
15
Prevalence of Intellectual Disabilities
This chapter reviews recent evidence on the prevalence of intellectual disability (ID) in the general population of children in the United States and compares this to trends in the frequency of ID allowances and recipients in the Supplemental Security Income (SSI) program as well as trends in ID prevalence among children enrolled in Medicaid.
ESTIMATES OF INTELLECTUAL DISABILITY PREVALENCE AND PREVALENCE TRENDS FROM THE GENERAL POPULATION
Prevalence of Intellectual Disabilities
Estimates of the prevalence of ID among children in the United States based on epidemiologic studies range widely, from 8.7 to 36.8 per 1,000 (Boyle and Lary, 1996; Camp et al., 1998) (see Table 15-1). A major source of this wide range in prevalence is variation in the inclusion of mild ID (often defined to include individuals with IQs in the range of 50–70 and deficits in adaptive behavior).1 While the prevalence of serious ID (IQ <50 with deficits in adaptive behavior) in the United States and other developed countries is consistently found to be in the range of 2.5 to 5 per 1,000 children, that of mild ID ranges from as low as 2 to more than 30 per 1,000. The risk of mild ID is highest among children of low socioeconomic status (Durkin et al., 2007; Maulik et al., 2011). From the evidence reviewed, disparities in the rates of ID by race and ethnicity are also reported.
_________________
1 See Chapter 9 for further discussion on the classification of severity of intellectual disabilities.
TABLE 15-1 Prevalence of Intellectual Disability per 1,000 Children
| Reference | Year | Location | Age Range | Mild | Severe ID | All | Comments |
| Camp et al., 1998 | 1966–1972 | U.S. multisite birth cohort | 7 years | N/A | Not provided | 36.8 | Prevalence higher in black children (55.0/1,000) than white children (17.0/1,000), and in children of low SES (70.0/1,000) than middle or high (28.0/1,000) SES. |
| Boyle and Lary, 1996 | 1991 | Atlanta, GA | 3–10 years | 5.7 | 0.9 | 8.7 | Overall prevalence higher in black children (13.2/1,000) than white children (6.1/1,000). |
| Bhasin et al., 2006 | 1996 | Atlanta, GA | 8 years | 10.0 | 4.3 | 15.5 | Prevalence higher in black children (22.7/1,000) than white children (9.8/1,000) and higher in boys (19.1) than girls (11.8). |
| Bhasin et al., 2006 | 2000 | Atlanta, GA | 8 years | 7.3 | 3.3 | 12.0 | Prevalence higher in black children (16.9/1,000) than white children (7.0/1,000) and higher in boys (14.0) than girls (9.9). |
| Van Naarden Braun et al., 2015 | 2010 | Atlanta, GA | 8 years | 9.4 | 3.8 | 13.6 | Prevalence of ID without co-occurring ASD declined from 13.0 in 1996 to 8.6 in 2010. Prevalence of ID with co-occurring ASD increased from 2.4 in 1996 to 5.0 in 2010. |
NOTES: ASD = autism spectrum disorder; N/A = not applicable; SES = socioeconomic status. The sum of mild and severe ID prevalence may be less than the overall ID prevalence due to some cases of undetermined severity.
SOURCES: Bhasin et al., 2006; Boyle and Lary, 1996; Camp et al., 1998; Van Naarden Braun et al., 2015.
TABLE 15-2 NHIS Prevalence of Intellectual Disability/Mental Retardation
| 1997–1999 | 2000–2002 | 2003–2005 | 2006–2008 | |
| ID/Mental Retardation Prevalence | 6.8/1000 | 7.3/1000 | 7.5/1000 | 6.7/1000 |
SOURCE: Boyle et al., 2011.
Socioeconomic status is a confounder for these disparities; however, there is also evidence that test bias and diagnostic bias contribute to these differences (Jencks and Phillips, 1998).
In addition to epidemiologic studies, evidence from the Metropolitan Atlanta Developmental Disabilities Surveillance Program (MADDSP) and two national surveys, the National Health Interview Survey (NHIS) and the National Survey of Children’s Health (NSCH) as well as receipt of special education services will be discussed.
National Health Interview Survey
The NHIS provides national-level data on the frequency of ID among children (ages 3–17 years) in the United States for the period 1997 to 2008. The NHIS data, which are based on parent-reported diagnoses of “mental retardation” or ID, are summarized in Table 15-2.
