
5
Select Country Experiences
Many countries have the challenge of meeting the demands for the provision of quality health services to its varied populations. With a purposeful sampling of countries and diverse perspectives from the public and private sectors, the workshop included a number of presentations that explored efforts within countries to achieve universal health coverage or occupational health and safety, or both, for the informal workforce. For several countries, more than one speaker presented a perspective on the country’s efforts as a way of providing diversity and depth to the depiction. The presentations included in this chapter are organized alphabetically based on the country of focus.
BRAZIL: BUILDING THE NATIONAL OCCUPATIONAL HEALTH SERVICES NETWORK: AN EXPERIENCE WITH UNIVERSAL HEALTH CARE PROVISION
Vilma Santana, Federal University of Bahia, Brazil
Vilma Santana from the Federal University of Bahia in Brazil described the experience of developing occupational health services (OHSs) in Brazil. Brazil is a large country with more than 200 million citizens and the world’s seventh largest economy, which has a major focus on food production. Santana shared that since the late 1990s, social policies in Brazil, including those focusing on universal health coverage, have been strong, and she suggested that many of the gains in the human develop-
ment index for Brazil in the last several decades have been the result of a focus on social development and policies. Santana provided some statistics to give a brief overview of the world of work in Brazil: There are more than 100 million workers, 20 percent of whom are rural workers, 44 percent are women, and 22 percent are living below the poverty line. Child labor is illegal under the age of 14, and decreasing child labor through policy efforts is currently an important social issue. The portion of the workforce that is informal is significant but has decreased in recent years, from 51 percent in 1999 to 42 percent in 2013.
Santana then described the institutional framework for workers’ protection in Brazil, which includes the ministries of social insurance, labor and employment, and health. The social insurance ministry provides compensation benefits for sickness-related disability, both occupational and nonoccupational, and pensions. This set of benefits is limited to registered workers who contribute 8 percent of their paychecks toward social insurance. The labor and employment ministry provides labor protection through the occupational health and safety authority, which carries out workplace inspections and various other safety-related measures. The labor protection measures are universal but apply only for specific legal issues such as bonded work, child labor, and illegal wage workers. Thus, informal workers are excluded from this aspect of labor protection. The health ministry provides overall health care, clinical care at all levels of complexity, health surveillance, prevention, hazards monitoring, and health promotion. The health ministry also serves as the coordinator for universal free services. In Brazil out-of-pocket costs are universally free, with private firms providing supplementary health care services. Universal coverage is enshrined in Article 196 of the federal constitution of 1988: “Health is everyone’s right and a State duty . . . that is guaranteed by social and economic policies aimed at reducing the risk of disease and other hazards . . . and to provide universal and equal access to healthcare services intended to health promotion, protection, and recovery.”
The efforts in Brazil to provide universal health care (UHC) are undertaken through the Brazilian National Health System (SUS). Santana noted that SUS was created as a result of the health reform movement that developed in the 1980s after the fall of the country’s previous dictatorship. The health system was built by a coalition of parties and labor unions, academics, and intellectuals under the political claim that health is a citizen’s right and a state duty. It was based on the premises that the major asset of a nation is its people and that it is the nation’s workers who build the nation’s wealth. Santana emphasized that because health is a citizen’s right, health care cannot be treated as a commodity like other goods. SUS is directed by a set of fundamental principles: Coverage should be universal and include informal or formal workers regardless of sex, age,
and ethnicity; health care should be equitable; there should be free access at all levels of the system; the health system should be integrated across all public management levels; health care should focus on prevention and health promotion; and the system should be based on participatory management.
Within the SUS, occupational health is integrated into primary health care services at the federal, state, and local levels. In every state there is a workers’ health state center which provides specialized expertise and support to all workers through Reference Centers for Occupational Health (CERESTs). There are more than 200 CERESTs distributed throughout Brazil which provide support to primary health care, family health programs, and community health agents at the household level. Santana noted that the centers provide occupational health and safety services which include clinical assistance, diagnosis, treatment, and recovery as well as workplace inspection, identification of hazards, and treatment of the hazards.
Some examples of the activities that CERESTs carry out are health promotion and protection based on priorities drawn from local epidemiological data; education and community participation through workshops, rallies, and local health councils; and enhanced dialogue with social movements, labor unions, and organizations. Additionally, Santana pointed out that CERESTs map all local economic activities, including the informal workforce, and they identify industry trades that have higher OHS risks, both in the formal and the informal economy.
Despite the progress that has been made in Brazil to provide UHC, to integrate OHS into UHC, and to target both formal and informal workers, Santana noted that there are still challenges remaining. There is a lack of training in OHS among health workers, for example, and the participation of informal workers in local or state OHS counsels is often weak because they are not well organized. Underfunding is also an issue. Furthermore, the geographic areas covered by some CERESTs are quite large, and access to and from these regional centers can be challenging because of the distances and poor road conditions.
INDIA: INEQUITIES IN FINANCING, COVERAGE, AND UTILIZATION OF HEALTH CARE BY INFORMAL SECTOR WORKERS
Charu Garg, Institute for Human Development, India
Charu Garg from the Institute for Human Development in New Delhi spoke on financing coverage and utilization among informal sector workers in India. According to 2014 data, almost 83 percent of the 487 mil-
lion workers in India that work for small enterprises (defined as having fewer than 10 employees) are informal sector workers, with another 9 to 10 percent working as casual laborers on a contract basis in the formal sector. The primary industries in which they are concentrated are agriculture, construction, shops and establishments, cigar manufacturing, waste management, food service, transportation, and home-based work. Some of the major occupational health problems that have been recognized are injuries due to accidents; chronic respiratory/lung diseases (asthma, chronic obstructive pulmonary disease, pneumoconiosis, and silicosis); musculoskeletal disorders (such as low back pain); skin diseases (contact dermatitis); noise-induced hearing loss; poisonings, especially due to pesticides; lung cancer; leukemia; and certain infectious, parasitic, and mental diseases.
