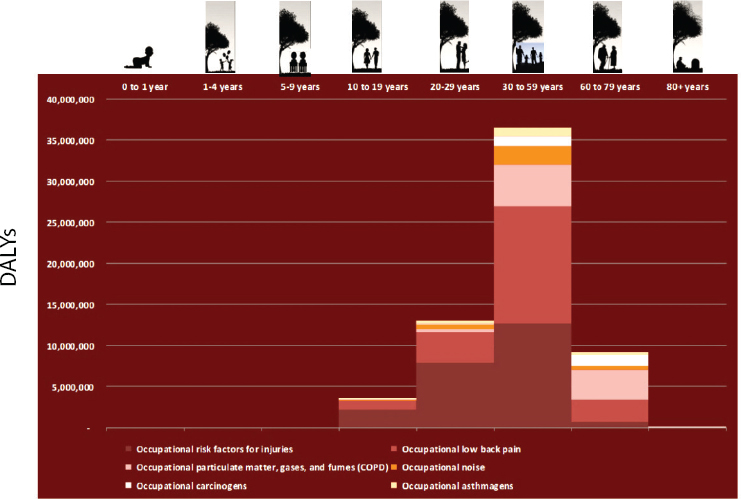
NOTE: DALY = disability-adjusted life year.
SOURCES: Ivan Ivanov presentation to workshop, July 29, 2014; data from ILO, WHO Global Health Risks 2010, IHME Global Burden of Disease Estimates 2010.
In discussing the burden of occupational risks and how to better understand occupational health needs for specific populations, such as informal sector workers, Ivanov shared a figure that listed the factors that determine the health of workers, such as their working environment, health behavior, social factors, and access to health services (see Box 2-2).
PARTNERSHIPS AS A MECHANISM FOR PROGRESS
Victor Dzau, National Academy of Medicine
One of the focuses of the workshop was exploring opportunities for public–private partnerships (PPPs) to advance the inclusion of informal sector workers in universal health coverage and occupational health and safety in developing countries. To illuminate the potential of PPPs for accelerating progress, Victor Dzau, president of the National Academy of Medicine, shared insights based on his experiences with partnership development. Dzau said that solving a complex global problem requires
multisectoral partnerships. Each sector offers different skill sets, expertise, resources, and perspectives for solving complex problems, such as those faced in health and health care.
As with many complex global problems, Dzau said, when it comes to addressing the challenge of universal health coverage and OHS for the informal workforce in developing countries, there are two ingredients necessary for success: innovation and implementation. In under-resourced countries and communities, innovation provides opportunities to change the way that things have traditionally been done to solve complex issues. There is evidence of innovations and solutions on the ground in LMICs, but the innovators there face many problems in implementing, sustaining, and scaling their work. The result is that even excellent innovations often remain quite local and small; scalability and replication are not easy. Dzau stated that once one comes up with an original idea, it is necessary to figure out business modeling, financing, and regulatory barriers, among many other issues. Dzau suggested that PPPs are a mechanism to bring together expertise from the private sector, public sector, academia, and
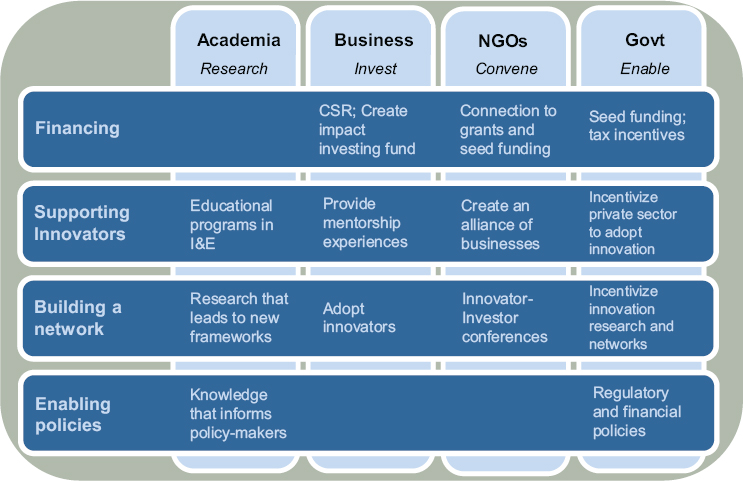
NOTE: CSR = corporate social responsibility; I&E = innovation and entrepreneurship; NGO = nongovernmental organization.
