
Proceedings of a Workshop
|
May 2017 |
IN BRIEF | |
Training the Future Child Health Care Workforce to Improve Behavioral Health Outcomes for Children, Youth, and Families
Proceedings of a Workshop—in Brief
Childhood diagnoses of cognitive, affective, and behavioral disorders are increasing in both absolute numbers and as a proportion of the total childhood population in the United States, and they are imposing a large and growing burden on children, youth, and families.1 However, the adoption of evidence-based interventions that have proven effective in preventing and treating behavioral health disorders in children has been slow.2 A contributing factor for this slow adoption may be that current training in many fields involving the behavioral health of children is falling short of meeting their needs.
To examine workforce development across the range of health care professions working with children and families, as well as to identify innovative training models and levers to enhance training, the Forum on Promoting Children’s Cognitive, Affective, and Behavioral Health held a workshop on November 29-30, 2016, “Training the Future Child Health Care Workforce to Improve Behavioral Health Outcomes for Children, Youth, and Families.” The main objective of the workshop was to examine the development and training of an integrated health care workforce that can promote family-focused behavioral health care for children and their families. As noted by Laurel K. Leslie, vice president of research at the American Board of Pediatrics, professor of medicine, pediatrics, and community medicine and public health at Tufts University School of Medicine, and cochair of the planning committee for the workshop, the nature and extent of this training can have a critical effect on care. “Between what is known and what is done is what is taught,” she said.
___________________
1The National Academies of Sciences, Engineering, and Medicine. (2015). Mental Disorders and Disabilities Among Low-Income Children. Washington, DC: National Academies Press.
2Institute of Medicine and National Research Council. (2014). Strategies for Scaling Effective Family-Focused Preventive Interventions to Promote Children’s Cognitive, Affective, and Behavioral Health: Workshop Summary. Washington, DC: National Academies Press.
VOICES OF PARENTS
The workshop’s first panel featured five parents, because “the experts are the parents, who really know day to day what is needed for their child with a behavioral health issue,” said Deborah Klein Walker, president of the Global Alliance for Behavioral Health and Social Justice and senior fellow at Abt Associates. All of the panelists pointed in particular to ways in which persisting stigma contributed to challenges in accessing, paying for, and participating in behavioral health treatment.
![]()
For Rebecca Mueller, her experience started when her son began to have difficulties during play groups and preschool. She and her husband had him tested and received a diagnosis of attention deficit hyperactivity disorder (ADHD). The next year, they were able to enroll their son in a subsidized study of a program called The Incredible Years. Once a week, the Muellers traveled to a meeting and spent several hours learning how to meet their son’s needs. He also went to classes that taught him how to manage his emotions, stay calm, and be more aware. If they had not found that program, “I don’t know what I would have done,” she said. However, they were fortunate, in that the full costs of the program are prohibitive for many families. “We won the lottery that day,” she said.
For Robyn Kinebrew, managing the medical aspects of her twin sons’ sickle cell disease was straightforward, but the emotional and behavioral aspects of their care were problematic. When her sons had a sickle cell crisis, they suffered from severe pain, and the unpredictable course of their symptoms put a great deal of stress on the entire family. They eventually began to see a therapist to work on pain management techniques separate from their primary clinicians’ treatment, but Kinebrew and her sons have had to overcome feelings of embarrassment about seeking help for behavioral health issues. Today, her feelings “have evolved and changed,” she said. “I will continue to encourage other families to use a mental health therapist. It helps.”
When Breck Gamel was 38 weeks pregnant with her second son, his colon burst because of cystic fibrosis. Since then, he has required extensive medical care, which has been hard on the rest of her family, and especially on her older son. “Don’t forget the siblings,” said Gamel. When a child has a disorder, the entire family suffers, not just that child who is sick, and she emphasized the toll a serious illness takes on parents and other caregivers. Families and caregivers need to find a way of gaining a sense of control and advocacy, she said, so they can deal with their own mental health challenges. They also need to know where to go to get information and find people who can help them.
Lynda Gargan’s son was 2 years old when she began to notice “red flags that he might be walking a bit of a different path than some of his classmates.” But she largely lived in secrecy about the issues her son was having until a public event brought them into the open. He went on to become a successful young man, but the experience taught her about the prejudice that is still associated with behavioral health challenges. Physical health challenges tend to generate compassion, she said, but behavioral health challenges tend to make people back away. “We put our heads down. We thank God it wasn’t our child. We have some work to do on normalizing behavioral health experiences.”
