
2
Understanding Stigma of Mental and Substance Use Disorders
The term “stigma” is used throughout this chapter and the report to represent the complex of attitudes, beliefs, behaviors, and structures that interact at different levels of society (i.e., individuals, groups, organizations, systems) and manifest in prejudicial attitudes about and discriminatory practices against people with mental and substance use disorders. Attention to stigmatizing structures of society, such as laws and regulations, enables examination of prejudice and discrimination against people with mental and substance use disorders. Discriminatory policies and practices can appear to endorse negative social norms and deepen self-stigma.
This chapter offers a brief overview of what is currently understood about stigma, including influencing factors and consequences of stigma from the level of society as a whole to the experience of people with behavioral health disorders. Targets for change and interventions for changing stigmatizing attitudes, beliefs, and behaviors are discussed in Chapter 4.
FINDINGS FROM SURVEYS OF PUBLIC KNOWLEDGE AND NORMS
Public knowledge and norms about people with mental and substance use disorders have been captured through population-based surveys with components focused on the stigma of mental and substance use
disorders as it is reflected in stereotypes, help- or treatment-seeking, and behavioral dispositions.
Results of an analysis of the National Comorbidity Survey-Replication that compared data from the early 1990s and early 2000s showed that stigma associated with mental health treatment decreased, and support among the general public for treatment-seeking increased (Mojtabai, 2007). A survey of states in 2007 and 2009 showed that more than 80 percent of U.S. adults agreed that mental illness treatment is effective; people living in states with higher per capita expenditures on mental health services were more likely to agree that treatment is effective and were more likely to report receiving treatment (Centers for Disease Control and Prevention et al., 2012).
The Substance Abuse and Mental Health Services Administration (2014), as detailed in Chapter 1, found that some common reasons reported for not receiving behavioral health care included inability to afford the cost of care (48%), believing that the problems could be handled without treatment (26.5%), not knowing where to go for services (25%), concerns about confidentiality (10%), that it might cause neighbors or the community to have a negative opinion (10%), that it might cause a negative effect on a person’s job (8%), fear of being committed (10%), inadequate or no coverage of mental health treatment (6% to 9%), and thinking that treatment would not help (9%).
Comparing results of the 1996 General Social Survey (GSS) stigma modules with those of surveys in the 1950s on U.S. attitudes about mental illness stigma showed that public knowledge about mental and substance use disorders increased, specifically as it related to the neurobiological underpinnings of these disorders. There was greater public awareness of the stigma associated with these disorders, but public stigma itself remained high (Pescosolido, 2013; Pescosolido et al., 2010). Results from the 2006 GSS found greater sophistication in the public’s knowledge of disorders and treatment than in the 1996 survey administration, but stigma levels for people with mental illness did not decrease over time (Pescosolido et al., 2010).
Results of the GSS have also shown that the level of public stigma varies along a gradient of social distance. In more intimate settings, the rate of stigma reflected as social rejection was higher, for example, a depressed person to “marry into the family” (60.5% rejection rate) versus the more distant “move next door” (22.9% rejection rate). Stigma against children and adolescents was lower compared to that of adults and also varied with social distance reporting higher rates of rejection for a friend with depression (29%) than for a classmate with depression (11%). One-half of all adult respondents said that treatment would result in discrimination and long-term negative effects on a child’s future (Pescosolido, 2013)
Across countries surveyed in the Stigma in Global Context Study, levels of recognition, acceptance of neurobiological causes of mental illness and substance use, and treatment endorsement were similarly high; however, a core of five prejudice items persisted. The researchers called this the “backbone of stigma”: issues of trust in intimate settings such as the family, potential contact with a vulnerable group such as children, the potential for self-harm, mental illness being antithetical to power or authority, and uneasiness about how to interact with people with mental illness (Pescosolido et al., 2013).
Finally, a review of studies of public stigma of mental illness, which included studies with variables related to substance use disorders, showed that over time the proportion of Americans who endorse neuroscientific views of schizophrenia and alcohol dependence has grown (Pescosolido, 2013). Americans also have endorsed the use of physicians and prescription medication for these disorders in greater numbers and reported being more willing to discuss behavioral health difficulties with family and friends. However, the persistence of core prejudice factors help explain why increased public knowledge has not decreased public stigma. Core indicators of stigma remain higher for people with schizophrenia and substance disorders than other conditions. Further, the highly stigmatizing public perception of violence as a component of mental illness has not decreased over time.
FACTORS THAT INFLUENCE STIGMA
In this chapter and throughout the report, in discussing stigma we begin with structural stigma and work from it to public stigma and self-stigma. This ordering reflects the committee’s views on the relationships among the three levels of stigma and on the importance of addressing structural stigma and its consequences as a means for also reducing public and self-stigma. Societal structures reflect public norms and values, and many of the factors that influence structural stigma are the same as those that influence public stigma. Self-stigma occurs when a person with mental or substance use disorder internalizes negative stereotypes and the public and structural stigma directed at these disorders.