Within the financing and delivery mechanisms for covering formal workers in India, financing is provided mainly by government and employers, with small premiums from employees. Comprehensive benefit packages include an entire continuum of care, including prevention, promotion, outpatient, inpatient services, medicines, and diagnostics. Garg noted that delivery is provided through a mix of public and private facilities.
After providing some perspective on the schemes and services available for formal sector workers, Garg presented a table with the major government initiatives to cover informal sector workers (see Table 5-1).
The Rashtriya Swasthya Bima Yojana (RSBY), which is the largest initiative for informal sector workers, covers about 400 districts across 27 states. It is financed through a mixture of contributory and noncontributory schemes. The center and the state split the financing 75 percent and 25 percent, respectively, and the beneficiary pays only a small registration fee. For example, the smart card costs only 30 rupees. For individual premium for the Yeshaswiny scheme is 200 rupees, and the other four schemes are entirely financed by the government. The benefit package mostly covers tertiary hospitalization and maternity care, with limits on the cash disbursed per unit per year per procedure. The annual inpatient benefits vary from about 32,000 to 192,000 rupees per family, and some schemes also cover secondary care but not outpatient care. There is some coverage for transportation, but the limit is about 1,280 rupees.
The government of India had provided coverage to the entire population in the public delivery system for nearly 30 years; however, the facilities and human resources had been limited and inadequate to serve the population needs and meet the standards for accessibility and acceptability. With recent reforms, the population coverage has improved significantly, from 55 million people being covered in 2003 to 375 million in 2014.
However, Garg stressed that the service is limited, covering only
TABLE 5-1 Financing and Delivery Mechanisms to Cover Informal Workers Presented by Charu Garg on July 30, 2014
| Scheme | State/ Year Started | Household Covered/Premiums | Annual Coverage per Household | Delivery – Hospitals Empanelled | Reimbursed in the Last Year (No.) | Implementing Authority |
| Rashtriya Swasthya Bima Yojana (RSBY) | 400 districts across 27 states | 37 million below poverty line (BPL) households and recently informal workers | Rs. 30,000 for a family of 5, plus annual transport limit Rs. 1000 | 11,000 | Approx 11 lakhs | MOLE + state nodal agency + insurer |
| 75%: 25% central and state government; Rs. 30 per beneficiary | 30% are public | |||||
| Rajiv Aarogyasri | Andhra Pradesh (2007) | 23 million Household’s annual income below Rs. 75,000 | Rs. 2 lakhs (family defined by BPL card) | 529 | Approx 4 lakhs | Rajiv Aarogyasri Trust |
| 85% state government | 20% are public | |||||
| Yeshasvini | Karnataka (2003) |
3 million households in a farmer’s cooperative
40–60% of reimbursements by state government + Rs. 200/enrolled |
Rs. 2 lakhs per member paying contribution. Secondary and tertiary and discounted medicines | 511 | 73,963 | Yeshasvini Coop Farmers Healthcare Trust + TPA |
| Scheme | State/ Year Started | Household Covered/Premiums | Annual Coverage per Household | Delivery – Hospitals Empanelled | Reimbursed in the Last Year (No.) | Implementing Authority |
| RSBY-CHIS | Kerala |
1.6 million household member of 25 workers welfare board
75%: 25% central and state government; Rs. 30 per beneficiary |
Rs. 2 lakhs (family defined by BPL card) | NA | NA | State government + insurer |
| CM’s -CHIS | Tamil Nadu (2011) |
13.5 million households earning less than Rs. 72,000
100% budgetary allocations |
Rs. 100,000 per family (defined in BPL card), Rs. 50,000 buffer | 850 + about 40 diagnostic facilities | NA | State government + insurer |
NOTE: CHIS = Comprehensive Health Insurance Scheme; CM’s= Chief Minister’s; MOLE = Ministry of Labour and Employment; NA = not available; Rs = rupees; TPA =Third Party Administrator.
SOURCE: Presented by Charu Garg on July 30, 2014; data compiled by author from available resources.
tertiary care and some medicines and diagnostics during hospitalization. There is limited financial protection for keeping individuals and families from falling below the poverty line from health expenses. Many of those who fall below the poverty line because of health expenses do so not because of hospital expenses but rather because of out-of-pocket expenditures for outpatient services and medicines. Garg also said that while there has been increased coverage, utilization has been limited. The barriers to utilization include a lack of knowledge about the availability of services, the stigma associated with certain conditions, and a lack of available facilities and providers.
Garg concluded that coverage has increased for informal sector workers but that the depth of coverage and financial protection is still very low. She suggested that the best way to improve the utilization of health services by informal sector workers, after coverage is increased, is to raise awareness of available services and remove the stigma associated with occupational diseases. On the supply side, risk assessment at the workplace, early screening, and better trained doctors at the first point of contact are required. To improve the benefits package design and better meet the needs of informal sector workers, Garg suggested that more robust data needs to be collected on the population characteristics and disease patterns of informal sector populations based on geographic locations, and more data is needed on the costs of services that are provided. She also stressed that more research needs to be conducted to illuminate the linkages between workers’ health and productivity and changes in the gross domestic product.
Mirai Chatterjee of the Self Employed Women’s Association (SEWA) also presented ideas for action from India (see Box 5-1).
