
5
Integrated Care Teams
The afternoon’s first session included four speakers presenting different perspectives on how to provide palliative care. Reverend Richard Freeman, Sr., a member of the Pastoral Team at the University of Pittsburgh Medical Center (UPMC) Children’s Hospital and Senior Pastor of the Resurrection Baptist Church, discussed how to integrate spiritual care into palliative care. Carol Levine, Director of the United Hospital Fund’s Families and Health Care Project, provided a family caregiver’s perspective, and John Cagle, Assistant Professor at the University of Maryland School of Social Work, spoke about the role that social workers play in palliative care. Ginger Marshall, National Director of Palliative Care for Hospice Compassus and President-Elect of the Hospice Palliative Nurses Association, then addressed the role of nurses in providing palliative care. An open discussion moderated by Yael Schenker, Assistant Professor in the Division of General Internal Medicine, Section of Palliative Care, and a member of the Clinical and Translational Science Institute at the University of Pittsburgh, followed the four presentations.
HOW TO BRING SPIRITUAL CARE INTO PALLIATIVE CARE1
“I believe that the essence of what we do in palliative care, what we do in spirituality, is tending to the broken heart,” said Richard Freeman as
__________________
1 This section is based on the presentation by Reverend Richard Freeman, Sr., a member of the Pastoral Team at the University of Pittsburgh Medical Center Children’s Hospital and Senior Pastor of the Resurrection Baptist Church, and the statements are not endorsed or verified by the National Academies of Sciences, Engineering, and Medicine.
an introduction to his presentation. His hope, he said, was that his remarks would help the workshop attendees gain an appreciation for the imperative of spiritual care, increase their personal posture of attending to patients’ spiritual needs, and develop a better repertoire of resources to aid in meeting the needs of patients. He also noted that palliative care is a “heart thing—it is moved by what drives us at the core of our being. If the core of our being is not engaged in this work, we will not move forward.” His challenge to the workshop was to not overintellectualize what the human spirit cannot comprehend and to not fall back to the position of developing another tool.
Freeman said that he was impressed with the field’s efforts in teaching and building what he called brand new hammers. “But my challenge is we have to build better carpenters, and we do that by dealing with the continuum of care and with the heart of people,” he said. The one thing that has been missing from the day’s presentations, he said, is any mention of a person’s life before they became ill. To truly understand patients and their needs from the health care system, it is necessary to understand the histories that are integral to them, explained Freeman. He used the story that Diane Meier told about Mr. R. and his need to speak to his son, talk to him about the burdens of his soul, and ask for forgiveness from his son. It was only then that he was able to find peace and die.
Freeman then talked about the synthesis of humanity as a meshing of body, mind, and spirit. Health care providers, he said, do well with the body and mind because they believe they can fix them when they are broken, but they do not do as well with a person’s spirit, which he defined as the repository of meaning making. Dealing with this last piece of humanity, he said, is where his responsibility as a pediatric chaplain lies, adding that the way these three pieces fit together is shaped by who each person is. He noted that he is also trained as a psychotherapist, and during his training he was forced to develop a keen sense of introspection to understand his own motivations. If he had one wish, he said, it would be for every clinician to go into therapy to truly understand what drives them to do what they do. “When they come to terms with that, they will no longer be exercising it in the context of being a caregiver,” said Freeman.
He then told a story of a mother who was tending to her son at Children’s Hospital. As is his practice, he came into the room, introduced himself as the manager of the pastoral department, and let her know that he was available to help. Later that day, he got a phone call from the boy’s nurse who said this woman wanted to talk to a psychologist—she had sequestered herself and was crying profusely. When he came to her son’s room, she said to him that she had asked for a psychologist, but that he would do, and she abruptly stopped crying. She then informed him that she was Jewish, and that she did not believe in Jesus Christ. He said that was
okay, that he did, and asked if they could talk. He recalled that she then started laughing when she realized he was not there to convert her but just to be with her, and for the remaining week and half that she was in the hospital before her son was sent home to die she talked to him every day. “That is the spiritual part that I am talking about,” said Freeman.
He then challenged the workshop by arguing that not doing spiritual care may in fact be unethical. The major tenets of ethics, he said are autonomy, nonmaleficence, beneficence, and justice. “If you don’t know my spiritual journey, how can you say you are allowing me to work autonomously?” he asked. “If you don’t know what vexes my spirit when you offer me a treatment that is going to prolong my life, but is never going to improve my lot and you are telling me I cannot go be with my God, you might be doing something that is maleficence. If you don’t know what drives and motivates me, you may be keeping me from the very thing that gives meaning to my life,” he said.
How then is it possible to avoid this ethical quagmire? Informed consent, he said, is a governing principle of patient interaction. Although often implied, there is another principle operative in medical delivery that he called informed treatment—that a patient gets what they desire. Spirituality, said Freeman, must be considered when determining what medical services are dispensed.
