
2
Current Knowledge and Status of Nutrition Practices in
Oncology Outpatient Care1
OVERVIEW
In Session 1, moderated by Cheryl Rock, speakers provided an overview of nutrition issues that individuals face during cancer treatment and as cancer survivors. First, Mary Platek discussed nutrition issues facing individuals in early oncology treatment. Early oncology care includes patients undergoing active treatment and patients recovering from treatment. Platek highlighted challenges created by nonstandardized screening for cancer patients at nutritional risk and the lack of available nutrition services in outpatient settings; provided an overview of the effects of cancer on nutritional status, the effects of treatment on nutritional status, and the effects of nutritional status on treatment and clinical outcomes; and discussed her search of the scientific literature for evidence of nutritional intervention in early oncology care. She concluded that overall findings indicate important roles for both nutritional counseling and nutritional support in improving clinical outcomes.
Rock addressed many of the same nutrition issues that Platek discussed, but in the context of long-term oncology care among cancer survivors. Because of the aging U.S. population and other factors, the past 30 years have seen a remarkable increase in the number of cancer survivors living post-treatment. The largest group of cancer survivors is breast cancer survivors (22 percent), followed by prostate cancer (20 percent). Rock discussed
___________________
1 The title of this chapter, as well as those of remaining chapters, is the same as the title of the workshop session being summarized (i.e., for this chapter, Session 1).
evidence linking diet and nutritional factors, obesity, and comorbidities (e.g., diabetes) to recurrence and survival; elaborated on several treatment-related nutritional problems that develop during the early phase of care and that sometimes continue and are endured throughout survivorship, such as changes in body composition, vasomotor symptoms in breast cancer survivors, and psychosocial problems; and described findings from nutrition intervention research in breast and prostate cancer survivors. The evidence she reviewed suggests that nutritional care may reduce the risk for cancer recurrence and progression. Rock cautioned, however, that while cancer survivors are an appropriate target for intervention because of their ability to make behavioral changes, they also present with special issues and concerns. Interventions used for the general population may be ineffective.
This chapter provides detailed summaries of both presentations and the discussion that followed.
NUTRITIONAL INTERVENTIONS AND ISSUES IN EARLY ONCOLOGY TREATMENT2
With 35 years of practice as a registered dietitian and a focus on head and neck cancer patients, Mary Platek expressed gratitude for the efforts that led to this workshop and passion for the topic of discussion. Back when she began practicing and was seeing patients in the intensive care unit, she always wondered how her patients did after sending them off. Then she became involved with conducting studies on outpatients at a comprehensive cancer center but still with a focus on early oncology care and, specifically, nutritional status of the outpatient. She noted that while much of what she would talk about relates to pediatric oncology, the focus would be on adult oncology patients, including adult patients undergoing radiation or chemotherapy; patients who have had surgery; patients who have been sent home and are being followed up in the clinic; and any combination of these situations. The patients who are at increased need of professional nutrition intervention, in her opinion, are those receiving multi-modal therapy.
Nutritional Status in the Outpatient
Nutritional status reflects how well a person’s physiological nutrition needs are actually being met. Adequate nutritional status results from a balance between what an individual is taking in and what his or her requirements are, with many factors at play (e.g., digestion, absorption, excretion). With cancer, if an individual’s needs are not being met, their nutritional
___________________
2 This section summarizes information and opinions presented by Mary Platek, Ph.D., M.S., RD, Roswell Park Cancer Institute, Buffalo, New York.
status is sometimes referred to as malnutrition, sometimes under-nutrition, and sometimes cachexia. Platek referred to Elaine Trujillo’s earlier remarks on obesity and the number of patients with cancer who are obese. (See Chapter 1 for a summary of Trujillo’s remarks.) Obesity in cancer is a difficult challenge to manage, Platek emphasized, especially when so many of those patients are experiencing sarcopenia (loss of muscle mass).
Registered dietitians use what is known as the Nutrition Care Process to identify nutritional status in the clinic. The first part of the process, Platek explained, is screening to identify patients at risk for a nutrition problem. Because people present in so many different ways, some patients may already have malnutrition. But for those who do not, if symptomology can be captured and dealt with early on, “We’re really ahead of the ball game,” Platek said, and the patient may never enter the realm of malnutrition or cachexia. One screening tool that has been well validated in the outpatient oncology setting is Patient Generated Subjective Global Assessment (PG-SGA) (Ottery, 1996; Vigano et al., 2014), which Platek explained involves a physical exam (conducted by a professional) and four boxes of questions (answered by the patient and then scored) to triage people into intervention. The questions pertain to nutritional intake, unintentional weight loss, and symptomology.
Screening initiates a nutritional assessment, Platek continued, which involves enlisting the help of a dietitian, collecting more information, and determining an intervention. The goal of the nutrition intervention is to remedy the nutrition problem, not the etiology. Nutritional interventions include everything from individualized nutrition counseling to finding out whether patients have enough food to eat when they go home to coordinating nutrition care within the hospital setting (i.e., among patients who are readmitted).
Until recently, Platek observed, much of the challenge to identifying nutritional status in the clinic was lack of consensus on definition. It is difficult to screen and identify something for which there is no consensus. Today, operational definitions exist for inadequate nutritional status in cancer patients, cancer-related malnutrition, and cancer cachexia. Today, the greater challenge in the outpatient cancer setting is nonstandardized screening. Screening is either not happening, according to Platek, or different tools, including tools that have not been validated, are being used. The lack of nonstandardized screening tools make for difficult comparative efforts and a lack of evidence-based nutrition care paths. An even greater challenge, in Platek’s experience, is the lack of available nutrition services in the outpatient setting. In a 2012 survey of what were then 40 comprehensive cancer centers, Platek and colleagues found that the majority of respondents used referral or consult-based services (Platek et al., 2014). That can work very well, she said, when outpatient dietitians are available to meet the call. But when dietitians are not part of a multidisciplinary
service and patients are referred instead, there is no assurance that patients actually receive that particular service.
