
5
International Approaches to Occupational Health Surveillance
An exploration of the occupational safety and health surveillance systems of other nations is useful in informing the design and development of occupational health and safety efforts in the United States. Although no other national surveillance system is directly comparable, primarily due to the structure of the workers’ compensation system in the United States, an overview of the characteristics of some of these systems informs possibilities for the evolution of the U.S. system. This chapter follows the organization of the previous chapter and is structured according to four general categories: occupational fatalities, occupational injuries and acute illnesses, occupational disease, and hazards and exposures. The work of Tedone (2017) was a useful resource in developing this chapter.
OCCUPATIONAL FATALITIES
The Census of Fatal Occupational Injuries (CFOI) system (described in Chapter 4) for identifying all occupational injury fatalities in the United States is different from and likely more comprehensive than those in other industrialized nations. For example, the major difference between CFOI and fatal occupational injuries published by countries contributing data to Eurostat is that the CFOI is an active surveillance system and Eurostat relies on passively reported fatalities (Benavides et al., 2003). As a consequence, it is believed that the CFOI system provides a more complete assessment of fatalities from work. Australia maintains a Work-Related Traumatic Injury Fatalities system that, like CFOI, collects reports of fatal injuries from a variety of sources (Safe Work Australia, 2017a). The Australian
system also includes as work fatalities those that occur when commuting to or from work.
OCCUPATIONAL INJURIES
Occupational injury surveillance generally includes both traumatic injuries and acute occupational disease. Surveillance of most chronic occupational disease is considered below. Musculoskeletal disorders are often managed as injuries although they may result from repetitive trauma over time.
Occupational injury surveillance is managed in a variety of different ways by different countries. Differences include source of data, types of injuries covered, and work population exclusions. In general, there are two types of approaches and often countries will use a combination of these: compensation-based and noncompensation schemes. The scope and coverage of each national scheme varies somewhat depending on the source of data used for surveillance: employer records (establishment surveys), employee interviews (household or labor force surveys), administrative compensation data (workers’ compensation), and regulatory reporting (mandated reports to enforcement authorities). As illustrated below, those countries with mandatory accident insurance generally use records of compensation as the primary source of occupational injury data. By contrast, the United States relies more on regulatory reporting, databases, and statistical methodologies such as surveys (Walters, 2007).
Workers’ Compensation
Many developed nations have some type of national compensation scheme often integrated with their national health systems. Although the specific coverages vary by country the compensated injuries provide counts of injuries that qualify. These systems are passive but have national scope and, in that way, are quite different from the state-based systems in the United States. Canada is the exception, having a provincial-based system where accepted workers’ compensation claims may differ among provinces. Nonetheless, accepted claims are forwarded to a single source using a common format concerning standard data elements for collating and reporting on compensated injuries (AWCBC, 2017). The European Union (EU) members have agreed to a standard for reporting occupational injuries that account for a minimum of 3 days away from work (Eurostat, 2017a). Australia nonfatal injury reports include only cases that have been accepted for workers’ compensation and have a minimum of 1 week away from work (Safe Work Australia, 2017b). New Zealand occupational injury reports include data from all accepted claims along with a subgroup of those
claims characterized by disability or time away from work (WorkSafe New Zealand, 2017). Japan collects compensated case information for those with 4 or more days away from work (JISHA, 2017).
Establishment Surveys
The committee identified several surveys worldwide that, similar to the Survey of Occupational Injuries and Illnesses, use a statistical sample of employers annually to collect records of occupational injuries or acute diseases. Japan conducts two different surveys, one for general industry and one for the construction industry. These surveys are limited to establishments of 10 or more employees and in general published data are provided for establishments with 100 or more employees (Japan Ministry of Health, Labour, and Welfare, 2017). The response rate for this survey is not reported. Although the European Union has no common requirement for an establishment survey, some countries undertake such an effort. The Netherlands National Organisation for Applied Scientific Research, for example, undertakes a periodic survey of employers (Employers’ Labour Survey) but the response rate has been low. The committee did not identify work establishment surveys in Canada, Australia, and New Zealand that collect occupational injury statistics.
Labor Force Surveys
Many countries supplement occupational injury information obtained from workers’ compensation systems with reports from a household survey. The prime example of this approach is represented by the United Kingdom’s (UK’s) Labour Force Survey (LFS). The LFS was developed as a condition of membership in the European Union with a purpose “. . . to provide information on the UK labour market which can then be used to develop, manage, evaluate and report on labour market policies” (HSE, 2017a). The Self-reported Work-related Illness (SWI) and Workplace Injury modules were introduced in 1990 and these have become annual since 1993. The modules include a core set of questions for those aged 16 or over who are currently employed or who have been employed in the previous year. The LFS is considered the preferred source (see Table 5-1) for occupational injury data in the UK because “data from the LFS represents the views of workers, providing a more complete view than RIDDOR, as it is not subject to changes in legislation or operational activity, nor subject to substantial levels of under reporting” (HSE, 2017b). These characteristics of a population survey are an important input for estimating burden of occupational injury.