Returning to the idea of building a better carpenter, Freeman listed a few steps to take to be prepared to care for all of a patient’s needs. It is important, he said, to identify personal hot buttons, the situations that takes someone out of their sphere of comfort. Most hot buttons, he said, are a by-product of a person’s construct of likes and dislikes and are informed by personal histories. It is important, too, to recognize that every caregiving experience is a learning experience that can help hone individual best practices. “Understand your value system and be acquainted with your nonnegotiables,” said Freeman. “Distinguish those values that are your essence from those that are just important, and safeguard those values that you esteem as your essence.” Lastly, he said, it is critical to have spiritual integrity, the ability to differentiate one’s values from those of a client without a compulsion to reshape the spiritual beliefs of the client. “Nurturing spiritual integrity requires searching for the questions that vex your spirit and that give meaning to you and you alone,” said Freeman. “Once you have gotten those answers, find peace with it, and then leave it alone. It is not to be dealt with in the context of a caregiver.”
It is important for health care providers to nurture spiritual integrity because they will be more empathic in their approach when their issues are not their patient’s issues, he explained. “We become more tolerant of differences that are apt to be discovered when working with the dying,” said Freeman. He noted that spiritual integrity is not the same thing as religious
training. Although religious traditions inform spiritual identity, religion is not the sum total of a person’s spiritual essence, he explained. It is possible to feel that one’s spiritual essence is seriously threatened, and when that happens one should appeal to other members of the care team and perhaps even step away as a caregiver if the situation dictates.
Freeman ended his presentation with two suggestions on how to enhance the delivery of spiritual care. The first is to be curious, to recognize the humanity in every patient as a common starting point from which to ask interesting questions. The second is to be courageous and ask potentially difficult questions. “This is not easy,” said Freeman. “Sometimes you are going to have to ask somebody about their spiritual journey and the meaning it gives them. It is a question that affirms the individual’s humanity, and if we do that we have been good caregivers.”
A FAMILY CAREGIVER’S PERSPECTIVE2
Carol Levine approaches the subject of palliative care from the dual perspective of someone who directs a project that works with family caregivers and who for 17 years was the caregiver for her late husband, who suffered a traumatic brain injury that left him quadriplegic and with a severe cognitive impairment. She said that when she was listening to Beverly Alves and Diane Meier, she could feel anger welling up inside her as she remembered all the things she dealt with during her years as her husband’s caregiver and saw that the situation for family caregivers has changed little over the past 20 years. She recounted that the attitude 20 years ago was that the wife would take care of things. “Some people go to the hospital and lose their eyeglasses,” she said “I lost my identity. I became the wife.” That personal experience, she said, combined with her 20 years of professional experience in the field, colors what she had to say at the workshop.
The person who is health literate, said Levine, needs to understand not only the medical situation, what the treatment might be, and how to make choices, but also understand bureaucratic language, insurance language, and institutional arrangements. From her perspective and experience, health literacy is not a problem solely of poor people, those with low education levels, or of any ethnic or racial group. Depending on the circumstances, anyone can be health illiterate as it is impossible to be completely up to date on all knowledge pertaining to health and health care. To make that point, she told the story of an ambulatory clinic administrator who asked her to explain the difference between hospice and ambulatory care. “Here is a per-
__________________
2 This section is based on the presentation by Carol Levine, Director of the United Hospital Fund’s Families and Health Care Project, and the statements are not endorsed or verified by the Academies.
son in the health care system and she did not know,” said Levine. “We have to assume that at some point, every one of us will need more information and better explanations.” In her opinion, she added, understanding services may be harder than understanding basic health information.
When she started her journey she expected the health care system to be a maze and expected that taking her husband home from the hospital was not going to be simple. “Nurses and the social worker waved good-bye to me from the rehab facility and said ‘You are on your own now, dear,’ and I was,” she recounted. She figured, though, that being smart and having accomplished much during her life that she could figure out how to get the services she needed to care for her husband. What she encountered, though, was not so much a maze as an abstract painting with no clear path and nobody to guide her. There were individuals who could help her navigate one little section of the journey, particularly with regard to the hospital experience, but there was nobody to help her once she was in the community.
There are several reasons, said Levine, that palliative care is hard to understand. To start, it is hard to spell and pronounce, and there is the confusion between hospice and palliative care. Health care professionals do not even share the same definition. There are palliative care doctors, who offer specialized medical care. Home care nurses think they are providing palliative care but they are really providing ordinary care for sick people. Long-term care staff believe they are providing palliative care when they are keeping residents quiet and comfortable. “If providers have different definitions, how can the patient and the family caregiver understand it?” asked Levine. She noted that there is much to be unlearned about palliative care before new information is presented to patients and families. Contrary to common belief, palliative care is not just for dying, it is not a program to save the government money, and it does not require hospitalization. Palliative care does not mean giving up hope, nor does taking pain medication lead to addiction. Most people believe that insurance will not cover palliative care at home, which may or may not be true, and it is common to assume that palliative care means the doctor is abandoning the patient and family.
