
17
Smoking Cessation Among Adults
For both individuals and for public health, the central potential benefit of e-cigarettes is to promote smoking cessation among established cigarette smokers or at least to reduce smokers’ exposure to combustible tobacco products. Although all tobacco use has health risks, the risk is highest when the user inhales the smoke produced by burning tobacco. Because e-cigarettes do not burn tobacco or generate smoke, the use of e-cigarettes likely confers a lower overall health risk than does smoking combustible tobacco products (see Chapter 18). Established combustible tobacco smokers who completely switch to using e-cigarettes therefore would be expected to reduce their tobacco-related health risks. Additional benefit would be expected if e-cigarette users subsequently stopped using both e-cigarettes and combustible tobacco products.
This section addresses the question: Do e-cigarettes help smokers quit smoking combustible tobacco cigarettes? In short, are e-cigarettes effective smoking cessation aids capable of increasing abstinence from combustible tobacco products compared with no treatment, a placebo treatment (usually a non-nicotine–containing e-cigarette), or a Food and Drug Administration (FDA)-approved smoking cessation aid such as a nicotine replacement product, varenicline, or bupropion?
A related but broader question is the following: What is the impact of the availability of e-cigarettes on population smoking cessation rates? The population impact of e-cigarettes will be a product not only of their effectiveness in an individual smoker but also of their reach, defined as the proportion of smokers who use them. E-cigarettes’ current status as
easily accessible consumer products may contribute to their appeal. If e-cigarettes have greater appeal to smokers than current FDA cessation aids, they could enhance population cessation rates simply by encouraging more current combustible tobacco cigarette smokers to make a quit attempt when they would not otherwise have attempted to quit tobacco.
CONCEPTUAL FRAMEWORK: PATTERNS OF E-CIGARETTE USE AMONG ESTABLISHED SMOKERS
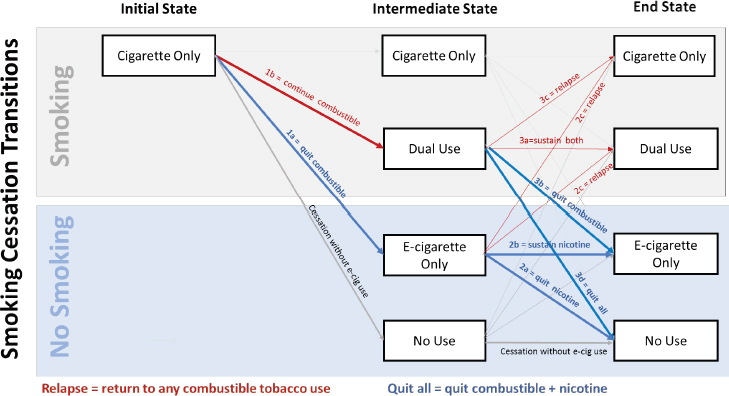
Ultimately, the potential health benefit of e-cigarette use for cigarette smokers will depend on the characteristics of the smoker, the product (including both the e-cigarette device and e-liquid), and how the device is used. The pattern of e-cigarette use is likely to vary among individual smokers and over time as regular combustible tobacco cigarette smokers experiment with and perhaps transition to e-cigarettes. Figure 17-1 illustrates a conceptual model of these transitions.
The extent of risk reduction will depend on several factors that are defined by the answers to the following questions:
- Does the smoker switch completely to e-cigarettes (1a in Figure 17-1) or use both combustible tobacco cigarettes and e-cigarettes, a pattern referred to as dual use (1b in Figure 17-1)? The extent of harm reduction should be much greater for a smoker who switches completely to e-cigarettes than for a smoker who uses e-cigarettes to replace
-
some, but not all, combustible tobacco cigarettes with e-cigarettes (dual use) because even small exposures to tobacco smoke increase health risks, especially the risk of cardiovascular disease (HHS, 2014). Because the risk of even small exposures to tobacco smoke may not be widely appreciated by the public, dual users may overestimate the degree to which they are reducing their tobacco-related risk and perhaps be less likely to continue efforts to stop combustible tobacco use altogether (Kasza et al., 2017).
- If the smoker switches completely to e-cigarettes, is the use of e-cigarettes:
- A temporary state leading to abstinence from both combustible tobacco cigarettes and e-cigarettes? (2a)
- A persistent state, in which exposure to e-cigarettes is sustained long-term? (2b)
- A temporary state followed by relapse to combustible tobacco products, with or without continued e-cigarette use? (2c)
E-cigarettes should have the greatest benefit for the cigarette smoker who switches completely from combustible tobacco cigarettes to e-cigarettes or uses e-cigarettes for a limited time and then quits using both cigarettes and e-cigarettes (2a in Figure 17-1), producing abstinence from both tobacco smoke and nicotine, as well as any other potentially harmful constituents of e-cigarette aerosol. However, a complete switch from combustible tobacco cigarettes to e-cigarettes, with e-cigarette use persisting indefinitely, is still likely to reduce harm (2b). By contrast, a temporary switch to e-cigarettes followed by relapse to combustible tobacco use (2c) is unlikely to confer meaningful long-term reduction in health risk and could add whatever risk is conveyed by e-cigarette use.
- If the smoker becomes a dual user of cigarettes and e-cigarettes, is e-cigarette use:
- A persistent state of continued exposure to both tobacco smoke and to e-cigarette constituents? (3a)
- A temporary state en route to exclusive and persistent use of e-cigarettes? (3b)
- A temporary state followed by relapse to smoking combustible tobacco products? (3c)
- A temporary state on route to abstinence from all nicotine products? (3d)
If dual use is a transitional state only, the extent of harm will depend on whether the individual returns to smoking only combustible tobacco cigarettes (relapse, 3c in Figure 17-1); transitions completely to e-cigarettes,
further reducing harm by reducing exposure to tobacco smoke (3b); continues dual use indefinitely (3a); or stops using both combustible tobacco cigarettes and e-cigarettes (3d). The last option, abstinence from tobacco smoke, nicotine, and other constituents of e-cigarette aerosol, is optimal. By contrast, a temporary switch to dual use followed by relapse to combustible tobacco use (3c in Figure 17-1) is likely to confer minimal long-term reduction in health risk.
Stopping smoking reduces the risk of tobacco-related diseases and extends life expectancy by up to a decade (Jha and Peto, 2014). The risks of cigarette smoking are well described, while the risks of e-cigarette use are just beginning to be assessed and much uncertainty remains. If e-cigarette use helps a smoker to completely quit combustible tobacco use (2a and 3d in Figure 17-1), some degree of e-cigarette risk could still generate a net health benefit, as long as exposure to e-cigarettes is temporary and the benefit exceeds net short-term risk. However, if the final state is persistent e-cigarette use replacing combustible tobacco cigarette use (2b and 3b in Figure 17-1), a lower level of e-cigarette risk would be required to generate an overall net benefit to the individual. Temporary e-cigarette use with return to combustible tobacco use (2c and 3c in Figure 17-1) would likely have no net individual health benefit.
Currently, little information is available about the relative frequency at which smokers using e-cigarettes follow each path or about how the risks and benefits of each path compare. For the purposes of this chapter, the committee defines smoking cessation as stopping all combustible tobacco product use. It could be achieved following paths 2a, 2b, 3b, or 3d in Figure 17-1. This definition allows for sustained exposure to nicotine and other constituents in e-cigarettes. A more stringent criterion requiring nicotine abstinence from all sources is represented by paths 2a and 3d in Figure 17-1.
EVIDENCE REVIEW: LEVELS OF EVIDENCE AVAILABLE
The interpretation of epidemiological evidence must consider both its internal and external validity. Internal validity is a measure of how likely the finding of an association or causal relationship is accurate, which is determined by the degree to which a study minimizes systematic error (bias). Self-selection and confounding are important threats to internal validity. External validity addresses the extent to which a finding can be generalized to another context or to the general population.
To assess the efficacy of e-cigarettes for smoking cessation, the randomized controlled trial (RCT) provides the strongest study design to protect against threats to internal validity. Ideally, an RCT would enroll cigarette smokers seeking to quit and randomly assign them to switch
from smoking combustible tobacco cigarettes to either using e-cigarettes or a comparison condition. The comparison condition could be no e-cigarettes (i.e., no treatment); a placebo (non-nicotine e-cigarette); an FDA-approved smoking-cessation pharmacotherapy, such as nicotine replacement, varenicline, or bupropion; or some other evidence-based cessation intervention, such as behavioral counseling. Each comparison condition would answer a slightly different variant of the question about e-cigarettes’ effectiveness. Ideally, the RCT’s primary outcome would be biochemically confirmed abstinence from combustible tobacco products 6 to 12 months later. Repeated assessments of adverse events occurring during the period of the study would allow for assessment of risks of e-cigarette use. As described below, the committee found that few RCTs have been conducted to address the question about effectiveness of e-cigarettes.
Prospective observational (cohort) studies offer less protection from threats to internal validity, but can provide valuable supporting evidence, especially when data from RCTs are limited (as in the current situation) or when randomization is unethical. A cohort study that could address the question could compare smokers who use e-cigarettes in a quit attempt with those who do not and assess the association between exposure to e-cigarettes and abstinence from tobacco products. An optimal prospective observational study design would identify and follow a large cohort of smokers who want to quit or are making a quit attempt, assess e-cigarette exposure in detail before the smoking cessation outcome is assessed, biochemically confirm self-reported tobacco abstinence, and adjust for multiple potential confounding factors associated with e-cigarette use and with smoking cessation. The limitation inherent in this study design is that smokers choose whether or not to use e-cigarettes. Those who do and do not choose to use e-cigarettes may differ in ways that independently influence a smoker’s likelihood of success, confounding the observed association of e-cigarettes to quitting. Statistical methods can adjust for these factors, but unmeasured confounding remains a potential threat and makes it difficult to infer causality to an observed relationship between e-cigarette use and smoking cessation success.
Cross-sectional studies compare the prevalence of current or past e-cigarette use between current and former smokers. They provide a lower level of evidence and generally cannot be used to ascertain causality.
External validity depends on the representativeness of the study sample to the overall population to which a scientist or policy maker may wish to apply the study’s findings. Studies that recruit or include nationally representative samples of smokers allow for broad generalizability of study findings and therefore maximize external validity. However, RCTs, which have the best internal validity, can rarely be conducted using large,
nationally representative samples of individuals that maximize external validity. There is usually a trade-off of internal and external validity in any study. The committee considered both factors in its review of the evidence to address questions about the efficacy of e-cigarettes for smoking cessation.
The public health impact of an intervention is a broader question that is a function of both the intervention’s efficacy and its reach (e.g., proportion of the at-risk population that uses it). As consumer products already easily accessible to smokers, e-cigarettes therefore have the potential to alter population cessation rates as a function of their efficacy as cessation aids and/or as a consequence of their appeal to smokers. RCTs measure the relative effectiveness of e-cigarettes in specific groups of smokers. However, the impact of e-cigarettes on population-level cessation rates will also depend on the proportion of smokers who use the products (i.e., reach) as well as characteristics of the products and how they are used (e.g., extent of nicotine delivery to the user). Population-level studies therefore provide an important additional type of evidence to evaluate in addressing the overall impact of e-cigarettes in a real-world setting. For studies of populations, prospective cohort and cross-sectional study designs are commonly used, with the former providing stronger internal validity to the latter.
