
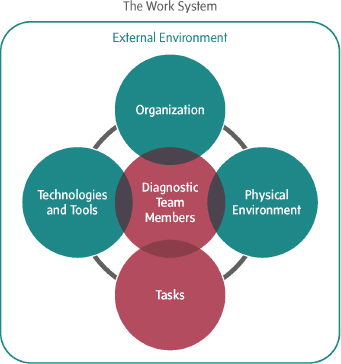
This chapter describes the team-based nature of the diagnostic process, the importance of clinicians partnering with patients and their families throughout the process, and the education and training that health care professionals need to participate effectively in the diagnostic process. Making accurate and timely diagnoses requires teamwork among health care professionals, patients, and their family members. In terms of the committee’s conceptual model of the diagnostic process, the focus of this chapter is on two of the elements of the work system: diagnostic team members (health care professionals, patients, and their families) and the tasks they perform in the diagnostic process (see Figure 4-1). The committee makes two recommendations targeted at improving teamwork and patient engagement in the diagnostic process and preparing health care professionals to effectively participate in the diagnostic process.
THE DIAGNOSTIC PROCESS AS A TEAM ENDEAVOR
This study was originally titled “Diagnostic Error in Medicine,” but based on discussions at its first meeting, the committee concluded that “Diagnostic Error in Health Care” was a more accurate description because it better reflected the patient-centered and teamwork-oriented aspects of the diagnostic process. This conceptualization of diagnosis grew out of the recognition that too often the diagnostic process is characterized as a solitary activity, taking place exclusively within an individual physician’s mind. While the task of integrating relevant information and communicating a diagnosis to a patient is often the responsibility of an
individual clinician, the diagnostic process ideally involves collaboration among multiple health care professionals, the patient, and the patient’s family. Patients and their families play a pivotal role in the diagnostic process. Thus, arriving at accurate and timely diagnoses—even those made by an individual clinician working with a single patient—involves teamwork. The number of health care professionals involved in the diagnostic process can vary substantially depending on the nature of the patient’s health problem: For example, McDonald (2014) noted that a diagnostic process could involve a single clinician if the suspected diagnosis is considered something straightforward, such as a common cold. However, at the other end of the spectrum, the diagnostic process could be quite complex and involve a broad array of health care professionals, such as primary care clinicians, diagnostic testing health care professionals, multiple specialists if different organ systems are suspected to be involved, nurses, pharmacists, and others.
Even though some diagnoses continue to be made by individual clinicians working independently, this solitary approach to the diagnostic
process is likely to be insufficient given the changing nature of health care (see Chapter 2). The mounting complexity of health care, including ever-increasing options for diagnostic testing and treatment and the movement toward precision medicine; the rapidly rising levels of biomedical and clinical evidence to inform clinical practice; and the frequent comorbidities among patients due to the aging of the population will require greater reliance on team-based diagnosis (IOM, 2008, 2013b). To manage the increasing complexity in health care and medicine, clinicians will need to collaborate effectively and draw on the knowledge and expertise of other health care professionals, as well as patients and families, throughout the diagnostic process. The committee recognizes that reframing the diagnostic process as a team-based activity may require changing norms of health care professional roles and responsibilities and that these changes may take some time and may meet some resistance. Nevertheless, the committee concluded that improving diagnosis will require a team-based approach to the diagnostic process, in which all individuals collaborate toward the goal of accurate and timely diagnoses. Consistent with the committee’s conclusion, recent reports in the literature make the case that the diagnostic process is a team-based endeavor (Graedon and Graedon, 2014; Haskell, 2014; Henriksen and Brady, 2013; McDonald, 2014). For example, Schiff noted that the new paradigm for diagnosis is that it is carried out by a well-coordinated team of people working together through reliable processes; in this view, diagnosis is the collective work of the team of health care professionals and the patient and his or her family (Schiff, 2014b).
In health care, teamwork has been described as a “dynamic process involving two or more health [care] professionals with complementary backgrounds and skills, sharing common health goals and exercising concerted physical and mental effort in assessing, planning, or evaluating patient care. This is accomplished through interdependent collaboration, open communication and shared decision-making” (Xyrichis and Ream, 2008, p. 238). Five principles of team-based care have been identified by the Institute of Medicine (IOM): shared goals, clear roles, mutual trust, effective communication, and measurable processes and outcomes (see Box 4-1). Research by a number of organizations, including the IOM, has highlighted the important role that teamwork plays in health care (Borrill et al., 2000; Boult et al., 2009; IOM, 2001, 2013a,b; Josiah Macy Jr. Foundation and Carnegie Foundation for the Advancement of Teaching, 2010; Naylor et al., 2010; WHO, 2010). A report commissioned by the Robert Wood Johnson Foundation identified several factors that are important to fostering and sustaining interprofessional collaboration: patient-centeredness, leadership commitment, effective communication, awareness of roles and responsibilities, and an organizational structure
BOX 4-1
Principles of Team-Based Health Care
Shared goals: The team—including the patient and, where appropriate, family members or other support persons—works to establish shared goals that reflect patient and family priorities and that can be clearly articulated, understood, and supported by all team members.
Clear roles: There are clear expectations for each team member’s functions, responsibilities, and accountabilities, which optimizes the team’s efficiency and often makes it possible for the team to take advantage of a division of labor, thereby accomplishing more than the sum of its parts.
Mutual trust: Team members earn each others’ trust, creating strong norms of reciprocity and greater opportunities for shared achievement.
Effective communication: The team prioritizes and continuously refines its communication skills. It has consistent channels for candid and complete communication, which are accessed and used by all team members across all settings.
Measurable processes and outcomes: The team agrees on and implements reliable and timely feedback on successes and failures in both the functioning of the team and achievement of the team’s goals. These are used to track and improve performance immediately and over time.
SOURCE: Adapted from IOM, 2012c.
that integrates interprofessional practice (CFAR et al., 2015). A review by the United Kingdom’s National Health Service found that teamwork has “been reported to reduce hospitalization time and costs, improve service provision, [and] enhance patient satisfaction, staff motivation and team innovation” (Borrill et al., 2000, p. 14). One study found that a “culture of collaboration” is a key feature shared by academic medical centers considered to be top performers in quality and safety (Keroack et al., 2007), and a literature review found moderate evidence for an association between teamwork and positive patient outcomes, with the most consistent evidence from the intensive care unit setting (Sorbero et al., 2008). Another study found that surgical teams that did not engage in teamwork had worse patient outcomes, including a higher likelihood of death or serious complications (Mazzocco et al., 2009). These findings are consistent with those from other sectors. For example, in the aviation and nuclear power industries, teamwork and training in team-based skills have been found
to improve performance and reduce errors related to communication and coordination problems (Leonard et al., 2004; Salas et al., 2008; Weaver et al., 2014).
Compared to teamwork in other areas of health care, teamwork in the diagnostic process has not received nearly as much attention. Teamwork in diagnosis is likely to be somewhat distinct from the teamwork that occurs after a diagnosis is made, in part due to the fluid, or unstable, collection of health care professionals involved in the diagnostic process. Fluid team membership has been recognized as a strategy to deal with fast-paced, complex tasks such as diagnosis where preplanned coordination may not be possible and where communication and coordination are a necessity (Bushe and Chu, 2011; Edmondson, 2012; Vashdi et al., 2013). Fluid team membership can introduce new challenges, such as a reduced sense of belonging to the team and a decrease in team efficacy (Bushe and Chu, 2011; Dineen and Noe, 2003; Shumate et al., 2010). A number of strategies have been identified as ways to lessen the negative impacts of fluid teams, including standardizing roles and skills, reducing task interdependence, and increasing health care professionals’ understanding of others’ roles (Bushe and Chu, 2011). Although teams focused on patient treatment may also exhibit fluidity, the uncertainty and complexity of the diagnostic process make unstable team membership more likely in the diagnostic process.
The committee concluded that literature on the role of teams in diagnosis is limited and that lessons from teamwork in other settings, including the treatment setting, are applicable to the diagnostic process. In testimony to the committee, Eduardo Salas of the University of Central Florida said that teamwork was likely to improve diagnosis and reduce diagnostic errors because teamwork has been found to mitigate communication and coordination challenges in other areas of health care. These same challenges have been found to have an impact on diagnostic performance (Gandhi, 2014; IOM, 2013b; The Joint Commission, 2014; Schiff, 2014a; Singh, 2014; Sutcliffe et al., 2004). Emerging research also suggests that teamwork will improve the diagnostic process; one study found that medical students working in teams made fewer diagnostic errors than those working individually, and other research has found that collaboration among treating clinicians and clinical pathology teams resulted in better diagnostic test selection (Hautz et al., 2015; Seegmiller et al., 2013).
Diagnosis depends on health care professionals with differing educational and training backgrounds working together and practicing to the full extent of their education and training (IOM, 2001, 2012c). Having clear roles and responsibilities leaves “those with greater training or responsibility free to perform tasks or to solve problems for which they are uniquely equipped” (Baldwin and Tsukuda, 1984, p. 427), while other
tasks in the diagnostic process can be distributed to health care professionals within their own scope of practice (Baldwin and Tsukuda, 1984; IOM, 2011a). Improving diagnostic performance requires participating individuals to recognize the importance of teamwork as well as the contributions of other health care professionals to the diagnostic process.
In recognition that the diagnostic process is a dynamic team-based activity, health care organizations should ensure that health care professionals have the appropriate knowledge, skills, resources, and support to engage in teamwork in the diagnostic process. Ensuring that individuals participating in the diagnostic process have the appropriate resources and support extends beyond the purview of this chapter and requires a systems approach to diagnosis, including consideration of health information technology (health IT) resources (see Chapter 5), an organizational culture and work system that supports teamwork (see Chapter 6), and payment and care delivery models that promote teamwork (see Chapter 7). This chapter focuses on describing the individuals involved in the diagnostic process, identifying opportunities to facilitate patient engagement and intra- and interprofessional collaboration in the diagnostic process, and ensuring that team members have and maintain appropriate competencies in the diagnostic process.
Participants in the Diagnostic Process
The committee described diagnostic teamwork as the collaboration of interrelated individuals working toward the goal of establishing and communicating an accurate and timely explanation of a patient’s health problem (Salas et al., 2008). Teamwork in the diagnostic process involves the collaboration of patients and their families; diagnosticians, such as physicians, physician assistants (PAs), and advanced practice nurses (APNs); and health care professionals who support the diagnostic process, such as nurses, pharmacists, laboratory scientists, radiology technologists, medical assistants, and patient navigators.
Figure 4-2 illustrates the relationship among individuals participating in the diagnostic process. Patients and their family members are located at the center because the ultimate goal of the diagnostic process is to explain a patient’s health problem and to inform subsequent decision making about a patient’s care. Surrounding patients and their families are diagnosticians, health care professionals whose tasks include making diagnoses. Encircling the diagnosticians are health care professionals who support the diagnostic process. Although Figure 4-2 distinguishes between diagnosticians and health care professionals who support the diagnostic process, this distinction may be less clear in practice. For example, triage—a complex cognitive nursing task designed to identify patients

needing immediate medical care—has not typically been included as a component in the diagnostic process, but it can often play a de facto role because a nurse may identify a suspected diagnosis during this process (Soni and Dhaliwal, 2012). Similarly, incorrect triage decisions can also introduce cognitive biases (such as framing or anchoring effects) that can contribute to diagnostic errors (see Chapter 2). The overlapping nature of the diagnostic team members in Figure 4-2 reflects the importance of effective communication and collaboration among all individuals in the diagnostic process.
Teamwork in the diagnostic process rarely involves static, fixed diagnostic teams; instead, participation in diagnosis is often dynamic and fluctuates over time, depending on what areas of expertise are needed to diagnose a specific patient and where the patient engages in the diagnostic process. The teamwork involved in the diagnostic process is illustrated in Figure 4-3. If there is good care coordination, a partnership is formed between a patient and his or her primary care team. If a patient develops
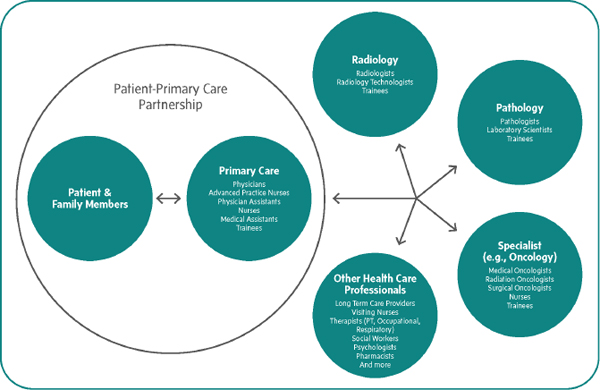
FIGURE 4-3 An example of diagnostic teamwork and the potential participants in the diagnostic process. The arrows in the figure illustrate the importance of communication among team members.
NOTE: PT = physical therapist.
symptoms that require further evaluation, the primary care team can collaborate with other health care professionals (such as pathologists, radiologists, and specialty care clinicians) in the diagnostic process and coordinate subsequent care. The depiction in Figure 4-3 of the various ways that patients and health care professionals interact during the diagnostic process is likely an idealization of clinical practice. For example, patients and their families will often take on a significant burden of care coordination because of the fragmentation of the health care system, a lack of interoperability of patients’ electronic health records (EHRs), and payment incentives that do not promote care coordination (Bodenheimer, 2008; Press, 2014). In addition, patients may lack a usual source of primary care, which can hinder care coordination efforts (CDC, 2014; HHS, 2013).
Patients and Their Family Members
The goal of patient engagement in diagnosis is to improve patient care and outcomes by enabling patients and their families to contribute valuable input that will facilitate an accurate and timely diagnosis and improve shared decision making about the path of care. Because patients are a heterogeneous population with varying needs, values, and preferences, their roles in diagnosis need to be individually tailored. Patients hold critical knowledge that informs the diagnostic process, such as knowledge of their health history, their symptoms, their exposure to individuals or environmental factors, the course of their condition, the medications they are taking, as well as knowledge gained from information searches that they conducted in advance of their appointment. In addition, patients and their families may also maintain a more complete version of their own medical records, and they can help ensure that test results are received and facilitate communication among their clinicians (Gruman, 2013).
Diagnosticians
Diagnosticians are health care professionals (physicians, PAs, APNs, and others) who are educated and licensed to provide patients with diagnoses. Although a diagnostician is defined as any health care professional with diagnosis in his or her scope of work, in general, physicians are expected to deal with a greater complexity of diagnostic tasks than other diagnosticians. In addition to diagnosing patients’ health problems, diagnosticians often participate in a variety of other health care tasks, such as the provision of preventive care and the management of patients’ chronic and acute health conditions. Diagnosticians work in all health care settings and include both general and specialist practitioners. Their clinical reasoning skills come into play as they collect and integrate information
from a patient’s clinical history, interview, physical exam, diagnostic testing, and consultations with or referrals to other health care professionals (see Chapter 2).
Pathologists and radiologists are diagnosticians who provide information and consultations that are critical to diagnosing patients’ health problems, such as advising on the appropriate diagnostic testing for a particular patient and conveying the implications of the test results to treating health care professionals.1 Despite the important roles that laboratory medicine, anatomic pathology, and medical imaging play in a diagnosis, pathologists and radiologists have sometimes been treated as ancillary or support services. Expert testimony to the committee found that many pathologists and radiologists have not been adequately engaged in the diagnostic process and that better collaboration among all diagnostic team members is necessary (Allen and Thorwarth, 2014; Kroft, 2014). The committee concluded that a culture that perpetuates the notion of anatomic pathology, laboratory medicine, and medical imaging as ancillary health care services will inhibit efforts to improve diagnosis. Thus, the committee recommends that health care organizations should facilitate and support collaboration among pathologists, radiologists, other diagnosticians, and treating health care professionals to improve diagnostic testing processes. This includes collaboration throughout the testing process, including the ordering of appropriate tests or images, analysis and interpretation, the reporting and communication of results, and subsequent decision making. Depending on a patient’s health problem, treating clinicians may also need to work collaboratively with other diagnosticians, such as sleep specialists, cardiologists, and others. Education and training of health care professionals also needs to ensure that they are prepared to work in this manner.
Health Care Professionals Who Support the Diagnostic Process
In addition to diagnosticians, the diagnostic process may involve an array of health care professionals, including nurses, medical assistants, radiology technologists, laboratory scientists, pharmacists, patient navigators, social workers, therapists, nutritionists, and many others. These health care professionals play a crucial role by facilitating the diagnostic process through the performance of their tasks.
Nurses in particular play a key role in the diagnostic process (see Box 4-2). Nurses may ensure communication and care coordination among diagnostic team members, monitor a patient over time to see if the patient’s course is consistent with a working diagnosis, and identify
______________
1 Treating health care professionals are clinicians who directly interact with patients.
BOX 4-2
Suggested Actions for Nurses to Improve Diagnosis and Reduce Diagnostic Error
- Know the major diagnoses of your patients.
- Be the voice of your patients and their advocate in navigating their health care.
- Be the eyes of the diagnostic team in detecting, reporting, and documenting changes in your patients’ symptoms, signs, complaints, or conditions.
- Be the monitor of the diagnostic team. Is your patient responding to treatment as expected?
- Help optimize communication between your patient and the care team:
- Help patients tell their story and relate all of their symptoms.
- Check patients’ understanding of their diagnoses and what they’ve been told.
- Be the watchdog for appropriate care coordination.
- Educate patients about the diagnostic process.
- Learn about how diagnostic errors arise and how they can be avoided.
- Educate patients about diagnostic tests and explain why they are needed, what the patient will experience, and what the results will reveal.
- Help patients with the emotional and psychological difficulties that arise when a diagnosis is not yet known or is known to be bad.
SOURCE: Adapted from SIDM and NPSF, 2014. Reprinted, with permission, from the Society to Improve Diagnosis in Medicine and the National Patient Safety Foundation.
potential diagnostic errors. Nurses facilitate patient engagement in the diagnostic process by communicating with patients about their history, actively listening to patients’ descriptions of their reasons for a visit, documenting patients’ symptoms, assessing vital signs, and conveying this information to other clinicians. Nurses need to be full and active members of the diagnostic team, with opportunities to present their observations and conclusions to other team members. The committee’s understanding of nurses as crucial contributors to the diagnostic process builds on the recommendations of the IOM report The Future of Nursing: Leading Change, Advancing Health (IOM, 2011a). This report provided a road map for transforming nursing practice in the United States. To achieve the necessary changes, the report offered four key recommendations (IOM, 2011a):
- Nurses should practice to the full extent of their education and training.
- Nurses should achieve higher levels of education and training through an improved education system that promotes seamless academic progression.
- Nurses should be full partners, with physicians and other health professionals, in redesigning health care in the United States.
- Effective workforce planning and policy making require better data collection and an improved information infrastructure.
In the 5 years since the report’s release, there has been increased awareness of and growing support for these recommendations in nursing schools, health care professional societies, and health care organizations. For example, AARP and the Robert Wood Johnson Foundation recently launched the “Future of Nursing: Campaign for Action,” an initiative designed to drive implementation of the report’s recommendations.2 Despite these efforts, progress in the implementation of these recommendations has been uneven. Reenvisioning the roles that nurses play in the diagnostic process is one component of these larger efforts to transform the practice of nursing in the United States.
Radiology technologists and laboratory scientists also play important roles in the diagnostic process. In some cases, radiology technologists take images and make decisions, such as how many and what type of images to take. For example, ultrasound technologists will capture images of normal structures and take additional images of any abnormalities they find. If the radiology technologist does not notice an abnormality, important information may not be conveyed to the radiologist, which may negatively impact the diagnostic process. Laboratory scientists are tasked with procuring samples, preparing samples for analysis, performing analyses, and ensuring that the testing tools are functioning properly. In some cases, these scientists may detect a specimen abnormality during the analysis process that suggests an unsuspected diagnosis or necessitates further investigation.
Pharmacists can make important contributions to the diagnostic process, especially in identifying and averting health problems that stem from drug side effects and interactions (Hines and Murphy, 2011; Malone et al., 2005). Pharmacists and treating clinicians can collaborate to identify whether a patient’s symptoms may be due to the side effects of a particular drug or the interaction of multiple medications. Because clinicians may not be aware of all possible drug side effects or interactions, pharmacists may also provide input in the selection of medications for a patient’s health problem.
______________
Facilitating Teamwork in Clinical Practice
Health care organizations play a critical role in ensuring effective teamwork. Thus, the committee recommends that health care organizations should facilitate and support intra- and interprofessional teamwork in the diagnostic process. There are a number of strategies that health care organizations can employ to improve teamwork in the diagnostic process. Creating a culture that encourages intra- and interprofessional collaboration is critical, as is designing a work system that is supportive of effective teamwork, including the use of results reporting tools that convey important information to the diagnostic team members (see Chapter 6). For example, the use of health IT and telemedicine may help facilitate communication and collaboration among team members, especially when geographically distant health care professionals are involved in the diagnostic process (see Chapter 5). The following section describes several opportunities for improving collaboration, such as care delivery reforms, treatment planning conferences, diagnostic management teams, integrated practice units, morbidity and mortality conferences, and multidisciplinary rounds.
