
4
Health Literacy Considerations for Outreach
The first panel of the workshop’s afternoon session discussed four areas: using health literacy concepts to teach English, messaging for disaster and emergency preparedness, outreach to uninsured foreign-born populations, and strategies for identifying and working with trusted advisors and decision makers. All mentioned their challenges with health literacy and ensuring they are able to fully capture their targeted populations. Maricel Santos, associate professor of English at San Francisco State University, discussed teaching English to non-native speakers using health and health literacy concepts. Justine Kozo, chief of the office of border health at the San Diego Health and Human Services Agency, spoke about the challenges of messaging for disasters and emergency preparedness. Rishi Sood, director of policy and immigration initiatives at the New York City Department of Health and Mental Hygiene, described outreach efforts to uninsured foreign-born populations in New York City. Mimi Kiser, program director for the interfaith health program at the Rollins School of Public Health at Emory University, gave the final presentation on strategies for identifying and working with trusted advisors and decision makers. An open discussion followed the presentations.
TEACHING ENGLISH USING HEALTH CONCEPTS AND HEALTH LITERACY1
Santos began her presentation with two takeaway messages. The first was that the adult literacy world and public health need to be spending more time in each other’s worlds. The second was that the goal is not to make things simple, but to make them understood. A teacher telling a class that his or her goal was to make things simple would not motivate learners to return, but telling students that his or her goal is to find out how that day’s lessons would intersect to the learners’ needs starts a conversation that is likely to continue. Santos, who spends the bulk of her time training teachers, said that many of her graduate students are interested in connecting English language education with the outside world, and a large part of her funding is associated with workforce training grants. She noted that she and her colleagues have been discussing how to address both workforce development and health literacy education to empower immigrant communities.
Santos then told a story to illustrate how English as a second language (ESL) teachers can introduce health concepts into English instruction (Santos et al., 2011). The story starts with a statement about posole: You don’t ever think about vegetables because you never ate enough meat in your country. You think that the best and most delicious thing is to prepare a very delicious posole. From this story, the ESL teacher can bring in themes and start a discussion around child nutrition, changing diets in immigrant families, and how to preserve home traditions in a new country. Using what is known as a “re-storying” approach to collaborative interpretation of texts, the teacher asks the students to describe what the story says about vegetables and to interpret why the writer talks about posole and why the writer talks about meat in the last two sentences. Finally, the students reflect on how this story reminds them of their own stories and talks about who should hear those stories.
In one class, this story triggered a disagreement between two Spanish-speaking students about whether or not the posole has vegetables in it, with one student arguing that beans are a vegetable, and the other disagreeing with her. What was important, said Santos, is that one beginning adult ESL learner understood the story well enough to disagree with it and that she and another student were expressing, in English, a reaction to the story. “Imagine that dynamic in a clinical encounter,” said Santos. One thing that happened in this conversation is that the two women eventually started interspersing Spanish into the conversation, a phenomenon that linguists
___________________
1 This section is based on the presentation by Maricel Santos, associate professor of English at San Francisco State University, and the statements are not endorsed or verified by the National Academies of Sciences, Engineering, and Medicine.
call translanguaging. The implications of this for health literacy among immigrants and refugee communities is that it should be thought of as a multimodal, multilingual competence. “If you look at what is going on in classrooms where people are developing this competence, you do not see it demonstrated in English only,” said Santos. “This has an important implication for how we assess the development of health literacy and its outcomes if we are only able to do it largely in English.”
She then recounted a story about when she first met the late Archie Willard, a leading figure in adult literacy who founded VALUEUSA, a national adult learner leadership organization. She was giving a talk to a group of adult learners and the subject was supposed to be on reading and how it connected to health. Willard pulled her aside and told her that the students are going to start telling their life stories and he predicted that her impulse was going to stop the discussion to get the students back on track but that she needed to resist. His point, she said, was that learners, in order to become leaders, need uninterrupted opportunities to tell their life story. “To gain a voice as a health literate person in this world requires opportunities not only to tell your story, it’s actually better framed as the right to impose listening onto others,” said Santos. (This characterization of health literacy competence as reflective in one’s ability to “impose listening on others” builds on the work of Bonny Norton [language education] and Pierre Bourdieu [sociology] [Norton, 2013].) “That has such important implications for patient engagement, but also in classrooms where we try to do a very active job of allowing ourselves to listen as best we can despite the comprehensibility of an accent and despite the fact that this person does not have the right vocabulary.”