SOURCE: Victor Dzau presentation to workshop, July 29, 2014.
nongovernmental organizations, to help innovators scale and replicate, so that their ideas can move beyond pilots and become large-scale solutions.
Dzau also said that PPPs can support innovations through financing, specific knowledge and expertise about management systems and platforms to help increase reach, incentivizing the sharing of resources, and enabling a policy network or framework to integrate innovation into public health systems. To provide context on how multiple partners and sectors can contribute to and accelerate progress toward universal health coverage and OHS for informal workers in developing countries, Dzau shared a framework that he had developed to illuminate what different sectors bring to the table in PPPs (see Figure 2-7).
UNIVERSAL HEALTH COVERAGE AND OCCUPATIONAL HEALTH AND SAFETY FOR INFORMAL WORKERS: A VIEW FROM INDIA
Mirai Chatterjee, SEWA Social Security
To provide an example of the problem that is being addressed by the workshop, including its challenges and the opportunities for addressing it, Mirai Chatterjee, director of the Self Employed Women’s Association (SEWA) in India, gave a presentation on universal health care coverage and occupational safety and health for the informal workforce in India. SEWA is a national union of nearly 2 million informal workers.
Drawing on inspiration from Mahatma Gandhi and his call to start with the poorest and the weakest and, from them and from that experience, to allow ideas for action to emerge, Chatterjee shared the stories of two SEWA members, Rajiben Chavda and Fatimaben Sheek. Rajiben is a small farmer who owns a small plot of land with her husband. When the rain fails or their yields are low, she will also work as a laborer, breaking stones along with her husband to make roads in the town nearby. Rajiben is also a community health worker at the LokSwastha Health Cooperative, along with 400 other women. She provides basic health education, simple dos and don’ts, linkages with the public health system, and referrals for emergency and immediate care. Rajiben also promotes and provides information about two health programs: the national health insurance scheme, which largely serves below-poverty-line families, and the health insurance cooperative VimoSEWA, which serves both those below the poverty line and those above the poverty line. In particular, VimoSEWA serves large numbers of workers who do not qualify as being below the poverty line but who are still poor and vulnerable.
Fatimaben, the second SEWA member Chatterjee spoke about, is a kite worker. She is from the city of Amirabad and makes about 1,000 kites
per day from her home. From this work, she earns about 120 rupees per day, approximately US$2, which keeps her family fed and her children in school. Fatimaben suffers from heavy bleeding, and the doctor advised a hysterectomy, but because she does not qualify as being below the poverty line, she was not part of the national health insurance plan, and she has been unable to afford the operation. Recently, her daughter had an emergency appendectomy which cost about 15,000 rupees, approximately US$250, which the family had to cover out of pocket (OOP). A few years ago Fatimaben joined SEWA. She now uses SEWA’s childcare center and is able to work more and provide better for her family.
Chatterjee emphasized that Rajiben’s and Fatimaben’s lives mirror those of thousands of informal workers, not only in India, but all over the globe. In India more than 94 percent of the workforce—or more than 430 million workers—is informal. These workers are poor, they are hardworking, and they work long hours. Theirs is a lifelong quest for basic security, including work security and social security.
Chatterjee said that many of the SEWA members see work security and social security as two sides of the same coin. In SEWA, social security refers to a minimum of health care, childcare, insurance, pension, and shelter, including basic amenities such as a tap and a toilet in every home. As in many countries, health care tops the list, as the lack of basic health care leads millions of families into poverty. It is estimated that about 60 million Indians fall into poverty every year due to sickness and health expenditures (Shepherd-Smith, 2012). A recent McKinsey Global Institute report on poverty in India calculated that 680 million Indians, or about 56 percent of the population, are without basic services, including health care, water, and sanitation. In India, OOP expenses account for about 67 percent of all health care costs (McKinsey Global Institute, 2014). Often, families sell their land or other belongings to save and care for a loved one. SEWA has its own bank, and Chatterjee said that sickness is the number one reason for SEWA members to take out loans from that bank. Thus, she suggested, a lack of health coverage is trapping individuals into a debt–poverty cycle.
Universal Health Coverage in India
According to Chatterjee, the provision of UHC in India is a major anti-poverty measure that is firmly on the national agenda. However, actually reaching all Indians is a huge challenge, given the large and diverse population.
