
The workshop featured two keynote addresses that laid out the broad challenges and opportunities for improving the behavioral health of young people created by passage of the ACA. The first presented some of the troubling measures of behavioral health issues in the United States and provided a framework for fundamental changes in the health care system that could ameliorate these problems. The second keynote presentation described some of the ongoing institutional, economic, and cultural shifts that are contributing to and could accelerate change in the health care system.
AN EPIDEMIC OF MENTAL, BEHAVIORAL, AND DEVELOPMENTAL PROBLEMS
Mental, behavioral, and developmental problems are at epidemic levels among children in the United States (Perou et al., 2013), observed Neal Halfon, director of the University of California, Los Angeles (UCLA), Center for Healthier Children, Families, and Communities and professor at UCLA’s David Geffen School of Medicine, the Fielding School of Public Health, and the School of Public Affairs, in his keynote address at the workshop. Nearly three-quarters of the cumulative prevalence of mental health problems, including substance abuse, anorexia nervosa, major depressive disorder, bipolar disorder, schizophrenia, and bulimia nervosa, have their onset before age 25 (see Figure 2-1). Among adolescents, 22 percent have mental health problems with impairment (Halfon et al., 2014c). The front-loaded attributable risk to society is “huge,” Halfon said.
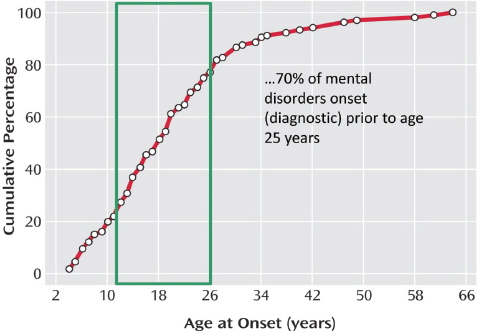
FIGURE 2-1 Mental disorder diagnosis by age.
SOURCE: Halfon, 2015. Data from Kessler et al., 2007.
Of the developed nations, the United States ranks among the lowest in terms of the material well-being, health, safety, and education of its children—with some of the highest levels of risky behaviors, and among the poorest housing and environmental conditions (UNICEF Office of Research, 2013). A growing number of children have multiple conditions, such as asthma, obesity, and attention deficit hyperactivity disorder (ADHD). Childhood disability nearly quadrupled in the 5 decades after 1960 (see Figure 2-2). In the 1960s, the poster child for disability was a girl with crutches who had polio, said Halfon. Today it is a boy with autism. “This steadily increasing trend in childhood disability is staring us right in the face, yet we are not doing much to change it.”
According to definitions established by the Maternal and Child Health Bureau, 4 to 6 percent of children have severe disabilities and 14 to 18 percent have special health care needs (Brault, 2012). But 30 to 40 percent have mental, behavioral, or learning problems or are at risk for such problems and require more typical pediatric care, said Halfon, because they will need additional screening, assessments, and evaluation. The remainder of children could be considered “good enough,” but even that designation is inadequate. “We actually want to know the percentage of children who
are thriving, yet at this point we only measure which children have some kind of problem.”
Halfon said that over the course of 1 year, one in five children and adolescents is seen as experiencing the signs and symptoms of a disorder listed in the Diagnostic and Statistical Manual of Mental Disorders, 4th edition (DSM-IV), with 15 to 22 percent seen as experiencing significant impairment (Halfon et al., 2014c; Merikangas et al., 2010). About 5 to 7 percent of young people—about 4 million altogether—experience extreme functional impairment. Yet in any given year, only about 20 percent of these are reported as receiving mental health services (NIH, 2007).