EVIDENCE REVIEW: METHODS
The committee’s initial scan of the evidence identified individual studies with varying designs and rigor and also identified multiple published reviews. Most of the latter were systematic reviews that summarized the evidence either qualitatively in a narrative format or quantitatively using meta-analysis. Many of them were very recent, having been published between 2016 and 2017. Given the availability of multiple recent systematic reviews, the committee chose as its principal strategy to conduct a review of the existing reviews.
Committee staff conducted a formal literature search to identify evidence reviews that were published through August 31, 2017, and that addressed the effectiveness of e-cigarettes for smoking cessation. The search strategy is described in Appendix B.
The search identified 21 review articles published between 2014 and 2017 (El Dib et al., 2017; Franck et al., 2014; Hajek et al., 2014; Harrell et al., 2014; Hartmann-Boyce et al., 2016; Heydari et al., 2014, 2017; Ioakeimidis et al., 2016; Kalkhoran and Glantz, 2016; Khoudigian et al., 2016; Knight-West and Bullen, 2016; Lam and West, 2015; MacDonald et al., 2016; Malas et al., 2016; McRobbie et al., 2014; Orr and Asal, 2014; Patnode et al., 2015; Rahman et al., 2014, 2015; Vanderkam et al., 2016; Waghel et al., 2015).
Table 17-1 summarizes characteristics of the studies that were identified by the literature search. One committee member reviewed the results and excluded four publications. One report (MacDonald et al., 2016) was a protocol for an ongoing review that was not yet completed. A second review was an earlier version of a review from the Cochrane Collaboration (McRobbie et al., 2014), whose update is included. Two reviews were excluded because they did not provide specific data on e-cigarettes and cessation; in both cases, the same lead author subsequently published a review of e-cigarettes and cessation that is included in this review (Heydari et al., 2017; Rahman et al., 2015).
One committee member reviewed each of the remaining 17 studies to determine whether they met criteria as systematic reviews, using criteria developed for a previous report (NASEM, 2017):
- Does the article describe a search involving at least two databases?
- Does the article describe a search involving appropriate search terms?
- Does the article describe a search involving pre-specified eligibility criteria?
- Does the article include a risk-of-bias discussion and/or quality assessment?
- Does the article include a meta-analysis or qualitative synthesis of findings?
Of the remaining reviews, 17 met these criteria. Four were published in 2014, four in 2015, seven in 2016, and two in 2017. Six of the reviews conducted a formal meta-analysis, pooling data from at least some of the identified studies (El Dib et al., 2017; Hartmann-Boyce et al., 2016; Kalkhoran and Glantz, 2016; Khoudigian et al., 2016; Rahman et al., 2014; Vanderkam et al., 2016). Two other reviews cited the results of a meta-analysis that had previously been published elsewhere (Ioakeimidis et al., 2016; Knight-West and Bullen, 2016). All assessed a smoking cessation endpoint and some of them also assessed other endpoints such as smoking reduction (see Chapter 18 on Harm Reduction).
The scan of the studies that were not included in the systematic reviews and were published through August 31, 2017, identified several population studies, whose results are described below. No new RCTs were identified. Additional observational and cohort studies were identified, but their results were generally consistent with studies in the systematic reviews.
TABLE 17-1 Systematic Reviews of E-Cigarettes and Smoking Cessation Identified by Literature Search
| Reference | Systematic Review | Meta-Analysis | Search Through | Studies Included |
|---|---|---|---|---|
| El Dib et al., 2017 | Yes | Yes | 12/29/2015 (updated until 5/2016) | 12 (3 RCT, 9 cohort) |
| Franck et al., 2014 | Yes | No | 9/15/2013 | 7 |
| Hajek et al., 2014 | Yes | No | 2/2014 | Not specified |
| Harrell et al., 2014 | Yes | No | 11/2013 | 15 |
| Hartmann-Boyce et al., 2016 | Yes | Yes | 1/2016 | 24 (3 RCT, 21 cohort) |
| Explicit Quality Assessment? | Conclusion Regarding E-Cigarettes and Cessation | Comments |
|---|---|---|
| Yes | “There is very limited evidence regarding the impact of e-cigarettes on tobacco smoking cessation, reduction or adverse effects: data from RCTs are of low certainty and observational studies of very low certainty…. This review underlines the need to conduct well-designed trials measuring biochemically validated outcomes and adverse effects” (El Dib et al., 2017, p. 1). | |
| Yes | “Given the limited available evidence on the risks and benefits of e-cigarette use, large, randomized, controlled trials are urgently needed to definitively establish their potential for smoking cessation” (Franck et al., 2014, p. 1945). | |
| No | None | Broad general review |
| No | “Data on the use of e-cigarettes for quitting smoking are suggestive but ultimately inconclusive” (Harrell et al., 2014, p. 381). | |
| Yes | “There is evidence from two trials that e-cigarettes help smokers to stop smoking in the long term compared with placebo e-cigarettes. However, the small number of trials, low event rates, and wide confidence intervals around the estimates mean that our confidence in the result is rated low” (Hartmann-Boyce et al., 2016, p. 2). | Update of 2014 Cochrane review (see McRobbie et al., 2014) |
| Reference | Systematic Review | Meta-Analysis | Search Through | Studies Included |
|---|---|---|---|---|
| Heydari et al., 2017 | Yes | No | 9/2014 | 69 |
| Ioakeimidis et al., 2016 | Yes | Yes (report result of other meta-analyses | 6/2015 | 2 RCT |
| Kalkhoran and Glantz, 2016 | Yes | Yes | 6/17/2015 | 20 (1 RCT, 1 NRCT, 15 cohort, 3 cross-sectional) |
| Khoudigian et al., 2016 | Yes | Yes | 5/2014 | 5 |
| Explicit Quality Assessment? | Conclusion Regarding E-Cigarettes and Cessation | Comments |
|---|---|---|
| No | “Enough evidence to suggest that e-cigarettes are effective for quitting smoking is lacking, as is the evidence for the lack of their harm for respiratory system and thus being alternatives for smoking. However, further studies are needed” (Heydari et al., 2017, p. 27). | Non-standard methods to synthesize results |
| Yes | “Further research is needed to examine the longer term safety, potential for long-term use and efficacy as a cessation aid” (Ioakeimidis et al., 2016, p. 5). | |
| Yes | “As currently being used, e-cigarettes are associated with significantly less quitting among smokers” (Kalkhoran and Glantz, 2016, p. 2). | |
| Yes | “Limited low-quality evidence of a non-statistically significant trend toward smoking cessation in adults using nicotine e-cigarettes exists compared with other therapies or placebo. Larger, high-quality studies are needed to inform policy decisions” (Khoudigian et al., 2016, p. 257). |
| Reference | Systematic Review | Meta-Analysis | Search Through | Studies Included |
|---|---|---|---|---|
| Knight-West and Bullen, 2016 | Yes | Yes (report result of other meta-analyses) | 9/2015 | 11 (3 RCT, 8 cohort) |
| Lam and West, 2015 | Yes | No | 2/2015 | 4 |
| Malas et al., 2016 | Yes | No | 2/1/2016 | 62 |
| Explicit Quality Assessment? | Conclusion Regarding E-Cigarettes and Cessation | Comments |
|---|---|---|
| No | “Collectively, these studies suggest modest cessation efficacy … at least with the short-term use. More research, specifically well-conducted large efficacy trials comparing e-cigarettes with standard smoking cessation management (e.g., nicotine replacement therapy plus behavioral support) and long-term prospective studies for adverse events, is urgently needed to fill critica knowledge gaps on these products” (Knight-West and Bullen, 2016, p. 111). | |
| Yes | “Based on the current available literature, e-cigarettes may constitute an effective smoking cessation tool” (Lam and West, 2015, p. 98). | Limited to RCTs of e-cigarettes and cessation |
| Yes | “While inconclusive due to low quality, overall the existing literature suggests e-cigarettes may be helpful for some smokers for quitting or reducing smoking. However, more carefully designed and scientifically sound studies are urgently needed to establish unequivocally the long-term cessation effects of e-cigarettes” (Malas et al., 2016, p. 1926). |
| Reference | Systematic Review | Meta-Analysis | Search Through | Studies Included |
|---|---|---|---|---|
| Orr and Asal, 2014 | Yes | No | 3/2014 | 6 |
| Patnode et al., 2015 | Yes (of reviews, not original studies) | No (for e-cigarettes) | 3/1/2015 | 2 |
| Rahman et al., 2015 | Yes | Yes | 5/2014 | 6 (2 RCT, 2 cohort, 2 cross-sectional) |
| Vanderkam et al., 2016 | Yes | Yes | 6/14/2015 | 13 (2 RCT, 2 NRCT, 9 cohort) |
| Explicit Quality Assessment? | Conclusion Regarding E-Cigarettes and Cessation | Comments |
|---|---|---|
| No | “There is limited evidence for the effectiveness of e-cigarettes in smoking cessation…. Additional well-designed, long-term cessation studies are warranted, especially in comparison to current FDA-approved products” (Orr and Asal, 2014, pp. 1502, 1505). | |
| Yes | “Only two trials addressed the efficacy and harms related to the use of electronic cigarettes and these trials suggested no benefit on smoking cessation among smokers intending to quit” (Patnode et al., 2015, p. v). | Review of reviews only. Done for the update of the U.S. Preventive Services Task Force review of smoking cessation therapies |
| Yes | “Use of e-cigarettes is associated with smoking cessation and reduction. More randomized controlled trials are needed to assess effectiveness against other cessation methods” (Rahman et al., 2015, p. 2). | Update of Rahman et al., 2014, a narrative review of multiple endpoints, not just tobacco cessation |
| Yes | “The use of electronic cigarettes with nicotine decreases tobacco consumption among regular smokers. Further studies are needed to specify electronic cigarettes’ safety profile and its ability to cause a reduction in consumption and long-term cessation in smokers” (Vanderkam et al., 2016, p. 972). | Text in French. Primary outcome was smoking reduction, but cessation was a secondary outcome |
| Reference | Systematic Review | Meta-Analysis | Search Through | Studies Included |
|---|---|---|---|---|
| Waghel et al., 2015 | Yes | No | 5/2014 | 7 |
| Excluded Reviews | ||||
| Heydari et al., 2014 | Yes, but not specific to e-cigarettes | No | n/a | n/a |
| MacDonald et al., 2016 | Yes | Not at present time | Ongoing | 13 (in initial scoping of the literature in April 2014; ongoing at the time of publication) |
| McRobbie et al., 2014 | Yes | Yes | 7/2014 | 13 (2 RCT, 11 cohort) |
| Explicit Quality Assessment? | Conclusion Regarding E-Cigarettes and Cessation | Comments |
|---|---|---|
| No | “The limited evidence available supports that e-cigarettes may be effective as monotherapy for smoking cessation and reduction. However, superiority to nicotine replacement therapy was not proven” (Waghel et al., 2015, p. 8). | |
| n/a | n/a | Systematic review of all cessation methods, little focus on e-cigarettes |
| Yes | Ongoing project; no conclusions yet | Protocol paper for an ongoing meta-narrative review |
| yes | “There is evidence from two trials that e-cigarettes help smokers to stop smoking long-term compared with placebo e-cigarettes. However, the small number of trials, low event rates and wide confidence intervals around the estimates mean that our confidence in the result is rated ‘low’ by GRADE standards. The lack of difference between the effect of e-cigarettes compared with nicotine patches found in one trial is uncertain for similar reasons” (McRobbie et al., 2014, p. 2). | Updated as Hartmann-Boyce et al., 2016 |
| Reference | Systematic Review | Meta-Analysis | Search Through | Studies Included |
|---|---|---|---|---|
| Rahman et al., 2014 | Yes | No | 1/2014 | 5 (for cessation endpoint) |
NOTE: FDA = Food and Drug Administration; NRCT = non-randomized controlled trial; RCT = randomized controlled trial.