Effect of Cancer on Nutritional Status
Cancer often results in some sort of nutrition imbalance at some point during treatment, recovery from treatment, and possibly beyond, Platek continued. The effects are either from the tumor itself, host response to the tumor, or other factors (e.g., stress, anxiety, or depression that make it difficult for people to focus on eating). The intensity of the nutrition consequence varies depending on the stage of cancer, where the cancer is and, importantly, according to the literature, whether treatment is multimodal (Dewys et al., 1980; Capra et al., 2001; Ravasco et al., 2003; Platek et al., 2011). Patients receiving surgery followed by radiation and chemotherapy are at very high risk, with up to 80 percent of patients receiving multimodal therapy experiencing unintentional weight loss and malnutrition. The majority of these patients, according to Platek, have head and neck, gastrointestinal (GI), lung, or any advanced cancer.
Platek emphasized the need to stage people correctly and to intervene before they reach cancer cachexia, a metabolic syndrome driven by a continuous decrease in food intake and abnormal metabolism and characterized by ongoing loss of skeletal muscle (Fearon et al., 2011). An estimated 50 to 80 percent of cancer patients are cachectic at some point during the continuum of care, according to Platek, and about 20 percent of the cancer patient population dies not from cancer but cachexia (Ryan et al., 2016).
Effect of Treatment on Nutritional Status
Now that improved definitive treatments are available and more people are surviving cancer, in addition to considering the effects of cancer itself on nutritional status, Platek considered the effects of cancer treatment on nutritional status. While surgery can increase the body’s need for calories so the extra work necessary for healing can be done, it can also cause anorexia, poor appetite, delayed gastric emptying, early satiety, and other GI discomforts (e.g., nausea, vomiting, and diarrhea). Platek and colleagues advise patients, surgeons, and other members of health care teams that patients who have had surgery need to eat more calories and protein in particular. But it is difficult to target patients who need this advice, Platek observed, when there is no systemic protocol in place for nutrition interventions.
Treatment effects of radiation and chemotherapy can be “astronomical,” Platek continued, with effects from radiation differing depending on where the radiation is focused. In her work with head and neck cancer patients, she deals with people with extreme mucositis, dry mouth, and
poor appetite. Effects of chemotherapy include nausea, vomiting, taste changes, and food aversions, with patients often eliminating foods they need because of taste changes and aversions.
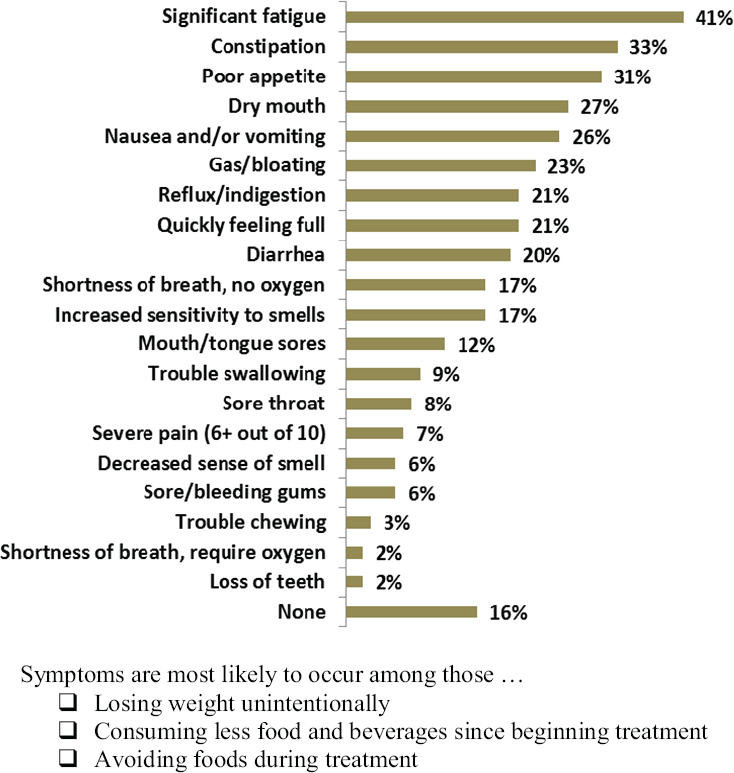
Compounding the challenge are the facts that not everyone who begins treatment is well nourished and that both cancer and treatment for cancer can aggravate preexisting nutrition problems. Many patients who have ignored their symptomology have already experienced a 10 percent or more unintentional weight loss. Platek remarked that patients often say their eating is fine and that it has not changed when really they have adapted to a new level of eating (e.g., soup becomes the “new normal,” when before it was a full plate of all kinds of foods). In a survey of 1,200 outpatients at seven comprehensive cancer centers, with patients having been diagnosed with all types of different cancers at an average of about 9 months before the survey, Platek and colleagues found that most patients experienced some sort of symptomology and that fatigue was at the top of the list of symptoms (Coa et al., 2015) (see Figure 2-1). The most interesting finding, in Platek’s opinion, was that symptoms were most likely to be reported among people who were losing weight unintentionally.
Effect of Nutritional Status on Treatment and Clinical Outcomes
Added to the effects of cancer and treatment on nutritional status are the effects of poor nutritional status on treatment. Poor nutritional status can have major effects on treatment. Platek listed several. They include decreased treatment response, increased treatment complications, and increased treatment toxicity (both with respect to the number of people experiencing toxicity and the intensity of toxicity). Altering or interrupting the treatment schedule or de-escalating the dose because of these effects has been associated with recurrence, increased hospital admissions or readmissions (because of infections), increased length of hospital stays, poor quality of life, and early mortality.
Malnutrition also affects drug metabolism. Patients who are malnourished have low albumin levels, which can make drugs more potent by increasing their availability to tissues. Platek explained that lower doses are often recommended for persons with low albumin to avoid poor seizure control, hemorrhage, and other side effects.
