
8
Payment Considerations
The Patient Protection and Affordable Care Act (ACA) contains a mandate for coverage of obesity treatment, corresponding to the recommendations of the U.S. Preventive Services Task Force for screening of all
adults and children aged 6 and older for obesity.1 However, coverage is highly variable among states (National Conference of State Legislatures, 2017), observed Don Bradley, associate consulting professor, Department of Community and Family Medicine, Duke University, and moderator of the panel on payment considerations. This variability also extends to Medicaid coverage for obesity services, he noted. The essential health benefits from the ACA apply to Medicaid programs, but Medicaid services have been expanded in some states and not in others (Kaiser Family Foundation, 2017). Coverage for obesity-related nutritional consult services, obesity-related disease management and education services, and obesity medications are similarly variable and partial across states, Bradley observed. However, he reported, almost all the states cover bariatric surgery through Medicaid (STOP Obesity Alliance, 2014). He listed a number of considerations that payers take into account in making coverage decisions: (1) customer demand/preference for a benefit or service; (2) cost (especially costs that are as low as possible and predictable); (3) evidence for effectiveness and efficiency; (4) deliverable quality outcomes, especially on metrics of the Centers for Medicare & Medicaid Services (CMS) and the National Committee for Quality Assurance; (5) network for delivery; (6) customer experiences and satisfaction; (7) ease of administration; (8) compliance/mandates/essential health benefits; (9) risk (including legal, financial, regulatory, public relations, and network forms of risk); and (10) profitability/margin. Three speakers followed Bradley’s introduction of the panel, addressing a number of these topics.
THE EMPLOYER’S PERSPECTIVE
Thomas Parry, president emeritus and co-founder of the Integrated Benefits Institute, began by observing that employers represent the single largest segment providing health care coverage (see Figure 8-1). For them, he said, obesity coverage is a challenge. Parry is a member of an advisory group for a study being supported by Novo Nordisk—the ACTION Study—that includes in its design surveys of 3,000 people with obesity, 600 providers and practitioners of care for obesity patients, and 150 employers. According to these surveys, two-thirds of employers believe obesity is a disease, which is “a very important starting point if you are going to talk to employers about coverage,” asserted Parry. Second, he said, 85 percent of employers agree
___________________
1 Adults: https://www.uspreventiveservicestaskforce.org/Page/Document/UpdateSummaryFinal/obesity-in-adults-screening-and-management (accessed November 14, 2017); children: https://www.uspreventiveservicestaskforce.org/Page/Document/RecommendationStatementFinal/obesity-in-children-and-adolescents-screening (accessed November 14, 2017).
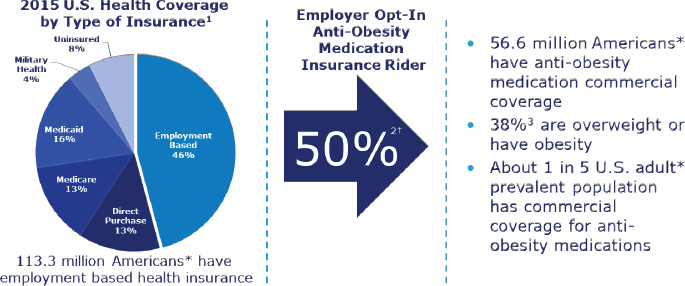
NOTES: *Adults 18 years and older; † Assumption: percentage of employer opt-in is reflective of the percentage of individuals covered.
SOURCES: Presented by Thomas Parry on April 6, 2017 (data from 1Barnett and Vornovitsky, 2016; 2Benfield Research, EMI Trends, 2014; 3Ogden et al., 2014). Reprinted with permission from Novo Nordisk.
that a 10 percent weight loss would be extremely beneficial to employees with obesity. Third, he reported, 70 percent of employers believe that the wellness programs they provide are valuable to employees; however, only 17 percent of people with obesity believe their employers’ wellness programs are effective for them (Kaplan et al., 2016).