Another important concept that comes up in the posole story, she said, is that learners need opportunities to ask questions, even risky ones, and this is particularly true in the context of a clinical encounter. The health literacy community knows this, and it also understands that English proficiency does not equal success (Gee, 2014).
To apply health literacy in adult ESL classrooms, Santos suggested using real-life stories to develop language lessons of high interest to learners and to use learner stories as texts. Classroom talk can serve as health literacy in action, and health literacy talk can serve as identity work. ESL classrooms, she noted, are good places to discuss health issues because they are viewed as safe places to get advice, ask questions, and analyze information. They can also provide access to hard-to-reach communities and links to existing social networks within marginalized communities (Santos et al., 2014).
Santos listed a number of keys to unlocking health literacy competencies of adult ESL learners. These included focusing on message abundancy (Gibbons, 2003); scaffolding, or breaking up learning into chunks and
providing a tool or structure with each chunk (Walqui, 2006); emphasizing oral interaction around texts (Bigelow and Tarone, 2004); harnessing the power of embodied language (Whiteside, 2008); emphasizing interaction and transaction (Whiteside, 2008); and honoring the lived experience in the classroom. She also said that teacher training and health educator training programs need to be speaking to each other more often and need to be incentivized to do so. “We are both very siloed because we have our own licensing expectations with very little connection,” said Santos.
She also called for new thinking about health literacy credentialing. “There are no certificates when an adult ESL learner completes 3 years of ESL and is actually better at health care navigation,” she said. One model may be efforts in the adult education system (e.g., corrections education, work-based education) that aim to provide a continuous sequence of adult education and reward intermediate milestones with a credential or certificate. “I wish we had something like that in adult education for health literacy because it would enable us to not only demonstrate linguistic outcomes—do they have better vocabularies—but also that they have better self-advocacy skills,” said Santos. Credentialing is particularly valuable for learners at the beginning levels of literacy learning, for whom there are often no formal ways to reward progress. While adult education is good at that kind of assessment, she said, it lacks the connection to public health to translate assessment into the health care context.
To close her presentation, Santos returned to the idea of learner leadership. “Where are the adult learners in our conversations?” she asked. She noted that community organizing is one place where the dynamic preserves a place at the table for the least proficient to be heard. As a final thought, she called on those in attendance to identify at least three or four adult education programs that they would call to start making the connection between adult ESL instruction and health literacy.
MESSAGING FOR DISASTERS AND EMERGENCY PREPAREDNESS2
Every day in San Diego approximately 75,000 northbound crossings occur, said Kozo, and roughly 32 percent of the city’s population is Latino. In addition, San Diego is a major resettlement destination, accommodating some 3,500 refugees annually. As a result, more than 100 languages are spoken in the city. Kozo noted that a recent report found that some 400,000 individuals report speaking a language other than English at home, speak English less than very well, and are not prepared for emergencies such as
___________________
2 This section is based on the presentation by Justine Kozo, chief of the office of border health at the San Diego Health and Human Services Agency, and the statements are not endorsed or verified by the National Academies of Sciences, Engineering, and Medicine.
the huge wildfires in 2007 and 2014 that led to the evacuation of more than 500,000 people.
The language diversity in San Diego creates a number of challenges with regard to messaging and emergency management, said Kozo. A study conducted by California State University at San Marcos on the experience of agricultural workers during those wildfires found that people were too terrified to come out of their homes when they received evacuation orders from law enforcement. “They were so terrified, for a number of reasons you can imagine, that many people just shut their blinds and prayed,” she said. Another study conducted in the aftermath of a 2011 24-hour blackout across San Diego County found that families in refugee communities sent their children to schools, which were closed, because they had no idea about what was happening.
Incidents such as these produced a great deal of public criticism about how San Diego County responds to these emergencies in terms of helping people in isolated communities. As a result, explained Kozo, the directors of public health and the office of emergency services got together and started an initiative under the auspices of the Live Well San Diego vision to create communities resilient to disaster and emergencies. The Office of Emergency services looked into translation software options that could be disseminated via the county’s reverse 911 system. “We looked into that and there is no system you can trust,” said Kozo. “When you are sending out lifesaving information such as ‘You need to evacuate your home’ or ‘You need to boil your water, it is not safe to consume,’ you cannot rely on Google Translate or any other computerized software to translate that information correctly.”
