
Three speakers at the workshop looked at the treatment of severe obesity in adults, including one who recounted her own experiences with bariatric surgery.
A MULTIFACETED APPROACH
People know they should lose weight, but physical changes that occur in the brain when a person gains weight make losing that weight difficult, observed Louis Aronne, Sanford I. Weill professor of metabolic research, Weill Cornell Medicine. Fattening food damages weight-regulating neurons, he elaborated, and weight-regulating pathways become less responsive to hormonal and neural signals (McNay et al., 2012; Thaler et al., 2012). The result is a system that is biased in favor of weight gain and against weight loss (Apovian et al., 2015). “Your brain loses control of how much food is coming in, how much fat is stored,” Aronne said. “It keeps telling you to gain more weight, either by eating too much or subtly slowing down your metabolism.” Antiobesity medicines work in the parts of the brain that are damaged, he explained. In addition, he noted, some studies have shown that the use of nerve growth factor in the presence of damaged neurons can cure obesity in animals.
According to Aronne, management of drug-induced weight gain is an important component of treatment. For example, many surgery patients fail to do as well as expected because they are taking medicines that prevent them from losing weight (Saunders et al., 2016). Thus, Aronne explained, switching to drugs that are weight neutral or promote weight loss can change outcomes. He cited the example of a patient who had lost 36 pounds after having lap band surgery but had regained all of his weight. Initially taking pioglitazone, metformin, and other medications, he was treated by increasing metformin, reducing pioglitazone, and initiating liraglutide. The result was a 60-pound weight loss, Aronne reported, and he has been stable for more than 1 year at around 190 pounds. “The idea that someone has surgery and they are cured—that is not true,” he said. “You constantly have to be watching to see what do you do next.” For example, he added, if someone with type 2 diabetes has bariatric surgery, “we will give that patient metformin if we see they are starting to get hungry, or if their weight plateaus at a higher level. We won’t force them to take it, but as soon as we see someone starting to have difficulty from their bariatric surgery, we will add a medication.”
Aronne reported that, according to a retrospective review, people who had Roux-en-Y gastric bypass lost more weight when medication was used (Stanford et al., 2017). “Probably the best time to start medical therapy is when someone hits a plateau,” he suggested. “We think that this is a strategy that should be encouraged in patients who have surgery.” He noted
that the treatment gap between the low and high ends of weight loss is being filled with new medications and less invasive procedures at the low end and by the addition of medication to bariatric surgery at the high end (see Figure 4-1). He offered the interesting observation that a medicine for weight loss that does not work before bariatric surgery can work afterward.
Treating severe obesity requires experienced teams, Aronne asserted, including bariatric surgeons, gastroenterologists, obesity medicine specialists, registered dieticians, psychologists, and support staff. “You need the proverbial village to treat the patient with severe obesity,” he said. However, he noted, many communities may not have such teams—they may have some of these specialists but not all. As a result, he said, patients do not get the “support and intuitive care that is necessary in managing problems when they arise.”
According to Aronne, the need for teams reflects the fact that different treatment approaches work together. The Comprehensive Weight Control Center at Weill Cornell Medicine, for example, has five physicians, two of whom are endocrinologists and one a nutrition specialist; a nurse practitioner who performs remote monitoring of patients; dieticians; an obesity medicine fellow; and various students and research aids. Aronne called particular attention to obesity medicine, a new and rapidly growing specialty. In the past few years, he reported, the number of certificates issued
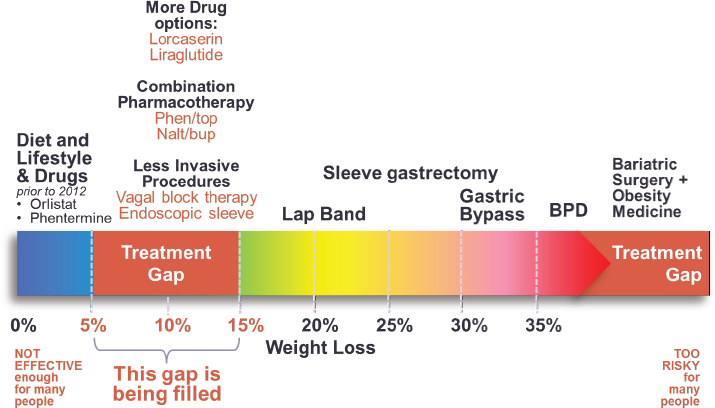
NOTE: BPD = Biliopancreatic Diversion Surgery.