In 2010 the Planning Commission of India set up a small team to develop an architecture for universal health care, and that commission developed a definition for India of UHC: “ensuring equitable access for all
Indian citizens, resident in any part of the country, regardless of income level, social status, gender, caste or religion, to affordable, accountable, appropriate health services of assured quality (promotive, preventive, curative, and rehabilitative) as well as public health services addressing the wider determinants of health delivered to individuals and populations, with the government being the guarantor and enabler, although not necessarily the only provider, of health and related services” (Planning Commission of India, 2011, p. 3).
Chatterjee stressed that equity is at the core of this definition, which is based on the recognition that lack of access to health care is both a continuing cause and a symptom of poverty and exclusion. The definition also recognizes that the government can play a crucial stewardship role but that it cannot be the only provider (currently about 80 percent of Indians seek private care for their health needs). What is envisioned by the planning commission are partnerships between government, private health care providers, the insurance industry, civil society, including workers’ organizations like SEWA, and citizens themselves.
The commission based its recommendations on how to establish UHC in India on 10 principles:
- Universality
- Equity
- Non-exclusion and non-discrimination
- Comprehensive care that is rational and of good quality
- Financial protection
- Protection of patients’ rights which guarantee appropriateness of care, patient choice, portability, and continuity of care
- Consolidated and strengthened public health provisioning
- Accountability and transparency
- Community participation
- Putting health in people’s hands
After discussions with various groups, including community-based organizations; state government officials across the country; doctors, nurses, and their associations; and the pharmaceutical industry and insurance companies, the commission recommended a national, essential health package that would cover primary, secondary, and tertiary care. This essential health package is yet to be finalized, and consultations are under way. There will be room for flexibility and inter- and intra-state variations in health care needs. But a basic package will be guaranteed to all, including outpatient and inpatient care, provided free of cost from government or contracted-in-private providers. Free essential drugs will be part of the basic health package.
It was decided that the package will cover high-cost, relatively low-frequency health events but will not be used as a financial protection mechanism for more common illnesses. This decision was based on previous examples where such inclusion has driven up costs and proved to be unsustainable in the long run. Also, with a large population of informal workers who have no easily identifiable employer—or no employer at all—the costs of collecting premium or contributions would be high, and the mechanisms would be difficult to set up. Currently, some state governments and the national government are running health insurance programs, with mixed results. These programs have been found to use up significant amount of resources at the expense of primary health care. Furthermore, these health insurance programs are not linked to preventive care, nor are they integrated with the health system. For all these reasons, the emphasis of the UHC provision is on primary health care with a preventive focus and on insurance as a support, but not lead intervention. SEWA’s own grassroot-level experience of providing health insurance to women suggests that this model will be successful.
Chatterjee provided an overview of what the commission has proposed, which has been broadly accepted and what the government and others in India should undertake over the next 10 years. Rather than discussing all of the details, she focused on some essential pillars of the UHC architecture, some of which are already in place and others of which will be worked out over the next few years.
Increased Investment
Chatterjee said one of the major recommendations for UHC in India is to increase the central and state governments’ investment in public health from about 1.2 percent of gross domestic product (GDP) to 2.5 percent by 2017 and to 3 percent of GDP by 2022. Chatterjee said that such a change would reduce OOP spending by about half (Planning Commission of India, 2011), affording financial protection for many citizens. The funding would come from general taxation.
Essential Medicines
Another key recommendation from the planning commission of India is providing all medicines included on the WHO list of essential medicines free of charge. This policy has already been implemented by several state governments and has been announced in the national budget by the new government, in response to the fact that almost 74 percent of OOP expenses are accounted for by drugs (Planning Commission of India, 2011). This recommendation from the planning commission will involve
many changes in the current drug policy and will require new systems of procuring drugs and even promoting the growth of India’s large and competitive indigenous drug industry.
Primary Care
Chatterjee said that primary health care will be the cornerstone of UHC, and in the proposed architecture it will account for 70 percent of all expenditures. This figure will include investments in human resources at the local level—front-line workers, paramedics, nurses, and a new category of doctors trained in public health. It is this team that will provide the first-line care, screening patients and referring them as appropriate to secondary health care.