Nutrition Interventions in Early Oncology Care
Evidence for nutrition interventions in early oncology care is available from many resources, including the Academy of Nutrition and Dietetics’ (AND’s) Evidence Analysis Library (EAL) and Oncology Evidence-Based Nutrition Practice Guideline (AND, 2013), which Platek noted was based
SOURCES: Presented by Mary Platek on March 14, 2016; Coa et al., 2015.
on a systematic review and grading of the literature by a team of 45 professionals, as well as PubMed and Embase. Using these resources, Platek searched the literature as far back as 1980, which is when, she said, “We started talking about the skeleton in the closet.” She found it very interesting to go that far back and trace the path forward and noticed a lot more randomized controlled trials (RCTs) and interventions in the more recent literature. She found a total of 653 papers published from 1980 to 2016, but reported during this workshop on overall results from only 36 of these plus 2 additional systematic reviews (all published between 2010 and 2016).
The majority of evidence in the 38 papers that Platek reviewed concerns patients with either upper or lower GI cancers or head and neck cancers, which in Platek’s opinion, is the cancer population at highest risk for nutritional problems. Among the RCTs she examined, the comparisons were between interventions and controls. Among the prospective studies, the comparisons were between cohorts where an intervention was started versus cohorts where what was done before was still being done. In the retrospective studies, researchers either compared a population in a certain time period to an older population prior to an intervention change or compared results to what had been reported in the literature.
Of these 38 papers, 4 RCTs and 1 prospective study related to systematic individualized nutrition counseling. Overall, systematic individualized nutrition counseling was associated with improved weight, improved quality of life, improved nutritional intake, improved nutritional status and, with radiation therapy in particular, decreased toxicity (both reports and intensity of toxicity). Additionally, one of the systematic reviews (of head and neck cancer studies conducted up through January 2012) identified 4 of 10 RCTs that examined the effects of nutrition counseling versus either no counseling at all or counseling by a nurse (Langius et al., 2013). All four studies showed a positive association on nutritional status among those who received nutrition counseling. Three of the four demonstrated decreased weight loss among those who received nutrition counseling, and three demonstrated decreased incidence of malnutrition. Two of the four studies also assessed quality of life and showed a decline in global score (using the measurement of quality life) with nutritional counseling. Thus, Platek concluded, nutrition counseling is important.
But so is nutrition support, she continued. Nutrition support includes oral nutrition supplementation, enteral feeding, parenteral feeding, and other modes. Of the 38 papers she reviewed, 11 RCTs, 4 prospective studies, and 6 retrospective studies concerned nutrition support. Overall, the studies show that early nutrition support, that is, nutrition support that is provided before a patient reaches criteria for malnutrition, is associated with improved nutritional status, GI recovery, enhanced immune response (as reflected by biomarkers), improved quality of life, decreased length of hospital stay, decreased incidence of surgical complications, and decreased readmissions to the hospital.
When nutrition counseling and support are combined, as they were in one RCT, one prospective study, and two retrospective reviews (again, all from 2010-2016), overall effects included improved weight status, improved functional walking (improved performance status), improved recovery from surgery, improved quality of life, improved treatment tolerance, decreased postoperative complications, and decreased treatment toxicity to chemoradiation.
In addition to nutrition counseling and support, the literature on immune-enhancing nutrition (IEN) support is increasing as well, according to Platek, although she emphasized the importance of clearly defining what is meant by IEN. She defined IEN as formulas having at least two of the following: arginine, omega-3 fatty acids, glutamine, and ribonucleic acid. Of the 38 reviewed papers, she found 4 RCTs and 2 prospective studies on IEN support. Her review of these studies showed improved body weight and lean body mass, as well as improved performance status, with use of IEN support. These same studies also showed decreased inflammation, decreased length of hospital stay, decreased postoperative complications, and decreased incidence of infections. In a meta-analysis of 27 RCTs on the effects of different IEN support regimes among patients who underwent surgery for resectable GI malignancies, Song et al. (2015) found a decreased risk for infectious complications in all settings (i.e., preoperative, perioperative, postoperative), a decreased risk of non-infectious complications in the perioperative setting, and a decreased length of both perioperative and postoperative hospitalization. According to Platek, Song et al. (2015) concluded that IEN is a promising alternative to standard enteral care and that IEN is optimal for managing perioperative care. In addition to these studies, Platek continued, the EAL provides strong evidence (i.e., from 24 studies) for fish oil being associated with preservation of weight and lean body mass.
Summary
In summary, Platek emphasized that there is an established role for individualized dietary counseling. She said, “I don’t think we need to look at this again.” Likewise, although it is difficult to conduct RCTs on nutrition support, it is established that there is a role for nutrition support as well. Now, she said, “We need to have people do this.” She made a call for the use of nutrition support accompanied by education and counseling. Additionally, evidence is growing that supplements containing immune enhancers, such as fish oil, may play a role in certain settings.
Intervention is especially needed, Platek urged, when treatment is multimodal; the earlier the intervention, the better. She noted evidence in the EAL (from 20 studies) providing strong evidence for improvement of treatment outcomes in patients undergoing outpatient chemotherapy and/or radiation treatment with medical nutrition therapy.
Finally, she emphasized that registered dietitians are an integral part of the outpatient multidisciplinary healthcare team and that administrative support is needed to make this happen. She encouraged the development of validated screening and assessment tools; more follow-up after clinical nutrition interventions; continued use of predictive modeling; and development of evidence-based nutrition protocols.
NUTRITIONAL INTERVENTIONS AND ISSUES IN LONG-TERM ONCOLOGY CARE3
Cheryl Rock addressed many of the same nutrition care issues that Platek discussed, but in the context of long-term oncology care. In the United States, the most frequently diagnosed cancer in men is prostate cancer (29 percent in 2012, according to the American Cancer Society [ACS]), followed by lung cancer (14 percent), then colon and rectal cancer (9 percent). In women, the most frequently diagnosed type of cancer is breast cancer (29 percent in 2012), followed by lung cancer (14 percent), then colon and rectal cancer (9 percent). For both men and women, all cancers, even the less common types, can have significant nutritional effects, Rock noted.