EVIDENCE REVIEW: RESULTS
Systematic Reviews
Overall, the reviews report on a small and overlapping evidence base. They consistently identified the same three RCTs whose characteristics and results are summarized in Table 17-2. The reviews also identified a few non-randomized interventional trials and a larger number of prospective observational trials and cross-sectional analyses. The reviews varied in the criteria used to include or exclude studies other than RCTs, with the result that the reviews summarized non-identical groups of observational cohort or cross-sectional studies. The committee reviewed in detail the most recent systematic reviews, defined as those published in 2016 or 2017, reasoning that these would be the most complete, and focused on those that conducted an independent formal meta-analysis. A total of five reviews met both criteria (El Dib et al., 2017; Hartmann-Boyce et al., 2016; Kalkhoran and Glantz, 2016; Khoudigian et al., 2016; Vanderkam et al., 2016). In addition, the committee examined in detail a 2016 systematic review that attempted a meta-analysis (Malas et al., 2016), but judged the studies to be too heterogeneous for this to be appropriate.
From this group, the committee identified two systematic reviews as those that provided the most comprehensive, most rigorous, and most recent summary of the available data (El Dib et al., 2017; Hartmann-Boyce et al., 2016). These two reviews were conducted independently by different groups of authors. Table 17-3 summarizes the two reviews’ methods, results, and conclusions and illustrates that the two reviews shared many similarities. Both were systematic reviews with meta-analysis. The search strategy for each began with the results of the search done for the 2014 Cochrane Collaboration review (McRobbie et al., 2014) and updated it,
| Explicit Quality Assessment? | Conclusion Regarding E-Cigarettes and Cessation | Comments |
|---|---|---|
| No | “E-cigarettes may have some potential as smoking cessation aids and, in the researchers’ view, should therefore be subject to further research and regulation similar to other nicotine replacement therapies” (Rahman et al., 2014, p. 1). | Narrative review that aims to cover multiple topics, not just cessation. Excluded because authors published an updated review focused on cessation (Rahman et al., 2015) |
adding studies that were published through December 2015 (El Dib et al., 2017) or January 2016 (Hartmann-Boyce et al., 2016). Both used comparable methods that are described in the Cochrane Handbook to screen studies, extract data, assess risk of bias, and assess the certainty of the overall body of evidence. Both included RCTs and prospective cohort studies that enrolled current combustible tobacco cigarette smokers regardless of intention to quit. They compared nicotine-containing e-cigarettes with non-nicotine e-cigarettes, other smoking cessation aids, or no aid. Both excluded cross-sectional studies. The primary measure of treatment effect was tobacco smoking cessation at the longest follow-up available (a minimum of 6 months) using biochemically validated cessation where available. There was general agreement about the results of the meta-analysis of RCTs and about the overall quality of the evidence. However, there were some differences between the methods used. The two reviews differed in their handling of missing outcome data in the statistical test used in the meta-analysis (fixed-effect or random-effect Mantel-Haenszel [MH] test), and the synthesis method used for non-randomized cohort studies (narrative review versus meta-analysis). They obtained similar results, but differed slightly in their interpretation of these results.
El Dib and colleagues (2017) conducted a systematic review and meta-analysis of the effect of e-cigarettes on tobacco use among cigarette smokers that was commissioned by the World Health Organization. The review compared nicotine-containing devices to non-nicotine e-cigarettes, no smoking cessation aid, or alternative smoking cessation aids. RCTs and prospective observational studies published up to December 2015 were screened independently by two independent reviewers who also extracted data and assessed studies’ risk of bias. The review identified three eligible randomized trials with a total of 1,007 participants. Results
| Reference | Country | No. of Subjects | Plan to Quit? | Study Arms | Duration of Treatment |
|---|---|---|---|---|---|
| Bullen et al., 2013 (ASCEND) | New Zealand | 657 | Yes | (1) INT:1st-generation e-cigarette (Elusion) (16 mg nicotine); (2) CTL: Placebo e-cigarette; (3) Active comparator: Nicotine patch (21 mg). |
12 weeks |
| Caponnetto et al., 2013 (ECLAT) | Italy | 300 | No | (1) INT: 1st-generation e-cigarette (Categoria) (7.2 mg nicotine); (2) INT: Same e-cigarette (7.2 mg × 6 weeks, 5.2 mg × 6 weeks); (3) CTL: Placebo e-cigarette. |
12 weeks |
| Adriaens et al., 2014 | Belgium | 50 | No | (1) INT: 2nd generation (Joyetech, 18 mg/ml nicotine); (2) INT: 2nd generation (Kanger T2, 18 mg/ml nicotine); (3) CTL: Delayed e-cigarette (offered weeks 8–16). |
8 weeks |
b Hartmann-Boyce et al., 2016.
NOTE: ASCEND = A Study of Cessation Using Electronic Nicotine Devices; CO = carbon monoxide; CTL = control; ECLAT = EffiCiency and Safety of an eLectronic CigAreTte; INT = intervention; RR = relative risk.
| Behavioral Support | Outcome Assessment | Difference | Data Pooled for Meta-Analysis?a,b | ||
|---|---|---|---|---|---|
| Follow-Up | Measure | Abstinence Rate | |||
| Offered phone or text (few used). No training in use of e-cigarette. |
6 months | CO-validated continuous abstinence | (1) INT = 7.3%; (2) CTL = 4.1%; (3) CTL = 5.8%. |
1 versus 2: 7.3% versus 4.1%, RR = 1.77, 95% CI = 0.54–5.77 n = 362. 1 versus 3: 7.3% versus 5.8%, RR = 1.26, 95% CI = 0.68–2.34, n = 584. | Yes |
| No quit assistance or training in use of e-cigarette. | 12 months | CO-validated continuous 6–12 months | (1) INT = 13%; (2) INT = 9%; (3) PCB = 4%. |
Pooling INT 1 + 2, versus CTL: 11% versus 4%, RR = 2.75, 95% CI = 0.97–7.76, n = 300. | Yes |
| (1) and (2) Training in e-cigarette use; (3) No e-cigarette training. | 2 months | CO-validated abstinence (no definition) | At 2 months: INT (1+2) = 34%; CTL = 0%. | No | |
TABLE 17-3 Selected Systematic Reviews: Part 1
| Characteristic | Hartmann-Boyce et al., 2016 (Cochrane Collaboration) | El Dib et al., 2017 (WHO commissioned) |
|---|---|---|
| Study designs included | RCTs and prospective cohort studies | RCTs and prospective cohort studies |
| Participants | Current smokers Motivated or unmotivated to quit | Current cigarette smokers Motivated or unmotivated to quit |
| Interventions | E-cigarettes | E-cigarettes (with or without nicotine) |
| Comparison conditions | Placebo e-cigarettes, other smoking cessation aid, or no cessation aid | Placebo e-cigarettes, other smoking cessation aid, or no cessation aid |
| Search strategy: databases used | Updated results of 2014 Cochrane review using Cochrane Tobacco Addiction Group Specialized Register, Cochrane Central Register of Controlled Trials, MEDLINE, EMBASE, PsycINFO | Included results of 2014 Cochrane review, searched MEDLINE, CINHAL, EMBASE, CENTRAL, PsycINFO, Web of Science, ClinicalTrials.gov, PubMed |
| Search strategy: terms used | e-cig$ OR elect$ cigar$ OR electronic nicotine OR vape OR vaper OR vapers OR vaping | MeSH subject headings: electronic nicotine, smoking-cessation, tobacco-use-disorder, tobacco-smoking, quit |
| Literature search ended | January 2016 | December 29, 2015 (updated until submission, May 2016) |
| Study selection and data extraction | Independently by two authors | Independently by three pairs of two authors |
| Risk of bias assessment | Cochrane Handbook for Systematic Reviews of Interventionsa | Modified version of Cochrane Handbook for Systematic Reviews of Interventionsb (RCTs); Ottawa-Newcastle instrument (cohort studies)c |
| Certainty of evidence assessment | GRADE methodology | GRADE methodologyd |
| Outcome measures | Cessation at longest follow-up point (6-month minimum), prefer biochemically validated outcome measure | Tobacco smoking cessation at longest follow-up (6-month minimum), prefer biochemically validated measure; or 50 percent or more reduction in cigarette use |
| Characteristic | Hartmann-Boyce et al., 2016 (Cochrane Collaboration) | El Dib et al., 2017 (WHO commissioned) |
|---|---|---|
| Measure of treatment effect | ITT analysis, calculate risk ratio at the longest follow-up | ITT analysis, calculate risk ratio at longest follow-up |
| Missing data | Missing outcome = smoker | Complete case analysis (excluded missing data); “worst case” sensitivity analysis done |
| RCTs | ||
| Identified meeting criteria | 3 (1,007 participants) | 3 (1,007 participants) |
| Pooled for meta-analysis | 2 (n = 662 subjects) | 2 (n = 481 subjects) |
| Calculation of effect size | Fixed-effect Mantel-Haenszel model | Random-effect Mantel-Haenszel model |
| Result (smoking cessation): E-cigarette versus placebo e-cigarette E-cigarette versus nicotine patch |
RR = 2.29, 95% CI = 1.05–4.96; RR = 1.26, 95% CI = 0.68–2.34; (1 study, no pooling) |
RR = 2.03, 95% CI = 0.94–4.38; RR = 1.10, 95% CI = 0.60–2.03 (1 study, no pooling) |
| Result (50% reduction or more) | Not done | RR = 0.97, 95% CI = 0.57–1.66 |
| Risk of bias in included studies | Low | Low |
| Overall quality of evidence (GRADE) | Low certainty (small number of studies) | Low certainty |
| Prospective Cohort Studies | ||
| Identified meeting criteria | 21 | 9 (13,115 participants) |
| Pooled for meta-analysis | 0 | 8 |
| Data synthesis method | Narrative review only | Random-effect Mantel-Haenszel model |
| Result (e-cigarette versus no e-cigarette) | Pooled analysis not done | OR = 0.74, 95% CI = 0.55–1.001, p = 0.051 |
| Risk of bias in studies | High (selection bias) | High (missing data, imprecision in outcomes and prognostic factors) |
| Overall quality of evidence | Low certainty | Very low certainty |
| Characteristic | Hartmann-Boyce et al., 2016 (Cochrane Collaboration) | El Dib et al., 2017 (WHO commissioned) |
|---|---|---|
| Conclusions | “There is evidence from two trials that e-cigarettes help smokers to stop smoking in the long term compared with placebo e-cigarettes. However, the small number of trials, low event rates and wide confidence intervals around the estimates mean that our confidence in the result is rated low by GRADE standards. The lack of difference between the effect of e-cigarettes compared with nicotine patches found in one trial is uncertain for similar reasons.”e | “Results from 2 RCTs suggest a possible increase in smoking cessation with ENDS in comparison with ENNDS….”f“There is very limited evidence regarding the impact of ENDS or ENNDS on tobacco smoking cessation, reduction or adverse effects: data from RCTs are of low certainty and observational studies of very low certainty … from which no credible inferences can be drawn…. This review underlines the need to conduct well-designed trials measuring biochemically validated outcomes and adverse effects.”g |
b El Dib et al., 2017. The authors (El Dib et al., 2017) cite the following reference, which has been modified: Guyatt, G. H., and J. W. Busse. n.d. Modification of Cochrane tool to assess risk of bias in randomized controlled trials. https://www.evidencepartners.com/resources/methodological-resources (accessed September 20, 2017).
c El Dib et al., 2017. The authors (El Dib et al., 2017) cite the following reference, which has been modified: Guyatt, G. H., and J. W. Busse. n.d. Modification of Ottawa-Newcastle to assess risk of bias in nonrandomized trials. https://www.evidencepartners.com/resources/methodological-resources (accessed September 20, 2017).
e Hartmann-Boyce et al., 2016, p. 2.
f El Dib et al., 2017, p. 12.
g El Dib et al., 2017, p. 1.