National Survey of Children’s Health
The NSCH began collecting information on the prevalence of ID or mental retardation in the 2011–2012 survey. Previous versions of the NSCH did not ask any questions about ID or mental retardation. The NSCH-estimated prevalence of children (2–17 years) who currently had the condition in 2011–2012 was 1.1 percent (confidence interval [CI] 0.9–1.2) (NSCH, 2012a).
Prevalence Trends for Intellectual Disabilities
It is important to acknowledge that there are no perfect sources of data for evaluating trends in the prevalence of ID in the United States. An ideal source that would allow evaluation of trends over time might be generated by large-scale, nationally representative, population-based epidemiologic studies conducted periodically, and using validated and comparable methods and diagnostic criteria over time. No such data source exists. The data sources used for the purposes of this study have complementary strengths and weaknesses. For example, the epidemiologic data source described
below, from the Centers for Disease Control and Prevention’s (CDC’s) MADDSP, has the advantages of being population-based, including one large and diverse populations of U.S. children, relying on validated methods for classifying cases of ID that were comparable over a multiple-year period (1991–2010), and allowing evaluation of trends over time. The MADDSP data are, however, not nationally representative and they rely exclusively IQ scores recorded in the records of health care providers or schools, without incorporating information on adaptive behavior. In contrast, the national survey data have the advantage of being based on national probability samples, but the disadvantages of relying on parental reports rather than diagnostic assessments, and of response rates less than 100 percent. Special education “child count” data have the advantages of being nationally representative and available annually, but do not necessarily rely on standard case definitions or diagnostic criteria that are comparable over time and across states and school districts. Despite the limitations each data source, taken together they provide valuable and complementary evidence for evaluating trends over time in the frequency of ID in U.S. children.
Metropolitan Atlanta Developmental Disabilities Surveillance Program
MADDSP, which is funded by the CDC, has monitored the prevalence of ID among children in the five counties of metropolitan Atlanta since 1991, and it recently published findings that allow an evaluation of trends in ID prevalence over time (Van Naarden Braun et al., 2015). The earliest estimate of the prevalence of ID from this program—for surveillance year 1991—was 8.7 per 1,000 children of ages 3–10 years (see Table 15-1) (Boyle and Lary, 1996). Subsequent estimates were restricted to 8-year-old children, as 8 years is the peak age for identification of ID. For the surveillance year 1996, MADDSP reported an ID prevalence of 15.5 per 1,000 8-year-old children, and for surveillance year 2000 the comparable estimate was 12.0 (see Table 15-1) (Bhasin et al., 2006). The most recent estimate, for surveillance year 2010, found the overall prevalence of ID among 8-year-old children to be 13.6 per 1,000 shown in Table 15-1 (Van Naarden Braun et al., 2015).
Special Education Services
As reported previously in comparison with prevalence trends for autism spectrum disorder, the rate of the receipt of special education services for ID among school-aged children in the United States declined steadily from 9.1 per 1,000 in 2004 to 6.6 per 1,000 in 2012. Table 15-3 shows the decreasing trend in the rate of children receiving special education services for ID from 2004 to 2012.
TABLE 15-3 Prevalence of Receipt of Special Education Services for Intellectual Disability in Children of Ages 6–17 Years, per 1,000 Children in the United States, 2004–2012
| Year | 2004 | 2005 | 2006 | 2007 | 2008 | 2009 | 2010 | 2011 | 2012 |
| Prevalence | 9.1 | 8.6 | 8.2 | 7.7 | 7.5 | 7.2 | 6.9 | 6.7 | 6.6 |
NOTE: Denominators of child population were obtained for ages 5–17 for the years 2004 to 2012. Numerators were obtained from Part B child count data for intellectual disability (called mental retardation before 2010) for the 50 states, Washington, DC, and Puerto Rico, ages 6–17 for the years 2004–2011. Numerator was obtained for intellectual disability for the 50 states, Washington, DC, and Puerto Rico for ages 6–17 for year 2012.
SOURCES: U.S. Census Bureau, 2011, 2015a; U.S. Department of Education, 2013, 2014.
TRENDS IN THE RATES OF INTELLECTUAL DISABILITY AMONG SSI AND MEDICAID POPULATIONS
This section of the report presents data on the trends in the rates of intellectual disability in the SSI program for children from 2004 to 2013 and in Medicaid from 2001 to 2010.
