
Chapter 5 gives an overview of the role of strengthening countries’ day-to-day health systems and public health infrastructures in preparing for effective outbreak management and emergency response, also highlighted in Chapter 3. Speakers and participants in this chapter discuss how to best augment existing systems for surge capacity needs during an emergency response. Many participants advised that this strong foundation should be supplemented by having concrete plans for outbreak management and emergency response systems that can be activated quickly, flexibly, and systematically when the need arises. Lamptey of FHI 360 urged the public sector to prepare for potential sector-wide responses that are not limited specifically to infectious diseases. He advised that the entire sector should be ready to respond horizontally to any emerging infections, as well as having the built-in capacity for vertical action. An emergency scenario can impact any country and overwhelm its resources, according to Rubinson, to the extent that the country needs assistance in regaining control. He suggested identifying and formulating plans for multiple common emergency scenarios that countries might experience, including for example, bioterrorism events, natural disasters, or large burdens of death and injury from noncommunicable diseases, taking into account knowledge gained from lessons reexperienced in similar settings.
Campbell explained how early reporting and rapid response early in a disease outbreak can dramatically reduce the number of potential cases and prevent further disease transmission (see Figure 5-1). He posited that increased investment in improved importing and response early in the Ebola virus disease (EVD) outbreak in Sierra Leone could have had meaningful effect on the impact of the disease.
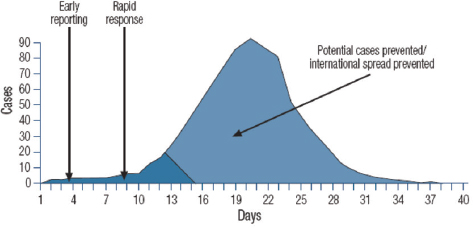
SOURCE: Campbell presentation, August 6, 2015.
Echoing Campbell’s point, Nguku and Nasidi termed this ideal sequence of events in an outbreak where surveillance and response are effective as the “left shift”: the epidemic curve moves to the left, representing a significant reduction in case numbers, morbidity, and mortality when early detection, laboratory confirmation, and response occur within roughly the first 2 weeks of an outbreak. They suggested a set of factors that can contribute to shifting the epidemic curve to the left:
- A functional and effective surveillance and response system (including infrastructure with isolation rooms, ventilation control, soap and clean water, and adequate personal protective equipment [PPE])
- A skilled public health workforce
- A functional and networked laboratory
- Inter-sectoral collaboration
- A strengthened public health system
- Public health funding and leadership
- Effective coordination
OUTBREAK RESPONSE: PRINCIPLES AND STRATEGIES
Perl defined five key elements of health care outbreak response that other speakers commented on throughout this section: outbreak management; care of large numbers of critically ill patients; protection of health care workers, patients, and volunteers; communication with health care workers, patients, families, community members, and public health authori-
ties; and multidisciplinary advanced planning. Outbreak investigation is one of the key components of outbreak management that feeds into quality care and prevention of disease transmission.
Outbreak Investigation
Perl outlined the key components of outbreak investigation. To explain the fundamentals of outbreak investigation and how investigation informs disease transmission prevention, she described her experience as part of a team investigating a 2013 nosocomial, or intrahospital, outbreak of Middle East respiratory syndrome coronavirus (MERS-CoV) at Al Hasa hospital in the Kingdom of Saudi Arabia. The initial focus was on several specific units in the hospital, but after reviewing medical records and collecting surveys it became evident that there was intrahospital spread. The next task was to identify how the infection was transmitted, with human-to-human transmission considered to be the likely source. They created a transmission map that indicated that a single person could transmit the infection to multiple other people (see Figure 5-2).
The next steps were calculating the incubation period (time from exposure to symptom development) and genetically sequencing specimens from
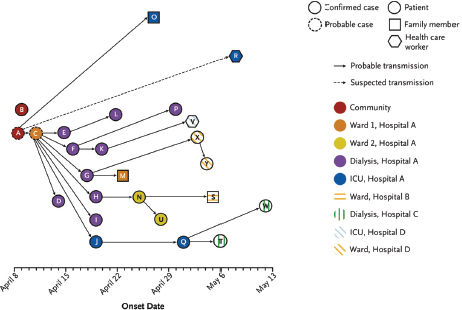
NOTE: ICU = intensive care unit.