Public perceptions and beliefs about mental and substance use disorders are influenced by knowledge about these disorders, the degree of contact or experience that one has had with people with mental and substance use disorders, and media portrayal of people with mental and substance use disorders, as well as media coverage of tragic events, notably gun violence and suicide (Swanson et al., 2015). Public perceptions are also strongly influenced by social norms concerning the attribution of cause, or blame, for mental and substance use disorders, and
the perceived dangerousness or unpredictability of people with these disorders. Race, ethnicity, and culture are embedded in social relationships and as such play a role in shaping attitudes, beliefs, and behaviors.
Blame
A biogenic model of the origins of mental and substance use disorders has been applied in an effort to reduce blame and promote positive attitudes about the value of treatment and the possibility of recovery. People with substance use disorders are generally considered to be more responsible for their conditions than people with depression, schizophrenia, or other psychiatric disorders (Crisp et al., 2000, 2005; Lloyd, 2013; Schomerus et al., 2011). Belief that a substance misuser’s illness is a result of the person’s own behavior can also influence attitudes about the value and appropriateness of publicly funded alcohol and drug treatment and services (Olsen et al., 2003).
There is a lack of empirical evidence supporting the stigma-reducing benefits of a neurobiological conceptualization of psychiatric illness (Trujols, 2015). Although some research suggests that attributing mental illness to biological causes may reduce the blame placed on individuals for their behavior (Rosenfield, 1997), other research has shown that attributing behavior to a genetic cause can increase perceptions of the difference of people with the disorder, and of the persistence, seriousness, and possible transmissibility of mental illness (Phelan, 2005). Overall, promulgation of the brain disease model of addiction does not appear to have reduced public stigma about substance use disorders and may decrease perceptions of self-efficacy and ability to cope among people with behavioral health disorders (Trujols, 2015).
Stereotypes of Dangerousness and Unpredictability
Americans are more likely to believe in the dangerousness of people with mental illness than are citizens of other developed, industrialized nations (Jorm and Reavley, 2014). In a recent national survey, four in ten Americans believed that children and adolescents with depression were likely to be violent, a finding that may be related to media coverage of school shooting incidents (Pescosolido, 2013). Stereotypes of violence and unpredictability are associated with higher levels of public stigma toward people with mental illness (Martin et al., 2000, 2007; Perry, 2011; Phelan et al., 2000). People with substance use disorders are considered even more dangerous and unpredictable than those with schizophrenia or depression (Schomerus et al., 2011). In a survey conducted in the United States (Link et al., 1997), a vast majority of respondents considered it
likely for a cocaine- or alcohol-dependent person to hurt others. People are less likely to endorse the stereotype of violence if they have had direct contact with people who have mental and substance use disorders and have not experienced violent acts by people with these disorders (Jorm and Reavley, 2014).
Stereotypes of dangerousness can influence public policy in terms of restricting the rights of persons with behavioral disorders (Pescosolido et al., 1999). In the current context of the increasing frequency of mass shootings in the United States (Blair and Schweit, 2013), beliefs about the dangerousness of persons with mental illness and substance use disorders have come to the forefront in public policy debates. To inform these debates, a review of epidemiological findings related to mental illness, gun violence, and suicide found that there is a greater relative risk of violence in people with mental illness than those without mental illness, but the risk is actually very small. The risk of violence is greater for people with schizophrenia, bipolar disorder, co-occurring substance use disorder, and those exposed to certain socioeconomic factors, such as poverty, crime victimization, early life trauma, and a high neighborhood crime rate (Swanson et al., 2015). People with substance use disorders and antisocial personality disorders have a higher risk of violence than people with other psychiatric disorders (Fazel et al., 2009). The risk of suicide, as another form of violence, is increased by concurrent substance use; symptoms, such as hopelessness and depression; psychotic disorders; bipolar disorder; and environmental factors, such as access to guns and media reporting of suicide (Swanson et al., 2015). Swanson and colleagues point to the gaps in the knowledge base on the relationship between behavioral disorders, violence, suicide, and guns, as well as to the gaps in knowledge on effective policies to reduce gun violence and suicide.
Knowledge about Mental and Substance Use Disorders
Knowledge about mental and substance use disorders can positively influence public norms, yet there is evidence that reframing these disorders as brain diseases produces mixed results on people’s attitudes and behavior toward people with mental and substance disorders. As noted above, public education campaigns that frame mental and substance use disorders as brain diseases can have unintended consequences, including increased perception of difference and disbelief in the likelihood of recovery (Pescosolido et al., 2010; Schomerus et al., 2012; Trujols, 2015).
People with substance use disorders, in particular, are viewed by the public as weak-willed (Schomerus et al., 2011) although evidence shows that they are as likely to adhere to treatment as people with other chronic medical conditions, such as hypertension or diabetes (McLellan
et al., 2000). Unfortunately, and in spite of efforts to educate the public, this misperception has increased over time according to the findings from national surveys in 1996 and 2006 (Pescosolido et al., 2010). Media portrayals of people with untreated and symptomatic substance use disorders, rather than depictions of those on a path to recovery, may be a factor in maintaining or increasing negative stereotypes and stigmatizing attitudes and beliefs about people with substance use disorders (McGinty et al., 2015).
Among health care providers, one consequence of bias against mental illness is the misattribution of physical symptoms of illness to concurrent mental disorders (Pescosolido et al., 2008b; Sartorius et al., 2010; Thornicroft et al., 2007), as well as lower rates of referral by primary care practitioners to appropriate physical health services like mammography, cardiovascular procedures, and pain management (Corrigan and Kleinlein, 2005).