From the perspective of the family caregiver, there are special challenges, said Levine. There is an intense emotional component, and it is important for clinicians to recognize that and confront it directly. Levine suggested that the simple statement, “I understand this is a difficult and emotional time for you,” can mean a great deal coming from members of the health care team. A challenging role that the family caregiver takes on is making health care decisions either with or for another person, which is not only difficult but can cause conflict within the family. Levine noted that there are often people within a family who each perceive they have an equal role to play in decision making yet come to the table from different
perspectives and with different information about and understanding of the family member’s medical situation.
Often, family caregivers feel excluded from the health care team. Levine recounted that when she was caring for her husband, she repeatedly asked to have a meeting with his health care team. It never happened even though she knew there were team meetings. Affordability is a major concern of family caregivers, and Levine noted that Medicaid Managed Long-Term Care may no longer cover all of the services the caregiver may want for their loved one. Family caregivers also worry about being able to provide complex care at home. “Palliative care as it is practiced today is not chicken soup and a pillow,” said Levine. Family caregivers are not getting the proper training to manage a morphine drip, a peripherally inserted central catheter, and other complicated procedures, and Levine questioned how that was acceptable practice.
United Hospital Fund’s free Family Caregiver Guide to Hospice and Palliative Care (United Hospital Fund, 2013) is an attempt to provide this kind of information, and it includes a chart comparing hospice and palliative care (see Table 5-1). Levine said both the English and Spanish versions are the most frequently downloaded guide to palliative care. It is also available in Chinese and Russian. Its popularity, she added, suggests that family caregivers are not getting information from health care providers.
Caregiver assessment can be used as a guide to discussion, but Levine suggested that it should not be done in the manner of a formal medical exam. Start by acknowledging that the caregiver has much to learn about palliative care and how it will affect the patient, and learn about the caregiver’s situation and who will do what for the patient. Ask the caregiver about his or her other responsibilities for an honest assessment of their limitations, and probe for worries and concerns, which is often the most revealing part of the assessment and can provide answers that range from the mundane—can I get home in time to pick up my child from school?—to the existential—why is this happening?
The most important thing to do for family caregivers, said Levine, is to involve them at every stage of the patient’s care and decision-making process so nothing comes as a big surprise. Start the discussions early, not when a crisis situation develops, and be available to offer support and training. Levine reminded the workshop participants about the importance of dispelling myths and answering questions as often as needed using clear, simple language. In conclusion, Levine described the four habits approach to effective communication (Frankel and Stein, 1999), which are to invest time at the beginning of the process to develop trust and learn about the patient’s and family caregiver’s perspective early rather than when a crisis arises. Demonstrate empathy, both in words and body language, and invest in the end by summarizing what was heard and what the next steps will be.
TABLE 5-1 United Hospital Fund’s Comparison of Hospice and Palliative Care
| Palliative Care | Hospice Care | |
| Goals | To assess and treat the patient’s pain and other physical, psychosocial, and spiritual problems. | To keep the patient comfortable, as free as possible from pain and symptoms, and allow him or her to maintain a good quality of life for the time remaining. Hospice accepts death as an inevitable outcome for a patient with a terminal (end-stage) illness. In hospice, both the patient and the family are the focus of care. |
| Patients | Palliative care accepts patients who have complicated or advanced medical disease. There is no time limit in terms of life expectancy—patients may or may not be dying. Patients can get treatments intended to cure. They also can participate in research studies. | Hospice only accepts patients who are near the “end of life” (meaning they have a terminal illness) and are likely to die within 6 months if the disease runs its normal course. |
| Where care occurs | Palliative care is usually given in hospitals. Sometimes it takes place at nursing homes or assisted living facilities. Palliative care at home is possible but not readily available. | Most hospice care happens at home, although it can also be given in other settings as well, such as the hospital, nursing home, or assisted living facility. |
| Who provides the care | Palliative care is a medical subspecialty. This means that doctors and nurses who practice palliative care extra training about ways to manage symptoms. They work with a team of other professionals. | Hospice care is a team approach, led by doctors and nurses with special training. Specialists may provide spiritual, psychosocial and other care. Hospice care may require a lot of time and effort from the family. |
| Paying for services | There is no special insurance benefit for palliative care. The patient’s health insurance generally covers palliative care services. | Hospice is a Medicare (federally funded) program. Many state Medicaid plans and private health insurance plans pay for hospice. |
| A patient who chooses the Medicare hospice benefit agrees to give up treatments meant to cure disease. This is in return for other types of support and supplies. | ||
SOURCE: Presented by Carol Levine on July 9, 2015.