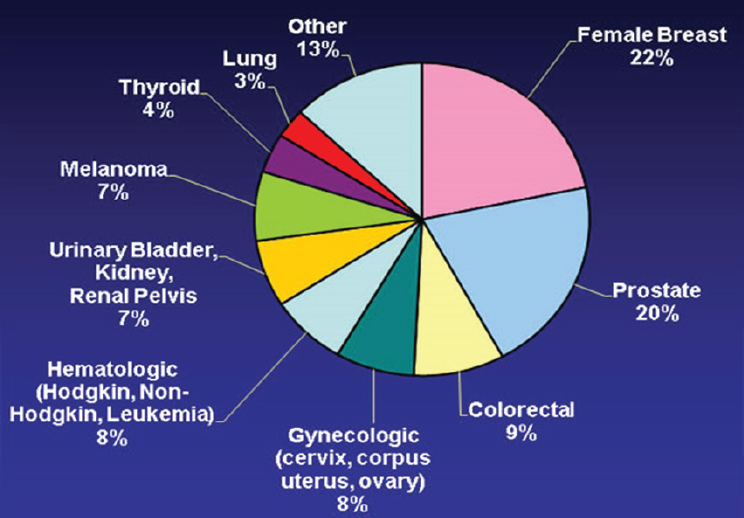
Among cancer survivors, the largest percentage are women who have been diagnosed with breast cancer (22 percent), followed by men who have been diagnosed with prostate cancer (20 percent), then persons diagnosed with colorectal cancer (9 percent) (Mariotto et al., 2011) (see Figure 2-2). That the largest percentage of cancer survivors are women who have survived breast cancer explains, Rock said, why so much of the evidence for the cancer survivor population is based on breast cancer patients.
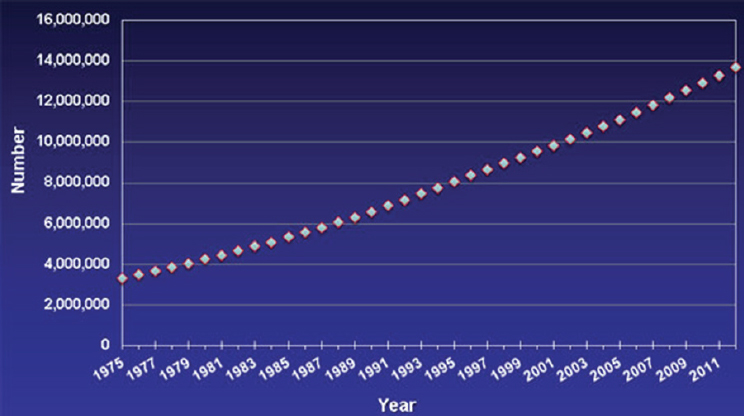
The past 30 years have seen a remarkable increase in the number of cancer survivors who are living post-treatment (Mariotto et al., 2011) (see Figure 2-3). Rock listed several reasons for this trend. First is the aging U.S. population. Given that cancer is very much a disease of aging, with a cancer diagnosis becoming more likely as one ages, the number of people in the United States who are potential cancer diagnosis cases has increased. It has been predicted that, by 2020, two-thirds of cancer survivors in the United States will be over the age of 65 years (Parry et al., 2011). Another reason for the growing number of cancer survivors is the availability of better screening approaches. The earlier a cancer is detected, the greater the likelihood of surviving treatment and becoming a long-term survivor. Although cancer screening is still not “great,” Rock said, with many organizations supporting this workshop actively involved in promoting better cancer screening, screening has improved. A third factor is the availability of better initial treatments. It wasn’t too long ago, Rock recalled, that many women with breast cancer were not diagnosed until their cancer was advanced and the only treatments available were surgery or cytotoxic chemotherapy. That is no longer the case, Rock said, “thanks to the war on cancer.”
Today, more than 14.5 million persons in the United States are cancer survivors, Rock observed. Owing to early detection and treatment, 65 percent of Americans diagnosed with cancer now live more than 5 years. For
___________________
3 This section summarizes information and opinions presented by Cheryl Rock, Ph.D., RD, University of California, San Diego.
SOURCE: Presented by Cheryl Rock, on March 14, 2016 (adapted and reprinted with permission from de Moor et al., 2013).
SOURCE: Cheryl Rock, March 14, 2016 (modified from Parry et al., 2011).
lower-stage cancers, the percentages are even higher, with close to a 98 percent 5-year survival rate for early-stage breast cancer. Rock remarked that many younger people do not realize how common cancer is and how many people around them who appear to be living wonderfully healthy lives are in fact cancer survivors. Again, of those 14.5 million, a large percentage are over the age of 65 years, with breast cancer survivors being the largest group, followed by prostate cancer survivors and colorectal cancer survivors. Among all survivors, over 4.7 million received their diagnosis 10 or more years earlier.
Rock reiterated Platek’s emphasis on the critical amount of evidence calling for early oncology nutrition care, but she explained that she would be focusing on long-term disease-free living. The ACS has delineated in its guidelines two goals for long-term disease-free living: (1) reduce the risk of cancer recurrence and progression, and (2) prevent and manage comorbidities. Because long-term cancer survivors are still at risk of dying from recurrent cancer or a second cancer, Rock identified palliative care as another important component of long-term care.
Diet, Recurrence, and Survival: The Evidence
Regarding available evidence indicating that diet and nutritional factors are related to recurrence and survival, first and, in Rock’s opinion, of “critical” importance, very strong biological evidence from the laboratory setting suggests that nutritional factors are likely to influence cancer progression. In fact, she explained, cell culture studies by their very nature are more reflective of cancer progression than they are of risk. To make cells grow in culture, those cells have to be transformed. Otherwise, they would die. Thus, much of what scientists have learned about nutritional factors is highly relevant to cancer progression simply because of the nature of the cell culture model.
In addition to this biological evidence, epidemiological studies conducted over the past 2 decades suggest that many of the nutritional factors associated with risk for primary cancer also seem to affect survival after diagnosis. While this epidemiological evidence is cruder than what has been seen in the lab, it is consistent, Rock remarked.