Health care practitioners outside fields of behavioral health also lack knowledge about mental illness, and there is evidence that this can lead to misdiagnosis of both mental and physical conditions, and to selection of improper and inadequate treatment regimens (Wang et al., 2002). In addition to knowledge gaps, negative attitudes toward individuals who have mental or substance use disorders are prevalent among health care providers (Meltzer et al., 2013; Van Boekel et al., 2013). For example, although high remission rates for alcohol dependence have been found in population-based studies (Bischof et al., 2005), many health professionals continue to view alcoholism as incurable. In one study, nurses’ self-reported lack of knowledge related to behavioral health was associated with greater reported fear and avoidance of people with mental illness (Ross and Goldner, 2009), demonstrating the link between lack of knowledge and the holding of prejudicial beliefs. Conversely, emergency room staff who reported having skills in treating these disorders held more positive views about the possibility of recovery than those who did not report having these skills (Clarke et al., 2014).
Contact and Experience
People’s immediate social networks and the extent of their contact with people with mental illness affect their understanding of and opinions about mental illness in general (Chandra and Minkovitz, 2006; Corrigan and Penn, 1999). However, increased contact with people with mental illness does not necessarily reduce stigmatizing beliefs, and some studies have found that contact with people with substance use disorders raises the level of stigma (Lloyd, 2013). Among health professionals, negative attitudes toward people with substance use disorders increased over time
during which they would have had more contact with people with those disorders (Christison and Haviland, 2003; Geller et al., 1989; Lindberg et al., 2006).
Several factors may explain why contact with people with mental and substance use disorders sometimes deepens stigma, including the affected individuals’ symptom severity and stage of recovery; and, in the context of contact-based interventions, the quality of the intervention itself, the fidelity with which it was implemented, and the quality of the peer training that had been provided to the individuals offering the contact services. (Peer support services are discussed in greater detail in Chapter 4).
Medical students in Australia reported more positive attitudes about illicit drug users after they experienced contact with them in small-group settings (Silins et al., 2007). In a qualitative study of pharmacists and drug users in a needle exchange program in the United Kingdom, both groups reported a decreased sense of stigma with increasing contact and familiarity (Lloyd, 2013). A review of two similar studies found that college students for whom at least 50 percent of their friends used drugs scored lower on a measure of public stigma (Adlaf et al., 2009). In another study, people who had a family member with an alcohol use disorder reported lower levels of stigma toward alcohol users than those without a diagnosed family member (Kulesza et al., 2013). A lower level of stigma does not imply support for substance misuse; rather, it reflects more positive attitudes toward people with substance use disorders.
Importantly, despite these variations in outcomes, the bulk of available evidence suggests that there is a strong and consistent inverse relationship between contact as an intervention and the level of stigma; more contact with people with mental and substance use disorders is associated with lower levels of stigma related to these disorders. (This topic is discussed in the review of stigma change interventions in Chapter 4).
Media Portrayals
The media provide ideas about and images of behavioral health that influence public attitudes, beliefs, and behaviors toward people with mental and substance use disorders (Edney, 2004; Klin and Lemish, 2008; Nairn et al, 2011; Nawková et al., 2012). An example of the role of media comes from a study of mainstream publications from 1998 to 2008 that covered the topic of postpartum depression and other mental illnesses. The test of communication theories showed that the media’s portrayals helped shape the public’s opinions about postpartum depression and that when the attention given to postpartum depression and other types of mental illness was negative, public opinion tended to mirror negative perceptions (Holman, 2011).
Much of the evidence on the media’s influence on stigma change is negative in direction (Pugh et al., 2015). The media play a crucial role in stoking fear and intensifying the perceived dangers of persons with substance use disorders (Lloyd, 2013). Similarly, media portrayals of people with mental illness are often violent, which promotes associations of mental illness with dangerousness and crime (Diefenbach and West, 2007; Klin and Lemish, 2008; Wahl et al., 2002). Furthermore, the media often depict treatment as unhelpful (Sartorius et al., 2010; Schulze, 2007) and portray pessimistic views of illness management and the possibility of recovery (Schulze, 2007).
There has been some positive change. An analysis of newspaper articles between 1989 and 1999 (Wahl et al., 2002) showed more coverage of issues related to stigma and mental health insurance parity in 1999 than 1989. The analysis also found that there were fewer articles that contained themes of dangerousness and negative tones in 1999 than in 1989. However, even in 1999, articles with themes of danger and negative tones were still more prevalent than positive themes in reported stories that included a focus on mental illness.
Another content analysis of a nationally representative sample of U.S. news coverage of mental health issues found that, in 39 percent of stories, an association was made between persons with mental illness and dangerousness (Corrigan et al., 2005a). Treatment was discussed in 26 percent of stories but only 16 percent of the stories included recovery as an outcome. Moreover, recent research suggests that, given the broad reach of U.S. media, the volume and intensity of negative coverage about mental and substance use disorders are increasing mental health stigma in other countries as well (Jorm and Reavley, 2014).