A developmental mismatch has emerged that is characterized by accelerated biological development, accelerated and unstable social development, unprotected and unsupported development for many adolescents, segregated development separate from parents and families, and technology- and market-dominated development, according to Halfon. The transition from childhood to adulthood has changed dramatically. It starts earlier and ends later, supportive scaffolding is lacking, and children’s emotional regulation and adaptation are suffering, Halfon noted. The potential for healthy development can be rapidly lost early in life, with factors such as adversity having dramatic effects on development. Adversity comes in many
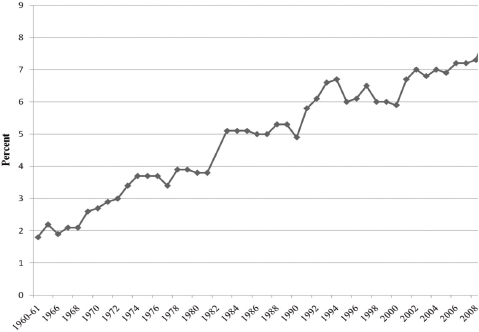
FIGURE 2-2 Childhood disability rate since 1960.
SOURCE: Halfon, 2015. Adapted from Halfon et al., 2012.
forms, including economic, social, environmental, familial, and behavioral adversity. About 45 percent of children have one adverse childhood experience, and 22 percent have two or more, with a steep social gradient in the distribution of such experiences (Bethell et al., 2014; Sacks et al., 2014). More than 40 percent of children live in low-income families, and more than 40 percent live in families with one parent, and such families are more likely than other families to have children who do not thrive. Rising rates of mental, behavioral, and developmental problems are a reflection of these growing levels of adversity, Halfon said.
Insufficient time, income, and services leave families with few resources for child rearing today, Halfon noted. Families are less stable, secure, and supported and have greater long-term uncertainty, both in terms of their own future and in terms of global affairs. Inequality has increased, with a steepening social gradient meaning that the ability to rise from one socioeconomic status level to the next is becoming harder (Kearney and Levine, 2015; Sawhill, 2015), which is “very frustrating and debilitating,” said Halfon. With dwindled supportive scaffolding and massive social changes under way—such as technology increasingly playing a role in the social development of children and adolescents—a growing mismatch has emerged between what is needed for healthy development and the complex modern context.
At the same time, the child health system is characterized by fragmented service delivery, difficulty accessing services, large inequities, low and uneven quality, models of care that are outmoded and do not match current needs, limited local responsibility, and enormous resource constraints, said Halfon. The overall result is a gap between current practice and the ideal child development trajectory. “It is an economic opportunity gap, . . . a human capital opportunity gap, a human potential opportunity gap, and this needs to be pushed onto the political agenda.”
“How do we take the health system and make it perform better?” asked Halfon. “I am going to argue that we need to change the operating system from one focused on diagnosing and treating chronic diseases to one focused on optimizing population health.” To do this we have to redirect health resources, said Halfon. Today, resources tend to flow to the end of life span, with a focus on biomedical issues (Halfon et al., 2014a). “We have a big challenge here,” he added.
Much can be done to improve the screening, diagnosis, and treatment of mental, behavioral, and developmental disorders in high-risk populations. Moving upstream and changing the median risk for children, rather
than just the marginal risk, is a fundamentally different way of approaching the problem.
However, the health care system is historically not well positioned to make this change. Health care historically has focused from the “neck down” rather than on what Halfon dubbed the “entals”—mental, developmental, and dental health. Strategies focused on only the marginal risk, which Halfon dubbed the “fix it” mentality, can be helpful, but real change will require more transformative changes. The ACA provides some tools for change, such as improved screening and bundled payments, but more fundamental changes are needed, he said (Halfon et al., 2014b). “We need a transformative analysis and approach.”
Halfon identified four kinds of change strategies. One is to fix the broken parts and pieces in a system, “and we have lots of broken parts in our health and health care system.” Another is to make incremental changes through evidence-based improvements in services and care, and most health care improvements fall into this category, such as new patient engagement and screening tools. A third strategy is to transition to a new way of doing things through innovations that drive improvements. This requires bigger changes, nudges, and jolts that make the system perform in a new and different way. And the fourth strategy is to undergo a transformation through a paradigm shift. This requires a change in the operating system, noted Halfon.