A SOCIAL WORK PERSPECTIVE3
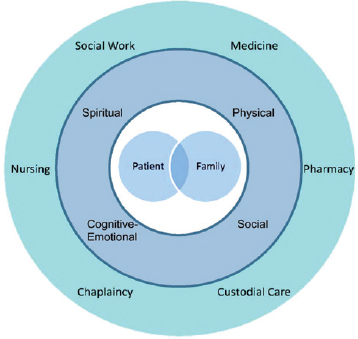
John Cagle, who was a hospice social worker for 10 years before assuming his current position, said he is ready for the culture change some of the speakers had discussed. “I would love to see what we have been practicing in the field implemented sustainably across the country,” said Cagle. He then gave his working definition of palliative care as being patient- and family-centered, interdisciplinary, focused on quality of life, and can take place either inside or outside of hospice. Social work, he said, is part of the interdisciplinary team that addresses the multidimensional needs of patient and family (see Figure 5-1). He noted that there cannot be palliative care without the family or a truly interdisciplinary team addressing these multidimensional needs.
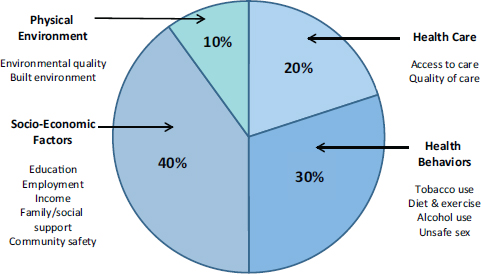
The different disciplines involved in true palliative care each bring a unique set of skills, though there is overlap. Cagle sees the interdisciplinary team as a Swiss Army knife for palliative care, with social functioning as the can opener because social workers get people to open up. Social care has to be integrated into palliative care given that socioeconomic factors account for as much as 40 percent of the determinants of health, while health care accounts for only 20 percent (see Figure 5-2). In fact, he views medical care much like water for a plant—it is important and good, but too much can be a bad thing.
The role of social workers within palliative care is to attend to many of the nonmedical social, emotional, behavioral, and environmental aspects of care. Social workers also provide a comprehensive psychosocial assessment of a patient and family, help patients and families navigate complex health care systems, and negotiate transitions across settings. Social workers can help foster coping and minimize psychosocial distress, provide emotional support, and facilitate decision, often by leading or coordinating family discussions about care goals. He said there is a belief that social workers are not conducting these family meetings but in fact they are (Meeker et al., 2014; Sharma and Dy, 2011). Other roles that social workers play include improving access and adherence to treatment and connecting families to needed resources available in the larger community.
Health literacy, palliative care, and social work intersects in five places, said Cagle. These include
- Careful attention to language
- Addressing myths and misperceptions
- Advocacy for social justice and vulnerable populations
__________________
3 This section is based on the presentation by John Cagle, Assistant Professor at the University of Maryland School of Social Work, and the statements are not endorsed or verified by the Academies.
SOURCE: Presented by John Cagle on July 9, 2015.
SOURCE: Presented by John Cagle on July 9, 2015.
- Facilitating coping and minimizing distress
- Acknowledging uncertainty and change
Schools of social work focus on communication and family dynamics, part of which involves paying close attention to language. Language is how people make sense of the world, yet the health care system fails repeatedly to use appropriate language. The potential pitfalls and missteps include using medical jargon, acronyms, and Latin phrases. Basic terms such as oncologist do not make sense to many people, said Cagle. The volume of information given to patients and families is often overwhelming, and as an example, he said he has seen families receiving 2-inch-thick stacks of information at hospice admission. “We cannot expect them to retain all of information,” said Cagle. Individuals on the health care team often lack the time to solicit information from and provide proper explanations to family members, suggesting the need to better manage the way team members work to meet family needs.
Metaphors may seem useful and are well intended, but metaphors such as “fighting against cancer” can put patients in a position where they feel they are fighting against themselves, producing an intrapsychic dilemma. Moreover, when a patient reaches a point where they are going to succumb to their illness, they can feel that they did not fight hard enough, producing subtle blame on the patient. Cagle also said that absolutes need to be avoided—instead of saying there is nothing more to do, say it is time for palliative care and expert pain and symptom management, which are not doing nothing. It may seem that there are few options when therapy fails, but the truth, he noted, is there is much that can be done, such as paying attention to quality of life and dignity; exploring and defining the family role from that point on; mobilizing social, emotional, and spiritual supports; and strengthening relationships. It is also important, he added, to be attuned to culturally specific terms. As an example of the latter, he has found in his own research that the term good death, which is used often in the medical setting, is not a term found in the Hispanic lexicon, and Hispanics are more likely than members of other ethnic groups to describe death as bad rather than good.
“We need to choose our words carefully because the way we frame decisions affects how decisions are made,” said Cagle. “It is important to recognize our own biases, our own perspectives, our own prejudices so when we go in to talk to the patient and family, we understand our own frame of reference.” Paying attention to body language is also imperative. “If we ask a question and we are nodding our head, we might be prompting a yes answer,” he said as an example.