Care Delivery Reforms
Two care delivery reforms—patient-centered medical homes (PCMHs) and accountable care organizations (ACOs)—have recently been implemented across the country as a means to improve patient care coordination and increase communication among health care professionals (see Chapter 7). PCMHs are designed to improve the quality of primary care by fostering a sense of partnership among patients and clinicians and by designating a particular health care practice as being accountable for a patient’s care (Health Affairs, 2010; Schoen et al., 2007). PCMHs can improve team-based care by acting as the nexus of coordination and communication for a patient and his or her health care professionals; recent evidence suggests that attempts to improve primary care by enhancing its role in coordination have shown some success in improving patient and staff experiences and reducing hospitalization (AHRQ, 2010a). Some PCMH demonstrations are still under evaluation, and other PCMHs are trying new formats; for example, Maryland Blue Cross Blue Shield is offering incentives for physicians to form virtual panels that serve as de facto PCMHs (CMS, 2013; Dentzer, 2012). Barriers to PCMHs include the high up-front costs associated with implementing the health IT infrastructure necessary for improved communication and collaboration and also difficulties in incentivizing outside clinicians to work with those in the PCMH (Crabtree et al., 2010; Rittenhouse et al., 2009).
ACOs are organized groups of health care professionals, practices, or hospitals that work together to assume responsibility for and provide cost-effective care to a defined population of beneficiaries. The Affordable Care Act created ACOs to address delivery system fragmentation and to align incentives to improve communication and collaboration among health care professionals (Berwick, 2011). Although the evidence needed to evaluate the impact of ACOs on improved communication and care coordination is still being collected, there are early indications that ACOs can improve patient care. For example, the Medicare Physician Group Practice, the predecessor to ACOs, demonstrated achievement of 29 of 32 quality measures (Iglehart, 2011), and an early study shows that some Pioneer ACOs were able to reduce overall costs (CMS, 2013). As with PCMHs, high initial costs associated with health IT implementation are a barrier to implementation (Kern, 2014).
Treatment Planning Conferences
Treatment planning conferences (also referred to as tumor boards) are a form of case review in which a multidisciplinary team of health care professionals “review and discuss the medical condition and treatment options of a patient” (NCI, 2015). Treatment planning conferences are often held for specific types of cancers, and their participants may include surgeons, medical oncologists, radiologists, radiation oncologists, pathologists, nurses, and other collaborating health care professionals. These conferences generally serve two purposes: to help diagnose complex cases involving cancer and to consider treatment options for patients with a cancer diagnosis. An advantage of this approach is that it provides a collaborative environment where an intra- and interprofessional team of clinicians can share information and opinions. The evidence on whether treatment planning conferences improve patient outcomes is inconclusive; although a number of studies have found that a small percentage of initial cancer diagnoses changed after review in a treatment planning conference (Chang et al., 2001; Cohen et al., 2009; Newman et al., 2006; Pawlik et al., 2008; Santoso et al., 2004), a multisite study found that treatment planning conferences did not significantly improve the quality of care of patients (Keating et al., 2012). Despite the mixed evidence, treatment planning conferences may help to identify and avoid potential diagnostic errors by bringing multiple perspectives to challenging diagnoses. This approach could also be applied to diagnoses other than cancer, especially ones with serious health consequences or complex symptom presentations.
Diagnostic Management Teams
Health care organizations can support teamwork among pathologists, radiologists, other diagnosticians, and treating health care professionals by forming diagnostic management teams (DMTs).3 For example, Vanderbilt University’s DMT is designed to improve diagnosis through improved communication and access to diagnostic specialists; it offers participating health care professionals assistance in selecting appropriate diagnostic tests and interpreting diagnostic test results (Govern, 2013). DMT consultations consider a patient’s clinical information to provide a context for the test result, and they ensure that a clinically valuable interpretation is included in the test result report. Clinicians who participate in this process report a favorable view of DMTs, and although perceived high initial costs are a potential barrier, there is some evidence that DMTs can lower overall costs (Seegmiller et al., 2013).
Integrated Practice Units
Integrated practice units (IPUs) have been proposed as a way to improve the value of health care and to address the communication problems that result from system fragmentation (Porter, 2010; Porter and Lee, 2013). An IPU is a group of clinicians and non-clinicians who are responsible for the comprehensive care of a specific medical condition and the associated complications or for a set of closely related conditions (Porter and Lee, 2013). The members of an IPU have expertise in the relevant condition and work together as a team to provide total care for patients, including inpatient care, outpatient care, and health care education. The IPU model, which has been applied to such conditions as breast cancer and joint replacement, has been shown to improve patient outcomes. For example, patients treated by a spinal care IPU were found to miss fewer days of work, require fewer physical therapy visits, and fewer magnetic resonance images to evaluate their back problems (Porter and Lee, 2013).
Morbidity and Mortality Conferences
Morbidity and mortality (M&M) conferences are forums that bring clinicians together to review cases involving medical errors and adverse events that have occurred. M&M conferences have been used to better understand how errors occur and to help health care organizations identify work system failures and develop interventions to address these failures
______________
3 Personal communication, M. Laposata, August 8, 2014.
(AHRQ, 2008). These conferences have been used to elucidate the causes of diagnostic error and to help improve diagnostic performance (Cifra et al., 2014, 2015).
Multidisciplinary Rounds
Multidisciplinary rounds (also referred to as interdisciplinary rounds) bring health care professionals from different disciplines together to consider the diagnosis and treatment of specific patients. These rounds may involve interacting with patients, or may be part of a lecture with a patient-actor. They provide an opportunity for health care professionals to learn how other health care professionals approach medical issues and to interact with health care professionals from different disciplines. Multidisciplinary rounds have been associated with improvements in care quality, shortened length of stays, and enhancements in resident education (O’Mahony et al., 2007).
PATIENT ENGAGEMENT IN DIAGNOSIS
The IOM report Crossing the Quality Chasm: A New Health System for the 21st Century highlighted patient-centeredness as a core aim of the health care system and defined it as “providing care that is respectful of and responsive to individual patient preferences, needs, and values and ensuring that patient values guide all clinical decisions” (IOM, 2001, p. 6). A critical feature of patient-centeredness is the active engagement and shared decision making of patients and their families in the patients’ health care. Patient engagement has been defined as “actions [people] take to support their health and benefit from health care” (CFAH, 2015) and has been shown to increase patient satisfaction with care and to improve health outcomes (Boulding et al., 2011; Etchegaray et al., 2014; Glickman et al., 2010; Lucian Leape Institute, 2014; Safran et al., 1998; Sequist et al., 2008; Weingart, 2013). The goal of patient engagement in diagnosis is to improve patient care and outcomes by enabling patients and their families to contribute valuable input that will facilitate an accurate and timely diagnosis and improve shared decision making about the path of care. There are a variety of factors that present challenges to patient engagement in diagnosis, and the committee makes one recommendation to improve patient and family engagement in the diagnostic process.
Challenges to Patient Engagement in Diagnosis
Patients and their families may not be effectively engaged in the diagnostic process for a variety of reasons, including both patient-related factors and health care professional and system factors (see Box 4-3).
Patient-Related Factors
The patient-related factors that prevent active engagement in the diagnostic process can include unfamiliarity with and poor access to the health care system; difficulty with communication due to language, health literacy, and cultural barriers; and a patient’s lack of comfort in taking
BOX 4-3
Challenges to Effective Patient and Family Engagement in the Diagnostic Process
Patients and families may:
- Fear complaining and being seen as difficult
- Feel a lack of control or vulnerability for many reasons (sick, scared, social status)
- Not always take their own problems seriously enough
- Lack understanding of the health care system or opportunities to become involved
- Encounter inexperienced health care professionals
- Have language and health literacy barriers
- Be unsure how to seek resolution to a problem when issues are not resolved at the point of care
Health care professionals may:
- Dismiss patients’ complaints and knowledge
- Act on implicit or explicit biases and stereotypes
- Incorrectly assume that a patient does not want to be involved in his or her care
Health care systems may exhibit:
- Disjointed care through a lack of coordination and teamwork
- Breakdowns in communication among health care professionals
- Failure to transmit information to patients
- Failure to adequately review or follow up on diagnostic testing results
- Lack of disclosure or apology after diagnostic errors
SOURCE: McDonald et al., 2013. Adapted by permission from BMJ Publishing Group Limited. The patient is in: Patient involvement strategies for diagnostic error mitigation. McDonald, K. M., C. L. Bryce, and M. L. Graber. BMJ Quality and Safety 22(2):30–36. 2013.
an active role in diagnosis. Patients are a heterogeneous population, and their needs, values, preferences, and ability to engage in the diagnostic process vary considerably.
Some patients may fear asserting themselves in the diagnostic process because they do not want to appear to be difficult and risk alienating their clinician, which could affect the quality of their care (Frosch et al., 2012). In one study involving cancer patients who thought there had been a serious breakdown in their care, 87 percent did not formally report their concern to the health care organization (Mazor et al., 2012). A patient may also feel uncomfortable asking for a referral to seek a second opinion or asking to see a more experienced clinician (Entwistle et al., 2010). The stress that patients feel related to their health, to navigating the health care system, to missing work, or to dealing with insurance issues can make them less likely to participate in their own care (Evans, 2013). A patient’s symptoms and severity of illness can also prevent active engagement in the diagnostic process.
Access to the health care system varies across patients, depending on factors such as health insurance coverage, socioeconomic status and the affordability of health care, and health care delivery system attributes, which in turn can affect the patient’s care. For example, the location of health care facilities and the hours of availability for patient care can affect a patient’s access to health care. Poor access to, and unfamiliarity with, the health care system may contribute to delays in seeking care for symptoms, which can result in a disease being more advanced when it is diagnosed, leading to a worse prognosis or a more invasive treatment which could have been avoided. Certain populations are more likely to have difficulty obtaining care, including racial and ethnic minorities and individuals of low socioeconomic status (AHRQ, 2013a,b).
Cultural and language barriers can be significant challenges that prevent patients from fully engaging in the diagnostic process. Approximately 22 percent of the 60 million people living in the United States who speak a language other than English at home report not being able to speak English well or at all (Ryan, 2013). The IOM report Unequal Treatment: Confronting Racial and Ethnic Disparities in Health Care noted that “Language barriers may affect the delivery of adequate care through poor exchange of information, loss of important cultural information, misunderstanding of physician instruction, poor shared decision making, or ethical compromises (e.g., difficulty obtaining informed consent)” (IOM, 2003b, p. 17). In addition, The Joint Commission has found that miscommunications and misunderstandings increase the risk for adverse events in health care (The Joint Commission, 2007). These barriers have also been associated with diagnostic errors (Flores, 2006; Marcus, 2003; Price-Wise, 2008). To meet the needs of patients with limited English pro-
ficiency, some health care organizations have instituted policies to ensure that language services, such as those provided by interpreters, are available and that educational literature is provided in languages other than English (HHS, 2015). Despite these steps, a study found that even when hospitals have a policy regarding language services, they often do not provide staff with the training necessary to access language services, they do not assess the competency of interpreters, and there is little oversight of the quality of the translated literature (Wilson-Stronks, 2007).
Even if a patient speaks the same language as his or her clinicians, there can be communication challenges if the patient has limited health literacy or if clinicians use unfamiliar medical terminology (IOM, 2004). In the United States more than 80 million adults have a poor level of health literacy, which has been defined as “the degree to which individuals have the capacity to obtain, process, and understand basic health information and services needed to make appropriate health decisions” (AHRQ, 2011, p. ES-1). Health literacy requires applying a complex set of skills involving reading, listening, analysis, and decision making to health settings (NNLM, 2013). Patients lacking health literacy skills may be limited in their ability to participate in the diagnostic process and in decision making about the planned path of care (Peters et al., 2007). A recent study indicated that a group of medical trainees, including PA and MD students, lacked confidence in their ability to communicate effectively with patients with low health literacy (Ali et al., 2014).
There is a tremendous amount of information and resources available on the Internet and mobile applications to help patients identify potential diagnoses and to plan for health care appointments. A 2013 Pew Research Center study found that 35 percent of American adults have used online resources to diagnose a condition in themselves or someone else (Fox and Duggan, 2013). These resources have varying levels of accuracy, and patients may have difficulty assessing the quality of the information available to them (NLM, 2012b; Semigran et al., 2015). Clinicians may also react negatively to patients’ use of this information in clinical visits (Julavits, 2014).
Patients’ level of comfort with actively engaging in care decisions, such as asking questions, stating preferences, or seeking alternative opinions, may differ considerably from one patient to another. Some patients may prefer to be actively involved in all aspects of the decision-making process, while others would rather defer to their clinicians’ judgment (Fowler, 2011). In a national survey, the majority of respondents reported that they would like clinicians to effectively engage them in health care decision making by talking about their diagnosis and explaining the options available, including the risks and their impact on quality of life and the costs associated with them (IOM, 2012b). Another survey found that 96 percent of respondents desired to be asked questions and to be given choices regarding their care,
and approximately half preferred to have their clinicians make the final decisions (Levinson et al., 2005). Clinicians may not be aware of—or they may misjudge—the role that a patient desires to play in decision making, and as a result they may make decisions that are misaligned with patient preferences, a phenomenon that has been referred to as a preference misdiagnosis (Mulley et al., 2012). Factors such as age, gender, medical history, familiarity with the health care system, socioeconomic status, and cultural issues can factor in to patients’ preferences regarding engagement and shared decision making (Boyer et al., 2001; Cox et al., 2012; Lipson et al., 2003; Longtin et al., 2010). Several studies have found that female patients who are younger and have more education tend to prefer a more active role in decisions regarding their health (Arora and McHorney, 2000; Deber et al., 2007; Say et al., 2006). A survey of low-income patients faced with major medical decisions found that 75 percent wanted to be very involved in the decision-making process (BSCF, 2014).
Health Care Professional and System Factors
A major concern cited by health care professionals is a lack of time to truly engage patients in the diagnostic process (Anderson and Funnell, 2005; Sarkar et al., 2012, 2014; Stevenson, 2003). Compared to more procedure-oriented tasks, fee-for-service payment does not incentivize the time spent on evaluation and management services that reflect the cognitive expertise and skills that clinicians employ in the diagnostic process (National Commission on Physician Payment Reform, 2013). This creates an environment in which communication, such as the clinical history and interview, may be rushed and patients may not have time to thoroughly discuss their symptoms and health concerns, although new models of payment and care delivery may make this a higher priority (AHRQ, 2014c; Cosgrove et al., 2013; Roades, 2013) (see Chapter 7). Time pressures may also lead to an overreliance on diagnostic testing in place of patient engagement, even when these may be inappropriate (Newman-Toker et al., 2013; Rao and Levin, 2012; Zhi et al., 2013) (see Chapter 3). The use of EHRs may also lead to problems with patient engagement, as health care professionals may be distracted from communicating with patients as they enter information in the EHR (O’Malley et al., 2010; Spain, 2014) (see Chapter 5).
Although many clinicians are positive about engaging with their patients (Stevenson, 2003), there are indications that some may be resistant to active patient involvement (Graedon and Graedon, 2014; Haskell, 2014; IOM, 2013a; Julavits, 2014). In interactions with patients, certain clinician behaviors can discourage open communication and patient engagement, including being dismissive of a patient’s complaints and their
knowledge of their symptoms, not listening, or interrupting frequently (Dyche and Swiderski, 2005; Marvel et al., 1999; McDonald et al., 2013). For example, one study found that after a clinician entered the room, patients spoke without being interrupted for an average of only 12 seconds; the clinicians frequently interrupted the patients before they had finished speaking (Rhoades et al., 2001). Clinicians’ vulnerability to cognitive and affective biases may also contribute to behaviors that hinder patient engagement and contribute to diagnostic errors (Croskerry, 2013; Klein, 2005). Clinicians may exhibit biases in regard to gender, race, ethnicity, sexual orientation, age, obesity, a patient’s health problem (e.g., chronic pain, mental health), or other factors (IOM, 2003b, 2011b,c, 2012e; Puhl and Brownell, 2001; Schwartz et al., 2003). For example, clinicians may be judgmental or blame patients for their illnesses, and this could affect a patient’s willingness to participate in the diagnostic process (Croskerry, 2003). Patients may fear disclosing sensitive information to their clinicians, such as their sexual orientation, due to a fear that such disclosure could negatively affect their care (Durso and Meyer, 2013; Foglia and Fredriksen-Goldsen, 2014; IOM, 2011b). If this information is not disclosed, Foglia and Fredriksen-Goldsen (2014) note that it could result in diagnostic error, such as a delay in diagnosing a serious health problem. The Unequal Treatment report found that “bias, stereotyping, prejudice, and clinical uncertainty on the part of health care providers may contribute to racial and ethnic disparities in healthcare” (IOM, 2003b, p. 12). For example, one study found that a patient’s race and gender independently influenced how physicians managed chest pain; physicians were significantly more likely to refer white men exhibiting signs of coronary artery disease for cardiac catheterization than to refer black women with the same symptoms (Schulman et al., 1999). Clinicians may also disregard symptoms in patients with previous diagnoses of mental illness or substance abuse and may attribute new physical symptoms to a psychological cause without a proper evaluation. Alternatively, clinicians may incorrectly diagnose or assume psychiatric, alcohol, or drug abuse diagnoses for serious medical conditions, such as hypoxia, delirium, metabolic abnormalities, or head injuries; a mistake known as a “psych-out error” (Croskerry, 2003).
Fragmentation of health care and poor coordination of care hinder patient engagement and can contribute to errors in diagnosis (CFAH, 2014c; Gandhi and Lee, 2010; Gandhi et al., 2006; IOM, 2013a; Schiff, 2008; Starfield, 2000). In cases where there is poor care coordination and communication among clinicians, patients and their families may need to convey their information among their health care professionals. For example, one survey found that approximately 25 percent of patients reported that their doctors did not share information about their medical history or
test results with other health care professionals involved in a patient’s care (Stremikis et al., 2011). Limited interoperability among EHRs and laboratory and medical informatics systems may also prevent the flow of information among clinicians and health care settings (see Chapter 5).
Improving Patient Engagement in the Diagnostic Process
Patients and their families play a crucial role in the diagnostic process but the ultimate responsibility for supporting and enabling patient and family engagement in the diagnostic process rests with health care professionals and organizations. Health care professionals need to embrace patients and their families as essential partners in the diagnostic process, with valuable contributions that can improve diagnosis and avert diagnostic errors. Thus, the committee recommends that health care professionals and organizations should partner with patients and their families as diagnostic team members and facilitate patient and family engagement in the diagnostic process, aligned with their needs, values, and preferences.
Learning About the Diagnostic Process
To facilitate patient and family engagement, the committee recommends that health care professionals and organizations provide patients with opportunities to learn about the diagnostic process. One of the challenges that patients and their families face with diagnosis is their unfamiliarity with the process; thus, informing patients and their families about it has the potential to improve engagement and reduce diagnostic errors. Patients may be unfamiliar with the terminology related to the diagnostic process, such as a “differential diagnosis” or a “working diagnosis,”4 and also with the role of time in the process. For example, a health care professional may propose a working diagnosis if there is some uncertainty in the diagnosis, and this may change with new information. For some health problems, watchful waiting is appropriate, and patients need to be informed that time can give clinicians a better understanding of their health problem. It is also important that patients understand when and who to contact if their symptoms do not resolve or if they experience new symptoms that do not seem to fit with a working diagnosis. Providing information explaining the roles and tasks of the various individuals
______________
4 A differential diagnosis is a list of possible diagnoses ranked from most probable to least probable based on the available information. A working diagnosis is a preliminary or provisional diagnosis, and it may be in the form of a differential diagnosis.
involved in diagnosis could also facilitate more active engagement in the diagnostic process.
A number of groups have developed information and resources to help patients become more actively involved in their health care, including the diagnostic process (CFAH, 2014c; The Joint Commission, 2015; Josiah Macy Jr. Foundation, 2014; Lucian Leape Institute, 2014). The Center for Advancing Health has developed a variety of resources to help patients gain maximum benefit from their health care, including information about communicating with clinicians, organizing health care, seeking knowledge about health, and other topics (CFAH, 2014a,b). The Speak Up™ Program offers materials to help patients become more actively involved in their care and avoid errors (The Joint Commission, 2015). The National Patient Safety Foundation, the Society to Improve Diagnosis in Medicine, and Kaiser Permanente have developed resources to help patients get the right diagnosis (see Boxes 4-4 and 4-5) (Kaiser Permanente, 2012; NPSF and SIDM, 2014). The actions suggested in the resources include having a thorough knowledge of medical history, formulating notes about symptoms and questions to bring to appointments, and maintaining a list of medications (such as prescriptions, over-the-counter medications, dietary supplements, and complementary and alternative medicines). Health care professionals and organizations can also inform patients and families about the reliability and accuracy of online resources and direct them to reputable sources (FamilyDoctor.org, 2014; Mayo Clinic, 2015; NLM, 2012a,b; Semigran et al., 2015).
Health Care Environments That Are Supportive of Patient and Family Engagement
Health care professionals and the organizations in which they practice can facilitate patient engagement in the diagnostic process by improving communication and shared decision making and by addressing health literacy barriers. Thus, the committee recommends that health care professionals and organizations should create environments in which patients and their families are comfortable engaging in the diagnostic process and sharing feedback and concerns about diagnostic errors and near misses. Health care organizations will need to carefully consider whether their care delivery systems and processes fully support patient engagement and work to improve systems and processes that are oriented primarily toward meeting the needs of health care professionals rather than patients and their families. One of the most important actions that health care professionals can take to implement this recommendation is to improve their communication skills because effective patient–clinician communication is critical to making accurate diagnoses and to averting diagnostic errors. Several organizations offer communication training
BOX 4-4
Checklist for Getting the Right Diagnosis
- Tell Your Story Well: Be clear, complete, and accurate when you tell your clinician about your illness.
- Be Clear – Take some time to think about when your symptoms started, what made your symptoms better or worse, or if your symptoms were related to taking medications, eating a meal, exercising, or a certain time of day.
- Be Complete – Try to remember all of the important information about your illness. Write down some notes and bring them with you. A family member may be able to help you with this.
- Be Accurate – Sometimes you may see multiple clinicians during a medical appointment. Make sure your clinicians hear the same story regarding your illness.
