
4
Professional Training
The workshop’s second panel featured two presentations on the need to train health care professionals to have health literate discussions about palliative care. Robert Arnold, Chief of the Section of Palliative Care and Medical Ethics, Director of the Institute for Doctor–Patient Communication, and Medical Director of the Palliative and Supportive Institute at the University of Pittsburgh Medical Center (UPMC), spoke about methods for improving doctor–patient communication about palliative care. Elaine Wittenberg, Associate Professor in the Division of Nursing Research and Education at City of Hope Comprehensive Cancer Center, discussed training programs for nurses. An open discussion was moderated by Renee McLeod-Sordjan, a nurse practitioner and Medical Ethics Attending for the Department of Medicine at North Shore–Long Island Jewish Health System and Clinical Assistant Professor in the Graduate Department at Lienhard School of Nursing.
TEACHING COMMUNICATION SKILLS TO CLINICIANS1
After remarking how angry he was about the state of the American health care system after listening to the last panel presentations, Robert
__________________
1 This section is based on the presentation by Robert Arnold, Chief of the Section of Palliative Care and Medical Ethics, Director of the Institute for Doctor–Patient Communication, and Medical Director of the Palliative and Supportive Institute at the University of Pittsburgh Medical Center, and the statements are not endorsed or verified by the National Academies of Sciences, Engineering, and Medicine.
Arnold wondered why there was a need for the term palliative care when the concepts embodied by palliative should be the norm in all health care. “I think we diminish what the health care system should do by calling it palliative care,” said Arnold. “We ought to just call it good health care.” He also remarked that getting American health care to embrace palliative care seems to him to be a culture change problem and not really about any one system, and that this culture change is just not happening. He recalled reading a book (Mishler, 1985) when he was studying medical ethics that talked about a world of medicine and a world of patients and that the two never talked to one another, and realized after hearing Thomas Smith’s presentation that nothing has changed. “The story that we tell in medicine is that it is all the family’s fault,” said Arnold.
He then commented on the book Knocking on Heaven’s Door: The Path to a Better Way of Death (Butler, 2013), whose author, like Arnold, no longer sees doctors as healers but as skilled technicians with their own agendas. Patients such as the book’s author have gotten smarter, he said, in that they believe in science but do not have the same view about their doctors because their doctors do not seem to care about what their patients’ lives are like. He told of conversations he has with the house staff at his hospital who have no idea of what is going to happen after they send a terminally ill patient home or to a nursing home and have done nothing to prepare the family for what might happen and how to respond. The cause of this seeming indifference, said Arnold, is that the culture of medicine has split into little tribes, none of which know the patient.
One of the things that angers Arnold is that experts still debate which medical professional should talk to patients and families about advance directives when 70 percent of the time nobody does it. The key question to him is whether there is way to change culture so clinicians can have real conversations with their patients about prognosis and end-of-life care. He and his colleagues at Vital Talk have been trying to do just that by teaching doctors to pay attention, at the times that matter most, to what their patients are saying to them and to talk back to them like human beings, not as if they are talking to the house medical staff. Today, he added, the patients who doctors like best are the ones who can report on their symptoms and treatments as if they were medical students during rounds.
The comprehensive program that he and his colleagues developed, OncoTalk, was started 15 years ago as a 4-day intensive skills retreat, funded by the National Cancer Institute (NCI), for 115 oncology fellows from 62 institutions using actors trained to be patients. The patients were of various ages and socioeconomic backgrounds who knew no medicine, and the fellows’ interactions with the mock patients were recorded before and after communication skills training sessions (Back et al., 2007). When the recordings were later played to a group of listeners, they could readily
tell whether the recordings were from before or after training and were amazed at the change in communication style. Of the eight communication skills that OncoTalk emphasizes, the most important is how to deal with emotion. Doctors, said Arnold, do not like emotions, and he blamed this on the way they are trained—to learn facts and to fall back on book knowledge when confronted with an uncomfortable situation. He noted that Lesley Fallowfield at Brighton and Sussex Medical School has taken the same approach and found that not only does training improve communication between doctor and patient, but that skills continued to improve 6 months after training because the physicians liked that they could have better conversations with their patients.