SSI
Within the SSI program, the number of allowances and recipients for ID substantially and continuously decreased between 2004 and 2013. The proportion of allowances and recipients attributable to ID among the 10 major mental disorders also decreased. In spite of these decreases, in 2013 ID was the basis for the third highest number of allowances (12,470) of the major mental disorders, the fifth highest number (13,613) of determinations, and the third highest number (120,248) of recipients. In addition, the allowance rate for ID remained above 90 percent for each year from 2004 to 2013, indicating that nearly all children with ID who applied for benefits were deemed eligible. Based on these findings, it appears that fewer children are being adjudicated as having a disability due to ID. The decreasing numbers of ID allowances and recipients is unique; decreasing trends of similar magnitude are not observed for any of the other selected mental disorders.
Table 15-4 presents the SSI administrative data on ID in children. Column 1 shows the number of child allowances made on the basis of ID at the initial level for each year. Column 2 shows the number of child recipients who received SSI benefits on the basis of ID in December of each year. Column 3 shows the estimated number of children in households with incomes under 200 percent of the federal poverty level (FPL) for each year. To control for the changes in the magnitude of child poverty, allowances and recipients are shown as a percentage of the number of children in
TABLE 15-4 SSI Child Initial Allowances and Recipient Numbers for Intellectual Disability
| Year | 1 | 2 | 3 | 4 | 5 |
| # of Child SSI Allowances for ID | # of Child SSI Recipients for ID | # of Children in Households Under 200% FPL | % of Children Under 200% FPL Allowed SSI Benefits for ID | % of Children Under 200% FPL Who Are Recipients of SSI Benefits for ID | |
| 2004 | 24,602 | 215,709 | 28,753,000 | 0.09% | 0.75% |
| 2005 | 22,237 | 204,755 | 28,539,000 | 0.08% | 0.72% |
| 2006 | 19,161 | 192,566 | 28,757,000 | 0.07% | 0.67% |
| 2007 | 17,152 | 178,042 | 28,999,000 | 0.06% | 0.61% |
| 2008 | 17,182 | 163,007 | 30,064,000 | 0.06% | 0.54% |
| 2009 | 17,831 | 151,887 | 31,505,000 | 0.06% | 0.48% |
| 2010 | 17,680 | 141,618 | 32,254,000 | 0.05% | 0.44% |
| 2011 | 16,456 | 132,906 | 32,678,000 | 0.05% | 0.41% |
| 2012 | 14,128 | 126,520 | 32,269,000 | 0.04% | 0.39% |
| 2013 | 12,470 | 120,248 | 31,364,000 | 0.04% | 0.38% |
NOTE: The Current Population Survey table creator was used to generate numbers of children below 200 percent of the federal poverty level. Parameters used to generate the numbers include get count of: persons in poverty universe (everyone except unrelated individuals under 15); years: 2004 to 2013; Census 2010 weights; row variable: age; column variable: income-to-poverty ratio; and customized formatting: income-to-poverty ratio percent cutoff of 200 percent.
SOURCES: U.S. Census Bureau, 2015b; unpublished data set provided by the Social Security Administration (SSA).
households under 200 percent FPL for each year. Column 4 shows the percentage of children in households under 200 percent FPL who were allowed benefits for ID (i.e., were found to be severely impaired, with a primary diagnosis of ID) in each year. Column 5 shows the percentage of children in households under 200 percent FPL who were recipients (including newly allowed and existing recipients) of SSI payments for ID in December of each year. Figure 15-1 plots the percentages from columns 4 and 5, along with the 10-year average of percentage of allowances and recipients for ID as a visual reference point.
Over the 10-year period from 2004 to 2013, the rates of child SSI ID allowances and recipients were decreasing. The rate of child ID allowances among children in households less than 200 percent FPL decreased between 2004 and 2013 by approximately 56 percent, from 0.09 to 0.04 percent.
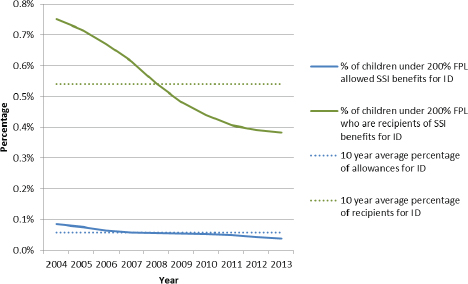
FIGURE 15-1 Percentages of SSI child initial allowances and recipients for intellectual disability below 200 percent FPL.