The ACA is stimulating turbulent disruptions and creating the potential for substantial system improvement and innovation, Halfon observed. It has created a rush to develop accountable care organizations (ACOs), unleash market forces, and bring about significant delivery system changes. It also has created growing pressure for different types of payment reform.
The act has had many positive outcomes for children, including expansion of parent health insurance, no lifetime caps, no discrimination based on preexisting condition, better access to preventive care, and bundled payments. However, the act also has produced negatives. The regionalization of care has been breaking down as the market takes over health care, said Halfon. Children’s health services have been squeezed, with many community health centers taking care of more “dual eligibles” who qualify for both Medicare and Medicaid. Children’s hospitals are facing challenges, and children’s benefit packages typically are inadequate. Children represent such a small proportion of overall health care expenditures that they tend not to receive sufficient attention (Cheng et al., 2014a,b). Investments in children produce benefits over long time horizons, while competitive health markets are narrowly focused on short-term high-cost patients. Dealing with mental, behavioral, and developmental issues calls for cross-sector approaches, but such approaches are difficult to fund. “We have very simple business and payment models that are not aligned with producing value for
kids, families, or our society,” said Halfon. “There is a value equation that needs to be redefined in terms of what we are doing for kids.”
Halfon identified three distinct models of health care (Halfon et al., 2014b). In the first, which Halfon dubbed health care 1.0, medicine was based on acute care, infectious diseases, and the biomedical model. Gradually this model was modified to recognize the influence of social environments, behaviors, and other factors. This process converted a simple, mechanistic, and linear model to one that Halfon called the health care 2.0 model. It is complex, dynamic, and focused more on development, prevention, and treatment of chronic diseases from a biopsychosocial standpoint.
In recent decades, this model has again been transformed to health care 3.0 as a result of new scientific breakthroughs focused on epigenetics and the developmental origins of health and disease. For example, toxic stress can influence the midbrain in terms of attachment and the prefrontal cortex in terms of executive function, leading to health and behavioral problems (Hertzman, 2012). “The people who have disabilities with mental and behavioral issues in their twenties, thirties, and forties are the people who are going to have heart disease, diabetes, and chronic disease in their fifties and sixties” (Audrey, 1988; Felitti et al., 1998) As another example, children on welfare, by their third birthday, hear on average 30 million fewer words and have less than half the cumulative vocabulary of the children of college-educated parents (Hart and Risley, 1995). Socioeconomic status is even correlated with the amount of gray matter in children’s brains (Hanson et al., 2013).
Halfon referred to this new model as the life course health development synthesis (see Figure 2-3). “This is a new and different kind of model, and we need to be pushing this forward.” For public policy, this health care 3.0 model (Halfon et al., 2014b) demonstrates the need to reduce risk factors and increase protective factors to achieve a healthy developmental trajectory (see Figure 2-4). “People in health, education, family support, police officers—they all understand this,” Halfon said. “We have to make this brain drain that’s happening in the first 5 years of life be unacceptable in this country.”
Today, U.S. health care is only at about version 1.5 using this metaphor, Halfon said, and the ACA is designed to bring medicine up to only about version 2.0. “We have to have a broader vision,” he said. “We need to think about what the logic for a 3.0 system is, how we think about the development of health, and how we optimize health. There is a different logic model that we [need to] use if we are going to move in this direction.”