Starting in 2012, the county began the process of planning a large community forum to bring together representatives from the top six languages other than English spoken in San Diego, which included Arabic, Chinese, Filipino, Korean, Spanish, and Vietnamese. Representatives from several refugee organizations pointed out that while smaller in number, refugee communities are more vulnerable and have fewer resources, so the list was expanded to included members of the Somali and Karen communities. At the first all-day meeting, directors of community-based organizations came along with a client, colleague, or patient from their communities. This meeting featured a keynote speaker from ECHO, an organization based in Minnesota that focuses on health communication, and eight focus groups, each professionally facilitated with simultaneous interpretation in all eight languages. The focus groups were asked the specific questions:
- During an emergency, where do you get your information?
- Who do you turn to, and who do you trust?
- Do you have a landline at home?
- What media does your community have access to?
- If you received some information from the county government, how would you respond?
- What is your level of trust with government?
Perhaps the key finding from this exercise was that during emergencies or when people are in need, they turn to one another for support and information. “Social networks are everything,” said Kozo. Another finding was that a community’s youth are a trusted source of information because younger members of the community tend to be bilingual, assimilate quicker, and they are more savvy with social media so they have quicker access to information. Schools were noted as a trusted source of information, as was the Red Cross. All eight focus groups listed various faith-based organizations in their communities, as well as media when available, as additional trusted information sources. Kozo explained that while the Latino population in San Diego has access to several local Spanish language news and radio stations, the Somali and Karen communities do not have access to the equivalent.
Another finding was that the level of English proficiency varies across these communities. The Korean and Karen communities reported very high levels of literacy, while the Somali and Latino communities reported lower levels. Also in some languages there are multiple dialects within communities. “We were told that there are 80 different dialects within the Filipino Tagalog language,” said Kozo. Yet despite these challenges, information travels quickly through these communities via word of mouth.
A key finding for Kozo and her colleagues was the varying degrees of trust in government. “Many groups said they flat out have mistrust [of the] government because of their experiences in their home countries,” she said. “Some groups said if they received a letter in the mail that had a government logo, that they might just simply toss it in the trash.” In fact, out of the eight groups, the Filipino group was the only one that recognized the county seal. Schools were the one exception to the mistrust of government.
The focus groups recommended using existing social networks to disseminate information at times of emergency. One of the best ways of doing that, said Kozo, is to use phone trees and partner relays. What this means, she said, is that her agency has worked to create partnerships with trusted community-based organizations and rely on those organizations to disseminate updated, accurate, and vetted information. “You have to engage with these partners ahead of time, and then they share that information with their clients in various languages or however they disseminate information,” she said.
In addition to holding one-on-one meetings with community-based agencies, she and her colleagues have been conducting trainings three times
per year that bring together community-based agencies serving refugee, immigrant, and newly arrived communities. “We train them on topics that are of interest to them related to public health and emergency preparedness,” said Kozo. Her agency has also conducted drills with an online, two-way communication platform it uses, called ReadySanDiego, as part of its partner relay. The county also uses this platform to disseminate pertinent public health information, such as on Zika. Currently, her agency has more than 300 partners.
Unfortunately, said Kozo, the communication drills her agency held in 2015 and 2016 had low participation, and the feedback was that the communication platform is clunky, requires a password that partners forget, is not searchable on Google, and does not come with a mobile app. As a result, Kozo’s team is exploring new communications platforms and hopes to have a new system in place by the summer of 2017.
In terms of what this program asks of its partners, Kozo said they need to join the partner relay, designate someone within the organization to be the point person, and to share pertinent information during emergencies. What the program offers in return is updated, vetted, trusted, and timely information during emergencies, as well as regular communication on pertinent health topics and trainings three times per year on important public health and emergency information. The program also provides a direct phone line and email address that allows the partner relay liaison to contact the county’s emergency operations center.
So far, the program has conducted 10 trainings among refugees on subjects including wildfire prevention and childhood lead poisoning. Law enforcement has spoken about what to expect during an evacuation. A training scheduled for May 2017 will focus specifically on the refugee community.