Millie Sweeney described a somewhat similar experience. When her daughter began to suffer from severe anxiety, Sweeney downplayed the problem and attributed it to a phase her daughter was going through. But as her daughter approached her teenage years, her anxiety was affecting everyone in the family. A critical breakthrough was the discovery that Sweeney’s daughter could channel her anxious energy into dance. “She’s learned coping skills through therapy, because the therapist partnered with us.” The benefits of the partnership demonstrate the importance of parents “as a critical emerging workforce in behavioral health,” Sweeney said. Support from parents and peers “can enhance any other service that’s going on.”
THE NATIONAL LANDSCAPE
The workforce involved in promoting children’s cognitive, affective, and behavioral health is broad and varied. It includes pediatricians, adult and child psychiatrists, family medicine physicians, obstetricians and gynecologists, nurses, social workers, community and public health professionals, and parents who have been trained to fill professional roles. However, Angela Beck, director of the Behavioral Health Workforce Research Center at the University of Michigan School of Public Health, pointed out that the field of behavioral health is in the midst of a workforce crisis for several reasons:
- an increased demand for behavioral health services,
- too few workers to meet the demand,
- a poorly distributed workforce,
- a need for additional training,
- an increased emphasis on integrated team-based care and treatment of co-occurring disorders, and
- a lack of systematic workforce data collection in behavioral health.
Source: Presentation at workshop by Angela Beck. Available: http://nas.edu/healthcareworkforce.
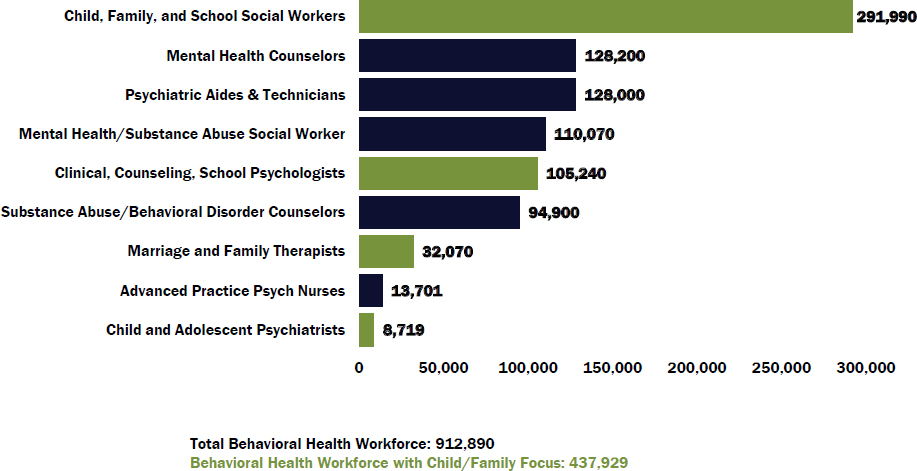
Overall, there is a shortage of trained professionals. More than 900,000 core licensed professionals work in behavioral health, including psychiatrists, psychologists, marriage and family therapists, social workers, licensed professional counselors, and psychiatric nurse practitioners: see Figure 1. Beck estimated that nearly half focus on this population.
Beck reported that the behavioral health workforce does not meet current needs, and shortages will continue to be substantial through 2025 in all the professions except behavioral health nurse practitioners and physician assistants: see Table 1. The total shortage in the selected behavioral health occupations is projected to be about a quarter million workers. In addition, the workforce is aging, more workers are needed in rural areas, the workforce needs to become more diverse, and people serving specialized populations need more specialized training, Beck observed.
Table 1 National Projections of Supply and Demand for Selected Behavioral Health Practitioners by 2025
| Occupation | Supply | Demand | Difference |
| Psychiatrists | 45,210 | 60,610 | -15,400 |
| Behavioral Health Nurse Practitioners | 12,960 | 10,160 | 2,800 |
| Behavioral Health Physician Assistants | 1,800 | 1,690 | 110 |
| Clinical, Counseling, and School Psychologists | 188,930 | 246,420 | -57,490 |
| Substance Abuse and Behavioral Disorder Counselors | 105,970 | 122,510 | -16,540 |
| Mental Health and Substance Abuse Social Workers | 145,700 | 172,630 | -26,930 |
| Mental Health Counselors | 243,450 | 321,500 | -78,050 |
| School Counselors | 109,220 | 157,760 | -48,540 |
| Marriage and Family Therapists | 29,780 | 40,250 | -10,470 |
| TOTAL | 883,020 | 1,133,530 | -250,510 |
Source: Presentation at workshop by Angela Beck. Available: http://nas.edu/healthcareworkorce.
