
2
Communication: Palliative Care’s Transformational Procedure1
The workshop opened with an overview presentation by Diane Meier, Director of the Center to Advance Palliative Care (CAPC) and Vice-Chair for Public Policy, Professor of Geriatrics and Palliative Medicine, and the Catherine Gaisman Professor of Medical Ethics at the Icahn School of Medicine at Mount Sinai Hospital, who made the case for integrating palliative care principles and practices across the entire health care spectrum for anybody with a serious illness. Before addressing that topic, she noted that the real challenge in health literacy does not rest with patients and their families, as many discussions on the topic assume, but with the health system. “The obligation to be literate in what matters most to patients and families is ours. It is not their obligation to be literate about our culture.”
Health spending, she then said, is highly concentrated among the sickest patients (see Figure 2-1), which she said is appropriate. “Spending money on very sick people is not waste,” Meier emphasized. “How we spend that money is a different question, but conflating high spending with waste should stop.” Health care spending data show that 1 percent of patients, the sickest and most vulnerable, account for 25 percent of all spending, and 5 percent of patients account for 50 percent (Schoenman
__________________
1 This section is based on the presentation by Diane Meier, Director of the Center to Advance Palliative Care (CAPC) and Vice-Chair for Public Policy, Professor of Geriatrics and Palliative Medicine, and the Catherine Gaisman Professor of Medical Ethics at the Icahn School of Medicine at Mount Sinai Hospital. The statements are not endorsed or verified by the National Academies of Sciences, Engineering, and Medicine.
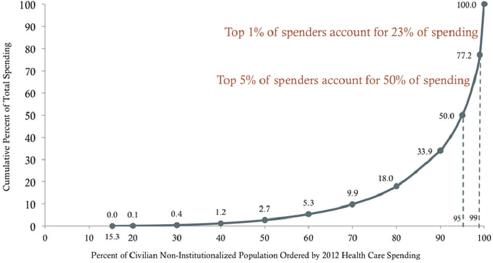
SOURCE: Schoenman and Chockley, 2012.
and Chockley, 2012). Given data showing the positive effect of palliative care on both the quality of care and the cost of care for the sickest patients (Meier, 2011), applying the principles and practices of palliative care more broadly is crucial to any effort to improve value in the U.S. health system, said Meier.
As an example of an illiterate health system, Meier recounted the story of Mr. B., an 88-year-old man with dementia who was admitted to the emergency department for management of back pain resulting from spinal stenosis and arthritis. Upon admission, his pain registered 8 on a scale of 10, and his 83-year-old wife reported he was taking 5 grams of acetaminophen daily for pain, a toxic dose. Mr. B. had been seen four times in the emergency department over the previous 3 months, and though Mr. B. pleaded not to be taken to the hospital again, Mrs. B. felt she had no choice but to call an ambulance given that her husband’s pain was terrible and that she could not move him herself, Meier recounted.
Meier became involved with Mr. and Mrs. B. when the attending physician in the emergency department called her and said he had a couple who were “abusing the emergency department for lower back pain” and wondered if she could see them even though the patient was not dying. Meier went down to the emergency department with her medical student and found Mr. B. in terrible pain and agitated from being brought to the emergency department—Mrs. B. had tried reaching Mr. B.’s doctor after hours and had gotten a voice recording saying “If this is a medical emer-
gency, hang up and call 911,” which is what she did. “Who is illiterate here?” said Meier. “She did exactly as she was told because it was a medical emergency. She could not move him, and there was nobody available to help her. Yet the perspective on our side is that this couple is abusing the emergency room.”
Before what she called her accidental and fortuitous involvement with Mr. B., he had been subjected to four ambulance rides to the emergency department, been hospitalized three times, developed a urinary tract infection from having been catheterized and became septic, and was declining functionally and cognitively simply from being hospitalized and suffering from complications. In addition, the family—primarily Mrs. B.—was in enormous distress, explained Meier. She noted that the attending physician had called Meier not because it was hospital policy, and not because of any intent to improve quality for patients like Mr. B. and his family, but because he had been a medical student at Mount Sinai years earlier and had spent a 1-week mandatory rotation in the palliative care service and happened to have been assigned to her. “Obviously, this should happen by design, not by accident,” said Meier.