SOURCE: Presented by Louis Aronne, April 6, 2017. Reprinted with permission.
for obesity medicine, which requires continuing medical education and board examination, has quickly surpassed the numbers issued for geriatric medicine, rheumatology, endocrinology, and infectious diseases.
A final need is for insurance coverage for treatment, Aronne argued. “Without coverage for care,” he said, “you can’t do anything. You can’t see the patients.”
BARIATRIC SURGERY
According to Bruce Wolfe, professor of surgery at Oregon Health & Science University, the Longitudinal Assessment of Bariatric Surgery (LABS) Consortium has demonstrated that bariatric surgery can produce major weight loss and health benefits. As an example, he reported that the remission rate for type 2 diabetes following gastric bypass surgery is 62 percent at year 3 (Courcoulas et al., 2013), and is still 59 percent at 7 years. The remission rate for type 2 diabetes with gastric banding is lower—37 percent—he noted. However, he said, remission is improved for a range of other conditions, including hypertension, dyslipidemia, sleep apnea, and psychosocial impairment, as well as for functioning and employment status, in the general population undergoing bariatric surgery.
According to Wolfe, multiple studies with comparison groups have shown improved survival when weight loss is achieved by bariatric surgery. The mortality rate from the surgery is 0.3 percent for all gastric bypass and 0.2 percent for laparoscopic gastric bypass patients (LABS Consortium, 2009), with serious complications in about 4 percent of all patients and about 5 percent of laparoscopic gastric bypass patients. Furthermore, Wolfe added, these data are about 10 years old, and safety has improved since then. “Those who believe that bariatric surgery is unsafe need to be updated regarding the latest data,” he asserted. He reported that about 700 centers have been certified to perform the surgery by the American College of Surgeons and the American Society for Metabolic and Bariatric Surgery, with certification encompassing surgeon training, the provision of data to a central registry, quality improvement, and standardized care protocols. For example, he said, data submitted to the central registry are analyzed, and results are risk adjusted and returned to the centers to serve as a basis for quality improvement. In this way, he explained, the performance of individual surgeons and centers is carefully monitored so that corrective action can be taken if problems are identified.
Wolfe observed that long-term complications are more difficult to study because patients disperse into the population and typically do not return to the center where the surgery was performed. Although the LABS Consortium still had contact with 92 percent of its participating patients at year 7, he noted, determining the frequency of iron deficiency, anemia, or other
problems was infeasible because the patients were going to their primary care providers to diagnose and treat such problems. He explained that the most common nutrient deficiency in these patients is iron deficiency anemia, which is readily correctable. There does not appear to be an adaptation over time to absorption of micronutrients, he said, so the risk of micronutrient deficiency is ongoing, and the need for supplementation continues. He added that, although nutrient deficiencies leading to central or peripheral neuropathy are rare, they can occur and can be tragic when they do.
The absence of a long-term control group makes it difficult to assess the issue of bone metabolism over time, said Wolfe. He noted that about 80 percent of bariatric surgery is performed in women, who have a problem with osteoporosis and fractures as they age, and this further complicates determining whether bariatric surgery has deleterious effects on bones.
Wolfe also pointed out that metabolic complications can occur over time. He explained that hypoglycemia tends to be postprandial and is more common among bariatric surgery patients who did not have diabetes at the time of the surgery. Severe hypoglycemia is rare, he said, but less severe cases are relatively common. He added that, because most people are treated for their symptoms before they ever get to an emergency department or undergo a health care intervention, the incidence of common hypoglycemia is difficult to determine.