Breaking down the silos in the current system will require a system that
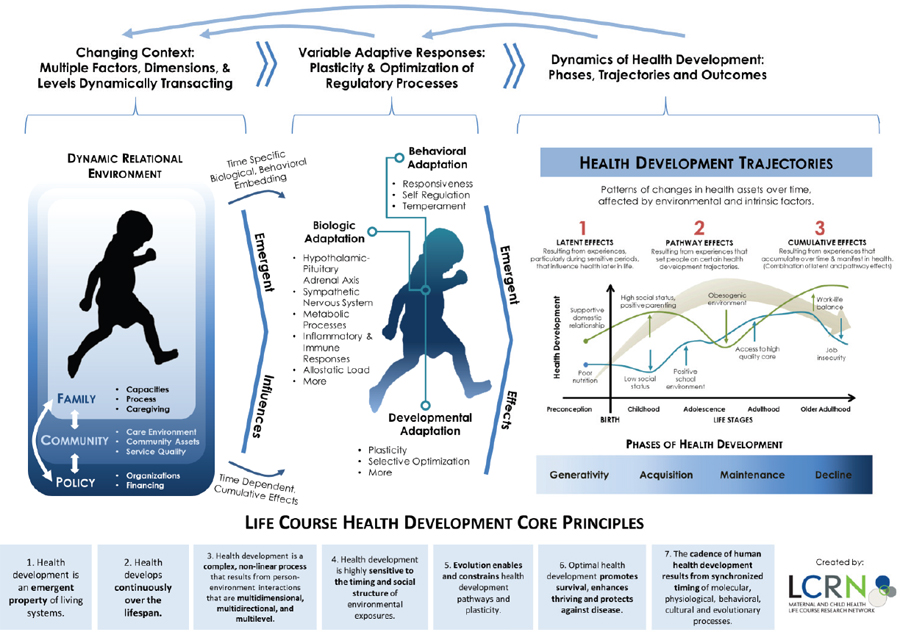
FIGURE 2-3 The life course health development synthesis. The perspective relates changing contexts and adaptive responses to the dynamics of health development.
SOURCE: Halfon, 2015. From Life Course Research Network (LCRN), 2014.
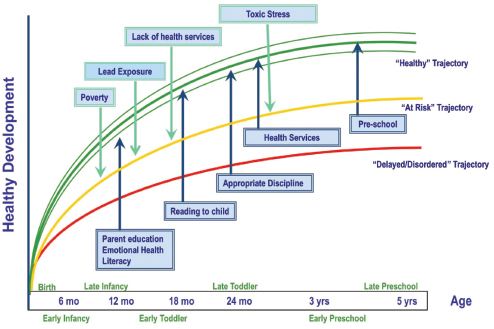
FIGURE 2-4 Risk and protective factors for healthy developmental trajectory.
SOURCE: Halfon, 2015. Adapted from Halfon et al., 2014a.
has been redesigned to be horizontally and vertically integrated, Halfon said. For example, a redesign to achieve a higher health trajectory might combine nurse–family partnerships, Early Head Start, child care resources and referrals, home-visiting networks, and parenting support. Such a system would require connecting pediatric offices to a much broader array of services and interventions. For example, instead of pediatric screens that result in 4 to 6 percent of children with disabilities being sent to the regional center, developmental health screens could be available in a variety of settings to identify the 30 to 40 percent of children who are at developmental risk. “The reason we cannot currently screen is there is no place to send them,” said Halfon. “We can come up with the best screening protocols in the world, but if there is no place to send them and we cannot send them anywhere, no one is going to do it.”
Measuring developmental trajectories is another major challenge that Halfon identified. The dawning era of big data creates many new possibilities. For example, measures of school readiness in Los Angeles are identifying the percentage of children who are vulnerable with respect to social competence and the percentage of mothers who are depressed, neighborhood by neighborhood. Such data can be used to fashion data dashboards, and local policy makers can use this information to assess policy priorities
and neighborhood needs in order to enact polices that reduce vulnerabilities in children and families.1
“We need to commit ourselves to a 2025 vision of transforming our children’s health system,” Halfon said. “We need to make the catastrophic and unnecessary loss of human potential be something that our politicians cannot run away from. We can’t be talking about incremental changes anymore. We need a child health development national network.”
Changing the political agenda will require audacity, he continued. The scale and scope of the problem argue for a major national effort, with a new narrative, leadership, measures, and approaches. Halfon said that people with whom he discusses this issue in the financial world are aware that underinvestments in children are not sustainable. “I think we can do it. I am more optimistic than pessimistic. But we have to have the vision and the leadership to do that, and we have to hold our politicians accountable.”