Third, at least for breast cancer, studies have been conducted to determine whether diet interventions can actually modify recurrence and survival. Rock was aware of at least two other ongoing studies.4
Finally, evidence from observational studies is fairly consistent. That is, a healthy dietary pattern, which Rock described as one that provides
___________________
4 Rock discussed these studies toward the end of her talk; see the section titled “Nutrition Intervention Research in the Long-Term Oncology Population: Current Evidence.”
vegetables, low-fat dairy foods, whole grains, tree nuts, olive oil, and fish and poultry rather than red meat, has been associated with lower risk for the most common cancers (i.e., breast, prostate, colon) and greater likelihood of survival after diagnosis. However, Rock pointed out, observational studies are confounded, which means that it might be that people who eat that way have had better treatment, for example, or there may be subtle differences in social support or demographic characteristics that explain the association. In Rock’s opinion, although results from observational studies do not provide definitive evidence, they are good for generating hypotheses.
Obesity and Cancer
It has been known for many years, Rock continued, that obesity is related to risks for disease like diabetes and cardiovascular disease. Only over the past 15 years or so has evidence begun to emerge suggesting that obesity is probably the strongest nutritional factor related to not only cancer diagnosis, but also survival after diagnosis. An estimated 14 percent of all deaths from cancer in men and 20 percent of deaths from cancer in women are related to obesity. While it was expected that hormone-related cancers, namely breast and prostate cancer, would be related to obesity, because adipose tissue is basically an extra-gonadal source of hormones, the surprise, Rock said, was that mortality from many other types of cancers are also associated with obesity. Obesity and overweight have been associated with increased mortality from cancers of the esophagus, colon and rectum, liver, gallbladder, pancreas, kidney, and stomach, as well as non-Hodgkin’s lymphoma and multiple myeloma.
In addition to its effects on survival after diagnosis, being lean and physically active appears to also be associated with fewer treatment-related problems during the initial treatment period (e.g., lymphedema with breast cancer, incontinence with prostate cancer, physical function with all cancers).
Thus, the effect of obesity begins during early treatment and extends through long-term survival. In a meta-analysis of more than 40 studies, while accounting for other influencing factors such as physical activity, demographic characteristics, and type of treatment, Protani et al. (2010) found that obesity was inversely associated with about a 30 percent increase in breast cancer–specific survival and also in overall survival among breast cancer survivors. This observed effect was apart from the fact that many women, about two-thirds, gain weight when they go through breast cancer treatment, according to Rock. The studies in the analysis were based on obesity (and body mass index [BMI] generally) at the moment of diagnosis.
Comorbidities
Comorbidities are a critical priority with respect to what needs to be accomplished with providing nutritional care to long-term cancer survivors, Rock continued. Again, cancer is a disease associated with aging, and over 80 percent of older adults have at least one comorbid condition, such as diabetes, cardiovascular disease, or hypertension, at the time of their cancer diagnosis, and 50 percent of older adults have more than two comorbidities at the time of diagnosis. With breast cancer in particular, more than 40 percent of survivors have other chronic comorbid conditions at the time of their cancer diagnosis, and developing new conditions post-diagnosis is common.
Comorbidities contribute to poorer long-term survival and increased overall mortality. Rock recalled studies she has been involved with where women who had diabetes when they were diagnosed with breast cancer were more likely to have an early death during the course of the study regardless of treatment. Also worth pointing out, Rock noted, post-menopausal breast cancer patients are far more likely to die from cardiovascular disease than from the effects of breast cancer. Additionally, having comorbidities while going through concomitant cancer treatments and dealing with the anxiety and stress of the treatments has been associated with poor physical and mental quality of life.
Treatment-Related Nutrition Problems
Rock discussed in detail several treatment-related nutrition problems that develop during the early phase of care and that sometimes continue and are endured throughout the entire cancer survivorship. First is evidence that treatment for cancer is associated with changes in body composition and metabolic consequences. Rock explained that when an active population suddenly becomes less active because they are ill or because they are going through treatment, which is especially true of older adults, the loss of physical activity that occurs during this period of time means that body composition changes. Changes in body composition include loss of lean body mass (i.e., sarcopenia) during initial treatments which, in the long run, have a big effect on energy balance. This is probably why certain groups of cancer survivors gain weight after they have gone through the initial treatment, Rock said. She explained that lean body mass is the primary determinant of resting energy expenditure which, in turn, is the main source of calorie expenditure. So a woman who might have a resting energy expenditure of 2,000 calories per day on the day of her diagnosis will have a substantially lower resting energy requirement after treatment because she will have lost so much lean muscle mass. Yet, she will probably have gained some adipose tissue during that time and, thus, weigh the same.
With less lean muscle mass and more adipose tissue, the ability to maintain weight by eating 2,000 calories per day becomes much more challenging. This change in body composition, Rock continued, is attributed mainly to reduced physical activity and, among pre-menopausal women, treatment-related ovarian failure. As a result of these changes, post-treatment weight gain is common in this population.
Another treatment-related problem with important nutrition implications is chemotherapy-induced peripheral neuropathy, which affects physical activity and function. This is particularly problematic for older adults who already have some gait instability.
Yet another treatment-related problem, one that has become a greater problem over the past decade or so, according to Rock, because of changes in cancer treatment, are bone health issues, especially for breast and prostate cancer patients. Many breast and prostate cancer patients are prescribed and benefit from either aromatase inhibitors or androgen deprivation therapy, respectively, both of which have effects on bone. Cytotoxic chemotherapy can also have direct effects on bone resorption and formation.
Several treatment-related problems are specific to the breast cancer population. One is vasomotor symptoms, which Rock described as hot flashes that develop as a result of hormonal therapies and the effects of treatment on ovarian function. They occur in 65 to 95 percent of patients and are much more severe than in the general population. She noted that, over her years of leading weight management interventions for breast cancer survivors, always at least half the women in the group sessions will have to fan themselves or open a window. Vasomotor symptoms are the type of thing that can affect not only quality of life, but also the ability to continue physical activity and make good diet choices. They are very disruptive, Rock said. They are not minor concerns.
In addition to vasomotor symptoms, another breast cancer treatment-related problem is lymphedema, which occurs in about 15 to 20 percent of breast cancer survivors. Rock noted that it is less common now than in the past because of differential diagnosis and sentinel lymph node biopsies, but it is still very common. A high BMI may increase the risk for lymphedema. Again, the physical discomfort can limit physical activity. Limited physical activity, in turn, affects energy balance, body composition and adiposity, and eventually recurrence.