Studies of new social media, experimental studies, and evaluations of anti-stigma initiatives point to the potential value and capacity of the media to counter stigma. For example, in a study of tweets comparing the use of words that referred to schizophrenia and diabetes (Joseph et al., 2015), researchers found that tweets about schizophrenia were more likely to be negative, medically inappropriate, and sarcastic than tweets about diabetes. But their results also suggested that such public misinformation could also be a target for anti-stigma efforts targeted at young people.
Media reporting of suicide can be stigmatizing through selective reporting on homicides and suicides, especially celebrity suicides, but they can also be platforms for prevention by providing positive messaging about available support and resources, coping, mastering personal crises, and the value of help-seeking (Niederkrotenthaler et al., 2014). One study of social media reactions to an attempted suicide showed that a greater proportion of microblogs expressed caring, empathy, or calling for help (37%) than posts that were cynical or indifferent (23%) (Fu et al.,
2015). More research is needed to identify effective strategies that combine media, education, and support for help-seeking (Niederkrotenthaler et al., 2014).
In an experimental study that compared attitudinal outcomes, researchers found that stories of recovery decreased prejudiced attitudes toward people with mental illness and drug addiction and increased belief in treatment efficacy (McGinty et al., 2015). Australia’s beyondblue campaign, a comprehensive social marketing campaign to destigmatize depression, provides another example of the impact of positive portrayals of mental illness. The researchers assessed changes in attitudes among the general public, controlling for different levels of exposure to the campaign, and found an increase in understanding of depression, awareness of discrimination, and self-reported use of mental health treatment (Jorm et al., 2005, 2006). (The beyondblue campaign, along with other national-scale stigma change efforts is discussed, in greater detail in Chapter 4.)
Race, Ethnicity, and Culture
Sociodemographic characteristics have been found to affect a large number of social beliefs, but when applied to stigma, the research findings are unclear (Pescosolido, 2013). Also important, the effect of sociodemographic characteristics differs depending on whether one is looking at the stigmatizer or the stigmatized person (Manago, 2015). Research is clearer on the relationship between culture, race, and ethnicity, and the quality of care that people receive (Bink, 2015). Ethnic and racial minorities access mental health care at a lower rate than whites, and when they do, the care they receive is often suboptimal (Schraufnagel et al., 2006; Substance Abuse and Mental Health Services Administration, 1999).
Several factors influence access, quality of care, and rates of treatment for mental disorders among ethnic and racial minorities and immigrant groups (Giacco et al., 2014; Schraufnagel et al., 2006). Quality of care is compromised by language barriers and provider misunderstanding of cultural ideas about illness, health, and treatment. Although most health care professionals agree that cultural competency training is important, lack of cultural awareness remains a problem in many health care settings (Giacco et al., 2014). Provision of physical and behavioral health services in integrated care settings has been shown to increase participation in mental health treatment for racial and ethnic minorities (Giacco et al., 2014; Schraufnagel et al., 2006).
CONSEQUENCES OF STIGMA
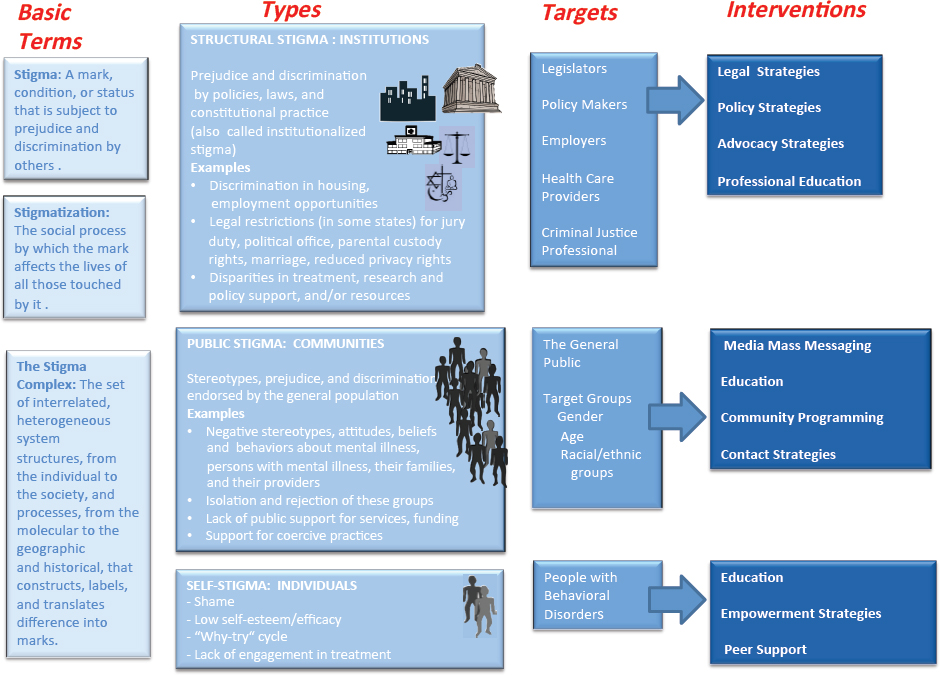
As defined in Chapter 1 and discussed in the introduction to this chapter, there are three distinct types of stigma: structural, public, and self. Figure 2-1 depicts these three main types of stigma and the consequences that result from each, as well as the possible targets for change and interventions that have been used to change stigmatizing attitudes, beliefs, and behaviors. This section reviews the evidence on the consequences of each type of stigma on both adults and children. However, because of the negative impacts of stigma on children and adolescents, we provide a separate discussion about young people with behavioral disorders from the perspective of the public, youth, families, and professionals.