After spending considerable time with Mr. and Mrs. B. assessing the situation, Meier decided to try ultra-low-dose morphine to see if that could address Mr. B.’s back pain and MiraLax for his constipation. Again, good fortune came into play because the pharmacy across the street from Mount Sinai carried the necessary formulation, an uncommon occurrence. While the student was fetching the prescription, Mr. B. had received a minute dose of morphine, which he tolerated well and enabled him to relax and even walk to the bathroom. Meier spent time teaching Mrs. B. how to administer the ultra-low-dose morphine and MiraLax, writing instructions in block capital letters and using teach back to ensure she understood the directions. Meier noted that it took three tries before her instructions were clear enough for her to become convinced that Mrs. B. knew what to do. She also phoned the director of Mount Sinai’s house calls program and arranged for a visit to the family’s home the next morning. What the visiting team found was a disaster waiting to happen, said Meier. There were loose throw rugs everywhere, electrical wires crisscrossing the floor, no grab bars in the bathroom, no elevated toilet seat, and the only thing in the refrigerator was leftover Chinese food. “Why was that?” asked Meier. “Mrs. B. could not go out to go grocery shopping because she could not leave Mr. B. alone. He would freak out and either try to follow her or fall in trying to follow her.” Lacking a computer, Mrs. B. could not order food from one of the delivery services operating in New York, but she did have a phone and called the Chinese restaurant next door.
With the family’s permission, Meier contacted the church where Mr. and Mrs. B. had gone before traveling became a problem. It turns out that
there was a new pastor at the church who had not known the couple and so did not realize they were no longer attending services, but who immediately connected them to the church’s friendly visitor program. Now, a member of the congregation or a high school student in a community service program spends a few hours with Mr. B. three times per week, enabling Mrs. B. to go shopping and spend time with her friends, which Meier said was probably the most important result of her involvement with this family. The palliative care service also organized Meals on Wheels for the family and contacted a daughter living in California, who now orders groceries online for her parents and visits them more often now that she knows what was happening back in New York. The end result is that 2 years later, Mr. B. is doing fine, and there have been no 911 calls, emergency department visits, and no hospitalizations since Meier’s initial involvement.
Mr. B.’s experience is not atypical, said Meier, who noted data showing that 75 percent of older Americans visit the emergency department at least once in the last 6 months of their lives because they do not see an alternative (Smith et al., 2012). These patients, she said, are typically not end-stage cancer patients, and most do not have a serious disease. Rather, she said, they are “condition driven.” Mr. B., for example, did not have heart failure, cancer, chronic obstructive pulmonary disease (COPD), or end-stage renal disease. He was simply frail, and impaired, both cognitively and functionally. “Being old plus caregiver exhaustion are driving his utilization,” said Meier.
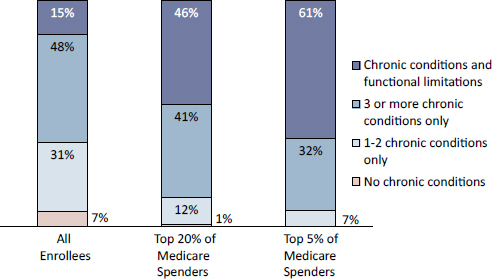
Health systems, she said, should be screening patients for palliative care using criteria that include functional limitation, frailty, dementia, exhausted and overwhelmed family caregivers, and social and behavioral health challenges, and she noted that data from the Medicare Current Beneficiary Survey support these criteria (see Figure 2-2). For example, 61 percent of the top 5 percent of spenders are functionally impaired, suggesting that functional status would be the single most important criteria for targeting high-risk patients, yet the most widely used electronic health records do not require documentation of functional status.