SOURCES: Perl presentation, August 5, 2015; Assiri et al., 2013.
infected patients to determine whether the organisms were similar. Sequencing revealed four specimens to be essentially identical, which suggests nosocomial transmission. Thus, the sequencing data are consistent with the epidemiologic data in indicating that transmission can occur from human to human with close contact. Perl noted that bat viruses are very similar to the human MERS-CoV virus that has been identified, and about 3.5 percent of bats in Saudi Arabia have a MERS-CoV-like virus or have evidence of having been infected.1 Similarly, there have been camel MERS-CoV infections with documented transmission to humans. Thus, their investigation suggested that the bat (as with severe acute respiratory syndrome [SARS]) may be the source of the virus, with the camel as a potential intermediary source in transmitting the virus to humans, as was the case in Saudi Arabia. She explained that this aspect of investigation is important because it has implications for infection control and limiting ongoing transmission of a particular organism.
A current challenge faced by outbreak investigations, according to Perl, is that most information about transmission, virulence, prevention, and vaccine effectiveness is still unknown during the investigation. Scientific responses have not been well-coordinated or have not utilized a translational approach with well-integrated and shared data. Available international resources are not effectively leveraged, and international laboratory capacity for testing is still limited. Determining the agent and mode of transmission are only part of outbreak investigation, as Perl explained; it should also serve to find ways to prevent transmission, terminate the outbreak, and prevent future occurrences. She noted that limited surveillance and case finding contributed to the outbreak, due to diagnostic and logistical delays as well failing to detect the spectrum of disease early enough. Poor internal and external communication also played a role, in the form of lack of transparency about the facts of the outbreak within country and to the World Health Organization (WHO). Communications problems also exacerbated what she pointed to as a key factor driving this outbreak and many others: the failure of infection control and prevention practices in health care.
Infection Control and Prevention
Perl stated that the outbreak at Al Hasa hospital was ultimately terminated when appropriate infection control practices were actually put in place, positing that the outbreak likely resulted from failure to adequately implement isolation and infection control measures. Isolation precautions
__________________
1 There has been at least one bat in which the MERS-CoV sequence has been identical to a patient MERS-CoV sequence.
and the use of barrier precautions were not understood or followed2 and the supply chain to support the materials needed for isolation precautions was inadequate. Intrahospital patient transfers led to ongoing transmission of undetected cases, which was also compounded by family visitations and crowding in the hospital. She emphasized the isolation precautions and infection control measures are highly effective when implemented properly, and as such should be a key priority.
Fowler characterized preventing outbreaks from spreading as even more important than the clinical work he performs. He described his experiences as a clinician during the 2013 SARS outbreak in Toronto, during which nosocomial amplification was a major problem. Of Toronto patients with SARS, 77 percent were exposed in the hospital and nearly half of the intensive care units (ICUs) in Toronto hospitals were quarantined, along with more than 1,000 ICU health care workers. Patients are not the only ones whose safety is compromised by nosocomial transmission: multiple participants highlighted the infection risk for health care providers. Campbell noted that health care workers bear the burden of infection, citing data regarding confirmed and probable health care workers with EVD in Guinea, Liberia, and Sierra Leone (880 cases and 510 deaths as of March 2015) (see Figure 5-3).
Fowler reported that 18 percent of SARS patients in Toronto were health care workers as well. He identified three risk factors that contributed largely to health care worker infection of SARS: dispersion of high-flow oxygen (Fowler et al., 2004b); risk to health care workers due to any involvement with intubation (Fowler et al., 2004a); and risk to health care workers ventilating patients with non-invasive positive pressure ventilation or high-flow oxygen (Fowler et al., 2004a).
Ensuring Health Care Workers’ Safety in Disease Response
The importance of practices for ensuring the safety of health care workers responding to an outbreak was raised by multiple participants in the workshop. Campbell urged for protecting health care workers more effectively by providing them with better education and training regarding infection control and prevention. Rubinson similarly highlighted the importance of health care workers’ safety and called for a commitment to disease transmission assessment that drives appropriate protection in terms of procedures, equipment, and training. He underlined the need for clinicians to understand how the disease is transmitted in the health care
__________________
2 She noted that there was confusion about which recommendations for barrier precautions to be used, as the U.S. Centers for Disease Control and Prevention (CDC) and WHO guidelines were not consistent.