Structural Stigma
Research on structural stigma is still in a developmental phase, and the research that has been done focuses primarily on mental illness rather than substance use disorders. While there is overlap between structural and public stigma, it is possible to define and distinguish between these phenomena. As shown in Figure 2-1, structural stigma is the societal and institutional manifestation of the attitudes, beliefs, and behaviors that create and perpetuate prejudice and discrimination. This section discusses structural stigma using examples of persistent prejudice and discrimination in public and private institutions, including government and legal systems, legislative bodies, employers, and educational institutions; health care and treatment systems; and the criminal justice system, including law enforcement, correctional institutions, and the courts.
Public and Private Institutions
One approach to operationalizing measurements of structural stigma has been through review of policies explicitly targeted at people with mental illness. A review of legislation in all 50 states found legal restrictions for people with mental illness in the following five domains: serving on a jury, voting, holding political office, parental custody rights, and marriage (Burton, 1990; Hemmens et al., 2002). A similar review of nearly 1,000 mental health-related proposed bills in 2002 found that 3 percent restricted liberties (e.g., allowed compulsory community treatment); 1 percent were discriminatory (e.g., restrictions on gun ownership, parental rights, placement of mental health facilities); and 4 percent reduced privacy (e.g., permitting disclosure of mental health information in special circumstances) (Corrigan et al., 2005b).
Although the National Alliance on Mental Illness (NAMI) described
many states’ mental health systems as being in disrepair, their report on state legislation in 2014 documented increased activity on mental health issues. For example, in seven states, legislation was enacted to protect the rights of individuals who are civilly committed, to clarify and improve civil commitment proceedings, and to encourage community-based court ordered treatment (National Alliance on Mental Illness, 2014).
Ironically, although much attention focuses on the dangerousness and violence of people with mental illness, numerous studies have found that they are at higher risk of victimization (Choe et al., 2008; Desmarais et al., 2014; Khalifeh et al., 2015; Wolff et al., 2007) and of experiencing unfair treatment by authorities when they attempt to report crimes than people without mental illness (Pettitt et al., 2013). Poorer legal outcomes are also observed among plaintiffs with mental illness in employment discrimination suits in comparison with plaintiffs without mental illness (Swanson et al., 2006).
People with mental illness are more likely to experience housing and employment discrimination and homelessness than people without mental illness (Corbière et al., 2011; Corrigan and Shapiro, 2010; Corrigan et al., 2006b). Two overt and well-documented manifestations of structural stigma (Callard et al., 2012) against people with mental illness are segregated housing, some resembling psychiatric institutions (Byrne, 2000; Melnychuk et al., 2009; Metraux et al., 2007; Riley, 2011), and community-wide rejection of mental health facilities (Not-in-My-Backyard) (Piat, 2000). Some supported housing programs also have strict rules that people with mental illness must observe to maintain housing assistance, including prohibition of family or visitors, and mandatory compliance with program requirements or medication regimens (Riley, 2011; Schneider, 2010).
People with mental illness are more likely than others to be counseled to accept a job for which they are overqualified (Wahl, 1999), and they often face increased scrutiny by social workers, educators, physicians, family court administrators, and child protective services personnel (Dolman et al., 2013; Jeffery et al., 2013). On a positive note, NAMI’s 2014 review of state legislation found examples of states addressing housing discrimination by enacting rules prohibiting homeless and emergency shelters from refusing services to persons with mental illness and providing funds for home ownership to families of children with disabilities. The NAMI report also documented efforts in some states to increase funding for or make other improvements to supported employment programs (National Alliance on Mental Illness, 2014).
In the arena of higher education, the Americans with Disabilities Act (ADA) and other federal disability laws prohibit discrimination against students with psychiatric disabilities and require that colleges and univer-
sities provide them with reasonable accommodations, for example, lighter course loads and extended deadlines. Unfortunately, in U.S. universities, fewer than one in four students with a mental illness will seek treatment or other supportive services (Downs and Eisenberg, 2012). A study of factors that inhibited disclosure of mental illness found these included a high level of self-stigma, fear of future discrimination, having few positive relationships, and sexual minority and Caucasian identity. Previous contact with mental health service users and belief in the effectiveness of treatment were associated with greater likelihood of disclosure and help-seeking (Downs and Eisenberg, 2012).
Another recent survey of campus experiences showed that college students with mental illness reported less social engagement and fewer relationships on campus than the general population, and felt that they were treated differently most of the time. These factors were, in turn, associated with lower graduation rates than the general student population (Salzer, 2012). Research that targets younger populations indicates that earlier experiences have already winnowed down this population, documenting reduced high school graduation rates and lower application rates to higher education (McLeod and Kaiser, 2004). Even when students with mental and/or substance use disorders do seek treatment, they often receive inadequate services, experience delays in obtaining supportive services, face segregation from other students, and receive harsher academic discipline than other students (Livingston, 2013; Losen and Welner, 2001; Skiba and Peterson, 2000; Wald and Losen, 2003).