Wolfe continued by focusing on renal function. Renal stones are more common among people with obesity, he noted, and there is concern that gastric bypass will decrease renal function and increase the incidence of renal stones. However, he said, the available data in this regard are not clear, with some data showing that people with impaired renal function at the time of bariatric surgery experience improvement in their renal function over time.
Complications requiring subsequent surgeries, such as intestinal obstruction or marginal ulceration, can occur, Wolfe stated. In the LABS Consortium, about 13 percent of patients over 7 years required subsequent surgery of some sort, most commonly for ventral hernia at one of the incision sites. “Hopefully these are all manageable and do not represent a major problem,” said Wolfe.
Indices of depression and quality of life tend to respond well to bariatric surgery, Wolfe observed. However, some cases of depression may not respond to weight loss, he noted, and suicide has been identified as somewhat increased following bariatric surgery. According to Wolfe, the numbers are very small, making them difficult to analyze statistically. Suicidal ideation is prevalent among this population before they undergo bariatric surgery, and its incidence following bariatric surgery appears to be about the same.
Wolfe reported that studies of access to bariatric surgery and of who undergoes the surgery show that, as noted above, women are much more
likely to seek and undergo the surgery; moreover, people with private insurance are 2.5 times more likely to undergo the surgery than people with public insurance (Bhogal et al., 2015). He noted that in the LABS Consortium, 8 percent of patients were Medicaid patients, whereas the rate should have been twice that according to epidemiologic data. Despite this population being heavier and having a higher prevalence of diabetes and severe walking and other limitations relative to the non-Medicaid population, Wolfe suggested that providers may be discouraged from accepting public insurance because of its lesser reimbursement.
Wolfe continued by remarking that “there is certainly room for improvement with regard to access and delivery of effective care for obesity.” He pointed out that fewer than 2 percent of patients who are eligible for bariatric surgery undergo such surgery in any given year, and the number being treated with pharmacotherapy is similarly low (Thomas et al., 2016).
Wolfe noted further that obesity is a heterogeneous condition, but clinical care providers tend to put all people with obesity in the same category. He suggested that if there were a basis for telling specific patients their risk for developing an obesity-related condition, such as an obesity-related cancer, doing so could have a great impact on interest in and motivation to enter the health care system and undergo obesity treatment. He asserted that individualization also could help match patients with interventions. “We need more detailed research in order to better characterize the disease risk that the patients face,” he argued, “as well as make better predictions of outcomes from intervention.”
Wolfe also made the interesting point that he routinely counsels patients to be prepared for friends, family, and others to be unkind or have other negative responses to their weight loss.
ONE PATIENT’S EXPERIENCE
“There has never been a time in my entire life, including after bariatric surgery, where I was not at least overweight,” said Nikki Massie, a professional writer, marketer, and online community leader living in Baltimore, Maryland. She started researching bariatric surgery when she weighed about 340 pounds and before trying other interventions. “I had an on-again/off-again relationship with primary care physicians,” she said, partly because her interactions with them around weight often were uncomfortable and unhelpful, and partly because of problems with insurance. “I never kept one for very long,” she noted.
At an informational session with a physician at St. Agnes Hospital in Baltimore, Massie learned that the practice performed Roux-en-Y gastric bypass and laparoscopic adjustable band surgery. After an initial physical examination, she was told that she probably would benefit more from sur-
gery if she had a primary care physician, so she found one who was amenable to the idea of bariatric surgery and willing to work with the bariatric team. Her surgeon originally suggested lap band surgery because she had no associated conditions, but her research had led her to conclude that lap band surgery was not right for her.