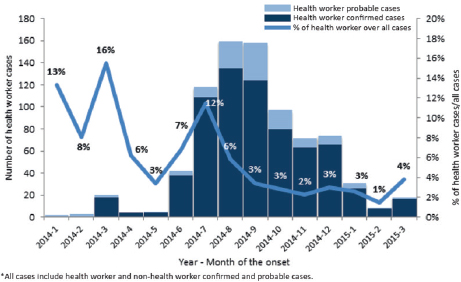
SOURCE: Campbell presentation, August 6, 2015.
setting, cautioning that epidemic surveys alone are not sufficient: a transmission assessment function should be embedded early on in the response to determine whether clinicians are using the appropriate equipment to prevent transmission (such as PPE, intravenous [IV] equipment, and drawing blood). Fowler remarked that the sphere of infection control and prevention extends beyond clinical practice to the domains of social mobilization, community engagement, and dispelling myths and misconceptions. As an example, he cited the sentiment (still common in many areas, but perhaps not as widespread) that EVD is a curse—held even among health care workers—which requires ongoing education to address.
Isolation and Case Management
Norton remarked that of the classic pillars of EVD response—isolation and case management, safe burials, epidemiologic surveillance, contact tracing, and community sensitization—lack of capacity for the first component can consequently impede capacity for the other four components. Aceng described the structure of the case management system in Uganda for EVD, which begins with logistical support in setting up barrier nursing or isolation facilities and ensuring access to safe water and proper sanitation. The system provides triage for patients at health facilities, clinical manage-
ment, and supportive and nursing care. Isolation facilities are set up in health facilities close to the affected communities to minimize the transfer of patients. Families are briefed on the situation of each patient in isolation on a daily basis, with psychosocial experts counseling patients and their immediate families about the natural progression of the disease and the expected outcomes. Burial teams help to ensure safe burial procedures are being followed; homes and properties are disinfected. Further services include offering psychosocial support to patients and relatives, as well as to health workers to help them avoid burnout and depression.
EMERGENCY WORKFORCE CAPACITY: PREPARING FOR SURGES
Norton’s presentation focused on strategies and principles for incorporating global health reserve teams on the ground in times of need. He remarked that surge capacity in public health and clinical response are synergistic and dependent on leadership and coordination by governments. Quality assurance and predictability of surge capacity allows governments and regions to adequately prepare for response; he observed that medical and public health practitioners are only as good as their logistics and operations support mechanisms. Global workforce capacity requires developing national capacities first, he emphasized.
Global Health Emergency Workforce
Turning to the global health reserve teams, Norton commented that response should be predictable, timely, and of appropriate quality to provide support to governments. Existing partnerships require clear mapping and streamlining; response should take into account lessons learned from previous disaster experience to engender an all-hazard approach to emergencies and outbreaks. Both individuals and team formats are required and it is important to understand the effectiveness and value of each. Norton detailed the components of the Global Health Emergency Workforce, comprising national teams (e.g., foreign medical teams [FMTs]); nongovernmental organizations (NGOs) in the form of FMTs as well as through the Global Health Cluster; the Global Outbreak Alert and Response Network (GOARN); the military; and standby partners. The workforce’s objective is to support local health services and help them recover after an emergency, and he suggested finding new ways to shift from a “push” to a “pull” model for assistance, i.e., offering to assist countries rather than waiting for them to request help.
He described how FMTs grew out of the response in Haiti, but were not coordinated or organized well; thus, a new standardized classification for FMTs was established. Type 1 (mobile) are mobile outpatient teams that
can access remote areas (capacity: > 50 outpatients per day). Type 1 FMTs (fixed) are outpatient facilities, with or without a tented structure (capacity: greater than 100 outpatients per day). Type 2 FMTs are inpatient facilities with surgery capability (capacity: greater than 100 outpatients per day; 20 inpatients) and Type 3 FMTs are referral-level care with inpatient facilities and surgery (capacity: greater than 100 outpatients per day; 40 inpatients). Specialist cells are teams that can join national facilities or FMTs to provide supplementary care services, including rehabilitation, surgical, pediatric, and infectious disease specialists. Norton explained that FMTs require four capacities for outbreak response: staff, supplies, space, and systems to coordinate. Key facilitating factors include training; logistics supply; pay; medical care, insurance and evacuation; and Ebola treatment unit (ETU) buildings. Quality assurance (QA) is a priority, and he suggested that the new FMT QA system could be a potential model for QA in other non-FMT public health teams even for more routine threats such as tuberculosis in low- and middle-income countries (LMICs).3
Norton added that the Global Health Emergency Workforce is part of the reform of WHO and the new Emergency Preparedness and Response Platform, incorporating the expansion of current partnerships such as FMTs and GOARN. He described the unified emergency response program as seeking to build energy by strengthening health systems’ resilience and surveillance capacities, developing research and development “blueprints,” and offering field support by delivering district teams using logistics arms.