Australia, in addition to its compensation-based primary source of work-related injuries (see above), has supplemented its labor force survey
TABLE 5-1 UK Preferred Sources for Injuries and Illnesses
| These ratings provide a general indication of the source’s strength for most purposes. Please note that there may be a preferred source for a particular item, but another source may be more appropriate for a particular data breakdown of the item. | ||||||||
| Strength of Source: |
||||||||
| Other So uree(s) Nature of Harm | Preferred Source |
Other Source(s) | ||||||
| Injuries | LFS | RIDDOR | ||||||
| Common conditions arising in a wide range of occupational settings | ||||||||
| Musculoskeletal disorders | LFS | THOR-GP | ||||||
| Stress | LFS | THOR-GP | IIDB | |||||
| Common conditions arising in a limited range of occupational settings | ||||||||
| Asthma | SWORD | THOR-GP | IIDB | LFS | ||||
| COPD | AF | IIDB | SWORD | |||||
| Cancer | AF | IIDB | SWORD | EPIDERM | ||||
| Noise induced hearing loss | AF | LFS | IIDB | |||||
| Skin disorders / dermatitis | EPIDERM | THOR-GP | LFS | IIDB | ||||
| Specific or rare conditions arising in a limited range of occupational settings | ||||||||
| Asbestos-related lung cancer | AF | SWORD | IIDB | |||||
| Diffuse pleural thickening | IIDB | SWORD | ||||||
| Hand-arm vibration | AF | IIDB | ||||||
| Mesothelioma | DC | IIDB | ||||||
| Pneumoconiosis & silicosis | IIDB | SWORD | DC | |||||
| Other respiratory disease | SWORD | IIDB | DC | |||||
|
Acronym Key
|
||||||||
SOURCE: HSE, 2017b.
with questions on occupational injury and acute illnesses periodically (2005-2006, 2009-2010, and 2013-2014) (Australian Bureau of Statistics, 2013). Some limited information is also collected as part of the Survey of Employment Arrangements and Superannuation and the National Health Survey. The European Union has an extensive system of labor force surveys that are based on household sample and provides results quarterly on aspects of labor force participation (Eurostat, 2017b). These surveys
are carried out by each member country according to a common format and structure then centrally managed by Eurostat. These surveys have been supplemented with modules about work injuries in 2007 and 2013. In addition, the European Foundation for the Improvement of Living and Working Conditions conducts European Working Conditions Surveys (see discussion below).
Mandated Reporting
The United Kingdom uses a reporting program, the Reporting of Injuries, Diseases and Dangerous Occurrences Regulations (RIDDOR), which obligates the employer or self-employed individual to report fatalities, injuries, or illnesses of specific types, and incidents that could lead to serious harm. The RIDDOR system serves as a secondary source of information for estimates of burden but primarily provides information to enhance prevention and to inform actions by the Health and Safety Executive (HSE) to address risk reduction in workplaces (HSE, 2017c). New Zealand supplements its compensation data with reports of serious injury outcome indicators that are derived according to public health categories of national importance (assaults, work-related injuries, suicide and intentional self-harm, falls, motor-vehicle injuries, and drowning or near drowning) (Statistics New Zealand, 2014). Serious injury outcome indicator events are collected from national mortality and hospital discharge systems. Among the international occupational and safety health surveillance systems examined by the committee, these are the only two national noncompensation-based mandatory systems.
Injuries that Occur During Commuting to Work
Injuries that occur during commuting to work is a category of work-related injury that is not dealt with consistently by the different national occupational injury systems. Apart from England and Ireland, European nations include road traffic injuries in their occupational statistics. In the United States, road traffic injuries are not included in occupational safety and health (OSH) surveillance systems if the fatality occurred while commuting or as a bystander. Many European nations, however, count commuting injuries as one category of occupational injuries. A summary of experience from Belgium, Finland, France, and Germany reported that between 10 and 15 percent of occupational injuries occur as a result of commuting and approximately 45 percent of fatalities were related to commuting (Munich Re Group, 2004). There is some evidence that commuting distances to work are increasing (Jarosz and Cortes, 2014; Kneebone and Holmes, 2015), which increases the probability that commuting collisions
will occur. Furthermore, one study from France found differential risk of commuting injuries among certain work groups. Women employed in health and community service professions had a threefold excess risk of a commuting accident and male sales workers had a sixfold risk (Hours et al., 2011). Consideration needs to be given to include commuting fatalities and injuries as work related.