Nurses and schools are particularly valuable providers of child and family behavioral health services, noted Susan Chapman, professor in the Department of Social and Behavioral Sciences in the School of Nursing at the University of California, San Francisco. For example, psychiatric mental health nurse practitioners can provide many of the same services that psychiatrists provide, including the ability to prescribe medications. Research shows that patient satisfaction with their care has been high, she said, and they have a shorter training time than that for psychiatrists. However, there are challenges for the profession: scope-of-practice limitations can restrict their roles, recruitment and retention is sometimes difficult, a lack of awareness surrounds their roles and competencies, their salaries are generally not competitive in public settings, and they still can have difficulties being accepted by other providers on health care teams.
Peer providers–people who have used their lived experiences of recovery from mental illness or addiction and have received training to work with others—represent another segment of the behavioral health care workforce. Johanna Bergan, executive director of an organization that uses peer providers, Youth Motivating Others through Voices of Experience (M.O.V.E.), explained how the organization promotes the use of peers to infuse the youth voice in systems transformation. Forty states have statewide certification for mental health peer support, and about a third have statewide certification for substance use disorders.
Peers can provide assistance in navigating systems, support youth participation in treatment and service meetings, model positive self-advocacy and leadership, and provide guided support in individual recovery and in building resiliency. A limited amount of research points toward the value of peer support—especially youth peer support, and especially with groups such as first-generation college students and students with disabilities, said Bergan—but additional research on this topic is needed. Funding and other forms of support for that role can vary depending on the leadership within a state or with policy changes.
Christen Johnson, a fourth-year medical student who is national president of the Student National Medical Association, reminded workshop participants about why it is important to teach medical students about the situations they are likely to encounter in delivering behavioral health services. “You have to give us the tools in our toolbox to be able to do what it is we need to do.” By doing so, she said, more students are likely to be willing to go into psychiatry and psychology and work with children.
PROMISING MODELS
A variety of models have shown promise in demonstrating how to improve training in behavioral and emotional health promotion, risk prevention, and treatment, and six of them were highlighted at the workshop.
The first model presented was the online Keep Yourself Strong and Secure Fellowship Program at The Ohio State University. It provides access to mental health education for health care providers and health sciences students across the United States, emphasizing screening, assessment, accurate identification, evidence-based management, and prevention. It also has skills-building components, noted Bernadette Melnyk, associate vice president for health promotion, university chief wellness officer, professor and dean at the College of Nursing, and professor at the College of Medicine at The Ohio State University. She added: “We know that information alone usually doesn’t translate to behavior change. People have to be given time to practice these skills.”
Primary Care Family Psychology Postdoctoral Fellowship at the University of Rochester was the second model presented at the workshop. This model integrates several theories and their applications to improve the health outcomes of children and their families, said Susan McDaniel, the Dr. Laurie Sands distinguished professor of psychiatry and family medicine, director of the Institute for the Family, and associate chair of the Department of Family Medicine at the university. The fellowship, which encompasses psychology postdoctoral fellows, family medicine students, and marriage and family therapy students, combines a family systems medicine seminar, practice with families on assessment and interviewing skills with children and their families, participation on interprofessional teams, a practicum placement, and discipline-specific training. The model has worked so well, said McDaniel, that it has been adapted to pediatrics, geriatrics, neurology, obstetrics and gynecology, and surgery.
The third model comes from the Division of Child and Adolescent Psychiatry and Psychol-
ogy at the MetroHealth system in Cleveland and was described by Terry Stancin, professor of pediatrics, psychiatry, and psychological sciences at Case Western Reserve University and director of child and adolescent psychiatry and psychology and vice chair for research in psychiatry at the MetroHealth Medical Center. The program includes increased access to health care, trained psychologists in integrated pediatric and specialty care settings, enhanced the developmental and behavioral skills of pediatric residents, and prepared interprofessional teams to collaborate by more effectively integrating behavioral health into primary care. A simulated clinic provides enhanced opportunities for interns and pediatric residents to learn, featuring simulations with actors who portray a parent of a 2-year-old with tantrums, a parent of a 13-year-old with diabetes, a 17-year-old with a history of suicidal ideation and depression, and a Spanish-speaking parent with a 12-year-old who has asthma.
The fourth model presented came from the profession of social work, which is today a major provider of behavioral health services in the United States and with projections of considerable future job growth in the field. Federal funding to master’s programs has had the goal of expanding the behavioral health workforce and hiring behavioral health professionals at community health centers. The program at the University of North Carolina at Chapel Hill was described by Lisa de Saxe Zerden, senior associate dean for master’s in social work education at the university’s School of Social Work. In this program, the federal funding has gone toward training social workers to focus on the behavioral health challenges and issues of young adults and toward a leadership program for social workers.