Although much of the research discussed above referred to people with mental illness, people with substance use disorders also experience structural discrimination in many forms. A national survey of people in recovery from alcohol and drug problems and their families (Hart Research Associates, 2001) documented barriers to treatment, such as lack of insurance and trouble obtaining insurance, the cost of treatment, and lack of access to treatment programs. They also reported fear of discrimination at work and previous experiences of being denied a job or promotion. Despite the hurdles people with substance use disorders face, the implementation of legislation such as the ADA and awarding of federal disability benefits can be more restrictive for people with substance use disorders than for those with mental illness (Join Together, 2003).
Health Care and Treatment Systems
Stigma in the U.S. health care system contributes to disparities in funding for research and treatment of mental disorders in comparison with physical disorders and to the negative attitudes, beliefs, and behaviors of health care professionals toward people with mental and substance
use disorders. Structural stigma is manifested in the health care system in the low quality of care for people with mental and substance use disorders and the limited access to behavioral health treatment and other services (Institute of Medicine, 2006; Schulze, 2007; Schulze and Angermeyer, 2003); a fragmented bureaucracy for accessing behavioral health treatment; overuse of coercive approaches to care; and inadequate funding compared with that for physical care (Heflinger and Hinshaw, 2010; Institute of Medicine, 2006; Schomerus and Angermeyer, 2008; Schulze, 2007; Schulze and Angermeyer, 2003).
Parity laws for mental and substance use disorders in the United States have become a cornerstone for efforts to combat the structural inequity of behavioral health coverage versus physical health coverage and to eliminate or reduce coverage restrictions so that behavioral health benefits equate with benefits related to physical health services (Hernandez and Uggen, 2012; Sipe et al., 2015). States with behavioral health parity laws have higher utilization of services among people working for small employers and those in low-income groups (Busch and Barry, 2008). Unfortunately, increased access to care does not necessarily mean increased access to high-quality care or evidence-based treatment.
Recent efforts to address structural stigma in the health care system through parity laws have been accompanied by evolving public attitudes regarding behavioral health in the United States. A 2015 Harris Poll found that close to 90 percent of U.S. adults surveyed considered their mental health and physical health to be equally important, but 56 percent reported that physical health is treated more importantly than mental health in the current health care system, and almost 33 percent thought there were barriers to mental health care in terms of accessibility and cost. In a 2013 survey, 76 percent of adults thought that all health care plans in the United States should be required to include coverage for mental health care (Moniz et al., 2014).
Structural stigma may also be reflected in the de-prioritization and lower levels of funding for behavioral health services and research compared to general physical health services and research, despite the high prevalence of these disorders in the United States and evidence of comparable return on investment (Kelly, 2006; Mark et al., 2014). Research on mental and substance use disorders receives less scientific funding than on physical health conditions (Aoun et al., 2004; Brousseau and Hyman, 2009; Fineberg et al., 2013; Livingston, 2013; Pincus and Fine, 1992). Inadequate investment in behavioral health services research also reduces the availability of evidence-based services, especially in facilities that provide care to the safety net population (Cummings et al., 2013). Quality measurements of behavioral health care amount to only a fraction of physical health care measures, and many are narrowly focused, poorly defined,
or lacking in evidence, validation, and meaningfulness (Kilbourne et al., 2010).
Low reimbursements are a factor contributing to the small percentage of psychiatrists who accept insurance (Bishop et al., 2014) and to the persistence of areas with shortages of mental health providers (Cummings et al., 2013). Even with the availability of providers and insurance coverage, insurance benefits have traditionally been more prohibitive of behavioral health services than physical health services, for example, by imposing constraints such as higher deductibles or requiring patients’ mental health status to deteriorate before treatment coverage is allowed (Angermeyer et al., 2003; Corrigan et al., 2004a; Livingston, 2013; Muhlbauer, 2002).
Criminal Justice Systems
Structural stigma is apparent in several areas related to the criminal justice system. The disproportionate representation of people with mental illness with criminal justice involvement (Angermeyer et al., 2003; Corrigan et al., 2004b; James and Glaze, 2006; Livingston, 2013; Muhlbauer, 2002; Sarteschi, 2013) and their treatment within the criminal justice system may be indicators of how criminal laws are designed and enforced in such a way as to differentially target and adversely affect people with mental illness. Nationally, more than one-half of jail and prison inmates in 2005 had mental health problems (Angermeyer et al, 2003; Corrigan et al., 2004b; James and Glaze, 2006; Livingston, 2013; Muhlbauer, 2002; Sarteschi, 2013; Teplin et al., 2005). Incarcerated individuals with mental illness were more likely to have experienced multiple arrests and incarcerations, and only one in three people with mental health problems in prisons and less than one in five of those in jails accessed treatment since their imprisonment. Most U.S. states have more people with mental illness in prisons or jails than in state-operated psychiatric hospitals (Torrey et al., 2014).
To counter these trends, 11 states passed legislation in 2014 to halt the inappropriate flow of people with mental illness into the criminal justice system. Strategies included, for example, increasing training programs for law enforcement officers, examining arrests of people with mental illness and developing diversion programs, addressing court systems responses to people with mental illness, and establishing county-level mental health courts (National Alliance on Mental Illness, 2014). In 2004, Congress authorized the Justice and Mental Health Collaboration Program through the Mentally Ill Offender Treatment and Crime Reduction Act. It is a grant program to help states, local governments, and tribal organizations improve responses to people with mental illness in the criminal justice system through collaboration of efforts among the
criminal justice, juvenile justice, and mental health and substance use treatment systems. Reauthorized for an additional 5 years in 2008, the act was expanded to address law enforcement responses (Council of State Governments Justice Center, 2015).