Parry believes this last point represents a key challenge for both people with obesity and employers. Employers tend to think about wellness in terms of eating habits, gym memberships, exercise, and similar activities, he noted, whereas people with obesity are looking for a broader and holistic approach to wellness.
Employers are greatly concerned about the costs of care, Parry observed (Kaplan et al., 2016). For example, he said, they are getting ready for an onslaught of costs around specialty pharmaceuticals. “If we don’t effectively deal with the question of cost of coverage,” he argued, “then we will never get the employer’s attention about this issue.”
Parry also has worked with Ronald Kessler of Harvard Medical School to analyze data from a research-validated self-reporting tool called the Work and Health Performance Questionnaire (HPQ), which has generated data on about 100,000 employees. According to these data, Parry reported, about two-thirds of employees with obesity have never been treated. “This represents a critical challenge for employers,” he asserted. “As long as employers think of this as a cost, then this idea of ‘we should increase treat-
ment penetration’ is a real challenge. Because what, of course, happens to cost when more people get care? In the short term, costs increase.”
The answer to this dilemma, Parry argued, is to move beyond medical and pharmaceutical expenses to a broader consideration of costs. He reported that according to a recent study of 10 employers for which the research team integrated medical and pharmacological claims data with absence and performance data from the HPQ, the costs of absences from work and lost productivity because of poor health exceed medical and pharmacy costs for a wide range of health conditions, including obesity (Loeppke et al., 2009). “We have to help employers understand that the window into what is important cannot be gleaned from only looking at medical and pharmacy claims data,” said Parry. “Other sources of information have to be part of that view.” Absenteeism and lost productivity are particularly germane to chief financial officers, CEOs, and other people who are running businesses, he asserted. He argued that using data to demonstrate that good care is going to lead to better outcomes that drive business performance, including costs, will produce “a conversation that the employers are willing to listen to.”
A PRIVATE PAYER’S PERSPECTIVE
California traditionally carries a lower population health burden than many other states, noted Bryce Williams, vice president for well-being at BlueShield of California, with prevalence rates for obesity, smoking, and comorbidities all being lower than the national average. However, he said, the difference “between one in three Americans and one in four Californians [having obesity] is really a distinction without a difference,” he said. “There is still a problem.”
Williams observed that with the sixth-largest economy in the world, California has populations and communities with widely varying levels of health, noting that a driver heading east from the Pacific Ocean will soon encounter communities very similar to communities in other parts of the United States. BlueShield of California recognizes “that we have to be a part of the solution for geographic, ethnic, and socioeconomic health disparities,” he said.
Williams explained that the company follows the compliance guidelines of the ACA, offering zero-cost-shared preventive member benefits in obesity screening and counseling. “Our provider community has come a long way in being more effective at doing obesity screening,” he reported. “Counseling is another matter,” he acknowledged. “Historically, this is a chronically underutilized benefit, for a variety of reasons.” Providers tend to be confused about what the benefit is, he noted, especially when commercial health plans put a slightly different twist on it, and they do not
necessarily have the referral networks for patients that need such services. They often report that they are still uncomfortable talking about obesity with their patients, he said, and “when they do, they don’t feel like they do a great job of it.”
Health plan members also are confused, Williams added, with statements being complex and difficult to interpret. Moreover, he observed, members generally do not feel comfortable talking with their providers about obesity. “Coverage doesn’t necessarily mandate success in this space,” he said.
With regard to treatment, Williams continued, BlueShield of California covers a number of pharmaceutical interventions for obesity based on eligibility criteria, prior authorization, and other criteria. However, “pharmacy can get really confusing,” he suggested. “There is brand. There is generic. There is tiering. There are copays. There are 8 million things that make pharmaceutical fills complex. My guess is [that] a good number of Californians figure it is easier to go to a private weight loss clinic and get a prescription for their medications that way. It is more convenient than dealing with the health plan.” Williams added that the company also covers bariatric surgery with certain conditions, and it works with the Blue Distinction Centers network, which comprises centers of excellence.