- Be a Good Historian:
- Remember what treatments you have tried in the past, if they helped, and what, if any, side effects you experienced.
- Think about how your illness has progressed over time.
- Think about your family’s medical history and if you may be at risk for similar illnesses.
- Keep Good Records:
- Keep your own records of test results, referrals, and hospital admissions.
- Keep an accurate list of your medications.
- Bring your medication list with you when you see your clinician or pharmacist.
- Be an Informed Consumer:
- Learn about your illness by looking at reliable sources on the Internet or visit a local library.
- Learn about the tests or procedures you are having done.
- Learn about your medications:
- Know the names of your medications (both brand names and generic). For example: Tylenol (brand name) and acetaminophen (generic name)
- Know what the medication is for.
- Know the amount (dose) you need to take.
- Know the time(s) you need to take it during the day.
- Know the side effects to watch for and report to your clinician.
- Know if the medication interacts with any food or drugs.
- Take Charge of Managing Your Health:
- When meeting with your clinician, use the Ask Me 3 brochure, Good Questions for Getting the Right Diagnosis:
- What could be causing my problem?
- What else could it be?
- When will I get my test results, and what should I do to follow up?
- If you have more than one clinician, make sure each clinician knows what the other person is thinking and planning.
- Make sure each clinician knows all of your test results, medications, or other treatments.
- Be informed and involved in decisions about your health.
- When meeting with your clinician, use the Ask Me 3 brochure, Good Questions for Getting the Right Diagnosis:
- Know Your Test Results:
- Make sure both you and your clinician get the results from any tests that are done.
- Don’t assume that no news is good news; call and check on your test results.
- Ask what the test results mean and what needs to be done next.
- Follow Up:
- Ask when you need to make another appointment (follow up) with your clinician once you start treatment.
- Ask what to expect from the treatment or what it will do for you.
- Ask what you need to do if you get new symptoms or start to feel worse.
- Make Sure It Is the Right Diagnosis:
- Sometimes your diagnosis is the most “likely” thing that is wrong, but it may not be the “right” diagnosis.
- Don’t be afraid to ask “What else could this be?”
- Encourage your clinicians to think about other possible reasons for your illness.
- Record Your Health Information and Monitor Your Progress:
- Track your health information and share it with your health care team in a structured format.a
——————
a One available resource is SIDM’s patient toolkit (SIDM, 2015).
SOURCES: Adapted from NPSF, 2015a; NPSF and SIDM, 2014. Reprinted, with permission, from the National Patient Safety Foundation and Society to Improve Diagnosis in Medicine. Ask Me 3 is a registered trademark of Pfizer Inc. and is licensed to the National Patient Safety Foundation.
BOX 4-5
Smart Partners About Your Health
SMART CHECKLIST
-
Symptoms
Tell your clinician what’s currently wrong . . . why you are here. Is this a new symptom, when did it start, what home remedies have you tried?
-
Medical/medication history
Provide medical information about your past. Be prepared to discuss your current medications and over-the-counter medicines or supplements that you take (Ibuprofen, vitamins, etc.) with your clinician.
-
Assessment
Describe what you think is going on. Express your feelings and your concerns.
-
Review
After your clinician diagnoses your condition, ask if it could be something else. Make sure you understand what is causing your symptoms. In your own words describe the diagnosis back to your clinician. Talk about things that might keep you from following your treatment plan.
-
To do
Make sure you understand what you need to do next. Repeat your treatment plan and the information you received from your clinician. Be sure to ask for your after-visit summary and follow all your clinician’s instructions or let him or her know if you can’t.
SMART SCRIPT
- Symptoms
“I’m concerned about . . .”
“Symptoms I’ve been having . . .” -
Medical/medication history
“Some of my medical history that might be important includes (a close family member had cancer).”
“To help me remember I have a list of my current medications and supplements.”
-
Assessment
“I’m worried I might have ___ and I have tried . . .”
After your clinician diagnoses your condition, ask questions and verify next steps.
-
Review
“Could you tell me what else it could be or if more than one thing is going on?”
- To do
“Just to make sure I haven’t missed anything, I need to . . .”
BEFORE YOUR VISIT THINK ABOUT . . .
- What you want to talk about during your visit
What symptoms are you having?
How long have you had them?
Do they go away?
Have you tried any home treatments? If so, what? -
Inviting someone to go with you
Bringing someone to your appointment can help you to answer questions and give your clinician information.
- Write down your questions or some words that will help remind you
What concerns do you have about your symptoms?
What concerns are most important to you? -
Be prepared
Be prepared to go over your medications, vitamins, and supplements.
Make sure you mention any changes that you have made.
DURING YOUR VISIT . . .
- Confirm with your clinician why you are there
- Your symptoms
When did your symptoms start?
Do they go away?
Where are they located?
How do they affect your daily activities? - Share what home treatments you have tried
Did they help or make your symptoms worse? - Share your worries about your symptoms
- Share what you think might be going on
YOUR DIAGNOSIS: CONSIDER ASKING THE CLINICIAN:
- What else could it be?
- Do all my symptoms match your diagnosis?
- Could there be more than one thing going on?
AT THE END OF YOUR VISIT . . .
-
Make sure you understand what you need to do next
Repeat your treatment plan and the information you received from your clinician.
If you don’t understand ask your clinician to explain any words or ideas that are confusing.
Talk about things that you feel might keep you from following the treatment plan.
Talk about other treatment plans or options.
- Be sure to ask for your after-visit summary
- Follow all your clinician’s instructions or let them know if you can’t
SOURCE: Reprinted, with permission, from Kaiser Permanente. Copyright 2012 by Kaiser Permanente.
courses for clinicians, including the Institute for Healthcare Communication and the American Academy on Communication in Healthcare (AACH, 2015; IHC, 2015).
There are several techniques and strategies that clinicians can use to improve communication and patient engagement. One of the most well-known methods is teach-back, which involves a clinician explaining a concept and then asking the patient to repeat in his or her own words what was said (Nouri and Rudd, 2015; Schillinger et al., 2003). The clinician can then evaluate whether the patient has a good understanding and, if the patient does not, can explain the concept further using a different approach in order to improve the patient’s comprehension. Patient–clinician communication can also be improved by using clear and simple language, encouraging questions, listening actively, allowing the patient to speak without interruption, and responding to the patient’s emotions. Such techniques may also help some patients overcome their fear of discussing their concerns and become more likely to share sensitive information that could provide valuable input to the diagnostic process. If patients are upset or anxious, they may be less likely to give a thorough and accurate account of their symptoms and health concerns. Inclusion of a patient’s family in a patient’s care may also facilitate engagement and comprehension.
Supportive health care environments are places where patients and families feel comfortable sharing their concerns about diagnostic errors and near misses and providing feedback on their experiences with diagnosis. As discussed in the education section of this chapter, providing feedback to health care professionals about the accuracy of their diagnoses can help improve their diagnostic performance. However, health care professionals often do not have opportunities to hear from patients about their diagnostic performance (Berner and Graber, 2008; Schiff, 2008). For example, a patient discharged from the emergency department may then see a primary care clinician, and the emergency department clinician may never hear whether the diagnosis on discharge was correct. To improve diagnostic performance, health care professionals and organizations should encourage patients and their families to follow up with their health care professionals to let them know about their experiences. Health care organizations can facilitate feedback from patients and their families by, for example, implementing procedures to follow up with patients after their visits. This feedback could also be used as a routine part of assessing patient satisfaction with clinicians and health care organizations.
In order to establish environments where patients and families can share their concerns, clinicians need to be ready to communicate with patients about the occurrence of diagnostic errors. A study involving 13 focus groups found that patients who have experienced a medical error wanted clinicians to disclose all harmful errors (Gallagher et al., 2003).
These patients sought information about what happened, why the error happened, how to mitigate the consequences of the error, and how clinicians would prevent recurrences (Gallagher et al., 2003). Clinicians have been reluctant to disclose medical errors to patients and their families because of the fear of litigation as well as anxiety over communicating these errors; however, disclosing errors has been broadly recognized as the right thing to do (AHRQ, 2014a). There is evidence that disclosure improves patient outcomes and may reduce malpractice claims and costs (AHRQ, 2014a; Hendrich et al., 2014; Kachalia et al., 2003; Mello et al., 2014) (see Chapter 7).
Fostering shared decision making, which is defined as “a collaborative process that allows patients and their providers to make health care decisions together, taking into account the best scientific evidence available, as well as the patient’s values and preferences” (IMDF, 2014), can also improve patient and family engagement in the diagnostic process. Tools to promote shared decision making are decision aids, which provide objective, evidence-based information on options that patients may have so that they can make informed decisions (IMDF, 2014; MedPAC, 2010). Although many decision aids are focused on treatment and screening decisions, some have been developed for diagnostic situations, such as an evaluation for low back pain or whether to do imaging studies for chest discomfort (Ronda et al., 2014; SCAI, 2014).
Addressing health literacy barriers may also improve patient and family engagement in the diagnostic process. Acknowledging that the health care system can place unreasonably high health literacy demands on patients and families, an IOM discussion paper identified 10 attributes of health-literate health care organizations, summarized in Box 4-6 (IOM, 2012a). For example, health care organizations can encourage the use of tools—such as Ask Me 3, Getting the Right Diagnosis, Smart Partners About Your Health, and Speak Up—in order to improve communication among patients and their clinicians. If health care organizations make it easier for patients and families to navigate, understand, and use health care services, then patients and their families can become more engaged in the diagnostic process. In addition, health care professionals and organizations can ensure that health care environments reflect cultural and language competencies (AHRQ, 2012). Some health care organizations have instituted policies to ensure that language services, such as those provided by interpreters, are available and that educational literature is provided in languages other than English. The IOM recommended the broader use of interpretation services where community need exists (IOM, 2003b), and the Department of Health and Human Services (HHS) has established national standards for culturally and linguistically appropriate care (HHS, 2015). Many health care professional schools offer cultural
BOX 4-6
Attributes of Health Literate Health Care Organizations
A health literate organization:
- Has leadership that makes health literacy integral to its mission, structure, and operations
- Integrates health literacy into planning, evaluation measures, patient safety, and quality improvement
- Prepares the workforce to be health literate and monitors progress
- Includes populations served in the design, implementation, and evaluation of health information and services
- Meets the needs of populations with a range of health literacy skills while avoiding stigmatization
- Uses health literacy strategies in interpersonal communications and confirms understanding at all points of contact
- Provides easy access to health information and services and navigation assistance
- Designs and distributes print, audiovisual, and social media content that is easy to understand and act on
- Addresses health literacy in high-risk situations, including care transition and communications about medicines
- Communicates clearly what health plans will cover and what individuals will have to pay for services
SOURCE: IOM, 2012a.
competency courses, and there are continuing education programs designed to increase cultural competency and sensitivity. Though there is evidence that improving cultural competency can improve patient satisfaction with care (Castro and Ruiz, 2009; Paez et al., 2009), the evidence connecting cultural competency with improvements in patient outcomes is limited (Beach et al., 2005; Lie et al., 2011).
Health care organizations can also facilitate patients’ reengagement with the health care system for unresolved symptoms or in other instances (such as a missed follow-up appointment). For example, Kaiser Permanente’s SureNet Program identifies people who have inadvertent lapses in care and uses electronic surveillance and staff to follow up with these patients (Danforth et al., 2014; Kanter, 2014). Closed-loop communication systems that require all information from referrals and consultations to be relayed to the treating clinician may also help ensure that patients reengage the health care system when necessary (Gandhi, 2014; Schiff, 2014a) (see Chapter 6).
Patient Access to Their Electronic Health Information
Another opportunity to encourage patient engagement in the diagnostic process is to make a patient’s health information more accessible and transparent. One way to accomplish this is through open medical records, or records that “patients, and others authorized by them, are allowed to read. . . . When used properly, they let patients see themselves through the eyes of their caregivers and give them insight into diagnoses and treatment options. Having access to such information permits patients to take a more active role in decisions about their care” (Frampton et al., 2009, p. 59). Thus, the committee recommends that health care professionals and organizations should ensure patient access to EHRs, including clinical notes and diagnostic testing results, to facilitate patient engagement in the diagnostic process and patient review of health records for accuracy. The Office of the National Coordinator for Health Information Technology’s Meaningful Use 2 requirements include patient access to their electronic health information (such as medication lists, diagnostic test results, allergies, and clinical problem lists), and organizations have begun to employ patient portals in order to enable patient access to this information (Adler-Milstein et al., 2014; Bruno et al., 2014; Furukawa et al., 2014; HealthIT.gov, 2015). Unfortunately, many organizations are having trouble meeting the Meaningful Use 2 requirement that 5 percent of patients “view, download, or transmit their health information” (Adler-Milstein, 2015).
The OpenNotes initiative, available to almost five million patients, has promoted even greater transparency of patients’ health information by inviting patients to view the notes recorded by health care professionals during a clinical visit (OpenNotes, 2015). In an analysis of patients who were invited to read their notes over the course of 1 year, approximately 70 to 80 percent surveyed said that they read their notes, understood their care plan better, and were better prepared for visits (Bell et al., 2014; Delbanco et al., 2012). Clinicians report that implementing OpenNotes results in few, if any, disruptions to their practice (Bell et al., 2014; Walker et al., 2014).
In input that was provided to the committee, the OpenNotes developers suggested that initiatives like OpenNotes have the potential to reduce diagnostic errors by enabling patients and families to catch errors within clinician notes, by encouraging patients to speak up, and by preventing diagnostic delay by helping patients better remember recommendations for tests and procedures. In addition, the developers cited transparency as a means to help patients better understand their clinicians’ thought processes, to enhance trust, and to engage family caregivers. In a pilot study, the developers found that patients with access to their medical information were more likely than those without such access to have questions,
to identify inaccuracies, and to offer additional information regarding the data in their health records (NORC, 2014).
Direct patient access to diagnostic testing results is also important to patient engagement because diagnostic errors commonly occur within the testing steps of the diagnostic process (Gandhi et al., 2006; Schiff et al., 2009). In 2014, HHS strengthened patients’ rights to directly access their laboratory test results (HHS, 2014). Prior to the implementation of this regulation, an analysis found that only 3 in 10 laboratories allowed patients or their legal representatives access to their clinical test results (Swain and Patel, 2014). Similarly, the Mammography Quality Standards Act mandated the direct reporting of mammography results to patients with a summary of the report written in easily understood terms. A study found that direct reporting improved patient satisfaction with mammography and the timeliness of the results reporting, although it did not significantly reduce patient anxiety or improve patient adherence to the recommendations (Priyanath et al., 2002). Although there is some concern that providing patients direct access to diagnostic testing results before they consult with their clinician may not be appropriate in all cases (e.g., for worrisome test results or for test results that patients may have difficulty in interpreting), there are a number of advantages to direct patient access, including reducing the likelihood that patients do not receive a test result and improving subsequent decision making and treatment (ASCP, 2014). Some organizations have implemented time delays to enable clinicians to communicate directly with patients before the patients access their diagnostic testing results electronically (Butcher, 2014).
Involvement of Patients and Families in Efforts to Improve Diagnosis
Patients and their families have unique insights into the diagnostic process, their health outcomes, and the occurrence of diagnostic errors (Etchegaray et al., 2014; Gertler et al., 2014; Schiff et al., 2014). Their perspectives are critical to identifying errors and near misses, especially ones that health care professionals may not be aware of, and they can also inform efforts to improve the diagnostic process (Gertler et al., 2014; Weingart et al., 2005). Thus, the committee recommends that health care professionals and organizations should identify opportunities to include patients and their families in efforts to improve the diagnostic process by learning from diagnostic errors and near misses. Some of the opportunities for learning include participation in root cause analyses and M&M conferences (Gertler et al., 2014; NPSF, 2015b; Schiff et al., 2014;
Zimmerman and Amori, 2007).5 For example, patients and family members may have information that is unavailable to health care professionals that can be used during a root cause analysis to identify contributors to a diagnostic error (Etchegaray et al., 2014). Participation in these events may also be satisfying to patients and their families because they have an opportunity to help improve safety and reduce the chance of future errors (Zimmerman and Amori, 2007). However, it is important for health care organizations to tailor patient and family involvement according to individual needs and preferences and to be aware of the legal constraints to involving patients and families in these efforts.
Health care organizations can also create patient and family advisory councils and use their input to design more patient-centered diagnostic processes. Patient and family advisory councils may be involved in the development, implementation, or evaluation of new programs; the design of materials or tools to improve patient–clinician relationships; and other activities (AHRQ, 2014b). These councils can involve patients and families in the design of care and can leverage their experiences in order to implement patient-centered changes, including changes that may reduce diagnostic errors (Coulter et al., 2008; IOM, 2013a). For example, a patient and family advisory council at Inova Health System played a role in designing a shift-change procedure for nursing staff that could reduce the potential for errors related to care transitions (Friesen et al., 2013).
HEALTH CARE PROFESSIONAL EDUCATION AND TRAINING
There are indications that health care professionals may not receive adequate preparation to function optimally in the diagnostic process (Brush, 2014; Dhaliwal, 2014; Durning, 2014; Richardson, 2007; ten Cate, 2014; Trowbridge et al., 2013). Education and training-related challenges include methods that have not kept pace with advances in the learning sciences6 and an insufficient focus on areas critical to the diagnostic process, such as clinical reasoning, teamwork, communication, and the use of diagnostic testing and health IT. Because there is limited research on how education and training can affect diagnosis, the committee drew from a broader literature that included research on the impact of education and training in other areas of health care, in other industries, as well as submitted expert input to the committee. Education and training across the career trajectory plays an important role in improving the diagnostic
______________
5 Root cause analysis is a problem-solving method that attempts to identify the factors that contributed to an error. M&M conferences are forums that allow clinicians to discuss and learn from errors that have occurred within an organization.
6 The learning sciences study how people learn in order to optimize education and training.
process and reducing diagnostic errors and near misses. This section describes the challenges to health care professional education and training and presents the committee’s recommendation. Though the focus is on leveraging changes in education and training to improve diagnosis, recommended actions could also have broader impact on clinical practice. For example, ensuring that clinicians have clinical reasoning skills may also improve clinicians’ abilities to treat and manage patients’ health problems. Although this section’s emphasis is on diagnosticians, the challenges and solutions are relevant to many health care professionals who participate in the diagnostic process.
Educational Approaches
The learning sciences are an interdisciplinary field that studies learning methods and principles in an effort to understand how to optimize learning (Torre et al., 2006). The findings from this field—including the importance of developing deep conceptual understandings, participative learning, building on prior knowledge, the use of reflection, and appropriate learning environments—are relevant to health care professional education and training (see Box 4-7) (Sawyer, 2006). For example, students often gain deeper knowledge when their learning involves activities that mimic those of professionals engaged in the relevant discipline, a learning style that has been described as “authentic practice” (Sawyer, 2008). The learning sciences have also found that some learning styles are better suited for some individuals than others (Dunn et al., 2002; Lujan and DiCarlo, 2006).
Health care professional education programs may not be adequately informed by advances in the learning sciences (Cooke et al., 2010; Rolfe and Sanson-Fisher, 2002). For example, programs may continue to emphasize memorization without helping students develop the deeper conceptual understandings that are needed to apply knowledge in novel, practice-based situations (Myers, 2013). This may result in them having difficulty diagnosing conditions in nonstandard contexts, such as cases involving atypical presentations or comorbidities. Educational experts have asserted that there is a tendency to focus learning on prototypical and representational cases of disease rather than on real-life presentations (AHRQ, 2010b; Papa, 2014a). While this may be appropriate for the early stages of learning, students need exposure to actual patient cases, including atypical cases, in order to be prepared to diagnose disease in practice (Dhaliwal, 2014). Programs that delay student interaction with patients until the later stages of education also miss opportunities to provide students with authentic practice (ten Cate, 2014). Given the mismatch of training and practice environments, it may be challenging to provide stu-
The following are important aspects of learning, identified by the learning sciences, for individuals engaged in knowledge work—i.e., professions that rely on using, manipulating, and generating knowledge.
- Developing deeper conceptual understanding
Students can apply learned material more broadly and across contexts if they have developed a deep conceptual understanding of the material. A deeper understanding requires learners to: (1) relate novel ideas to previous knowledge, (2) integrate knowledge into conceptual systems, (3) seek out patterns and connecting principles, (4) consider new ideas critically, (5) understand the structure of arguments and the process through which knowledge is generated, and (6) reflect on how they learn and what they understand.
- Focusing on learning
Students learn in different ways and these differences need to be considered as educational programs are designed and implemented. Programs that include participatory learning may benefit students and should be considered.
- Creating learning environments
Specifically designed learning environments can positively impact the learning process.
- Building on prior knowledge
Learning processes that move from concrete to abstract facts facilitate the knowledge integration and retention necessary to develop deep conceptual understandings.
- Reflecting on one’s knowledge
Taking time to reflect on one’s state of knowledge enhances the learning process.
SOURCE: Sawyer, 2006.
dents with authentic practice; for example, a majority of graduate medical education (GME) training occurs in inpatient settings, even though many physicians will work in outpatient settings (ACGME, 2015; Cooke et al., 2010; IOM, 2014; Josiah Macy Jr. Foundation, 2011).
Some health care professional education programs may not be providing learners adequate opportunities to achieve expertise in diagnosis. For example, educators may attempt to teach students to think like experienced clinicians even though they lack the experience and knowledge base necessary to function in this manner (ten Cate, 2014). Programs may also place insufficient emphasis on developing the skills and methods
required to pursue self-motivated, lifelong learning. Individuals who lack these skills may find it more difficult to develop diagnostic skills beyond the formal education setting, leading to challenges in remaining abreast of findings throughout a clinician’s career (IOM, 2010, 2011a).
