
6
Health Literacy in
Palliative Care Programs
The workshop’s final session presented four examples of how health literacy and palliative care can be integrated into a successful program. Stacie Pinderhughes, Director of Palliative Medicine at Banner-University Medical Center in Phoenix, Chair of the Division of Palliative Care at Banner Health, and Clinical Associate Professor of Internal Medicine at the University of Arizona, described some of the ways in which health literacy plays out in Banner Health’s palliative care program. Dana Lustbader, Clinical Professor Critical Care and Palliative Medicine at Hofstra North Shore–Long Island Jewish (LIJ) School of Medicine, Department Chair of Palliative Medicine at ProHEALTH Care Associates, and Medical Director of ProHEALTH Care Support, then discussed a program for providing palliative care at home. Anne Kinderman, Director of the Supportive and Palliative Care Service at San Francisco General Hospital and Assistant Clinical Professor of Medicine at the University of California, San Francisco, showed how her service helps patients navigate difficult decisions in the hospital, and Reverend Tyrone Pitts, co-chair of the Interfaith and Diversity Workgroup at the Coalition to Transform Advanced Care, Ecumenical Officer and General Secretary Emeritus of the Progressive National Baptist Convention, and President and Chief Executive Officer of Bridges International LLC, described a faith-based movement to transform health disparities. An open discussion moderated by Marian Grant, a nurse practitioner and assistant professor at the University of Maryland School of Nursing, followed the four presentations.
Grant, while introducing the panel, remarked that the workshop so far had addressed some difficult topics and highlighted some opportuni-
ties for progress. It was her hope that the four presentations would be “little pools of light that will ultimately become beacons and that all of us will work to together to make this type of care more widely available in the United States.” She also acknowledged what she called a “brave move on the part of our government yesterday,” when the Centers for Medicare & Medicaid Services announced that it was going to propose billing codes that would allow providers to bill for advance care planning conversations. Recalling the days when some pundits were raising alarms about death panels, which she considers an example of health illiteracy, she called this announcement the start of a brave new day. “I am hoping that the fact that in the last 23 hours since the announcement was made that we have not heard about death panels is a sign that maybe those days are behind us,” said Grant.
HEALTH LITERACY AND PALLIATIVE CARE IN A LARGE HEALTH SYSTEM1
Stacie Pinderhughes started her presentation with a story about Mrs. W., a 61-year-old Navajo American woman who she met in the intensive care unit (ICU). Mrs. W., who had a history of autoimmune hepatitis, hepatocellular carcinoma, and hepatitis B, was nearing the end of her life and had many of the complications common among critically ill patients in the ICU. Mrs. W. was on dialysis, on a ventilator, and in septic shock, and was so ill that she had been removed from the liver transplant list. The ICU director had called Pinderhughes when the ICU staff had reached an impasse with the family regarding what their goals were for Mrs. W.—the ICU staff thought that Mrs. W. should have a do-not-resuscitate (DNR) order, but the family did not. When Pinderhughes arrived at Mrs. W.’s room, she was struck by how this tiny woman was connected to so much machinery, and she remembered that she did not even see her husband through all of this equipment until she went around to the other side of the bed.
Pinderhughes pulled up a chair, sat down, and introduced herself to Mr. W. and asked him what the best way of honoring his needs were regarding his communication style. For many Native Americans, talking directly about death and dying is taboo, but Mr. W. told Pinderhughes that he wanted her to be direct with him and give him the facts about what was occurring with his wife. First, though, she asked him to tell her
__________________
1 This section is based on the presentation by Stacie Pinderhughes, Director of Palliative Medicine at Banner-University Medical Center in Phoenix, Chair of the Division of Palliative Care at Banner Health, and Clinical Associate Professor of Internal Medicine at the University of Arizona, and the statements are not endorsed or verified by the National Academies of Sciences, Engineering, and Medicine.
about his wife. He said they had been married for more than 20 years and had many children, and she was an independent, vibrant, and easy-going woman who liked having pedicures and manicures. When asked about his faith and spirituality, Mr. W. said that his family believes in the creator, and when asked what he thought was happening to his wife, he paused for a moment and then said it looks like she is dying. After another quiet moment, he told Pinderhughes that his wife had been in another hospital’s ICU 6 years earlier, connected to multiple machines, and the doctor then had told them she was probably going to die, just as they had now. He then said that when people die, they go out into the galaxy, past all the planets and the stars, to be with their ancestors in a place filled with peace and love, and 6 years ago, his wife told him that was where she was, and that when she looked back she saw the earth as a tiny insignificant speck. At the time, her family was holding a ceremony with the tribe’s medicine man and he was blowing an eagle bone whistle, a sacred religious musical instrument used in ceremonies to call the spirits. Mrs. W. told her husband that when she heard the eagle bone whistle, she knew it was not her time to die and she described to him that she then moved rapidly past all of the galaxies and planets to Earth and her body. “That was a very powerful story,” said Pinderhughes. “We were silent for a minute—you cannot fill that space up with words.”
Pinderhughes then said to Mr. W. that it sounds like he needed to go back to the reservation, hold a ceremony for his wife, and blow the eagle bone whistle. Mr. W. agreed, and Pinderhughes told the ICU director what was going to happen and to continue providing critical care in the meantime. Much to its credit, said Pinderhughes, the ICU team supported that decision. A few days later, Pinderhughes was called down to the ICU because Mrs. W.’s room was full of people. When she arrived, she sat down with Mr. W., who told her that they had held the ceremony, blew the whistle, and his wife did not come back. At that moment, the family decided it was time to focus on comfort and dignity measures.