OUTREACH TO UNINSURED FOREIGN-BORN POPULATIONS3
Though the percentage of people uninsured in New York State and New York City has dropped to historic lows since the passage of the Patient Protection and Affordable Care Act (ACA), the uninsured rate among noncitizens and the undocumented population remains high, said Sood. He explained that the undocumented population in New York City represents approximately 1 in 16 residents, and two-thirds of that population, or 345,000 people, lacks coverage as of 2013. In addition, approximately
___________________
3 This section is based on the presentation by Rishi Sood, director of policy and immigration initiatives at the New York City Department of Health and Mental Hygiene, and the statements are not endorsed or verified by the National Academies of Sciences, Engineering, and Medicine.
245,000 undocumented and uninsured adults aged 19 and older live in households with income under 200 percent of the federal poverty level as of 2013. In New York State, he added, all children regardless of immigration status are eligible for health insurance.
In 2014, New York City Mayor Bill de Blasio launched a taskforce to identify ways to improve health care access for the more than 3 million foreign-born residents of the city, with a specific focus on those left behind by the ACA. The centerpiece recommendation borrowed heavily from models in California, including Healthy San Francisco, My Health LA, and the Health Program of Alameda County, as well as the My Health model in Harris County, Texas, and models from Massachusetts and Nevada. “Everyone does it slightly differently, but through months of conversation we documented what was done around the country and determined it was time for New York City to launch what we call a direct access health care program,” said Sood. This program, ActionHealthNYC, builds on the city’s robust public hospital system, which includes 11 public hospitals and dozens of other facilities, and dozens of community health centers, many of which are federally qualified health centers, he explained.
The benefits of the direct access model, said Sood, begin with the enrollment process, which is tied to other city programs such as New York City’s municipal identification card (IDNYC). Enrollees in the program choose a primary care home that provides coordinated care with consistent fees. In addition, this program pays providers to deliver remote care coordination, rather than care management provided solely within the walls of a particular health facility. At the time of the workshop, ActionHealthNYC was in the midst of a 1-year demonstration phase, with the goal of enrolling 2,400 people from the Lower East Side and Chinatown neighborhoods of Manhattan; the Jackson Heights, Corona, and Elmhurst neighborhoods in Queens; and the Sunset Park and Borough Park neighborhoods of Brooklyn.
ActionHealthNYC partnered with six community-based organizations in the demonstration neighborhoods to reach its target populations. It also used paid advertising and generated 41 earned media hits in its 5 months since the program was announced on March 10, 2016. In addition, the program mailed notices to IDNYC participants and Emergency Medicaid recipients in the demonstration neighborhoods and worked with allied organizations to spread the word. Sood noted that the network of health facilities involved in the demonstration includes many that lie outside of the target neighborhoods because people often get health care services near their place of employment or where they know they will receive care in the language that they speak rather than where they live. Enrollment in the program began May 2, 2016, and ended August 13, 2016, with clinical services starting on July 1, 2016. Sood noted that people could make appointments through the city’s 311 system, though it had to stop the 311
system from accepting appointments 10 days before the enrollment period ended because of a large spike in enrollment thanks to the mailings. “A good problem to have, but not something you really wanted to run into,” said Sood. Though the program prepared health education materials in 13 languages, Sood said the participants in the demonstration speak 32 different languages and come from 77 countries. Enrollees live in 139 zip codes in every borough of the city.
In the final moments of his presentation, Sood spoke about the challenges of reaching ActionHealthNYC’s target population, which turned out to be harder than expected. “How hard can it be to reach 1 percent of a particular population to provide a health care program that charges no quarterly or monthly fees, only point-of-service fees?” asked Sood. “The truth is, it was much more complicated than we thought.” In the end, only one-third of the enrollees came through the community-based partners. Another one-third were walk-ins who found out about the program through word of mouth or an advertisement, and the remaining one-third came in through the 311 system. “What that tells us is that the varied approach was important and that we cannot just send out letters, we cannot just work with community-based groups, and we cannot just rely on word of mouth,” said Sood.
Another important lesson from the enrollment process was that although people distinguish between federal and local government, local government is still government and partnering with trusted community-based organizations is more important than ever given the distrust of governments among the target population, said Sood. “We should not understate the political climate,” he said. “I did some of the enrollments myself at a number of our sites and the questions that we heard most often were from people asking how we were going to protect their information.” This study, he explained, had institutional review board approval and he and his team are taking every precaution to protect the participants’ information. Nevertheless, he said, some people thought the risk was still too high and declined participation in the program.