BlueShield of California is not in the business of delivering clinical services—it is a health plan, Williams clarified. However, he added, it is interested in providing care in the area of lifestyle medicine. “We believe that, in the area of diet and lifestyle, the market solution isn’t out there yet,” he explained. “We are not saying it is anybody’s fault. It is not the providers’ fault. It is not the health and wellness industry’s fault. But we believe there is room to actually go out and do that.” He observed that nutrition, exercise, smoking, insufficient sleep, and chronic diseases such as diabetes all are linked to obesity. Proven intensive lifestyle interventions affect these risk factors and outcomes, but, he asserted, they are not having a large enough influence. “There is a big discrepancy between what the research literature is showing and what is actually happening with our consumers, with our members, with average Americans,” he said.
Interventions that work need to be convenient, Williams suggested. For example, brick and mortar programs need to be accessible, close to work and home, and easy to get into and out of (e.g., easy parking). Williams added that convenience often also means embracing digital technologies such as phones, pads, fitness trackers, scales, blood pressure cuffs, and other individual technologies. “We have to connect people either in person or digitally to help build support networks so people can succeed,” he argued. Interventions also need to be credible and supported by evidence, he asserted. For example, he cited a physical activity initiative called the Walkadoo program, a mobile-based physical activity platform integrated
with all the popular fitness trackers (Poirier et al., 2016). Data from the trackers are used to shape and deliver personalized goals via text or email and connect to support networks. According to Williams, “It engages the consumer and provides personalized, contextualized data for you, not just 10,000 steps a day.” According to one study, he noted, more than 75 percent of participants were still engaged after 90 days, and physical activity showed a 20 percent improvement (or more than 1,000 steps per day).
Williams reported that BlueShield of California also has embraced the Centers for Disease Control and Prevention’s Diabetes Prevention Program, which it has rolled out statewide to all its members, although the program is still just beginning. With 600 community partners in 43 of California’s 53 counties, he explained, the program provides multiple digital options, including online, smartphone, and text, since people want to engage in different ways. It uses fitness trackers and wireless scales to engage people and gather data that document the program outcomes.
“We believe there is a right solution for anybody,” Williams said in closing. “This is going to be multifactorial and multidisciplinary. We firmly believe in raising the game on diet and lifestyle interventions that are clinically effective, cost-effective, come with virtually no side effects and no risks—and we want to make it free to everybody.”
A PUBLIC PAYER’S PERSPECTIVE
Medicaid is the largest single payer of health care for people in the United States, covering more than 70 million children and adults. Medicaid and the Children’s Health Insurance Program (CHIP) can therefore play a key role in increasing access to obesity prevention and treatment services, asserted Deirdra Stockmann, lead for secondary prevention in the Division of Quality and Health Outcomes, Center for Medicaid and CHIP Services, CMS. She described the potential of Medicaid and CHIP to cover obesity prevention and treatment services.
Medicaid is a federal–state partnership that allows states flexibility to design programs that address their needs and reflect their priorities, Stockmann explained, which results in considerable variation across states in what obesity-related services, including obesity treatments, are covered for children and adults, and reflects the variability in the statutory authorities and regulations under which those services are defined. She highlighted some of the most common ways states are choosing to cover obesity prevention and treatment services in their Medicaid and CHIP programs.
In terms of coverage for children, through Medicaid’s Early and Periodic Screening, Diagnostic, and Treatment (EPSDT) benefit, Medicaid-eligible children under age 21 are assured coverage of preventive and comprehensive health services, noted Stockmann. She explained that the
EPSDT benefit includes screening, vision services, dental services, hearing services, and all services necessary to ameliorate health conditions discovered through the screenings that are covered. Under the screening component of EPSDT, she continued, state Medicaid programs are responsible for ensuring that children receive periodic physical examinations, including well visits, complete health and developmental histories, and health education. She added that screening for obesity falls under both the screening component of EPSDT and health education, which serves as an opportunity for a provider to discuss health concerns such as healthy weight and nutrition with a child, parent, guardian, and family. In addition, she noted, any medical service or treatment determined to be medically necessary for a child, such as nutritional assessments and counseling, medications, or surgery, would be available through the Medicaid EPSDT benefit.