NOTE: GRADE = Grading of Recommendations Assessment, Development, and Evaluation; ITT = intent-to-treat; OR = odds ratio; RCT = randomized controlled trial; RR = relative risk; WHO = World Health Organization.
from two of the three RCTs were appropriate for pooled analysis (Bullen et al., 2013; Caponnetto et al., 2013). The third was excluded because the effect of e-cigarettes versus no e-cigarettes could be compared for only 8 weeks (Adriaens et al., 2014). The treatment effect was calculated using the random-effect MH test and using complete case analysis (excluding cases with missing outcome data), producing a total sample of 481 participants. The result was a non-significant increase in smoking cessation with nicotine-containing e-cigarettes compared with non-nicotine e-cigarettes (RR = 2.03; 95% CI = 0.94–4.38; p = 0.07; quit rate = 11.7 percent nicotine, 6.3 percent non-nicotine; risk difference = 64/1,000 over 6 to 12 months). Combining the data on reduction in cigarettes per day, the two RCTs found no difference between the e-cigarette group and the non-nicotine e-cigarette group (RR = 0.97; 95% CI = 0.57–1.66; p = 0.92). The individual studies were judged to have low risk of bias, but the overall body of evidence was rated as low certainty due to the small number of trials and the extent of missing data.
The review also identified nine eligible cohort studies with a total of 13,115 participants. In contrast to the RCTs, combining the results from cohort studies produced a nearly significant reduction in quit rates with use of e-cigarettes compared with no use of e-cigarettes (OR = 0.74; 95% CI = 0.55–1.001; p = 0.051). Limitations of the cohort studies noted by the authors included the fact that not all participants were using e-cigarettes to quit. Additionally, missing outcome data and an imprecise assessment of prognostic factors and outcomes were judged to have produced a risk of bias. Consequently, the evidence provided by the cohort studies was judged to be very low certainty “from which no credible inferences can be drawn” (El Dib et al., 2017, p. 1). Because of the low-quality evidence, the review made no conclusion about the effectiveness of e-cigarettes as cessation aids. Instead, it identified the need for well-designed RCTs measuring biochemically validated outcomes to answer the question. In 2016, Hartmann-Boyce and colleagues updated the Cochrane Tobacco Addiction Group’s 2014 systematic review and meta-analysis of the effectiveness of e-cigarettes for smoking cessation (Hartmann-Boyce et al., 2016; McRobbie et al., 2014). The authors identified RCTs in which current smokers (motivated or unmotivated to quit) were randomly assigned to e-cigarettes or to a control condition and followed for 6 months or longer. They also included prospective observational studies with at least 6-month followup. To assess treatment effect, authors used the most rigorous definition of tobacco abstinence available, ideally, biochemically validated abstinence. In contrast to the El Dib and colleagues (2017) review, the Hartmann-Boyce (2016) review included participants with missing outcome data as continued smokers for the pooled analysis. Standard Cochrane methods for screening studies and extracting data were used. Risk ratios and 95% CIs
were calculated using a fixed-effect MH model for each study, and pooled where appropriate. The review identified 24 completed studies (3 RCTs and 21 cohort studies) and 27 ongoing studies. It specifically excluded cross-sectional studies that collected data at only one time point due to the potential for confounding and recall bias.
The same two RCTs that were judged appropriate for pooling by the El Dib and colleagues (2017) analysis were also pooled in the Hartmann-Boyce and colleagues (2016) analysis. Both studies compared nicotine-containing e-cigarettes with non-nicotine e-cigarettes. However, because Hartmann-Boyce included participants with missing data as smokers (rather than excluding them, as El Dib did), its pooled analysis had a larger combined sample size of 662 participants. In the meta-analysis of the two studies, e-cigarettes produced a higher smoking abstinence rate compared with non-nicotine–containing e-cigarettes and one that achieved statistical significance (RR = 2.29; 95% CI = 1.05–4.96; e-cigarette 9 percent versus placebo 4 percent). The one study that compared an e-cigarette to nicotine patch found no significant difference in 6-month abstinence rates (RR = 1.26; 95% CI = 0.68–2.34; 584 participants). Individual RCTs were assessed to be at low risk of bias but the overall quality of the evidence was rated as “low” or “very low” because of imprecision due to the small number of trials. The authors concluded that evidence from two trials indicated that “ECs help smokers to stop smoking in the long term compared with placebo ECs” (Hartmann-Boyce et al., 2016, p. 2), although they also acknowledged that their confidence in the result was low by GRADE standards. Only one trial compared e-cigarettes to a proven smoking cessation aid, nicotine patches. The authors interpreted the lack of difference between the effects of e-cigarettes and nicotine patches for cessation in that trial as inconclusive.
The Hartmann-Boyce review also described the non-randomized prospective observational studies it had identified, separating them into two categories, intervention versus non-intervention. Studies in which e-cigarettes were given to participant smokers as part of the study protocol were categorized as non-randomized intervention studies. Studies that simply recorded smokers’ use of e-cigarettes at baseline and follow-up were termed “non-intervention studies.” The review did not attempt to pool data from any of the non-randomized observational studies because, it stated, “these studies are heavily confounded due to the nature of their design” (Hartmann-Boyce et al., 2016, p. 8). Specifically, the authors noted that smokers who have already succeeded in quitting with e-cigarettes would not be eligible for non-randomized observational studies, which recruit only current smokers. They argued that enrolling only “e-cigarette treatment failures” into an e-cigarette intervention study would bias the result toward a null finding.
Summary of These Two Systematic Reviews
The two systematic reviews identified a similar group of studies and generally came to similar conclusions, specifically that the body of available evidence was small and that a critical need existed for additional evidence to provide definitive answers to the questions posed. However, the reviews differed slightly in their interpretation. The Cochrane review found a statistically significant effect of nicotine e-cigarettes compared with non-nicotine e-cigarettes and interpreted this as demonstrating a positive effect of e-cigarettes on quitting, albeit with low confidence that the estimate would not change when more evidence became available. It judged that the risk of confounding from observational data was so high that it did not pool those data. Using the same two RCTs, the El Dib review produced a similar but not quite significant effect of e-cigarettes versus non-nicotine e-cigarettes. El Dib and colleagues (2017) judged the low confidence in the evidence base and the opposite result of the cohort studies to be sufficient to preclude any conclusion about effectiveness of e-cigarettes at this time.
Other Systematic Reviews
Table 17-4 describes four of the five other systematic reviews that were published during 2016–2017 (Kalkhoran and Glantz, 2016; Khoudigian et al., 2016; Malas et al., 2016; Vanderkam et al., 2016). A fifth systematic review from this period is not discussed because it was of lower quality and used non-standard methods to summarize the search results (Heydari et al., 2017). In addition, Table 17-4 includes one earlier systematic review that included an independent meta-analysis (Rahman et al., 2015).
Khoudigian and colleagues (2016) conducted a systematic review and meta-analysis of RCTs and observational studies that were published through May 2014 and compared e-cigarettes with other non-randomized trials or placebo e-cigarettes. It included smokers regardless of their intention to quit smoking. The outcome of interest for this analysis was smoking abstinence for at least 6 months after the start of e-cigarette use. The literature search and data extraction were well conducted. The review identified five eligible studies, but only two of these had cessation outcomes. These were the same two RCTs that are included and pooled in the reviews described above (El Dib et al., 2017; Hartmann-Boyce et al., 2016). Pooling of these two studies produced a non-significant RR of 2.02 (95% CI = 0.97–4.21). Despite this, the authors observed that their results “suggest that the use of nicotine e-cigarettes increased the proportion of patients who stopped smoking, although this change was not statistically significant” (Khoudigian et al., 2016, p. 265). Overall, they concluded, “limited low-quality evidence of a non-statistically significant
TABLE 17-4 Selected Systematic Reviews: Part 2
| Characteristic | Khoudigian et al., 2016 | Malas et al., 2016 |
|---|---|---|
| Study designs included | RCT and prospective cohort studies | RCTs, prospective cohort, experimental, and cross-sectional |
| Participants | Current smokers Motivated or unmotivated to quit | Current smokers Motivated or unmotivated to quit |
| Interventions | E-cigarettes (with nicotine) | E-cigarettes (with nicotine) |
| Comparison conditions | Placebo e-cigarettes or NRT | Not specified |
| Search strategy: databases used | MEDLINE, Embase, PsycINFO, Cochrane Central Registry of Controlled Trials; also found gray literature through searching websites of health technology assessment and related agencies, in addition to reports of major smoking cessation conference proceedings; also used Google for more Web-based materials | PubMed, MEDLINE, PsycINFO, CINAHL, ERIC, ROVER, Scopus, ISI Web of Science, Cochrane Library, Ontario Tobacco Research Unit library catalogue; gray literature identified using Grey Matters, OAIster, OpenGrey, NYAM website, Legacy Library, BIOSIS Previews, Conference Papers Index, ISI Proceedings, Dissertation Abstracts International, CIHI, GreyNet International |
| Search strategy: terms used |
Searched controlled vocabularies (MeSH and EMTREE) and keywords on concept of “electronic cigarette” or “e-nicotine”:
|
Electronic nicotine delivery system, ENDS, electronic cigarette, e-cigarette, e-cig, e-juice, e-liquid, e-hookah, cartomizer, alternative tobacco product, tobacco use cessation product, smoking cessation aid, vape, vaping, vaporizer, vape-pen |
| Literature search ended | May 2014 | February 1, 2016 |
| Kalkhoran et al., 2016 | Vanderkam et al., 2016 | Rahman et al., 2015 |
|---|---|---|
| RCTs, prospective cohort, and cross-sectional studies | Interventional trials (RCTs and non-RCTs), prospective cohort | RCTs, prospective cohort, and cross-sectional studies |
| Current smokers Motivated or unmotivated to quit | Current smokers, 10 cigarettes per day or more, ages 18–60, no severe comorbidity or psychiatric illness | Current smokers Motivated or unmotivated to quit |
| E-cigarettes (with nicotine) | E-cigarettes (with nicotine) | E-cigarettes (with nicotine) |
| Not using e-cigarettes | Placebo e-cigarette | Placebo e-cigarette or other |
| PubMed, Web of Science Core Collection | MEDLINE, Cochrane | PubMed, Web of Knowledge, Scopus |
| Electronic cigarette, e-cigarette, electronic nicotine delivery, 1 or 2 or 3, stop, quit, cessation, abstain, abstinence, 5 or 6 or 7 or 8 or 9, 4 and 10 | Electronic cigarette, electronic nicotine delivery device, electronic nicotine delivery system, vaping, e-cigarette | “electronic cigarettes OR e-cigarettes” AND “smoking cessation OR quit smoking” |
| June 17, 2015 | June 14, 2015 | May 2014 |
| Characteristic | Khoudigian et al., 2016 | Malas et al., 2016 |
|---|---|---|
| Study selection and data extraction | 2 authors | 2 authors |
| Risk of bias assessment | Yes Cochrane Risk of Bias tool (RCTs); same criteria for controlled before–after studies, but “random sequence generation” and “allocation concealment” domains were reported as “high risk of bias” |
Yes Modified version of QualSysta tool by combining quantitative and qualitative checklists and revising criteria based on Cochrane Handbook guidelines |
| Outcome measures | Smoking abstinence for 6 months or more; also desire to smoke, number of cigarettes smoked, withdrawal symptoms | Smoking abstinence for 30 days; also reduction, withdrawal symptoms, craving |
| Studies identified | 5 (4 RCTs [2 of which used in meta-analysis], 1 controlled before–after study) | 62 |
| Meta-analysis done | Yes (2 RCTs) | No (attempted, but data considered too heterogeneous) |
| Result (cessation): E-cigarette versus placebo e-cigarette | RR = 2.02; 95% CI = 0.97–4.21 | n/a |
| E-cigarette versus no e-cigarette | n/a | n/a |
| Kalkhoran et al., 2016 | Vanderkam et al., 2016 | Rahman et al., 2015 |
|---|---|---|
| 1 author, with review by a second author | 2 authors | 2 authors |
| Yes ACROBAT-NRSI (observational) Cochrane Risk of Bias tool (clinical trials) |
Yes Cochrane risk of bias tool |
Yes Cochrane risk of bias tool (RCTs), Downs and Black instrument (observational studies) |
| Cigarette smoking abstinence of any duration. E-cigarette use explicitly allowed | Reduction of 50% in cigarettes/day for at least 3 months (primary outcome). Smoking abstinence for 3 months or more, validated biochemically (secondary outcome). | Smoking abstinence of any duration |
| 38 (20 used in meta-analysis) | 13 (2 RCTs used in meta-analysis) | 6 (2 RCTs, 2 cohort, 2 cross-sectional) |
| Yes (20 studies: RCT, cohort, cross-sectional designs) | Yes (2 RCTs) | Yes (2 RCTs) |
| n/a | RR = 1.91; 95% CI = 0.93–3.89 | RR = 2.29; 95% CI = 1.05–4.97 |
| OR = 0.72; 95% CI = 0.57–0.91 | n/a | n/a |
| Characteristic | Khoudigian et al., 2016 | Malas et al., 2016 |
|---|---|---|
| Conclusions | “Limited low-quality evidence of a non-statistically significant trend toward smoking cessation in adults using nicotine e-cigarettes exists compared with other therapies or placebo. Larger, high-quality studies are needed to inform policy decisions.”b | “The results of this systematic review lead us to conclude that evidence for the effectiveness of e-cigarettes as a cessation aid is inconclusive. There is too much uncontrolled variation to allow for any general conclusion to be made.”c “While inconclusive due to low quality, overall the existing literature suggests e-cigarettes may be helpful for some smokers for quitting or reducing smoking. However, more carefully designed and scientifically sound studies are urgently needed to establish unequivocally the long-term cessation effects of e-cigarettes”d |
c Malas et al., 2016, p. 1931.