What these approaches share, said Arnold, is they provide trainees with the opportunity to address barriers and to both practice the skills they were learning and watch their colleagues engage in simulated conversations. Individualized feedback is also important, as is providing a supportive and safe environment in which to learn and practice these skills that do not come naturally to most physicians. They emphasize “ask before tell” and letting the patient lead the conversation, and they teach physicians how to attend to emotions and give information in simple language based on patient need.
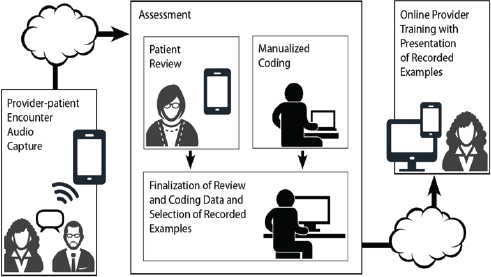
The problem with these approaches, said Arnold, is they are time intensive in that they need to take place over 3 to 4 days. In an attempt to remedy that problem, he and his colleague James Tulsky at Duke Medicine have been testing a theory-based, self-administered, 1-hour intervention provided on a CD-ROM designed to improve an oncologist’s response to a patient’s expressions of negative emotion in outpatient encounters. In a randomized, controlled trial, participating oncologists were recorded speaking to their patients during clinic visits. The oncologists then received a lecture on how to improve their communication skills, and 1 year later half of them received the CD-ROM, included didactic information, video demonstrations, and audio clips from the oncologist’s own recorded conversations (see Figure 4-1). At the end of each module, the oncologist was asked to commit to try targeted communication behaviors and prior to the next clinic visit, the oncologist receives an email reminder of their commitment. The two key findings from this study, said Arnold, were that oncologists receiving the CD-ROM doubled the percentage of times they responded to negative emotions, and their patients said the doctors’ communication had greater impact (Tulsky et al., 2011).
One challenge that needs addressing is that of scale, or teaching all doctors to communicate effectively with their patients, said Arnold. He and his colleagues are now engaged in a study funded by the Patient-Centered Outcomes Research Institute and the American Board of Internal Medicine to see if this intervention can be delivered as a Maintenance of Certification course for continuing education credits and still have the same positive
SOURCE: Presented by Robert Arnold on July 9, 2015.
effect on oncologists’ communication skills. Perhaps the bigger challenge, though, is to create the political will to change culture. “Doctors are comfortable doing what doctors have always done, and oncologists do not have it in their DNA to be good communicators,” said Arnold. “My view is they either need it in their DNA or they need to get out of medicine. We, as a culture, need to say medicine needs to change.”
NURSE TRAINING2
Nurses are the frontline of care across disease and settings, and they spend a significant amount of time with family caregivers, providing education and support, said Elaine Wittenberg. When it comes to communicating with patients and families, nurses, unlike doctors, do not need training to initiate conversations because patients and family members typically are the ones who start conversations with nurses. In addition, nurses are often asked to translate what the physician has said or what a patient or family member has read on the Internet, and in fact, one of the key roles nurses play is to educate and promote communication among team members, patients, and family members. Nurses provide an immense amount
__________________
2 This section is based on the presentation by Elaine Wittenberg, Associate Professor in the Division of Nursing Research and Education at City of Hope Comprehensive Cancer Center, and the statements are not endorsed or verified by the Academies.
of psychosocial support to patients and family members—dealing with emotions is not foreign to nurses—and they often serve as key mediators between patients and family members in making decisions about treatments and about goals for care.
Wittenberg explained that primary training for nurses in palliative care started at the City of Hope with Betty Ferrell’s work creating the End-of-Life Nursing Education Consortium (ELNEC). To date, the consortium has provided more than 170 courses to nurses and has trained almost 20,000 nurses in all 50 states, the District of Columbia, and 88 countries. What started as a core curriculum has evolved into different versions for specific nursing subgroups, such as pediatric, geriatric, and critical care nurses. Health literacy holds an important place in these curricula because nurses are often asked to translate complex medical words, abbreviations, and procedures, and to describe medications and teach patients and family members how to use medications at home.