Strengthening Countries’ Ability to Receive Support
Enhancing a country’s ability to receive international support teams was another topic of discussion. Sarley stated that humanitarian response is important, but if there are robust, resilient, and routine systems in place that integrate all stakeholders, then when experts come in from the outside there is a platform upon which they can work. Rubinson commented that global teams are received by countries but the teams are not always well matched. Appropriate metrics could help to match teams and guide proper responses. He suggested that clinical care, rather than an “afterthought,” should reorganize to be featured more prominently in the response model. Norton suggested that domestically, countries could prepare for the arrival of international teams (e.g., by preexercising or pretraining national teams). Granting the license to practice as a team, he suggested, would make it
__________________
3 After being approved for a new user account and submitting an expression of interest, applicants’ self-declared information is peer-reviewed by a mentor. The organization is preregistered and receives a validation site visit; registered organizations then complete a biannual cycle of validation site visits, virtual validation, and deployment validation.
easier for international teams to be welcomed and absorbed effectively. Campbell remarked that to receive an international support team requires a minimum capacity, understanding, and awareness consistent with the WHO International Health Regulations (IHR).
Strategies for Incorporating Clinicians Effectively in Outbreak Response
Rubinson offered a set of strategies for more effectively incorporating clinicians in outbreak response: “Clinical response is not just about bedside providers.” He argued for the utility of attempting supportive care, remarking that many diseases are survivable with adequate supportive care, so it is crucial to give clinicians an accurate picture of what they will be doing and any information available about whether their care may be helping. Furthermore, he highlighted the need to establish a number of common scenarios that countries can experience, and plan for how to bring teams in effectively. His first recommendation was that clinicians are much less useful without a systematic clinical strategy. Clinicians need to fit into a system: case finding, community outreach, and ETUs must to work together to be functional. He stressed the need to consider data and analysis as more than merely research but as essential to a meaningful outbreak response, differentiating between data used to study diseases and data employed to become more efficient at care delivery.
He reiterated the need for clinicians to understand how the disease is transmitted in particular health care settings, very early in the disease response, and taking the necessary preventive steps (see Box 5-1). In addition to this, clinicians can often act as a frontline surveillance system and
become key resources in early detection and response. This incorporation of disease understanding informs a systematic clinical response strategy comprising short-, mid-, and longer-term functional objectives to ensure that care iteratively improves and appropriate metrics are employed to accurately assess status such as critical mortality, preventable deaths, and system stress. An international cohort of out-of-country experts should ideally be available to consult on clinical problems encountered. Further, he highlighted the importance of assessing the course of the disease and anticipating the resources needed (e.g., the appropriate arrangement of clinicians, support staff, and equipment, and early observations regarding predictors of mortality for triage purposes).
Rubinson’s next recommendation was that responding clinicians should be practicing clinicians until the response is mature, especially given that the distributions of clinicians is heterogeneous and spread throughout the world. Determining whom to deploy can be a challenge, and decisions need to take into account the basic tools necessary to provide care. Early in the event, though, he advised that those deployed should be seasoned clinicians comfortable with acute care, specialists as needed (such as pediatricians4), and mentally and physically fit people who are effective team members.
Rubinson’s final recommendation was that clinicians should train and deploy in teams, with organic nonclinical capabilities, rather than operate as a labor pool. Team deployment offers the advantages of coordinated command and control, logistical independence, and enhanced security and safety. It facilitates standardized functional capabilities, and training together fosters familiarity before the team enters a high-stress environment. Norton suggested the benefits of “twinning” Western clinicians so that when they are ready to deploy to the twinned country they are familiar with the available resources and setting-specific needs and can be as effective as possible.5
Engaging Community Health Workers in Outbreak Response
Panjabi of Last Mile Health recommended professionalizing community health care workers not only for primary care delivery but also for disease response, branding it as particularly critical in the aforementioned
__________________
4 He advised never turning away pediatricians, because of the impact of disease outbreaks on children in affected communities.