OCCUPATIONAL DISEASE
Surveillance of occupational disease is challenging for a number of reasons that apply in many countries. An underlying challenge is the lack of knowledge by general practitioners and medical specialists about the role of work as a primary factor or as one of several factors that can cause or exacerbate disease. This problem is compounded by whether the physician reports the occupational disease, how physicians understand the compensation system, and the efficiency of the reporting system. Furthermore, patient care-seeking behavior may or may not be coupled with whether the patient reports the possibility of an association of symptoms with work. There may also be additional factors that can hamper occupational disease surveillance, including employer pressures on physicians and workers not to report the relationship of a disease with work, workers’ fears of the consequences of reporting, and undeclared or informal work.
Schedules of Occupational Diseases
The challenges noted above have led many nations to rely on schedules (lists) of occupational diseases such as those developed by the European Union or the International Labour Organization (ILO) as the primary means of identifying the work relationship of a disease (ILO, 2010; European Agency for Safety and Health at Work, 2017). Many of the diseases are included because they are associated with specific work-related exposures known to cause the disease. Schedules are established on a national basis and primarily serve to identify conditions that are eligible for workers’ compensation (European Commission, 2013). There is variation among countries in the list of occupational diseases and in the presumption of work-related origin. The lists of occupational diseases developed by both the EU and the ILO are similar, with the EU making a distinction between recognized and suspected diseases and ILO combining both in one list. Since 2003, five EU members have adopted the full EU list while the rest vary in what is considered an occupational disease. The data for the reporting of occupational diseases is primarily derived from the compensation or social security system while a few use an independent system. Underreporting was assessed in a EUROGIP study (2015) where the experience in five countries
that represented the diverse insurance models were compared. A fourfold difference was seen between the highest and lowest claim rates and, although in different relative proportion, the same diseases led reporting in all countries: musculoskeletal disorders, hearing loss, skin diseases, and cancer.
Canada collects evidence of occupational diseases through its compensation system. Although there is a reporting requirement for employers to report occupational diseases that they become aware of, this system is likely much less useful than the reports from the compensation programs. A summary assessment of occupational diseases suggests that “[v]irtually every board in Canada would accept any of the 29 groups of occupational diseases recognized by the International Labour Organization as being work-related, but acceptance of less well-established conditions, such as suspected but not proven causes of cancer, would vary among the boards” (Guidotti, 2013). Japan appears to collect information on occupational disease through their compensation system (physician reporting is not mandated) and utilizes a form of a list for eligible conditions (Takahashi and Ishii, 2014). New Zealand uses a list of occupational diseases coupled with a voluntary notification system (Armstrong and Bunn, 2012). Reviews of occupational disease reporting in New Zealand suggested that only the compensation statistics were useful and those underestimated the true count (Driscoll et al., 2004; Pearce et al., 2005).
Multisystem Approaches
The United Kingdom has the most comprehensive approach to occupational disease surveillance that includes required reporting of one of eight conditions included in a published list, reports of cancer or acute infectious diseases meeting minimal criteria, and reports from a voluntary physician reporting system called The Health and Occupation Research (THOR) network (Carder et al., 2017). The occupational diseases required to be reported by employers and the self-employed are carpal tunnel syndrome, severe cramp of the hand or forearm, occupational dermatitis, hand-arm vibration syndrome, occupational asthma, tendonitis or tenosynovitis of the hand or forearm, any occupational cancer, and any disease attributed to an occupational exposure to a biological agent. Cancer cases are reported if there is an established link and the worker was exposed to the agent(s). Illness due to a biological agent is reportable if it occurs in association with an accident that created likely exposure or an infection reasonably associated with a work exposure. Guidance is provided for each of these categories (HSE, 2017d).
The THOR physician reporting approach is innovative and includes reports of any occupational disease by general practitioners and specific occupational conditions by specialist physicians. THOR-GP began in 2005
and utilizes more than 200 general practitioners as the source of reports of occupational disease. These reporters have received postgraduate education in occupational medicine and practice and are distributed throughout the United Kingdom. Currently these physicians are asked to report conditions that “more likely than not” are work related. They do so for one randomly selected month each year. Audits of the system suggest that underreporting is common due to the small number of reporters (approximately 1 percent of general practitioners in the United Kingdom), only captures conditions seen in practices of general practitioners, and depends on patient care-seeking and reporting behavior. However, efforts have been made to estimate burden from these reports, which help focus revisions to the system (Hussey, 2016).
THOR specialist reporting schemes have been introduced for several conditions and two appear to be particularly successful: Surveillance of Work-related Occupational Respiratory Disease (based on reports from respiratory disease specialists) and the skin specialist surveillance scheme (EPIDERM) (based on reports from consultant dermatologists). Both have proved useful in characterizing the distribution and burden of the two conditions (HSE, 2016a,b). Both schemes suffer the same limitations as THOR-GP but the reporting appears more consistent and has led to useful investigations (Stocks et al., 2011; Warburton et al., 2015). Nonetheless, the HSE considers these two systems superior to the Labour Force Survey for occupational asthma and skin disorders (Table 5-1). Other efforts, no longer operating, have focused on occupational physicians and rheumatologists.