Massie underwent Roux-en-Y gastric bypass surgery in January 2008. Her outcomes were good, and she has maintained a weight loss of 125 pounds while undergoing repeated follow-ups. She said she has tended to maintain a higher weight than she perceived herself to have, which caused some psychological difficulties. “There was not a psychologist on staff in my bariatric practice,” she said. “It was up to me to keep up and maintain psychological care on my own. I had trouble with that, because I had some gaps in my insurance. Navigating those schisms between what size you are in clothes and what size you are on the scale . . . became difficult for me.”
For the past 4 years Massie’s weight has been at about 205 pounds, which is “a weight that I can maintain pretty easily.” She exercises regularly, maintains a regular vitamin regimen, and meets with a dietician to regulate her eating. She still sees her bariatric surgeon once per year. “That comes in very handy,” she explained, “because of the fact that my bariatric surgery care is a part of my overall health care. It affects other things in my life and other realms of health care in my life. Last year, I was diagnosed with a very early stage of breast cancer. I had a bilateral mastectomy for treatment. Afterward, my micronutrient levels did some funny things. My doctor wasn’t understanding the pattern of how that was happening. I was able to get him connected to my bariatric surgeon to talk about whether or not these were things that were necessarily of concern because of the surgery I had, because of being treated for cancer, or whether it was something that was relatively normal for somebody who is 8 or 9 years post-op gastric bypass surgery. I thought that was very important, that link between my primary care physician and my bariatric surgeon.”
Since Massie’s surgery, the practice has added dieticians and a series of classes for preoperative education. Patients can enter a longer postoperative program focused on dietary and behavior changes if they regain weight. In-person and online support is available via a private Facebook group.
“I consider the outcome that I got very successful in terms of lifestyle intervention and changing how I move and how I eat,” Massie stated. Since her surgery, she has become a community leader and patient advocate within the bariatric community and serves as a board member of the Obesity Action Coalition. She noted that her social relationships “completely changed for me after bariatric surgery.” She derives value from talking to other people about their experiences and providing support. “Peer support is a very important part of aftercare with weight loss surgery,” she said. “Peer supporters have to be very careful not to try to imitate medical pro-
fessionals. On my platform in my community, I always send people to their professionals if they ask a question that is inappropriate for me to answer. . . . But in the social relationships that are built, and the whole culture that is built around weight loss surgery, there is a lot of affirming power.”
FOLLOW-UP CARE
A topic discussed during the question-and-answer session was how to encourage patients to get follow-up care after surgery. Aronne noted that his center tells surgical patients that, at the first sign of weight gain or excessive hunger, they should come in right away. “We look at it the way cardiologists look at chest pain,” he explained. “That, we find, gets people to come back.”
Wolfe said he and his colleagues provide a packet of information informing primary care providers about what to look for in patients who have undergone bariatric surgery and what should be done if any problems are identified. Many of his patients have to travel great distances, he noted, and people from Alaska or Montana are not going to come back to Portland, Oregon, for all their follow-up visits. “If there is an obesity medicine specialist in their community, that is great,” he said. “There often is not, so we are looking for an intermediate way to provide information.”
The moderator of the session, Adam Tsai of Kaiser Permanente in Denver, noted that the Kaiser system has integrated electronic medical records that can be shared and an advice referral function. He explained that this “allows our primary care physicians to consult with us and with our surgeons when they need to know what to do with a micronutrient deficiency, for example.”
Massie emphasized the importance of informing patients that surgery alone is not intended to cure their obesity. “There is this misconception in the patient community that the surgery is supposed to be the end of the line for your obesity treatment,” she observed. As a result, patients can conclude that they have failed if surgery does not completely resolve their obesity. “There is a lot of shame that keeps people from going back to their surgeon,” she said. “I interact with hundreds of post-ops every day through my online community who are straight out ashamed to go back to their surgeon, or are waiting to lose 10 or 15 pounds before they go to see their surgeon about problems, which is working against what they want to do. Pointing out to your patients at the outset of treatment that bariatric treatment may not be the only intervention required to treat their obesity—and to stress that it is a lifelong approach that they are taking, and a lifelong thing that they are embarking on—is probably helpful in getting people back into the room in the long term.”