INDONESIA: THE EFFECTIVENESS OF OCCUPATIONAL HEALTH INTERVENTIONS FOR THE INFORMAL SECTOR AND OPTIONS FOR DELIVERY
Hanifa Denny, Department of Occupational Health and Safety at Diponegoro University, Semarang, Indonesia
Hanifa Denny from Diponegoro University provided an overview of OHS interventions for informal sector workers in Indonesia, their effectiveness, and options for their delivery. She began with an overview of the situation in Indonesia. Indonesia’s population of 237 million people has a population density of 323.05 per square mile and is spread out over 17,000 islands. There are approximately 5,000 occupational health posts at the village level (POS UKKs) in Indonesia that promote occupational health as part of an initiative to empower communities through participation. POS UKKs are established where there is both a need and a willingness for volunteerism from workers, including workers in informal sectors, home industries, and small-scale enterprises. The government assists in setting up a POS UKK.
The activities of the POS UKKs are assisted by the community health centers, or PUSKESMASs. Denny noted that Indonesia has nearly 10,000 PUSKESMASs, which offer inpatient or outpatient services or both. Indonesia also has four referral centers specifically for occupational health services that were established as part of a pilot study.
Denny described the OHS government policies in Indonesia. In 2009 a law was passed to ensure coverage of occupational health services for workers in both the formal and informal sectors. In 2005 the scope of the Center for Occupational Health within the Ministry of Health was expanded under the new Directorate of Occupational Health. The annual budget for the Occupational Health Program has increased three-fold since 2005, from US$1.5 million to US$5 million currently. Fifty percent of the budget is for the delivery of occupational health services to informal sector workers. Besides the spending by the central government, a discretionary spending budget has been made available to the provincial health offices. Additionally, local governments contribute some money, although their funding is generally patchy and mostly engaged in pilot projects.
Denny listed several service delivery interventions for occupational health for the informal sector that have occurred in Indonesia:
- What started as pilot projects for the establishment POS UKKs in 2002 and 2006 has to date resulted in 5,518 operational posts.
- A pilot project focused on the establishment of the Center for Occupational Health Services in 2002 has resulted in five operational occupational health services referral centers.
- Occupational health risk mapping has been done by Directorate of Occupational Health together with some provincial health offices at selected provinces and workplaces, including informal sectors, home industries, and small-scale enterprises.
- Training volunteers for the POS UKKs (e.g., farmers, craftsmen, fishermen, traditional divers, etc.) is conducted by the Directorate of Occupational Health together with some provincial health offices.
- Occupational health training for PUSKESMAS personnel has been carried out for 3,000 PUSKESMASs in Indonesia.
- Training and technical assistance on occupational health has been provided for traditional divers and fishermen at Cilacap, Maluku, Riau Island, Semarang, Seribu Island, and Situbondo.
- Training on the diagnosis of occupational diseases was delivered and general physicians were recruited to participate.
- Occupational health guidelines and information education communication materials for informal sectors of specific occupations, such as farmers, traditional fishermen, traditional divers, and footwear workers, have been distributed.
- Since the enactment of the universal health care program in 2014, medical services in Indonesia have been free for any person who has obtained a Social Security card.
To illustrate the multisectoral nature of OHS, Denny noted that government agencies in sectors other than the health sector are involved, including the ministry of manpower and transmigration, ministry of agriculture, and ministry of industries.
Concerning the sustainability and scaling of OHS services for informal sector workers in Indonesia, Denny said that the primary issues are financing, technical assistance, service delivery, and relationships and partnerships. The success that Indonesia has experienced is based on the government’s supervision and assistance for PUSKESMASs, and the PUSKESMASs’ assistance to the POS UKKs and outreach programs aimed at improving the skills of workers in workplace hazard identification and solutions.
SOUTH AFRICA: SERVICES TO WORKERS IN THE INFORMAL ECONOMY
Barry Kistnasamy, Department of Health, South Africa
Barry Kistnasamy from the Department of Health in South Africa described the situation and characteristics of workers in the informal economy in South Africa and also the mix of services and interventions that are available to those workers.
Overall unemployment is high in South Africa, with only 17 million of the 53 million citizens employed. Of the 17 million workers who make up the labor force, 34 percent are informal workers. Thus, Kistnasamy pointed out, South Africa has a smaller percentage of workers who are informal than many other countries in Africa, such as Zambia, where 90 percent of the labor force is informal workers. However, the informal sector in South Africa still accounts for $30 billion, or 7.1 percent, of the South African gross domestic product. The largest portion of the informal economy is classified as retail (41.5 percent), with other significant contributions from transport (18.5 percent), construction (10 percent), and subsistence agriculture (9.3 percent) sectors.
Kistnasamy said that there is a sizeable population of migrant and cross-border workers in South Africa who are acutely vulnerable. Their informal employment is typically as farm workers and domestic workers. Many of the policy pronouncements and the legislative instruments in South Africa cover only workers in the formal economy.
In South Africa there are 15 million individuals who are covered by social security and poverty alleviation measures, such as child support grants, pensions that are means tested, and disability benefits. The key problem that informal workers such as street traders face in South Africa is that although they have a free primary health care service that they can access, they lose money whenever they leave work for health care or other reasons. Unlike the workers in the formal employment, where sick leave is covered by legislation covering basic conditions of employment, a street trader who leaves the job to visit a primary health care center may lose a day’s earnings, even though the care itself is free. So, invariably, such workers do not choose to use the system until the onset of a serious illness.
Concerning data on occupational health problems, Kistnasamy said that epidemiological studies are lacking and that workplace hazards are not well understood because there are no inspections of informal workplaces. The occupational health problems are often a combination of occupational hazards and poor living conditions. Poor working practices and conditions include long work hours, widespread failure to maintain
workplace facilities, the lack of even simple personal protective equipment, the absence of inspection authorities, the lack of an organizational base for support of workers, and the absence of a system for collecting, compiling, and disseminating information. Even if individual workers are aware of hazards and risks, there is little that they can do about the hazards, and they continue to work in risky environments.
