
2
Conceptualizing Childhood Disability
Chapter 1 (see Box 1-2) presents the committee’s adopted working definition of childhood disability—“an environmentally contextualized health-related limitation in a child’s existing or emerging capacity to perform developmentally appropriate activities and participate, as desired, in society” (Halfon et al., 2012). Thus, the committee examined childhood disability from a biopsychosocial perspective in which disability results from the interaction of an individual’s health conditions with personal and environmental factors that result in limitations in activities and participation. However, it is important to acknowledge that there is no universally accepted definition of childhood disability. Clinicians, researchers, agencies, service providers, and people with disabilities may use different conceptual frameworks to understand disability and have different definitions of disability for program inclusion, classification, and monitoring purposes.
This chapter begins by reviewing operational definitions of disability and related concepts. The second section explores the contemporary conceptual understanding of childhood disability. This section includes a discussion of a point seminal to this study: the need for a life course perspective on childhood disability and the importance of social–environmental factors in understanding and addressing the needs of children with disabilities. The discussion reflects the fact that human development, socialization, and adaptation are lifelong processes of both continuity and change throughout the life span. This section also describes the committee’s approach to conceptualizing how personal characteristics, environmental factors, and the collective set of programs and services may impact near- and long-term outcomes for children with disabilities. The third section presents three
case studies that collectively portray the complex and changing nature of disability and the variety of supports required to provide care for children with disabilities and their families as their needs evolve. Throughout the remaining chapters, it is important to note that the meaning of “family” can be highly variable and fluid in the context of children with disabilities. Accordingly, services and programs that support families of children with disabilities need to recognize the unique needs that may be associated with nontraditional family units and caregivers, such as grandparents, foster parents, and other nontraditional caregivers. The final section of the chapter presents a summary.
OPERATIONAL DEFINITIONS OF DISABILITY AND RELATED CONCEPTS
The U.S. government has a long history of providing protections for persons with disabilities, including children, and creating programs that specifically address the increased needs of persons with disabilities. However, such initiatives have often operationally defined disability in varying ways in accordance with their legislative purposes, rendering access to and eligibility for services different across federal agencies. Therefore, the precise number of U.S. children who have a disability is exceedingly difficult to enumerate because of the inconsistent definitions of what constitutes a disability used by various national data collection sources.
General federal definitions of disability range from broad to very narrow. On the broad end of the spectrum, the Americans with Disabilities Act (ADA) defines disability as “a physical or mental impairment that substantially limits one or more major life activities of such individual; a record of such impairment; or being regarded as having such impairment.”1 Similarly, the Centers for Disease Control and Prevention (CDC) defines disability as “any condition of the body or mind (impairment) that makes it more difficult for the person with the condition to do certain activities (activity limitation) and interact with the world around them (participation restrictions)” (CDC, 2017b). Although both definitions require the existence of an impairment that limits activities and/or participation, they do not delineate any specific impairments or activities or the extent to which impairments impact activities and participation. Alternatively, the Social Security Administration (SSA) very narrowly defines adult disability as “the inability to engage in any substantial gainful activity (SGA) by reason of any medically determinable physical or mental impairment(s) which can be expected to result in death or which has lasted or can be expected to last
___________________
1 Americans With Disabilities Act of 1990, Public Law 101-336, § 12102, 104 Stat. 328 (1990).
for a continuous period of not less than 12 months” (SSA, 2017a). Specific impairments for which a person may qualify for Social Security Disability Income (SSDI) are delineated in the Social Security Listing of Impairments, and program eligibility is further contingent on the impairment being so severe as to prevent engagement in any work in the national economy. Federal programs have also defined disability as it specifically relates to children, as described herein.
Supplemental Security Income
SSA also administers the Supplemental Security Income (SSI) program, the creation of which was intended as an economic security measure of last resort for low-income people who have disabilities. Accordingly, SSI has a legislative mandate to focus on low-income individuals with disabilities, including children. For the purposes of this program, SSA (2016) defines childhood disability as “a medically determinable physical or mental impairment, which results in marked and severe functional limitations, and which can be expected to result in death or which has lasted or can be expected to last for a continuous period of not less than 12 months.”2 The childhood disability definition focuses on the resultant “marked and severe functional limitations,” allowing a child to be found to have a disability even when his or her impairments do not meet or medically equal a listing. In other words, the impairment may functionally equal the listings if it results in an “extreme” limitation in one domain of functioning or “marked” limitations in two domains. The six domains of functioning considered are “(1) acquiring and using information, (2) attending and completing tasks, (3) interacting and relating with others, (4) moving about and manipulating objects, (5) caring for oneself, and (6) health and physical well-being.”3 SSA uses a focused definition of disability because the program is not intended, nor does it have the financing, to serve all children with disabilities—only those with the most severe disabilities whose family income is such that the cost of providing care would otherwise be out of reach. In December 2016, SSI provided income support to approximately 1.04 million children aged 6–17 with disabilities (2.0 percent of the total U.S. population in this age group5). The pool of potentially eligible children is much greater than the number actually receiving SSI benefits (NASEM, 2015, 2016b).
