
6
Using Existing Platforms to Reach and Invest in Vulnerable Populations
Vulnerable populations are especially likely to have children and caregivers with needs that early childhood development services can help meet. The question then becomes how best to reach these populations and what kinds of services they need.
Three speakers at the workshop examined this question, first by looking at the advantages and disadvantages of targeted programs and then by discussing specific programs targeted at vulnerable populations.
TARGETED VERSUS UNIVERSAL PROGRAMS
Many studies and observations have shown that those most likely to benefit from early childhood programs are also the least likely to be participating in them, observed Nicholas Burnett, managing director at Results for Development. In addition, governments either cannot afford, or at least believe they cannot afford, early childhood development for everyone.
One way to get around these barriers is to target resources at the most vulnerable and disadvantaged, as opposed to making a program universally available. However, targeting is more or less politically acceptable in different places, Burnett said. Questions also surround how to include poor households and exclude nonpoor households. Successful targeting builds on robust data concerning households’ characteristics and on transparency and accountability throughout the targeting process. It
also requires local validation to include eligible households and resolve disputed cases.
The decision of whether to target a program at particular groups or make it universal requires making trade-offs between equity and efficiency, Burnett noted. The decision also can involve quality issues. Universal programs tend to be more structured, have more formally qualified teachers, provide more established hours, and offer other benefits, Burnett said—an overall finding that “surprised me.” However, universal programs may not be cost-effective, because the better-off portions of a community generally can afford to purchase their own services. Targeted programs tend to be looser than universal programs, though they also tend to have higher-quality interactions among the children and between the children and the caregivers.
Despite these differences, comparisons between targeted and universal programs generally show no significant differences in achievement by children, Burnett said, though this observation raises questions about how achievement is defined and measured.
Targeting can be done in many ways. The simplest is to use some criterion that already exists in a given context, such as geographic targeting, income targeting, or ethnic targeting. For early childhood development services, targeting may consist of putting money, or at least purchasing power, into the hands of poor families so they can access such services. Conditional cash transfers, family allowances, or voucher systems are all ways of doing this kind of targeting.
The other main type of targeting is actual delivery of services to children. This may take the form of in-kind transfers, bundled services delivered through centers or home-based services, or community-based interventions. As with money transfers, many ways exist of doing this that have been “reasonably successful in different contexts,” according to Burnett.
A major problem with targeting, he continued, is achieving a societal consensus that it should be done. Whether the data are available for targeting is another issue. Finally, inconsistent targeting within programs that are not integrated, so that vulnerable families receive some services but not others, can pose problems for the acceptability of targeting.
In the discussion period, Burnett recommended a systematic review of targeting to pull together the research that has been done on its benefits and disadvantages. He also urged that attention be given to low-data situations. “We can go around saying we need more data, fine. But we have to deal with the situations we are actually in.”
In addition, as one forum participant pointed out, a targeted program can be added on top of a universal program, to provide additional ser-
vices to those who need them most, and this approach would also be a valuable subject for additional research.
IMPLEMENTATION OF THE AUSTRALIAN NURSE–FAMILY PARTNERSHIP PROGRAM
An example of a targeted program is the Australian Nurse–Family Partnership Program. The parent program, which has been developed for more than 3 decades by David Olds at the University of Colorado on the basis of strong theoretical platforms and randomized controlled trials, consists of home visits by nurses over the course of 30 months (Stavrakos et al., 2009). The Australian program is targeted to women who are pregnant with an Aboriginal or islander child in the particular site where the program is being conducted, explained Claire Runciman, a consultant to the program. The program is run out of community-controlled Aboriginal health service organizations, which means that the program is run by organizations that are trusted by the community and have very strong links with the community. Guidelines for the visiting nurses outline what they are to do on those visits, with the nurses using their clinical judgment to adapt the guidelines to their clients’ unique situations. The nurses also collect data on program implementation data and demographic, health, risk factor, developmental, and life-course data relating to clients and their children during their visits, which has enabled strong program evaluations. To achieve a license to deliver the program, an organization needs to make a commitment to 18 elements developed for the program.