Medicaid programs differ more from state to state on coverage of obesity-related services for adults noted Stockmann. She explained that federal Medicaid law requires states to cover certain mandatory benefit categories, such as hospital services, and allows them to choose whether to cover other, optional benefit categories, such as diagnostic screening and preventive services. She added that states can include obesity treatment services under a number of different benefit categories, required or optional, depending on how they have structured their Medicaid plan.
Stockmann described a newer and important state plan option for providing obesity treatment to both children and adults—the use of health homes, which can coordinate care for enrollees with chronic conditions, including overweight and obesity. She explained that health homes operate with a whole-person philosophy, whereby providers integrate and coordinate all primary, acute, and behavioral health care services, as well as long-term services and supports, to treat a whole person. Health home services include comprehensive care management, care coordination, health promotion, patient and family support, and referral to community and social support services.
As an example of this approach, Stockmann cited Missouri, which has established health homes for a number of different conditions and recently made a change so that obesity qualifies as a stand-alone condition, rather than people being required to have two or more chronic conditions. “We are really looking forward to seeing what benefits [are included] and the outcomes and performance of those health homes,” she said.
Another option for states to improve access to obesity care and reduce cost described by Stockmann is the Preventive Services Provider Rule. She explained that in 2014, CMS revised regulations to accurately reflect the statutory provision that states have the option of allowing preventive services to be provided by practitioners other than physicians or licensed practitioners as long as a physician or licensed practitioner recommends
the service. She observed that this rule could be used to provide services to people who have obesity or are overweight and potentially lower costs. In general, she noted, if states want to make changes to the obesity services provided in their Medicaid and CHIP programs, they need to consider their state plan, context, and priorities and work with CMS to identify the best authorities under which to make the changes. “It does and will continue to look different from state to state,” she said.
Coverage of services does not automatically lead to utilization of services or imply a particular quality of care, Stockmann emphasized. To improve this situation, she suggested, states could consider how to work with their Medicaid managed care organizations and their health plans as partners to increase the delivery and quality of obesity treatment and services. As an example, she suggested that managed care organizations could conduct performance improvement projects as part of their Medicaid contracts, including obesity prevention and treatment as an important focus. She also observed that states could incorporate pay-for-performance arrangements that include metrics related to obesity care into their managed care contracts. She added that CMS has core sets of measures for children and adults enrolled in Medicaid and CHIP that include a measure for body mass index (BMI) assessment. “While I am well aware that it is a process measure with many limitations,” she said, “we do encourage states to consider including it as part of a set of metrics that they collect and use to drive improvement for the quality of care delivered in their states.” Adult measures also exist for screening and managing diabetes and managing blood pressure.
Stockmann stressed that beneficiary and provider outreach is critical to improving the delivery of care, particularly behavioral interventions and chronic disease management interventions and services. She noted that in 2015, CMS released a set of free and customizable materials, called Living Well, to help states promote their preventive services. Posters, fact sheets, and an image library can be adapted to states’ needs and cobranded with the logos that state residents recognize.
Finally, Stockmann emphasized that collaboration across state agencies and with other public health partners is essential to making progress on any chronic disease prevention and management goal. For example, she observed, many different organizations and states are working together on diabetes prevention and management from different angles and making progress. “There may be effective ways to link some of the momentum and efforts around diabetes prevention and management with obesity treatment to have a greater impact,” she suggested. For example, she noted in response to a question, collaborations with the Special Supplemental Nutrition Program for Women, Infants, and Children (WIC) could offer a way to “meet people where they are.”