Pinderhughes shared that story because she believes that it illustrates how palliative medicine is a natural fit for health care literacy. “I think the key elements of palliative care service delivery creates an environment that allows health literacy to emerge,” she said. “It is an intervention focused on aligning with patients around their goals and values and what matters most to them.” The conceptual model that she follows, which comes from Diane Meier, is that palliative care is a dedicated team of professionals with different skill sets who spend the time and focus with patients and their family members to make decisions, have a clear picture of a patient’s values, and then create a plan aligned around those values. The application of this model at Banner Health is done through the combined efforts of a large educational team and the palliative medicine team.
Banner Health, Pinderhughes explained, is a large health care system comprising 28 hospitals in seven states, including the recently acquired University of Arizona Health Network. The Banner Medical Group includes more than 2,500 physicians, and the Banner Health Network includes 19 graduate medical education resident and fellowship programs training more than 290 residents and fellows per year. Banner Health views its palliative care program as a systemwide program that operates across all of its facilities, with a high-level executive support and strong support from the organization’s chief executive officer. The program works, she noted, as a dyad partnership with the medical directors of each facility. Banner Health’s vision, added Pinderhughes, is to expand the program’s involvement in inpatient care from 8 hospitals to 12 by 2016 and to expand into the ambulatory setting. Currently, the palliative care program has a home-based program and is creating two large ambulatory programs. It also has a new fellowship residency program that accepted its first two fellows in July 2015.
One area of emphasis going forward is to improve education of providers, and toward that end Banner Health has created a new palliative care clinical consensus group, joining the 22 other consensus groups in the system. These consensus groups, explained Pinderhughes, develop evidence-based clinical practices that affect patient care for the entire Banner Health system. She believes that by working collaboratively with the other 21 clinical consensus groups, the palliative care group will be able to affect health care literacy. Banner Health System Education team, through its patient education resource center, is creating standardized content, written at a fifth grade reading level and approved by a council of community members, that providers can use with their patients. The System Education team is also instructing providers on how to use these materials in conjunction with teach-back methods. Pinderhughes noted that all new registered nurse hires receive teach-back education and that clinical education teams engage all nursing staff with regard to teach-back methods. One result of involving every nurse in health literacy training is that health literacy now starts at a patient’s admission and continues every day until a patient is discharged. “It is an integrated process to ensure that our patients are able to understand and process the information we give them, take it with them from the hospital, and then implement it when they are home and when they are in the community,” said Pinderhughes. In closing, she said the palliative care program has prioritized equipping providers with the tools to deliver primary palliative care in a health literate manner.
A HOME-BASED PALLIATIVE CARE PROGRAM2
For the past year, Dana Lustbader and her colleagues have been creating ProHEALTH Care Support, a home-based palliative care in the New York market. From her experience over the past year of having conversations in the familiar environment of a patient’s living room, with family members and the dog sitting on the couch, she has learned how different it is compared to having the same conversation in the ICU at midnight when everyone is exhausted and stressed. As an example, she told the story of Sarah, a 45-year-old with metastatic cancer, malignant ascites, and pain. Her care is comanaged with the oncology practice, and she still comes into the clinic weekly for intravenous chemotherapy. She also has 10 to 15 liters of abdominal ascites drained weekly, either by the palliative care team or by a home health agency nurse.
Lustbader explained that the ProHEALTH Care Support team is attempting to break down the silos that currently exist in Sarah’s care. The team supports her during her visits to the oncology clinic and provides support to her family during home visits. For pain management, the team uses long-acting opioids combined with short-acting agents for breakthrough pain that Sarah experiences because her oncologist is not comfortable prescribing the high doses of opioids that she requires. They work collaboratively with the visiting nurse to comanage Sarah’s care, such as when she needs additional fluid withdrawn at times when her abdomen is particularly distended. The ProHEALTH Care Support team provides 24-hour-per-day access to either a nurse or a doctor and conducts secure video virtual visits using telemedicine with the patient and her family members. In one instance, Lustbader conducted a virtual visit at night with Sarah and her son to evaluate a leg cellulitis. She prescribed oral antibiotics from a pharmacy that was able to deliver them to the house within 2 hours, protecting Sarah from having to go to the emergency room or urgent care center.
ProHEALTH also has a volunteer department with 15 individuals who do massage therapy, Reiki therapy, or just sit with patients and listen. Sarah, for example, gets Reiki therapy during her chemotherapy from one of the program’s newest volunteers. The goal, said Lustbader, is to have a high-touch model of total care so patients get many touches, not just medical treatments. Her team, she explained, is doctor lean and nurse, volunteer, and social worker heavy.
With regard to advance care planning, ProHEALTH Care Support uses New York State’s Medical Orders for Life Sustaining Treatment (MOLST)
__________________
2 This section is based on the presentation by Dana Lustbader, Clinical Professor Critical Care and Palliative Medicine at Hofstra North Shore–LIJ School of Medicine, Department Chair of Palliative Medicine at ProHEALTH Care Associates, and Medical Director of ProHEALTH Care Support, and the statements are not endorsed or verified by the Academies.
form to document DNR and do-not-hospitalize wishes that allow patients to receive end-of-life care at home. However, they leave all the other boxes on the form blank because they are too treatment specific, often leading to an ineffective serious illness conversation. The MOLST form is put in an envelope and taped to the refrigerator door. The MOLST form is not completed at the initial visit with a patient, unless it is appropriate. She noted that one of ProHEALTH Care Support’s payers wanted every patient to have a signed MOLST form, but she argued against that as it is most useful for people with serious illness in the final year or so of life. “Everyone who died on our program had had a MOLST so they could have their wishes followed,” said Lustbader.