NOTE: The Current Population Survey table creator was used to generate numbers of children below 200 percent of the federal poverty level. Parameters used to generate the numbers include get count of: persons in poverty universe (everyone except unrelated individuals under 15); years: 2004 to 2013; Census 2010 weights; row variable: age; column variable: income-to-poverty ratio; and customized formatting: income-to-poverty ratio percent cutoff of 200 percent.
SOURCES: U.S. Census Bureau, 2015b; unpublished data set provided by the SSA.
Similarly, the rate of child ID recipients decreased between 2004 and 2013 by 49 percent, from 0.75 to 0.38 percent.
Medicaid
Table 15-5 shows the percentage of children who were diagnosed with ID in two different groups of Medicaid enrollees for each year from 2001 to 2010. Column 1 shows the percentage of ID diagnoses among all Medicaid enrollees2 for each year. Column 2 shows the percentage of ID diagnoses among the smaller subpopulation of Medicaid enrollees who were eligible to be enrolled in Medicaid on the basis receiving SSI benefits.3
_________________
2 Refer to Appendix F for Rutgers methods section.
3 Ibid.
TABLE 15-5 Percentage of Child Medicaid Enrollees and SSI Medicaid Enrollees Diagnosed with Intellectual Disability
| Year | 1 | 2 |
| % of All Child Medicaid Enrollees with ID Diagnosis | % of Child SSI Medicaid Enrollee Subpopulation with ID Diagnosis | |
| 2001 | 0.60% | 6.60% |
| 2002 | 0.60% | 6.50% |
| 2003 | 0.60% | 6.20% |
| 2004 | 0.50% | 6.20% |
| 2005 | 0.50% | 6.40% |
| 2006 | 0.60% | 6.40% |
| 2007 | 0.60% | 6.80% |
| 2008 | 0.60% | 7.10% |
| 2009 | 0.60% | 6.60% |
| 2010 | 0.50% | 6.40% |
SOURCE: Medicaid Analytic eXtract (MAX) data.
As shown in Figure 15-2, the rate of ID diagnoses among all children enrolled in Medicaid was mostly flat, remaining very close to the 10-year average each year. The rate of ID diagnoses among all Medicaid enrollees decreased by 16.67 percent from 2001 to 2010, from 0.6 to 0.5 percent. The rate of ID diagnoses among the SSI-eligible subpopulation of Medicaid enrollees decreased by −3.03 percent, from 6.6 to 6.4 percent. There was a peak in the rates of ID diagnoses among SSI-eligible Medicaid enrollees in 2008 which does not seem to appear in any of the other trends observed.
For the years in which the Medicaid data and the SSI administrative data overlapped, 2004–2010, there was no change in the rate of ID diagnoses among all Medicaid enrolled children, the rate of ID diagnoses among SSI eligible Medicaid enrolled children increased 3.23 percent, and the prevalence of SSI recipients for ID among children in households below 200 percent FPL decreased by 41 percent. A clear decreasing trend is observed in the SSI program, while no clear decreasing trend is observed in the Medicaid population.
DISCUSSION
SSI data and special education service utilization data show a uniformly decreasing trend in ID prevalence for the time period roughly between
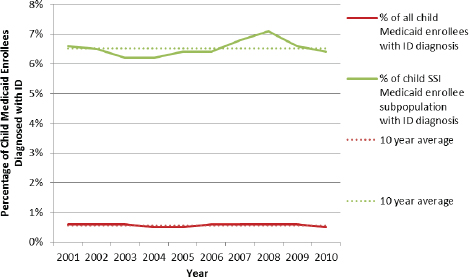
FIGURE 15-2 Percentage of child Medicaid enrollees and SSI Medicaid enrollees diagnosed with intellectual disability.
SOURCE: MAX data.