Dementia, she said, is another major predictor of risk for high levels of spending (see Table 2-1), largely, she added, because of caregiver exhaustion that results from a lack of social supports. She cited data (Bradley et al., 2011) showing that the United States has among the lowest ratios of social services to health services expenditures among countries in the Organisation for Economic Co-operation and Development (OECD) (see Figure 2-3). Belgium, Denmark, Germany, Italy, and Sweden, for example, spend about $2.70 on social supports for every dollar spent on medical care. In contrast, the United States spends 70 cents on social supports for every dollar spent on medical care. “Hence the dementia data,” said Meier. “Hospitals are a substitute for absent social supports.”
SOURCE: Presented by Diane Meier on July 9, 2015.
TABLE 2-1 Use of Health Services by Medicare and Medicaid Patients with and Without Dementia
| Dementia | No Dementia | |
| Medicare SNF use | 44.7% | 11.4% |
| Medicaid NH use | 21% | 1.4% |
| Hospital use | 76.2% | 51.2% |
| Home health use | 55.7% | 27.3% |
| Transitions | 11.2% | 3.8% |
NOTE: NH = nonhospital; SNF = skilled nursing facility.
SOURCE: Presented by Diane Meier on July 9, 2015.
When this country does experiment with a more rational allocation of funding that helps patients stay at home, quality does improve and spending falls, she noted. Based on reports from the 25 states that allow Medicaid to pay for home- and community-based long-term services and supports, rather than incentivizing them to go into a nursing home, patients who take advantage of that waiver cost the system one-third as much as those who choose nursing home care (Thomas, 2014). Similarly, increasing funds for Meals on Wheels programs by 1 percent nationally would keep an estimated 1,722 older adults with low-care needs out of nursing homes
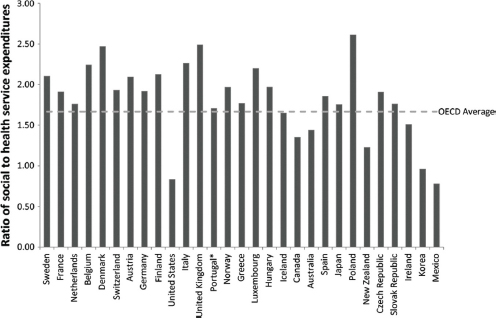
NOTE: OECD = Organisation for Economic Co-operation and Development.
* Expenditures for Portugal are from 2004, owing to missing data for 2005.
SOURCE: Bradley et al., 2011.
and save 26 states an estimated $109 million in reduced Medicaid spending, which would more than offset the cost of providing the meals (Thomas and Mor, 2013). Unfortunately, Meier added, funds for Meals on Wheels were cut in half during the federal budget sequester, and these funds have yet to be restored.
In explaining what palliative care is, Meier emphasized that the definition that Bernard Rosof gave in his introductory remarks does not mention prognosis, end-of-life care, death, or dying. Rather, it focuses on improving quality of life by addressing pain, symptoms, and the stress associated with serious illness. Mr. B., for example, was not dying and is doing well with the supports that were put in place. He would not, in fact, be eligible for hospice care, which is what many people associate with palliative care. “Is he benefiting from palliative care? Enormously,” said Meier. “If we stick to prognostic criteria, we are missing the boat.”
Palliative care is provided by an interdisciplinary team that works with patients, families, and other health care professionals to provide an added layer of support, Meier explained. It is appropriate at any age, for any diagnosis, and at any stage in a serious illness. It is important to make a
conceptual shift, she added, that moves away from thinking about palliative care as something that occurs when there is nothing more that can be done for a person to thinking about it as care delivered at the same time as treatment (see Figure 2-4).
Data show clearly that palliative care improves quality and by doing so reduces spending and does so, said Meier, not by rationing health care dollars or withholding necessary care but by heading off preventable crises and meeting people’s needs where they are, including nursing homes. As an example of palliative care in a nursing home setting, she recommended an article in The New Yorker (Mead, 2013) that described how an Arizona nursing home focuses care for dementia patients on what the residents say they need as opposed to doing so on strict schedules and regulatory requirements. To illustrate the power of palliative care in the home setting, she cited a randomized controlled trial from Kaiser Permanente in which patients with heart failure, COPD, or cancer were enrolled in either a home palliative care intervention or usual Medicare home care. Though the patients in the palliative care intervention received more home visits, they required fewer physician office visits, used the emergency department less, were hospitalized less, and spent fewer days in skilled nursing facilities (Brumley et al., 2007) (see Figure 2-5). Meier noted that Kaiser Permanente can measure and capture these cost savings because of the way its system is organized.