Halfon and a group of colleagues have proposed elevating the Maternal and Child Health Bureau to a much more prominent position and linking it to the Federal Reserve to move a child development agenda forward (Halfon et al., 2014c). “We need to get not just 10 communities but 1,000 communities over the next 10 years to transform their children’s health systems and make those kinds of innovations.” New apps for pediatric care, child health trusts, community-accountable child health development systems, and an early life course infrastructure are among the innovations that could help transform pediatric health care. A research agenda and new measurement and sensing systems could mate population health systems and clinical systems.
Halfon and his colleagues have been working on a Child Health System Transformation Initiative (CHSTI) that is designed to leverage the implementation of the ACA to transform the child health system and rapidly establish a systematic process for monitoring, analyzing, and responding to emerging threats and opportunities. The challenge is to move beyond incremental strategies and solutions and to treat the issue as a complex adaptive systems problem, one that requires the contributions of systems and implementation scientists, not just pediatricians and child psychiatrists and psychologists. Similarly, Halfon’s Transforming Early Childhood Community Systems (TECCS) initiative is seeking to bring together not just the health community and the early childhood community but police, housing, economic development, and others. “It’s about linking a whole-child,
______________
1Additional information can be found at: http://www.healthychild.ucla.edu/wp-content/uploads/2015/05/Pasadena-ECD-Policy.compressed.pdf (accessed July 31, 2015).
whole-family focus to a whole-city, whole-community approach.” These kind of community-wide collective impact strategies have been deployed to address the current obesity epidemic with some success, said Halfon, adding that similar types of cross-sector community-wide strategies will also work for improving the lives of young children. For example, when the development of children is mapped neighborhood by neighborhood and matched with housing data, people involved in the housing sector begin to understand that early childhood outcomes reflect the vitality of their neighborhood. Halfon also noted that when child development data are mapped against police data, law enforcement can see that the two are linked and begin to think more about how upstream policing may be an effective crime prevention strategy.
In response to an analogy drawn by a workshop participant between the current situation and early public health campaigns to provide clean water and sanitation to communities and households, Halfon pointed to four factors that were critical to the success of those early campaigns. One is that they had a solid scientific basis—the germ theory of disease and data showing that exposures to risk yield bad outcomes. Second, they had good measures, such as infant mortality and deaths that could quantify impacts. Third, universal approaches were taken that crossed racial, ethnic, and class lines. Fourth, they had local accountability. All four characteristics will continue to be important in child health development. “We need to be thinking about different strategies that are about all kids, not just about poor kids.”
Beyond any specific act of legislation or court case, a cultural change is going on, said Jeff Levi, executive director of the Trust for America’s Health, in the second keynote address of the workshop. The health system has begun to think beyond the immediate physical health needs of individuals. Prevention is increasingly—though not yet sufficiently—being recognized and supported. The social determinants of health have become part of the health discussion. The health system is talking less about the health of individuals or collection of individuals and more about the health of communities.
One measure of this change is the creation of new structures that acknowledge many contributions to health and allow the braiding and blending of resources and programs to meet the needs of individuals, despite the silos in which systems have worked in the past. For example, Levi chairs the Advisory Group on Prevention, Health Promotion, and Integrative and Public Health, which advises the National Prevention Council. This council includes 20 federal agencies and offices, including agencies like the Department of Defense, the Department of Housing and Urban Development, the
Department of Transportation, the Environmental Protection Agency, and the Department of Homeland Security. “All have different perspectives and different lenses on what contributes to health, but all [are] being told that prevention is now part of their job.”
Population health means many different things to many different people. To Levi, the concept implies that “no one can do it alone.” Thus, a health clinic cannot achieve its goals unless the activities of the clinic are linked to and address the conditions that occur outside the clinic. Reducing the big cost drivers in health, such as diabetes and heart disease, requires a safe, healthy, and supportive community environment, he said. This requires encompassing behavioral health issues as well as the traditional chronic physical conditions. It also requires moving beyond targeted interventions for those who are at greater risk to universal interventions that make the community healthier for everyone, Levi said.