2001 and 2013. Epidemiologic data also suggest a decline in ID prevalence between the 1960s and 2000 (Bhasin et al., 2006; Camp et al., 1998). On the other hand, available national survey data and Medicaid data show no evidence of a change in the frequency of ID in recent decades. A possible explanation for the differences in the observed trends is that the data based on SSI allowances and recipients, special education, and epidemiologic surveillance are secondary uses of diagnostic categories that are required for benefit and service eligibility, while the Medicaid and population survey data are based, respectively, on the use of clinical or treatment services and on parent reports. As discussed in Chapter 14, diagnostic substitution may contribute to the decrease in ID observed in the SSI program and in special education service use data. The use of the autism spectrum disorder diagnostic category may be incentivized—and therefore preferentially used—due to the availability of more or better services and supports or because of less social stigma. In contrast, the diagnostic criteria used in a clinical setting might be less prone to substitution.
The similarity of the decreasing trends observed in the SSI program and in the Individuals with Disabilities Education Act data does provide some confirmation that the trends observed in the SSI program are not unexpected or inconsistent with trends in the general population.
Based on general population estimates of ID and the rate of child poverty, it may be the case that the SSI program is providing benefits to a relatively small proportion of the population of children who would otherwise be eligible to receive benefits. The NSCH 2011–2012 estimate of the prevalence of children (ages 2–17) with severe or moderate ID, as reported by parents, was 0.7 percent (NSCH, 2012b). The estimated number of children below 200 percent FPL in 2012 was 32,269,000 (U.S. Census Bureau, 2015b).4 Therefore the expected number of children with current moderate to severe ID below 200 percent FPL would be 225,883. In 2012 there were 126,520 child recipients of SSI benefits for ID, less than 60 percent of the expected number. Figure 15-3 illustrates these relationships.
FINDINGS
- Estimates of the prevalence of ID in the general population have varied somewhat over time, but have remained largely unchanged. These estimates range from 8.7 to 36.8 per 1,000 children.
- The number of children and the proportion of children in low-income households who are receiving SSI benefits for ID is decreasing. The decreasing trend is consistent with trends observed in the rates of special education service utilization for children with ID and may relate to diagnostic substitution with ASD.
- The rates of children being diagnosed with ID among all child Medicaid enrollees did not appear to decrease between 2001 and 2010. The percentage of children diagnosed with ID who are on Medicaid on the basis of SSI eligibility may have increased slightly.
CONCLUSION
- Rough estimates of the number of children in low-income households with moderate to severe ID suggests that less than 60 percent of children who are likely eligible for SSI benefits due to ID are recipients of SSI benefits for ID.
_________________
4 The Current Population Survey table creator was used to generate numbers of children below 200 percent of the federal poverty level. Parameters used to generate the numbers include get count of: persons in poverty universe (everyone except unrelated individuals under 15); years: 2004 to 2013; Census 2010 weights; row variable: age; column variable: income-to-poverty ratio; and customized formatting: income-to-poverty ratio percent cutoff of 200 percent.
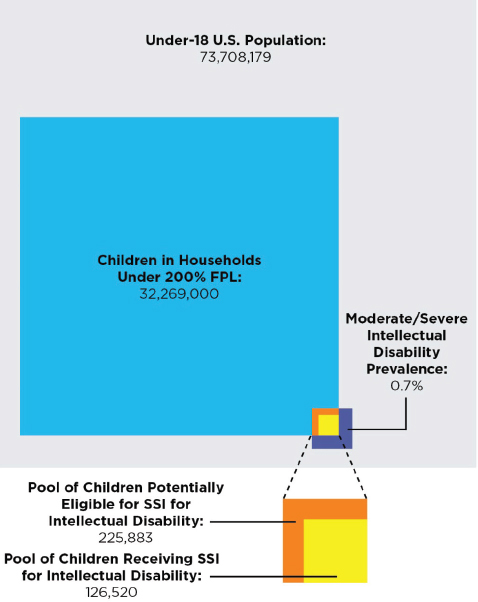
FIGURE 15-3 Children potentially eligible for SSI for intellectual disability versus children receiving SSI for intellectual disability in 2012, according to the NSCH.
NOTE: The Current Population Survey table creator was used to generate numbers of children below 200 percent of the federal poverty level. Parameters used to generate the numbers include get count of: persons in poverty universe (everyone except unrelated individuals under 15); years: 2004 to 2013; Census 2010 weights; row variable: age; column variable: income-to-poverty ratio; and customized formatting: income-to-poverty ratio percent cutoff of 200 percent.
SOURCES: NSCH, 2012b; U.S. Census Bureau, 2014, 2015b; unpublished data provided by the SSA.