Cherokee Health Systems, the fifth model discussed, is both a federally qualified health center and a community mental health center. Parinda Khatri, the organization’s chief clinical officer, characterized its health care approach as “behaviorally enhanced family health care.” Behaviorists are embedded in primary care clinics, and it provides a continuum of behavioral health services, because, Khatri said, “nobody should have to wait a day even to see a development psychologist or behaviorist.” A tracking system has documented increased patient, family, and provider satisfaction; improved clinical outcomes; and improved health behavior change outcomes, which has allowed the organization to gain more resources to do better work for its patients.
The last model highlighted at the workshop was on training that can develop competencies to work with chronically ill children and their families includes interdisciplinary clinical rounds, bereavement rounds, role playing, consults, and modeling. Mary Ann McCabe, associate clinical professor of pediatrics at the George Washington University School of Medicine and an affiliate faculty member in applied developmental psychology at George Mason University, described some of the innovations in the university’s program. They include outreach to new populations, multidisciplinary inpatient or outpatient programs, automatic behavioral health consults and screening, and early exposure to the issues.
ACCREDITATION, CERTIFICATION, AND CREDENTIALING
Changes in accreditation, certification, and credentialing can have an influence on the numbers and backgrounds of the individuals who deliver behavioral health care to children and families. Challenges include different practices and policies across jurisdictions, a tendency for activities to be siloed, and uncertain sources of funding to make changes.
One important trend in credentialing, and increasingly in certification, is the move toward competency-based credentialing, explained Alison Whelan, chief medical education officer at the Association of American Medical Colleges. In this context, improving behavioral health outcomes for children and families requires considering the critical competency gaps at each level of physician training. For example, she said, there are large gaps in cultural competency, an understanding of unconscious bias, and interprofessional education, all of which have been added to medical school accreditation and to medical student exams.
The certification of pediatric nurses provides another example of how oversight processes can improve the health care workforce, explained Adele Foerster, chief credentialing officer of the Pediatric Nursing Certification Board (PNCB). In 2011, PNCB launched a specialty exam for advanced practice registered nurses to validate their knowledge and competencies in providing care related to common pediatric developmental, behavioral, and mental health
conditions. In addition, behavioral and psychological concerns have ranked fourth or fifth on the pediatric nurse practitioner exam.
The American Board of Pediatrics (ABP) also has been leveraging its influence to ensure that pediatricians are appropriately trained in behavioral health care, noted Julia McMillan, emerita professor in the Department of Pediatrics at the Johns Hopkins School of Medicine. For example, the ABP and other medical boards have been developing entrustable professional activities (EPAs), which are agreed-upon lists of activities within a given specialty or subspecialty that a physician would be expected to be able to perform competently and without supervision. For example, EPA 9 (of 17 EPAs) for general pediatricians is assessment and management of patients with common behavioral and mental health problems. However, about two-thirds of pediatricians surveyed said that they lacked training in the assessment and treatment of children and adolescents with mental health problems, McMillan reported.
Accreditation of graduate medical education is another way of changing curricula, said Jeffrey Hunt, professor in the Division of Child and Adolescent Psychiatry at the Alpert Medical School of Brown University. Responding to several sources of pressure to define and assess physician competencies and outcomes, milestones were developed to move away from idiosyncratic training experiences toward more deliberate practice. For example, in child psychiatry, 22 subcompetencies have been specified, with developmental progressions and milestones at five levels: this approach has allowed gaps in curricula and assessments to be identified.
At the University of Delaware, several projects have been seeking to close the science-to-service gap, “where what we know works in the laboratory isn’t necessarily working in the community,” said Ryan Beveridge, director of the Center for Training, Evaluation and Community Collaboration and associate professor of psychological and brain sciences at the university. The goal is not only to give students more experience translating their laboratory work into the community, he said, but also for them to think “about how their community experiences, both clinically and with research, would feed back into their laboratory work so we might develop more relevant, potent, feasible interventions.”
A recent effort to formalize the work of family peer support and develop family peer support services into a recognized profession has led to the development of a consensus definition for family peer support services, noted Susan Burger, director of family peer advocate credentialing and workforce development at Families Together. Activities fall into several broad categories: outreach and information, engagement, bridging and transition support, advocacy, self-efficacy and empowerment, community connections and natural support, parent skill development, and promoting effective family-driven care. Similarly, accreditation of patient-centered medical homes can help integrate behavioral health services into primary care, noted Marci Nielsen, president and chief executive officer of the Patient-Centered Primary Care Collaborative.