Cagle agreed with Levine that it is important to educate patients and families and to address myths and misperceptions. He noted that only
20–30 percent of Americans have heard the term palliative care, and while 85 percent have heard of hospice, nearly two-thirds do not know that hospice requires patients to forego curative treatment. When he and his colleagues administered a true-false test related to hospice, the mean score was 78 percent, a C plus grade. Common misconceptions about hospice include it is only for cancer patients, it is a place, it is only for the patient, it is expensive, and it stops after 6 months. Patients and family members also overestimate the likelihood that treatment will succeed and underestimate the risks and costs of therapy even though many of the best interventions have low rates of success and high rates of burden, said Cagle. He is particularly concerned, he said about the disparities in understanding and utilization among African Americans and Hispanics, as well as among other high-risk populations. He noted that an estimated 40 percent of patients who qualify for hospice care never receive it (Harrison et al., 2005).
It is also vital, said Cagle, to address the emotional and psychological factors, such as shock, denial, anger, blame, depression, and anxiety that can impede the ability of a patient or family member to process health-related information. Helping patients and families dealing with uncertainty and change is another important consideration for the health care team. The truth, said Cagle, is that there are many unknowns when it comes to serious illnesses and the potential effects of treatment, yet health care professionals most often focus on facts. “We need to have frank conversations about what we do not know,” he stated. Regarding change, health literacy and preferences may change as a result of medication side effects, disease progression, and emotional capacity.
In conclusion, said Cagle, health illiteracy is invisible and requires vigilance on the part of the health care team. It is important to assess for it, to start where the patient and family are when they enter the health care system. Communication is key to addressing health literacy, and while it is impossible not to communicate in some way, not all communication is effective or appropriate, he emphasized. Health care team members need to pay attention to nonverbal cues and the way they communicate expectations. Empathy is vital, as is involving the family whenever possible, including in team meetings. Greater transparency with regard to health care costs is badly needed, he said, and paying attention to individual preferences is paramount. “I think that should be the prime directive for palliative care, and whatever metrics we develop to measure the success of palliative care should account for patient preferences,” said Cagle. To illustrate that last point, he told the story of a patient whose pain was registering 8 on a scale of 10 but did not want pain medication because the pain made him feel alive even though he was dying.
A NURSING PERSPECTIVE4
Ginger Marshall started her presentation with a “connect-to-purpose” story involving a recent clinical encounter during which she and a medical resident met with young woman to discuss treatment goals for her mother, who was unable to make decisions because of confusion she was experiencing. The resident began explaining some of the medical issues confronting their mother, using terms such as hepatic involvement, renal insufficiency, encephalopathy, head CT [computed tomography] consistent with malignancy, and resuscitation. Marshall, whose own anxiety level was rising with each piece of jargon, saw the daughter’s face reflect fear, frustration, and boredom as the explanation continued. The resident finished and asked the daughter if she had any questions, but before she could respond, Marshall asked the daughter if it would be helpful if she summarized a few of the points the resident had made. She explained to the daughter that her mother had colon cancer and it had moved to her liver, and because of that, her liver was not filtering out toxins in her blood as well as it used to, causing her confusion and affecting her kidneys. She also explained the special X-ray that had been done on her mom’s brain and that it had found a new site of cancer.
Marshall then talked more specifically about what her mom would want done if her heart stopped or if she stopped breathing, and she explained that she understood the huge responsibility involved with making those decisions for her mother. Marshall also encouraged her to allow her mother’s voice to speak through her to be able to make decisions, not on what she felt would be best but what her mother would say if she was there with them. When she finished, she asked the daughter if she had any questions and she asked Marshall if she could give the same information to her brother and sister, who would be arriving shortly. Marshall replied she would be happy to, and as she and the resident turned to leave the room, the daughter leaned forward and said to the resident that it was okay for him to be there when her siblings arrived, but that she wanted Marshall to do all of the talking.
Turning to the subject of her talk, she cited Terri Ann Parnell’s definition of health literacy (Parnell, 2015): “The relationship between the skills of persons receiving care or treatment and the professionals or systems that are providing the care and treatment.” She favors this definition because it emphasizes the intersection of how well the patient takes in information with how well that information is delivered. That intersection, she said, is
__________________
4 This section is based on the presentation by Ginger Marshall, National Director of Palliative Care for Hospice Compassus and President-Elect of the Hospice Palliative Nurses Association, and the statements are not endorsed or verified by the Academies.
what enables patients and families to exercise their autonomy in making decisions.