PARTNERSHIPS IN BUILDING TRUSTED COMMUNITY NETWORKS4
In 2009, Kiser and her colleagues at Emory University began a project to build and mobilize capacity within networks of faith-based and com-
___________________
4 This section is based on the presentation by Mimi Kiser, program director for the interfaith health program at the Rollins School of Public Health at Emory University, and the statements are not endorsed or verified by the National Academies of Sciences, Engineering, and Medicine.
munity organizations at 10 sites around the country. These organizations had established links with public health, and the goal was to extend their reach to vulnerable, at-risk, and minority populations in order to improve influenza vaccine outreach and uptake. The 10 sites included in this project were a subset of those that were part of a leadership development program that the Centers for Disease Control and Prevention (CDC) funded, called the Institute for Public Health and Faith Collaborations. Kiser’s team had trained 78 teams of religious and public health leaders in 24 states to collaborate on eliminating health disparities for the CDC-funded program. During the H1N1 outbreak of 2009, the U.S. Department of Health and Human Services’ Faith-Based and Neighborhood Partnerships program, which knew of this network, thought that tapping into the resources and community capacity of these sites might be an expedient way to deliver H1N1 services to some of the priority populations, she explained.
Understanding the nature of these partners is important, said Kiser. Five are large faith-based health systems that, because of their faith-based mission, have a strong commitment in their community outreach programs to build strong institutional relationships with the faith-based community in their catchment areas. Kiser noted that the partners in this project included the Arkansas Department of Health; a small faith-based organization that conducts large-scale health promotions and disease prevention activities in underserved communities in Detroit; the Buddhist Tzu Chi Foundation in Los Angeles; a federally qualified health center in Lowell, Massachusetts, that works with refugee and immigrant communities; a small nonprofit organization in Pennsylvania that serves a rural community; and large faith-based health systems in Chicago, Memphis, Minnesota, and New York City.
The project’s accomplishments, said Kiser, are measured in the number of people vaccinated across the 10 sites and the number of vaccination events the partners have held. She noted that along with vaccinations, the sites conduct education outreach and engagement with partners. Some sites, she added, have adopted the Arkansas Department of Health’s influenza prevention workshop approach. One site has an academic partner who conducted qualitative research on trust with religious leaders and used the findings to build some educational outreach tools. Minnesota’s site, on behalf of the state health department, conducted interviews on emergency communication with community leaders and as a result conducted outreach using e-newsletters, radio, family nurses, and faith-based organizations.
One partner in Minnesota, Fairview Health Services, had a CDC Epidemic Intelligence Service officer who helped develop a survey to administer at its vaccination clinics to learn about people’s attitudes and decisions about vaccination. Administered to between 1,600 and 2,800 people per year since the 2011-2012 influenza season, this survey showed that people
TABLE 4-1 Results of Surveys on Attitudes and Behaviors Regarding Influenza Vaccination
| 2011-2012 | 2012-2013 | 2013-2014 | 2014-2015 | 2015-2016 | |
|---|---|---|---|---|---|
| No health insurance | 55.5% | 45.2% | 40.9% | 30.4% | 32% |
| No regular doctor | 19.2% | 15.1% | 13% | 13.6% | 13% |
| Shots provided free | 65.8% | 51% | 48% | 49.6% | 52% |
| Trusted place/setting | 42.5% | 28.3% | 26% | 24.9% | 26% |
| Convenience | 16.3% | 19.6% | 22.2% | 46.1% | 46% |
| Interpreters | 23% | 12.1% | 13.6% | 9.1% | 12% |
SOURCE: Emory Interfaith Health Program as presented by Mimi Kiser at Facilitating Health Communication with Immigrant, Refugee, and Migrant Populations Through the Use of Health Literate Approaches: A Workshop on March 15, 2017.
come to the clinics because they have no health insurance, the shots are free, the clinic is a trusted place, and it is convenient, among other reasons (see Table 4-1).