The three tiers of government in Australia have made rolling out the program difficult, Runciman explained, because of cost shifting that goes on among the levels of government. For example, the community-controlled health services are funded by the national government, but other health services are funded by state governments. As a result, the community-controlled health services may not have strong links to state-run programs, which may be required for some referrals. However, the program also can help these community-controlled health service organizations forge links with state-run programs.
Two key adaptations have been made to the program in the Australian context. First, the community-controlled organizations that were approached about investing in the program insisted that indigenous people be involved in the program. However, the program is a nurse-run program, and there are not many indigenous nurses in Australia. Involvement has been enhanced through the use of family partnership workers who introduce the nurses to clients and ensure that the relationship is strong.
Maintaining the integrity of the model while adapting to local cir-
cumstances is also a factor in scalability (Hill and Olds, 2013). Runciman emphasized that scaling up needs to be methodical, intentional, and iterative. “We need to keep going back and looking at it and working out what is working and what is not.” Scaling up also needs to be informed by data, though as Runciman acknowledged, there are never enough data, and the data that do exist need to be treated with caution.
Securing a trained workforce is a challenge with the program. Australia has not had a strong home-visiting program in the past, so many nurses in the program are relatively unfamiliar with the process. “They have to unlearn a lot of their skills and relearn relationship-based skills.” Nurses also undergo training in what Runciman called micro-communication skills, so they can avoid saying things that are culturally inappropriate to clients.
The funding of the program is based on both evidence and politics, Runciman observed. Australia has a bipartisan commitment to close the gap in maternal and child health indicators between indigenous and non-indigenous people. The level of commitment varies depending on which party is in power, but it nevertheless “provides a very strong foundation for the program’s survival,” said Runciman. One exciting development is that the community-controlled health service organizations are starting to work with their funders to argue for evidence-based programs. “The demand is coming from the bottom for evidence-based programs, and that is really exciting.”
An unexpected advantage of the program is that it has slowed down the implementation process. The need to comply with the requirements of the program has “been quite helpful for us in terms of negotiating with government demands or imperatives to achieve outcomes quickly,” Runciman said. Slowing down the process also creates time to innovate. With the Nurse–Family Partnership Program, innovation requires sending data to the international group, developing new tools, and incorporating new evidence into the program. “The program is always changing, dynamic, and moving forward,” Runciman concluded. “That is something that sometimes is not easy to sell to governments who want to buy a solution that will be the solution forever.”
A COMMUNITY-BASED HEALTH PROMOTION PROGRAM IN SRI LANKA
Kalana Peiris, public health advisor at Plan International, described a program targeted at 77 communities that have bordered areas of armed conflict in Sri Lanka. Traditional health indicators, including maternal mortality, infant mortality, facility delivery, skilled birth attendance, and immunization, tend to be better in Sri Lanka than in the rest of South Asia.
But these communities were subject to a variety of disruptions, including night-time displacements, sporadic terrorist attacks on civilians, and disruption of livelihoods. The intervention began about a year after the conflict in a setting where community cohesion and spirit had not fully recovered.
About 4,000 children under the age of 5 lived in these 77 communities. Interestingly, said Peiris, basic health services continued even during the conflict, so the traditional health indicators stayed high in these villages. But among the children, 64 percent of those between the ages of 2 and 5 were underweight, with boys and girls equally affected. Furthermore, the population of underweight children was dynamic because new children were constantly being added to the group that was undernourished.
In these villages, 70 percent of livelihoods were from day-wage labor in paddy fields, and 23 percent were from slash-and-burn agriculture. Men had an average education level of grade seven, and women of grade nine. Exclusive breastfeeding rates for the first 6 months were above 90 percent, but diets were undiversified, and maternal and child care practices were in general poor. However, health seeking was prompt and effective, and access to health care was good. Every village had a community midwife, and 90 percent of the communities were within 5 kilometers of a free government health care facility.
In this situation, what to do seemed obvious, said Peiris: educate about nutrition, promote exclusive breastfeeding, encourage parental stimulation, reduce stressful experiences, and so on. As Peiris said, “Education and supplementation were the panacea.”