The THOR system has notably been explored for surveillance of mental health with some success. From 1999-2009, an effort was organized for reporting by consultant psychiatrists to the Surveillance of Occupational Stress and Mental Illness program. Over 3,500 case reports were used by the HSE to identify areas and occupational categories at greatest risk from occupational mental ill-health. During the same period and continuing today, the general practitioners participating in THOR-GP also reported cases of mental ill-health among their patients. Examination of the mental health burden of work suggests that these reporting schemes prove useful in surveillance of mental health at work (Agius and Turner, 2004; Hussey et al., 2013; Zhou et al., 2017).
WORK HAZARDS OR EXPOSURES
Most occupational health surveillance focuses on outcomes rather than exposures or hazards. While this proves less of a problem for occupational injuries, which are acute events, its importance is evident when considering work-related diseases. Many occupational diseases result long after the exposures are initiated or even well after employment with the relevant
exposure ceases. Therefore, currently diagnosed occupational diseases often reflect exposures that occurred in the past. Formal study of these conditions may improve understanding of the etiology but exposure (and therefore risk) continues. When the exposure-disease connection is known, tracking these exposures and acting to reduce or eliminate them is a sound public health approach (see Chapter 6).
Finnish Job Exposure Matrix
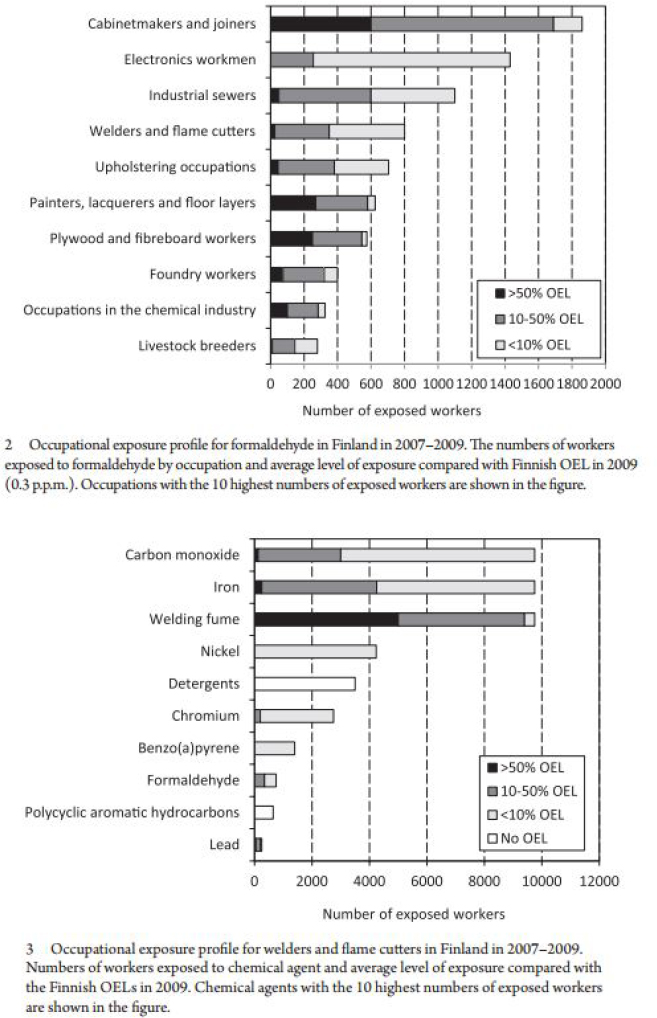
The Finnish Job Exposure Matrix (FINJEM) provides an example of a surveillance system focused on assessing the extent of worker exposure to chemical and physical agents. Estimates from FINJEM of the extent of exposures experienced by Finnish workers are used as the national source for quantitative risk assessments (Kauppinen et al., 2014). Updated exposure estimates are provided every 3 years for most agents (Kauppinen et al., 2014). Cross-sectional data, data on exposure trends over time, and exposure profiles by occupation and agent are provided by FINJEM. Figure 5-1 shows examples of chemical exposure profiles (Kauppinen et al., 2014). To identify possible hazardous exposures by occupation and agent, these exposure estimates are compared with Finnish occupational exposure limits (Kauppinen et al., 2014).
FINJEM’s trend information and exposure estimates have also been used to explore the extent of potential future attributable cases in Finland and have also been used in a European project that is examining the potential consequences of changing the occupational exposure limits of some carcinogens (Rushton et al., 2008; Kauppinen et al., 2014). The European project primarily used the methods for risk assessment developed in the United Kingdom and the industry-based CARcinogen EXposure (CAREX) system approach.