The evaluation of students may need to be better aligned with best practices from the learning sciences. Some health care professional schools rely on training time as a means of evaluating student performance, but it has been suggested that competency-based evaluation (CBE), which evaluates students based on their competency in certain areas, may be a better method because it is a better predictor of future performance (Holmboe et al., 2010). CBE is still in development, however, and there is some disagreement about using it exclusively to assess learners’ abilities. There is limited evidence connecting CBE to improvements in student learning, and it is difficult to assess certain characteristics, such as professionalism, through a competency-based approach (Jarvis-Selinger et al., 2012; Lurie, 2012; Morcke et al., 2013).
A number of methods to assess competency have been proposed, including written and computerized testing, performance appraisals, medical record reviews, and simulations; some methods may be better suited for assessing specific competencies than others (Kak et al., 2001). Psychometric testing methods such as multiple choice and vignette-based exams have been used to evaluate clinicians’ medical knowledge, though they often do not capture key aspects of clinical reasoning that contribute to diagnostic expertise (Holmboe and Durning, 2014) (see Chapter 2). Given the importance of clinical reasoning to practice, there is now a growing movement to develop assessment methods that are better able to evaluate clinical reasoning competencies (ABIM, 2014; Holmboe and Durning, 2014). For example, the American Board of Internal Medicine’s Assessment 2020 Initiative is focused on improving cognitive assessment in internal medicine. It is evaluating the role of computer-based clinical simulations, in which a simulated patient’s condition changes as clinicians make decisions in the diagnostic and treatment processes (ABIM, 2015). Oral exams, such as chart stimulated recall and case-based discussions, as well as audio and video reviews of actual clinical encounters have also been suggested as assessment methods for clinical reasoning (Holmboe and Durning, 2014). Simulation exercises have been used to assess teamwork skills and communication competencies (Scalese et al., 2008).
Experts who provided input to the committee focused on the use of feedback to improve diagnostic performance and promote self-reflection (Schiff, 2014a; Singh, 2014; Trowbridge, 2014). Feedback is an integral part of continuous learning and can help health care professionals understand how well they are performing (Croskerry, 2000b). However, there are indications that current educational settings are not providing sufficient
opportunities for learners to receive timely feedback, and students often perceive that they receive inadequate feedback (Hekelman et al., 1993; Milan et al., 2011; Nutter and Whitcomb, 2001). Insufficient time for feedback, teacher reluctance to provide feedback, a lack of continuity in the learner–teacher relationship, and a lack of observation time necessary for feedback may all contribute to an inadequate focus on providing feedback (Bernard et al., 2011; Schiff, 2008).
A recent IOM report concluded that continuing education is also disconnected from theories of how adults learn and from the delivery of patient care (IOM, 2010). Many continuing education requirements and evaluations focus on achieving credit hours instead of on educational outcomes and competencies (IOM, 2010). The result is a continuing education system that does not meet the needs of health care professionals in practice; for example, didactic activities such as lectures are large components of continuing education, even though participatory learning opportunities may be more appropriate (Hager et al., 2008).
In light of these findings, the committee concluded that health care professional education and training needs to better reflect findings from the learning sciences. Thus, the committee recommends that educators should ensure that curricula and training programs across the career trajectory employ educational approaches that are aligned with evidence from the learning sciences. Given the heterogeneity of learners and the variety of educational objectives, it is important that educational programs consider the spectrum of learning sciences approaches when developing curricula and training opportunities. Although it is beyond the committee’s charge to recommend specific changes that should be made in health care professional education, the committee identified a number of opportunities for educators to consider. For example, programs may need to accommodate different learning styles, to include mechanisms to provide immediate feedback to learners (both positive and negative), to use CBE to assess performance, to increase the time allotted for clinical experience and patient interaction, and to place a larger emphasis on self-directed learning (Cooke et al., 2010; Hirsh et al., 2014; McLaughlin et al., 2014; Trowbridge, 2014). It may also be necessary to develop more effective forms of instruction and instructional media (Mayer, 2010), including the use of simulation-based exercises (McGaghie et al., 2011; Patel et al., 2009a). Employing deliberate practice approaches that focus on “frequent practice, rapid feedback to understand and correct errors, and raising bars with new attempts” may also be helpful (Durning, 2014; ten Cate, 2014). Changes to GME could include replacing traditional discipline-specific block rotations with longitudinal integrated clerkships in order to improve relationship building skills, both interprofessionally and among patients and clinicians (Teherani et al., 2013; ten Cate, 2014; Thibault,
2013). In addition, the IOM report The Future of Nursing: Leading Change, Advancing Health recommended the development and implementation of nursing residency programs to facilitate nursing graduates’ transition to practice and to ensure that nurses develop the knowledge and skills to deliver safe, high-quality care (IOM, 2011a). This report also emphasized the importance of developing an expectation for lifelong learning.
A number of academic institutions have implemented changes in their health professional programs, including a major shift toward incorporating more authentic practice. For example, most medical schools have introduced clinical practice experience much earlier in their curriculum rather than delaying this experience until after students have completed the basic sciences training. Programs are also experimenting with innovative ways to help students develop a deeper conceptual understanding of human biology and disease, including an increased emphasis on individualized learning, self-teaching and assessment, and an exposure to more and varied cases of disease (OHSU, 2014). Northwestern University’s Feinberg School of Medicine is adopting CBE, removing time requirements for degree completion, and moving from lecture-based instruction to small group and practice-based learning (Feinberg School of Medicine, 2015).
There is a growing recognition of the need to better align training and practice environments. For example, the Health Resources and Services Administration’s Teaching Health Center Graduate Medical Education program is providing more opportunities for authentic practice by funding community-based primary care residency programs (HRSA, 2015). The IOM report Graduate Medical Education That Meets the Nation’s Health Needs concluded that the Medicare GME payment system discourages physician training outside of the hospital setting and may not provide graduates the skills necessary for office-based practice, even though most are likely to practice in community settings (IOM, 2014). In addition, The Future of Nursing report highlighted the need to develop nursing expertise outside of hospital-based care settings. Because of the aging of the population and the shift from hospital-based to community-based care settings, there is a greater “need for nursing expertise in chronic illness management, care of older adults in home settings, and transitional services” (IOM, 2011a, p. 121).
Though many programs are beginning to initiate changes that better align with current knowledge about health care professional education, a larger focus on aligning education with the learning sciences is warranted across the career trajectory. This includes a focus on continuing education to ensure that individuals maintain and continue to develop the competencies necessary for the diagnostic process. Models of continuing education that are competency based or that focus on quality improvement
have been proposed and may improve the effectiveness of continuing education (Campbell et al., 2010; Shojania et al., 2012).
The Diagnostic Process
Improving the content of health care professional education can improve diagnostic performance and reduce the potential for diagnostic errors and near misses. Thus, the committee recommends that educators should ensure that curricula and training programs across the career trajectory address performance in the diagnostic process. The committee identified a number of areas of performance that could be improved. These are
- Clinical reasoning
- Teamwork
- Communication with patients, their families, and other health care professionals
- Appropriate use of diagnostic tests and the application of these results on subsequent decision making
- Use of health IT
Clinical Reasoning
Clinical reasoning, including diagnostic decision making, is underemphasized in current health care professional education and training (Graber et al., 2012; IOM, 2011a; Richardson, 2014; Stark and Fins, 2014; ten Cate, 2014; Trowbridge et al., 2013). This lack of focus on clinical reasoning and on the development of critical thinking skills throughout the education process is a contributor to diagnostic error (Brush, 2014; Durning, 2014; Richardson, 2007; ten Cate, 2014). A recent study found that a majority of the academic difficulties that medical students face “are of a cognitive nature and include difficulties in clinical reasoning” (Audétat et al., 2012, p. 217). Poor performance in clinical reasoning is generally discovered during later stages of training, which makes remediation more difficult (Audétat et al., 2012; Hauer et al., 2007). In recognition of the importance of clinical reasoning in health care professional education, the Medical College Aptitude Test (MCAT) recently added a critical analysis and reasoning skills section (AAMC, 2015a).
As discussed in Chapter 2, health care professionals have an ethical responsibility to improve clinical reasoning skills in order to improve diagnostic performance and avert diagnostic errors (Stark and Fins, 2014). Thus, educators need to ensure that students receive education and training opportunities that develop these skills—both fast system 1 processes
and slow system 2 processes (Brush, 2014; Durning, 2014; Richardson, 2014; ten Cate, 2014). The development of clinical reasoning includes critical thinking skills such as analysis, evidence evaluation, and interpretation (Papp et al., 2014). Opportunities to improve clinical reasoning include instruction and practice on how to develop and refine a differential diagnosis and a focus on developing probabilistic reasoning skills (see Chapter 2) and also an understanding of likelihood ratios (Brush, 2014).7 Students also need feedback and training in self-assessment and cognitive reflection in order to identify mistakes in their clinical reasoning and to assess their diagnostic performance. Without this, they may have trouble with calibration, or the development of an accurate sense of one’s diagnostic abilities. Poor calibration contributes to clinician overconfidence and diagnostic errors (Berner and Graber, 2008; Croskerry and Norman, 2008; Meyer et al., 2013; Yang et al., 2012).
The success of diagnostic reasoning often depends on one’s knowledge base of disease and the accompanying illness scripts8 (Durning, 2014; Norman, 2014; ten Cate, 2014). Students need this wide knowledge base, especially to develop fast system 1 processes that rely on pattern recognition. However, there are concerns that the exposure that students receive to disease cases, actual or simulated, is inadequate to develop effective diagnostic decision making based on pattern recognition (Dhaliwal, 2014; Eva, 2005; Norman, 2014; ten Cate, 2014; Trowbridge et al., 2013). Early clinical experience, either through simulations or with patients, as well as an exposure to a variety of cases, including atypical cases, can help develop this knowledge base (Papa, 2014b; Richardson, 2014; ten Cate, 2014).
Equally important, students need to understand and become comfortable with the uncertainty that is inherent in the diagnostic process (Durning, 2014; Kassirer, 1989). Developing a better sense of and comfort with uncertainty may help clinicians avoid diagnostic errors related to premature closure as well as inappropriate use of diagnostic testing. Improved understanding of diagnostic uncertainty can help clinicians make decisions about whether further diagnostic testing or treatment is warranted. This could also facilitate improved collaboration with other health care professionals and better communication with patients and their families about the nature of a working diagnosis.
______________
7 The prior probability of a diagnosis is the probability assigned before new information regarding the patient is used to “update” the probability in order to arrive at the posterior probability. A likelihood ratio is defined as the percentage of diseased patients with a given test result divided by the percentage of well people with that same test result (Brush, 2014).
8 Illness scripts are mental models of disease that include information about a disease, including potential causes of the disease, the pathophysiological process, and the signs and symptoms of the disease (Boshuizen and Schmidt, 2008).
Students also need exposure to easy-to-miss diagnoses and common causes of diagnostic error (Graber et al., 2012). This includes a focus on the work system factors that can contribute to diagnostic errors, such as communication and collaboration challenges among diagnostic team members; health IT tools that are not supportive of clinical reasoning activities; cultural, organizational, and physical environmental factors; and the impact of reporting, medical liability, and payment.
In addition, there needs to be a focus on heuristics (mental shortcuts) and biases, which play a role in clinical reasoning and present a major challenge to diagnosis (Croskerry, 2003, 2009, 2014; Eva and Norman, 2005; Kahneman, 2011; Klein, 1993) (see Chapter 2). Education and training that focuses on the cognitive heuristics and biases that can affect diagnosis and on how to counteract their effects are particularly important. Debiasing strategies, such as engaging in metacognition (i.e., critically thinking about one’s thinking, reasoning, and decision making) have been proposed as a means to address the negative effect that heuristics can have on decision making. A number of debiasing strategies have been proposed, including considering the opposite, debiasing through awareness of bias, becoming aware of what one does not know, and others (Hirt and Markman, 1995; Hodges et al., 2001; Mumma and Steven, 1995; Mussweiler et al., 2000; Redelmeier, 2005). There is some debate about the effectiveness and feasibility of debiasing strategies (Norman, 2014; ten Cate, 2014); for example, monitoring every decision to ensure that no bias has occurred would be inefficient because heuristics work most of the time. However, because heuristics tend to fail in predictable ways, it is possible to determine the types of situations in which some heuristics are likely to lead to error.
For example, heuristic failure is likely to occur in the emergency medicine setting, given that this environment is highly complex, inconstant, and uncertain, and that emergency clinicians often work under time constraints that force them to rely heavily on heuristics (Croskerry, 2000a, 2002). Given the susceptibility of this environment to heuristics failure, several proposed solutions focus on the use of debiasing strategies in emergency medicine (Croskerry, 2000a, 2002; Pines, 2006). Additional strategies to reduce errors related to heuristics and biases include a greater focus on the development of expertise, offering clinicians more realistic training settings, providing decision support tools, and ensuring that the work system in which the diagnostic process occurs better supports decision making (Eva and Norman, 2005; Gigerenzer, 2000; Gigerenzer and Goldstein, 1996; Marewski and Gigerenzer, 2012; Weed and Weed, 2014; Wegwarth et al., 2009) (see Chapter 6). Because there is uncertainty regarding which strategies are best at reducing the impact
of bias on diagnostic decision making, it is an area that needs further research (Croskerry et al., 2013a,b).
Several medical programs have begun offering clinical reasoning courses. For example, Dalhousie University offers a critical thinking course for medical students that teaches how decision making occurs, discusses cognitive biases and potential debiasing strategies, and provides students with tools for improved self-assessment and critical thinking development (Dalhousie University, 2015). Dalhousie also offers an online faculty development course to improve the education and training that medical students receive.
Developing clinical reasoning skills is important for practicing health care professionals who are beyond formal education and training settings. Continuing health care professional education can be leveraged to develop clinical reasoning skills as a lifelong competency. There are several continuing education opportunities available that focus on clinical reasoning and diagnosis, but a greater focus on them is needed (Cruz et al., 2009).
Teamwork and Communication
Despite widespread attention to the importance of teamwork skills, health care professionals are not adequately prepared to employ these skills in practice (IOM, 2014; Patel et al., 2009a; Pecukonis et al., 2008; Schmitt et al., 2011). The focus in this report on improving education and training in teamwork skills builds on earlier IOM work. For example, the study on continuing education concluded that professional development activities should ensure that health care professionals are proficient in the collaborative skills required for team-based care (IOM, 2010), and another study highlighted the need for transforming nursing education in order to prepare nurses to engage other health care professionals in a collaborative manner (IOM, 2011a). In addition, the IOM recently highlighted the importance of evaluating interprofessional education approaches and made recommendations on generating evidence to better identify successful interprofessional education practices (IOM, 2015).
Several leading organizations have concluded that interprofessional and teamwork training opportunities have been slow to materialize (Josiah Macy Jr. Foundation and Carnegie Foundation for the Advancement of Teaching, 2010). Barriers to teamwork and team-based education include “logistical challenges inherent in coordinating between two or more autonomous health professions schools, deep-rooted cultural differences between the health professions, differences in the educational curricula and pathways of the various health professions, and issues
around program sustainability and funding” (Josiah Macy Jr. Foundation and Carnegie Foundation for the Advancement of Teaching, 2010, p. 3).
Academic institutions and training programs are beginning to offer more opportunities for health care professionals to improve their teamwork skills. As of 2012, 76 percent of medicals schools required students to participate in interprofessional education (AAMC, 2015b). The goals of the interprofessional education programs varied, but most aimed to familiarize students with the roles of other health care professionals (89 percent) and to teach students teamwork skills (76 percent) (AAMC, 2015b). Educational settings also varied, with schools offering training in classroom programs (77 percent), simulation center programs (60 percent), and clinical practice settings (44 percent) (AAMC, 2015b). For example, the University of Virginia’s Center for Academic Strategic Partnerships for Interprofessional Research and Education offers workshops and clinical programs to improve teamwork skills and provides workshops for clinician–educators. Other programs offer courses taught jointly with students from both nursing and medical schools, provide interdisciplinary team-based training for the care of individuals with advanced illness, and use interactive interdisciplinary Web-based learning modules (Josiah Macy Jr. Foundation and Carnegie Foundation for the Advancement of Teaching, 2010). Academic centers have also been implementing simulation-based team training opportunities, which have shown promise in improving team performance and in the development of teamwork skills (Patel et al., 2009b). Although these efforts are encouraging, the committee concluded that a much greater emphasis on developing teamwork skills is needed. Rather than each program developing its own curriculum on an ad hoc basis, health care professional educators could collaborate in the development of curricula and training opportunities in teamwork.
An important teamwork skill in diagnosis is communication with patients, their families, and other health care professionals. Communication failures between health care professionals are recognized as a leading cause of patient harm and error, while poor communication between clinicians and patients is recognized as a barrier to accurate and timely diagnoses (Dingley et al., 2008; IHC, 2011). Although interpersonal communication skills are listed as a competency by the Accreditation Council for Graduate Medical Education (ACGME) and most medical specialty boards recognize communication as a core competency for practice, these skills may not be taught to students in a focused and standardized manner (Rider and Keefer, 2006). Health care professionals need to receive training in interpersonal communication skills to ensure that they can function effectively in teamwork settings. For example, one study found that students receiving communication training exhibited improved communication skills, such as relationship building and shared deci-
sion making (Yedidia et al., 2003). Effective communication training programs tend to last at least 1 day, to involve feedback, and to include role play and small group discussions (Berkhof et al., 2011). Tools to improve communication among health care professionals, such as the Situation-Background-Assessment-Recommendation Tool, help clinicians convey the most important information in an organized manner (Haig et al., 2006; Leonard et al., 2004) (see Box 4-8).
Health care professionals also need training in how to communicate openly and effectively with patients and their families. This training may include an emphasis on basic communication skills and also on
Before you call, be prepared! Be clear, concise, focus on the problem and only report what is relevant to the current situation!
Be sure you do the following:
- Assess the patient.
- Determine the appropriate person to call.
- Have the medical record available when you call.
- Review appropriate parts of the medical record (e.g., flow sheet, medication administration record, clinician notes/orders, labs).
- Use the following form to organize your conversation.
Situation: 5–10 second “punch line”—What is happening now? What are the chief complaints or acute changes?
This is __________. I’m calling about _________________________________
Background: What factors led up to this event? Pertinent history (e.g., admitting diagnosis) and objective data (e.g., vital signs, labs) that support how patient got here.
The patient has___________________________________________________
Assessment: What do you see? What do you think is going on? A diagnosis is not necessary; include the severity of the problem.
I think the problem is_______________________________________________
Recommendation: What action do you propose? State what the patient needs (get a time frame).
I request that you__________________________________________________
SOURCE: Adapted from Dingley et al., 2008.
topics such as communication with patients who are perceived as difficult, culturally and linguistically appropriate communication, interviewing techniques, history-taking skills, and delivering difficult diagnoses (AHRQ, 2015b; Smith and Longo, 2012). Other relevant strategies that could receive more attention include the teach-back method described in the patient engagement section of this chapter, encouraging questions from patients, and responding to patient emotions. In recognition of the importance of patient–clinician communication, a number of schools have implemented curricula designed to improve this communication (Georgetown University, 2015; University of Pittsburgh, 2015).
Outside of formal education settings, health care organizations can play a role in improving teamwork performance through team-based training practices (Salas et al., 2008). For example, a recent literature review found “moderate-to-high-quality evidence suggest[ing] team-training can positively impact healthcare team processes and, in turn, clinical processes and patient outcomes” (Weaver et al., 2014, p. 369). A training program designed by the Department of Defense and the Agency for Healthcare Research and Quality (AHRQ), Team Strategies and Tools to Enhance Performance and Patient Safety (TeamSTEPPS), has been used to improve teamwork in health care environments by increasing team awareness, clarifying roles and responsibilities, improving information sharing, and building efficient teams that optimize people and information to provide high quality care (AHRQ, 2015a; Straus et al., 2014). The system is at various stages of implementation in numerous facilities throughout the Military Health System (King et al., 2008). In recent years, AHRQ has launched a nationwide implementation program that trains master trainers to work with health care organizations interested in implementing TeamSTEPPS.
Diagnostic Testing
Diagnostic testing has become an integral component of the diagnostic process, yet medical school curricula have not kept pace with the advances in diagnostic testing and with how these advances affect diagnosis (Hallworth, 2011; Laposata and Dighe, 2007; Smith et al., 2010).
A 2009 report from the Centers for Disease Control and Prevention on laboratory medicine noted that there is inadequate attention and emphasis on laboratory testing in the medical school curriculum, even though it plays a central role in medical practice (CDC, 2009). Another survey detailed the lack of emphasis on laboratory medicine within medical training programs: Although approximately 78 percent of medical schools require coursework in laboratory medicine, the median time dedicated to this topic is 12.5 hours, not including exposure to laboratory medi-
cine gained through clinical rotations. However, training during clinical rotations is problematic because it is not standardized and may rely on clinician–educators who do not have an adequate background in laboratory medicine (Smith et al., 2010). Many of the processes within laboratory medicine—such as ordering the correct tests, understanding test performance characteristics (sensitivity and specificity), and interpreting tests results and, subsequently, making decisions—cannot be addressed using the teaching methods that many programs employ (Wilson, 2010).