She then listed five key characteristics of effective palliative care:
- It targets the highest risk people.
- It asks them what matters most to them.
- It supports family and other caregivers.

SOURCE: Presented by Diane Meier on July 9, 2015.
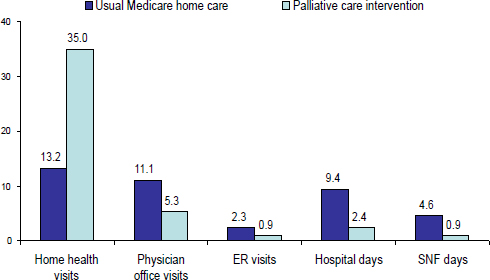
NOTE: ER = emergency room; SNF = skilled nursing facility.
SOURCE: Presented by Diane Meier on July 9, 2015.
- It includes expert pain and symptom management.
- It provides 24-hour access to services, 7 days per week.
The place where health literacy is most involved, explained Meier, is in goal setting, which requires asking the person and family what is most important to them, and she told the stories of four of her patients to illustrate this point. The first story was that of Mr. R., a 67-year-old Latino man that she met on the palliative care service after he had been on a ventilator in the hospital for 4 months. Meier asked Mr. R., who had no family visitors, if he wanted to be removed from the ventilator and allowed to die, and he did not. After fitting his tracheotomy tube with a speaker valve and bringing in a Spanish translator, Meier discovered Mr. R. had a son he wanted to see. After a great deal of research, the staff social worker located a son in Chicago and paid his way to New York to visit his father. The son revealed that his father had been terribly abusive to him and his siblings, and none of them had seen their father for decades. Nonetheless, the son came, the father asked for forgiveness, and the son forgave his father. The patient died on his own the next day. “Where is the illiteracy here?” asked Meier.
She then told the story of Mr. W., a 44-year-old man with acquired immunodeficiency syndrome (AIDS) encephalopathy who had been on a
ventilator, dependent on total parenteral nutrition (TPN), and unresponsive for 2 months. Still, his mother and sister, one of whom was always at his bedside, refused to let him die, and staff was angry, considering this behavior abusive to the patient. Over a weekend, Meier sat down with the mother and sister and asked what they were hoping to accomplish. The response was logical: they wanted to fatten him up so that the open coffin, which was mandatory in their faith community, would not make it obvious that he had died of AIDS. After Meier explained that TPN would not reverse the muscle wasting that had occurred and that the funeral home could do much more to restore his looks, the family decided to remove support and Mr. W. passed away that Monday.
Mrs. P., a 60-year-old first-generation Greek immigrant who ran a hot dog stand in Central Park, had a witnessed cardiac arrest in Central Park, was resuscitated by a bystander, but had severe anoxic encephalopathy and never regained consciousness. Though she still had brain activity, she had spent 6 months on a ventilator receiving TPN and had developed the worst pressure ulcers anyone on staff had ever seen. Her three adult children visited regularly, frequently coming to blows in the intensive care unit (ICU) and requiring the intervention of hospital security personnel, but it was her daughter’s behavior that led staff to call Meier to intervene. This daughter spent every day at her mother’s bedside and brought her 6-year-old after school to sleep on a hard plastic chair next to her grandmother’s bed every evening, which staff felt was abusive. Meier and a nurse she works with sat down with the daughter and asked her to tell them about her family. “Out poured this incredible story of child abuse by this mother and all of the sudden the behavior made perfect sense,” said Meier. This family was used to suffering—that is what they did to each other. As soon as the daughter became conscious of this fact, she agreed to take her mother off of the ventilator. “Nobody had asked what the back story was,” said Meier.