Human Resources for Health
Investing in human resources for UHC is the fourth recommendation from the planning commission. This investing should focus mostly on community-level workers but also on doctors in states where there are the greatest shortages. The goal will be to achieve at least 23 health workers per 10,000 people, as is recommended by the WHO. To achieve this, Chatterjee stressed, significant changes must be undertaken in medical and nursing curricula, in increased investments in other health workers through state and district-level training and research institutes, and in ensuring quality education. One mechanism to meet the human resource challenge is to create a new public health cadre, with people professionally trained in public health and the administering of UHC. This has already been found to be effective in the southern state of Tamil Nadu, a leader in public health and a state with among the best health indicators in the country. Another mechanism is to engage with and harness human resources, both doctors and others, from India’s indigenous and traditional systems of medicine such as Ayurveda. As there are many of these doctors and healers in India, this represents a great opportunity.
Community Engagement
The fifth recommendation from the planning commission is to engage communities and citizens in their own health and well-being. Given the diversity of the population in India, Chatterjee said, communities need to be equipped to assess their own needs and then to act to improve their own health, with the government and the private sector supporting and enabling the process. To this end, local health committees in both rural and urban areas—with representatives that include local
leaders, members of civil society and women’s groups, and public health functionaries—are being entrusted with budgets to undertake health-related action, including providing extra food to malnourished children, ensuring that clean water reaches all, and arranging for garbage disposal. UHC reform in Thailand has provided an example of how to develop such mechanisms, with the country’s system of health assemblies from the local, regional, and national levels used to determine health priorities and, ultimately, to act for health.
Regulations and Standards
India has one of the largest unregulated private health care industries in the world and there is variation in quality standards among private and public health providers and institutions. Chatterjee said that patients have very little bargaining power. For these reasons, UHC in India will be regulated with standard treatment protocols, rational therapy, and cost regulation. The private sector will be very much involved in UHC. However, it will have to adhere to standards of treatment, quality, and costs.
Chatterjee acknowledged that regulatory systems and laws will not be easy to develop and monitor. She stressed that significant dialogue will be required with doctors, hospital associations, and others, so that there is consensus and not resistance to regulation, adhering to standard treatment protocols, and accepting ceilings on charges to patients. The move to regulation in the health sector is slow, but she predicted that policy makers and others will eventually recognize that this is essential.
Urban Health
Another recommendation from the planning commission is that there should be a focus on the health of urban India. Nearly one-third of all Indians live in urban areas, where there is a lack of appropriate health infrastructure, especially of primary health care centers. The result, Chatterjee said, is that hospitals are full of patients who could have been screened and treated near their homes, instead of waiting in long queues in large tertiary care facilities.
Social Determinants of Health
Chatterjee emphasized that UHC cannot be achieved without positive steps to address the social determinants of health, including improving water and sanitation, instituting measures to end hunger and to improve food security, improving education, developing measures to promote women’s equality, increasing employment opportunities, and providing
regular and decent work and income for all Indians. While addressing all of these determinants may seem like a daunting task, Chatterjee said that she has learned from her experience at SEWA that there can be no shortcuts. It is this integrated approach to people’s well-being that will ultimately lead to a reduction in poverty and improved health. UHC is part of the fight against poverty, and it will be realized only if adequate attention is paid to social determinants.
Occupational Health and Safety for Informal Sector Workers in India
Chatterjee said that SEWA’s 40-plus years of organizing women for work security and basic social security, including health care, supports the approach chosen by India for UHC. She suggested, however, that there are some gaps that will require special attention. One of the major gaps is OHS, especially for workers engaged in the informal economy. Informal workers account for more than 94 percent of the Indian workforce and for more than 50 percent of the nation’s GDP, yet their occupational health has remained neglected, particularly for women in the informal economy.
Chatterjee suggested several reasons for the neglect of OHS for informal workers: the overall neglect and underfunding of health care, the difficulty of organizing informal workers into their own unions and cooperatives which would enable them to raise these issues, continuing gender inequality and a limited understanding of women’s health, and a poor research and evidence base.
In April 2013, SEWA organized a national conference on the occupational health of women workers in the informal economy. The conference was carried out in partnership with government, some employers, ILO, the WHO, researchers from occupational health and design institutes, and some workers from the informal economy. It was supported by the WIEGO Network. WIEGO arranged for colleagues from South Africa and Brazil to describe their experiences in occupational health and speak about how their services are integrated into their public health systems and into UHC.
Chatterjee said that the key issues discussed at the conference were that there is an absence of a policy on OHS for informal workers; that partnerships have great potential to lead to safe work tools and processes and to higher productivity and incomes for workers; and that there should be a greater awareness about occupational health all around—among workers, researchers, employers, and health care professionals. The conference was a first step toward a nationwide process of consultation with unions, workers’ groups, employers’ associations, researchers, policy makers, and legislators. This process was led by the National Advisory Council, a body of advisors to the government from civil society.