Returning to Sarah’s story, the things that are most important to her are to die at home, never go to the hospital again, and to attend her son’s high school graduation, which she did. Lustbader said that ProHEALTH Care Support has been working with Sarah and her family for 9 months, and not once has she had to go to a hospital or emergency room.
As another example of how ProHEALTH Care Support uses telemedicine in home-based palliative care, Lustbader discussed the case of Mrs. M., a 77-year-old woman with multiple sclerosis who lives alone and is wheelchair bound. Mrs. M. fell and hit her leg on a radiator, went to the emergency department to have it sutured, and 6 weeks later called ProHEALTH Care Support at 10 p.m. when she developed a fever and was experiencing wound pain. Lustbader had a virtual visit with Mrs. M., and by 11 p.m. she had the appropriate antibiotics delivered to her home, with a follow-up home visit by a registered nurse 2 days later. As a result, Mrs. M. did not have to call 911 and did not have to go to the emergency room, which likely would have led to her being admitted to the hospital given her complex medical situation. “She had perfect care and everything was done within an hour,” said Lustbader.
Many of ProHEALTH Care Support’s patients have what she called “the dwindles,” and do not have a hospice-certifiable diagnosis. In fact, if a person has a hospice-certifiable diagnosis, Lustbader or one of her team members has a phone conversation with the patient, reviews the extra layer of support provided by hospice, and recommends that they get hospice care at home. Typically, ProHEALTH Care Support’s patients do not qualify for hospice because they have dementia, two or more chronic conditions, kidney disease, or heart failure (but not with an ejection fraction below 20 percent), or are still getting chemotherapy and other treatments. They have very poor functional status, said Lustbader, and most are homebound.
The ProHEALTH Care Support team comprises Lustbader and 1 other physician, a program coordinator, 5 registered nurses, a licensed clinical social worker, and 10 to 15 volunteers. The reason for the heavy emphasis on registered nurses is that financing is not on a fee-for-service basis but
through a shared savings program with payers that delivers the care people want and need. “Our patients do not need a lot of medical intervention, prescriptions, or tests,” explained Lustbader. “We are available when that is appropriate, and we leverage our technology to have physician expertise overseeing the registered nurses.” She emphasized this is a patient- and family-centered, nurse-driven model of care.
She sees ProHEALTH Care Support’s main job as one of treating people with serious or advanced illness at home and tending to the family caregiver. When she first joined the company 1 year ago, she added a caregiver assessment to the electronic medical record (EMR) that it uses because there was no place in the EMR to assess the 90-year-old wife taking care of the 95-year-old husband, she explained. The team works with the patient’s other physicians or provides total care to the patient, particularly regarding expert pain and symptom management, and it helps patients and families with advance care planning and facilitates hospice enrollment when appropriate through skilled conversations about serious illness.
Each team, or pod, comprises 3 registered nurses, 1 social worker, and 1 physician working with approximately 200 patients, or 1 registered nurse per 70 to 90 patients. Lustbader explained that she goes to great lengths to select the right nurses, several of which are certified hospice nurses. “They love this sort of work,” said Lustbader. ProHEALTH Care Support collaborates with local hospice and home health agencies, as well as with ProHEALTH Urgent Care and community paramedics. It makes heavy use of virtual visits to leverage physician expertise and provide around-the-clock availability.
As an example of the type of collaboration that ProHEALTH Care Support engages in, Lustbader discussed the case of a homebound patient with cellulitis in his legs. Instead of having to bring him into the hospital, his team arranged for him to be taken by ambulance to the interventional radiologist, who placed a peripherally inserted central catheter line for the administration of medication and sent him home. The ProHEALTH Care Support team was then able to administer intravenous antibiotics at the patient’s home for 6 weeks. Lustbader noted their program has been garnering support from community paramedics who are interested in not bringing people who are terminally ill and would rather be at home to the hospital. Working with community paramedics, ProHEALTH Care Support has been able to develop a protocol for resuscitating, treating, and releasing patients in their homes. As an example, she recounted a case where an 87-year-old man with dementia, diarrhea, and dehydration called ProHEALTH Care Support at 9 p.m. because he was dizzy. In a virtual visit that included the responding paramedic, Lustbader was able to order 2 liters of intravenous saline, and by 11 p.m. the man was tucked safely in bed. She noted that it is often much safer to protect people from hospitalization, and keep them at home.
Currently ProHEALTH Care Support’s parent organization, ProHEALTH Care Associates, sees 800,000 patients in the New York metropolitan area, including all of Long Island. She noted that there are no hospitals in this health system, just 32 urgent care centers, ambulatory surgery centers, 260 outpatient clinics, and ProHEALTH Care Support. She explained that ProHEALTH Care Support is targeting the 2 percent of patients that most concern payers in a Medicare Advantage risk-based payment world. The average spend of this top 2 percent is more than $109,000 per year per beneficiary, compared to an average beneficiary spend of $9,100 per year. “We are able to negotiate with payers for a per member per month rate to pay for home-based palliative care,” said Lustbader. “We don’t have to worry about billing because we are getting paid a fixed rate every month to cover this kind of care.” Her program also has eight shared savings programs that will bring in revenues if it can deliver better care more efficiently as measured by reduced hospital admissions and emergency room visits and increased hospice use. In addition, ProHEALTH Care Support receives a small amount of revenue from the limited fee-for-service billing that exists for this type of home-based, high-touch care, though this fee comes nowhere close to covering the cost of the services provided.