In corrections systems, whether prisons or jails, people with mental illness are more frequently abused by staff and inmates (Human Rights Watch, 2015; Wolff et al., 2007); more likely to receive sanctions like solitary confinement (Cloud et al., 2015; James and Glaze, 2006; Subramanian et al., 2015); given longer sentences; and more often denied parole (Livingston, 2013) than inmates without mental illness. While under community supervision, people with mental illness experience more intense supervision and face a higher likelihood of receiving technical violations than others under supervision even though the rate of new offenses is similar between people with and without mental illness (Eno Louden and Skeem, 2013).
The complex relationship between substance use and criminal behavior is beyond the scope of this report. However, in terms of structural stigma, it is important to note that institutional policies that treat substance use disorders primarily as a criminal issue (e.g., the U.S. war on drugs) rather than a health concern have promoted a stigmatizing environment that excludes and marginalizes people with substance use disorders (Bluthenthal et al., 2000; Inciardi, 1986; Livingston, 2012). Anti-drug messages and harsh criminal sentences for drug use appear to label people with these disorders as unwanted by society (Rivera et al., 2014). Thus the social processes designed to control substance misuse may actually promote its continuation by increasing shame (Livingston, 2012) and deepen the public and structural stigmatization of this population.
Public Stigma
Public stigma refers to the attitudes of the general public and also to attitudes of subgroups, such as first responders or clergy that may have norms that differ from the general public or other social groups. Public stigma persists in part because structural stigma in the form of laws, regulations and policies appears to endorse prejudice and discrimination against people with behavioral health disorders. A recent systematic review (Parcesepe and Cabassa, 2013) identified 36 articles published over the last 25 years that reported on results from population-based studies of public stigma in the United States. Many of the articles were secondary analyses of findings from national surveys, including the National Comorbidity Survey-Replication and the GSS’s National Stigma Studies. These surveys examined public stigma toward people with a broad array of disorders, including adults with depression, schizophrenia, alcohol or
drug dependency and children with depression, attention-deficit hyperactivity disorder, and oppositional defiant disorder.
The results of this review, confirmed by other researchers, indicate that public stigma leads to social segregation as well as diminished self-efficacy in people with mental and substance use disorders (Corrigan and Shapiro, 2010; Parcesepe and Cabassa, 2013; Pescosolido et al., 2007). Stigmatizing beliefs about the competency of people with mental illness compromise these individuals’ financial autonomy, restrict opportunities, and may lead to coercive treatment, such as mandatory participation in treatment (Corrigan and Shapiro, 2010; Pescosolido et al., 2007). Despite the importance of social support for the recovery of those with substance use disorders, stigma instead contributes to social exclusion (Room, 2005). Also of importance, stigma may affect not only the substance user but his or her family members and friends as well (Corrigan et al., 2006a). Over time in both the United States and other countries, knowledge about mental and substance use disorders is increasing, but issues related to social exclusion also remain high (Pescosolido et al., 2007, 2010).
Self-Stigma
As people with mental and substance use disorders become aware of public stigma and of related discriminatory practices, they internalize the perceived stigma and apply it to themselves. The effects of self-stigma include lowered self-esteem, decreased self-efficacy, and psychologically harmful feelings of embarrassment and shame. Low self-esteem and low self-efficacy can lead to what Corrigan refers to as the “why try” effect, meaning why should a person try to live and work independently if he or she is not valued (Corrigan et al., 2009a).
Among people with mental and substance use disorders, low self-efficacy is associated with failure to pursue work or independent living; a greater degree of self-esteem is associated with goal attainment (e.g., symptom reduction, financial and academic problems), quality of life (e.g., satisfaction with work, housing, health, and finance), and help-seeking behavior (Corrigan et al., 2009b). A substantial body of research has shown that there is a negative relationship between stigma and help-seeking (Clement et al., 2015; Corrigan et al., 2014). Self-stigma can also be a barrier to recovery and community integration.
People who have disclosed their experiences report lower levels of self-stigma (Chinman et al., 2014). In a systematic review of research published between 1980 and 2011 examining associations between mental health-related stigma and help-seeking for mental health problems, Clement and colleagues (2015) found that stigma related to fears about the consequences of disclosure was the fourth highest ranked barrier to
help-seeking. Members of racial and ethnic minorities, youth, men, military service members, and health professionals were disproportionately deterred from seeking help by fears of being stigmatized. In addition, the level of public stigma shaped both reported experiences of stigma, self-stigma, and an unwillingness to use services (Evans-Lacko et al., 2012a; Mojtabai, 2010).
Stigma against children and adolescents is a serious concern because of its negative impacts, including decreased feelings of self-worth and willingness to enter treatment, and because of the deleterious long-term effects of untreated mental or substance use disorders. Compared with the adult population, stigma against children with mental disorders is less well studied. A 2010 review of studies of stigma related to childhood mental disorders concluded that stigma research lacked conceptual underpinnings and that the evidence base was quite sparse (Mukolo et al., 2010).