Health literacy affects quality of care, said Wittenberg. Patients with compromised health literacy, for example, have a hard time adhering to medication regimens. She noted that the seriously ill patient population and their caregivers are aging, which increases the health literacy challenge. She also said she thinks of health literacy as including oral literacy, which refers to a person’s ability to speak and listen. Lower listening skills, she explained, complicate the ability to understand and recall complex oral information and have a negative impact on medication management. Family meetings are common in palliative care, but her research has found that not all patients and families are comfortable communicating in a small group, let alone a large one that includes the entire health care team. Regardless, the health care system puts a great deal of pressure on oral literacy skills because the most common method for getting information from patients and family members is by asking them to provide the patient’s medical history orally.
Over the past 5 years, Wittenberg has been working with Debra Parker Oliver at the University of Missouri to record hospice teams talking with patients and family caregivers and measure caregiver outcomes for anxiety and quality of life. One finding from this work was that as the grade-level talk in the conversation increased, so too did the anxiety level of caregivers (Wittenberg-Lyles et al., 2013a), which in turn led to confusion among caregivers about how to properly provide pain medication at home. Another finding was that hospice team members used six times as many medical words as caregivers (Wittenberg-Lyles et al., 2013b). “Yes, we do have caregivers who can learn how to present to an attending physician, but those are few and far between in our family caregiver population,” said Wittenberg. The majority of the medical words used were drug names, which sometimes were brand names, other times generic names, and 75 percent of the medi-
cal words were not explained to the caregivers. Moreover, the parts of the conversations that had the most medical words proceeded at a faster pace, giving caregivers little time to respond and understand.
According to the National Library of Medicine, the appropriate level of educational health information should range between a sixth and seventh grade reading level, which Wittenberg acknowledged, based on her experience with her sixth grade daughter, is not easy to achieve. Nonetheless, training for nurses in palliative care is needed to develop this communication skill, and toward that end, she and colleagues Joy Goldsmith, Betty Ferrell, and Sandra Ragan have developed the COMFORT communication curriculum (Wittenberg-Lyles et al., 2015). This curriculum is based on seven core principles of palliative care communication: communication, orientation and options, mindful communication, family caregivers, openings, relating, and team. The modules on communication, for example, emphasize clinical narrative practice. The orientation and options module teaches nurses to describe the big picture of a diagnosis, summarize the disease path, and share options for treatment and care in plain language and with sensitivity to a patient’s and family’s cultural background. One of the tools they have developed is the plain language planner for palliative care, which translates the 20 most commonly used medications and symptoms into plain language at the sixth grade level based on five readability indices. The planner includes such plain language essentials as using the active voice, using the patient’s and doctor’s names, speaking in the second person, limiting jargon and defining new words, and keeping sentences to 15 words or less as a means of limiting the amount of information provided at one time.
The initial research with the planner compared the written responses from 155 nurses recorded before and after the planner was introduced and used by the nurses (Wittenberg et al., 2015). The nurses were asked to explain a medication and symptom to a patient, and results showed they were able to integrate and use plain language after attending an educational session on the planner. Most importantly, said Wittenberg, the amount of jargon decreased and the use of active voice increased.
In January 2015, the COMFORT communications team launched its first training efforts, including instruction on how to use the plain language planner, for 30 hospital-based palliative care teams across California. Wittenberg and her colleagues have more recently trained 100 nurses nationwide, with plans to train another 100 in October 2015. To help further disseminate the planner, her team has created a pocket guide and integrated it into an app called Health Communication for Apple devices. She and her colleagues are also adding additional information on oncology symptoms and medication side effects to the planner at the request of some of the providers who have participated in their studies. They are also translating the planner and the app into Spanish. In closing, Wittenberg
mentions that the Textbook on Palliative Care Communication, which has five chapters on health literacy, would be published in October 2015.