Intervention models for addressing the occupational health and safety of informal workers are limited. Kistnasamy noted that the Brazilian and Thai models are examples from which to learn; however, in Africa there are very few models.
Kistnasamy suggested that several elements are needed in order to move forward in implementing effective interventions to address the occupational health and safety needs of workers in the informal economy in South Africa:
- Policy dialogue that is inclusive of political parties, ministries, organized labor, standing committees in parliament, relevant stakeholders, and the workers themselves
- Ongoing discussions at multilateral, regional, national, and technical levels
- An evidence base on the size and scope of the sector, its contributions to the economy, the risks and hazards that workers face, and existing interventions
- Capacity building and training for health professionals
- Surveillance that can create a loop from data to interventions
- A networking strategy that includes discussions with informal workers on agendas for change
- The promotion of safety, health, and environment activities
- Universal coverage and financing for a national health insurance model that covers informal economy workers
- Integration into the primary health care system
SOUTH AFRICA: OCCUPATIONAL HEALTH AND SAFETY: TOWARD THE INCLUSION OF INFORMAL WORKERS
Francie Lund, WIEGO Social Protection
To open her remarks, Francie Lund from Women in Informal Employment: Globalizing and Organizing (WIEGO) Social Protection offered several lessons learned from her experiences and the work of WIEGO in addressing OHS for informal sector workers:
- Employment is the most important way in which the benefits of economic growth can be shared.
- For poorer people, their own labor is their most valuable asset.
- The health of the worker and health conditions in the workplace are key factors in the quality of informal work.
- Informal workers have little autonomy or control in the places they work.
With these framing comments, Lund discussed efforts aimed toward the inclusion of informal workers in occupational health and safety (OHS). Within the formal sector, OHS is part of the legal obligation of employers, she said. There are inspectors equipped with standards and tools for the identification of problems, and there are clear paths for reporting injuries and diseases, appeal mechanisms for workers and employers, and rules for compensation. By contrast, the efforts by international organizations aimed at establishing OHS for self-employed small businesses and industrial outworkers tend to emphasize self-regulation, placing the responsibility largely with workers themselves. Lund said that WIEGO is attempting to go further in finding ways to extend OHS to informal workers.
Various forces of exclusion prevent informal sector workers from receiving OHS protections and benefits, Lund said, including a lack of recognition as workers and a lack of reliable statistics on informal work in labor force surveys. For example, surveys may ask a household whether an injury has taken place at home, but no distinction is made between work-related injuries and domestic violence–related injuries. Another force of exclusion is the lack of connections between governmental agencies, both vertically (between the national and local levels) and horizontally (between departments at the local level).
Lund listed several barriers to improving work conditions for informal workers. At the government level, resources for OHS are frequently insufficient even to cover the formal workforce. There is also a lack of coordination among departments, often because of a lack of political will rather than costs. Employers, especially those with disguised employment relationships, have no responsibility for the informal places of work or conditions under which producers or service workers work. Within the trade union movement, there is a lack of recognition of informal workers and their organizations. Lund also stressed that the informal workers themselves may be a barrier to improvement of working conditions. Their income is their priority. For example, headload porters are paid per load carried and thus may carry extra loads, which may to lead to injury to back and neck over time. Additionally, the high turnover of workers may mean that informal employers resist paying for health screenings, as
these are expensive. Furthermore, there is a lack of information among the workers about the consequences of poor work practices.
Lund described a 4-year occupational health project being carried out by WIEGO. The project is investigating the possibilities of an OHS discipline and practice that is more inclusive of informal workers, especially poorer working women. Urban sites in five countries were chosen for the project— Brazil, Ghana, India (two sites), Peru, and Tanzania—and informal workers from multiple sectors (such as street vendors and home-based workers) were included. The project seeks to understand better the risks faced by the different sectors of informal workers, how to modify legal and institutional barriers to inclusion. It is also analyzing whether the most important priorities are legal or resource deficits, and whether improvements could be made through better coordination and by working with organizations of informal workers to shape demands for OHS interventions. The project is building in-country research and organizing capacity in OHS for informal workers, to improve the collection of statistics, to contribute to the development of a module for data collection on OHS for informal workers in labor force surveys, and to contribute to the development and implementation of an expanded or alternative curriculum that integrates OHS for informal workers and work places into mainstream training institutions.
Lund noted that the main activities of the project include establishing partnerships in each country; carrying out research with worker groups on mobility mapping, risks and hazard analysis, and prioritization of problems; performing country-based institutional analysis and mapping of who controls, regulates, trains, and has resources for OHS; instituting policy dialogues at the local government level; and sharing best practices concerning national level policy change.
Lund offered several lessons that have been learned from work on the project over the past 4 years:
- A sectoral approach helps in understanding the challenges to and opportunities for inclusion of informal work and workplaces.
- Municipal infrastructure such as water, sanitation and lighting are vital to workers’ health, regardless of workplace.
- There is a need for a coherent, consistent, and supportive stance from local and national authorities.
- There are positive lessons from the active and enduring involvement of organizations of informal workers in health policy development.
- There is a need for greater and expanded support for an ergonomics focus for informal workers and workplaces.
- There are benefits of integrating OHS into primary health care, but such an action also risks losing the preventive component of OHS.