Finally, arthralgias and myalgias, that is, joint and muscle pain, occur in more than 40 percent of women with breast cancer who are treated with chemotherapy and in up to 50 percent of women who are treated with aromatase inhibitors. According to Rock, these problems are more common in obese women and can contribute to reduced physical activity.
In addition to these numerous physical problems that can persist well beyond initial treatments, a substantial proportion of cancer survivors (20
to 30 percent) experience dysphoria, with depression and fatigue being the most common problems. Different studies define fatigue differently, with estimates of the prevalence of fatigue among cancer survivors ranging from 15 to 90 percent. Several mechanisms have been proposed to explain cancer-related fatigue, including neurotoxicity of the cancer treatments, chronic stress, inflammatory responses, and hormonal change. Rock noted that younger cancer survivors report greater psychosocial distress than older survivors.
Additionally, because cancer patients are a group for whom there has been a major life change, that is, the diagnosis of a life-threatening medical condition, many cancer survivors have a heightened awareness and concerns about foods. Because of these heightened concerns, Rock said, “You can’t just take [a nutrition intervention] that has some success in the general population and throw it into this population, this target group, and expect that it would be successful.”
Childhood cancer survivors represent a newly burgeoning population of long-term cancer survivors, with 5-year survival rates among this population now more than 80 percent. Yet, despite these fantastic 5-year survival rates, Rock remarked, survivors of acute lymphoblastic leukemia, the most common cancer diagnosed in children, have a life expectancy of only 54.7 years. All childhood cancer survivors are at increased risk of cardiovascular disease and are 10 times more likely to develop cardiovascular disease and 8 times more likely to die of heart failure during their first 30 years post-diagnosis. These long-term consequences of childhood cancer indicate potential benefit for nutrition intervention, in Rock’s opinion. There is a fair amount of evidence from observational studies that diet, low physical activity, and obesity all contribute to the very short life expectancy in this population compared to the general population.
GI and head and neck cancer patients represent another special population for whom nutrition intervention likely has potential benefit, given the enduring effects of surgery among these patients on dietary intake and nutrient absorption. Finally, cancer patients undergoing palliative care represent yet another special group for whom nutritional support and counseling may help patients to live as actively as possible and improve quality of life.
Rock ended her overview of nutritional issues related to long-term cancer care with a few remarks on dietary supplements. Evidence from a number of studies indicates that 64 to 81 percent of cancer survivors use dietary supplements. While the evidence further suggests that perhaps some supplements may be appropriate for patients with inadequate dietary intake, in the long run, if anything, supplements are unlikely to improve prognosis or overall survival and may actually increase mortality. There is also a potential risk for interactions between dietary supplements and prescription medications.
Nutrition Intervention Research in the Long-Term Oncology Population: Current Evidence
Rock was aware of only two completed randomized clinical trials on dietary intervention in breast cancer survivors. First, the Women’s Intervention Nutrition Study enrolled approximately 2,500 postmenopausal women who had been diagnosed and treated for early stage (i.e., I, II, III) cancer (Chlebowski et al., 2006). The women were followed for 5 years, on average. The diet intervention aimed to reduce percent energy from fat to 15 percent, although the researchers went into the study expecting to be doing well if they were able to get people to consume less than 20 percent of their calories from fat. It was a complicated study, Rock explained, because the primary analysis indicated only a borderline significant effect on recurrence and no significant effect on survival. However, a secondary analysis among women with estrogen receptor (ER)-negative cancer, which was a little over one-third of the women, showed a significant benefit. The study was further complicated by the fact that the group targeted with the low-fat dietary intervention actually showed greater weight loss, which means that some of the benefits may have been due to weight loss, not the dietary intervention itself.
The second study, the Women’s Healthy Eating and Living (WHEL) Study (Pierce et al., 2007), was not as complicated to interpret, Rock said. The study enrolled both premenopausal and postmenopausal women who had been diagnosed and treated for early-stage breast cancer and followed the women for about 7 years. The dietary intervention was not a weight loss intervention. In fact, the women were encouraged to maintain weight because weight change was viewed as a potentially confounding factor. The intervention emphasized a plant-based diet, with, on a daily basis, five vegetable servings plus 16 ounces of vegetable juice or equivalent, three fruit servings, 30 grams of fiber, and again a reduction in dietary fat intake (15 to 20 percent energy from fat). The dietary biomarkers that were measured in the study indicated very good adherence. The study revealed no differences in breast cancer recurrence or survival. Though, again, in a secondary analysis, which Rock noted is problematic from a scientific standpoint, but nonetheless interesting, the researchers found that women without hot flashes at enrollment (indicative of higher circulating estrogens) experienced a substantial reduction in their risk of breast cancer events (i.e., either recurrence or new primary breast cancer). Rock explained that a lot of dietary fiber in the diet can increase the gastrointestinal loss of estrogens, which may explain why this intervention was beneficial for that subgroup in particular. Higher estrogens in the blood are associated with a greater risk for breast cancer and greater likelihood of death from breast cancer. While not as difficult to interpret as the previous study, one notable complication
is that women when enrolled in the study were already eating over seven servings of vegetables and fruits daily.
In addition to these two completed studies Rock mentioned two ongoing studies of effects of lifestyle (i.e., weight loss, diet, physical activity) on breast cancer outcomes: the SUCCESS C trial in Germany and the DIANA-5 study in Italy.
Numerous other studies, at least more numerous than in other areas of research in nutrition and cancer, have examined the effect of weight loss interventions on weight and selected biomarkers in overweight and obese breast cancer survivors. Upon reviewing the literature, Rock identified 13 RCTs that have done so and an additional five single-arm or other design studies. Rock recalled unease 20 years ago about recommending weight loss interventions in cancer survivors. These studies have shown overwhelmingly that achieving weight loss is not only feasible, but safe. The majority of the 13 RCTs identified by Rock showed greater than 5 percent weight loss as a result of the intervention.