Her final tale was about Jenny, who’s story Meier had told in an article for Health Affairs with the approval of the patient and her family (Meier, 2014). The article, Meier explained, was an oncologist’s response to her question about what he hoped to accomplish with intrathecal chemotherapy for Jenny, a nonsmoker diagnosed at 59 with non-small-cell lung cancer that had metastasized to the brain. Meier had been on Jenny’s care team for 2 years because Jenny, a psychologist, knew that her oncologist could not talk to her about what would happen as the disease progressed. Toward the end of her life, the oncologist offered intrathecal chemotherapy, and Jenny asked Meier what she thought about this treatment. Not knowing enough to respond then, she told Jenny that she or the oncologist would get back to her. Meier went to her colleague and asked him what he hoped to accomplish with this procedure, and after a long pause, he said it would not help her but that he did not want Jenny to think he was abandoning her. “The
oncologist did not know any other way of showing his care and love for his patient other than to give her intrathecal chemotherapy because his training included nothing about accompanying patients when chemotherapy no longer helps,” said Meier. She added, “I am very grateful to that oncologist because he taught me more than I ever had understood before about what motivates my colleagues when they do things that don’t make sense to me. It is love. It is not venality. It is not greed. It is not indifference.”
Though initially given a prognosis of 6 to 12 months to live, Jenny lived more than 6 years after her diagnosis thanks to the efforts of her oncologist, enjoying many trips to Europe with her husband and daughter. Over the last year of her life, she received both palliative care and treatment as her symptoms worsened, and when treatment was no longer effective she was referred to hospice at her home. When Meier went to visit her there, all Jenny wanted to talk about was how her oncologist never called or came to visit and how hurt she was by that. With her permission, Meier called the oncologist and told him that Jenny wanted him to visit, but he did not understand why because there was nothing he could do for her. “She wants to see you to thank you and say goodbye, that she is very grateful to you,” Meier told her colleague. He did visit her and she died soon after.
Literacy and palliative care intersect at the question, “What is most important?” said Meier, and she cited the results of a survey of older people at a senior center and assisted living facility who were asked to rank the order of what was most important: living longer, achieving symptom relief, or remaining independent (Fried et al., 2011). Some 76 percent of these seniors responded that independence was the most important, followed by pain and symptom relief, with staying alive ranking last. “How is the health care system designed?” asked Meier. “Just the opposite.”
Meier noted that some 40 million family caregivers like Mrs. B. provide 37 billion hours of unpaid care worth $470 billion per year while putting themselves at high risk of death, disease, and personal bankruptcy. She also quoted from a book by Atul Gawande (2014), who said, “I learned a lot of things in medical school, but mortality wasn’t one of them,” and from The New Yorker cartoon by Peter Vey (2003) in which a doctor is telling his patient, “There is no easy way I can tell you this, so I’m sending you to someone who can.” While these anecdotal comments point out the challenge of addressing health literacy as a problem of the health system, not of patients and families, Meier said that there is hope thanks to the eight Institute of Medicine (IOM) reports calling for better access to palliative care. “The IOM report that I was privileged to participate in calls for palliative care as a standard of care essentially for people with serious complex illness,” said Meier.
What has to happen to realize the IOM’s recommendations, she said, is that the practices that are helping Mr. and Mrs. B. have to be expanded
to the home and community setting for every patient with a serious illness. Every oncologist, cardiologist, primary care doctor, and nurse in a nursing home have to be trained in the core principles and practices of palliative care because there will never be enough palliative care specialists to come close to meeting the nation’s needs. She applauded the American Cancer Society for running a series of ads that illustrate the importance of palliative care. These ads, she said, convey the central idea that palliative care sees the person beyond the cancer treatment and gives the patient control, and they make the point that palliative care represents a big shift in focus for health care delivery that works to improve the lives of patients. She closed her comments by noting that in the past, physicians considered themselves successful when they cured ovarian cancer or myeloma even though patients lived with terrible consequences of this treatment, such as severe neuropathic pain. In contrast, patients today are living longer and with a better quality of life thanks to the incorporation of palliative care principles.
This page intentionally left blank.