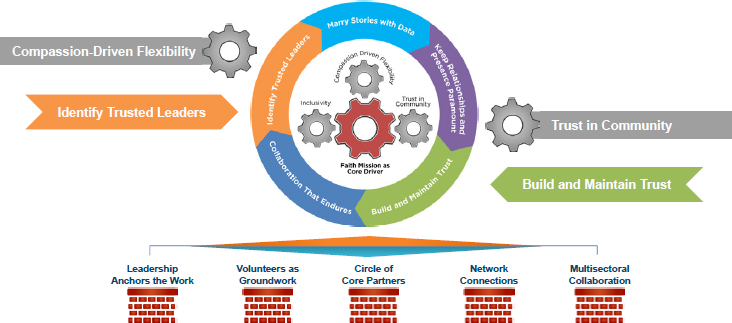
Kiser and her collaborators conducted a modified Delphi technique to identify some of the key practices associated with the successes the programs were having in reaching their focus populations. This analysis identified 14 practices organized in four core drivers—having a faith mission, inclusivity, trust in their communities, and compassion-driving flexibility—and five associated processes (see Figure 4-1). According to Kiser, these processes—marrying stories with data, keeping relationships and presence paramount, building and maintaining trust, developing enduring collaborations, and identifying trusted leaders—are the day-to-day work that contribute to program success. Supporting the core drivers and five processes are five enduring infrastructure capacities: leadership that anchors the work, volunteers on the ground, a circle of core partners, network connections, and multisectoral collaborations. Kiser and her collaborators partnered with the Association of State and Territorial Health Officials to build a toolkit based on this framework.5
One model Kiser highlighted was that of the Buddhist Tzu Chi Medical Foundation, which she characterized as being light on bureaucracy and able to respond rapidly in a way that her public health partners were often not able to do. This organization, which serves a large portion of the Asian population in Los Angeles, sets up clinics to provide health services at migrant farm worker camps early in the morning, before the workers
___________________
5 See http://ihpemory.org/ihp-programs/public-health-and-faith-community-partnerships (accessed May 5, 2017).
SOURCE: Emory Interfaith Health Program as presented by Mimi Kiser at Facilitating Health Communication with Immigrant, Refugee, and Migrant Populations Through the Use of Health Literate Approaches: A Workshop on March 15, 2017.
have to be in the fields, or late in the evening when the workers return to camp. They follow the same pattern at homeless shelters. They also provide services at cultural celebration venues, said Kiser.
She also discussed the Lowell (Massachusetts) Community Health Center, a federally qualified health center with a long history of responding to the needs of immigrant communities, particularly the Cambodian refugee community and most recently African immigrants. To deliver services to the Cambodian community, the Lowell center partnered with a local Buddhist center and built a mediation room in the health center itself. To service the African immigrant community, the Lowell center has established a strong outreach relationship with a network of African churches. Kiser noted that this organization has been intentional about hiring staff who represent the ethnicity and culture of those they serve, and it has developed a large community health worker program. “They have adapted that to work and build relationships and connectivity to these different ethnic populations through the faith-based and community organizations,” said Kiser.
In Chicago, two organizations with a long-standing partnership—faith-based Advocate Health Care system and the University of Illinois at Chicago’s Neighborhood Initiative—formed the Center for Faith and Community Health Transformation. The center capitalizes on the partnership’s unique communication capacity from an extensive network of faith-based and other like-minded partners with whom it has built trusted relationships. In one case, the center worked with the Council of Islamic Organizations

NOTE: UCC/UUA = United Church of Christ/Unitarian Universalist Association of Congregations.
SOURCE: Emory Interfaith Health Program as presented by Mimi Kiser at Facilitating Health Communication with Immigrant, Refugee, and Migrant Populations Through the Use of Health Literate Approaches: A Workshop on March 15, 2017.
of Greater Chicago to develop a flu prevention method framed by the commitments and theological perspectives of the Islamic faith tradition. This method was disseminated through a newsletter that reached more than 9,000 readers. These collaborators also created a website with 2-minute videos of religious leaders providing encouraging words out of that faith tradition around promoting flu prevention and flu shots. These videos are in Arabic, Chin, Haitian Creole, and Hispanic.6
In Minnesota, Fairview Health Services partnered with the Minnesota Department of Health and a network of core partners who together reach a diverse set of ethnic immigrants in settings such as churches, mosques, a Hindu temple, a Sikh temple, a Buddhist monastery and temple, a Burmese Baptist church, the local Tibetan Foundation, a Somali mall, a Hmong flea market, homeless shelters, English as a second language centers, child care centers, food pantries, and the Mexican Consulate (see Figure 4-2). Together, these partners hold large-scale vaccination events, and Kiser characterized them as the “go-to vaccine sites for many of those populations.” The partners only hold these vaccination clinics when invited by the
___________________
6 The videos are available at http://www.faithhealthtransformation.org/resources-and-toolkits/health-topics/flu-prevention-and-immunization-resources/diverse-spiritual-leaders-encourage-flu-prevention (accessed June 14, 2017).