REFERENCES
Bhasin, T. K., S. Brocksen, R. N. Avchen, and K. V. N. Braun. 2006. Prevalence of four developmental disabilities among children aged 8 years: Metropolitan Atlanta Developmental Disabilities Surveillance Program, 1996 and 2000. Mordity and Mortality Weekly Report 55(SS01):1–9.
Boyle, C. A., and J. M. Lary. 1996. Prevalence of selected developmental disabilities in children 3–10 years of age: The Metropolitan Atlanta Developmental Disabilities Surveillance Program, 1991. Morbidity and Mortality Weekly Report 45(SS02):1–14.
Boyle, C. A., S. Boulet, L. A. Schieve, R. A. Cohen, S. J. Blumberg, M. Yeargin-Allsopp, S. Visser, and M. D. Kogan. 2011. Trends in the prevalence of developmental disabilities in U.S. children, 1997–2008. Pediatrics 127(6):1034–1042.
Camp, B. W., S. H. Broman, P. L. Nichols, and M. Leff. 1998. Maternal and neonatal risk factors for mental retardation: Defining the “at-risk” child. Early Human Development 50(2):159–173.
Durkin, M., N. Schupf, Z. Stein, and M. Susser. 2007. Mental retardation. In Public health and preventive medicine, edited by R. Wallace. Stamford, CT: Appleton & Lange. Pp. 1173–1184.
Jencks, C., and M. Phillips. 1998. The black-white test scope gap: Why it persists and what can be done. The Brookings Review 24–27.
Maulik, P. K., M. N. Mascarenhas, C. D. Mathers, T. Dua, and S. Saxena. 2011. Prevalence of intellectual disability: A meta-analysis of population-based studies. Research in Developmental Disabilities 32(2):419–436.
NSCH (National Survey of Children’s Health). 2012a. Data query from the child and adolescent health measurement initiative. http://childhealthdata.org/browse/survey/results?q=2530&r=1 (accessed July 16, 2015).
NSCH. 2012b. Data query from the child and adolescent health measurement initiative. http://childhealthdata.org/browse/survey/results?q=2533&r=1 (accessed August 3, 2015).
U.S. Census Bureau. 2011. National intercensal estimates (2000–2010): Table 1 Intercensal estimates of the resident population by sex and age for the United States: April 1, 2000, to July 1, 2010. www.census.gov/popest/data/intercensal/national/nat2010.html (accessed July 28, 2015).
U.S. Census Bureau. 2014. Total population by child and adult populations. http://datacenter.kidscount.org/data/tables/99-total-population-by-child-and-adult-populations?loc=1&loct=1#detailed/1/any/false/35,18,17,16,15/39,41/416,417 (accessed November 14, 2014).
U.S. Census Bureau. 2015a. Annual estimates of the resident population for selected age groups by sex for the United States, states, and counties, and Puerto Rico Commonwealth and municipios: April 1, 2010, to July 1, 2014. http://factfinder.census.gov/faces/tableservices/jsf/pages/productview.xhtml?src=bkmk (accessed July 15, 2015).
U.S. Census Bureau. 2015b. CPS table creator. www.census.gov/cps/data/cpstablecreator.html (accessed July 13, 2015).
U.S. Department of Education. 2013. Thirty-fifth annual report to Congress on the implementation of the Individuals with Disabilities Education Act, Parts B and C. 2013: Part B data descriptions and data files. http://www2.ed.gov/about/reports/annual/osep/2013/parts-b-c/part-b-data/index.html (accessed July 28, 2015).
U.S. Department of Education. 2014. 2012 IDEA part B child count and educational environments. https://inventory.data.gov/dataset/2012-idea-part-b-child-count-and-educationalenvironments/resource/a68a23f3-3981-47db-ac75-98a167b65259?inner_span=True (accessed August 3, 2014).
Van Naarden Braun, K., D. Christensen, N. Doernberg, L. Schieve, C. Rice, L. Wiggins, D. Schendel, and M. Yeargin-Allsopp. 2015. Trends in the prevalence of autism spectrum disorder, cerebral palsy, hearing loss, intellectual disability, and vision impairment, metropolitan Atlanta, 1991–2010. PLoS ONE 10(4):e0124120.
This page intentionally left blank.