The National Stigma Study-Children, which was the first to include a nationally representative sample of participants to examine public stigma of childhood mental disorders specifically focused on attention-deficit/hyperactivity disorder (ADHD) and depression, comparing public attitudes and knowledge of these disorders with asthma or “daily troubles.” One set of analyses showed that 81 percent of the adult sample perceived children with depression to be dangerous to themselves or others, compared with children who had asthma or “daily troubles” (Pescosolido et al., 2007). A smaller but substantial proportion (33%) also perceived children with ADHD to be dangerous. Large proportions of the sample thought that children and adolescents with mental health problems would likely experience rejection at school (45%) and would experience stigma into adulthood (43%). Many respondents also had negative views of the benefits of medication (Pescosolido et al., 2007). The researchers concluded that some public beliefs about mental illness and treatment were based on a lack of accurate information and could present barriers for providers and for parents and others who seek treatment (Pescosolido et al., 2008a).
A growing body of research focuses on young people’s subjective experiences of stigma. Interviews with 56 adolescents in a midwestern U.S. city found that 62 percent of youth experienced stigma with peers; 46 percent reported feeling stigmatized by their families; and 35 percent reported experiencing fear, dislike, avoidance, and underestimation of their abilities by school staff (Moses, 2010).
In a study of 40 adolescents taking psychiatric medication for a diagnosed mental illness, 90 percent reported experience of at least one stigma construct of secrecy, shame, and limited social interaction (Kranke et al., 2010). The study also found that adolescents’ perceptions of the norms of family members and school environments can increase their experience of
stigma or protect against it. Results of a large study of youth in Australia suggested that using accurate psychiatric labels reduces stigma and may assist youth by reducing perceptions of weakness (Wright et al., 2011).
The Web-based Injury Statistics Query and Reporting System (WISQARS™) shows that suicide is the second leading cause of death among young people in the United States aged 15 to 34 years (Centers for Disease Control and Prevention, 2015). There is strong evidence that stigma is an impediment to help-seeking on the part of young people and their families. Studies of family engagement in treatment have provided insight into how stigma poses barriers to care. A review of 12 qualitative studies in the United Kingdom on factors that facilitate or inhibit access and engagement in parenting programs for children with disruptive behavior problems pointed to factors directly or indirectly related to stigma (Koerting et al., 2013). Stigma was one of the factors that emerged as a prominent barrier to service from the perspective of both parents and professionals. In these studies, stigma was manifested as shame about needing help, perceived parental failure, and fear of being labeled. Lack of information and lack of awareness about services were also major barriers to accessing care. Mainly from the professionals’ perspectives, one of the main facilitators of access was effective advertisement and service promotion using media, such as leaflets or posters in locations visited by parents, promotion on the internet, local newspapers, radio stations, newsletters, and parenting forums.
TARGETS AND INTERVENTIONS TO ADDRESS STIGMA
In subsequent chapters of the report, the committee reviews the evidence on the effectiveness of stigma reduction interventions and approaches. In this section, we provide an overview of the potential targets and interventions that emerged from the committee’s examination of the factors influencing each type of stigma and its consequences. Figure 2-1 illustrates the relationships among consequences of stigma at various levels and potential targets and interventions to reduce stigma at each level.
As shown in Figure 2-1, targets of structural stigma would include legislators, institutions, and policy makers of systems and organizations that fund and regulate the places and situations where discrimination, lack of opportunities, and lack of access to quality treatment persist. The interventions that would be appropriate for this level are legal, policy, advocacy, and professional education strategies. Strategies would be aimed at changing decision-making processes, policies, and regulations that support discrimination against people with mental and substance use disorders.
Targets for interventions to reduce public stigma include the general public and landlords, employers, health care providers, and groups within the criminal justice system. The corresponding interventions would be aimed at changing behaviors and interactions from discrimination, fear, neglect, and sometimes abuse to extending support, high-quality treatment, and equal opportunities for housing, employment, and personal success. Examples of such interventions include use of media for mass messaging to dispel myths regarding behavioral health disorders and treatment, education to counter the lack of knowledge about disorders and treatment, contact with people with behavioral disorders, and protest strategies against discrimination.
The general effects of self-stigma and the “why try” effect may be diminished by interventions that target individuals with behavioral disorders. As shown in Figure 2-1, such interventions would focus on promoting self-esteem and self-efficacy; empowerment through peer support, mentoring, and education to dispel myths and increase social and coping skills; and education to encourage treatment engagement (Corrigan et al., 2009a). Treatment engagement is significant because evidence-based treatments have been shown to facilitate recovery by promoting behaviors, such as symptom monitoring, continuing to take prescribed medications, and seeking out supported employment opportunities; and by encouraging family interventions, increasing skills related to illness management, and promoting entry into integrated treatment for mental and substance use disorders (Corrigan et al., 2009a, 2009b, 2014). For many individuals, disclosure may be an initial step in the process of reducing self-stigma when it can be done in a safe and strategic manner (Bos et al., 2009; Corrigan and Rao, 2012).
Chapter 4 will review the growing evidence base on the effectiveness of these types of intervention strategies as approaches to reducing stigma at each of the major levels.




