5 As Norton explained, “twinning” is a process by which doctors in two or more countries train in each other’s country to prepare for effective foreign deployment as necessary. Training in another country allows a foreign doctor to understand a country’s resources, needs, health system mechanisms, and other elements in order to practice there more effectively. For example, a German clinician may train in Turkey (and vice versa), before deployment to Turkey, allowing him or her to be more effective in practice there.
“blind spots” where zoonoses pandemics can originate and be the most difficult to manage. He described how community health care workers can provide a critical surveillance, preparedness, and response network for epidemics through active case finding, contact tracing, facilitating community trust and education, rapidly identifying and referring patients in need of medical care, and offering prehospital care (Heymann et al., 2015; Ly et al., n.d.; Perry et al., n.d.). Further, they can serve as a link between the community and outbreak response teams, by educating the communities and helping survivors to reintegrate back into their communities. By training them to identify suspected cases, community health workers can then isolate the patient, contact the relevant facility, educate the patient’s caregiver, and keep the community calm. Regarding surveillance and preparedness, he suggested identifying the potential role of community health workers in reserve teams, risk stratification, and decentralizing surveillance from the facility to village level in remote areas (Kenny et al., 2015; Tanser et al., 2006). The objective is determining how to integrate these preparedness functions with everyday service delivery.
INCREASING WORKFORCE CAPACITY IN EMERGENCIES: HIGHLIGHTED OPPORTUNITIES
At the root of most of the discussion on workforce capacity was the concept of task shifting or task sharing. Norton characterized task sharing as “an answer for everything” and recommended increasing sectors of the health care workforce other than physicians, who are expensive. This would involve, for example, finding the appropriate ratio of physicians to nurses, or exploring models run by rural nurse practitioners under remote supervision by a doctor with prescribing rights. Discussion of task sharing also touched on the potential for using alternative technologies such as telemedicine or mobile health for rapid response and diagnosis. Another suggestion made by a few participants was the development of a new cadre of health care providers, such as clinical associates. South Africa employs a clinical associate workforce because the need for doctors exceeded their availability. Others suggested recruiting retired health workers to augment capacity during crisis periods, and devising “crash” training programs to be implemented quickly during times of need to bring the workforce up to basic capacity. Nasidi emphasized the importance of a workforce trained and educated in principles of public health, to both regional and global public health, describing them as “foot soldiers” who have responded to outbreaks worldwide and who are critical to building the system.
In his presentation, Norton outlined several types of individual and teams (other than clinical or FMTs) that could contribute to global surge capacity. Public health individual technical experts could be deployed
through WHO’s GOARN or other mechanisms, coupled with public health teams from national public health services. Logistics teams could provide services, including operations support, health systems repairs or building, and supply chain assistance. Emergency operatives and managers could offer leadership, coordination, and emergency operations center support.
Nguku and Nasidi of the Nigerian CDC outlined some of the features that underpinned Nigeria’s strong EVD response. There was government leadership from the outset through the Nigerian emergency operations center. Community outreach began on the same day as the first diagnosis. There was a comprehensive preparedness plan in place prior to the outbreak, which enabled a rapid response. Multiple sectors were involved, including public–private partnerships. Through Nigeria’s Field Epidemiology Laboratory Training Program (FELTP) program, there was a highly skilled workforce immediately available to carry out a full range of surveillance and response activities. Leung remarked that another sector that is usually engaged only at the last minute is the military, suggesting that the military has useful skills and lessons to offer that should be proactively incorporated during times of peace. However, Fallah warned that military involvement can often inhibit a community’s response, so caution and balance is warranted.
PLANNING EMERGENCY OPERATIONS STRATEGIES
Hanfling of UPMC’s Center for Health Security called for recasting public health to include emergency preparedness and response. This integration would involve thinking about incident management systems with concrete strategies, tactics, and objectives; improvements in public health infrastructure are imperative to achieving this.