Levi expressed the opinion that, given the importance of social determinants on health outcomes, both the public health and the health care system have to be re-envisioned to create a comprehensive approach to health. The public health system is organized much like the health care system—“disease by disease, silo by silo”—and rarely do we think across those silos and across communities and invest in creating healthier communities in a systematic way.” A number of levers in the ACA provide an opportunity to do this re-envisioning. Financial incentives are emphasizing outcomes over volume. Partnerships with a broader range of providers and broader range of services are taking shape. New systems of care delivery are creating a range of opportunities. However, these structural changes are happening faster than the payment changes. Experiments are not necessarily being sustained over time, with the result that incentives for long-term change are not in place.
Large-scale change requires figuring out the financial incentives, Levi observed. One question is whether a shift from volume to value is sufficient, because perceptions of value differ. The timeframe over which value occurs for children is longer than for adults, but shareholders want to see short-term returns on their investments. Another question involves whether a decrease of illness or an increase of well-being, including mental health, is valued? And if it is the latter, how can an increased sense of well-being be ascribed a financial value? Finally, do the providers of health include only licensed professionals or members of the community who can influence health?
PREVENTION IN THE AFFORDABLE CARE ACT
Some of the less visible levers in the ACA center on prevention, Levi noted. For example, the Prevention and Public Health Fund is a billion
dollar mandatory funding stream that is available every year to support prevention and public health programs, including community-based prevention programs. This fund and other resources have let communities know that they now can access the resources to come together and build coalitions with multiple players, multiple constituencies, and multiple stakeholders.
The new community benefit requirements for nonprofit hospitals require that they give back to their communities in other ways, now that more people are insured. In addition, a new vision of the workforce, including community health workers, is part of the ACA.
A report from the National Prevention Council, cleared by all the members of the council, laid out a very expansive vision for the goals, strategic directions, and priorities of a National Prevention Strategy, Levi noted. The strategy rests on four major goals: healthy and safe community environments, clinical and community preventive services, elimination of health disparities, and empowered people. Building on these directions, it lays out seven priorities: reproductive and sexual health, mental and emotional well-being, active living, healthy eating, preventing drug abuse and excessive alcohol use, tobacco-free living, and injury- and violence-free living.
Many potential advances in prevention require the formation of partnerships, Levi observed. Education and health constitute the easiest case to be made about the co-benefits of working together. For example, the advisory group that Levi chairs spawned a separate group called the National Collaborative on Education and Health, which has been looking at how schools and the health system can come together. One focus of the collaborative’s work has been the issue of chronic absenteeism. Children who miss more than 10 percent of school, especially in the early years, are less likely to graduate from high school. Early interventions to address such problems as chronic disease, lack of access to health or dental care, poor transportation, trauma, and no safe path to school can make a difference for these children. “From the perspective of the National Prevention Strategy, this is wonderful, because it brings in five or six federal agencies” that can work together to reduce the problem, he said. It is also a perfect example, he added, of how both health issues and the social determinants of health need to be addressed for children to perform better. “This is just one example of thinking differently about who needs to be at the table.”
Another example Levi described is the Section 1115 waiver that Hennepin County in Minnesota received to create a social ACO model that seamlessly integrates social services and health care services. “If you show up in the health care system and you have a problem with stable housing, you can get linked to the social services that the county provides. If you show up on the social services side and you have a health care need that needs to be addressed, you can get that referral, because the data systems and referral systems are well integrated.” An integrator organization
called Hennepin Health is bringing the county hospital, the county community health center, and the county-run social services agencies together and asking what else is missing. With a capitated rate from the Centers for Medicare & Medicaid Services (CMS), it can take expected savings and invest in new programs, such as an outpatient oral health clinic and a sobering center. “They’ve been able to capture savings, they’ve been able to reinvest, and they’ve been able to show that providing this broad range of services can be helpful both on the health side and on the social services side.” CMS is now interested in testing this approach in more complex political structures.