From these nationwide discussions, a set of recommendations was developed; these recommendations have been accepted by the government and are awaiting implementation. Chatterjee highlighted some of the recommendations that were proposed via this process. The first recommendation Chatterjee highlighted was that a task force should be assembled, consisting of government representatives, OHS professionals, researchers, employers and workers, and their organizations, with the goal of the task force to develop a national OHS policy that will adequately recognize the needs and reflect the realities of India’s workforce. This task force would be under the stewardship of the Ministry of Labor, but with the ministries of health, agriculture, and women and child development, among others, also in the task force. The focus would be on how to implement the policy by developing programs and mechanisms, adequately financed, that will reach the poorest and most vulnerable of workers.
A second recommendation was that a national database on OHS should be developed that includes data collected at state and central levels. While there are significant gaps in data, she said, there are enough data to get started, and the data need to be put together and shared widely.
The third recommendation Chatterjee noted was that OHS services should be integrated with primary health care and UHC, so that primary health care workers recognize possible work-related diseases and that workers are screened and referred in a timely manner to higher levels of care. Another recommendation was to invest in educational programs from schools onward in order to develop awareness among workers and the general public, with the aim of enabling prevention and the early detection of conditions. There is a huge gap of knowledge and information among workers, despite the fact that they suffer daily and that there are known ways to prevent many conditions.
The fifth recommendation was for the development of tools and equipment to safeguard workers’ health and productivity—an area that Chatterjee suggested can only be addressed by partnerships. Chatterjee said that SEWA has found that the low-cost development and production of tools and equipment leads to significant productivity and income increases for these poorest of workers. It also leads to a reduction in drudgery and in the aches and pains that workers experience daily but that are often ignored because they are not life-threatening or else because they are poorly understood. SEWA’s experience with partnering with others to improve tools and equipment has shown that there is much to be learned by all involved. One challenge is the cost of some of the tools. An improved sickle for Rajiben costs US$2, which even she could afford. And Fatimaben’s income increased by US$8 per day with the improved
kite-making table she got from SEWA. But she and other kite workers cannot afford to buy the new table, which would reduce back pain but costs US$35. There is a strong case for cofinancing such tools by employers through the governments’ workers welfare boards and even loans from neighborhood banks.
A sixth recommendation was to invest in the development of more health care professionals in the OHS sector—in particular, in those willing to research and develop services for informal workers. The task force suggested starting with training programs for existing primary health care doctors, nurses, and other frontline workers.
The final recommendation Chatterjee mentioned was that the state governments, the main implementers of all health services, and the relevant government ministries should undertake OHS impact assessments in their sectors before undertaking new development programs and projects.
Lessons Learned from SEWA
Chatterjee closed her remarks by sharing what SEWA has learned over the years about the broader vision for UHC with a special emphasis on informal workers. She said that improving the health of workers and others is a long-term endeavor that requires action at both the macro and micro levels. A strong base of workers’ and people’s organizations can help ensure that the recommendations from the UHC commission reach the most vulnerable in society, including informal workers. Chatterjee suggested that the political economies of villages and urban settlements, the exploitative nature of work arrangements, the lack of essential services and basic social security, and other factors lead to the perpetuation of sickness, deprivation, and poverty. Thus, she said, the struggle for OHS and UHC is closely linked to the struggle for justice in the workplace and in society and to the struggle for gender equality for women workers facing discrimination and violence within their very homes and families. The various barriers and hurdles can only be overcome when people come together, organize for their own rights, and find local solutions to their own health problems, with the government and others as enablers and supporters. Her SEWA experience has shown her, Chatterjee said, that frontline health workers like Rajiben are key.
Chatterjee suggested that it is not the lack of resources that is the major challenge but rather the lack of political will and an inability to develop strong partnerships and to include all in the long journey for OHS and UHC. India has acknowledged the gaps in policies at the macro level for UHC and is willing to engage with others in the search for solutions. It has recognized that poverty reduction and health improvements must go hand in hand. Meeting the challenges ahead, Chatterjee stressed,
will require much greater investments, greater political will, and more partnerships.
DISCUSSION
In response to Emrey’s and Dzau’s presentations, Roger Glass from the Fogerty International Center of the National Institutes of Health said that although the topic of research had not entered the conversation, there are significant contributions that it can make. As examples of research that could make such contributions, he mentioned research on conditional cash transfers, delivery mechanisms, and innovation through mobile technology.