Marshall noted that more than 80 percent of older adults suffer from at least one chronic condition, and nearly 90 percent of deaths involving patients over age 65 are directly associated with one of nine chronic illnesses: cancer, chronic liver disease, chronic lung disease, congestive heart failure, coronary artery disease, dementia, diabetes, peripheral artery disease, and renal disease. Rarely, she said, does she see a patient with only one of these illnesses. Chronic disease is tied to health outcomes, she added, by health literacy because, “If patients with chronic disease are not able to understand what we need them to do to achieve their goals, either because they do not have the ability to understand or we have not done a good job explaining, there will be a significant impact on their health outcome,” said Marshall. Moreover, she added, when a patient’s condition requires palliative care, health literacy also affects autonomy and a patient’s ability to give informed consent regarding what they want and do not want in terms of care.
Nurses, said Marshall, provide patient education and care for a diverse population across the life span in multiple health care environments. As of June 2015, there are close to 4 million nurses working in the United States, with more than 120,000 nurses working in Virginia and the District of Columbia alone (Henry J. Kaiser Family Foundation, 2015). It is difficult, she said, to determine how many of these nurses are working in palliative care or hospice, but the Hospice & Palliative Nurses Association has more than 11,000 members, and approximately 14,000 nurses are board certified in hospice and palliative care, including advanced practice nurses, registered nurses, pediatric registered nurses, and licensed practical and vocational nurses. Hospice and palliative nurses provide care in the acute setting, outpatient clinics, skilled nursing facilities, assisted living facilities, hospice facilities, at home, parish nursing, prisons, and community centers.
A study (Roter, 2000) found that patients recall and understand as little as half of what they are told by their health care provider. Marshall said her expectations are lower, and she tells patients and families that she anticipates they will retain 20 percent of the information she provides them, which is why she repeats information every time she encounters them. The reasons for such poor retention, she said, include the fact that patients and families are often experiencing emotional instability, which can impair information processing (Wittenberg-Lyles et al., 2013a), and that patients and family members may not all be on the same page or there may be family dynamics that prevent consensus. Interdisciplinary team communication and poor communication across the care continuum, which can stretch from the emergency department to a long-term care or hospice facility, also contribute to poor information retention. Nurses, given their frontline
presence in hospice and palliative care, can play a role in alleviating poor information retention and improving patient autonomy by becoming more involved in patient education. Appropriate patient teaching, said Marshall, reflects a patient’s developmental stage, age, culture, spirituality, preferences, and health literacy considerations.
Health literacy, she said, has to become as automatic for nurses as is hand washing. “It would be wonderful if every time we had a conversation with a patient, we would be asking ourselves if we are conveying information and if we are reading the patient correctly that they are understanding things,” said Marshall. She believes that nurses can be on the frontline of watching for jargon and alerting other members of the health care team when their explanations are missing the mark with patients and families. Nurses, she added, can be advocates for health literacy across the entire spectrum of care. In fact, said Marshall, the Hospice & Palliative Nurses Association’s Advancing Expert Care initiative emphasizes health literacy. It has created patient and family teach sheets, many of which are available in Chinese, English, and Spanish, as well as tips sheets for nursing assistants and quick information sheets for nurses that provide brief overviews of diseases that can be shared with patients and families. This initiative also offers online learning courses, and both education and research scholarships in health literacy. Marshall noted that being a member of this association has provided a wonderful opportunity to be mentored in her role as a leader of health literacy in her organization. It also provides resources, such as special interest blogs that she has used as a source of information to help patients. She recounted an example in which she had a patient with a calciphylaxis, a painful wound condition that can accompany renal disease. This patient did not want to take pain medications because she was the household member who balanced the checkbook, so she turned to one of the association’s special interest blogs and learned about topical opioids. With some further research, she was able to provide information to the inpatient pharmacy, which created a topical formulation that took the patient’s pain score from 10 to 3 within 48 hours.
Marshall then described two palliative care programs. The Carolinas HealthCare System’s inpatient, outpatient, and virtual care programs have been able to have all of their patient education material reviewed and approved by the system’s health literacy committee. To improve the cultural relevance of health information and care, the Carolinas system created a website, Culture Vision, that enables any employee to enter, for example, “end-of-life care for patients who are practicing Buddhists” and get information on how to better care for those patients. The Carolinas system has also created a 7-hour compassionate care course, based heavily on the End-of-Life Nursing Education Consortium course, and has educated more than 900 nurses about primary palliative care. Marshall noted that each
member of the Carolinas HealthCare System’s interdisciplinary teams meet in a morning huddle to decide which skill set on the team can best meet a patient’s need for that day.
She then discussed the Hospice of the Western Reserve in Cleveland, which participated in the Family Caregiver Project run by the City of Hope. This 18-month national education pilot project focused on assessing oncology caregivers needs, developing an education program to meet those needs, and then evaluating caregiver confidence and satisfaction. Marshall said this pilot program determined that teaching instrumental caregiver skills, such as how to turn a patient in bed, assess if a patient is in pain, and assist with activities of daily living, improved caregiver confidence by 75 percent. It also revealed the importance of educating hospice nursing assistants to be able to identify a caregiver’s learning type and how to use adult learning principles to teach caregivers essential skills. Through education, hospice nursing assistants have been able to take information developed initially for the caregivers of cancer patients and use it with caregivers regardless of their patients’ diagnoses.