Finally, Levi mentioned the Truman Medical Center in Kansas City, which invited a bank to open a branch in the hospital so that low-wage employees would not have to use check-cashing services. The branch served not only the low-wage employees but also the neighborhood, which desperately needed banking services.
Successful experiments tend to have several common elements, said Levi. They have visionary leadership. They have some sort of integrator that can bring multiple funding streams to the table and braid if not blend them. They have a good data system across the system. And they have start-up funds. A big unknown, he acknowledged, is whether they have sustainable long-term financial models.
The stakeholders on this issue are numerous and diverse, Levi pointed out in response to a question. The United States has thousands of public health departments and several times that many school districts. Given that diversity, the best approach sometimes is simply to identify best practices and work with people at the local level to implement those practices. For example, the United Way can work with their chapters, whose priorities include education, health, and poverty, “so there is a perfect confluence there, and can this be replicated at the local level.”
He also pointed out, in response to another question, that particular communities are making great progress in integrating the actions of stakeholders. In these settings, innovations developed within sectors are being linked with other sectors to move forward. Financing structures are an important factor in this process, he said, because of the simultaneous difficulties and potential of cross-sector financing. “We need to be thinking about very different kinds of fiscal structures.” For example, if changes reduce costs, the savings should be available to sustain the interventions over time, but “it is not clear that we have figured that out.”
Many organizations are recognizing that health is a part of their core mission, said Levi, whether the Federal Reserve providing oversight of community reinvestment requirements, the Internal Revenue Service being more stringent around community benefit oversight for hospitals, or the Chamber of Commerce catalyzing community-based prevention efforts. This does not
reflect a health-in-all-policies approach, Levi said. “These people are coming to the table recognizing that to achieve their mission of improving, for example, the economic climate in a community, they have to think about health, and therefore they need to partner.”
Public health has always seen itself as fixing problems, Levi concluded. But in the future, public health will serve more as a chief health strategist for creating partnerships. This role will help it acquire the resources it needs to bring partners to the table. Public health can identify the problems, gather the data, and illuminate the choices to be made, “and then bring those coalitions together to make them happen.”
The conversation about prevention can become paralyzing if it calls for, first, eliminating poverty and racism, Levi acknowledged. But, as with the conversation around climate change, there are things people can do to help mitigate and adapt to a massive problem. “How these questions are going to be resolved is still up in the air, but there are a lot of resources, and a lot of exciting things are happening.”
Audrey, M. 1988. Psychiatric disorder in a sample of the general population with and without chronic medical conditions. American Journal of Psychiatry 145:976-998.
Bethell, C. D., P. Newacheck, E. Hawes, and N. Halfon. 2014. Adverse childhood experiences: assessing the impact on health and school engagement and the mitigating role of resilience. Health Affairs 33(12):2106-2115.
Brault, M. W. 2012. Americans with disabilities: 2010. Current Population Reports. U.S. Census Bureau.
Cheng, T. L., P. H. Wise, and N. Halfon. 2014a. Promise and perils of the Affordable Care Act for children. JAMA 311(17):1733-1734.
Cheng, T. L., P. H. Wise, and N. Halfon. 2014b. Quality health care for children and the Affordable Care Act: A voltage drop checklist. Pediatrics 134(4):794-802.
Felitti, V. J., R. F. Anda, D. Nordenberg, D. F. Williamson, A. M. Spitz, V. Edwards, M. P. Koss, and J. S. Marks. 1998. Relationship of childhood abuse and household dysfunction to many of the leading causes of death in adults: The Adverse Childhood Experiences (ACE) Study. American Journal of Preventive Medicine 14(4):245-258.
Halfon, N. 2015. Optimizing the Behavioral Health of All Children: Implications for Policy and Systems Change. Presented at IOM and NRC Workshop on Opportunities to Promote Children’s Behavioral Health: Health Care Reform and Beyond, Washington, DC.
Halfon, N., A. Houtrow, K. Larson, and P. W. Newarcheck. 2012. The changing landscape of disability in childhood. Future Child 22(1):13-42.