The shortcomings in laboratory medicine education are well recognized by clinicians. According to several surveys, clinicians and students report feeling uncertain about which tests to order because of naming conventions, unfamiliarity with the available tests, and the rapid development of new diagnostic tests (Hickner et al., 2014; Laposata and Dighe, 2007). One of the largest sources of error in the test-ordering phase is health care professionals requesting an incorrect test (Laposata and Dighe, 2007). Clinicians order laboratory tests in 31.4 percent of primary care visits; however, they report uncertainty when ordering tests 14.7 percent of the time and confusion about interpreting results in 8.3 percent of the cases where they ordered tests (Hickner et al., 2014). There is also uncertainty among clinicians about applying test results to subsequent decision making, such as refining or expanding a differential diagnosis, determining the likelihood that a patient has a specific diagnosis on the basis of a positive or negative test result, deciding whether retesting or ordering new tests is appropriate, and beginning appropriate treatment. There are indications that students and practicing clinicians struggle with concepts like sensitivity and specificity and lack an understanding of how disease prevalence contributes to making decisions about a patient’s diagnosis (Kroenke, 2013; Manrai et al., 2014; Ross, 2014). In a small survey of health care professionals, three-quarters of respondents failed to correctly calculate the positive predictive value of a test result for a specific disorder (Manrai et al., 2014). Similar surveys completed several decades ago found that many health care professionals had trouble applying statistical methods and understanding statistical concepts, suggesting that this may be a longstanding gap in health care professional education (Berwick et al., 1981; Casscells et al., 1978). Another study found that medical students are generally able to describe Bayes’ theorem but are subsequently unable to apply this theorem to clinical practice (Bergus et al., 2004). These educational gaps negatively affect a clinician’s ability to appropriately assign and update diagnostic probabilities in light of test findings.
In addition, there are concerns about an inadequate focus on anatomic pathology in medical education (Magid and Cambor, 2012). While aspects of anatomic pathology are covered in the medical school curriculum, the amount has decreased significantly over the years, particularly
as medical schools have adopted integrated curricula (Talbert et al., 2009; Taylor et al., 2008). An inadequate understanding of anatomic pathology may negatively affect clinical decision making and the diagnostic process. For example, inadequate understanding of the mechanisms underlying inflammation might affect the ability to recognize diseases or disease processes and the selection of appropriate treatment to address inflammation. In addition, students may not understand the limitations of certain anatomic pathology tests (e.g., the limited sensitivity of Pap smears) and how to collect, prepare, and transport specimens (Magid and Cambor, 2011).
The use of medical imaging as a diagnostic tool has also increased substantially, and for many symptoms, medical imaging has become an integral part of the diagnostic process. Although many clinicians request medical imaging for their patients, the ordering of this imaging and the application of medical imaging interpretations to subsequent decision making are not emphasized in the medical school curriculum and subsequent training (Kondo and Swerdlow, 2013; Rubin and Blackham, 2015). Errors in imaging can occur during all phases of the process, from the ordering and selection of medical imaging to the interpretation of results and subsequent decision making. The majority of allopathic and osteopathic medical schools do not have a focused course on medical imaging, and medical imaging rotations are required in only 29 percent of medical schools (Rubin and Blackham, 2015). Typically, for most medical students medical imaging instruction is integrated into other coursework or clinical rotations in a very limited fashion (Kondo and Swerdlow, 2013; Rubin and Blackham, 2015). The teaching of important concepts in medical imaging, such as the scientific principles of imaging techniques, radiation safety, modality differences, and the use of contrast materials, is limited (Rubin and Blackham, 2015). A recent survey of fourth-year medical school students noted that the majority of students underestimated the risks associated with medical imaging techniques and were not informed about the American College of Radiology Appropriateness Criteria (Prezzia et al., 2013; Rubin and Blackham, 2015). Many medical schools do not follow the radiology-dedicated curriculum designed by the Alliance of Medical School Educators in Radiology (Rubin and Blackham, 2015).
Thus, health care professionals need improved education and training on the appropriate use of diagnostic tests and the application of these results to subsequent decision making. The committee recognizes that, given the growing number and complexity of the options available, it is not feasible to expect that clinicians will be familiarized with every available diagnostic test procedure. Therefore, in addition to improved education in diagnostic testing, improved collaboration among treat-
ing clinicians and pathologists and radiologists is warranted. Education and training focused on how to most effectively convey findings from pathologists and radiologists to treating clinicians may alleviate some of the challenges clinicians face with respect to understanding results and subsequent decision making.
Health IT
Health IT is an important component of the diagnostic process, including the involvement of EHRs, laboratory and medical imaging information systems, and decision support tools (see Chapter 5). As health IT becomes increasingly integrated into all aspects of health care, clinicians will likely rely more on it to facilitate diagnostic decision making and communication and collaboration among health care professionals and patients (Thibault, 2013). Thus, clinicians need to develop competencies in the use of health IT tools; however, many health care professionals do not receive adequate education and training in the use of health IT (Graber et al., 2012; McGowan et al., 2007). Individuals who lack competencies in health IT use will be unable to take advantage of these opportunities to improve diagnosis and reduce diagnostic error. Training health care professionals to work with health IT has been found to be a major challenge (NIST, 2010). In an effort to address this, the Office of the National Coordinator has been working with licensing bodies and medical societies to better integrate health IT into the medical education curriculum (Buntin et al., 2010). The Affordable Care Act includes provisions to incorporate health IT training into the education of primary care clinicians (Buntin et al., 2010). The IOM report Health IT and Patient Safety also emphasized the importance of improving workforce education and training on safe health IT use, using mechanisms such as formal education and postgraduate training as well as health care organization–facilitated training (IOM, 2012d).
Ensuring Competency in the Diagnostic Process
In addition to improving the content and teaching methods for health care professional education and training, oversight processes can help ensure that individuals achieve and maintain competency in the diagnostic process, including clinical reasoning, teamwork, communication, and the use of diagnostic testing and health IT. Health care professional oversight processes include education and training program accreditation, licensure, and certification. These oversight processes act as levers to induce change in the health care system: “Educational accreditation serves as a leverage point for the inclusion of particular educational content in a curriculum.
Licensure assesses that a student has understood and mastered formal curricula. Certification ensures that a practitioner maintains competence in a given area over time” (IOM, 2003a, p. 5). The committee received input suggesting that accreditation, licensure, and certification processes can be introduced to help ensure that health care professionals possess diagnostic competencies throughout the career trajectory (Brush, 2014; Papa, 2014a,b).
Organizations that accredit health care professional education and training programs (see Box 4-9) can use their accreditation requirements as a mechanism to ensure that these programs include appropriate curricular content to prepare students in the areas of the diagnostic process
Accreditation Commission for Education in Nursing uses a core of standards to evaluate and accredit nursing education programs (ACEN, 2013).
Accreditation Council for Continuing Medical Education evaluates and accredits institutions and organizations offering continuing medical education for physicians and other health care professionals (ACCME, 2015).
Accreditation Council for Graduate Medical Education accredits graduate medical education programs (i.e., residency and fellowship programs) for physicians. Student performance on milestones or time-based competencies are used to assess graduate medical education programs (ACGME, 2015).
Accreditation Review Commission on Education for the Physician Assistant accredits physician assistant education programs (ARC-PA, 2015).
American Association of Colleges of Nursing’s Commission on Collegiate Nursing Education accredits baccalaureate, graduate, and residency nursing programs (AACN, 2015).
American Osteopathic Association’s (AOA’s) Commission on Osteopathic College Accreditation accredits osteopathic medical schools, and the AOA Council on Continuing Medical Education accredits continuing medical education activities (AOA, 2015).
Liaison Committee on Medical Education, which is sponsored by the American Medical Association and the Association of American Medical Colleges, accredits medical education programs. For accreditation, programs must demonstrate that their graduates achieve the competencies necessary for subsequent training and for ensuring continuous learning and proficient practice (LCME, 2015).
that the committee has articulated. Accreditation organizations for all levels of health care professional education and training—that is, undergraduate, graduate, and continuing education—need to address diagnostic competencies. Many accreditation organizations already include skills important for diagnostic performance in their accreditation requirements, but these organizations can make competencies in the diagnostic process a larger priority within their requirements. For example, the IOM report The Future of Nursing: Leading Change, Advancing Health recommended that the “Commission on Collegiate Nursing Education [CCNE] and the National League for Nursing Accrediting Commission [NLNAC] should require that all nursing students demonstrate a comprehensive set of clinical performance competencies that encompass the knowledge and skills needed to provide care across settings and the lifespan” (IOM, 2011a, p. 282). Building on this recommendation, the CCNE and NLNAC could require nursing schools to offer interprofessional collaboration education and training opportunities focused specifically on the diagnostic process and the role of teams in achieving diagnostic accuracy. The Liaison Committee on Medical Education (LCME) and the ACGME include diagnostic competencies in accreditation requirements. For example, the LCME requires medical education programs to prepare students to “recognize and interpret symptoms and signs of disease” and “develop differential diagnoses and treatment plans” (LCME, 2015, p. 10). The ACGME and the American Board of Medical Specialties (ABMS) have identified six core competencies that all physicians should acquire during residency and fellowship programs and should maintain throughout practice (see Box 4-10) (ACGME, 2015). The ACGME is beginning to use milestones to evaluate performance on these competencies; several of these competencies are applicable to those the committee articulated (Nasca et al., 2012). For example, the ACGME requires that participating programs provide their students with opportunities to develop the skills necessary for lifelong, self-motivated learning; communication with patients, families, and other health care professionals; and a systems understanding of health care, including the importance of coordination and intra- and interprofessional teamwork (ACGME, 2015).
Organizations responsible for health care professional licensure and certification can help ensure that individual health care professionals have achieved and maintain competency in the skills essential for diagnosis. For example, the United States Medical Licensing Exam for physicians and the Uniform Licensure Requirements for practicing nurses could emphasize diagnostic competencies tailored to the scope of work of these professions (NCSBN, 2015). The ABMS, which grants board certification in more than 150 medical specialties and subspecialties, could ensure competencies in the diagnostic process both in initial board certification and
- Practice-Based Learning and Improvement: Show an ability to investigate and evaluate patient care practices, appraise and assimilate scientific evidence, and improve the practice of medicine.
- Patient Care and Procedural Skills: Provide care that is compassionate, appropriate, and effective treatment for health problems and to promote health.
- Systems-Based Practice: Demonstrate awareness of and responsibility to the larger context and systems of health care. Be able to call on system resources to provide optimal care (e.g., coordinating care across sites or serving as the primary case manager when care involves multiple specialties, professions, or sites).
- Medical Knowledge: Demonstrate knowledge about established and evolving biomedical, clinical, and cognate sciences and their application in patient care.
- Interpersonal and Communication Skills: Demonstrate skills that result in effective information exchange and teaming with patients, their families, and professional associates (e.g., fostering a therapeutic relationship that is ethically sound, uses effective listening skills with nonverbal and verbal communication; working as both a team member and at times as a leader).
- Professionalism: Demonstrate a commitment to carrying out professional responsibilities, adherence to ethical principles, and sensitivity to diverse patient populations.
SOURCES: ABMS, 2015; ACGME, 2015.
in the maintenance of certification efforts. For example, some specialty boards have begun assessing clinical reasoning skills through cognitive knowledge testing that requires clinicians to evaluate clinical scenarios in addition to content knowledge (Graber et al., 2012). Initial certification of health care professionals is important, but it may be insufficient to ensure sustained diagnostic competency throughout the career trajectory. Due to advances in the biomedical sciences, the knowledge required to maintain competency is rapidly growing; at the same time, health care professionals may also experience knowledge decay or the loss of previously learned knowledge (Cassel and Holmboe, 2008; IOM, 2013a; Su et al., 2000). Thus, many health care professional organizations, such as ABMS and the American Association of Physician Assistants, have developed renewal and maintenance of certification (MOC) programs (AAPA, 2015; ABMS, 2015). Though there has been controversy surrounding MOC, recent evidence suggests that it can improve performance (Iglehart and
Baron, 2012; O’Neill and Puffer, 2013; Teirstein, 2015). Meaningful and effective continuing education is important for all clinicians, and MOC efforts can ensure that clinicians have the appropriate competencies in the diagnostic process throughout the career trajectory. Many health care organizations now require MOC as a precondition for renewing staff privileges. Other licensure and certification organizations, including those for other health care professions, can also emphasize competency in the diagnostic process.
The committee concluded that oversight organizations, including accreditation organizations and professional licensure and certification bodies, can play an important role in improving diagnostic performance. Thus, the committee recommends that health care professional certification and accreditation organizations should ensure that health care professionals have and maintain the competencies needed for effective performance in the diagnostic process, including
- Clinical reasoning
- Teamwork
- Communication with patients, their families, and other health care professionals
- Appropriate use of diagnostic tests and the application of these results on subsequent decision making
- Use of health IT
Goal 1: Facilitate more effective teamwork in the diagnostic process among health care professionals, patients, and their families
Recommendation 1a: In recognition that the diagnostic process is a dynamic team-based activity, health care organizations should ensure that health care professionals have the appropriate knowledge, skills, resources, and support to engage in teamwork in the diagnostic process. To accomplish this, they should facilitate and support:
- Intra- and interprofessional teamwork in the diagnostic process.
- Collaboration among pathologists, radiologists, other diagnosticians, and treating health care professionals to improve diagnostic testing processes.
Recommendation 1b: Health care professionals and organizations should partner with patients and their families as diagnostic team members and facilitate patient and family engagement in the diag-
nostic process, aligned with their needs, values, and preferences. To accomplish this, they should:
- Provide patients with opportunities to learn about the diagnostic process.
- Create environments in which patients and their families are comfortable engaging in the diagnostic process and sharing feedback and concerns about diagnostic errors and near misses.
- Ensure patient access to electronic health records (EHRs), including clinical notes and diagnostic testing results, to facilitate patient engagement in the diagnostic process and patient review of health records for accuracy.
- Identify opportunities to include patients and their families in efforts to improve the diagnostic process by learning from diagnostic errors and near misses.
Goal 2: Enhance health care professional education and training in the diagnostic process
Recommendation 2a: Educators should ensure that curricula and training programs across the career trajectory:
- Address performance in the diagnostic process, including areas such as clinical reasoning; teamwork; communication with patients, their families, and other health care professionals; appropriate use of diagnostic tests and the application of these results on subsequent decision making; and use of health information technology.
- Employ educational approaches that are aligned with evidence from the learning sciences.
Recommendation 2b: Health care professional certification and accreditation organizations should ensure that health care professionals have and maintain the competencies needed for effective performance in the diagnostic process, including the areas listed above.
AACH (American Academy on Communication in Healthcare). 2015. American Academy on Communication in Healthcare. www.aachonline.org (accessed March 16, 2015).
AACN (American Assocation of Colleges of Nursing). 2015. American Association of Colleges of Nursing. www.aacn.nche.edu (accessed May 10, 2015).
AAMC (Assocation of American Medical Colleges). 2015a. About the MCAT exam. www.aamc.org/students/applying/mcat/about (accessed March 18, 2015).
AAMC. 2015b. Curriculum inventory and reports: Interprofessional education. www.aamc.org/initiatives/cir (accessed March 18, 2015).
AAPA (American Academy of Physician Assistants). 2015. American Academy of Physician Assistants. www.aapa.org (accessed March 12, 2015).
ABIM (American Board of Internal Medicine). 2014. ABIM announces initiative to seek input on physician knowledge and skill assessment approaches. www.abim.org/news/abim-initiative-seek-input-on-physician-knowledge-skill-assessment-approaches.aspx (accessed July 24, 2015).
ABIM. 2015. Assessment 2020: Feedback in action. assessment2020.abim.org/projects (accessed July 24, 2015).
ABMS (American Board of Medical Specialties). 2015. Based on core competencies. www.abms.org/board-certification/a-trusted-credential/based-on-core-competencies (accessed July 24, 2015).
ACCME (Accreditation Council for Continuing Medical Education). 2015. Accreditation Council for Continuing Medical Education. www.accme.org (accessed March 12, 2015).
ACEN (Accreditation Commission for Education in Nursing). 2013. Accreditation Commission for Education in Nursing. www.acenursing.org/?refreshed (accessed June 5, 2015).
ACGME (Accreditation Council for Graduate Medical Education). 2015. Accreditation Council for Graduate Medical Education. www.acgme.org/acgmeweb (accessed March 12, 2015).
Adler-Milstein, J. 2015. America’s health IT transformation: Translating the promise of electronic health records into better care. Paper presented at U.S. Senate Committee on Health, Education, Labor and Pensions, March 17.
Adler-Milstein, J., C. M. DesRoches, M. F. Furukawa, C. Worzala, D. Charles, P. Kralovec, S. Stalley, and A. K. Jha. 2014. More than half of U.S. hospitals have at least a basic EHR, but stage 2 criteria remain challenging for most. Health Affairs 33(9):1664–1671.
AHRQ (Agency for Healthcare Research and Quality). 2008. Transforming the morbidity and mortality conference into an instrument for systemwide improvement. In K. Henriksen, J. B. Battles, M. A. Keyes, and M. L. Grady (eds.), Advances in patient safety: New directions and approaches (Vol. 2. Culture and redesign) (pp. 357–363). AHRQ Publication No. 08-0034-2. Rockville, MD: Agency for Healthcare Research and Quality. www.ncbi.nlm.nih.gov/books/NBK43710/?report=reader#_NBK43710_pubdet (accessed July 2, 2015).
AHRQ. 2010a. The roles of patient-centered medical homes and accountable care organizations in coordinating patient care. AHRQ publication no. 11-M005-EF. Rockville, MD: Agency for Healthcare Research and Quality. http://pcmh.ahrq.gov/page/roles-patient-centered-medical-homes-and-accountable-care-organizations-coordinating-patient (accessed June 5, 2015).
AHRQ. 2010b. In conversation with. . . Pat Croskerry, MD, PhD. Web M&M morbidity and mortality rounds on the web. http://webmm.ahrq.gov/perspective.aspx?perspectiveID=87 (accessed July 24, 2015).
AHRQ. 2011. Health literacy interventions and outcomes: An updated systematic review. AHRQ Publication No. 11-E006. Rockville, MD: Agency for Healthcare Research and Quality.
AHRQ. 2012. Improving patient safety systems for patients with limited english proficiency. AHRQ Publication No. 12-0041. Rockville, MD: Agency for Healthcare Research and Quality. www.ahrq.gov/professionals/systems/hospital/lepguide/lepguide.pdf (accessed July 24, 2015).
AHRQ. 2013a. 2012 national healthcare disparities report. AHRQ publication no. 13-0003. Rockville, MD: Agency for Healthcare Research and Quality.
AHRQ. 2013b. 2012 national healthcare quality report. AHRQ publication no. 13-0002. Rockville, MD: Agency for Healthcare Research and Quality.
AHRQ. 2014a. Error disclosure. http://psnet.ahrq.gov/primer.aspx?primerID=2 (accessed March 16, 2015).
AHRQ. 2014b. Patient and family advisory councils. https://cahps.ahrq.gov/quality-improvement/improvement-guide/browse-interventions/Customer-Service/Listening-Posts/Advisory-Councils.html (accessed March 18, 2015).
AHRQ. 2014c. Patient centered medical home resource center. http://pcmh.ahrq.gov/page/defining-pcmh (accessed April 9, 2014).
AHRQ. 2015a. About TeamSTEPPS. http://teamstepps.ahrq.gov/about-2cl_3.htm (accessed March 26, 2015).
AHRQ. 2015b. Training to advance physicians’ communication skills. https://cahps.ahrq.gov/quality-improvement/improvement-guide/browse-interventions/Communication/Physicians-Comm-Training/index.html (accessed March 26, 2015).
Ali, N. K., R. P. Ferguson, S. Mitha, and A. Hanlon. 2014. Do medical trainees feel confident communicating with low health literacy patients? Journal of Community Hospital Internal Medicine Perspective 4(2).
Allen, B., and W. T. Thorwarth. 2014. Comments from the American College of Radiology. Input submitted to the Committee on Diagnostic Error in Health Care, November 5 and December 29, 2014, Washington, DC.
Anderson, R. M., and M. M. Funnell. 2005. Patient empowerment: Reflections on the challenge of fostering the adoption of a new paradigm. Patient Education and Counseling 57(2):153–157.
AOA (American Osteopathic Association). 2015. American Osteopathic Association. www.osteopathic.org (accessed March 12, 2015).
ARC-PA (Accreditation Review Commission on Education for the Physician Assistant). 2015. Accreditation Review Commission on Education for the Physician Assistant. www.arc-pa.org (accessed March 12, 2015).
Arora, N. K., and C. A. McHorney. 2000. Patient preferences for medical decision making: Who really wants to participate? Medical Care 38(3):335–341.
ASCP (American Society for Clinical Pathology). 2014. Patient access to test results. www.ascp.org/Advocacy/Patient-Access-to-Test-Results.html (accessed March 16, 2015).
Audétat, M.-C., V. Dory, M. Nendaz, D. Vanpee, D. Pestiaux, N. Junod Perron, and B. Charlin. 2012. What is so difficult about managing clinical reasoning difficulties? Medical Education 46(2):216–227.
Baldwin, D. C., and R. A. W. Tsukuda. 1984. Interdisciplinary teams. In C. K. Cassel and J. R. Walsh (eds.), Geriatric medicine: Volume III: Fundamentals of geriatric care (pp. 421–435). New York: Springer-Verlag.
Beach, M. C., E. G. Price, T. L. Gary, K. A. Robinson, A. Gozu, A. Palacio, C. Smarth, M. W. Jenckes, C. Feuerstein, E. B. Bass, N. R. Powe, and L. A. Cooper. 2005. Cultural competence: A systematic review of health care provider educational interventions. Medical Care 43(4):356–373.
Bell, S., M. Anselmo, J. Walker, and T. Delbanco. 2014. Input submitted to the Committee on Diagnostic Error in Healthcare, December 2, 2014, Washington, DC.
Bergus, G., S. Vogelgesang, J. Tansey, E. Franklin, and R. Feld. 2004. Appraising and applying evidence about a diagnostic test during a performance-based assessment. BMC Medical Education 4:20.
Berkhof, M., H. J. van Rijssen, A. J. M. Schellart, J. R. Anema, and A. J. van der Beek. 2011. Effective training strategies for teaching communication skills to physicians: An overview of systematic reviews. Patient Education and Counseling 84(2):152–162.