OTHER CHILD-SERVING SETTINGS
Individuals in many other settings, including the education, welfare, foster care, and juvenile justice systems, work with children who have behavioral health needs, and training for these individuals can improve coordination across sectors and lead to better outcomes for children and families. An example related to schools was described by Elizabeth Connors, a clinical psychologist and assistant professor at the University of Maryland School of Medicine and a faculty member at the Center for School Mental Health. School behavioral health programs that provide a full array of evidence-based services and strategies can complement community programs that may feature a different distribution of behavioral health promotion, targeted prevention, and intensive support. The center is helping to build implementation supports for school-based professionals, while learning communities and collaboratives, such as the Collaborative Improvement and Innovation Network of the School Health Services National Quality Initiative, allow for the sharing of ideas and knowledge in rapid quality improvement cycles.
The child welfare system seeks to provide children with safety, security, and well-being, which requires addressing the effects of trauma, behavioral health problems, and family adversity, said David Kolko, professor of psychiatry, psychology, pediatrics, and clinical and translational science at the University of Pittsburgh School of Medicine. Kolko noted that screening and assessment tools are now help-
ing to inform treatment, but challenges include the scope of their use, limited psychometrics, the proven utility of these tools, and their costs. Kolko suggested that more thought be given to developing a core set of efficient and valid tools that a community can and will use to assess behavioral health problems. He also urged that child welfare workers be trained to identify behavioral health problems and refer children for evidence-based treatment.
Addressing behavioral health in the juvenile justice setting can save considerable money by providing less expensive preventive and treatment interventions before arrest, rearrest, or placement in more restricted settings, said José Szapocznik, professor of public health sciences, architecture, psychology and educational research, and counseling psychology at the University of Miami. Cities, counties, and states may offer a more viable basis for action than the federal government in current circumstances, he added.
Governments, national organizations, foundations, accreditation entities, private agency-university partnerships, youth engagement specialists, parents, and faith-based programs and partnerships can enhance or provide treatment, education, socialization, support, and protection to children and youth in residential treatment settings, observed Christopher Bellonci, a child, adolescent, and adult psychiatrist and associate professor of psychiatry at Tufts University School of Medicine. Bellonci also suggested developing a legally binding document similar to an individualized education plan for children’s behavioral health disorders. When children display any behavioral health disorder, they would undergo a standardized assessment that would determine their treatment needs, which would drive a treatment or service plan with measurable goals.
COLLABORATIVE EFFORTS
Opportunities for federal agencies, states, professional organizations, health care payers, foundations, and others to work collaboratively on issues affecting the behavioral health of children, youth, and families are limitless. At the federal level, for example, the Maternal and Child Health Bureau within the U.S. Department of Health and Human Services emphasizes workforce development across its programs, across the lifespan, and from the undergraduate to the practicing level, said Lauren Raskin Ramos, director of the bureau’s Division of Maternal and Child Health Workforce Development. Altogether, the bureau’s leadership programs reach more than 33,000 trainees annually, with the fields of psychology, public health, medicine, and social work having the most trainees. The intention, said Ramos, is to have trained professionals available anywhere that children are present.
Philanthropies can also help provide the infrastructure for the training of professional licensed behavioral health and pediatric providers. Barbara Ward-Zimmerman, an integrated care consultant and chair of the Connecticut Psychological Association’s Health Care Reform Task Force described the Child Health and Development Institute, a nonprofit subsidiary of the Children’s Fund of Connecticut. At the institute, pediatric and family medicine practitioners and behavioral health providers in the state are receiving training designed to be a catalyst for practice transformation. Over the course of 12 years, this training has helped more than 80 percent of Connecticut’s pediatric practices improve the quality of care and expand the range of services.
Because behavioral health extends across multiple sectors, reforms similarly need to extend across sectors, observed Benjamin Miller, associate professor in the Department of Family Medicine at the University of Colorado School of Medicine and director of the Eugene S. Farley, Jr. Health Policy Center. For example, he pointed out, global payments for behavioral health services could support team-based care and provide compensation for personnel, interventions, and related infrastructure specific to individual practices. The goal is to redistribute the trained professionals to settings where they are needed, such as primary care, and enable them to successfully implement evidence-based interventions.
Doug Tynan, at the American Psychological Association and a professor of pediatrics at Thomas Jefferson University, made a similar point, observing that all mental health providers need to receive training in delivering effective, evidence-based therapies in primary care settings. A wide range of programs can provide such training, he said, and progress is slowly being made to ensure that it occurs and can be paid for.