d Malas et al., 2016, p. 1926.
e Kalkhoran and Glantz, 2016, p. 2.
f Vanderkam et al., 2016, p. 972.
trend toward smoking cessation in adults using nicotine e-cigarettes exists compared with other therapies or placebo. Larger, high-quality studies are needed to inform policy decisions” (Khoudigian et al., 2016, p. 257). Overall, this review was carefully conducted, but did not identify studies published after May 2014.
Malas and colleagues (2016, p. 1927) conducted a systematic review of English-language studies containing “original data related to e-cigarettes and smoking cessation” that were identified from database searches through February 1, 2016, or a search of unpublished studies or abstracts (i.e., “gray literature”). Comparison conditions were not specified. Eligible study designs included RCTs, experimental studies, prospective observational studies, and cross-sectional studies. The primary outcome was cessation, defined as smoking abstinence or reduction with at least a
| Kalkhoran et al., 2016 | Vanderkam et al., 2016 | Rahman et al., 2015 |
|---|---|---|
| “As currently being used, e-cigarettes are associated with significantly less quitting among smokers.”e | “The use of electronic cigarette with nicotine decreases tobacco consumption among regular smokers. Further studies are needed to specify an electronic cigarette’s safety profile and its ability to cause a reduction in consumption and long-term cessation in smokers.”f | “Use of e-cigarettes is associated with smoking cessation and reduction. More randomized controlled trials are needed to assess effectiveness against other cessation methods.”g “Limitations: Included studies were heterogeneous, due to different study designs and gender variation.”h |
g Rahman et al., 2015, p. 2.
h Rahman et al., 2015, p. 2.
NOTE: NRT = nicotine replacement therapy; OR = odds ratio; RCT = randomized controlled trial; RR = relative risk.
30-day follow-up period. Identified studies underwent a systematic quality assessment and received a rating of weak, moderate, or strong. The review identified 11 relevant studies with moderate or strong results that enrolled smokers from the general population. The authors summarized the studies qualitatively and attempted to do a quantitative synthesis, combining all study designs, but they concluded it could not be done due to heterogeneity of outcome measures and study designs. They stated, “The results of this systematic review lead us to conclude that evidence for the effectiveness of e-cigarettes as a cessation aid is inconclusive. There is too much uncontrolled variation to allow for any general conclusion to be made” (Malas et al., 2016, p. 1931). The authors identified an urgent need for “more carefully designed and scientifically sound studies … to establish unequivocally the long-term cessation effects of e-cigarettes and
to better understand how and when e-cigarettes may be helpful” (Malas et al., 2016, p. 1926).
Kalkhoran and Glantz (2016) conducted a systematic review and meta-analysis of English-language studies that assessed the relationship between e-cigarette use and cigarette smoking cessation among adult smokers, regardless of their interest in quitting smoking. They included RCTs and non-RCTs, cohort studies, and cross-sectional studies that were identified by a search ending June 17, 2015. The authors also monitored the literature for studies published before publication of their paper in January 2016 and added two studies. Outcomes were either self-reported or biochemically confirmed combustible tobacco cigarette smoking abstinence, with no required minimum duration of abstinence required. E-cigarette use was permitted under the definition of smoking abstinence. A total of 38 eligible studies were identified. They were heterogeneous in study design, duration, and definition of the e-cigarette exposure measure and the smoking cessation outcome. Twenty studies with control groups were included in a random-effects meta-analysis that found a negative effect of e-cigarette use on cessation (OR = 0.72; 95% CI = 0.57–0.91). Unlike other meta-analyses that separated RCTs and observational studies, this meta-analysis combined all study designs (15 cohort studies, 3 cross-sectional studies, and 2 clinical trials [only 1 randomized]). Sensitivity analyses compared the results of meta-analyses stratified by several factors, including interest in quitting, study design (clinical trial versus observational, longitudinal versus cross-sectional), biochemical verification, and recent e-cigarette use. The ORs generated in the sensitivity analysis for each of the different factors were not statistically significantly different from one another. The authors concluded, “As currently being used, e-cigarettes are associated with significantly less quitting among smokers” (Kalkhoran and Glantz, 2016, p. 2). They suggest that one explanation may be that e-cigarettes are used differently in a controlled clinical trial than in the real world, where e-cigarettes are readily available consumer products without clear instructions for use. They suggest that the results of observational trials provide insight into the effect of real-world e-cigarette use on cessation.
Vanderkam and colleagues (2016) conducted a systematic review and meta-analysis of randomized and non-randomized intervention trials and prospective cohort studies that were published up to June 14, 2015. They compared nicotine-containing e-cigarettes to non-nicotine–containing e-cigarettes. The primary endpoint was 50 percent reduction of combustible tobacco cigarettes or more for at least 3 months, confirmed by a biochemical measure. However, they also included as a secondary measure of smoking cessation for at least 3 months, confirmed by biomarker. Their search identified 13 papers, of which 2 were the same 2 RCTs
identified by other reviews (El Dib et al., 2017; Hartmann-Boyce et al., 2016; Khoudigian et al., 2016). In these authors’ hands, pooling the cessation data produced a non-significant effect of e-cigarettes over placebo e-cigarettes (RR = 1.91; 95% CI = 0.93–3.89). They did find a significant increase in the proportion of smokers with a validated self-report of 50 percent or greater reduction in daily cigarette consumption (RR = 1.30; 95% CI = 1.02–1.66). The authors concluded that evidence was insufficient to determine effectiveness of e-cigarettes for quitting smoking.
The committee identified only one earlier systematic review that included a meta-analysis. Rahman and colleagues (2015) reviewed controlled trials, prospective cohort studies, and cross-sectional studies of e-cigarette use that were published up to May 2014. The review included studies that compared current smokers (variously defined and irrespective of interest in quitting) who used e-cigarettes for at least 3 months with those who used any other method. The outcome measure was smoking cessation, not necessarily biochemically validated. The search and data extraction were carefully done and risk of bias was assessed. The search identified six studies, including the same two RCTs (Bullen et al., 2013; Caponnetto et al., 2013) that were identified in other reviews. A meta-analysis of these two studies, including missing data on smokers and using a random-effects MH test, produced an identical relative risk of quitting as that reported in the Hartmann-Boyce and colleagues (2016) review (RR = 2.29; 95% CI = 1.05–4.96). However, Rahman and colleagues’ interpretation of this finding was stated more positively than that of the Hartmann-Boyce and colleagues (2016) review; they concluded that the “use of e-cigarettes is associated with smoking cessation and reduction” (Rahman et al., 2015, p. 2). However, the review did acknowledge the small size and heterogeneity of the evidence base and called for more RCTs to be done to answer the question. Additionally, reduction in rate of smoking does not ensure reduction in tobacco-related harm.
Evaluation of the Evidence from Systematic Reviews
Overall, the systematic reviews identified by the committee generally came to similar conclusions, despite some methodological differences in the conduct of the meta-analyses. Table 17-1 includes the verbatim conclusions of all the systematic reviews to illustrate this similarity. Furthermore, the same two RCTs were consistently identified by most authors and were included in a formal meta-analysis by five of the systematic reviews. Both RCTs compared nicotine-containing e-cigarettes to non-nicotine placebo e-cigarettes. The relative risks generated in the meta-analyses ranged from 1.91 to 2.29, with 95% confidence limits falling near a relative risk of 1.0 in all cases. In two reviews (Hartmann-Boyce et al., 2016; Rahman
et al., 2015), the 95% CI around the estimate excluded 1.0, indicating that the superiority of e-cigarettes over placebo e-cigarettes was statistically significant, but in three other reviews, the 95% CI included 1.0, ranging from 0.93 to 0.97, thereby missing statistical significance. Although this difference led to slightly different interpretations, all reviews agreed that their confidence in their conclusion was low and that additional evidence might shift their conclusions.