SOUTH AFRICA AND GHANA: LINKING OCCUPATIONAL HEALTH AND UNIVERSAL HEALTH COVERAGE
Laura Alfers, WIEGO
Laura Alfers described two WIEGO projects that have been conducted over the past 3 years with partners in Ghana and South Africa. She noted that while they are small projects, they illustrate some of the bigger problems with the institutional setup of health systems when it comes to covering informal workers.
Alfers pointed out that Ghana and South Africa have very different labor markets. Ghana has a much higher share of informal employment—more than 90 percent, versus around 33 percent in South Africa. Still, both countries have significant numbers of street and market traders, many of whom are self-employed and do not employ others. The street and market traders who were the focus of the project work in urban public spaces.
In both Ghana and South Africa the move toward universal health coverage has resulted in a move toward national health insurance schemes. Ghana has a national health insurance scheme which has been running since 2003. In South Africa there is a free public health care system, although the quality of its services can be limited. There is also a very strong private health care system in South Africa. Currently, a national health insurance plan for South Africa has been proposed and is in a pilot stage. Alfers said that these reforms address the imbalance between the private and the public sectors.
In Ghana the national health insurance scheme is a version of social health insurance that includes a voluntary component for informal workers to insure themselves. On the invitation of the Ghana Trades Union Congress, WIEGO conducted a small study on the barriers that informal workers face in accessing the scheme. Alfers pointed out that from the results of that study, although the cost of the premiums was a problem, especially for the poorer workers, and an even bigger problem was administrative issues on the ground and how long it took people to get registered.
In the field of occupational health and safety, one common institutional problem is a lack of coordination between the ministry of health and the ministry of labor. When dealing with informal workers working in open public spaces, there are additional layers of complexity—that is, the ministries of local government and, beneath them, the municipality’s
local government, including the departments of environmental health, waste management, and urban infrastructure. Alfers also said that, in the case of street vendors, workplace hazard problems are not limited to neglect in terms of non-provision of basic services to informal workplaces like sanitation and water; the municipal regulations can actively threaten the health and safety of these workers through violent evictions, the confiscations of goods, and the mental stress that street traders and market traders go through on a daily basis, knowing that they are constantly under threat from municipal regulation.
Alfers described the Accra Health and Safety Platform, which was started in Ghana in 2010. Its activities focus on building a platform for informal workers to engage with municipal institutions, including building the capacity of worker organizations so that they will be able to articulate their problems and concerns appropriately and in a strategic manner. The results of the engagements with local government have included the establishment of waste management committees, the provision of fire extinguishers, and the clearing of drains. Alfers noted that, through the Accra Health and Safety Platform, they learned that it takes many interactions on a constant basis to implement reforms. One of WIEGO’s goals is to institutionalize the platform for informal workers who, unlike formal workers, do not have bargaining councils and other platforms with which to communicate with employers and with governments.
In 2014, with a grant from The Rockefeller Center Centennial Innovation Fund, WIEGO adapted the Accra program to implement a project in Durban, South Africa. In collaboration with a local nongovernmental organization, Asiye eTafuleni, WIEGO helped to develop the Phephanathi Platform. The platform provides a basic institutional architectural framework in which a range of health interventions, including occupational health interventions, public health interventions, and urban health interventions, can be embedded. Alfers noted that at the center of the project is the Phephanathi Health and Risk Management Committee, made up of 12 elected traders from each of the markets in Warwick Junction in Durban. Each market has its own association of arbitrators, and they are trained now in basic first aid and fire safety. Municipal officials, local university occupation and environmental health departments, and public health officials also have been invited to join the platform. The committee helps to bridge the institutional divides among the national health services and the municipal health services. The platform also provides training in fire safety, first aid, and basic understanding of workplace hazards and in hazard mapping and the urban design process, including experimenting with crowd mapping technology and developing basic emergency plans and installing basic infrastructure.
In the future, the goals for Phephanathi Phase 2 are to partner with
universities that have specific knowledge on ergonomics, occupational hygiene, and workers’ health education; to facilitate health and hygiene mentorship systems among food vendors; to run health diagnostics camps; and to think about further urban design solutions.
THAILAND: UNIVERSAL HEALTH COVERAGE SYSTEM AND INFORMAL WORKERS
Somsak Chunharas, National Health Foundation, Thailand
Somsak Chunharas from the National Health Foundation in Thailand provided an overview of the universal coverage system in Thailand and how it applies to the informal workforce. In Thailand total health expenditures account for 3.9 percent of the gross domestic product, or US$194 per capita. However, Chunharas said that in the Thai experience, it is important to recognize that health reform did not start with financing but rather with system development. With the opportunity to develop the system gradually, Thailand managed to create a system at various levels from the grassroots level upward. The system includes a mix of private and public providers, with the private sector accounting for about 30 percent of all providers.
Chunharas mentioned several key historical developments in health financing in Thailand. Before 1975, the government had provided health security to civil servants on a retrospective reimbursement basis. Then, starting in 1975, the government provided indigent cards for the poor that granted free health services at public sector facilities. In 1990 social security was established, with health insurance as an integral component for formal sector workers. With the introduction of these new policies, coverage steadily increased. However, by 2001 around 25 percent of the population was still without any health security. At this time, the indigent cards for the poor were discontinued, and a general tax was instituted to start a new universal coverage system to cover those who were without coverage, including those previously covered by the indigent cards.
When Thailand started introducing reforms in 1975, the government had limited experience in managing money on an insurance base. The civil service medical benefits scheme that predated the expanded coverage reforms provided a starting point, Chunharas said. He noted that the government began monitoring the scheme and found that its spending had been excessive, partly because of the retrospective reimbursement on a fee-for-service basis. In 1990 the government started a social security system with the first per capita prospective payment financing model, and then it gradually moved toward a participatory policy process. Currently there are three systems working together: universal coverage, the Social
Security Scheme (SSS), and the Civil Servant Medical Benefit Scheme (CSMBS), with 75 percent of the population covered by universal coverage, and a total of 99.87 percent of the population covered by one of the systems. In the movement toward universal coverage, government financing through taxation has increased substantially, from US$25 per capita in 2000 to US$45 per capita in 2013 for the outpatient services; inpatient services have also been increasing.