An analysis of the trends and potential trends of work-related exposure to 41 chemical agents in Finland from 1950 to 2020 used the following four metrics to calculate national exposure: the prevalence of exposure, the prevalence of high levels of exposure, the average level of exposure, and the national occupational inhalation exposure (Kauppinen et al., 2013). An estimate of dermal exposure was determined based on the number and extent of occupational skin diseases. From 1950-1970, it was found that there was a general pattern of increased exposure, followed by a decrease from 1970-2008 with an expected decrease to continue from 2008 and onward (Kauppinen et al., 2014).
The developers of FINJEM also pioneered efforts to account for psychosocial stressors in job exposure matrices. The FINJEM was used in 2004 successfully to examine psychosocial work stressors and dementia in Germany (Seidler et al., 2004).
Job exposure matrices (JEMs) have also been used to assess other national trends in work-related exposures and hazards. In 2008, a Danish study used a JEM developed from the Danish Work Environment Cohort Study in a large case control study to show psychosocial job stressors were associated with anxiety disorders and with depression showing some variation by sex (Wieclaw et al, 2008). A record linkage study that linked a French JEM to a decennial health survey found a robust association of job strain with depressive symptoms (Cohidon et al, 2012). Most recently Australian investigators have validated a JEM for psychosocial stressors comparing assignments from the JEM with labor force survey responses for job stressors (Milner et al., 2016).
European Working Conditions Survey
The European Working Conditions Survey (EWCS) conducted by Eurofound since 1991 (also discussed in Chapter 6) includes the exploration of a range of working conditions including physical and social environment. The EWCS is a household survey of populations of adults selected by a multistage, stratified, random sample of the working population in each country. For most countries, the sample size is 1,000 although larger samples come from several countries with large working populations. The sixth survey was conducted in 2015 and interviewed approximately 44,000 workers, which included both employees and the self-employed. This survey included 35 European countries, which consists of 28 EU member states, 5 EU candidate countries, and Norway and Switzerland (Eurofound, 2016). Survey questions included questions related to employment status, work organization, work-life balance, health and safety, learning and training, working time duration and organization, and physical and psychosocial risk factors (Eurofound, 2016). Seven job-quality indices, representing different dimensions of job quality, are assessed: physical environment, work intensity, working time quality, social environment, skills and discretion, prospects, and earnings. The questionnaire answers allow respondents to be classified into one of ten major occupational groups and one of ten major industry groups. Results show that in the past 10 years, there has been limited progress towards improvement in some job-quality indices (Eurofound, 2016).
Reporting of Injuries, Diseases, and Dangerous Occurrences Regulations
As introduced above, the United Kingdom’s RIDDOR program examines dangerous occurrences in the workplace that may require prompt reporting. These fall into three general categories:
- An event that occurs at any workplace “involving lifting equipment, pressure systems, overhead electric lines, electrical incidents causing explosion or fire, explosions, biological agents, radiation generators and radiography, breathing apparatus, diving operations, collapse of scaffolding, train collisions, wells, and pipelines or pipeline works” (HSE, 2017f).
- Incidents occurring at any onshore workplace that involve structural collapses, explosions or fires, releases of flammable liquids and gases, and hazardous escapes of substances.
- Incidents that have characteristics that are separately specified for reporting when they occur at offshore workplaces, at mines or quarries, or at relevant transport systems (HSE, 2017e).
Conclusions
This examination of experience from other nations informs the efforts to develop a smart surveillance system for the United States. While the social systems and the political economies among the countries described differ in important ways, the lessons learned offer insights into how the United States might adapt aspects of the systems described to fill some of the gaps in our current approaches to surveillance of occupational injury and illnesses.
Fatal injury surveillance appears to be one area where the United States leads the way. The CFOI has evolved into the most comprehensive and specific system for identifying occupational fatalities with sufficient information to target intervention efforts. Surveillance of occupational commuting fatalities, however, is one area that has not been considered in the United States. Australia’s experience suggests that surveillance of these events is possible and deserves consideration in the United States.
Conclusion: Except for no access to CFOI data for case follow-up, this system for occupational fatality surveillance is internationally the most advanced.
Non-fatal occupational injury surveillance, by contrast, is better developed in other countries. Employer reports elsewhere suffer similar problems to those in the U.S. Survey of Occupational Injuries and Illnesses, with underreporting a common problem. However, other nations rely more commonly on injury information available within national workers’ compensation systems. For the most part workers’ compensation systems in the United States are private and it would be difficult to adapt these to the same purpose. On the other hand, the success of the Safety and Health Assessment and Research for Prevention (SHARP) surveillance program in Washington State provides an excellent case example of how translating the international experience to the United States has been possible.