In contrast to RCTs, different groups of observational studies, primarily longitudinal cohort studies, were included in the systematic reviews. Only two systematic reviews conducted a meta-analysis of the cohort studies that they had identified (El Dib et al., 2017; Kalkhoran and Glantz, 2016). In contrast to the results of meta-analyses of RCTs, both meta-analyses of cohort studies found a negative association between e-cigarette use and cessation. Most other systematic reviews provided only a narrative summary of their observational studies. This summary identified limitations that may account for some of the discrepancy. These limitations include imprecision in measurement of e-cigarette exposure, inclusion of smokers not using e-cigarettes to quit, limited adjustment for confounding factors, and variable outcome measures of cessation (Levy et al., 2017).
In particular, observational studies included in systematic reviews consistently noted an apparent association between the measure of exposure to e-cigarettes and likelihood of smoking cessation. Several observational studies found an association between frequent (i.e., daily or at least 20 of the past 30 days) e-cigarette use and smoking cessation success (Beard et al., 2015; Biener and Hargraves, 2015; Brose et al., 2015; Hitchman et al., 2015) or quit attempts made (Brose et al., 2015), while measures of less frequent e-cigarette use were associated with less smoking cessation than non-use of e-cigarettes (Beard et al., 2016; Biener and Hargraves, 2015; Brose et al., 2015; Hitchman et al., 2015).
In summary, the existing systematic reviews consistently agreed that the available evidence base was insufficient to definitively answer the question of whether e-cigarettes helped smokers to quit. They uniformly identified the urgent need for additional studies of high scientific quality, especially RCTs.
Effect of E-Cigarettes on Population-Level Cessation Rates
The committee identified only a small number of studies that enrolled nationally representative samples of individuals to assess the effect of e-cigarette availability on population cessation rates. Available studies used prospective cohort or repeat cross-sectional study designs. No RCTs are available. Few studies are available because e-cigarettes have been
broadly available consumer products for only a few years and national surveys, from which study data were drawn, started to collect data on e-cigarette use only recently.
The most recent and largest study in the United States provides evidence of an association between e-cigarette use and smoking cessation rates at the population level. Zhu and colleagues (2017) analyzed data from five waves (i.e., repeated cross-sections) of the large, nationally representative U.S. Current Population Survey–Tobacco Use Supplement (CPS-TUS). The authors used these cross-sectional data to create a retrospective cohort of individuals who reported having been smokers one year prior to the survey. The analysis compared the quit rate (defined as the proportion who reported having been abstinent for at least 3 months at the time of the survey among those who were smoking 1 year earlier) between those who had ever used or currently used (defined as now used every day or some days) an e-cigarette. In the most recent survey of more than 160,000 respondents conducted in 2014–2015, smokers who used e-cigarettes in the previous 12 months were more likely to have made a quit attempt during that period and to have achieved at least 3 months of tobacco cessation than smokers who were not e-cigarette users.
In the same publication, Zhu and colleagues (2017) also used repeated cross-sectional CPS-TUS surveys to examine the population-level rates of making a quit attempt in the past year and of quitting smoking. Both measures increased significantly in 2014–2015 after remaining stable in four previous surveys beginning in 2001–2002. The population-level smoking cessation rate increased by 1.1 percentage points (4.5 percent to 5.6 percent) between 2010–2011 and 2014–2015. This coincided with the increase in e-cigarette use in the population, but it could also have been the result of other broad population-level influences on smoking cessation rates. The authors carefully considered concurrent factors, including an increase in federal tobacco excise tax in 2009 and annual national media campaigns beginning in 2012. They argue that these are not likely to have caused the change in quit rates. The study findings are consistent with findings of a study from England that also analyzed repeated cross-sections of nationally representative population samples (Beard et al., 2016). That study found a higher success rate of quit attempts among smokers who used e-cigarettes during a quit attempt, compared with those who did not use e-cigarettes during a quit attempt. It did not, however, find an association between e-cigarette use and the likelihood of a smoker making a quit attempt, as the Zhu and colleagues (2017) study did. It may also have been confounded by secular changes in the availability of treatment in the National Health Service (Britton, 2016).
Like Zhu and colleagues (2017), Levy and colleagues (2017) also analyzed data from the cross-sectional 2014–2015 CPS-TUS. They retrospec-
tively created a cohort of individuals who were smoking 1 year prior to the survey. Their analysis focused on the relationship between the frequency of e-cigarette use at the time of the survey and two outcomes: (1) having made a quit attempt in the past year, and (2) having been abstinent from cigarettes for at least 3 months at the time of the survey if a quit attempt was made. Using multiple logistic regression analysis, the authors found consistent evidence between the frequency of e-cigarette use and both outcomes. Having made a quit attempt in the past year was associated with having ever used or currently using e-cigarettes, and the strength of this association increased with increasing number of days of e-cigarette use in the 30 days before the survey was conducted. Furthermore, among smokers who had made a quit attempt in the past year, the likelihood of having quit for 3 months or more at the time of the survey was significantly associated with current e-cigarette use. The strength of the relationship increased in a dose–response relationship with the number of days of e-cigarette use in the past 30 days. The adjusted odds ratio (AOR) for smokers who had used e-cigarettes on 20 or more days in the past 30 days (versus no use) was 2.81 (95% CI = 2.26–3.49), compared with 1.59 (95% CI = 1.31–1.92) for 5 or more days of use and 1.22 (95% CI = 1.02–1.46) for any number of days of current use. By contrast, there was an inverse relationship between being abstinent and ever use of an e-cigarette (AOR = 0.80; 95% CI = 0.69–0.92).
Giovenco and Delnevo (2018) used a similar approach to analyze a different large nationally representative annual cross-sectional survey, the National Health Interview Survey. They pooled data from the 2014 and 2015 surveys, which were the first to collect data on e-cigarette use. They constructed a retrospective cohort by including current smokers and any former smoker who quit in 2010 or later. They chose this date because e-cigarettes were rarely used in the United States prior to that date. Among this group of current and former smokers, daily e-cigarette users at the time of the survey (2014–2015) were more likely to be former smokers than e-cigarette–never users (52 percent versus 28 percent, adjusted prevalence ratio [aPR] = 3.15; 95% CI = 2.66–3.73). By contrast, those who previously tried e-cigarettes but did not use them currently and those who used them on only some days were less likely to be former smokers at the time of the survey than those who never used e-cigarettes (aPR = 0.67 [95% CI = 0.61–0.75] and 0.38 [95% CI = 0.32–0.47], respectively).
Recall bias of e-cigarette use and quit attempts is a limitation of the Giovenco and Delnevo (2018), Levy and colleagues (2017), and Zhu and colleagues (2017) studies’ retrospective cohort design, as the authors acknowledge. They also recognize that reverse causation (i.e., quitting led to e-cigarette use to prevent relapse) also cannot be excluded. Other limitations include lack of information on potential confounders such as the
type of e-cigarette used, the reason for e-cigarette use, or factors reflecting motivation or confidence in the ability to quit or past quit attempts. For example, smokers who use e-cigarettes daily could also be the ones most motivated to quit and therefore most likely to succeed. A strength of the Giovenco and Delnevo (2018) study was its unique ability to adjust for one potential confounder, serious psychological distress, which is associated with a lower success in quit attempts. This information is rarely available from population-based surveys. Using the stronger prospective longitudinal cohort design that avoids recall bias and reverse causation, Zhuang and colleagues (2016) conducted a U.S. population-based study of 2,028 smokers who were interviewed in 2012 and followed for 2 years. Smokers who reported using e-cigarettes at both points were defined as long-term users, while smokers reporting use at only one time were defined as short-term users. Long-term e-cigarette users had a higher cessation rate at 2 years compared with short-term e-cigarette users or non-users (42.4 percent versus 14.2 percent versus 15.6 percent). The difference in cessation rates between long-term users and either short-term or non-users was statistically significant after multivariable adjustment, suggesting that long-term but not short-term e-cigarette use promotes smoking cessation.
Shi and colleagues (2016) also conducted a prospective longitudinal population-based study to examine the relationship between e-cigarette use and smoking cessation, but found a different result. A nationally representative cohort of 2,454 smokers responding to the 2010 CPS-TUS was contacted 1 year later. The analysis found a negative association between ever use of e-cigarettes and quitting smoking for at least 1 month at followup. However, the measure of e-cigarette use was limited to ever use. No more detail about the intensity or duration of use, which the Zhuang and colleagues (2016) study suggests may be important factors, was available. Furthermore, the authors point out that only first-generation e-cigarettes were available to U.S. smokers at the time of the study. These may have been less effective for cessation because they delivered less nicotine to the user than do later-generation devices.
SYNTHESIS
There is general agreement that the number, size, and quality of studies for judging the effectiveness of e-cigarettes as cessation aids in comparison with cessation aids of proven efficacy are limited, and therefore there is insufficient evidence to permit a definitive conclusion at this time. Not only are existing studies limited in number, but the randomized trials provide a limited range of treatment comparisons. Interpretation of relevant observational studies on the topic of the effectiveness of
e-cigarettes as cessation aids is complicated by the fact that they generally do not account for important covariates that may affect the success of e-cigarettes as cessation aids. These covariates include (1) the e-cigarette product (e.g., type of device, nicotine content and delivery, flavorings or other contents of the e-liquid), (2) pattern of current use (e.g., frequency of use, duration of use), and (3) user characteristics (particularly interest in quitting and prior history of e-cigarette use, but also demographics and smoking history) (Malas et al., 2016). By contrast, some of the more recently published (e.g., since 2016) cohort studies and nationally representative cross-sectional studies have included one key variable, the frequency of e-cigarette use. Based on this rationale, as described below, the evidence from more recent cohort studies and cross-sectional studies provides the foundation for the committee’s conclusion about the frequency of e-cigarette use in relation to likelihood of smoking cessation. Future studies, both observational and experimental, will be strengthened by carefully measuring characteristics of the e-cigarette product, the pattern of use, and characteristics of the users.
Within the current body of evidence, different study designs have produced conflicting findings. The results of the few RCTs, the study design with the least risk of bias and greatest internal validity, suggest a possible though not definitively positive association with quitting smoking (Adriaens et al., 2014; Bullen et al., 2013; Caponnetto et al., 2013) (see Table 17-2). In these trials, the strongest results were observed in the trials that compared the efficacy of a nicotine-containing e-cigarette with a non-nicotine placebo e-cigarette. Two RCTs addressed this narrow question about the marginal benefit of having nicotine in a vaping device. Both trials compared a nicotine-containing e-cigarette with an e-cigarette without nicotine (Bullen et al., 2013; Caponnetto et al., 2013). They found consistent results that were statistically significant in one of two meta-analyses that pooled data from the two trials (El Dib et al., 2017; Hartmann-Boyce et al., 2016). There are no opposing findings from RCTs. The committee also considered the substantial body of RCT evidence demonstrating the efficacy of nicotine replacement products compared with placebo products as smoking cessation aids as evidence that provided plausibility for the role of nicotine in enhancing the likelihood of smoking cessation. The combination of RCT evidence and indirect supportive evidence was judged by the committee to provide moderate evidence that e-cigarettes with nicotine are more effective than e-cigarettes without nicotine for smoking cessation.
While scientifically valuable, this evidence does not address a question that is more relevant to public health: how do e-cigarettes with or without nicotine compare to proven FDA-approved cessation aids or to no specific treatment among smokers who are trying to quit? Only one
trial has compared an e-cigarette to a nicotine patch (Bullen et al., 2013). No statistically significant difference in quit rates was observed in that trial, and the absolute quit rates were low in all groups. Without replication, this trial by itself provides insufficient evidence at present to support a conclusion of the relative effectiveness of e-cigarettes versus other cessation aids among smokers who are motivated to quit. This is a question of critical public health importance that deserves priority for federal funding agencies. A separate key question for public health impact is whether the availability of e-cigarettes induces more smokers to try to quit, because smokers perceive e-cigarettes to be a more appealing option than FDA-approved cessation aids.