host sites. “That relationship is really nurtured and respected,” said Kiser. Trained volunteers staff the clinics, which are held at hours convenient to the particular population. Most of the clinics have an extensive network of translators on hand.
Kiser concluded by noting that these programs all deliver trusted and accessible messages outside of the health care system through trusted networks and relations. In every case, the partners have a flexible and adaptive organizational capacity that enables them to quickly deliver messages in a relevant language and with relevant cultural meaning. Most communities, said Kiser, have leaders and organizations who have the relationships and commitments that can leverage connections and social capital for the well-being and health of all. “It is very rewarding to see what these community networks and leaders have been able to build over time in their communities, and I’m honored to be working with them and sharing their work with you here,” said Kiser, ending her remarks.
DISCUSSION
Robert Logan began the discussion by noting that libraries become trusted places and safe havens after disasters without any outreach. He asked the panelists to comment on the potential to integrate libraries in their work. Sood did not know if any of the outreach efforts in his program included libraries, but he acknowledged that they should. “When I talk about the outreach efforts of the program, I usually mention churches and temples and other places of worship, but point well taken,” said Sood. “I can say that at the least my team will take that into account as we move forward.” Kozo also thanked Logan for that suggestion and said she would reach out to libraries directly when she returned to San Diego. “I’m excited to take this back to my team,” she said.
Santos replied that she does not work directly with libraries in her work, but she said adult education has a strong hold in libraries. She also said that librarians tend to be ahead of the curve on media literacy and the tools that are available, and that expertise could play an important role in mapping networks. She did note that in rural areas, libraries are often mobile and not someplace a person can walk into whenever they want. She also pointed out that librarians in San Francisco and the Bay Area are important health literacy intermediaries. Umair Shah said that in Harris County (Texas), public health already works with the library system and is looking at co-locating public health services and libraries to enable joint programming.
Shah then asked the panelists to talk about any impacts that today’s resource-constrained environment has had on the importance of partnerships and working with diverse groups outside of the silos of public health
and health care. Sood said that such partnerships are quite important in New York City. For example, he noted that the Mayor’s Office of Immigrant Affairs has a partnership with the city health, education, and social services departments to align messages that then go to the public through community-based organizations. Kiser said that she has seen the reduction in dollars make it difficult for agencies to spend time on forming partnerships given that funds for outreach activities are often the first ones cut as budgets tighten. “I think it is a fairly resource-intensive activity,” she said. Where she has seen success is when larger faith-based health systems have reached out to the faith community to bring it alongside public health.
Santos said there are certain populations for which additional resources are needed to make a difference, such as adult learners with limited years of schooling and adolescents who have “maxed out” of high school but are too young to enter the adult education system. “There are these populations that deserve more individualized attention and are going to need innovation,” she said. As an example, she cited a recently published paper by the Open Door Collective which spotlights four different health literacy projects and all have some funding from the Workforce Investment Act or from a health insurance foundation that decided to invest in adult literacy professional development.7 These projects were able to integrate the health component into a program that would meet the learning needs of their learner community and the needs of their funders.
Bernard Rosof asked Sood about his experience working with the large not-for-profit health systems in New York City that have an obligation under the ACA to be involved in the type of work described during this session. Sood replied that from the health department perspective, it is sometimes easier to work with the public hospital system than with private health systems. The long-term goal of his program is to work with private hospitals in addition to public hospitals. Kiser added that in all of her years working to link public health with the faith community, New York City public health has always had a devoted staff member working with the faith community and taking that role seriously.