A common source of surveillance information on nonfatal injuries in
other nations comes from labor force surveys. According to the HSE, this is the preferred source of information for occupational injuries in the UK. The Household Survey of Occupational Injuries and Illnesses (HSOII) proposed by the Bureau of Labor Statistics (BLS) is equivalent to a labor force survey although the survey is still in the planning stages with feasibility assessments under way.
Conclusion: Occupational injury surveillance in the United States lags that of other developed nations. This is in part due to the absence of a national workers’ compensation system and in part due to the absence of a comprehensive labor force survey, both which are common in many developed nations.
Surveillance of occupational disease is challenging in all countries. This is recognized to be a consequence of the universal problem of poor training of physicians in the recognition of the role of occupation in the etiology of or as a contributing cause to disease. In many countries, the surveillance of occupational disease is based on a “schedule” of occupational diseases. For those patients found to have specific jobs or exposures associated with a specific list of diseases, the presumption is the condition is occupational in origin and is to be reported as such. The schedule concept serves to facilitate allocation of health care costs to the workers’ compensation system. There is no comparable system in the United States although it might be possible to consider this approach on a state-by-state basis.
The UK model has adopted a somewhat different approach that offers some advantages and deserves scrutiny. The HSE requires direct reporting of eight specific conditions as well as reports of specific cancers or acute infectious disease when associated with known causes. This is supplemented by a voluntary physician reporting system (THOR) that has proved quite effective for select conditions. Among these are mental illnesses, conditions that are on the rise among the working population in the UK and likely in the United States. The Sentinel Event Notification System for Occupational Risks (SENSOR) system in the United States (see Chapter 4) has used variants on this system for asthma and pesticide poisoning and further developments in such an approach that could be given serious consideration.
Conclusion: Occupational disease surveillance in most developed countries relies on a “schedule” of diseases that are presumed occupational if the schedule’s known exposures are present. There is no equivalent in the United States. The voluntary physician reporting scheme in the UK offers promise and the United States has limited experience in utilizing this type of surveillance.
Hazard and exposure surveillance, especially in Europe, has made important advances, and offers promising opportunities for the United States. One approach uses job exposure matrices to group jobs into exposure categories allowing an estimation of the distribution and location of priority
hazards. Another includes the use of household surveys constructed to assess work and work exposures that can be effectively identified through worker self-reports. These have provided useful data on trends for common exposures among work populations for over two decades. Finally, there is the UK RIDDOR system that requires reporting of “dangerous occurrences without injury,” certain specified near-miss events that are well characterized in HSE documents.
Conclusion: Exposure surveillance efforts in other developed nations have proved useful for surveillance and offer significant promise for adoption in the United States.
There are several approaches used by other countries that offer case studies of approaches to occupational injury and illness reporting that could be adapted to the U.S. setting. The experience is rich with examples that can serve to guide exploration of enhanced and more robust surveillance practices in the United States toward the further development of a smart surveillance system.
REFERENCES
Agius, R., and S. Turner. 2004. Work-related mental ill health and development of the Surveillance of Occupational Stress and Mental Illness (SOSMI) reporting scheme. Psychiatric Bulletin 28:174-176.
Armstrong, H., and K. Bunn. 2012. Experience rating and occupational disease: A New Zealand case study. Policy and Practice in Health and Safety 10(1):63-75.
Australian Bureau of Statistics. 2013. Occupational injuries and disease. Chapter 15 in Labour Statistics: Concepts, Sources and Methods, 2013. Available online at http://www.abs.gov.au/ausstats/abs@.nsf/Lookup/6102.0.55.001Chapter252013 (accessed June 19, 2017).
AWCBC (Association of Workers’ Compensation Boards of Canada). 2017. About AWCBC. Available online at http://awcbc.org/?page_id=10 (accessed June 19, 2017).
Benavides, F. G., G. L. Delcios, S. P. Cooper, and J. Benach. 2003. Comparison of fatal occupational injury surveillance systems between the European Union and the United States. American Journal of Industrial Medicine 44(4):385-391.
Carder, M., L. Hussey, A. Money, M. Gittins, R. McNamee, S. J. Stocks, D. Sen, and R. M. Agius. 2017. The Health and Occupation Research Network: An evolving surveillance system. Safety and Health at Work. 8(3):231-236.
Cohidon, C., G. Santin, J. F. Chastang, E. Imbernon, and I. Niedhammer. 2012. Psychosocial exposures at work and mental health: Potential utility of a job-exposure matrix. Journal of Occupational and Environmental Medicine 54(2):184-191.
Driscoll, T., A. Mannetje, E. Dryson, A.-M. Feyer, P. Gander, S. McCracken, N. Pearce, and M. Wagstaffe. 2004. The burden of occupational disease and injury in New Zealand. Available online at http://psm-dm.otago.ac.nz/ipru/ReportsPDFs/OR057.pdf (accessed May 5, 2017).