The final speaker at this session was Ellen-Marie Whelan, chief population health officer at the Center for Medicaid and CHIP Services and se-
nior advisor at the Innovation Center within the Centers for Medicare & Medicaid Services. She said that such reforms as value-based purchasing, accountable care organizations, episode-based payments, medical homes, and a focus on quality and cost transparency can all affect training and care. At the same time, the federal government has been working with the states to clarify issues involving the behavioral health workforce, such as encouraging states to provide a continuum of care for children with behavioral health conditions, she said.
POSSIBLE NEXT STEPS
In the final session of the workshop, participants met in eight breakout groups to discuss ideas to move workforce issues forward and the stakeholders that need to be involved in these efforts. These possible next steps were offered as suggestions intended to stimulate further discussion of the best ways to prepare and maintain the workforce needed to enhance the cognitive, affective, and behavioral health of children. Each of the breakout sessions focused on one of eight topics:
- behavioral health promotion and risk prevention through multigenerational surveillance;
- incorporating exposure to evidence-based practices into content and assessment of training programs focused on the need for changing systems to support implementation;
- fostering integrated, interprofessional care;
- training the future child health care workforce to meet the needs of children with disabilities and chronic medical conditions;
- engaging patients and parents in copromotion of behavioral health to improve care;
- enhancing training through the power of accreditation, certification, and credentialing;
- enhancing training for health care professionals to improve the behavioral health of children, youth, and families involved in other child-serving systems; and
- how current reimbursement for training and clinical care impacts the focus on behavioral health for children, youth, and families.
Multigenerational Surveillance
The group that considered behavioral health promotion and risk prevention through multigenerational surveillance explored ideas around competencies, curriculum development, and training programs. Walker reported ideas generated by the session: (1) Discipline-specific competencies could be reviewed for behavioral health promotion and risk prevention through multigenerational surveillance to identify cross-disciplinary overlap and gaps, with any competencies that have gaps being updated (examples of competencies include taking complete family histories, parent/family involvement, positive parenting, motivational interviewing, and care across the continuum from prevention to treatment). (2) Curricula, tools, programs, and centers could be developed to incorporate competencies in training. (3) Federal training grant programs for child behavioral health could be expanded.(4) Stakeholders might include families and the public; providers of behavioral health care for children and youth in any setting; education and accreditation organizations; and foundations, Congress, and other funders.
Exposure to Evidence-Based Practices
In the breakout group that considered incorporating exposure to evidence-based practices into content and assessment of training programs, Hendricks Brown, Northwestern University, reported the following ideas from this session for changing systems to support implementation, including the importance of input, agreement, and engagement from community organizations who are implementing evidence-based practices within their local communities: (1) A shared work plan could be developed for embedding training on evidence-based practices into educational change efforts. (2) A “lessons learned” document could be created on the incorporation of evidence-based practices into training systems. (3) Workshops could be held on the development and roles of backbone and intermediary organizations that can support and sustain systems change. (4) Stakeholders might include research funders and programs; intermediary organizations; city, state, and regional governmental organizations (including the National Association of State Alcohol and Drug Abuse Directors and the National Association of State Mental Health Providers); and federal agencies.
Fostering Integrated, Interprofessional Care
The group that considered fostering integrated, interprofessional care focused on advocacy for training models as well as incorporating these models in preprofessional education. Harolyn Belcher, a member of the workshop planning committee, reported the following ideas from this session: (1) Multiple sectors and populations could be engaged in advocating for and participating in integrated interprofessional health care training experiences, including discipline-specific training funders, developers, and implementers. parents and patients; community providers; insurance companies; and faith-based communities. (2) Integrated, interprofessional health care education and training opportunities could be included in preprofessional education and in clinical training experiences. (3) Integrated, interprofessional care could be developed in settings defined both physically and culturally. (4) Stakeholders might include the American Psychological Association, the members of the Integrated Primary Care Alliance, the Centers for Medicare & Medicaid Services, education and accreditation organizations, and insurance companies.
Meeting the Needs of Children with Disabilities and Complex Health Conditions
For the group that focused on training the future child health care workforce to meet the needs of children with disabilities and complex health conditions, McCabe reported ideas generated by the discussion: (1) Alternative payment models could be created that are consistent with transdisciplinary and interprofessional training and practice. (2) Available models and metrics could be mobilized on the cost effectiveness and health outcomes of preventive models of care for children with disabilities and chronic medical conditions. (3) Quality training experiences could be developed and disseminated across the career span that broaden exposure to lived experiences with diverse family situations and cross-sectoral partnerships. (4) Stakeholders might include families, providers, education and system administrators, payers, and policy makers.