In the benefit package there has been a continuous evolution of what is covered, as can be seen in Figure 5-1. The changes and additions to the benefits package have resulted from continuous review and revisions based on cost–benefit analysis, assessments of new technologies, and lobbying by advocacy and other interested groups. The system includes separate funds for specifically recognized special conditions, such as HIV treatment and renal dialysis. There is also a separate fund for prevention and health promotion.
Thailand created a separate organization within the ministry of public health to serve as the purchaser; this is the National Health Security
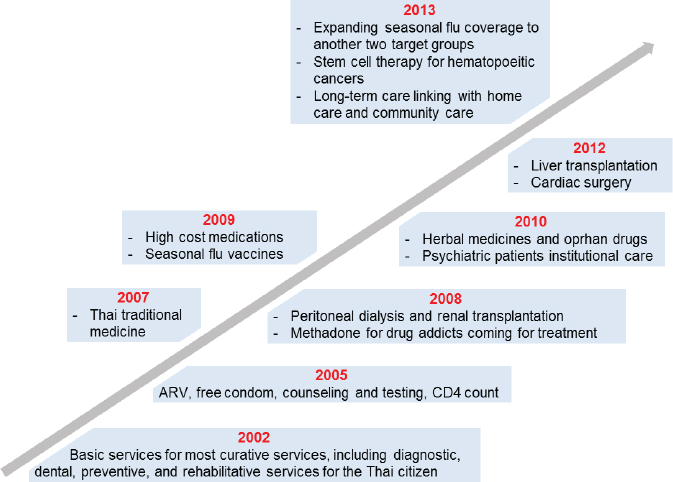
NOTE: ARV = antiretroviral; CD4 = cluster of differentiation 4.
SOURCES: Somsak Chunharas presentation to workshop, July 30, 2014; data from National Health Security Office.
Office. Within the system, at the community level in rural areas the primary care units are used as the key provider. District or community hospitals are given funds to pay the primary care providers that are providing service linkage and referrals to the hospitals. Furthermore, Chunharas said, there are modest community funds which provide the community with the opportunity to work with the purchaser and the providers to address the social determinants of health.
To improve quality of care within the system, Chunharas said, Thailand uses an accreditation system for service facilities and has seen steady improvements. Satisfaction differs between the users and the providers. Survey data show that satisfaction among the general population has been quite high since the beginning of universal coverage reforms. Among providers, in the beginning there were a number of concerns about increased workload and other changes to the provider side. Over time, provider dissatisfaction has decreased, but not significantly. Public spending has increased from 45 percent to 65 percent of total health expenditures. There are efforts in the government to cap public spending at 50 percent; however, there are debates based on budget projections and spending concerning the need for such caps. There is evidence that universal coverage has prevented poverty caused by health expenditures (see Figure 5-2).
Chunharas said that while universal health coverage in Thailand has helped to ensure that almost all informal workers in Thailand have health insurance, the preventive and promotive dimension has not been robust. As described below in the presentation from Orraphan Untimanon from the Ministry of Health in Thailand, some OHS interventions by the government and by nongovernment organizations have been piloted on a small scale and have shown positive outcomes, but the resources for such interventions are limited. Chunharas suggested exploring a separate fund for preventive and promotive health efforts among informal workers. With the existence of community funds and the increasing roles of the local government, Chunharas said, there are opportunities for reorienting the universal coverage funds to increase the motivation and capability of the health system to better address avoidable health risks of informal workers and to avoid a health service infrastructure specifically for informal workers.
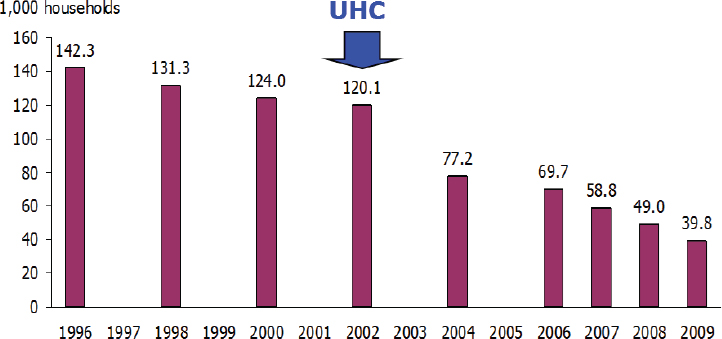
SOURCES: Somsak Chunharas presentation to workshop, July 30, 2015; adapted from Tangcharoensathien et al., 2014.
THAILAND: OCCUPATIONAL HEALTH SERVICES DELIVERY FOR INFORMAL WORKERS AND FINANCIAL RESOURCES
Orrapan Untimanon, Ministry of Health, Thailand
Orrapan Untimanon from the Ministry of Health in Thailand described access to occupational health services for informal workers in that country. Thailand has a total population of 65.8 million, with 39 million of them employed. Around 64.2 percent of the workforce is in the informal sector. Within the informal sector, workers are divided into three groups: agricultural, trade and services, and manufacturing, with the agricultural group representing the largest percentage (61.3 percent).