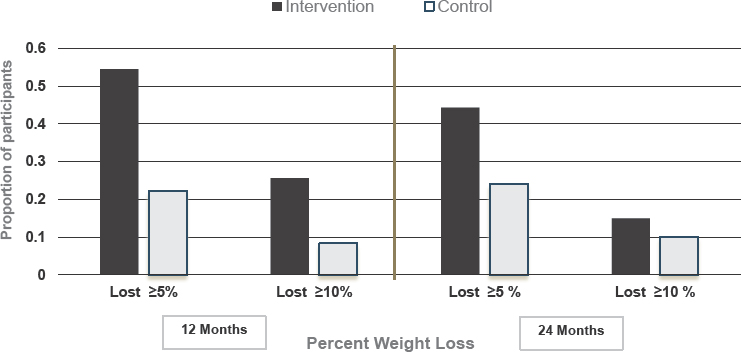
The largest weight loss intervention study to date, according to Rock, is the ENERGY trial, a multi-state RCT of both pre- and post-menopausal women who were overweight or obese and who were diagnosed with stage I-III breast cancer between 6 months and 5 years earlier (i.e., women who had completed their initial treatments) (Rock et al., 2015). The intervention was an intensive 1 year of group cognitive behavioral therapy, supported by telephone or email contacts and newsletters. At 12 months, the average weight loss across all sites was 6 percent in the intervention group, compared to 1.5 percent in the control group (see Figure 2-4). The second year of the study involved very little contact with participants, so not unexpectedly, there was some recidivism, with many women regaining the weight they had lost during the first year. However, even at 24 months, many more women in the intervention group achieved clinically significant weight loss (i.e., 5-10 percent) compared to women in the control group (see Figure 2-4). There were also favorable effects of the intervention on physical activity and blood pressure.
There have also been a fair number of studies of interventions targeting prostate cancer survivors, Rock noted. She identified 12 small randomized controlled diet intervention studies among prostate cancer survivors that have examined various biochemical and quality-of-life outcomes. Additionally, she identified two larger studies that included not only prostate cancer survivors, but also either breast cancer survivors or breast cancer and colon cancer survivors. The first of these, the FRESH START study, enrolled more than 500 prostate and breast cancer survivors with early-stage disease (Demark-Wahnefried et al., 2003, 2007). Participants were randomized to having either tailored or standardized print material aimed at increasing exercise, increasing fruit and vegetable servings, decreasing saturated fat
SOURCE: Presented by Cheryl Rock on March 14, 2016. Reprinted with permission. © 2016 American Society of Clinical Oncology. All rights reserved.
intakes, and maintaining a BMI less than 25. Results indicated that the intervention resulted in increased fruit and vegetable servings and decreased saturated fat intakes, compared to the control group. The second study, the Reach Out to ENhancE Wellness in Older Survivors (RENEW) study, enrolled 641 prostate, colorectal, or breast cancer survivors, most over the age of 65 years. The intervention was an 18-month mailed material/telephone counseling program. Results indicated an association between the intervention and improved physical functioning, improved strength and endurance, improved diet quality, and a modest reduction in BMI (Morey et al., 2009).
Rock found only one dietary intervention weight loss study among childhood cancer survivors (Huang et al., 2014), but she did find several physical activity intervention studies that have either been completed or are underway. The goal of these physical activity interventions is to stop sedentary behavior before it becomes habituated. Overall, the results have been modest, Rock said.
Conclusions, Considerations, and Challenges
In closing, first, Rock repeated that cancer survivors present with special issues and concerns. She cautioned against using interventions developed for the general population. Not only would doing so be inappropriate, but the interventions probably would not be effective. Involvement of an oncology nutrition dietitian who is knowledgeable about the special issues and
concerns of cancer survivors greatly increases the likelihood of provision of appropriate care. Rock emphasized her choice of the word involvement. She said that the person knowledgeable about the nutritional needs of cancer survivors does not necessarily have to be the person who provides the care, but he or she should play an important role in overseeing and monitoring these particular interventions. Second, Rock emphasized how the evidence suggests that nutritional care may reduce the risk for cancer recurrence and progression and should help prevent and manage comorbidities. Finally, she remarked that studies conducted to date suggest that cancer survivors are an appropriate target for interventions because they are able to make behavioral changes.
PANEL DISCUSSION WITH SPEAKERS: DATA GAPS IN CURRENT NUTRITION PRACTICE IN ONCOLOGY OUTPATIENT CARE
Following Rock’s presentation, she, Platek, and Clinton answered questions from the audience on a wide range of topics related to the current knowledge and status of nutrition practices in oncology outpatient care (see Chapter 1 for a summary of Clinton’s keynote presentation). This section summarizes the discussion that took place.
Educating Oncology Clinicians About Cancer-Related Nutrition Issues
Ann Fonfa mentioned having attended the American Society for Clinical Oncology (ASCO) meeting on survivorship in January 2016 and heard nutrition mentioned only three times, twice by board members of her organization while asking questions and once by a speaker. “We need to involve the actual practitioners in this,” she said. Later during the discussion, Suzanne Dixon added that she had experienced something similar at an obesity workshop at ASCO. “I think we have our work cut out for us in that regard,” she said.
Clinton was disappointed to hear of Fonfa’s experience, but remarked that at least ASCO has a survivorship program and clinicians are participating in it. In his opinion, part of why there is not more nutrition representation in ASCO, a professional organization that represents clinical oncology, is that very few medical oncologists are actually trained in nutrition. He expressed hope that, with time, ASCO’s new involvement in survivorship will bring more nutrition expertise into play. He mentioned that the society had recently issued an announcement that anyone who wanted to serve on a committee could volunteer. He himself has volunteered and said he was looking forward to helping.