Bernard, A. W., N. E. Kman, and S. Khandelwal. 2011. Feedback in the emergency medicine clerkship. Western Journal of Emergency Medicine 12(4):537–542.
Berner, E. S., and M. L. Graber. 2008. Overconfidence as a cause of diagnostic error in medicine. American Journal of Medicine 121(5 Suppl):S2–S23.
Berwick, D. M. 2011. Launching accountable care organizations—The proposed rule for the Medicare Shared Savings Program. New England Journal of Medicine 364(16):e32.
Berwick, D. M., H. V. Fineberg, and M. C. Weinstein. 1981. When doctors meet numbers. The American Journal of Medicine 71(6):991–998.
Bodenheimer, T. 2008. Coordinating care—A perilous journey through the health care system. New England Journal of Medicine 358(10):1064–1071.
Borrill, C. S., J. Carletta, A. J. Carter, J. F. Dawson, S. Garrod, A. Rees, A. Richards, D. Shapiro, and M. A. West. 2000. The effectiveness of health care teams in the National Health Service. Birmingham, UK: University of Aston in Birmingham.
Boshuizen, H. P. A., and H. G. Schmidt. 2008. The development of clinical reasoning expertise: Implications for teaching. In J. Higgs, M. Jones, S. Loftus, and N. Christensen (eds.), Clinical reasoning in the health professions (pp. 113–121). Oxford: Butterworth Heinemann/Elsevier.
Boulding, W., S. W. Glickman, M. P. Manary, K. A. Schulman, and R. Staelin. 2011. Relationship between patient satisfaction with inpatient care and hospital readmission within 30 days. American Journal of Managed Care 17(1):41–48.
Boult, C., A. F. Green, L. B. Boult, J. T. Pacala, C. Snyder, and B. Leff. 2009. Successful models of comprehensive care for older adults with chronic conditions: Evidence for the Institute of Medicine’s “Retooling for an Aging America” report. Journal of the American Geriatrics Society 57(12):2328–2337.
Boyer, L., M. Williams, L. Callister, and E. Marshall. 2001. Hispanic women’s perceptions regarding cervical cancer screening. Journal of Obstetrics, Gynecologic, and Neonatal Nursing 30(2):240–245.
Bruno, M. A., J. M. Petscavage-Thomas, M. J. Mohr, S. K. Bell, and S. D. Brown. 2014. The “open letter”: Radiologists’ reports in the era of patient web portals. Journal of the American College of Radiology 11(9):863–867.
Brush, J. E. 2014. Forming good habits to decrease diagnostic error: A case for likelihood ratios. Input submitted to the Committee on Diagnostic Error in Health Care, October 21, 2014, Washington, DC.
BSCF (Blue Shield of California Foundation). 2014. Engaging California patients in major medical decisions. San Francisco, CA: Blue Shield of California Foundation.
Buntin, M. B., S. H. Jain, and D. Blumenthal. 2010. Health information technology: Laying the infrastructure for national health reform. Health Affairs 29(6):1214–1219.
Bushe, G. R., and A. Chu. 2011. Fluid teams: Solutions to the problems of unstable team membership. Organizational Dynamics 40(3):181–188.
Butcher, L. 2014. The patient portal to the future. Healthcare Financial Management Association. www.hfma.org/Leadership/Archives/2014/Spring/The_Patient_Portal_to_the_Future (accessed May 11, 2015).
Campbell, C., I. Silver, J. Sherbino, O. ten Cate, and E. S. Holmboe. 2010. Competency-based continuing professional development. Medical Teacher 32(8):657–662.
Casscells, W., A. Schoenberger, and T. B. Graboys. 1978. Interpretation by physicians of clinical laboratory results. New England Journal of Medicine 299(18):999–1001.
Cassel, C. K., and E. S. Holmboe. 2008. Professionalism and accountability: The role of specialty board certification. Transactions of the American Clinical and Climatological Association 119:295–304.
Castro, A., and E. Ruiz. 2009. The effects of nurse practitioner cultural competence on Latina patient satisfaction. Journal of the American Academy of Nurse Practitioners 21(5):278–286.
CDC (Centers for Disease Control and Prevention). 2009. Patient-centered care and laboratory medicine: National status report: 2008–2009 update.
CDC. 2014. Early Release of Selected Estimates Based on Data from the National Health Information Survey, January-September 2014: Usual place to go for medical care. www.cdc.gov/nchs/data/nhis/earlyrelease/earlyrelease201503_02.pdf (accessed May 7, 2015).
CFAH (Center for Advancing Health). 2014a. Be a prepared patient. www.cfah.org/prepared-patient (accessed March 18, 2015).
CFAH. 2014b. Center for Advancing Health engagement behavior framework. www.cfah.org/engagement/research/engagement-behavior-framework (accessed April 3, 2014).
CFAH. 2014c. What does it take for all Americans to find good health care and make the most of it? www.cfah.org/about/about-us (accessed April 3, 2014).
CFAH. 2015. Patient engagement. www.cfah.org/engagement (accessed March 16, 2015).
CFAR (Center for Applied Research), J. Tomasik, and C. Fleming. 2015. Lessons from the field: Promising interprofessional collaboration practices. White Paper, Robert Wood Johnson Foundation. www.rwjf.org/content/dam/farm/reports/reports/2015/rwjf418568 (accessed June 5, 2015).
Chang, J. H., E. Vines, H. Bertsch, D. L. Fraker, B. J. Czerniecki, E. F. Rosato, T. Lawton, E. F. Conant, S. G. Orel, L. Schuchter, K. R. Fox, N. Zieber, J. H. Glick, and L. J. Solin. 2001. The impact of a multidisciplinary breast cancer center on recommendations for patient management: The University of Pennsylvania experience. Cancer 91(7):1231–1237.
Cifra, C. L., K. L. Jones, J. A. Ascenzi, U. S. Bhalala, M. M. Bembea, J. C. Fackler, and M. R. Miller. 2014. The morbidity and mortality conference as an adverse event surveillance tool in a paediatric intensive care unit. BMJ Quality & Safety 23(11):930–938.
Cifra, C. L., K. L. Jones, J. A. Ascenzi, U. S. Bhalala, M. M. Bembea, D. E. Newman-Toker, J. C. Fackler, and M. R. Miller. 2015. Diagnostic errors in a PICU: Insights from the morbidity and mortality conference. Pediatric Critical Care Medicine: A Journal of the Society of Critical Care Medicine and the World Federation of Pediatric Intensive and Critical Care Societies 16(5):468–476.
CMS (Centers for Medicare & Medicaid Services). 2013. Pioneer accountable care organizations succeed in improving care, lowering costs. Baltimore, MD: Department of Health and Human Services. www.cms.gov/Newsroom/MediaReleaseDatabase/Press-releases/2013-Press-releases-items/2013-07-16.html (accessed June 5, 2015).
Cohen, P., A. L. Tan, and A. Penman. 2009. The multidisciplinary tumor conference in gynecologic oncology—Does it alter management? International Journal of Gynecological Cancer 19(9):1470–1472.
Cooke, M., D. M. Irby, and B. C. O’Brien. 2010. Summary of educating physicians: A call for reform of medical school and residency. San Francisco, CA: Jossey–Bass.
Cosgrove, D. M., M. Fisher, P. Gabow, G. Gottlieb, G. C. Halvorson, B. C. James, G. S. Kaplan, J. B. Perlin, R. Petzel, G. D. Steele, and J. S. Toussaint. 2013. Ten strategies to lower costs, improve quality, and engage patients: The view from leading health system CEOs. Health Affairs 32(2):321–327.
Coulter, A., S. Parsons, and J. Askham. 2008. Where are the patients in decision-making about their own care? Copenhagen, Denmark, June 25–27: World Health Organization Regional Office for Europe.
Cox, E. D., K. A. Nackers, H. N. Young, M. A. Moreno, J. F. Levy, and R. M. Mangione-Smith. 2012. Influence of race and socioeconomic status on engagement in pediatric primary care. Patient Education and Counseling 87(3):319–326.
Crabtree, B. F., P. A. Nutting, W. L. Miller, K. C. Stange, E. E. Stewart, and C. R. Jaén. 2010. Summary of the National Demonstration Project and recommendations for the patient-centered medical home. Annals of Family Medicine 8(Suppl 1):S80–S90.
Croskerry, P. 2000a. The cognitive imperative: Thinking about how we think. Academic Emergency Medicine 7(11):1223–1231.
Croskerry, P. 2000b. The feedback sanction. Academic Emergency Medicine 7(11):1232–1238.
Croskerry, P. 2002. Achieving quality in clinical decision making: Cognitive strategies and detection of bias. Academic Emergency Medicine 9(11):1184–1204.
Croskerry, P. 2003. The importance of cognitive errors in diagnosis and strategies to minimize them. Academic Medicine 78(8):775–780.
Croskerry, P. 2009. A universal model of diagnostic reasoning. Academic Medicine 84(8): 1022–1028.
Croskerry, P. 2013. From mindless to mindful practice—Cognitive bias and clinical decision making. New England Journal of Medicine 368(26):2445–2448.
Croskerry, P. 2014. Bias: A normal operating characteristic of the diagnosing brain. Diagnosis 1(1):23–27.
Croskerry, P., and G. Norman. 2008. Overconfidence in clinical decision making. American Journal of Medicine 121(5 Suppl):S24–S29.
Croskerry, P., G. Singhal, and S. Mamede. 2013a. Cognitive debiasing 1: Origins of bias and theory of debiasing. BMJ Quality and Safety 22(Suppl 2):ii58–ii64.
Croskerry, P., G. Singhal, and S. Mamede. 2013b. Cognitive debiasing 2: Impediments to and strategies for change. BMJ Quality and Safety 22(Suppl 2):ii65–ii72.
Cruz, D. M., C. M. Pimenta, and M. Lunney. 2009. Improving critical thinking and clinical reasoning with a continuing education course. Journal of Continuing Education in Nursing 40(3):121–127.
Dalhousie University. 2015. Dalhousie University Medical School critical thinking program. http://medicine.dal.ca/departments/core-units/DME/critical-thinking.html (accessed March 26, 2015).
Danforth, K. N., A. E. Smith, R. K. Loo, S. J. Jacobsen, B. S. Mittman, and M. H. Kanter. 2014. Electronic clinical surveillance to improve outpatient care: Diverse applications within an integrated delivery system. eGEMS 2(1):1056.
Deber, R. B., N. Kraetschmer, S. Urowitz, and N. Sharpe. 2007. Do people want to be autonomous patients? Preferred roles in treatment decision-making in several patient populations. Health Expectations 10(3):248–258.
Delbanco, T., J. Walker, S. K. Bell, J. D. Darer, J. G. Elmore, N. Farag, H. J. Feldman, R. Mejilla, L. Ngo, J. D. Ralston, S. E. Ross, N. Trivedi, E. Vodicka, and S. G. Leveille. 2012. Inviting patients to read their doctors’ notes: A quasi-experimental study and a look ahead. Annals of Internal Medicine 157(7):461–470.
Dentzer, S. 2012. One payer’s attempt to spur primary care doctors to form new medical homes. Health Affairs 31(2):341–349.
Dhaliwal, G. 2014. Blueprint for diagnostic excellence. Presentation to the Committee on Diagnostic Error in Health Care, November 21, 2014, Washington, DC.
Dineen, B. R., and R. A. Noe. 2003. The impact of team fluidity and its implications for human resource management research and practice. In J. J. Martocchio and G. R. Ferris (eds.), Research in personnel and human resources management, Vol. 22 (pp. 1–37). Oxford, England: Elsevier Science Ltd.
Dingley, C. D., K. Daugherty, M. K. Derieg, and R. Persing. 2008. Improving patient safety through provider communication strategy enhancements. In K. Henriksen, J. B. Battles, M. A. Keyes, and M. L. Grady (eds.), Advances in patient safety: New directions and alternative approaches (Vol. 3: Performance and tools) (pp. 90-107). AHRQ publication no. 08-0034-3. Rockville, MD: Agency for Healthcare Research and Quality. www.ahrq.gov/professionals/quality-patient-safety/patient-safety-resources/resources/advances-in-patient-safety-2/vol3/Advances-Dingley_14.pdf (accessed June 5, 2015).
Dunn, R., J. S. Beaudry, and Klavas.Angela. 2002. Survey of research on learning styles. California Journal of Science Education 2(2):75–98.
Durning, S. J. 2014. Submitted input. Input submitted to the Committee on Diagnostic Error in Health Care, October 24, 2014, Washington, DC.
Durso, L. E., and I. H. Meyer. 2013. Patterns and predictors of disclosure of sexual orientation to healthcare providers among lesbians, gay men, and bisexuals. Sexuality Research and Social Policy 10(1): 35-42.
Dyche, L., and D. Swiderski. 2005. The effect of physician solicitation approaches on ability to identify patient concerns. Journal of General Internal Medicine 20(3):267–270.
Edmondson, A. C. 2012. Teaming: How organizations learn, innovate, and compete in the knowledge economy. San Francisco: Jossey-Bass.
Entwistle, V. A., D. McCaughan, I. S. Watt, Y. Birks, J. Hall, M. Peat, B. Williams, J. Wright, and Patient Involvement in Patient Safety Group. 2010. Speaking up about safety concerns: Multi-setting qualitative study of patients’ views and experiences. Quality and Safety in Health Care 19:1–7.
Etchegaray, J. M., M. J. Ottosen, L. Burress, W. M. Sage, S. K. Bell, T. H. Gallagher, and E. J. Thomas. 2014. Structuring patient and family involvement in medical error event disclosure and analysis. Health Affairs (Millwood) 33(1):46–52.
Eva, K. W. 2005. What every teacher needs to know about clinical reasoning. Medical Education 39(1):98–106.
Eva, K. W., and G. R. Norman. 2005. Heuristics and biases—A biased perspective on clinical reasoning. Medical Education 39(9):870–872.
Evans, M. 2013. Doctors argue for decision aids to promote patient engagement. Modern Healthcare. www.modernhealthcare.com/article/20131127/MAGAZINE/311309982 (accessed April 4, 2014).
FamilyDoctor.org. 2014. Health information on the web: Finding reliable information. http://familydoctor.org/familydoctor/en/healthcare-management/self-care/health-information-on-the-web-finding-reliable-information.printerview.all.html (accessed March 16, 2015).
Feinberg School of Medicine. 2015. Education: MD curriculum at Feinburg. www.feinberg.northwestern.edu/education/curriculum/index.html (accessed March 16, 2015).
Flores, G. 2006. Language barriers to health care in the United States. New England Journal of Medicine 355(3):229–231.
Foglia, M. B., and K. I. Fredriksen-Goldsen. 2014. Health disparities among LGBT older adults and the role of nonconscious bias. Hastings Center Report 44(s4):S40–S44.
Fowler, F. 2011. Patients want to be involved. http://informedmedicaldecisions.org/wp-content/uploads/2011/05/Perspectives_Patient_Involvement.pdf (accessed June 5, 2015).
Fox, S., and M. Duggan. 2013. Health online 2013. www.pewinternet.org/2013/01/15/health-online-2013 (accessed March 18, 2015).
Frampton, S. B., S. Horowitz, and B. J. Stumpo. 2009. Open medical records. The American Journal of Nursing 109(8):59–63.
Friesen, M. A., A. Herbst, J. W. Turner, K. G. Speroni, and J. Robinson. 2013. Developing a patient-centered ISHAPED handoff with patient/family and parent advisory councils. Journal of Nursing Care and Quality 28(3):208–216.
Frosch, D. L., S. G. May, K. A. S. Rendle, C. Tietbohl, and G. Elwyn. 2012. Authoritarian physicians and patients’ fear of being labeled “difficult” among key obstacles to shared decision making. Health Affairs (Millwood) 31(5):1030–1038.
Furukawa, M. F., J. King, V. Patel, C. J. Hsiao, J. Adler–Milstein, and A. K. Jha. 2014. Despite substantial progress in EHR adoption, health information exchange and patient engagement remain low in office settings. Health Affairs 33(9):1672–1679.
Gallagher, T. H., A. D. Waterman, A. G. Ebers, V. J. Fraser, and W. Levinson. 2003. Patients’ and physicians’ attitudes regarding the disclosure of medical errors. JAMA 289(8):1001–1007.
Gandhi, T. K. 2014. Focus on diagnostic errors: Understanding and prevention. Presentation to the Committee on Diagnostic Error in Health Care, August 7, 2014, Washington, DC.
Gandhi, T. K., and T. H. Lee. 2010. Patient safety beyond the hospital. New England Journal of Medicine 363(11):1001–1003.
Gandhi, T. K., A. Kachalia, E. J. Thomas, A. L. Puopolo, C. Yoon, T. A. Brennan, and D. M. Studdert. 2006. Missed and delayed diagnoses in the ambulatory setting: A study of closed malpractice claims. Annals of Internal Medicine 145(7):488–496.
Georgetown University. 2015. First year curriculum module: Physician–patient communication. https://som.georgetown.edu/medicaleducation/curriculum/firstyearmodules/modules/ppc (accessed March 26, 2015).
Gertler, S. A., Z. Coralic, A. Lopez, J. C. Stein, and U. Sarkar. 2014. Root cause analysis of ambulatory adverse drug events that present to the emergency department. Journal of Patient Safety. February 27. Epub ahead of print.
Gigerenzer, G. 2000. Adaptive thinking: Rationality in the real world. New York: Oxford University Press.
Gigerenzer, G., and D. G. Goldstein. 1996. Reasoning the fast and frugal way: Models of bounded rationality. Psychology Review 103(4):650–669.
Glickman, S. W., W. Boulding, M. Manary, R. Staelin, M. T. Roe, R. J. Wolosin, E. M. Ohman, E. D. Peterson, and K. A. Schulman. 2010. Patient satisfaction and its relationship with clinical quality and inpatient mortality in acute myocardial infarction. Circulation: Cardiovascular Quality and Outcomes 3(2):188–195.
Govern, P. 2013. Diagnostic management efforts thrive on teamwork. http://news.vanderbilt.edu/2013/03/diagnostic-management-efforts-thrive-on-teamwork (accessed February 11, 2015).
Graber, M., R. Wachter, and C. Cassel. 2012. Bringing diagnosis into the quality and safety equations. JAMA 308(12):1211–1212.
Graedon, T., and J. Graedon. 2014. Let patients help with diagnosis. Diagnosis 1(1):49–51.
Gruman, J. C. 2013. An accidental tourist finds her way in the dangerous land of serious illness. Health Affairs 32(2):427–431.
Hager, M., S. Russell, and S. W. Fletcher. 2008. Continuing education in the health professions: Improving healthcare through lifelong learning, Proceedings of a conference sponsored by the Josiah Macy Jr. Foundation. Bermuda. New York: Josiah Macy Jr. Foundation. www.josiahmacyfoundation.org (accessed June 5, 2015).
Haig, K. M., S. Sutton, and J. Whittington. 2006. SBAR: A shared mental model for improving communication between clinicians. Joint Commission Journal on Quality and Patient Safety 32(3):167–175.
Hallworth, M. J. 2011. The “70% claim”: What is the evidence base? Annals of Clinical Biochemistry 48(6):487–488.
Haskell, H. W. 2014. What’s in a story? Lessons from patients who have suffered diagnostic failure. Diagnosis 1(1):53–54.
Hauer, K. E., A. Teherani, K. M. Kerr, P. S. O’Sullivan, and D. M. Irby. 2007. Student performance problems in medical school clinical skills assessments. Academic Medicine 82(10 Suppl):S69–S72.
Hautz, W. E., J. E. Kämmer, S. K. Schauber, C. D. Spies, and W. Gaissmaier. 2015. Diagnostic performance by medical students working individually or in teams. JAMA 313(3):303–304.
Health Affairs. 2010. Patient-centered medical homes: Health affairs policy brief. Health Affairs. September 14. http://healthaffairs.org/healthpolicybriefs/brief_pdfs/healthpolicybrief_25.pdf (accessed June 5, 2015).
HealthIT.gov. 2015. Patient ability to electronically view, download & transmit (VDT) health information. www.healthit.gov/providers-professionals/achieve-meaningful-use/core-measures-2/patient-ability-electronically-view-download-transmit-vdt-health-information (accessed March 15, 2015).
Hekelman, F. P., E. Vanek, K. Kelly, and S. Alemagno. 1993. Characteristics of family physicians’ clinical teaching behaviors in the ambulatory setting: A descriptive study. Teaching and Learning in Medicine: An International Journal 5(1):18–23.
Hendrich, A., C. K. McCoy, J. Gale, L. Sparkman, and P. Santos. 2014. Ascension Health’s demonstration of full disclosure protocol for unexpected events during labor and delivery shows promise. Health Affairs 33(1):139–145.
Henriksen, K., and J. Brady. 2013. The pursuit of better diagnostic performance: A human factors perspective. BMJ Quality and Safety 22(Suppl 2):ii1–ii5.
HHS (Department of Health and Human Services). 2013. Usual source of care: Women’s health USA: An illustrated collection of current and historical data, published annually. http://mchb.hrsa.gov/whusa13/health-services-utilization/p/usual-source-care.html (accessed May 7, 2015).
HHS. 2014. HHS strengthens patients’ right to access lab test reports. www.hhs.gov/news/press/2014pres/02/20140203a.html (accessed June 5, 2015).
HHS. 2015. What are the national CLAS standards? www.thinkculturalhealth.hhs.gov/Content/clas.asp#clas_standards (accessed May 11, 2015).
Hickner, J., P. J. Thompson, T. Wilkinson, P. Epner, M. Shaheen, A. M. Pollock, J. Lee, C. C. Duke, B. R. Jackson, and J. R. Taylor. 2014. Primary care physicians’ challenges in ordering clinical laboratory tests and interpreting results. Journal of the American Board of Family Medicine 27(2):268–274.