Strategic Planning of Operations Around Infectious Disease Outbreaks
Strategic planning of operations around disease outbreaks was a topic of dialogue among participants in the focus area on incorporating global reserve teams on the ground. Campbell reported that participants discussed the importance of the strategic plan being multisectoral, suggesting the integration of clinical care, public health capacity, logistics, information technology (IT), communications, transportation, leadership, traditional healers, NGOs, and civil society. In terms of coordination, he stated that the role of government is central. Operationally, Norton suggested the plan should address the four “Ss” (staff, supplies, space, and systems to coordinate) that are fundamental capacities for FMTs, but often lacking in LMIC health systems—particularly supplies and space. A time-phase resource model would clearly establish the functions that should occur at
which levels at specific times. Partners involved in constructing the plan, reported Campbell, could include (in addition to governments) WHO, United Nations (UN), relevant specialists, academia, and the private sector. Campbell noted that within a country, sufficient national operational capacity and a national emergency operations center are vital resources for constructing the planning of operations.
Campbell emphasized that reinstating national ownership and national decision making in implementing these strategic plans will make a crucial difference in the future in determining when regional or international support is required. Furthermore, understanding how countries formulate, develop, and implement an emergency operations center and coordinate leadership will require actually working through those strategies in practice and in training at the national level. This is how to build the capacities to sustain these systems on a continuing basis. López-Acuña recommended that systems strengthening should be operationalized and supported by concrete performance measurements: rather than referring to “principles, attributes, pillars, or blocks,” planning strategies should distill clear definitions of the functions that are actually being performed and monitored by performance metrics.
Nasidi suggested that time to respond could be improved by repurposing existing emergency response systems or mechanisms for other diseases. Analyzing existing systems, mapping mechanisms, and geographic distributions with the view to how they could be utilized for other diseases could lead to having a set of systems based on a single agenda. Sarley noted that a preexisting, resilient eHealth patient tracking system for polio patients in Nigeria was transitioned for tracking patients with EVD. Audesmore of eHealth Africa mentioned that such systems are also in place in Liberia and Nigeria to track vaccinations, which could be suitable for repurposing.
Models of Emergency Preparedness Systems
Hanfling introduced a framework that is applicable across emerging infectious disease outbreaks, and at its foundation are ethical considerations, as well as the legal authority and environment (see Figure 5-4).
Hanfling stressed the importance of situational awareness—“how do we know what we don’t know”—in response to an emergency event, which requires implementing a process for identifying those unknowns. While Mexico and the United States had a pandemic influenza plan in place from 2004 to 2006, it was developed for an epidemic coming from a distant location, never assuming it may emerge nearby. Further, there need to be cogent processes in place for identifying the appropriate time to move on to the next level of response; implementing clinical processes and operations; and making mid-course decisions. Many emergency plans can be narrative and
administratively focused, but adding flexibility and adaptability in terms of operational models can assist in implementing the plan’s actions to the specific needs.
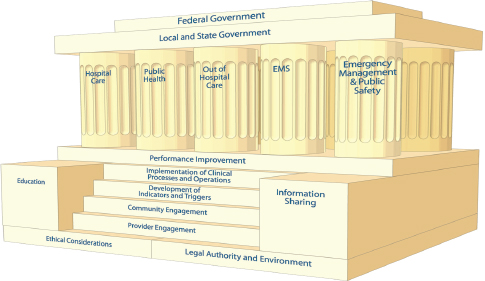
SOURCE: Hanfling presentation, August 6, 2015.
Indicators and Triggers
Hanfling explained that determining indicators and triggers for action are what guide decisions about moving on to the next level of response (IOM, 2013). Indicators are measurements, or predictors, of change in demand for health care service delivery or in the availability of resources. “Indicators” should go through a process of analysis or vetting to develop into scripted triggers and tactics that produce outcomes. “Triggers” are decision points that are based on changes in the availability of resources; they need to be adapted to health care services delivery all along the care continuum.6 According to Hanfling, this requires considering what information about demand and resources is available across the health system, understanding how this information is shared and integrated across stakeholders, determining how this information drives actions, and ultimately
__________________
6 Perl suggested that when dealing with certain pathogens, there can be an element of security that necessitates developing triggers when the good of the people outweighs sovereignty.
deciding what actions might be taken to provide the best health care possible in the particular situation. Many of these indicator measurements could be taken from the various surveillance and information sharing systems described in Chapter 4. The command and control component of the system is tasked with monitoring of indicators and triggers. Hanfling cited and concurred with the recommendation that to facilitate leadership and coordination, “deliberate efforts should be made to identify one agency with the charge to prepare, oversee, coordinate and be accountable for health security actions during a public health emergency” (Salinsky and Gursky, 2006).