Eurofound. 2016. Sixth European Working Conditions Survey: Overview report. Available online at https://www.eurofound.europa.eu/sites/default/files/ef_publication/field_ef_document/ef1634en1_0.pdf (accessed June 22, 2017).
EUROGIP. 2015. Reporting of Occupational Diseases: Issues and Good Practices in Five European Countries. Paris: EUROGIP. Available online at http://www.eurogip.fr/images/documents/3933/Report_DeclarationMP_EUROGIP_102EN.pdf (accessed June 21, 2017).
European Agency for Safety and Health at Work. 2017. Commission recommendation concerning the European schedule of occupational diseases. Available online at https://osha.europa.eu/en/legislation/guidelines/commission-recommendation-concerning-theeuropean-schedule-of-occupational-diseases (accessed June 19, 2017).
European Commission. 2013. Report on the current situation in relation to occupational diseases’ systems in EU member states and EFTA/EEA countries, in particular relative to commission recommendation 2003/670/EC concerning the European schedule of occupational diseases and gathering of data on relevant related aspects. Available online at https://osha.europa.eu/en/legislation/guidelines/commission-recommendation-concerning-the-european-schedule-of-occupational-diseases (accessed June 21, 2017).
Eurostat. 2017a. Eurostat methodology. Available online at http://ec.europa.eu/eurostat/web/health/methodology (accessed May 8, 2017).
Eurostat. 2017b. European Union labour force survey. Available online at http://ec.europa.eu/eurostat/web/microdata/european-union-labour-force-survey (accessed June 19, 2017).
Guidotti, T. L. 2013. Occupational diseases. In Canadian Encyclopedia. Available online at http://www.thecanadianencyclopedia.ca/en/article/occupational-diseases (accessed June 21, 2017).
Hours, M., E. Fort, B. Charbotel, and M. Chiron. 2011. Jobs at risk of work-related road crashes: An analysis of the casualties from the Rhone Road Trauma Registry (France). Safety Science 49(8-9):1270-1276.
HSE (Health and Safety Executive). 2016a. Work-related skin disease in Great Britain, 2016. Available online at http://www.hse.gov.uk/statistics/causdis/dermatitis/skin.pdf (accessed June 21, 2017).
HSE. 2016b. Work-related respiratory disease in Great Britain, 2016. Available online at http://www.hse.gov.uk/statistics/causdis/respiratory-diseases.pdf?pdf=respiratory-diseases (accessed June 21, 2017).
HSE. 2017a. About the Labour Force Survey (LFS). Available online at http://www.hse.gov.uk/statistics/lfs/about.htm (accessed June 19, 2017).
HSE. 2017b. Table of preferred sources for injuries and ill health. Available online at http://www.hse.gov.uk/statistics/preferred-data-sources.htm (accessed June 19, 2017).
HSE. 2017c. Data sources. Available online at http://www.hse.gov.uk/statistics/sources.htm (accessed May 8, 2017).
HSE. 2017d. Reportable diseases. Available online at http://www.hse.gov.uk/riddor/occupational-diseases.htm (accessed June 19, 2017).
HSE. 2017e. RIDDOR—Reporting of Injuries, Diseases and Dangerous Occurrences Regulations 2013. Available online at http://www.hse.gov.uk/riddor (accessed June 22, 2017).
HSE. 2017f. Dangerous occurrences. Available online at http://www.hse.gov.uk/riddor/dangerous-occurences.htm (accessed December 4, 2017).
Hussey, L. 2016. THOR-GP input to the HSE annual statistics, 2015/2016. Available online at http://www.hse.gov.uk/statistics/calculation-thor-gp-data.pdf (accessed June 19, 2017).
Hussey, L., M. Carder, A. Money, and R. Agius. 2013. Comparison of work-related ill-health data from different GB sources. Occupational Medicine 63(1): 30-37.
ILO (International Labour Organization). 2010. ILO list of occupational diseases (revised 2010). Available online at http://www.ilo.org/safework/info/publications/WCMS_125137/lang--en/index.htm (accessed June 19, 2017).
Japan Ministry of Health, Labour, and Welfare. 2017. Survey on industrial accidents. Available online at http://www.mhlw.go.jp/english/database/db-l/industrial_accidents.html (accessed May 8, 2017).
Jarosz, B., and R. T. Cortes. 2014. In U.S., new data show longer, more sedentary commutes. Population Reference Bureau article. Available online at http://www.prb.org/Publications/Articles/2014/us-commuting.aspx (accessed June 19, 2017).
JISHA (Japan Industrial Safety & Health Association). 2017. Industrial accidents statistics in Japan, 2010. Statistics in Japan. Available online at http://www.jisha.or.jp/english/statistics/accidents2010.html (accessed May 8, 2017).