DISCUSSION
To open the discussion, moderator Renee McLeod-Sordjan asked the two panelists to talk about how the medical profession is preparing the next generation to be better communicators and produce the necessary culture change. Wittenberg said she is excited, not dismayed, about the future because the stage has been set to determine what palliative care communication should look like and how it should be delivered given what has been learned through research over the past 15 years. The challenge, she said, is to develop tools for health care providers to use. She noted the decision aids and question prompt lists that Thomas Smith spoke about as good examples of the kind of tools that are needed. “Some specific disease areas, such as oncology, are already developing those tools, but from a palliative care perspective, we do not have palliative care decision aids per se,” said Wittenberg. The next step, she said is to conduct quality research on communication strategies that can be used to train providers in all areas of medicine. She also said interprofessional education should be prioritized as a key component of this effort to drive home the point that it is the entire health care team’s responsibility to provide information to patients and family members at the appropriate health literacy level. “There is a team process piece that has to be accounted for when we think about training providers about communication,” she said.
Arnold said that medical schools are doing more today to teach communication skills. Vital Talk, for example, is working with cardiologists, nephrologists, and neonatologists, and he has heard that a course for pediatric cardiologists is being developed as part of physician training. To him, there are two big challenges facing the next generation of health care providers. The first is to ensure that once they train to be good communicators that they move into an environment that rewards them for that skill. “Are they going to be in an environment in which a 10-minute conversation is 5 minutes too long because they have too many other things to do that the health care system says are more important than communication?” asked Arnold. Second, he said, it is important not to just add more cognitive material to the training the next generation receives because decisions are not made entirely on the basis of facts. He mentioned emotional intelligence as being important. “We need to think about what will help clinicians have emotional resiliency to have these hard and sad conversations,” said Arnold.
McLeod-Sordjan said that was an excellent point and asked the panelists about their expectations for health literacy given that health care providers are no longer getting trained in silos. Arnold said that interprofessional
communication training is a good idea, though he had no idea how to do it. “We do not even know how to make sure that doctors and nurses have good communication skills let alone how to put them together so that they do not conflict with one another,” said Arnold. This is particularly true, he added, given that in today’s health system the same nurse and doctor rarely work together on a regular basis. He used a school band as an analogy. “It would be like every week having a different band because you took kids from different schools and put them together every week and expected them to play well.” Though there are many opportunities, he said, the health care enterprise still needs to figure out which systems will work better for patients and how to create a health care system that better meets patient needs.
One advantage of working with a palliative care team, said Wittenberg, is that its members stay fairly constant. “If you have everybody using the same language and practicing together in a team-based approach, that is going to initiate cultural change at your institution,” she said. “It is also going to help patients and families when they hear the same message and the same language from the palliative care social worker as they do from the palliative care nurse and palliative care physician.” Toward that end, she encourages palliative care teams to work together to develop unified definitions and explanations that are specific for the patient population they serve, as well as culturally appropriate metaphors. She also believes that if every member of the palliative care team is consistent in the language they use with patients and families, then patients and families are going to have expectations of consistency and express that to other providers they encounter. That, she said, will further the culture change that needs to happen.
Winston Wong from Kaiser Permanente asked Wittenberg if she knew of any curricula that were being developed for interdisciplinary training for nursing and medical schools. Wittenberg replied that she does not know of any standardized communication training programs that are available today, though ELNEC is developing an undergraduate nursing curriculum on communication that will be tested online in four states in the upper Midwest. Arnold added that the Macy Foundation has funded a number of initiatives in this area. The University of Pittsburgh, for example, offered a course that nurses and medical students took together when they took care of patients in long-term care. What is not clear from studies of these efforts is how well the different professions give consistent information to patients, as opposed to how well they get along with each other and understand what each other does. Most of the work, he said, has focused on measuring the latter. McLeod-Sordjan added that schools need to move away from teaching nurses and doctors how to break bad news to patients and then move on to teaching them more broadly how to have difficult conversations about chronic disease.