In closing, Marshall recommend that nurses, physicians, and other hospice and palliative care team members receive communication training, and that such training should be extended to all health care providers regardless of their role or specialty. Current materials and resources related to health literacy should be revised to include content related to chronic illness and end-of-life care. She concluded her presentation by reading from a thank-you card that she received when she was director of the University of Utah Palliative Care Service. “Your team answered our questions before we knew we had them,” read the card. That comment, she said, was a sign that health literacy was front and center in the health care team’s interaction and that as a result, she and her team had done a great job in caring for that family. It is messages like this, she said, that do wonders for her after a rough day at the hospital.
DISCUSSION
Yael Schenker started the discussion by referring to Freeman’s comment about needing to nurture the soul and spirit of patients and families and asked the panelists if they had thoughts about how to nurture the soul and spirits of the palliative care team. A simple answer, said Freeman, is to find the things that give meaning to life. “If you like playing golf, go do it. Relax. Do what is necessary to bring peace to yourself,” he said. “It is really as simple as that.” Another piece of advice he offered is to talk about work with colleagues, who understand the trials and tribulations of working with seriously ill patients better than family members. He holds gripe sessions and cry sessions in his office to help staff make it through the
hard moments. “We are but human,” said Freeman. “Do whatever nurtures your humanity.”
Schenker then asked Marshall if she had any ideas about how to work more effectively in teams to extend the impact that palliative care can have given workforce shortages that exist in health care systems. Marshall referred to Freeman’s comment about tapping into passions with regard to letting team members work on tasks that may be outside the boundaries of their professional assignments but for which they have a passion. Incorporate personal goals into team assignments, she added. “We have to think outside the box,” said Marshall.
Cindy Brach from the Agency for Healthcare Research and Quality (AHRQ) asked the panelists to comment more on the inclusion of patients and caregivers in teams, but not as information conduits between family members. Carol Levine said that teams need to do some self-reflection on why they are resistant to including patients and family members as teammates. She believes that one reason is fear—teams are afraid they will not be able to talk about hard things because the patients or family members will get too emotional. Another reason is that teams have no clear picture of what each team member’s responsibilities are, and so there is no clear structure for the team into which patients or family members can fit. She added that patients and family members should have the option, not obligation, to be part of the team, and noted that while there is no I in team, there is a U in team when you are a family caregiver, as in “You do it,” and you get told what to do. “The reason to involve someone in the team is not to give them instructions but to listen to them,” said Brach. “That is part of the culture change we need.”
Marshall made the point that she believes palliative care consulting teams do a great job of incorporating patients and families into the decision-making process. “I have never worked with a palliative care team that makes a plan outside of the presence of a patient or family members, and that does not give patients or family members control over who gets to help with the decision-making process,” said Marshall. As an example, Marshall recounted a case in which she saw a patient in a pulmonary clinic and the social worker who was working with her picked up on the fact that Marshall had missed the patient’s concern that her daughter, who was living with her, would be involved in decision making. “She did not want the daughter involved but was not able to tell her that,” recalled Marshall. The social worker was able to mediate the conflict and start the discussion.
Cagle added that Debra Parker Oliver has used video links in the home to bring caregivers into team meetings so they do not have to leave home but can still participate in the discussion. He noted, though, that the paternalistic settings with strong hierarchies in place in many health care settings can create challenges to including patients and caregivers on teams.
Organizational support from system leadership is essential for creating true teams, said Cagle. “We are seeing many watered-down versions of interdisciplinary teams out there,” he said.
Freeman commented that some health care systems do not value all of the potential members of a team, such as social workers or chaplains. “They do not value those nonreimbursed entities in hospitals,” he said. He also noted that if a health care system does not start engaging every employee—the chaplains, social workers, environmental service people, cafeteria workers, and others—in the holistic care of the entire family, it will sow the seeds of its own destruction because another health care system will do those things.
Steven Rush from UnitedHealth Group commented that the definition of health literacy used for this workshop focuses on getting and understanding information to enable appropriate decisions, and he wondered if there is a role for the palliative care team to help people make appropriate decisions. Freeman replied with a statement that he acknowledged might be controversial: that rather than following the Golden Rule of doing unto others as you would have them do unto you, the paradigm for medical care should be to do unto others as they want done to them. “We have to challenge ourselves to say that we want to give you what you want,” said Freeman. “This top-down hierarchical structure, believing we understand what everybody needs and wants, is a flawed paradigm.” He then recalled a time when Robert Arnold came to his hospital and asked staff how many of them wanted to be on a ventilator—nobody raised their hands. When he asked how many would want to be on a ventilator for 1 week and then be fully recovered and a few hands went up, but when he asked how many wanted to be on a ventilator if it were just for a few hours and then be completely restored, every hand went up. The lesson of this exercise, said Freeman, is that what people want depends on the real circumstances, and to know what they want in a given circumstance requires asking them. “If we do not do a good job of asking, we are just dictating and we have a problem,” Freeman said.