Halfon, N., K. Larson, M. Lu, E. Tullis, and S. Russ. 2014a. Lifecourse Health Development: Past, Present and Future. Maternal and Child Health Journal 18:344-365.
Halfon, N., P. Long, D. I. Chang, J. Hester, M. Inkelas, and A. Rodgers. 2014b. Applying a 3.0 transformation framework to guide large-scale health system reform. Health Affairs (Millwood) 33(11):2003-2011.
Halfon, N., P. H. Wise, and C. B. Forrest. 2014c. The changing nature of children’s health development: new challenges require major policy solutions. Health Affairs (Millwood) 33(12):2116-2124.
Hanson, J. L., N. Hair, D. G. Shen, F. Shi, J. H. Gilmore, B. L. Wolfe, and S. D. Pollak. 2013. Family poverty affects the rate of human infant brain growth. PLoS ONE 8(12):e80954.
Hart, B., and T. Risley. 1995. Meaningful differences in the everyday experience of young American children. Baltimore, MD: Paul H. Brookes Publishing.
Hertzman, C. 2012. Putting the concept of biological embedding in historical perspective. Proceedings of the National Academy of Sciences of the United States of America 109(Suppl 2):17160-17167.
Kearney, M. S., and P. B. Levine. 2015. Economic despair: The vicious circle of inequality and social mobility [Internet]. May 29, 2015. The Brookings Institution. http://www.brookings.edu/blogs/social-mobility-memos/posts/2015/05/29-despair-great-gatsby-curve-kearney-levine (accessed July 31, 2015).
Kessler, R. C., G. P. Amminger, S. Aguilar-Gaxiola, J. Alonso, S. Lee, and T. B. Ustun. 2007. Age of onset of mental disorders: A review of recent literature. Current Opinion in Psychiatry 20(4):359-364.
Life Course Research Network. 2014. “The Life Course Health Development Model.” Web. November 1, 2014. http://www.lcrn.net/life-course-health-development-diagram (accessed September 29, 2015).
Merikangas, K. R., H. Jian-ping, M. Burstein, S. A. Swanson, S. Avenevoli, L. Cui, C. Benjet, K. Georgiades, and J. Swendsen. 2010. Lifetime Prevalence of Mental Disorders in U.S. Adolescents: Results from the National Comorbidity Survey Replication-Adolescent Supplement (NCS-A). Journal of the American Academy of Child & Adolescent Psychiatry 49(10):980-989.
NIH (National Institutes of Health). 2007. Biological Sciences Curriculum Study. Information about Mental Illness and the Brain. NIH Curriculum Supplement Series [Internet]. Bethesda (MD): National Institutes of Health (US). http://www.ncbi.nlm.nih.gov/books/NBK20369 (accessed July 31, 2015).
Perou, R., R. H. Bitsko, S. J. Blumberg, P. Pastor, R. M. Ghandour, J. C. Gfroerer, S. L. Hedden, A. E. Crosby, S. N. Visser, L. A. Schieve, S. E. Parks, J. E. Hall, D. Brody, C. M. Simile, W. W. Thompson, J. Baio, S. Avenevoli, M. D. Kogan, and L. N. Huang. 2013. Mental Health Surveillance Among Children—United States, 2005–2011. Morbidity and Mortality Weekly Report 62(Suppl):1-35.
Sacks, V., P. Murphey, and K. Moore. 2014 (July). Adverse childhood experiences: National and state level prevalence. Child Trends Publication #2014-28.
Sawhill, I. V. 2015. Inequality and social mobility: Be afraid [Internet]. May 27, 2015. The Brookings Institution. http://www.brookings.edu/blogs/social-mobility-memos/posts/2015/05/27-inequality-great-gatsby-curve-sawhill (accessed July 31, 2015).
UNICEF Office of Research. 2013. Child well-being in rich countries: A comparative overview. Innocenti Report Card 11. Florence, Italy: UNICEF Office of Research.
This page intentionally left blank.
