But there was a glass wall that prevented education and improved knowledge from translating into action, he continued. For one thing, women were overburdened. They had an economic role, household work, and child care responsibilities. They were subject to domestic violence, limited recreation, malnutrition (both over and under), and poor mental well-being. Even though food security was not an issue, values, the media, myths, and misconceptions led to inappropriate food selection. Good and diverse foods were available, said Peiris, “but people were selling it to the shops and buying commercial products, which indicated a social value toward commercially available, processed, advertised food.” Men often controlled the finances of homes, and they spent a lot of money on alcohol and smoking. Due in part to the long period of conflict, parents lacked aspirations for their children and themselves.
No vaccine exists for these conditions, Peiris observed. The only solution was social transformation.
A change in household practices required change in unhealthy social norms, cultural practices, and gender norms, said Peiris. These were collective communities where others have a great influence on what hap-
pens in a given household. Community-led collective action for change therefore became the theory of change for the program.
Plan Sri Lanka, the Foundation for Health Promotion, and the Ministry of Health implemented a program to catalyze collective community action. The main objective was to improve the healthy growth and development of children under 5 years of age. The program was “entirely owned by the communities,” Peiris explained. “The action was not prescribed. They owned it. And these were not outside events. They were embedded in their daily routines.” For example, one approach was to work with community midwives to make them more skillful and give them more favorable attitudes toward enabling people to come up with actions to address their own problems.
Another major change is that many fathers became more involved in household work and child care. An innovation known as the Happiness Calendar helped them realize that they were happier when they were contributing to rather than detracting from their family’s security. They were more willing to ignore comments that contributing to their households was women’s work. That “self-realization . . . made them advocate with other fathers to get involved in such things, and also to stick to it.”
Because the activities promoted by the program were interesting, easy to do, and productive, they were contagious. Communities collectively monitored their own progress, and the process was treated as equally or more important than the result. As an example of these activities, Peiris cited the creation of baby corners for “feeding the five senses.” “Five families would start it, and when you go 1 month later you see the whole community is doing it. When you are walking on the road, you will see every household that has a child under 5 years has a play house dangling little things.”
Another solution was group play houses, which helped to alleviate the workload issue. Families and neighborhoods gathered to give their children a chance to play and eat together. “They soon realized that when the children are together, they eat more. Even the things that they never eat at home, they were eating.”
These and other simple interventions helped reduce the percentage of underweight children from 64 percent to 28 percent, Peiris said (see Figure 6-1).
Comparable reductions occurred in areas both more affected and less affected by the conflict. Dietary diversity increased, as did the amount of stimuli children received and the time parents spent with children. Low birthweight and underweight in preschoolers decreased substantially, and growth failure in the first 2 years went from 18 percent to virtually nothing.
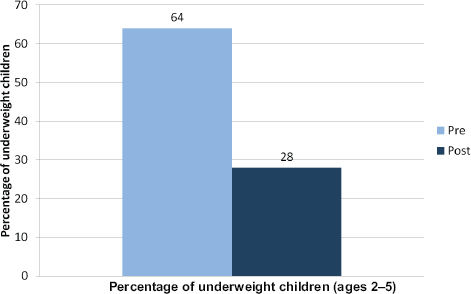
FIGURE 6-1 Early childhood interventions in communities affected by violence in Sri Lanka have substantially reduced the percentage of underweight children.
SOURCE: Plan Sri Lanka, 2013.
The program did face challenges, Peiris said. At first communities did not believe that they had the potential to transform their own environments, “so we had to do some convincing.” Replication was a challenge, because every community and household is different, which requires that the approach be customized for different places.
UNICEF and the government of Sri Lanka partnered with Plan Sri Lanka to expand the program into 9,000 communities, though the government has changed since the program was initiated. But more research is still needed, Peiris said, to determine the elements of success, which bottom-up approaches work best, and how to take “soft elements” into account, such as how communities can best be engaged.
This page intentionally left blank.