Hines, L. E., and J. E. Murphy. 2011. Potentially harmful drug–drug interactions in the elderly: A review. The American Journal of Geriatric Pharmacotherapy 9(6):364–377.
Hirsh, D. A., E. S. Holmboe, and O. ten Cate. 2014. Time to trust: Longitudinal integrated clerkships and entrustable professional activities. Academic Medicine 89(2):201–204.
Hirt, E., and K. Markman. 1995. Multiple explanation: A consider-an-alternative strategy for debiasing judgments. Journal of Personality and Social Psychology 69:1069–1086.
Hodges, B., G. Regehr, and D. Martin. 2001. Difficulties in recognizing one’s own incompetence: Novice physicians who are unskilled and unaware of it. Academic Medicine 76(10 Suppl):S87–S89.
Holmboe, E. S., and S. J. Durning. 2014. Assessing clinical reasoning: moving from in vitro to in vivo. Diagnosis 1(1):111–117.
Holmboe, E. S., J. Sherbino, D. M. Long, S. R. Swing, and J. R. Frank. 2010. The role of assessment in competency-based medical education. Medical Teacher 32(8):676–682.
HRSA (Health Resources and Services Administration). 2015. Teaching health center graduate medical education (THCGME). http://bhpr.hrsa.gov/grants/teachinghealthcenters (accessed March 16, 2015).
Iglehart, J. K. 2011. Assessing an aco prototype—Medicare’s physician group practice demonstration. New England Journal of Medicine 364(3):198–200.
Iglehart, J. K., and R. B. Baron. 2012. Ensuring physicians’ competence—Is maintenance of certification the answer? New England Journal of Medicine 367(26):2543–2549.
IHC (Institute for Healthcare Communication). 2011. Impact of communication in healthcare. http://healthcarecomm.org/about-us/impact-of-communication-in-healthcare (accessed March 26, 2015).
IHC. 2015. Institute for Healthcare Communication. www.healthcarecomm.org (accessed March 16, 2015).
IMDF (Informed Medical Decisions Foundation). 2014. What is shared decision making? www.informedmedicaldecisions.org/what-is-shared-decision-making (accessed March 18, 2015).
IOM (Institute of Medicine). 2001. Crossing the quality chasm: A new health system for the 21st century. Washington, DC: National Academy Press.
IOM. 2003a. Health professions education: A bridge to quality. Washington, DC: The National Academies Press.
IOM. 2003b. Unequal treatment: Confronting racial and ethnic disparties in health care. Washington, DC: The National Academies Press.
IOM. 2004. Health literacy: A prescription to end confusion. Washington, DC: The National Academies Press.
IOM. 2008. Retooling for an aging America: Building the health care workforce. Washington, DC: The National Academies Press.
IOM. 2010. Redesigning continuing education in the health professions. Washington, DC: The National Academies Press.
IOM. 2011a. The future of nursing: Leading change, advancing health. Washington, DC: The National Academies Press.
IOM. 2011b. The health of lesbian, gay, bisexual, and transgender people: Building a foundation for better understanding. Washington, DC: The National Academies Press.
IOM. 2011c. Relieving pain in America: A blueprint for transforming prevention, care, education, and research. Washington, DC: The National Academies Press.
IOM. 2012a. 10 attributes of a health literate organization: Discussion paper. Washington, DC: Institute of Medicine
IOM. 2012b. Communicating with patients on health care evidence: Discussion paper. Washington, DC: Institute of Medicine.
IOM. 2012c. Core principles and values of effective team-based health care: Discussion paper. Washington, DC: Institute of Medicine.
IOM. 2012d. Health IT and patient safety: Building safer systems for better care. Washington, DC: The National Academies Press.
IOM. 2012e. The mental health and substance use workforce for older adults: In whose hands? Washington, DC: The National Academies Press.
IOM. 2013a. Best care at lower cost: The path to continuously learning health care in America. Washington, DC: The National Academies Press.
IOM. 2013b. Delivering high-quality cancer care: Charting a new course for a system in crisis. Washington, DC: The National Academies Press.
IOM. 2014. Graduate medical education that meets the nation’s health needs. Washington, DC: The National Academies Press.
IOM. 2015. Measuring the impact of interprofessional education on collaborative practice and patient outcomes. Washington, DC: The National Academies Press.
Jarvis-Selinger, S., D. D. Pratt, and G. Regehr. 2012. Competency is not enough: Integrating identity formation into the medical education discourse. Academic Medicine 87(9):1185–1190.
The Joint Commission. 2007. “What did the doctor say?” Improving health literacy to protect patient safety. www.jointcommission.org/What_Did_the_Doctor_Say/default.aspx (accessed May 11, 2015).
The Joint Commission. 2014. Sentinel event data: Root causes by event type 2004-2q2014. www.jointcommission.org/Sentinel_Event_Statistics (accessed February 4, 2015).
The Joint Commission. 2015. Speak Up initiatives. www.jointcommission.org/speakup.aspx (accessed March 16, 2015).
Josiah Macy Jr. Foundation. 2011. Ensuring an effective physician workforce for the United States: Recommendations for graduate medical education to meet the needs of the public, the second of two conferences—The content and format of GME, chaired by Debra Weinstein, M.D. May, 2011, Atlanta, GA. New York: Josiah Macy Jr. Foundation.
Josiah Macy Jr. Foundation. 2014. Partnering with patients, families, and communities: An urgent imperative for health care, Conference recommendations. New York: Josiah Macy Jr. Foundation. www.macyfoundation.org/publications/publication/partnering-with-patients-families-and-communities-an-urgent-imperative-for (accessed June 5, 2015).
Josiah Macy Jr. Foundation and Carnegie Foundation for the Advancement of Teaching. 2010. Educating nurses and physicians: Towards new horizons. Advancing inter-professional education in academic health centers, Conference summary. New York: Josiah Macy Jr. Foundation. www.macyfoundation.org/docs/macy_pubs/JMF_Carnegie_Summary_WebVersion_%283%29.pdf (accessed June 5, 2015).
Julavits, H. 2014. Diagnose this! How to be your own best doctor. Harper’s April:25–35.
Kachalia, A., K. G. Shojania, T. P. Hofer, M. Piotrowski, and S. Saint. 2003. Does full disclosure of medical errors affect malpractice liability? The jury is still out. Joint Commission Journal on Quality and Patient Safety 29(10):503–511.
Kahneman, D. 2011. Thinking, fast and slow. New York: Farrar, Straus and Giroux.
Kaiser Permanente. 2012. Smart partners about your health, edited by K. Permanente. http://c.ymcdn.com/sites/www.npsf.org/resource/collection/930A0426-5BAC-4827-AF94-1CE1624CBE67/SMART-Partners-Guide1.pdf (accessed June 26, 2015).
Kak, N., B. Burkhalter, and M. Cooper. 2001. Measuring the competence of healthcare providers. Bethesda, MD: Published for USAID by the Center for Human Services, Quality Assurance Project.
Kanter, M. 2014. Diagnostic errors—Patient safety. Presentation to the committee on Diagnostic Error in Health Care, August 7, 2014, Washington, DC.
Kassirer, J. P. 1989. Our stubborn quest for diagnostic certainty. A cause of excessive testing. New England Journal of Medicine 320(22):1489–1491.
Keating, N. L., M. B. Landrum, E. B. Lamont, S. R. Bozeman, L. N. Shulman, and B. J. McNeil. 2012. Tumor boards and the quality of cancer care. Journal of the National Cancer Institute. doi: 10.1093/jnci/djs502. http://jnci.oxfordjournals.org/content/early/2012/12/24/jnci.djs502 (accessed June 5, 2015).
Kern, C. 2014. ACOs face barriers to implementing health IT. www.healthitoutcomes.com/doc/acos-face-barriers-to-implementing-health-it-0001 (accessed March 25, 2015).
Keroack, M. A., B. J. Youngberg, J. L. Cerese, C. Krsek, L. W. Prellwitz, and E. W. Trevelyan. 2007. Organizational factors associated with high performance in quality and safety in academic medical centers. Academic Medicine 82(12):1178–1186.
King, H. B., J. Battles, D. P. Baker, A. Alonso, E. Salas, J. Webster, L. Toomey, and M. Salisbury. 2008. TeamSTEPPS™: Team strategies and tools to enhance performance and patient safety. In K. Henriksen, J. B. Battles, M. A. Keyes, and M. L. Grady (eds.), Advances in patient safety: New directions and alternative approaches (Vol. 3: Performance and tools). AHRQ publication no. 00-0034-3. Rockville, MD: Agency for Healthcare Research and Quality. www.ahrq.gov/professionals/quality-patient-safety/patient-safety-resources/resources/advances-in-patient-safety-2/vol3/Advances-King_1.pdf (accessed June 5, 2015).
Klein, G. 1993. Sources of error in naturalistic decision making tasks. Proceedings of the Human Factors and Ergonomics Society, 37th Annual Meeting 368–371.
Klein, J. G. 2005. Five pitfalls in decisions about diagnosis and prescribing. BMJ 330(7494):781–783.
Kondo, K. L., and M. Swerdlow. 2013. Medical student radiology curriculum: What skills do residency program directors believe are essential for medical students to attain? Academic Radiology 20(3):263–271.
Kroenke, K. 2013. Diagnostic testing and the illusory reassurance of normal results: Comment on “Reassurance after diagnostic testing with a low pretest probability of serious disease.” JAMA Internal Medicine 173(6):416–417.
Kroft, S. H. 2014. Statement of Steven H. Kroft, American Society for Clinical Pathology (ASCP). Presentation to the Committee on Diagnostic Error in Health Care, April 28, 2014, Washington, DC.
Laposata, M., and A. Dighe. 2007. “Pre-pre” and “post-post” analytical error: High-incidence patient safety hazards involving the clinical laboratory. Clinical Chemistry and Laboratory Medicine 45(6):712–719.
LCME (Liaison Committee on Medical Education). 2015. Functions and structure of a medical school: Standards for accreditation of medical education programs leading to the M.D. Degree. Liaison Committee on Medical Education. www.lcme.org/publications.htm#standards-section (accessed July 24, 2015).
Leonard, M., S. Graham, and D. Bonacum. 2004. The human factor: The critical importance of effective teamwork and communication in providing safe care. Quality and Safety in Health Care 13(suppl 1):i85–i90.
Levinson, W., A. Kao, A. Kuby, and R. A. Thisted. 2005. Not all patients want to participate in decision making. Journal of General Internal Medicine 20(6):531–535.
Lie, D. A., E. Lee-Rey, A. Gomez, S. Bereknyei, and C. H. Braddock, 3rd. 2011. Does cultural competency training of health professionals improve patient outcomes? A systematic review and proposed algorithm for future research. Journal of General Internal Medicine 26(3):317–325.
Lipson, J. G., H. M. Weinstein, E. A. Gladstone, and R. H. Sarnoff. 2003. Bosnian and Soviet refugees’ experiences with health care. Western Journal of Nursing Research 25(7):854–871.
Longtin, Y., H. Sax, L. L. Leape, S. E. Sheridan, L. Donaldson, and D. Pittet. 2010. Patient participation: Current knowledge and applicability to patient safety. Mayo Clinic Proceedings 85(1):53–62.
Lucian Leape Institute. 2014. Safety is personal: Partnering with patients and families for the safest care. Report of the Roundtable on Consumer Engagement in Patient Safety. Boston, MA: National Patient Safety Foundation.
Lujan, H. L., and S. E. DiCarlo. 2006. First-year medical students prefer multiple learning styles. Advances in Physiological Education 30(1):13–16.
Lurie, S. J. 2012. History and practice of competency-based assessment. Medical Education 46(1):49–57.
Magid, M. S., and C. L. Cambor. 2011. The integration of pathology into the clinical years of undergraduate medical education: a survey and review of the literature. Human Pathology 43(4):567–576.
Malone, D. C., D. S. Hutchins, H. Haupert, P. Hansten, B. Duncan, R. C. Van Bergen, S. L. Solomon, and R. B. Lipton. 2005. Assessment of potential drug–drug interactions with a prescription claims database. American Journal of Health-System Pharmacy 62(19):1983–1991.
Manrai, A. K., G. Bhatia, J. Strymish, I. S. Kohane, and S. H. Jain. 2014. Medicine’s uncomfortable relationship with math: Calculating positive predictive value. JAMA Internal Medicine 174(6):991–993.
Marcus, E. 2003. Cases: When a patient is lost in the translation. The New York Times, April 8.
Marewski, J. N., and G. Gigerenzer. 2012. Heuristic decision making in medicine. Dialogues in Clinical Neuroscience 14(1):77–89.
Marvel, M. K., R. M. Epstein, K. Flowers, and H. B. Beckman. 1999. Soliciting the patient’s agenda: Have we improved? JAMA 281(3):283–287.
Mayer, R. E. 2010. Applying the science of learning to medical education. Medical Education 44(6):543–549.
Mayo Clinic. 2015. Patient care and health information. www.mayoclinic.org/patient-care-and-health-information (accessed March 26, 2015).
Mazor, K. M., D. W. Roblin, S. M. Greene, C. A. Lemay, C. L. Firneno, J. Calvi, C. D. Prouty, K. Horner, and T. H. Gallagher. 2012. Toward patient-centered cancer care: Patient perceptions of problematic events, impact, and response. Journal of Clinical Oncology 30(15):1784–1790.
Mazzocco, K., D. B. Petitti, K. T. Fong, D. Bonacum, J. Brookey, S. Graham, R. E. Lasky, J. B. Sexton, and E. J. Thomas. 2009. Surgical team behaviors and patient outcomes. American Journal of Surgery 197(5):678–685.
McDonald, K. M. 2014. The diagnostic field’s players and interactions: From the inside out. Diagnosis 1(1):55–58.
McDonald, K. M., C. L. Bryce, and M. L. Graber. 2013. The patient is in: Patient involvement strategies for diagnostic error mitigation. BMJ Quality and Safety 22(2):30–36.
McGaghie, W. C., S. B. Issenberg, E. R. Cohen, J. H. Barsuk, and D. B. Wayne. 2011. Does simulation-based medical education with deliberate practice yield better results than traditional clinical education? A meta-analytic comparative review of the evidence. Academic Medicine 86(6):706–711.
McGowan, J., M. Passiment, and H. M. Hoffman. 2007. Educating medical students as competent users of health information technologies: The MSOP data. Studies in Health Technologies and Informatics 129(Pt 2):1414–1418.
McLaughlin, J. E., M. T. Roth, D. M. Glatt, N. Gharkholonarehe, C. A. Davidson, L. M. Griffin, D. A. Esserman, and R. J. Mumper. 2014. The flipped classroom: A course redesign to foster learning and engagement in a health professions school. Academic Medicine 89(2):236–243.
MedPAC (Medicare Payment Advisory Commission). 2010. Shared decision making and its implications for Medicare. In MedPAC, Report to the Congress: Aligning incentives in medicine (pp. 191–210). Washington, DC: MedPAC. www.medpac.gov/documents/reports/Jun10_Ch07.pdf?sfvrsn=0 (accessed June 5, 2015).
Mello, M. M., R. C. Boothman, T. McDonald, J. Driver, A. Lembitz, D. Bouwmeester, B. Dunlap, and T. Gallagher. 2014. Communication-and-resolution programs: The challenges and lessons learned from six early adopters. Health Affairs 33(1):20–29.
Meyer, A. N. D., V. L. Payne, D. W. Meeks, R. Rao, and H. Singh. 2013. Physicians’ diagnostic accuracy, confidence, and resource requests: a vignette study. JAMA Internal Medicine 173(21):1952–1958.
Milan, F. B., L. Dyche, and J. Fletcher. 2011. “How am I doing?” Teaching medical students to elicit feedback during their clerkships. Medical Teacher 33(11):904–910.
Morcke, A., T. Dornan, and B. Eika. 2013. Outcome (competency) based education: An exploration of its origins, theoretical basis, and empirical evidence. Advances in Health Sciences Education 18(4):851–863.
Mulley, A. G., C. Trimble, and G. Elwyn. 2012. Stop the silent misdiagnosis: Patients’ preferences matter. BMJ 345(1).
Mumma, G., and W. Steven. 1995. Procedural debiasing of primary/anchoring effects in clinical-like judgments. Journal of Clinical Psychology 51(6):841–853.
Mussweiler, T., F. Strack, and T. Pfeiffer. 2000. Overcoming the inevitable anchoring effect: Considering the opposite compensates for selective accessibility. Personality and Social Psychology Bulletin 26(9):1142–1150.
Myers, L. 2013. Medical student perspective: Memory mountain: A more pleasurable route. www.acponline.org/medical_students/impact/archives/2013/07/perspect (accessed March 16, 2015).
Nasca, T. J., I. Philibert, T. Brigham, and T. C. Flynn. 2012. The next GME accreditation system—Rationale and benefits. New England Journal of Medicine 366(11):1051–1056.
National Commission on Physician Payment Reform. 2013. Report of the National Commission on Physician Payment Reform. Washington, DC: National Commission on Physician Payment Reform.
Naylor, M. D., K. D. Coburn, E. T. Kurtzman, H. Buck, J.Van Cleave, and C. Cott. 2010. Inter-professional team-based primary care for chronically ill adults: State of the science. Unpublished white paper presented at the ABIM Foundation Meeting to Advance Team-Based Care for the Chronically Ill in Ambulatory Settings, March 24–25, 2010, Philadelphia, PA.
NCI (National Cancer Institute). 2015. NCI dictionary of cancer terms: Tumor board review. www.cancer.gov/dictionary?cdrid=322893 (accessed March 16, 2015).
NCSBN (National Council of State Boards of Nursing). 2015. National Council of State Boards of Nursing. www.ncsbn.org/index.htm (accessed June 5, 2015).
Newman, E. A., A. B. Guest, M. A. Helvie, M. A. Roubidoux, A. E. Chang, C. G. Kleer, K. M. Diehl, V. M. Cimmino, L. Pierce, D. Hayes, L. A. Newman, and M. S. Sabel. 2006. Changes in surgical management resulting from case review at a breast cancer multidisciplinary tumor board. Cancer (107):2346–2351.
Newman-Toker, D. E., K. M. McDonald, and D. O. Meltzer. 2013. How much diagnostic safety can we afford, and how should we decide? A health economics perspective. BMJ Quality and Safety 22(Suppl 2):ii11–ii20.
NIST (National Institute of Standards and Technology), J. Redish, and S. Lowry. 2010. Usability in health IT: Technical strategy, research, and implementation. Rockville, MD: National Institute of Standards and Technology. Summary of Workshop and Usability in Health IT, Washington, DC, July 13.
NLM (National Library of Medicine). 2012a. Evaluating Internet health information: A tutorial from the National Library of Medicine. www.nlm.nih.gov/medlineplus/webeval/webeval.html (accessed March 16, 2015).
NLM. 2012b. MedlinePlus guide to healthy Web surfing. www.nlm.nih.gov/medlineplus/healthywebsurfing.html (accessed February 11, 2015).
NNLM (National Network of Libraries of Medicine). 2013. Prevalence of low health literacy. nnlm.gov/outreach/consumer/hlthlit.html#A3 (accessed April 4, 2014).
NORC. 2014. Demonstrating the effectiveness of patient feedback in improving the accuracy of medical records. Chicago, IL: NORC. www.healthit.gov/sites/default/files/20120831_odrfinalreport508.pdf (accessed June 5, 2015).
Norman, G. 2014. Diagnostic errors. Input submitted to the Committee on Diagnostic Error in Health Care, October 24, 2014, Washington, DC.
Nouri, S. S., and R. E. Rudd. 2015. Health literacy in the “oral exchange”: An important element of patient–provider communication. Patient Education and Counseling 98(5):565–571.
NPSF (National Patient Safety Foundation). 2015a. Ask me 3. www.npsf.org/?page=askme3 (accessed March 25, 2015).
NPSF. 2015b. RCA2: Improving root cause analyses and actions to prevent harm. http://c.ymcdn.com/sites/www.npsf.org/resource/resmgr/PDF/RCA2_first-online-pub_061615.pdf?hhSearchTerms=%22rca%22 (accessed July 6, 2015).
NPSF and SIDM (Society to Improve Diagnosis in Medicine). 2014. Checklist for getting the right diagnosis. www.npsf.org/?page=rightdiagnosis and http://c.ymcdn.com/sites/www.npsf.org/resource/collection/930A0426-5BAC-4827-AF94-1CE1624CBE67/Checklist-for-Getting-the-Right-Diagnosis.pdf (accessed June 26, 2015).
Nutter, D., and M. Whitcomb. 2001. The AAMC Project on the Clinical Education of Medical Students. Washington, DC: Association of American Medical Colleges.
OHSU (Oregon Health & Science University). 2014. A bold new curriculum aligns physician education with our health care future. School of Medicine, Oregon Health & Science University. www.ohsu.edu/xd/education/schools/school-of-medicine/about/curriculum-transformation/upload/SoM-Curriculum-transformation-interactive-12.pdf (accessed July 23, 2015).
O’Mahony, S., E. Mazur, P. Charney, Y. Wang, and J. Fine. 2007. Use of multidisciplinary rounds to simultaneously improve quality outcomes, enhance resident education, and shorten length of stay. Journal of General Internal Medicine 22(8):1073–1079.
O’Malley, A. S., G. R. Cohen, and J. M. Grossman. 2010. Electronic medical records and communication with patients and other clinicians: Are we talking less? Center for Studying Health System Change, Issue Brief No. 131:1–4. www.hschange.com/CONTENT/1125 (accessed June 5, 2015).
