
3
Disability Names and Numbers
In the keynote address at the workshop, Maureen Durkin presented an overview of disability data, definitions, and research gaps. Most important, the prevalence of childhood disabilities has risen steadily in recent years, she observed, which has major implications for policy and practice.
TRENDS IN THE PREVALENCE OF U.S. CHILDREN WITH DISABILITIES AND COMPLEX NEEDS
One of the greatest U.S. public health achievements of the past century was the reduction in infant mortality. In 1915, 10 percent of children born did not live to their first birthday. A century later, according to data from the Centers for Disease Control and Prevention, only 6 of every 1,000 children die before the age of 1—a rate of 0.6 percent (Hoyert and Xu, 2012). Deaths of children from 1 to 4 years of age also have fallen dramatically, noted Durkin, from 2 percent in 1900 to 0.0255 percent (Child Trends Databank, 2015).
In contrast, the percentage of children with disabilities and complex needs has been rising in recent decades, though these data are less certain than the data on childhood mortality. Since the 1950s, the National Health Interview Survey has been asking parents about activity limitations in their children. In 1960, parents reported that less than 2 percent of children had an activity limitation due to a chronic health condition. According to the most recently available data, from 2011, the percentage had quadrupled to 8 percent (see Figure 3-1). One problem with these data is that they are based on household surveys and do not include children living in institu-
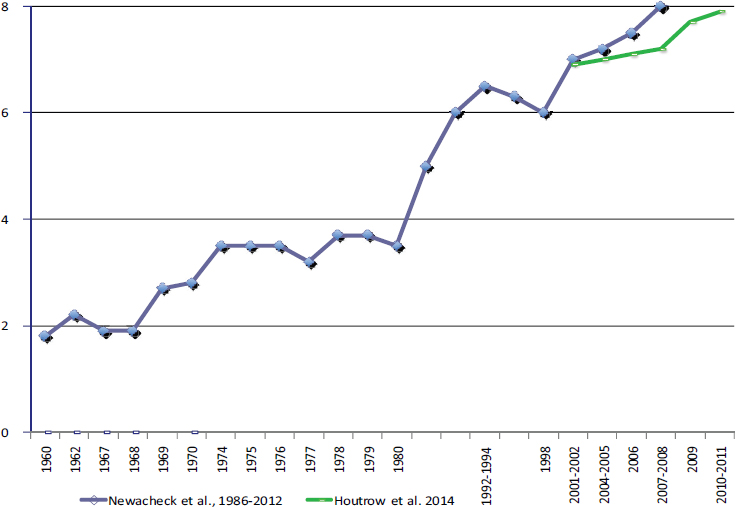
SOURCE: Durkin (2015). Available: http://sites.nationalacademies.org/dbasse/bcyf/dbasse_170078 [September 2016]. Data from Halfon et al. (2012) and Houtrow et al. (2014).
tions. Some of the rise could be due to the fact that the percentage of children living in institutions has declined over the years. Also, the wording of the questions has changed somewhat across survey years, which may have contributed to the rise. Nevertheless, said Durkin, “there’s no doubt that the improvements in survival, especially of children with special health care needs, during this time period have contributed to increases in prevalence.” As an example she cited Down syndrome, which is a common cause of developmental disability and complex health and educational needs. In 1960, the average life expectancy for a child with Down syndrome was estimated at about 10 years; today, due to advances in health care and other services, it is about 60 (Leonard et al., 2000). “It’s not unusual now for individuals with Down syndrome to graduate and go into the workforce,” said Durkin. “This is a huge change.”
Usually in epidemiology, a rising prevalence rate of something is a bad thing. But a rising prevalence of disabilities caused by a reduction in mortality is a good thing, Durkin observed, and it is occurring throughout the
world. “In a way it is a sign of progress in a country when the prevalence of disability is increasing,” she said.
Many other data sources reflect the same trend of increasing disability rates among young people. According to the National Health Interview Survey, the percentage of children with developmental disabilities has risen since the 1990s, with the greatest increases in autism and attention deficit hyperactivity disorder (Boyle et al., 2011). Data from the Children with Special Health Care Needs (CSHCN) survey also show an increase in the number of children with special health care needs, from about 13 percent in 2001 to about 20 percent in 2011-2012 (Bethell et al., 2002). Furthermore, the needs have shifted from physical disabilities more toward mental health conditions and behavioral disorders (Houtrow et al., 2014).