Wilma Alvarado-Little noted that the presentations have focused on adult palliative care, and she asked if any considerations have been made regarding pediatric palliative care. Arnold said that there are a number of ongoing efforts in that area. A program at Johns Hopkins Medicine, for example, trains neonatologists to talk to parents about their critically ill infant, and the University of Pittsburgh has a program for pediatric intensivists. The University of Indiana is teaching pediatric oncologists how to talk with parents and children, and Vital Talk has a group of individuals who are beginning to do work in pediatrics. Wittenberg said that ELNEC is working with its core curriculum to develop one specific for pediatrics.
Cindy Brach from the Agency for Healthcare Research and Quality (AHRQ) commented that while there have been several mentions of the need for culture change, the two panelists both spoke about stand-alone interventions to intervene with specific clinicians, which she said does not sound like a recipe for culture change. She then asked the panelists if either of them had any experience trying to change an entire institution or health care system and sustain change. Arnold said that the first step that he has taken at UPMC Health System has been to measure how many seriously ill patients there are at each of the system’s hospitals and to then measure how many of these patients have a documented discussion about goals of care. He is now developing metrics that he can take back to the chief medical officer of each hospital and the heads of each service line to document the scope of the problem. Starting in 2015, UPMC is conducting 1-day courses for practicing clinicians—the fellows already take courses—and the heads of every service line have agreed that every clinician will take this course. The course will use simulated patients to illustrate how to talk about goals of care.
His next move, he said, will be to enact policy that will forbid any medical student or intern to have this conversation with a patient, given that they have not been trained to do so. “We do not let medical students or interns put in Swan-Ganz catheters, and any intensivist will tell you that it is harder to have a conversation about goals of care than it is to put in a Swan-Ganz catheter,” said Arnold. In his opinion, what is more important than establishing these systems and rules in the hospital is to develop programs for use in the home care and ambulatory-based setting to really produce culture change. The goal, he said, should be to have these conversations with people before they need to be treated in the hospital.
Wittenberg remarked that the first national nurse communication training program just started in 2015. Nonetheless, some of the participants in this program have already been recognized in their institutions as being leaders in communication training and being initiators of culture change. One of the goals of her program, she said, is that the nurses will themselves become trainers when they go back to their institutions and implement some sort of cultural change. She noted there is a competitive application
process to be accepted into the course, and one of the requirements is to identify three goals for when the applicant goes back to his or her institution. As part of the evaluation of the communication training course, she and her colleagues follow up at 6 months and 12 months to find out what the trainees have done since returning to their institution with regard to how many people in how many disciplines they have trained and what new systems they have implemented. Part of the COMFORT curriculum, in fact, includes supplemental resources to initiate change, including research-based decision aids, question prompt lists, and tools to measure and evaluate the communication skills of the providers that they then train.
Michael Paasche-Orlow from the Boston University School of Medicine applauded both speakers for talking about culture change and pushing that conversation forward. He also noted the parallel focus on communication between health literacy and palliative care. He then asked the panelists to comment on how they think about the problem in a broader cultural context rather than in terms of one institution or health care system at a time. Arnold said that he would like to see more emphasis on community and public education and getting to the public before they enter the health care system. Part of this effort will be to train patients and caregivers to expect something different from the health care system than the promises that the next miracle is right around the corner. He commended the Center to Advance Palliative Care for its efforts in public education, and also called out newspapers and science reporters for their role in touting the next promising cure.
Wittenberg said that she would like to see the topics and scope of communication training broadened. As an example, she said she would like all health care providers to receive spiritual care communication training and more interprofessional training. She would also like to see training for family caregivers and noted that ELNEC is about to run a trial that offers a communication guide for caregivers that aims to ease the burden placed on caregivers to relay hard news to, and mediate among, family members. “We need to pay more attention to this communication task that family caregivers take on and provide some training and support for that as well,” she said, adding that nurses are in a good position to help support caregivers with that task.
Bernard Rosof closed the discussion for this panel with the comment that it is time to stop teaching medical students as individuals and start teaching them as part of a health care team, perhaps with patient advocates such as Beverly Alves involved in that team. “The real opportunity to address these challenges is to do it with the team and not with the individual,” said Rosof. He noted that there are, in fact, medical schools that are taking this approach, and his prediction is that they will be more successful training physicians to be good communicators and team members.