Because ProHEALTH Care Support is in a Medicare shared savings accountable care organization (ACO), it is able to get raw claims data from Medicare. This enables it to find the sickest patients who can most benefit from the program. The results from its first 92 clients show that there was a 50 percent reduction in 90-day spend following enrollment in ProHEALTH Care Support, and a 19 percent reduction in emergency department visits postenrollment. In addition, 92 percent of the patients who died were able to die at home, rather than a hospital setting. “We are in a geographic area where dying at home is very unusual,” said Lustbader. “To have a 92 percent at-home death rate is extremely good, and it is a result of our high-touch model. We normalize dying. We don’t medicalize it.”
Lustbader concluded her presentation by noting there are five elements to making a home-based palliative care program work well. It must be family- and patient-centered, and intervention dosing is key. Some patients, for example, are seen once per month, others three times per week. Some need a nurse, others a doctor, she explained. “We dose the intervention based on need, and since we are not a billing machine, we are not doing this in a fee-for-service model,” said Lustbader. Providing around-the-clock coverage through phone consultation and virtual visits is important, and Lustbader said that most of the questions that come in late at night are appropriate. “We want to hear what family caregivers are worried about,” she said, adding that her staff reviews all of the questions that come in overnight to see how they could do a better job preparing family members for what happened late the night before. The last key component is to form
innovative partnerships. “We try to form new partnerships as we break down health care silos,” said Lustbader.
HELPING PATIENTS NAVIGATE DIFFICULT DECISIONS IN THE HOSPITAL3
San Francisco General Hospital and Trauma Center, the place where Anne Kinderman works, is a level I trauma center for the county that cares for anyone at any socioeconomic level in a serious accident. As a result, Kinderman, as a palliative care provider, sees people from the whole spectrum of San Francisco, and even the world, recalling some of the Asian patients she saw who were in an airplane that crashed at San Francisco International Airport. San Francisco General Hospital is also the safety net hospital for the city, providing 80 percent of all charity care in the city and treating a disproportionate number of uninsured and Medicaid patients, with minimal numbers of patients with commercial insurance. It is also the second most ethnically diverse U.S. medical center—in any given month, 140 languages are spoken on the campus.
A large proportion of the immigrants treated at San Francisco General have limited English proficiency, education, literacy, and contact with the medical system, and for many, the U.S. medical system is foreign in terms of how patients interact with health care providers and the way care is compensated. She and her colleagues also see a large number of socially isolated marginalized patients who suffer from mental illness and substance abuse, have limited social supports, are homeless or marginally housed, have limited coping strategies and contact with primary medical and mental health care, are more frequent users of emergency services, and have shortened life expectancies.
What is known about advance care planning in vulnerable patient populations such as these is that low health literacy is associated with less advance directive completion and less certainty about choices, even with targeted interventions, according to research conducted with patients in San Francisco General’s general medicine clinic (Sudore and Schillinger, 2009; Sudore et al., 2010). Latinos and Asians in particular are less certain than Caucasians in choosing their wishes in advance (Waite et al., 2013).
Too often, said Kinderman, providers have the discussion about what patients want at a time when their conditions worsen acutely. The problem is, that is a time when information becomes harder to process and patients
__________________
3 This section is based on the presentation by Anne Kinderman, Director of the Supportive and Palliative Care Service at San Francisco General Hospital and Assistant Clinical Professor of Medicine at the University of California, San Francisco, and the statements are not endorsed or verified by the Academies.
may have a limited understanding of the implications of the choices they are making in the acute setting and at a time when providers are asking for life-and-death decisions with urgency. “This is a tough situation for anyone, but particularly for those who are starting with low health literacy,” said Kinderman.
When seriously ill patients are hospitalized, they experience a culture that is foreign to most people. “We as medical providers forget how foreign the hospital culture is to normal people,” said Kinderman. This is particularly true, she added, for the population of patients she sees at San Francisco General. Almost weekly she hears from one of her Chinese American patients that she is taking too much blood, referring to the morning blood draw for laboratory tests. Patients whose primary coping strategy outside of the hospital is to chain smoke suddenly has a nicotine patch instead, in addition to a horrific diagnosis, and all they want to do is go outside for a smoke. In addition, people in the hospital are often disconnected from primary care and other trusted providers in the community, and they face multiple communication barriers, often because of language barriers. Kinderman noted that the check-in desk at the radiology department has a sign in multiple languages informing patients of their right to have an interpreter present, but the type on the sign is so small that it is unreadable even at a distance of 2 feet.
Other factors that cause confusion in the hospital setting arise from the way physicians interact with patients. Too often, as other speakers have noted, physicians present too much information and they use too much jargon. Patients can be overwhelmed, too, by information from multiple providers, some of which may conflict with the information they get from other sources. Conversations with providers often focus on treatment decisions rather than values, and then when the end of life is near, providers turn over responsibility for decision making to the patient or a surrogate under the guise of helping patients be autonomous and in control of their lives.
These factors combine to produce a great deal of conflict, said Kinderman. From the provider’s perspective, the patient who has low health literacy and is facing life-and-death decisions may come across as quiet or disengaged, ambivalent or confused about their choices because they cannot recall the information dumped on them at an earlier encounter. Rather than dragging their feet about completing advance directives, patients may merely be overwhelmed. From the patient perspective, providers can come across as impatient or applying pressure about different decisions. Providers may seem redundant, repeating the same information again and again, and uncomfortable dealing with patients.