Reports on special education since the 1970s show that the percentage of children qualifying for special education services nationally has increased from about 8 percent to 13 percent today (Scull and Winkler, 2011). The number of children with disabilities receiving Supplemental Security Income more than tripled from 1991 to 2011 (Tambornino et al., 2015). Furthermore, this increase is not due entirely to more children living in poverty, which is a condition of receiving Supplemental Security Income. Controlling for poverty, the percentage of children with a disability who received Supplemental Security Income was less than 3 percent in 1991 and has risen to about 8 percent, again with the prevalence of mental disabilities rising faster than physical disabilities (National Academies of Sciences, Engineering, and Medicine, 2015).
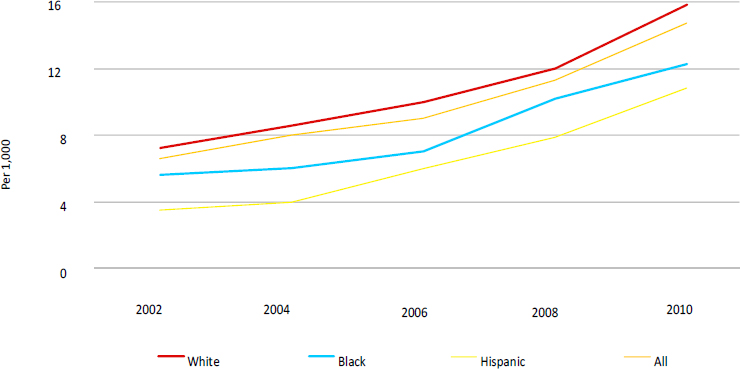
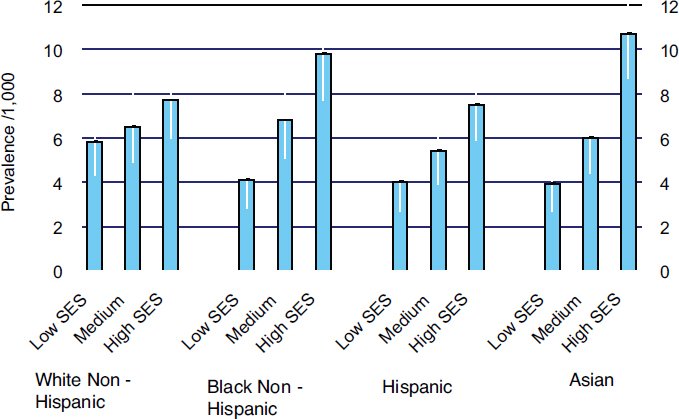
The prevalence of autism spectrum disorder (ASD) also has risen dramatically since 2002 in the United States (see Figure 3-2). The highest prevalence is in white children, with a lower prevalence in African American and Hispanic children. Across ethnic and racial groups, ASD is found at higher prevalences in higher-income families than medium- and lower-income families (see Figure 3-3). “That’s one of the questions that we may address in this workshop,” said Durkin. “Is it true that it’s occurring more in children of high socioeconomic status, or is this a disparity because higher-income children with autism are the ones getting access to services? If the latter, then we might need to do something to make sure that the children in greatest need are actually being identified and getting access to services.”
SOCIAL CONTRACT THEORY AND UTILITARIANISM
Turning to the underpinnings of the policies directed toward children with disabilities and complex health and educational needs, Durkin explained that two traditions of thought, each extending hundreds of years into the past, shape current thinking.
SOURCE: Durkin (2015). Available: http://sites.nationalacademies.org/dbasse/bcyf/dbasse_170078 [September 2016]. Data from the Centers for Disease Control and Prevention (2014).
Utilitarianism focuses on cost effectiveness: How can limited resources be allocated to maximize happiness and well-being for the population overall? From a utilitarian perspective, which calls for the greatest good for the greatest number, a system with high inequality, health disparities, and suffering of a minority, including people with disabilities, may be acceptable if it produces maximum benefit for the population overall.