Engaging Patients and Parents
For the group that considered engaging patients and parents in copromotion of behavioral health to improve care, the discussion centered on the need for parent and family engagement in all aspects of training as well as identifying measurable outcomes of their involvement. Kristina West, Office of the Assistant Secretary for Planning and Evaluation, reported ideas from this discussion: (1) Families could be engaged in all aspects of training programs, such as advisory boards, training simulation models, and the development of clinical care satisfaction surveys. (2) Gaps and best practices could be identified for parent and patient involvement, including payment incentives. (3) Outcomes of parent and patient involvement could be measured, including culture change in organizations and systems. (4) Stakeholders might include parents and patients, practitioners and administrators, whole systems, professional associations, and federal agencies.
Accreditation, Certification, and Credentialing
Two ideas from the discussion of enhancing training through the power of accreditation, certification, and credentialing, were reported by Costella Green, Substance Abuse and Mental Health Services Administration: (1) Accreditation models and financing could be prioritized by the Forum on Promoting Children’s Cognitive, Affective, and Behavioral Health, thereby helping to change medical education from the beginning to develop an effectively trained workforce. (2) Stakeholders might include policy makers, funders, accrediting officials, consumers and families, students in the health professions, faculty, and schools.
Other Child-Serving Systems
The group that considered enhancing training for health care professionals to improve the behavioral health of children, youth, and families involved in other child-serving settings focused on systems transformation and team development. Szapocznik reported on ideas from individual group participants: (1) Systems could be transformed to create a culture of shared benefits through such tools as three-dimensional matrixes of competencies (reflecting disciplines, settings, and systems). (2) As part of this transformation, trainees could be taught to become facile with system transformation and to work in teams. (3) Practice coaching could be provided to support the development of teams and system transformation. (4) Stakeholders might include payers, policy makers, competency-developing organizations,
education and health care organizations, and the National Academies of Sciences, Engineering, and Medicine (as not only a competency-developing, but also convening organization).
Reimbursement for Training and Clinical Care
Ideas that emerged from the group discussion of how current reimbursement for training and clinical care affects the focus on behavioral health for children, youth, and families, were reported by Mary Jane Rotheram-Borus, University of California, Los Angeles: (1) Positive models of value-based care could be evaluated and identified that optimizes a broad range of outcomes and ensure quality improvement. (2) Incentives could be created for training programs, systems, and accrediting agencies to shift their programs to enhance the delivery of optimal and cost-effective care. (3) Stakeholders might include payers and businesses (including such groups as the Pacific Business Group on Health, the National Coalition on Heath Care, the United States Chamber of Commerce, and America’s Health Insurance Plans), teams from academic institutions that conduct training, foundations and institutes that fund innovative care models, and organizations like the National Alliance on Mental Illness.
PLANNING COMMITTEE FOR THE WORKSHOP TRAINING THE FUTURE CHILD HEALTH CARE WORKFORCE TO IMPROVE BEHAVIORAL HEALTH OUTCOMES FOR CHILDREN, YOUTH, AND FAMILIES
THOMAS F. BOAT (Cochair), University of Cincinnati College of Medicine and Cincinnati Children’s Hospital Medical Center; LAUREL K. LESLIE (Cochair), American Board of Pediatrics and Tufts University School of Medicine; HAROLYN M.E. BELCHER, Johns Hopkins University School of Medicine and Kennedy Krieger Institute; GREGORY FRITZ, Bradley Hasbro Children’s Research Center; BIANCA K. FROGNER, University of Washington; ELIZABETH HAWKINS-WALSH, Catholic University of America; KIMBERLY EATON HOAGWOOD, Society of Clinical Child and Adolescent Psychology, American Psychological Association; and Department of Child and Adolescent Psychiatry, School of Medicine, New York University; MARSHALL “BUZZ” LAND, JR., American Board of Pediatrics and University of Vermont; MARY ANN McCABE, Society for Child and Family Policy and Practice; Society of Pediatric Psychology; School of Medicine, George Washington University; and Affiliate Faculty in Psychology, George Mason University; and SARAH M. TRACEY, Study Director.
DISCLAIMER: This Proceedings of a Workshop in Brief has been prepared by Steve Olson, rapporteur, as a factual summary of the presentations and discussion at the workshop. The statements made are those of the individual speakers and do not necessarily represent the views of all participants, the planning committee, or the National Academies of Sciences, Engineering, and Medicine. The planning committee was responsible only for organizing the workshop, identifying the topics, and choosing speakers.