An important note is that characteristics of the study design of the few published RCTs may have minimized the potential effectiveness of e-cigarettes as cessation aids. First, participants in two of three trials were not limited to smokers who wanted to quit smoking. One trial specifically recruited smokers not intending to quit (Caponnetto et al., 2013). An e-cigarette may be more effective in helping smokers who are motivated to quit, although this is a hypothesis that requires testing. Second, the existing RCTs used early e-cigarette models with low nicotine content and poor battery life that likely produced insufficient nicotine delivery. Newer-generation e-cigarettes, which deliver higher doses of nicotine to the user, may be more effective than first-generation devices, which are the ones that have largely been studied in clinical trials. Studies with newer e-cigarettes might produce larger effects, although this remains to be demonstrated. Third, the amount of behavioral support (including instruction in proper use of the product) may affect the effectiveness of e-cigarettes, but existing trials have offered low levels of behavioral support, which might have increased cessation rates of both e-cigarettes and other methods tested (Malas et al., 2016).
RCTs are superior to observational studies with respect to internal validity, but a strength of observational studies is that they reflect the effectiveness of e-cigarettes as they are being used in real-world settings, rather than how a specific device would perform under controlled or optimal conditions. Observational studies reflect how e-cigarettes are actually being used in the population, where they are consumer products sold without specific instructions to aid cessation. The evidence from observational studies is discrepant between studies published through 2015 and those published subsequently. The results of cohort studies have produced mixed results, but the associations in cohort studies published prior to 2016 generally indicate that e-cigarette users are less likely than non-users of combustible tobacco cigarettes to quit smoking. The two systematic reviews that included cohort studies published between 2013 and 2015 in meta-analyses each found a negative association between e-cigarette use
and cessation, with ORs of 0.74 and 0.72, respectively (El Dib et al., 2017; Kalkhoran and Glantz, 2016). In one case (El Dib et al., 2017), the result was not statistically significant. The disparate results of data from RCTs and cohort studies published prior to 2016 are striking and contribute to the uncertainty about the overall effect of e-cigarettes on cessation.
One potential explanation for the discrepancy is a difference between observational studies and RCTs in the measurement of e-cigarette use. As described above, the measurement of e-cigarette exposure in most of the cohort studies is relatively blunt. It is often a dichotomous measure such as “ever use” versus “never use” that cannot account for individual differences in the intensity or frequency of use or in the type of device used. The exposure measured in these earlier cohort studies is likely to have been less frequent or intensive that those in the RCTs. Another important reason for the discrepancy is bias in cohort studies due to self-selection. This would occur if the smokers who choose to use e-cigarettes are less likely to succeed because of stronger nicotine dependence, less access to or interest in using effective smoking cessation medications, having failed to quit after having exhausted all other smoking cessation aids, or other factors that could bias relative risk estimates of associations with e-cigarette use toward less favorable cessation outcomes. Furthermore, the motivation for e-cigarette use (e.g., to quit smoking or to be a dual user) was usually not measured in the older cohort studies. While a number of cohort studies used multivariable analysis to attempt to adjust for these factors, unmeasured confounding is always a threat to internal validity in observational studies. Notably, an analogous discrepancy exists between the results of RCTs and cohort studies regarding the effectiveness of nicotine replacement products, but because these products were consistently shown to be efficacious in numerous RCTs the efficacy of these products is well established (Fiore et al., 2008; Stead et al., 2012; USPSTF, 2015).
Observational data may largely reflect dual or intermittent use of e-cigarettes. This pattern may not contribute to cessation success any more than does poor adherence to FDA-approved cessation medications. Most cohort and cross-sectional studies published through 2015 have not characterized patterns of use sufficiently to allow stratified analysis by this or similar factors. Further complicating the interpretation of observational studies is the fact that real-world use of e-cigarettes changed during the period of time when the studies were conducted because e-cigarette have been evolving as consumer products. The committee thus gave greater weight to more recently published data from both prospective cohort and cross-sectional studies that measured frequency of e-cigarette use. With respect to prospective cohort studies, a population-based prospective longitudinal study found persistent e-cigarette use to be associated with cessation while short-term use was not (Zhuang et al., 2016). Other prospec-
tive longitudinal studies report that daily or very frequent e-cigarette use may be associated with cessation while intermittent use may not (Biener and Hargraves, 2015; Brose et al., 2015; Delnevo et al., 2016; Hitchman et al., 2015; Levy et al., 2017; Malas et al., 2016). Furthermore, several recent cross-sectional studies using nationally representative population-based samples of adults measured exposure frequency in even finer detail (e.g., number of days of use in a defined time period). Four of five studies analyzing U.S. population samples found an association between more frequent e-cigarette use and smoking cessation. The importance of the measurement limitations in the older studies is highlighted by the fact that even within these U.S. cross-sectional studies, when the measures of “ever use” or “intermittent use” of e-cigarettes were considered, several of the studies showed an inverse relationship between these measures of e-cigarette use and cessation.
The committee judged the results from more recent observational studies to be biologically plausible, as these findings are conceptually consistent with the large body of evidence that smokers trying to quit benefit from adequate nicotine replacement to reduce nicotine withdrawal symptoms. More frequent use of an e-cigarette (or a licensed short-acting nicotine replacement product) should deliver more nicotine. Furthermore, substantial evidence exists to associate higher cessation rates with better adherence to FDA-approved cessation aids among smokers who are attempting to quit.
Based on this biological plausibility and the strong, consistent body of evidence from higher-quality studies published more recently that overcome measurement limitations of studies published in the past, the committee concluded that there was moderate evidence that more frequent use of e-cigarettes is associated with quitting smoking. Observational studies are inherently limited for causal inferences due to the potential for selection bias and unmeasured confounding. The committee gave greater weight to the evidence from RCTs but acknowledged the overall evidence from observational studies in describing the strength of its overall conclusion on the effectiveness of e-cigarettes as a cessation aid. In combination with the limited evidence from RCTs, this body of observational evidence also contributed to the committee’s judgment that the total body of evidence that e-cigarettes may be an effective smoking cessation aid was limited.
Future cohort studies will be most useful if they measure more detailed information about e-cigarette use. Factors likely to be important include the type of e-cigarette product (first-generation versus second- and later-generation devices), the frequency of use (daily/regularly or not), the method of use (complete switch to e-cigarettes versus dual use), and the goal of use (to quit smoking versus primarily to reduce number of
combustible tobacco cigarettes smoked or otherwise reduce harm without quitting). For both randomized trials and observational studies, critical modifiers of the association of e-cigarette use and smoking cessation may exist, such that certain patterns of use or types of e-cigarettes may be more effective as cessation aids than others.
CONCLUSIONS
Conclusion 17-1. Overall, there is limited evidence that e-cigarettes may be effective aids to promote smoking cessation.
Conclusion 17-2. There is moderate evidence from randomized controlled trials that e-cigarettes with nicotine are more effective than e-cigarettes without nicotine for smoking cessation.
Conclusion 17-3. There is insufficient evidence from randomized controlled trials about the effectiveness of e-cigarettes as cessation aids compared with no treatment or to Food and Drug Administration–approved smoking cessation treatments.
Conclusion 17-4. While the overall evidence from observational trials is mixed, there is moderate evidence from observational studies that more frequent use of e-cigarettes is associated with an increased likelihood of cessation.
REFERENCES
Adriaens, K., D. Van Gucht, P. Declerck, and F. Baeyens. 2014. Effectiveness of the electronic cigarette: An eight-week Flemish study with six-month follow-up on smoking reduction, craving and experienced benefits and complaints. International Journal of Environmental Research & Public Health 11(11):11220–11248.
Beard, E., J. Brown, A. McNeill, S. Michie, and R. West. 2015. Has growth in electronic cigarette use by smokers been responsible for the decline in use of licensed nicotine products? Findings from repeated cross-sectional surveys. Thorax 70(10):974–978.
Beard, E., R. West, S. Michie, and J. Brown. 2016. Association between electronic cigarette use and changes in quit attempts, success of quit attempts, use of smoking cessation pharmacotherapy, and use of stop smoking services in England: Time series analysis of population trends. BMJ 354:i4645. https://doi.org/10.1136/bmj.i4645 (accessed February 9, 2018.
Biener, L., and J. L. Hargraves. 2015. A longitudinal study of electronic cigarette use among a population-based sample of adult smokers: Association with smoking cessation and motivation to quit. Nicotine & Tobacco Research 17(2):127–133.
Britton, J. 2016. Electronic cigarettes and smoking cessation in England. BMJ 354:i4819. https://doi.org/10.1136/bmj.i4819 (accessed February 9, 2018).
Brose, L. S., S. C. Hitchman, J. Brown, R. West, and A. McNeill. 2015. Is the use of electronic cigarettes while smoking associated with smoking cessation attempts, cessation and reduced cigarette consumption? A survey with a 1-year follow-up. Addiction 110(7):1160–1168.
Bullen, C., C. Howe, M. Laugesen, H. McRobbie, V. Parag, J. Williman, and N. Walker. 2013. Electronic cigarettes for smoking cessation: A randomised controlled trial. Lancet 382(9905):1629–1637.
Caponnetto, P., D. Campagna, F. Cibella, J. B. Morjaria, M. Caruso, C. Russo, and R. Polosa. 2013. Efficiency and safety of an electronic cigarette (ECLAT) as tobacco cigarettes substitute: A prospective 12-month randomized control design study. PLoS ONE 8(6):e66317. https://doi.org/10.1371/journal.pone.0066317 (accessed February 9, 2018).
Delnevo, C. D., D. P. Giovenco, M. B. Steinberg, A. C. Villanti, J. L. Pearson, R. S. Niaura, and D. B. Abrams. 2016. Patterns of electronic cigarette use among adults in the United States. Nicotine & Tobacco Research 18(5):715–719.
El Dib, R., E. A. Suzumura, E. A. Akl, H. Gomaa, A. Agarwal, Y. Chang, M. Prasad, V. Ashoorion, D. Heels-Ansdell, W. Maziak, and G. Guyatt. 2017. Electronic nicotine delivery systems and/or electronic non-nicotine delivery systems for tobacco smoking cessation or reduction: A systematic review and meta-analysis. BMJ Open 7(2):e012680. https://doi.org/10.1136/bmjopen-2016-012680 (accessed February 9, 2018).
Fiore, M. C., C. R. Jaen, and T. B. Baker. 2008. Clinical practice guideline: Treating tobacco use and dependence: 2008 update. Rockville, MD: U.S. Department of Health and Human Services, Public Health Service.
Franck, C., T. Budlovsky, S. B. Windle, K. B. Filion, and M. J. Eisenberg. 2014. Electronic cigarettes in North America: History, use, and implications for smoking cessation. Circulation 129(19):1945–1952.
Giovenco, D. P., and C. D. Delnevo. 2018. Prevalence of population smoking cessation by electronic cigarette use status in a national sample of recent smokers. Addictive Behaviors 76:129–134.