Laurie Francis commented about the need to move care outside of the health care system in order to maximize the effectiveness of constrained resources for improving health. Working with community partners would be one way of spreading resources. She then asked Santos if she could speak more about her concept of the right to impose listening. Santos said that this idea comes from Bonny Norton, an identity theorist who would say to stop treating health literacy as a set of reading and writing skills and instead look at it as a change in identity. “When you gain new practices,
___________________
7 See paper at http://www.opendoorcollective.org/adult-basic-education-and-community-health-center-partnerships.html (accessed August 11, 2017).
new navigation skills, new competencies, you change who you are able to interact with,” said Santos. In her view, health literacy is a means of increasing social participation, which suggests there are theories and models from the social participation field to bring to bear on the challenges of improving health literacy. It also suggests to her that the adult education system needs to be a partner of the health care system so that the classroom rather than the 11-minute clinical encounter becomes a place for working on health literacy.
Willis asked Sood if ActionHealthNYC was incorporating mental and oral health in its agenda, and Sood replied that that the seven federally qualified health centers and two public hospitals in its pilot program do offer mental health services and New York City’s ThriveNYC program aims to improve mental health for all New Yorkers. He noted that some of the federally qualified health centers are seeing people who are physically healthy and enrolled in the program strictly for behavioral health services. Oral and dental services are covered and are available at half of the program’s primary care homes. Clients of the other health centers are free to go to another site to get dental care.
Kozo said her program recognizes the extreme importance of mental health, especially when dealing with refugee and migrant communities who have experienced trauma in their home countries, on the journeys to the United States, and even in this country. She did note that it was only recently that mental health was raised as a topic of interest at one of the program’s trainings, but once it came up it became a huge discussion point. As a result, the May/June training session will include a presentation on available mental health resources in the community. Kiser added that some of the organizations she works with have started asking for suicide prevention education and are starting to receive training in mental health first aid.
Rosof then asked if any of the programs were addressing autism. Kozo replied that there is always a focus on autism at the annual binational health month that is held every October. This program is put on by the University of California, Berkeley, Health Initiative of the Americas and all Mexican consulates in the United States. While this is not connected to her program in emergency preparedness, it is an important issue to the Latino community in San Diego. Santos noted that adult education programs based in unified school districts are helping families who fear deportation get their child’s individualized education program together in case they have to leave suddenly.
Kozo added that public health uses the partner relay system during non-emergency times to share helpful resources with the community, and these resources have included information on mental health. It has not been used to push out resources on autism, learning disabilities, or developmental disabilities, but she said she will do that. Julia Ackley, the health
literacy program manager at Sutter Health, said that in a previous role she worked for Help Me Grow, a national network that does care coordination for children through age 5 with developmental delays including autism. This organization, she said, does extraordinary work partnering with pediatricians to create a health literate, multilingual, trauma-informed care approach to support families. These families, in turn, serve as advisory members for organizations and could be good partners for the type of programs discussed at this workshop, particularly given the shortage of resources available for children with mental health issues.
Santos noted the importance of having discussions among content experts and teachers when thinking about how to address hard health topics such as gestational diabetes, a program she is currently developing. “People may not know how to engage in talk about gestational diabetes even though they are interested in it,” she said. Teachers, though, are good at looking at the “on ramps” that create meaningful opportunities for learners to talk to each other and engage in a topic.
She also responded to a question from Ackley about how a large health care organization such as hers can partner with adult education programs by noting that most adult education programs are registered with an organization called the Outreach and Technical Assistance Program for Adult Educators.8 This organization has an online directory that can be searched by zip code, which is typically how she finds programs with which to work. However, she added, it helps to have a faculty member to be a community partner, so she suggested going to a nearby university and finding its office of civic and community engagement. “Those folks have the infrastructure to bridge build for you,” said Santos. Many universities also have a service learning component that requires students to do service work in the community. “Then you have a cadre of individuals who are in training who might be able to work for you,” she said. Adult English as a second language teachers are also good sources of ideas on issues that arise in a community. “That is how I found out about lead poisoning in Salinas,” she said. Santos then noted that there is a need for a crowdsourcing portal to identify good ideas and share them.
Wilma Alvarado-Little, principal and founder of Alvarado-Little Consulting, asked the panel if their programs had made any allowances for the deaf and hard-of-hearing communities, especially those for whom American Sign Language is not their primary or preferred language. Kozo said that San Diego County’s communication relay has a technology in place for alerting both the hearing and visually impaired communities.
___________________
8 See http://www.otan.us (accessed May 5, 2017).
This page intentionally left blank.


