REVIEWERS: To ensure that it meets institutional standards for quality and objectivity, this Proceedings of a Workshop in Brief was reviewed by Bianca K. Frogner, Center for Health Workforce Studies, Department of Family Medicine, University of Washington, and Jeffrey Hunt, Child and Adolescent Psychiatry Fellowship and Combined Program in Pediatrics, Psychiatry, and Child Psychiatry, Alpert Medical School, Brown University. Patricia L. Morison, Division of Behavioral and Social Sciences and Education, served as review coordinator. The review comments and draft manuscript remain confidential to protect the integrity of the process.
SPONSORS: The Forum on Promoting Children’s Cognitive, Affective, and Behavioral Health is partially supported by the American Academy of Pediatrics; the American Board of Pediatrics; the American Psychological Association; Autism Speaks; U.S. Department of Health and Human Services, Assistant Secretary for Planning and Evaluation; the Conrad N. Hilton Foundation; Community Anti-Drug Coalitions of America; the Centers for Disease Control and Prevention; Department of Justice; the Hogg Foundation for Mental Health; Global Alliance for Behavioral Health and Social Justice; the Robert Wood Johnson Foundation; the Society for Child and Family Policy and Practice; the Society of Clinical Child and Adolescent Psychology; the Society of Pediatric Psychology; Substance Abuse and Mental Health Services Administration.
For additional information regarding the meeting, visit http://nas.edu/healthcareworkforce.
Suggested citation: National Academies of Sciences, Engineering, and Medicine. (2017). Training the Future Child Health Care Workforce to Improve Behavioral Health Outcomes for Children, Youth, and Families: Proceedings of a Workshop—in Brief. Washington, DC: The National Academies Press. doi: https://doi.org/10.17226/24789.
FORUM ON PROMOTING CHILDREN’S COGNITIVE, AFFECTIVE, AND BEHAVIORAL HEALTH
WILLIAM R. BEARDSLEE (Cochair)
Boston Children’s Hospital and Harvard Medical School
C. HENDRICKS BROWN (Cochair)
Feinberg School of Medicine, Northwestern University
KAREEMAH ABDULLAH
Community Anti-Drug Coalitions of America
DARA BLACHMAN-DEMNER
National Institute of Justice, U.S. Department of Justice
THOMAS F. BOAT
Cincinnati Children’s Hospital Medical Center
FELESIA R. BOWEN
School of Nursing, Rutgers University
DAVID A. BRENT
School of Medicine, University of Pittsburgh
LAUREN CALDWELL
American Psychological Association
ALEXA EGGLESTON
Conrad N. Hilton Foundation
RICHARD G. FRANK
U.S. Department of Health and Human Services
COSTELLA GREEN
Substance Abuse and Mental Health Services Administration, U.S. Department of Health and Human Services
RICK HARWOOD
National Association of State Alcohol and Drug Abuse Directors
J. DAVID HAWKINS
School of Social Work, University of Washington
KIMBERLY EATON HOAGWOOD
Society of Clinical Child and Adolescent Psychology and New York University
COLLEEN HORTON
Hogg Foundation for Mental Health, University of Texas at Austin
JENNIFER W. KAMINSKI
U.S. Centers for Disease Control and Prevention
KELLY J. KELLEHER
Nationwide Children’s Hospital
UMA KOTAGAL
Cincinnati Children’s Hospital Medical Center
LAUREL K. LESLIE
American Board of Pediatrics and Tufts University School of Medicine
MARY ANN MCCABE
Society of Pediatric Psychology, Society for Child and Family Policy and Practice, George Washington University, and George Mason University
JENNIFER NG’ANDU
Robert Wood Johnson Foundation
LAWRENCE A. PALINKAS
School of Social Work, University of Southern California
MARY JANE ROTHERAM-BORUS
University of California, Los Angeles
JOYCE K.SEBIAN
Substance Abuse and Mental Health Services Administration, U.S. Department of Health and Human Service
PAT SHEA
National Association of State Mental Health Program Directors
ANDY SHIH
Autism Speaks
JOSÉ SZAPOCZNIK
University of Miami
VERA FRANCIS “FAN” TAIT
American Academy of Pediatrics
JENNIFER TYSON
Office of Juvenile Justice and Delinquency Prevention, U.S. Department of Justice
DEBORAH KLEIN WALKER
American Orthopsychiatric Association and Abt Associates
For additional information about the Forum, visit http://nas.edu/ccab.
Division of Behavioral and Social Sciences and Education
![]()
Copyright 2017 by the National Academy of Sciences. All rights reserved.