O’Neill, T. R., and J. C. Puffer. 2013. Maintenance of certification and its association with the clinical knowledge of family physicians. Academic Medicine 88(6):780–787.
OpenNotes. 2015. What is OpenNotes? www.myopennotes.org/about-opennotes (accessed January 2, 2015).
Paez, K., J. Allen, M. Beach, K. Carson, and L. Cooper. 2009. Physician cultural competence and patient ratings of the patient–physician relationship. Journal of General Internal Medicine 24(4):495–498.
Papa, F. J. 2014a. Learning sciences principles that can inform the construction of new approaches to diagnostic training. Diagnosis 1(1):125–129.
Papa, F. J. 2014b. A response to the IOM’s ad hoc Committee on Diagnostic Error in Health Care. Input submitted to the Committee on Diagnostic Error in Health Care, October 24, 2014, Washington, DC.
Papp, K. K., G. C. Huang, L. M. Lauzon Clabo, D. Delva, M. Fischer, L. Konopasek, R. M. Schwartzstein, and M. Gusic. 2014. Milestones of critical thinking: A developmental model for medicine and nursing. Academic Medicine 89(5):715–720.
Patel, V., N. A. Yoskowitz, and J. F. Arocha. 2009a. Towards effective evaluation and reform in medical education: A cognitive and learning sciences perspective. Advances in Health Sciences Education 14(5):791–812.
Patel, V., N. A. Yoskowitz, J. F. Arocha, and E. H. Shortliffe. 2009b. Cognitive and learning sciences in biomedical and health instructional design: A review with lessons for biomedical informatics education. Journal of Biomedical Informatics 42(1):176–197.
Pawlik, T. M., D. Laheru, R. H. Hruban, J. Coleman, C. L. Wolfgang, K. Campbell, S. Ali, E. K. Fishman, R. D. Schulick, J. M. Herman, and the Johns Hopkins Multidisciplinary Pancreas Clinic Team. 2008. Evaluating the impact of a single-day multidisciplinary clinic on the management of pancreatic cancer. Annals of Surgical Oncology 15(8):2081–2088.
Pecukonis, E., O. Doyle, and D. L. Bliss. 2008. Reducing barriers to interprofessional training: Promoting interprofessional cultural competence. Journal of Interprofessional Care 22(4):417–428.
Peters, E., J. Hibbard, P. Slovic, and N. Dieckmann. 2007. Numeracy skill and the communication, comprehension, and use of risk–benefit information. Health Affairs 26(3):741–748.
Pines, J. M. 2006. Profiles in patient safety: Confirmation bias in emergency medicine. Academic Emergency Medicine 13:90–94.
Porter, M. E. 2010. What is value in health care? New England Journal of Medicine 363(26):2477–2481.
Porter, M. E., and T. H. Lee. 2013. The strategy that will fix health care. Harvard Business Review 91(10):50–70.
Press, M. J. 2014. Instant replay—A quarterback’s view of care coordination. New England Journal of Medicine 371(6):489–491.
Prezzia, C., G. Vorona, and R. Greenspan. 2013. Fourth-year medical student opinions and basic knowledge regarding the field of radiology. Academic Radiology 20(3):272–283.
Price-Wise, G. 2008. Language, culture, and medical tragedy: The case of Willie Ramirez. http://healthaffairs.org/blog/2008/11/19/language-culture-and-medical-tragedy-the-case-of-willie-ramirez (accessed May 11, 2015).
Priyanath, A., J. Feinglass, N. C. Dolan, C. Haviley, and L. A. Venta. 2002. Patient satisfaction with the communication of mammographic results before and after the Mammography Quality Standards Reauthorization Act of 1998. American Journal of Roentgenology 178(2):451–456.
Puhl, R., and K. D. Brownell. 2001. Bias, discrimination, and obesity. Obesity Research 9(12):788–805.
Rao, V. M., and D. C. Levin. 2012. The overuse of diagnostic imaging and the Choosing Wisely Initiative. Annals of Internal Medicine 157(8):574–576.
Redelmeier, D. A. 2005. The cognitive psychology of missed diagnoses. Annals of Internal Medicine 142(2):115–120.
Rhoades, D. R., K. F. McFarland, W. H. Finch, and A. O. Johnson. 2001. Speaking and interruptions during primary care office visits. Family Medicine 33(7):528–532.
Richardson, W. S. 2007. We should overcome the barriers to evidence-based clinical diagnosis! Journal of Clinical Epidemiology 60(3):217–227.
Richardson, W. S. 2014. Twenty suggestions that could improve clinical diagnosis and reduce diagnostic error. Input submitted to the Committee on Diagnostic Error in Health Care, October 24, 2014, Washington, DC.
Rider, E. A., and C. H. Keefer. 2006. Communication skills competencies: Definitions and a teaching toolbox. Medical Education 40(7):624–629.
Rittenhouse, D. R., S. M. Shortell, and E. S. Fisher. 2009. Primary care and accountable care—Two essential elements of delivery-system reform. New England Journal of Medicine 361(24):2301–2303.
Roades, C. 2013. The new imperative of patient engagement for hospitals and health systems. Health Affairs Blog. http://healthaffairs.org/blog/2013/02/15/the-new-imperative-of-patient-engagement-for-hospitals-and-health-systems (accessed April 9, 2014).
Rolfe, I. E., and R. W. Sanson-Fisher. 2002. Translating learning principles into practice: A new strategy for learning clinical skills. Medical Education 36(4):345–352.
Ronda, G., J. Grispen, M. Ickenroth, G.–J. Dinant, N. De Vries, and T. Van der Weijden. 2014. The effects of a Web-based decision aid on the intention to diagnostic self-testing for cholesterol and diabetes: A randomized controlled trial. BMC Public Health 14(1):1–12.
Ross, J. S. 2014. Editor’s note: Ensuring correct interpretation of diagnostic test results. JAMA Internal Medicine 174(6):993.
Rubin, Z., and K. Blackham. 2015. The state of radiologic teaching practice in preclinical medical education: Survey of American medical, osteopathic, and podiatric schools. Journal of the American College of Radiology 12(4):403–408.
Ryan, C. 2013. Language use in the United States: 2011, American community survey reports. www.census.gov/prod/2013pubs/acs-22.pdf (accessed July 25, 2015).
Safran, D. G., M. Kosinski, A. R. Tarlov, W. H. Rogers, D. H. Taira, N. Lieberman, and J. E. Ware. 1998. The primary care assessment survey: Tests of data quality and measurement performance. Medical Care 36(5):728–739.
Salas, E., D. DiazGranados, S. J. Weaver, and H. King. 2008. Does team training work? Principles for health care. Academic Emergency Medicine 15(11):1002–1009.
Santoso, J. T., B. Schwertner, R. L. Coleman, and E. V. Hannigan. 2004. Tumor board in gynecologic oncology. International Journal of Gynecological Cancer 14(2):206–209.
Sarkar, U., D. Bonacum, W. Strull, C. Spitzmueller, N. Jin, A. Lopez, T. D. Giardina, A. N. Meyer, and H. Singh. 2012. Challenges of making a diagnosis in the outpatient setting: A multi-site survey of primary care physicians. BMJ Quality and Safety 21(8):641–648.
Sarkar, U., B. Simchowitz, D. Bonacum, W. Strull, A. Lopez, L. Rotteau, and K. Shojania. 2014. A qualitative analysis of physician perspectives on missed and delayed outpatient diagnosis: The focus on system-related factors. Joint Commission Journal on Quality and Patient Safety 40(10):461–470.
Sawyer, R. K. (ed.). 2006. The Cambridge handbook of the learning sciences. New York: Cambridge University Press.
Sawyer, R. K. 2008. Optimising learning: Implications of learning sciences research. Paris: OECD. www.oecd.org/edu/ceri/40805146.pdf (accessed June 5, 2015).
Say, R., M. Murtagh, and R. Thomson. 2006. Patients’ preference for involvement in medical decision making: A narrative review. Patient Education and Counseling 60(2):102–114.
SCAI (Society for Cardiovascular Angiography and Interventions). 2014. SCAI expands auc calculator app to support clinical decision making for diagnostic catheterization and imaging for heart failure: Society for Cardiovascular Angiography and Interventions. www.scai.org/Press/detail.aspx?cid=edaf8ad9-4d7a-4147-ac4f-4d62585b7f56#.VY2FbLHD9zN (accessed June 25, 2015).
Scalese, R., V. Obeso, and S. B. Issenberg. 2008. Simulation technology for skills training and competency assessment in medical education. Journal of General Internal Medicine 23(Suppl 1):46–49.
Schiff, G. D. 2008. Minimizing diagnostic error: The importance of follow-up and feedback. American Journal of Medicine 121(5):S38–S42.
Schiff. G. D. 2014a. Presentation to IOM Committee on Diagnostic Error in Health Care, August 7, 2014, Washington, DC.
Schiff, G. D. 2014b. Diagnosis and diagnostic errors: Time for a new paradigm. BMJ Quality and Safety 23(1):1–3.
Schiff, G. D., O. Hasan, S. Kim, R. Abrams, K. Cosby, B. L. Lambert, A. S. Elstein, S. Hasler, M. L. Kabongo, N. Krosnjar, R. Odwazny, M. F. Wisniewski, and R. A. McNutt. 2009. Diagnostic error in medicine: Analysis of 583 physician-reported errors. Archives of Internal Medicine 169(20):1881–1887.
Schiff, G., P. Griswold, B. R. Ellis, A. L. Puopolo, N. Brede, H. R. Nieva, F. Federico, N. Leydon, J. Ling, D. Wachenheim, L. L. Leape, and M. Biondolillo. 2014. Doing right by our patients when things go wrong in the ambulatory setting. Joint Commission Journal on Quality and Patient Safety/Joint Commission Resources 40(2):91–96.
Schillinger, D., J. Piette, K. Grumbach, F. Wang, C. Wilson, C. Daher, K. Leong-Grotz, C. Castro, and A. B. Bindman. 2003. Closing the loop: Physician communication with diabetic patients who have low health literacy. Archives of Internal Medicine 163(1):83–90.
Schmitt, M., A. Blue, C. A. Aschenbrener, and T. R. Viggiano. 2011. Core competencies for interprofessional collaborative practice: Reforming health care by transforming health professionals’ education. Academic Medicine 86(11):1351.
Schoen, C., R. Osborn, M. M. Doty, M. Bishop, J. Peugh, and N. Murukutla. 2007. Toward higher-performance health systems: Adults’ health care experiences in seven countries, 2007. Health Affairs 26(6):w717–w734.
Schulman, K. A., J. A. Berlin, W. Harless, J. F. Kerner, S. Sistrunk, B. J. Gersh, R. Dubé, C. K. Taleghani, J. E. Burke, S. Williams, J. M. Eisenberg, W. Ayers, and J. J. Escarce. 1999. The effect of race and sex on physicians’ recommendations for cardiac catheterization. New England Journal of Medicine 340(8):618–626.
Schwartz, M. B., H. O’Neal Chambliss, K. D. Brownell, S. N. Blair, and C. Billington. 2003. Weight bias among health professionals specializing in obesity. Obesity Research 11(9):1033–1039.
Seegmiller, A. C., A. S. Kim, C. A. Mosse, M. A. Levy, M. A. Thompson, M. K. Kressin, M. H. Jagasia, S. A. Strickland, N. M. Reddy, E. R. Marx, K. J. Sinkfield, H. N. Pollard, W. D. Plummer, W. D. Dupont, E. K. Shultz, R. S. Dittus, W. W. Stead, S. A. Santoro, and M. M. Zutter. 2013. Optimizing personalized bone marrow testing using an evidence-based, interdisciplinary team approach. American Journal of Clinical Pathology 140(5):643–650.
Semigran, H. L., J. A. Linder, C. Gidengil, and A. Mehrotra. 2015. Evaluation of symptom checkers for self diagnosis and triage: Audit study. BMJ 351:h3480.
Sequist, T., E. Schneider, M. Anastario, E. Odigie, R. Marshall, W. Rogers, and D. Safran. 2008. Quality monitoring of physicians: Linking patients’ experiences of care to clinical quality and outcomes. Journal of General Internal Medicine 23(11):1784–1790.
Shojania, K. G., I. Silver, and W. Levinson. 2012. Continuing medical education and quality improvement: A match made in heaven? Annals of Internal Medicine 156(4):305–308.
Shumate, M., R. Ibrahim, and R. Levitt. 2010. Dynamic information retrieval and allocation flows in project teams with discontinuous membership. European Journal of International Management 4(6):556–575.
SIDM (Society to Improve Diagnosis in Medicine). 2015. Patient Toolkit. www.improvediagnosis.org/?page=PatientToolkit (accessed August 27, 2015).
SIDM and NPSF (National Patient Safety Foundation). 2014. Reducing diagnostic error: Nurses and clinical staff: Ten things I could do tomorrow. http://c.ymcdn.com/sites/www. npsf.org/resource/collection/0716DBAD-99BB-460E-9837-1E357423C51C/Reducing-Diagnostic-Error-Nurses-and-Clinical-Staff-Ten-Things-I-Could-Do-Tomorrow.pdf (accessed May 11, 2015).
Singh, H. 2014. Building a robust conceptual foundation for defining and measuring diagnostic errors. Presentation to the Committee on Diagnostic Error in Health Care, August 7, 2014, Washington, DC.
Smith, B. R., M. Aguero-Rosenfeld, J. Anastasi, B. Baron, A. Berg, J. L. Bock, S. Campbell, K. P. Crookston, R. Fitzgerald, M. Fung, R. Haspel, J. G. Howe, J. Jhang, M. Kamoun, S. Koethe, M. D. Krasowski, M. L. Landry, M. B. Marques, H. M. Rinder, W. Roberts, W. E. Schreiber, S. L. Spitalnik, C. A. Tormey, P. Wolf, and Y. Y. Wu. 2010. Educating medical students in laboratory medicine: A proposed curriculum. American Journal of Clinical Pathology 133(4):533–542.
Smith, T. J., and D. L. Longo. 2012. Talking with patients about dying. New England Journal of Medicine 367(17):1651.
Soni, K., and G. Dhaliwal. 2012. Misleading complaint: Commentary by Krishan Soni, M.D., M.B.A., and Gurpreet Dhaliwal, M.D. http://webmm.ahrq.gov/case.aspx?caseID=273 (accessed June 5, 2015).
Sorbero, M. E., D. O. Farley, S. Mattke, and S. L. Lovejoy. 2008. Outcome measures for effective teamwork in inpatient care: Final report. Santa Monica, CA: RAND Corporation.
Spain, E. 2014. Do doctors spend too much time looking at computer screen? Gazing at electronic health records diverts doctors’ attention from patients. Northwestern University, January 23. www.northwestern.edu/newscenter/stories/2014/01/do-doctors-spend-too-much-time-looking-at-computer-screen.html (accessed June 5, 2015).
Starfield, B. 2000. Is U.S. health really the best in the world? JAMA 284(4):483–485.
Stark, M., and J. J. Fins. 2014. The ethical imperative to think about thinking: Diagnostics, metacognition, and medical professionalism. Cambridge Quarterly of Healthcare Ethics 23(4):386–396.
Stevenson, F. A. 2003. General practitioners’ views on shared decision making: A qualitative analysis. Patient Education and Counseling 50(3):291–293.
Straus, C. M., E. M. Webb, K. L. Kondo, A. W. Phillips, D. M. Naeger, C. W. Carrico, W. Herring, J. A. Neutze, G. R. Haines, and G. D. Dodd, 3rd. 2014. Medical student radiology education: Summary and recommendations from a national survey of medical school and radiology department leadership. Journal of the American College of Radiology 11(6):606–610.
Stremikis, K., C. Schoen, and A. K. Fryer. 2011. A call for change: The 2011 Commonwealth Fund survey of public views of the U.S. health system. Commonwealth Fund issue brief. www.commonwealthfund.org/~/media/Files/Publications/Issue%20Brief/2011/Apr/1492_Stremikis_public_views_2011_survey_ib.pdf (accessed June 5, 2015).
Su, E., T. A. Schmidt, N. C. Mann, and A. D. Zechnich. 2000. A randomized controlled trial to assess decay in acquired knowledge among paramedics completing a pediatric resuscitation course. Academic Emergency Medicine 7(7):779–786.
Sutcliffe, K. M., E. Lewton, and M. M. Rosenthal. 2004. Communication failures: An insidious contributor to medical mishaps. Academic Medicine 79(2):186–194.
Swain, M., and V. Patel. 2014. Patient access to test results among clinical laboratories. ONC Data Brief No. 13:1-9. Washington, DC: Office of the National Coordinator for Health Information Technology. www.healthit.gov/sites/default/files/onc-data-brief-13-labsurveydatabrief.pdf (accessed June 5, 2015).
Talbert, M. L., E. R. Ashwood, N. A. Brownlee, J. R. Clark, R. E. Horowitz, R. B. Lepoff, A. Neumann, C. N. Otis, S. Z. Powell, and T. M. Sodeman. 2009. Resident preparation for practice: a white paper from the College of American Pathologists and Association of Pathology Chairs. Archives of Pathology & Laboratory Medicine 133(7):1139–1147.
Taylor, C. R., B. R. DeYoung, and M. B. Cohen. 2008. Pathology education: quo vadis?. Human Pathology 39(11):1555–1561.
Teherani, A., D. M. Irby, and H. Loeser. 2013. Outcomes of different clerkship models: Longitudinal integrated, hybrid, and block. Academic Medicine 88(1):35–43.
Teirstein, P. S. 2015. Boarded to death—Why maintenance of certification is bad for doctors and patients. New England Journal of Medicine 372(2):106–108.
ten Cate, O. 2014. Advice to the Institute of Medicine Committee on Diagnostic Error. Input submitted to the Committee on Diagnostic Error in Health Care, November 25, 2014, Washington, DC.
Thibault, G. E. 2013. Reforming health professions education will require culture change and closer ties between classroom and practice. Health Affairs 32(11):1928–1932.
Torre, D. M., B. J. Daley, J. L. Sebastian, and D. M. Elnicki. 2006. Overview of current learning theories for medical educators. American Journal of Medicine 119(10):903–907.
Trowbridge, R. 2014. Diagnostic performance: Measurement and feedback. Presentation to the Committee on Diagnostic Error in Health Care, August 7, 2014, Washington, DC.
Trowbridge, R., G. Dhaliwal, and K. Cosby. 2013. Educational agenda for diagnostic error reduction. BMJ Quality and Safety 22(Suppl 2):ii28–ii32.
University of Pittsburgh. 2015. Institute for Doctor–Patient Communication. www.dom.pitt.edu/dgim/IDPC/about.html (accessed March 26, 2015).
Vashdi, D. R., P. A. Bamberger, and M. Erez. 2013. Can surgical teams ever learn? The role of coordination, complexity, and transitivity in action team learning. Academy of Management Journal 56(4):945–971.
Walker, J., J. D. Darer, J. G. Elmore, and T. Delbanco. 2014. The road toward fully transparent medical records. New England Journal of Medicine 370(1):6–8.
Weaver, S. J., S. M. Dy, and M. A. Rosen. 2014. Team-training in healthcare: A narrative synthesis of the literature. BMJ Quality and Safety 23(5):359–372.
Weed, L. L., and L. Weed. 2014. Diagnosing diagnostic failure. Diagnosis 1(1):13–17.
Wegwarth, O., W. Gaissmaier, and G. Gigerenzer. 2009. Smart strategies for doctors and doctors-in-training: Heuristics in medicine. Medical Education 43(8):721–728.
Weingart, S. N. 2013. Patient engagement and patient safety. Agency for Healthcare Quality and Research. http://webmm.ahrq.gov/perspective.aspx?perspectiveID=136 (accessed February 7, 2014).
Weingart, S. N., O. Pagovich, D. Z. Sands, J. M. Li, M. D. Aronson, R. B. Davis, D. W. Bates, and R. S. Phillips. 2005. What can hospitalized patients tell us about adverse events? Learning from patient-reported incidents. Journal of General Internal Medicine 20(9):830–836.
WHO (World Health Organization). 2010. Framework for action on interprofessional education and collaborative practice. Geneva: World Health Organization.
Wilson, M. L. 2010. Educating medical students in laboratory medicine. American Journal of Clinical Pathology 133(4):525–528.
Wilson-Stronks, A., and E. Galvez. 2007. Hospitals, language, and culture: A snapshot of the nation, exploring cultural and linguistic services in the nation’s hospitals. The Joint Commission. www.jointcommission.org/assets/1/6/hlc_paper.pdf (accessed June 5, 2015).
Xyrichis, A., and E. Ream. 2008. Teamwork: A concept analysis. Journal of Advanced Nursing 61(2):232–241.
Yang, H., C. Thompson, and M. Bland. 2012. The effect of clinical experience, judgment task difficulty and time pressure on nurses’ confidence calibration in a high fidelity clinical simulation. BMC Medical Informatics and Decision Making 12(1):113.
Yedidia, M. J., C. C. Gillespie, E. Kachur, M. D. Schwartz, J. Ockene, A. E. Chepaitis, C. W. Snyder, A. Lazare, and M. Lipkin, Jr. 2003. Effect of communications training on medical student performance. JAMA 290(9):1157–1165.
Zhi, M., E. L. Ding, J. Theisen-Toupal, J. Whelan, and R. Arnaout. 2013. The landscape of inappropriate laboratory testing: A 15-year meta-analysis. PLoS ONE 8(11):e78962.
Zimmerman, T. M., and G. Amori. 2007. Including patients in root cause and system failure analysis: Legal and psychological implications. Journal of Healthcare Risk Management 27(2):27–34.








































