Guyatt, G. H., A. D. Oxman, R. Kunz, J. Brozek, P. Alonso-Coello, D. Rind, P. J. Devereaux, V. M. Montori, B. Freyschuss, G. Vist, R. Jaeschke, J. W. Williams, Jr., M. H. Murad, D. Sinclair, Y. Falck-Ytter, J. Meerpohl, C. Whittington, K. Thorlund, J. Andrews, and H. J. Schunemann. 2011a. GRADE guidelines 6. Rating the quality of evidence—Imprecision. Journal of Clinical Epidemiology 64(12):1283–1293.
Guyatt, G. H., A. D. Oxman, R. Kunz, J. Woodcock, J. Brozek, M. Helfand, P. Alonso-Coello, Y. Falck-Ytter, R. Jaeschke, G. Vist, E. A. Akl, P. N. Post, S. Norris, J. Meerpohl, V. K. Shukla, M. Nasser, H. J. Schunemann, and GRADE Working Group. 2011b. GRADE guidelines: 8. Rating the quality of evidence—Indirectness. Journal of Clinical Epidemiology 64(12):1303–1310.
Guyatt, G. H., A. D. Oxman, R. Kunz, J. Woodcock, J. Brozek, M. Helfand, P. Alonso-Coello, P. Glasziou, R. Jaeschke, E. A. Akl, S. Norris, G. Vist, P. Dahm, V. K. Shukla, J. Higgins, Y. Falck-Ytter, H. J. Schunemann, and GRADE Working Group. 2011c. GRADE guidelines: 7. Rating the quality of evidence—Inconsistency. Journal of Clinical Epidemiology 64(12):1294–1302.
Guyatt, G. H., A. D. Oxman, V. Montori, G. Vist, R. Kunz, J. Brozek, P. Alonso-Coello, B. Djulbegovic, D. Atkins, Y. Falck-Ytter, J. W. Williams, Jr., J. Meerpohl, S. L. Norris, E. A. Akl, and H. J. Schunemann. 2011d. GRADE guidelines: 5. Rating the quality of evidence—Publication bias. Journal of Clinical Epidemiology 64(12):1277–1282.
Guyatt, G. H., A. D. Oxman, G. Vist, R. Kunz, J. Brozek, P. Alonso-Coello, V. Montori, E. A. Akl, B. Djulbegovic, Y. Falck-Ytter, S. L. Norris, J. W. Williams, Jr., D. Atkins, J. Meerpohl, and H. J. Schunemann. 2011e. GRADE guidelines: 4. Rating the quality of evidence—Study limitations (risk of bias). Journal of Clinical Epidemiology 64(4):407–415.
Hajek, P., J. F. Etter, N. Benowitz, T. Eissenberg, and H. McRobbie. 2014. Electronic cigarettes: Review of use, content, safety, effects on smokers and potential for harm and benefit. Addiction 109(11):1801–1810.
Harrell, P. T., V. N. Simmons, J. B. Correa, T. A. Padhya, and T. H. Brandon. 2014. Electronic nicotine delivery systems (“e-cigarettes”): Review of safety and smoking cessation efficacy. Otolaryngology—Head and Neck Surgery (United States) 151(3):381–393.
Hartmann-Boyce, J., H. McRobbie, C. Bullen, R. Begh, L. F. Stead, and P. Hajek. 2016. Electronic cigarettes for smoking cessation. Cochrane Database of Systematic Reviews 9:CD010216.
Heydari, G., M. Masjedi, A. E. Ahmady, S. J. Leischow, H. A. Lando, M. B. Shadmehr, and L. Fadaizadeh. 2014. A comparative study on tobacco cessation methods: A quantitative systematic review. International Journal of Preventive Medicine 5(6):673–678.
Heydari, G., A. E. Ahmady, F. Chamyani, M. Masjedi, and L. Fadaizadeh. 2017. Electronic cigarette, effective or harmful for quitting smoking and respiratory health: A quantitative review papers. Lung India 34(1):25–28.
HHS (U.S. Department of Health and Human Services). 2014. The health consequences of smoking—50 years of progress: A report of the Surgeon General. Atlanta, GA: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Disease Prevention and Health Promotion, Office on Smoking and Health.
Higgins, J. P., D. G. Altman, P. C. Gotzsche, P. Juni, D. Moher, A. D. Oxman, J. Savovic, K. F. Schulz, L. Weeks, J. A. Sterne, Cochrane Bias Methods Group, and Cochrane Statistical Methods Group. 2011. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 343:d5928. https://doi.org/10.1136/bmj.d5928 (accessed February 9, 2018).
Hitchman, S. C., L. S. Brose, J. Brown, D. Robson, and A. McNeill. 2015. Associations between e-cigarette type, frequency of use, and quitting smoking: Findings from a longitudinal online panel survey in Great Britain. Nicotine & Tobacco Research 17(10):1187–1194.
Ioakeimidis, N., C. Vlachopoulos, and D. Tousoulis. 2016. Efficacy and safety of electronic cigarettes for smoking cessation: A critical approach. Hellenic Journal of Cardiology 57(January–February):1–6.
Jha, P., and R. Peto. 2014. Global effects of smoking, of quitting, and of taxing tobacco. New England Journal of Medicine 370(1):60–68.
Kalkhoran, S., and S. A. Glantz. 2016. E-cigarettes and smoking cessation in real-world and clinical settings: A systematic review and meta-analysis. The Lancet Respiratory Medicine 4(2):116–128.
Kasza, K. A., B. K. Ambrose, K. P. Conway, N. Borek, K. Taylor, M. L. Goniewicz, K. M. Cummings, E. Sharma, J. L. Pearson, V. R. Green, A. R. Kaufman, M. Bansal-Travers, M. J. Travers, J. Kwan, C. Tworek, Y. C. Cheng, L. Yang, N. Pharris-Ciurej, D. M. van Bemmel, C. L. Backinger, W. M. Compton, and A. J. Hyland. 2017. Tobacco-product use by adults and youths in the United States in 2013 and 2014. New England Journal of Medicine 376(4):342–353.
Khoudigian, S., T. Devji, L. Lytvyn, K. Campbell, R. Hopkins, and D. O’Reilly. 2016. The efficacy and short-term effects of electronic cigarettes as a method for smoking cessation: A systematic review and a meta-analysis. International Journal of Public Health 61(2):257–267.
Kmet, L. M., R. C. Lee, and L. S. Cook. 2004. HTA Initiative #13: Standard quality assessment criteria for evaluating primary research papers from a variety of fields. Edmonton, Alberta: Alberta Heritage Foundation for Medical Research.
Knight-West, O., and C. Bullen. 2016. E-cigarettes for the management of nicotine addiction. Substance Abuse and Rehabilitation 7:111–118.
Lam, C., and A. West. 2015. Are electronic nicotine delivery systems an effective smoking cessation tool? Canadian Journal of Respiratory Therapy 51(4):93–98.
Levy, D. T., Z. Yuan, Y. Luo, and D. B. Abrams. 2017. The relationship of e-cigarette use to cigarette quit attempts and cessation: Insights from a large, nationally representative U.S. survey. Nicotine & Tobacco Research. https://doi.org/10.1093/ntr/ntx166 (accessed February 9, 2018).
MacDonald, M., R. O’Leary, T. Stockwell, and D. Reist. 2016. Clearing the air: Protocol for a systematic meta-narrative review on the harms and benefits of e-cigarettes and vapour devices. Systematic Reviews 5(1):85. https://doi.org/10.1186/s13643-016-0264-y (accessed February 9, 2018).
Malas, M., J. van der Tempel, R. Schwartz, A. Minichiello, C. Lightfoot, A. Noormohamed, J. Andrews, L. Zawertailo, and R. Ferrence. 2016. Electronic cigarettes for smoking cessation: A systematic review. Nicotine & Tobacco Research 18(10):1926–1936.
McRobbie, H., C. Bullen, J. Hartmann-Boyce, and P. Hajek. 2014. Electronic cigarettes for smoking cessation and reduction. Cochrane Database of Systematic Reviews 12:CD010216.
NASEM (National Academies of Sciences, Engineering, and Medicine). 2017. The health effects of cannabis and cannabinoids: The current state of evidence and recommendations for research. Washington, DC: The National Academies Press.
Orr, K. K., and N. J. Asal. 2014. Efficacy of electronic cigarettes for smoking cessation. Annals of Pharmacotherapy 48(11):1502–1506.
Patnode, C. D., J. T. Henderson, J. H. Thompson, C. A. Senger, S. P. Fortmann, and E. P. Whitlock. 2015. Behavioral counseling and pharmacotherapy interventions for tobacco cessation in adults, including pregnant women: A review of reviews for the U.S. Preventive Services Task Force. Annals of Internal Medicine 163(8):608–621.
Rahman, M. A., N. Hann, A. Wilson, and L. Worrall-Carter. 2014. Electronic cigarettes: Patterns of use, health effects, use in smoking cessation and regulatory issues. Tobacco Induced Diseases 12(1):21. https://doi.org/10.1186/1617-9625-12-21 (accessed February 9, 2018).
Rahman, M. A., N. Hann, A. Wilson, G. Mnatzaganian, and L. Worrall-Carter. 2015. E-cigarettes and smoking cessation: Evidence from a systematic review and meta-analysis. PLoS ONE 10(3):e0122544. https://doi.org/10.1371/journal.pone.0122544 (accessed February 7, 2018).
Shi, Y. Y., J. P. Pierce, M. White, M. Vijayaraghavan, W. Compton, K. Conway, A. M. Hartman, and K. Messer. 2016. E-cigarette use and smoking reduction or cessation in the 2010/2011 TUS-CPS longitudinal cohort. BMC Public Health 16:1105. https://doi.org/10.1186/s12889-016-3770-x (accessed February 9, 2018).
Stead, L. F., R. Perera, C. Bullen, D. Mant, J. Hartmann-Boyce, K. Cahill, and T. Lancaster. 2012. Nicotine replacement therapy for smoking cessation. Cochrane Database Systematic Reviews 11:CD000146.
USPSTF (U.S. Preventive Services Task Force). 2015. Behavioral and pharmacotherapy interventions for tobacco smoking cessation in adults, including pregnant women: U.S. Preventive Services Task Force recommendation statement. Annals of Internal Medicine 163(8):622–634.
Vanderkam, P., R. Boussageon, M. Underner, N. Langbourg, Y. Brabant, P. Binder, B. Freche, and N. Jaafari. 2016. Efficacy and security of electronic cigarette for tobacco harm reduction: Systematic review and meta-analysis. Presse Medicale 45(11):971–985.
Waghel, R. C., D. M. Battise, and M. L. Ducker. 2015. Effectiveness of electronic cigarettes as a tool for smoking cessation or reduction. Journal of Pharmacy Technology 31(1):8–12.
Zhu, S. H., Y. L. Zhuang, S. Wong, S. E. Cummins, and G. J. Tedeschi. 2017. E-cigarette use and associated changes in population smoking cessation: Evidence from U.S. current population surveys. BMJ 358:j3262. https://doi.org/10.1136/bmj.j3262 (accessed February 7, 2018).
Zhuang, Y. L., S. E. Cummins, J. Y. Sun, and S. H. Zhu. 2016. Long-term e-cigarette use and smoking cessation: A longitudinal study with U.S. population. Tobacco Control 25:i90–i95. http://dx.doi.org/10.1136/tobaccocontrol-2016-053096 (accessed February 7, 2018).
















