Addressing health literacy in the hospital, said Kinderman, entails a number of communication techniques that optimize conditions and provide
support for decision making and advance care planning. With patients of limited English proficiency, it is imperative to have a professional translator present at the time of a discussion and to pay attention to the vocabulary the patient uses. The interpreter can help with this assessment. It is important to address the impact of culture and beliefs on decision making and care preferences, and to empathize and validate a patient’s concern rather than being antagonistic about it. It is also important to address communication barriers that patients face when voicing their needs in the hospital. As an example, Kinderman cited the case of a Cantonese-speaking woman who does not speak English and is in pain. How does she communicate that she needs pain medication if there is no interpreter on the floor then?
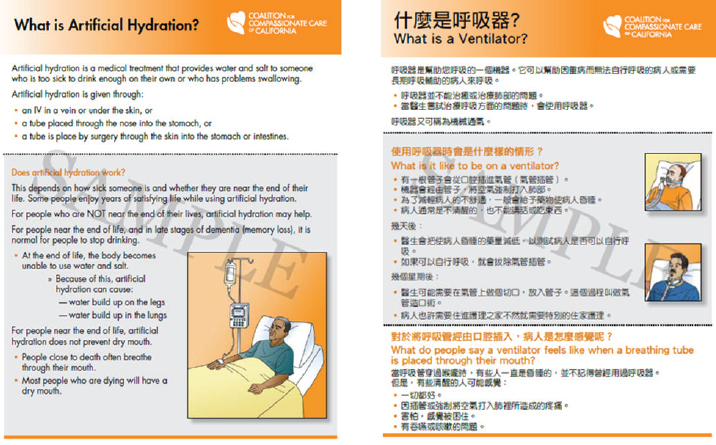
Reiterating what previous speakers had said, it is important in verbal communication to present information in small amounts, check regularly for understanding, avoid jargon and euphemisms, organize provider input so it is consistent and does not cause confusion, and keep patient values in mind. Presenting information in written form can improve communications. Pictures and diagrams can be helpful, but any written material should be available in multiple languages (see Figure 6-1). Patients also need time to review any materials or to have an interpreter read them and review them with the patient.
It is important, said Kinderman, to optimize cognition. Reviewing medications can help make sure patients are not disoriented because of the medication side effects. Ensuring patients have their glasses and hearing aids available is essential when presenting important information, and it can be helpful to have families present but to also control the conversation so people are not talking over one another. Optimizing the patient’s environment by getting the patient on a normal day-and-night schedule can also help improve comprehension.
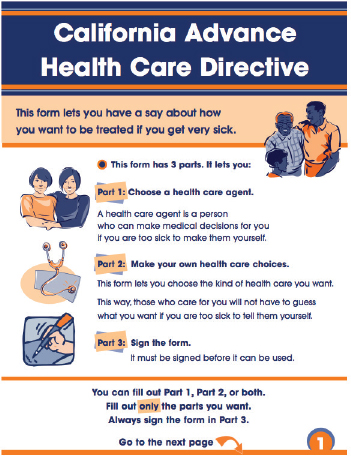
To support decision making and advance care planning, Kinderman recommended involving surrogates, family members, and other caregivers, as well as trusted providers. It is common, she said, for her socially marginalized patients to bring case managers or other trusted community members to appointments. Also, given how uncertain her patients are about completing advance directives, it has proven important to assess the patients’ interests and let them have their way on those, even if they will never fill out an advance directive or a Physician’s Orders for Life-Sustaining Treatment (POLST). She did refer, though, to the California Advance Health Directive developed for patients with low health literacy (see Figure 6-2).
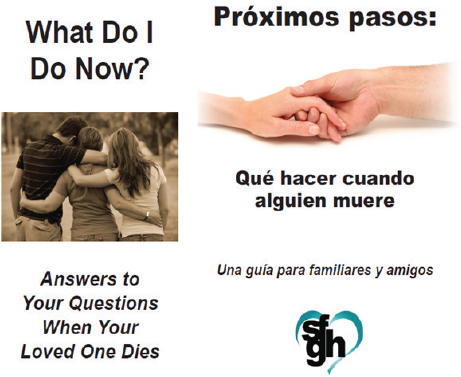
Kinderman concluded her presentation talking about some of the quality improvement initiatives at San Francisco General Hospital. One such effort has focused on providing information to family members about what happens after a patient dies, and to help answer the many questions families have at that moment, the hospital developed a brochure, avail-
SOURCE: Presented by Anne Kinderman on July 9, 2015.
SOURCE: Presented by Anne Kinderman on July 9, 2015.
able in Chinese, English, and Spanish, that is handed out immediately after a patient dies (see Figure 6-3). Another project developed cue cards with words and pictures that communicate basic needs and concerns for patients with limited English proficiency (see Figure 6-4). Kinderman, collaborating with colleague Alicia Fernandez, also developed a curriculum for interpreters in palliative care that is designed to help professional health care interpreters negotiate these difficult conversations among patients, families, and health care providers. The materials for this 8-hour training course are available free at www.chcf.org/interpreting. On-demand access to the curriculum for individual interpreters is available for a small fee at learn.hcin.org.