Within the Thai health system, Untimanon said, most occupational health services are provided at the subdistrict level through primary care units. A successful example of OHS services has been the farmer clinic project, which has been expanded nationwide through primary care units that have experience with OHS. The clinics are structured to meet the needs of the target community, and dissemination efforts are made to inform workers about the clinic and when it will be available. At the clinic, a worker’s health problems are assessed, and a determination is made as to whether the specific problems are occupational in nature or from an underlying disease. When a problem is determined to be occupation-related, treatment is provided. Common occupational diagnoses include contact dermatitis and musculoskeletal disorder, and the
treatments include traditional Thai massage and drugs. Health education is provided to the farmers as well. Diagnoses of occupational diseases are recorded in an existing central data system. For proactive OHS, the clinic collaborates with relevant agencies to conduct risk management for occupational diseases or injury prevention.
Around 10 percent of the primary care units in Thailand have participated in the farmer clinic project. Most of these primary care units were able to provide occupational health services as described above; however, since the clinics were set up on a temporary basis or open only 1 or 2 days per week, many agricultural workers were not reached. Untimanon suggested that fully integrating OHS into primary care could overcome this barrier to access and availability. Other limitations of the clinic intervention were that the primary care unit staff were limited in their ability to make early diagnoses of occupational disease and that some of the data collected were incomplete. Furthermore, while common hazards related to health problems have been identified, risk management needs to be developed further.
Budgetarily, OHS is included as a very small percentage of the allocations under universal care for prevention and promotion, which makes up 10 percent of the total allocation per person and includes many other prevention and promotion interventions. Thus, Untimanon suggested that the specification of OHS intervention in a benefit package of universal care will be crucial to strengthen OHS for informal workers.
THAILAND: EXPERIENCES FROM A PILOT PROJECT ON OCCUPATIONAL SAFETY AND HEALTH PROMOTION FOR INFORMAL WORKERS
Poonsap Tulaphan, HomeNet Thailand
Poonsap Tulaphan from HomeNet Thailand described a government pilot project for an occupational health scheme for informal workers in Thailand.
To provide a perspective on the condition of informal workers’ health in Thailand, Tulaphan shared some data from health checkups of 416 home-based workers, including doll makers, sweetened fish producers, spirit house makers, and cleaners of fish sauce containers who worked in one district of Ratchaburi Province in 2009 and 2010. Thirty to 40 percent of the workers suffered from high blood pressure, and 25 percent suffered from high blood sugar levels. In terms of work-related problems, 50 to 60 percent suffered from chronic muscle pain such as back pain or leg pain. Approximately 60 percent suffered from blurred and distorted vision or astigmatism, while 10 percent—particularly among doll makers,
many of whom are exposed to noise—suffered from hearing impairment. Tulaphan said that the national health system in Thailand covers medical treatment for informal workers as well as health promotion and prevention activities; still, however, the informal workers’ knowledge concerning work-related diseases and preventive measures is generally limited.
In 2001, with support from the Health System Research Institute, HomeNet Thailand studied occupational safety and health (OSH) problems among six producer groups, including workers who performed gem cutting, bronze making, fishing net finishing, traditional cloth weaving, garment sewing and tomato seed production. Then in 2002, with the International Labour Organization and Mahidol University, HomeNet Thailand developed WISH (Work Improvement for Safe Home) manuals for training home-based workers. From 2004 to 2007, with support from the Health Promotion Foundation, HomeNet Thailand promoted OSH among home-based workers in 17 provinces in Thailand. In 2009 and 2010, with support from WIEGO, HomeNet Thailand was able to document lessons learned from their OSH promotion experience. At present with support from the National Health Security Office via a scheme called Promotion and Prevention for workers, HomeNet Thailand is implementing a pilot project to support OSH promotion. The objectives for the pilot are to provide OSH knowledge to and promote prevention activities among informal workers, to support informal workers in accessing the local health community fund, and to facilitate the implementation of OSH promotion activities by primary care units.
Tulaphan described HomeNet Thailand’s work process. It starts by providing training on OSH knowledge to service providers at primary care units. Next, it sets up an OSH working committee which involves all of the stakeholders, including the hospitals, primary care units, subdistrict offices, small enterprise employers, and home-based workers organizations. It conducts a survey on the working environments for risk assessment and, from the assessment date, develops the interventions for home-based workers. These interventions can include health checkups, training, improvements to the working environment, and establishing safety rules. OSH clinic will set up at the hospital level.
At the same time, HomeNet works to identify OSH volunteers; often they are leaders of the home-based workers groups or community health workers volunteers. The volunteers help follow up on the implementation of interventions and assist in seeing how there interventions are affecting the health and behavior of the target populations.
Tulaphan said that the following results have been observed after the second year of the pilot:
- About 1,000 informal workers gained knowledge on OSH and have changed their behavior and improved their working environment to ensure greater occupational health and safety.
- Five hospitals are actively collaborating with subdistrict offices to provide OSH knowledge and skills to home-based workers.
- Other hospitals have come up against limitations to promoting OSH due to their management policy or a lack of interest.
- Only one hospital has the capacity to work as a node to support other hospitals and primary care units.
- Subdistrict offices have exhibited an increasing interest in working with the working-age population.
Regarding constraints, Tulaphan said that most hospitals lack staff with sufficient knowledge and skills on OSH promotion and there is no incentive to promote OSH through assessment standards for primary care units. Health practitioners normally have a high workload, and OSH is often dismissed. Furthermore, those implementing the local health fund frequently do not have sufficient knowledge or experience in promoting the OSH of informal workers. While the HomeNet project is aimed at facilitating the development of qualified staff and encouraging budget allocations for integrating OSH promotion into regular prevention activities, some hospitals mistakenly assumed that the project itself would provide the budget. Additionally, the scattered locations of the target areas within the pilot program required significantly greater resources than if the areas had been more geographically convenient.