Ali Ardalan, Associate Professor and Chair, Disaster and Emergency Health Academy, Tehran University of Medical Sciences, Iran, described the Incident Command System (ICS), a standardized approach to command, control, and coordination that provides a common hierarchy within which responders from multiple agencies can be effective. Its fundamental concepts are unity of command, common terminology, management by objective, span of control, and flexible and modular organization. Structurally, the ICS comprises four subsections: operations, planning, logistics, and finance and administration. Public information officers, safety offers, and liaison officers serve supportive and coordinating functions. He referred to the Infectious Disease Emergency Response Plan in San Francisco7 and CDC’s modified Liberia model (Pillai et al., 2014) as examples of models that are based on the ICS structure; however, he noted as of now, there is no high-level evidence to support or to compare effectiveness and efficiency of different management models for pandemics.
Martineau identified a challenge with respect to the utility of a hierarchical model of control, i.e., the difficulty of communicating certain kinds of insights and information “to the top” in order for effective decisions to be made. He suggested the use of scripted triggers and tactics as well as unscripted ones. Hanfling responded that some “flatter” models do exist, but that they require technology and processes for bringing in information at all levels, synthesizing and analyzing the information, and then using that to influence decisions.
Crisis Management Models in Africa
Hanfling provided an overview of several crisis management models in Africa (Rohwerder, 2015). In 1999, Nigeria created a framework for response at the local, district, and national levels. The framework incorporates an Incident Command System and Emergency Operations Center. He mentioned that in Ethiopia, Kenya, and Niger, the models have a food security focus. Generally, those models involve multiple ministries with different
__________________
7 See http://www.sfcdcp.org/iderplan.html (accessed October 2, 2015).
responsibilities, but limited resources to actually execute their powers. However, he noted that their famine early warning systems serve as good examples of “indicators.” Aceng explained that Uganda has created a national response system, with district and subdistrict levels, that promotes an integrated and multisectoral approach aimed toward continually strengthening the system’s framework and its institutional capacities.
REGIONAL COOPERATION AND CAPACITY SHARING
To maximize resource and capacity management in the long term, all countries do not need to develop full capacities for every service or function if their neighboring countries in the region have existing systems capable of supplementing and supporting them, both during and between outbreaks. Tomori of the Nigerian Academy of Science called for more sharing through regional bodies and international support to ensure that countries build capacity without duplication. Dovlo of WHO also characterized sharing capacities between countries as critically important. For instance, training capacity in some countries could help to close the gap in training for less developed countries. Norton noted that neighboring countries can make a huge difference in terms of timely response and providing the appropriate context and skills; Myers noted similarly that if medical teams are available and on standby, and if a government can trust that the neighboring assistance will actually arrive, then perhaps countries would not need to build up that capacity themselves, and can focus on endemic issues. Another participant remarked that countries with existing services, such as an established training system, could provide a place for countries without existing services to train. Campbell remarked that every country does not necessarily need to have specialist capacity, for example, if its neighbor has a better resource system and has an existing 10-year capacity that is established. He further called for integrating regional capacity and the global international specialized capacity, rather than treating the latter as an international firefighting brigade or a Special Weapons and Tactics (SWAT) team.
Several participants called for regional and national initiatives for capacity sharing of clinical and public health teams and, more broadly, regionally preparing for response and surge-capacity sharing. Leung spoke to the issue of harmonization in supranational efforts, citing as an example the convergence of a new leadership team in the WHO Regional Office for Africa (WHO-AFRO), the U.S. Secretary of State meeting with the African Union commissioner for an agreement about the African CDC, and the subcontinental regional organizations in Africa. He wondered how those groups will effectively work together, if they do at all, and how any overlaps or gaps will be addressed unless there is proper harmonization among them. In that vein, Kimball recognized the West African Health Organization and the African Union as promoting sharing capabilities.
This page intentionally left blank.

