Contractarianism emphasizes implicit social contracts, Durkin said. From this perspective, everyone must give up something in exchange for social protections. As philosopher John Rawls pointed out, this tradition posits that if people do not know what position they are going to occupy in society, rational people will choose policies that benefit the least advantaged, perhaps including those with disabilities and complex health and educational needs.
A contemporary example of utilitarianism is the use of disability-adjusted life years to estimate the social value of different health interventions. This approach can devalue people with disabilities, Durkin observed, if it holds that they are not as valuable to society as people without disabilities. Another example would be a program that excludes people with disabilities in order to reach more people, because most do not have disabilities.
Under a contractarian approach, the range of inequality is generally narrower than under a strictly utilitarian approach, she pointed out. Inequality still exists, but the extremes on both the high side and the low side are less severe. This approach is consistent with many U.S. policies directed
NOTE: Based on the Autism and Developmental Disabilities Monitoring Network, data from 12 U.S. states with a population of 557,689 8-year-old children in 2002, including 3,680 with autism spectrum disorder.
SOURCE: Durkin (2015). Available: http://sites.nationalacademies.org/dbasse/bcyf/dbasse_170078 [September 2016]. Data from Durkin et al. (2010).
toward children with special needs. As early as 1931, at the White House Conference on Child Health and Protection, President Herbert Hoover said, “Children are our most precious possession. The Children’s Charter was written by 3,500 experienced men and women, after many months of study. It condenses into few words the fullest knowledge and the best plans for making every child healthier, safer, wiser, better and happier. These plans must be constantly translated into action” (Hoover, 1931). A specific policy from the Children’s Charter (White House Conference on Child Health and Protection, Committee on the Infant and Preschool Child, 1931) recommends, “for every child who is blind, deaf, crippled, or otherwise physically handicapped, and for the child who is mentally handicapped, such measures as will early discover and diagnose his handicap, provide care and treatment, and so train him that he may become an asset to society rather than a liability. Expenses of these services should be borne publicly where they cannot be privately met.”
More recent examples of contractarianism include the expansion of the Supplementary Security Income Program to children with disabilities
in 1974, the Individuals with Disabilities Education Act (IDEA) of 1975 and 1990, and the Americans with Disabilities Act (ADA) of 1990. The contractarian approach is also evident internationally in the U.N. Conventions on the Rights of the Child (CRC) and on the Rights of Persons with Disabilities. For example, article 23 of the CRC states, “A mentally or physically disabled child should enjoy a full and decent life in conditions which ensure dignity, promote self reliance, and facilitate the child’s active participation in the community.” The preface of a 2015 report from the National Academies of Sciences, Engineering, and Medicine also expresses a contractarian approach (National Academies of Sciences, Engineering, and Medicine, 2015): “Children with disabilities in the United States, particularly those with mental, emotional, or behavioral disorders, are deserving of the highest level of planning and implementation for family support programs. Both at-risk families and society as a whole stand to benefit.” From this perspective, Durkin observed, people with disabilities are not viewed as objects of charity, medical treatment, or social protection, but as subjects with rights.
This perspective recognizes that health has multiple determinants and that much more than just medical care affects the functioning and well-being of people with disabilities. It calls for a restructuring of society to be more inclusive and accepting of people with disabilities for them to be able to achieve their ultimate capabilities.
It remains to be seen whether implementation of the Affordable Care Act will take a more utilitarian approach, Durkin noted. How can more be done with less? How can this be done most efficiently? The needs of children and families with special health care needs might not be met under such a system, she said, unless special efforts are made to do so.
DEFINITIONS OF DISABILITY AND RESEARCH GAPS
Definitions of disability in policies differ. The ADA defines disability as a physical or mental impairment that substantially limits one or more major life activities of an individual, with an expected duration of not less than 6 months.1 The Supplemental Security Income Program defines disability as “a medically determinable physical or mental impairment, which results in marked and severe functional limitations, and which can be expected to result in death or which has lasted or can be expected to last for a continuous period of not less than 12 months.”2 The CSHCN states that disability is consequence based and characterized by the need for or use of health care or special education for chronic conditions.
__________________
1 ADA Amendments Act of 2008, PL 110-325 (S 3406), 42 U.S.C. § 12102.
2 Social Security Act, Title II, § 223(d)(2)(A), and Title 16, § 1614(a)(3)(B).