Based on the lessons learned from the first 2 years, HomeNet has adjusted its plan for year 3. Tulaphan said that the major focuses are
- investing in a hospital that can potentially become a node with the capability to provide support, particularly in terms of personnel capacity, knowledge, and information system that are favorable for OSH promotion;
- raising awareness and encouraging participation of the National Health Security Office (NHSO) at zone level to address the issue and support OSH promotion by encouraging their involvement in the project; and
- disseminating knowledge and experience gained from the project to NHSO from other zones.
ZAMBIA: PUBLIC–PRIVATE PARTNERSHIPS IN HEALTH
Karen Sichinga, Churches Health Association of Zambia
Karen Sichinga from the Churches Health Association of Zambia (CHAZ) discussed health services in Zambia with an emphasis on the partnership that exists between CHAZ and the Zambian government to provide health services. Before describing the health services, Sichinga provided some country context. Zambia is geographically large but has a population of only 14 million people. It is a landlocked country with eight bordering neighbors, which has major implications for public health and disease control. An epidemic in any bordering countries affects Zambia. Furthermore, Zambia has hosted refugee populations from neighboring countries at different times since the country’s independence from the British in 1964.
The vision behind Zambia’s national health strategy is of a nation of healthy and productive people with a health system based on the principles of primary health care, equity of access, affordability, cost-effectiveness, accountability, partnerships, decentralization, and leadership. Sichinga stressed that the main emphasis of the strategy is on universal coverage, including “equity of access to cost-effective quality health services as close to the family as possible.”
Sichinga said that developing a national strategy requires the consideration of trends in both socioeconomic and health indicators within the country, and she shared some of the relevant indicators from Zambia, including targets that have been set for 2015 (see Table 5-3).
TABLE 5-3 Selected Indicators for Zambia
| Indicator | 2000 | 2007 | 2010 | 2015 Target |
| Socioeconomic indicators | ||||
|
1. Population (millions) |
9.9 | 12.09 | 13.09 | 15.5 |
|
2. Extreme poverty (%) |
46 | 51 | 42.3 | 29 |
|
3. GDP per capita (US$) |
944 | 1233 | 1508 | 1951 |
| Health indicators | ||||
|
4. New malaria cases (per 1,000) |
388 | 358 | 330 | < 255 |
|
5. HIV prevalence rate (%) |
15.6 | 14.3 | 12.7 | < 15.6 |
|
6. Under-5 mortality rate (per 1,000) |
168 | 119 | 137.6 | 63.6 |
|
7. Maternal mortality rate (per 100,000) |
729 | 591.2 | 483 | 162.3 |
NOTE: GDP = gross domestic product; IMF = International Monetary Fund; MDG = Millennium Development Goal; UNDP = United Nations Development Programme.
SOURCE: Karen Sichinga presentation to workshop, July 30, 2014.
DATA SOURCES: Indicators 1 and 3: IMF World Economic Outlook Database, April 2014. Indicators 2, 4, 5, 6, and 7: Zambia MDGs Progress Report 2013, UNDP.
Sichinga listed several key determinants of health in Zambia based on the Zambian government’s National Health Policy (2013), which, she noted, are similar to those in many low- and medium-income countries:
- Environment: 80 percent of the health conditions in patients seen at health institutions are related to poor water supply, inadequate sanitation, food safety, housing and amenities, and climate change.
- Nutrition: Lack of access to good nutrition contributes significantly to mortality and morbidity in Zambia. Malnutrition underlies up 52 percent of all under-5 deaths. Stunting rate is at 45 percent (CSO et al., 2009).
- Education and literacy: Education equips people with knowledge and skills for problem solving and the ability to access and understand information on health, and it can help them to control some of their life circumstances. Literacy in Zambia is estimated at 72 percent—64 percent for women and 82 percent for men, with lower rates in rural areas (CSO et al., 2009).
- Occupational health: Occupational disability, morbidity, and mortality are also major problems in Zambia. Occupation-related injuries affect productivity and the social and physical well-being of workers and their families.
In its attempts to address the determinants of health, provide universal coverage that is consistent with the principles in its national health strategy, and improve its health and socioeconomic indicators, Zambia has faced significant challenges from the limitations on its health care system capacity and resources. Thus, Zambia has embraced partnerships for health. The partners who make up the national health system in Zambia include the government, the church, private corporations, nongovernmental organizations (NGOs), and traditional health practitioners. Sichinga said that these partnerships for health in Zambia have existed since Zambia’s independence in 1964. She added that church health services are private and nonprofit and are responsible for 30 percent of health services in the country, making the church the second largest health care provider (after the Zambian government). In its partnerships, the government provides leadership and guidance for private partners to operate.
Sichinga said that private corporations fill critical and commercially viable gaps. Partnerships have increased options, reduced congestion at public health facilities, strengthened the efficiency and quality of services in the system, created backup options, and pooled comparative advantages. However, she cautioned, there are areas where partnerships have not worked well. Policy changes within a partnering corporation or NGO
have led to the misalignment of expectations between the government and the private partners. Another challenge is sustainability. Sometimes a private partner, such as a corporation, NGO, or the church, will start a program or facility and then run out of the resources needed to maintain it. The expectation then may be for the government to take over the operations, but that is not always feasible. To address sustainability issues, CHAZ and other, similar organizations are encouraging dialogue with the government and the district health offices from the beginning of an initiative so that plans for sustainability will include all partners and be transparent. Sichinga concluded by saying that “public–private partnerships are the only way to sustainable development particularly in resource constrained countries like Zambia. PPPs [public–private partnerships] are making a difference in Zambia.”


