Kinderman said she has learned several lessons from her work at San Francisco General. “We expect a great deal from our patients in navigating
SOURCE: Presented by Anne Kinderman on July 9, 2015.
the health care system, so pacing of how we share information is critical,” she said. It is important, too, to consider the patient’s emotional readiness to receive information, to adapt communication styles and materials to accommodate the ability of patients to understand and assimilate medical information, and to bring in allies from both the patient and provider side to help with the task of communicating with patients of low health literacy.
A FAITH-BASED MOVEMENT TO TRANSFORM HEALTH DISPARITIES4
Tyrone Pitts began the workshop’s final presentation with the story of a man who insisted he was ill. After many years, he went to his family and
__________________
4 This section is based on the presentation by Reverend Tyrone Pitts, co-chair of the Interfaith and Diversity Workgroup at the Coalition to Transform Advanced Care, Ecumenical Officer and General Secretary Emeritus of the Progressive National Baptist Convention, and President and Chief Executive Officer of Bridges International LLC, and the statements are not endorsed or verified by the Academies.

SOURCE: Presented by Anne Kinderman on July 9, 2015.
his family decided he should see a doctor, and they made an appointment for him. He had a physical examination and was found to be in perfect health. Several years later, he died, but before he died he had his tombstone engraved to read, “I told you I was sick.” This story, said Pitts, highlights the reality that individuals who deal with issues of palliative care and advance directive face. This man insisted that he was sick, but his family did not believe him. He experienced symptoms that his caregivers, those who loved him most, dismissed, perhaps because they thought he was a hypochondriac or because they thought he was suffering from Alzheimer’s or some other mental disorder. There also was a gap between the symptoms he experienced, the tests that were administered, and the diagnosis provided
by his doctors. Perhaps he was poor and did not have adequate health insurance, or perhaps there was a gap in his communication system where he communicated or did not communicate his symptoms adequately, which is often the case with people whose first language is not English and low-income individuals who do not speak the same medical language as their health providers. This story also provides an example of a person of faith who was determined to have the last word, Pitts added, noting the message he had carved on his tombstone. “It highlights the need for trust between person, his family, and health professionals, and illustrates the complexity of communication with people with advanced illness,” said Pitts.
Noting that people often do not receive the care they want and need during advanced illness, Pitts cited the Institute of Medicine report Dying in America: Improving Quality and Honoring Individual Preferences Near the End of Life (IOM, 2014, p. 40) to point out what is needed to close this gap:
Broad engagement of actors in the health care field, social and supporting services sector, as well as the organizations and institutions on which Americans rely for practical assistance, spiritual support, information, and advice.
The Coalition to Transform Advanced Care (C-TAC) was formed to close the gap between what people want and what they get in advanced illness. C-TAC’s vision, explained Pitts, is that all Americans with advanced illness, especially the sickest and most vulnerable, receive comprehensive, high-quality, person- and family-centered care that is consistent with their goals and values and honors their dignity. Powering that vision are more than 120 organizations and leaders who work to empower consumers, change the health care delivery system, improve public and private policies, and enhance provider capacity. He noted when he joined C-TAC 4 years ago, he thought its mission was crazy. “The audacity of a group of individuals saying that they were going to transform advance care in U.S. society is unheard of,” said Pitts. “And yet after being at C-TAC for 4 years, it has become clear that there is a movement afoot unlike any other movement in this nation. A cultural change is happening where individuals and groups of networks across this country are coming together to deal with this issue of palliative care and hospice and advanced care.” This effort, he added, is built on one simple word: trust.
One of the challenges the medical profession faces is how to deal with diversity and race and how to help the most vulnerable members of society. In the African American community, trust of the medical community has been a problem for years because of a history of inappropriate actions, such as the Tuskegee experiments. Pitts then cited something that Albert Einstein said, which is that no problem can be solved from the same level
of consciousness that created the problem. Einstein is also noted for defining insanity as “doing the same thing the same way, again and again, and expecting different results.” C-TAC, he explained, is focusing on building bridges and making connections where none now exist.
One thing that C-TAC has found in faith communities is that clergy, imams, rabbis, and other people of faith are the connecting links between people who suffer from serious illness and palliative care, hospice, and advanced care. “It is the clergy and faith leaders who encourage them to seek these avenues of care,” said Pitts. Fewer Americans are going to church, he noted, but whenever they have a crisis or are sick, they call their religious leaders.
A series of listening sessions that C-TAC held in 2014 with community members, caregivers, and members of the clinical community identified a key question: Even if you have a seat at the table, do you have a say in the care for your community as part of the health system? The problem, said Pitts, is that there are many people who have seats at the table, but they do not have a voice at the table and they are not empowered to participate at the table. High-level findings from the listening sessions included
- There are latent, underused resources that are not well linked between communities and providers.
- Systematic linkages that integrate clinical and community models would yield outcomes aligned with patient goals, such as reducing unwanted hospitalizations.
- American Africans identified their faith-based organization (FBO) as a trusted resource.
- FBOs need training and partners to serve as a link between the health system and the community.
In response to the messages heard in the listening sessions, C-TAC launched a Community Action Project with health systems and community organizations around the country, including pilot projects in Alameda County in California, Detroit, the District of Columbia, and Rhode Island. Each of these pilot projects, explained Pitts, is bringing together health plans, health organizations, and community members, including clergy and other navigators, with the objectives of fostering partnerships between health systems and faith community organizations to fill critical gaps in care delivery, give each partner tools and knowledge, and help extend existing advanced illness management programs to reach underserved people.
So far, said Pitts, six practical insights have come from these pilots:
- Advanced illness is already a priority in churches, and every church that was engaged in a pilot program had an intricate network of
-
individuals working on this issue. The challenge is connecting these networks with the health system and health plans in a way that is collaborative and respects the community.