Derek Yach from The Vitality Institute said that he noticed a contrast in the presentations between the opportunities and potentials for tackling the issue through innovation and partnerships and the view that currently progress is slow. Yach urged the workshop participants to think about how innovations in technology and insights into behavioral economics can transform opportunities in LMICs.
In response to a question from Paurvi Bhatt about the inclusion of services for the management of noncommunicable diseases within the benefits packages that are being designed, Emrey said that while there is certainly a growing awareness within the global health community about the burden of noncommunicable diseases in LMICs, in many cases the resources have not been made available through any financing arrangement or delivery system to adequately cope with the growing burden that those diseases present. In any country, from India to small countries in sub-Saharan Africa, designing the benefits package requires working with the resources available to cover the costs. There has to be a political and rational economic conversation about how to align benefits packages with needs and resources. Fortunately, there are readily available tools with which to look at a benefits package and try to perfect it in a way that more fully addresses the burden of disease and covers parts of the population that do not yet have coverage, but there is no way to cover everything for everybody tomorrow; it will take time. However, Emrey stressed that while conversations about benefits design need to be both reality-based and evidence-based, there are opportunities for innovations to provide some solutions for how to cover more services with given resources.
Martha Chen from Harvard University commented on the burden of disease from the perspective of informal workers. Chen said that there is a need to better understand the burden of chronic disease on these workers, whose only asset is their labor, and how that burden affects their earning opportunities. She added that the indirect costs of disease include the
opportunity costs related both to earning income and to negotiating the bureaucracy in order to access the health services.
In response to a question from Bob Bollinger of Johns Hopkins University about the potential to leverage innovation and technology to enhance and accelerate community participation and the accountability and transparency of developing communities of health, Chatterjee mentioned several promising opportunities, some of which are very low tech and low cost. For example, some states have written details about services in the local language on the walls of the primary health center so that people know what services and medicines they are entitled to and which are free of charge. Another example is instituting certain community processes into the government public health system, including a social audit, which involves periodically sending a joint team of public–private community organizers into communities and holding large public meetings. Chatterjee said that it is not easy for people to speak out, particularly women, but slowly they will begin to speak out, and this provides a public platform so that they can democratically exercise their right to ask questions and to find out more information; meanwhile, the public health authorities and the private providers can hear from the communities. Chatterjee also mentioned promising opportunities that use technology. One example is Swasthya Slate, a tool being developed by the Public Health Foundation of India. It is a small tablet for frontline health workers that can be used to collect data to be sent and shared centrally. Putting this type of tool in the hands of frontline workers who are more concerned about their neighbors’ children than anybody makes it more likely that authentic data will be provided.
Peter Berman commented on the shifts between formal and informal employment. Given the data from countries where 50, 60, or even 90 percent of the workforce is informal, he asked, what does it mean to be formal in those countries? The data on the size of the informal workforce indicates a profound transformation in the model of the future of employment and services. Historically the assumption has been that people would move into formal sector employment and that some combination of the state and formal sector employers would assure their coverage. Countries differ greatly in their arrangements for care, for example, in whether it takes place through mandates or through taxes. Although the mix of the arrangement differs from one developed country to another, there is usually the same outcome—that is, that nearly all individuals have fairly good coverage with a fairly good package of benefits. Considering this, Berman asked, Is this model delayed, or is it profoundly restructuring in a world that has changed? He said that there has been a growing concern that UHC could increase informality, because with more
public-sector coverage there can be less responsibility placed on employers for providing coverage.
Francie Lund from WIEGO highlighted the complexity of establishing a defining line between formal and informal workers through the example of a large factory producing car parts. The informal workers are not outside of the factory. They are inside in a corner working for themselves by making belts to put into the engines. However, when a new large order comes in, they are pulled in under contract for several weeks to work on filling that particular order. Drawing a line and defining whether these are formal or informal workers and whether they should be the focus of different interventions is very complex.
Charu Garg from the Institute for Human Development in India brought up the example of another subpopulation that adds complexity to the discussion—informal sector workers who have stopped working because of age or illnesses. If individuals in this subpopulation develop diseases or conditions based on their previous exposure to occupational hazards, Garg asked, then how are those conditions to be defined and treated?
This page intentionally left blank.
