Kauppinen, T., S. Uuksulainen, A. Saalo, and I. Mäkinen. 2013. Trends of occupational exposure to chemical agents in Finland, 1950-2020. Annals of Occupational Hygiene 57(5):593-609.
Kauppinen, T., S. Uuksulainen, A. Saalo, I. Mäkinen, and E. Pukkala. 2014. Use of the Finnish Information System on Occupational Exposure (FINJEM) in epidemiologic, surveillance, and other applications. Annals of Occupational Hygiene 58(3):380-396.
Kneebone, E., and N. Holmes. 2015. The growing distance between people and jobs in metropolitan America. Available online at https://www.brookings.edu/research/the-growing-distance-between-people-and-jobs-in-metropolitan-america (accessed June 19, 2017).
Milner, A., I. Niedhammer, J. F. Chastang, M. J. Spittal, and A. D. LaMontagne. 2016. Validity of a job-exposure matrix for psychosocial job stressors: Results from the Household Income and Labour Dynamics in Australia Survey. PLoS ONE 11(4): e0152980.
Munich Re Group. 2004. Commuting accidents: A challenge for workers’ compensation systems. Available online at http://s3.amazonaws.com/zanran_storage/www.munichre.com/ContentPages/19215127.pdf (accessed June 19, 2017).
Pearce, N., E. Dryson, A. M. Feyer, P. Gander, S. McCracken, and M. Wagstaffe. 2005. Surveillance of Occupational Disease and Injury in New Zealand: Report to the Minister of Labour. Wellington, New Zealand: Occupational Health and Safety Advisory Committee. Available online at http://psm-dm.otago.ac.nz/ipru/ReportsPDFs/OR056.pdf (accessed May 5, 2017).
Rushton, L., S. Hutchings, and T. Brown. 2008. The burden of cancer at work: Estimation as the first step to prevention. Occupational and Environmental Medicine 65(12):789-800.
Safe Work Australia. 2017a. Work-related fatalities. Available online at https://www.safeworkaustralia.gov.au/statistics-and-research/statistics/fatalities/fatality-statistics (accessed June 19, 2017).
Safe Work Australia. 2017b. Explanatory notes for Safe Work Australia datasets. Available online at https://www.safeworkaustralia.gov.au/system/files/documents/1702/explanatory-notes-datasets.pdf (accessed June 19, 2017).
Seidler, A., A. Nienhaus, T. Bernhardt, T. Kauppinen, A. L. Elo, and L. Frolich. 2004. Psychosocial work factors and dementia. Occupational and Environmental Medicine 61:962-971.
Statistics New Zealand. 2014. Serious injury outcome indicators: 2000–13. Available online at http://www.stats.govt.nz/browse_for_stats/health/injuries/serious-injury-outcome-indicators-2000-13.aspx (accessed June 15, 2017).
Stocks, S. J., S. Turner, R. McNamee, M. Carder, L. Hussey, and R. M. Agius. 2011. Occupation and work-related ill-health in UK construction workers. Occupational Medicine (London) 61(6):407-415.
Takahashi, K., and Y. Ishii. 2014. Historical Developments of Administrative Measures for Occupational Diseases in Japan. Geneva: International Labor Organization. Available online at http://www.ilo.org/safework/info/publications/WCMS_234221/lang--en/index.htm (accessed June 15, 2017).
Tedone, T. S. 2017. Counting injuries and illnesses in the workplace: An international review. Monthly Labor Review, September. Available online at https://www.bls.gov/opub/mlr/2017/article/counting-injuries-and-illnesses-in-the-workplace.htm (accessed December 21, 2017).
Walters, D. 2007. An International Comparison of Occupational Disease and Injury Compensation Schemes. Report. Cardiff Work Environment Research Centre, Cardiff University. Available online at https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/330347/InternationalComparisonsReport.pdf (accessed September 20, 2016).
Warburton, K. L., R. Urwin, M. Carder, S. Turner, R. Agius, and S. M. Wilkinson. 2015. UK rates of occupational skin disease attributed to rubber accelerators, 1996-2012. Contact Dermatitis 72(5):305-311.
Wieclaw, E., E. Agergo, P. B. Mortensen, H. Burr, F. Tuchsen, and J. P. Bonde. 2008. Psychosocial working conditions and the risk of depression and anxiety disorders in the Danish workforce. BMC Public Health 8:280.
WorkSafe New Zealand. 2017. Sources of work-related injury data. Available online at http://www.worksafe.govt.nz/worksafe/research/health-and-safety-data/sources-of-work-related-injury-data (accessed May 8, 2017).
Zhou, A. Y., M. Carder, L. Hussey, M. Gittins, and R. Agius. 2017. Differential reporting of work-related mental ill-health in doctors. Occupational Medicine 67(7):522-527.
This page intentionally left blank.


