- Language is important; clergy refers to patients and persons, and talk about healing instead of curing, the vulnerable instead of the sickest of the sick, the beginning of life instead of the end of life. These are not just Christian, Buddhist, Muslim, or traditional African concepts but universal to all humanity.
- It is about the money, but it is not about the money, meaning that there is a need for financial support, but people in these communities are perishing for lack of basic aid and services.
- Like health systems, churches and communities have their own systems, so it is important to engage the community, not just one partner or one church, and to understand the dynamics of the entities within the community.
- This is an intergenerational issue, where grandparents are caring for grandchildren and vice versa.
- Ultimately, shared decision making is based on the South African principle of Ubuntu, or the interconnectivity that says “I am because community is, and community is because I am part of the community.”
Historically, said Pitts, health and healing went together for places of worship, and the opportunity exists to rekindle that connection to the benefit of the most vulnerable in society. He ended his presentation with the comment that this is not a financial issue, but one of capacity and working together. The problem, he said, lies in the disconnection between what faith communities are doing and what health care systems are doing. “No one can do this on their own,” said Pitts. “The good thing is, no one has to.”
DISCUSSION
Grant asked Pinderhughes to elaborate on what she meant when she used the expression teach-back. Pinderhughes replied that teach-back is a procedure used to engage patients around their understanding of their conditions. It involves asking them to recount what they heard regarding instructions for their care once they leave the hospital or clinic. One approach is to ask patients how they would explain to family members how they are supposed to take their medications. “It is about engaging patients daily through the course of their hospitalization so when they leave they demonstrate a true understanding of the consequences of not taking the medication or not participating in a particular treatment and being able to describe that to others,” explained Pinderhughes. Grant commented that
having the patient give information back in a different context instead of just repeating it verbatim was a good approach.
Noting the importance of community voice and participation that Pitts highlighted, Winston Wong asked the panelists how their institutions actively engage community in discussions of how advance care needs to change. Lustbader replied that because her program is not affiliated with a hospital, she and her colleagues have even more incentive to go into the community and bring in community volunteers, massage therapists, and Reiki therapists. They have also begun meeting with local church groups and temples and conducting workshops with the Bikur Cholim, the Jewish organization that visits sick people in the hospital, to give them ideas on how they can help those with chronic conditions who receive care at home. “We are starting to try to give these community groups more ideas of how they could be helpful, because I believe many of them would like to be helpful, they just don’t know how,” said Lustbader. She noted that she and her colleagues have had good success over the past 6 months engaging the temples on Long Island to rally around the critically ill in their communities, Jewish or not.
Pinderhughes said that Banner Health has just started working with various community organizations, particularly senior centers that already have connections with and provide services to the elderly who need help. Kinderman admitted that San Francisco General currently does a terrible job of involving patients in planning. “It is more convenient and easier for us to come up with a solution and then impose it on people,” she said. “It does not work well, particularly when talking about advance care planning. The best example of engaging the community, she said, was the community-wide task force on palliative care that was created in the summer of 2014. The task force was broad based, she noted, and the majority of its members were representatives from community organizations, with some representatives from palliative care providers and hospitals.
Pitts described two models for community involvement that he believes have been successful. In what he called the Tennessee model, hospitals have brought in navigators from churches to serve as the link to their communities. The C-TAC model starts in the community, where there is disjointed expertise, and brings in the hospitals to provide help in how to be organized and use that expertise most effectively. In Oakland, for example, the community and Kaiser Permanente have become equal partners in the process of changing how palliative care is provided, with the University of California, Davis, now conducting an evaluation of this program. Pitts explained that the Oakland project was designed to build a relationship between the clinical community and the larger community, and it started with one pharmacist and one surgeon getting involved with the community.
Cindy Brach said that one of the struggles in delivering the right care at the right time and the right place is developing a payment system that
rewards those providing services. Traditionally, she said, money has not followed the individual through the system of care but instead it has stayed in the emergency department or the hospital. She asked Pinderhughes and Lustbader if they are beginning to show that the services they provide are producing savings that offset the costs of those services, and if they had ideas on how she and her colleagues at the Agency for Healthcare Research and Quality might think about measures of quality for those services given that there is the unfortunate financial incentive to stint on care or engage in gate keeping to reduce financial risk.
Lustbader replied that ProHEALTH Care Associates has relations with payers to deliver home-based palliative care for a per member per month rate and that there are several metrics they must meet, including admissions per thousand members. For that metric, Lustbader looks at preventing avoidable hospital admissions because most of the family members do not want to go to the emergency department in the middle of the night with their 87-year-old parent or spouse. She noted that admissions per thousand members is both a quality and cost metric. A second metric is location of death in the patient’s preferred location, which is most often at home. ProHEALTH Care Associates meets that goal more than 90 percent of the time, she said. Lustbader noted that ProHEALTH Care Associates is developing a first-of-its-kind survey that will enable the patients in its program to rate how well they are doing on pain and symptom management and quality of life, and give caregivers the opportunity to weigh in on the burdens they face and any surprises they encountered.
As she noted in her presentation, Lustbader was able to convince payers to not use a metric for MOLST completion because it is not a good metric for the population her organization serves. “We took that metric out because we are at the table and we have a voice,” said Lustbader. “It is important the people in this room are sitting at the table as the metrics for these arrangements are outlined because we are the ones doing the work and know what to measure.” As an example, one payer in a shared savings program wanted to include a metric that everyone discharged from a hospital has a follow-up appointment at the doctor’s office within 30 days. She argued successfully that if a patient has a bone fracture that the orthopedist has repaired, there is little value in having that patient return to the primary care physician in 30 days. A better metric in that case might be that a medically complex person who is discharged should receive a follow-up phone call within 72 hours and touch therapy within 7 days.