Rock agreed that very few oncologists are trained in nutrition. Rather, their extensive specialist knowledge is in drugs, treatment complications,
and related issues. She suggested that oncology nutrition specialists help to educate oncologists about nutrition problems. She mentioned the number of women who have participated in her interventions and research projects and then go back to their clinicians and mention having experienced a little bit of leg pain because they have been walking 4 miles every day. But their oncologists immediately think the pain is related to the cancer. Or, participants in weight loss interventions go back to their physician having lost 20 pounds, and the physicians “freak out” because they cannot imagine it was voluntary, not involuntary, weight loss, and they order more scans, which triggers anxiety in the patients, which makes it difficult for the patients to maintain the behavior changes that enabled them to lose the weight. It is not just the oncologists, but families too, Rock said, that react to a survivor’s weight loss or change in behavior. Too often they think, “Oh, no, the cancer’s back.” It used to be that unexplained weight loss was one of the “seven signs of cancer.” That mentality has persisted, Rock said. She remarked that, while nutrition education at the undergraduate level has expanded, nutrition education efforts should also be targeting the clinical setting.
“Everything always starts with education,” Platek agreed. The more you know, the better your decisions will be, and the better care your patient will receive. She reiterated the importance of registered dietitians having conversations with medical and radiation oncologists and others so that the clinicians know what to be concerned about and also what to not be concerned about (e.g., weight loss through survivorship). But in order for the oncologists to gain this knowledge, the registered dietitian, Platek said, needs to be “brought to the table.”
There was a brief discussion about how, among physicians, sometimes a little bit of nutrition knowledge goes a long way, but, as Rock said, often the wrong way. The discussion was prompted by a question from an audience member about all the “hype” in the media about soy and breast cancer and the controversy around the relation between soy and breast cancer. Rock found it interesting that this controversy exists given the overwhelming evidence indicating that there is no reason to be concerned with soy. In fact, she said, epidemiological evidence suggests that, if anything, soy is helpful. Another source of the problem, Rock continued, is physicians knowing too little. She noted that the next batch of ACS guidelines for survivors would be addressing soy to a greater extent than in the past.
Educating the Public About Cancer-Related Nutrition Issues
An audience member who identified herself as an oncology dietitian working “in the trenches” has been trying to encourage women who are diagnosed with breast cancer to meet with her before surgery. Many of
these women are overweight, the audience member said. Moreover, many come to see her once but then never return even though she offers a free service (e.g., to help them lose weight to prevent recurrence). She asked, “Why are these women not coming to see a dietitian when it’s even a free service?” Rock responded that, again, the challenge is education, in this case, education of the public. She credited organizations such as the ACS for communicating to the public about the importance of nutrition, diet, and weight control for cancer patients.
Fonfa, speaking as both an advocate and patient, suggested that weight loss not be presented as weight loss. Rather, it should be presented as nutrition. The focus is on health, not weight loss. That opens the door, she said, without “attack” and in a way that will not trigger a reaction during what is a very sensitive time. Additionally, Fonfa suggested that, in the beginning, rather than one-on-one education, the focus should be on group discussions.
Rock agreed that the message should be “healthy lifestyle,” not “weight loss.” However, in response to Fonfa’s suggestion that initial education efforts be group discussions, Rock said she finds the one-on-one visits with patients very empowering. There are so many things about cancer that you cannot do anything about, but lifestyle is something that is modifiable, she stated.
Clinton identified a need for research on how to optimally integrate patient education about nutrition into the process of cancer care. While it is easy to wonder why women are not taking advantage of such a wonderful opportunity, he said, “You have to look at what is going on in many of these people’s lives.” These women are often working, taking care of their families, and doing all sorts of other things that do not immediately get turned off when they get their diagnosis. It is very difficult for someone to look ahead when she is worried about how she is going to get through the next few weeks of chemotherapy, hormone therapy, radiation, and surgery. He encouraged more thinking about the optimal time to intervene. “We may all think it should be day 1,” he said, “but that may not always be the most practical point.” In his opinion, the most important time for long-term nutrition intervention is when the really intense therapy begins to wind down.
Another audience member, self-described as an “in-the-trenches” outpatient oncology dietitian of 33 years, suggested that dietitians be part of the survivorship plans that the Commission on Cancer is beginning to implement. In her experience, many patients are so overwhelmed at the onset that they are just grappling with “the C word” and trying to get through treatment. She agreed with Clinton that the perfect time for intervention might be when they are done with treatment and are asking, “Now what?”
Suzanne Dixon brought the discussion back to education of the clinician. She suggested that providers mentioning to their patients the impor-
tance of nutrition and physical activity to survivorship would go a long way toward motivating patients to take care of themselves. Though providers would need to be trained on how to approach their patients with that information, she added.
Data Gaps
Toward the end of her presentation, Platek had emphasized the need to implement what has been learned from research already conducted rather than conduct more research. Recognizing that need, an audience member asked what research gaps still exist. Platek called for more work on standardized nutrition screening, at least in head and neck cancers, which she noted was her area of expertise. She also called for more validation of prognostic indicators and entering of that information into predictive modeling so a person’s risk can be determined. Cancers have definitive treatments—everyone knows the stage, the site, and the comorbidities. In her opinion, the same work needs to be done with nutrition so particular treatments can be applied to prevent poor nutritional status and better outcomes. Risk needs to be modeled and nutrition care paths developed and compared.
Immune-Enhancing Nutrition Support
Also during her presentation, Platek had reviewed evidence on the effects of immune-enhancing nutrition (IEN) support. A webcast participant asked for a better definition of IEN. Platek explained that, in the studies she reviewed, IEN was defined as such if it contained at least two of following items: arginine, omega-3 fatty acid, ribonucleic acid, or glutamine. Clinton remarked that he does not like the term. It is too vague and nonspecific, in his opinion. The immune system and its role in cancer is complex. He asked, “What does immune enhancing mean when it is many components working in concert and beautifully orchestrated?” He called for more careful and precise use of language and encouraged consumers to be very conscious about products being marketed with such a vague and nonspecific name. An omega-3 supplement is omega-3. An arginine supplement is arginine. Marian Neuhauser agreed with Clinton and suggested being more specific about which supplements and doses were tested when communicating findings from those studies. Clinton added that the problem begins when vague terminology enters the literature early on—it becomes self-perpetuating. He compared the use of “immune-enhancing nutrition support” to the struggle with “anti-oxidant.” “What are we talking about, and what does it mean?” he asked. Platek concurred with Clinton and reiterated that the way she presented the information is the way it is presented in the literature.






