In Marshall’s experience, every time one of her teams gets asked to participate in a consult to assist with a discussion about treatment goals, the reason is that there is a problem with health literacy. She believes that palliative care has a large responsibility to address this issue, but she also agreed with Arnold’s statement that it would be ideal if the palliative care specialty did not need to exist. “Every one of the medical providers should have the ability to recognize when there are challenges involved with understanding.” Cagle cautioned against giving advice to patients and family members based on what they, the team member, would do. “As soon as we start talking about the role of the team in leading patients to make decisions about appropriate care, the question becomes whose definition
of appropriate care,” said Cagle. That decision, he emphasized, has to be centered on the patient. Rush seconded that statement. Freeman recalled an incident where an oncologist told him not to mention death or dying if there was a 75 percent chance of a cure, and his response was that if a patient wants to talk about death and dying, that is what he will talk about with them. Though the oncologist was not pleased then, he has come around to realize that Freeman was right—those decisions are about the patient’s journey, not the doctor’s.
Jennifer Cabe from the Canyon Ranch Institute said she appreciated the “delicious morsels of hard truth from this panel,” and said that one thing that she holds to be true is that health literacy is about advancing self-efficacy and empowerment. “It is a two-way street between the people we call patients and the people we call health professionals,” said Cabe. One idea that has intrigued her is the need to increase public awareness about the concept of pain management. Marshall replied that while she supported that idea, she thought that providers need to be educated first. “Any type of education about pain management to increase their autonomy and help them make good decisions is a wonderful idea, but I think it has to be balanced with educating health care providers about services that may not be available everywhere,” said Marshall.
Cagle thought that it would be difficult to conduct a broad-based public education campaign on pain management but that targeting people who are in pain or caregivers that are caring for patients in pain can be effective. He cited a recent study that he and his colleagues conducted on addressing barriers to pain management and hospice with family caregivers (Cagle et al., 2015). They saw improved caregiver efficacy related to pain and symptom management and improvement in patient pain within 2 weeks after the intervention. “I am optimistic about targeted approaches such as this,” said Cagle. The problem with a larger public education effort is that the information may not be needed for a number of years and is forgotten, “but if you get the people who are dealing with it right then, there are ways to open the door,” he noted.
Jennifer Dillaha from the Arkansas Department of Health’s Center for Health Advancement asked about other disciplines that would be helpful to bring into palliative medicine, and Levine replied that pharmacists need to be involved. It is important, she said, to have someone on the team who truly understands what medications do and do not do, how to prescribe them, and if there are alternate methods of delivering them. In addition, many patients get better information about their medications from pharmacists than they do from their doctors. Cagle said that hospital aides play a vital role in caring for patients and often they develop intimate relationships with patients and family members. He noted his surprise that aides are not heard from more in forums such as this workshop. He
also thought that perhaps someone who is technologically savvy could be part of the team.
Marshall seconded Levine’s statement about pharmacists and said they are often skilled at education and teaching. Another addition might be to have people skilled in complementary medicine disciplines such as acupuncture or Reiki. “It does not matter if as a provider you feel there is a need for that expertise on the team, but it is about what our patients feel they need,” said Marshall. She also remarked that she worries about pushback from hospital administrators who are concerned about the effect on budgets of creating bigger teams.
Michael Paasche-Orlow thought the panelists were being too polite about the dominance that physicians have in creating teams. As a physician, he felt he could state that “there are a lot of people who have power and who are not sharing it.” He noted that one reason that physicians may be reluctant to have patients and family member on their teams is that they will then have to stop using jargon and communicate more clearly even in that environment, not just at the patient’s bedside. He admitted that on occasion he uses made-up acronyms in meetings with his medical colleagues just to see if anyone will admit that they do not know something, and nobody does. “Communication at the team level has to be improved, too,” he said. “There are many hierarchies that need to be unpacked.”
Wilma Alvarado-Little asked the panel how interpreters were used in their teams when patients or families members have a primary language other than English or if they are hearing impaired, and if they were briefed before being in the room with patients and family members. Marshall said that in the best-case scenario, an organization has interpreters available. In her organization, it is standard practice to meet with the interpreter to make sure they have a good understanding of what will be discussed with the patient and family. In smaller communities and in smaller geographically located communities, she added, it is not unusual for those interpreters to know the patients, and in that case it is important to make sure that the interpreter will not have a problem interpreting for someone they know. In the end, though, the mandate is to use interpreters. “It should never be acceptable to have a family member interpret and make them responsible for delivering difficult news,” said Marshall. Brach quickly noted that AHRQ has a curriculum on working in teams with specific modules, including video demonstrations, on how to integrate an interpreter into a team.




