Pinderhughes said that Banner Health is still trying to work out payment arrangements and metrics for its home-based program. For the patients who are members of the Banner Health Network, her service has negotiated a per member per month rate. For metrics, she and her colleagues are looking at completion rates for advance care directives, symptoms in opioid
and bowel regimens, satisfaction scores, and the percentage of patients that transition into hospice and how long they stay on hospice.
Michael Paasche-Orlow asked if health ministries—a recognized team of people who sponsor regular educational events and experiences that promote well-being—can serve as a vector for health literacy work in the palliative care and advance care areas. Pitts said that most faith-based groups have health care ministries and that C-TAC’s model involves, in part, connecting those ministries to the larger health care system. He noted that different faiths have different models for how those health ministries work with the community and the health care system. African American churches, for example, work in hospitals and with individuals who are homebound. Churches that belong to the National Council of Churches have very structured health ministries that belong to a national health ministry network, said Pitts, and the Jewish community has its own unique system for dealing with palliative and hospice care. However, Pitts added, health ministries in other interfaith groups, such as the Bahá’í and African traditional religious groups, are not well connected to the larger community.
Richard Freeman said the challenge is twofold. In his tradition, there is the story of the Good Samaritan, and while the members of his congregation may act like the Good Samaritan, they forget the part about being transformers so the Jericho Road ceases to exist. The Jewish community, he said, has access and the power to make transformational changes more immediately that many of the congregations he works with on matters of social justice lack. What has to happen, he said, is all communities of faith must take an active role in first handling the crisis and then be transformative, which goes right to the heart of the literacy conversation.
Grant noted that in her work as a palliative care nurse practitioner, she has had many amazing experiences in which clergy addressed health literacy issues. In one case, she had a meeting with an African American family that was having a hard time making a decision about whether to provide total parenteral nutrition (TPN) to their loved one, which is an emotional and value-based conversation. The pastor spoke to the family about their church’s tradition of fasting, something Grant said she would have never thought of, and in that context the family was able to come to a better understanding of what would be appropriate in this case. In another example, a pastor to an uneducated family from Appalachia served as a translator of sorts, explaining technical words and concepts in a way that they could understand and believe because he was so trusted. She said she often asks families if they are part of a faith-based community because in many cases, clergy have a credibility and relationship that health care providers will never have with their patients. “When you are talking about discussing life-and-death advance directive decisions, we are the wrong people to have that conversation,” said Grant. “If you are a person of faith,
you have a community that has a point of view on those subjects, and that is the group that is most appropriate to at least consult.”
Ernestine Willis from the Medical College of Wisconsin asked Pitts if he had any thoughts on how to overcome the distrust of the medical system that exists in many underresourced communities, including communities of color and many rural communities. Addressing that mistrust, said Pitts, is one of the major areas of focus for C-TAC, and the organization is tackling it in several ways. One is to develop relationships, a critically important step that explains why Ubuntu is so important to C-TAC’s efforts. He recounted a story of when C-TAC first started working in Alameda County that illustrated the importance of building relationships. A foundation challenged C-TAC to hold a meeting of clergy and they set up the meeting by opening the Yellow Pages and calling all of the churches listed there. Nobody showed up for the meeting. The people who started C-TAC’s pilot instead began working with those in the community that they knew and with whom there was already a relationship and trust and from there built a network that extended throughout the community. They also brought in health partners that had already built trusted relationships with the community, and because there was a shared trust with C-TAC as the bridge, these two groups began to have a dialog and the Alameda County Community Action Project was born.
One of the lessons this program learned regarding trust was that some of the health care organizations in the county were including pastors at the table but only allowing them to make general comments. “They were not included in these institutions’ decision-making process,” said Pitts. Another observation was that there were people in the institutions who did not look like those they were servicing, and so C-TAC has begun to talk about diversity within the institutional structures that are ministering to people. “The health profession is not a service, it is a ministry,” said Pitts, and in that regard, health care institutions need to begin a dialog with clergy and others in the community to talk about issues of language, health literacy, and need, and to build programs that are beneficial to all. In the long run, he added, this will save money and it will save lives. “The reality is if you have fewer people going to the emergency department and better services and more community support that leads to community transformation, what you are doing is not only saving money but saving lives,” said Pitts.
Commenting as an African American clinician, Pinderhughes said, “We talk about the mistrust patients have, but in reality the system has been inherently untrustworthy to these individuals for years. There is a history of systemic inequality and lack of access to care that is not a problem of the African American patient or the Latino patient. It is a problem of institutional racism in America.” In her opinion, clinicians need to acknowledge what she called the elephant in the room—the inequity that exits, the lack
of fairness, the lack of trust—and then go forward. “I cannot fix what has happened, but I can fix what is happening now. I can partner with patients and align around where their values are,” she said.
As a closing comment to the discussion, Freeman applauded Pinderhughes’s personal approach to addressing inequities and then asked his white colleagues to challenge themselves to address implicit bias, to ask themselves to think about the baggage they bring to the table. “Do I see every African American patient as disadvantaged?” he said. “Let’s ask those questions and be honest with our answers.”
This page intentionally left blank.
