___________________
2 SSA POMS DI 11055.005.
3 20 C.F.R. § 416.926a.
4 See https://www.ssa.gov/policy/docs/statcomps/ssi_asr/2016/sect04.html#table20 (accessed April 8, 2018).
5 Based on a population estimate of 49.7 million children aged 6–17; see https://www.childstats.gov/americaschildren/tables/pop1.asp (accessed April 8, 2018).
Table 2-1 shows the most common allowances under the SSI program by diagnostic group and age in December 2016. These data do not capture comorbidities, so they do not paint the full picture of disability for children who receive SSI. And as noted in the 2015 National Academies report referenced earlier (NASEM, 2015), many children receiving SSI do in fact have comorbidities that are not reflected in the data shown in Table 2-1.
In many, but not all, states, SSI eligibility automatically guarantees Medicaid eligibility. Accordingly, Medicaid maintains its own population statistics through the Medicaid Analytics eXtract Study (MAX). The study population included all Medicaid-eligible youth aged 3–17 years from a
TABLE 2-1 SSI Recipients, by Diagnostic Group and Age, December 2016
| Diagnostic Group | Ages 3–5 (%) |
Ages 6–12 (%) |
Ages 13–17 (%) |
|---|---|---|---|
|
Congenital anomalies |
9.5 | 4.7 | 3.1 |
|
Endocrine, nutritional, and metabolic diseases |
1.3 | 0.8 | 0.6 |
|
Infectious and parasitic diseases |
(L) | 0.1 | 0.1 |
|
Injuries |
0.6 | 0.5 | 0.4 |
|
Mental disorders |
|||
|
Autistic disorders |
18.1 | 17.2 | 11.6 |
|
Developmental disorders |
29.3 | 22.4 | 16.3 |
|
Childhood and adolescent disorders not elsewhere classified |
2.6 | 21.0 | 25.8 |
|
Intellectual disability |
3.0 | 8.4 | 15.2 |
|
Mood disorders |
0.2 | 2.0 | 6.2 |
|
Organic mental disorders |
2.9 | 2.3 | 2.1 |
|
Schizophrenic and other psychotic disorders |
(L) | 0.1 | 0.5 |
|
Other mental disorders |
1.6 | 0.9 | 0.7 |
|
Neoplasms |
1.6 | 0.9 | 0.7 |
|
Diseases of the |
|||
|
Blood and blood-forming organs |
1.1 | 1.0 | 0.9 |
|
Circulatory system |
0.6 | 0.3 | 0.3 |
|
Digestive system |
3.2 | 0.7 | 0.4 |
|
Genitourinary system |
0.3 | 0.2 | 0.2 |
|
Musculoskeletal system and connective tissue |
1.1 | 0.7 | 0.7 |
|
Nervous system and sense organs |
10.3 | 8.2 | 6.8 |
|
Respiratory system |
3.2 | 2.0 | 1.6 |
|
Skin and subcutaneous tissue |
0.3 | 0.2 | 0.1 |
|
Other |
9.1 | 2.9 | 2.4 |
|
Unknown |
1.3 | 1.1 | 1.0 |
NOTES: All numbers are reported as percentages; (L) = less than 0.05 percent.
SOURCE: SSA, 2017b.
TABLE 2-2 Diagnoses by Age, SSI/Disability Enrollees Within Medicaid Claims Data, 2010
| Diagnosis | Ages 3–5 (%) |
Ages 6–11 (%) |
Ages 12–17 (%) |
|---|---|---|---|
|
Attention-deficit hyperactivity disorder (ADHD) |
6.5 | 21.9 | 17.6 |
|
Conduct disorder |
3.0 | 4.4 | 5.3 |
|
Emotional disturbances |
1.9 | 5.2 | 6.8 |
|
Oppositional defiant disorder |
1.0 | 4.3 | 5.8 |
|
Depression |
0.6 | 3.8 | 8.7 |
|
Bipolar disorders |
0.2 | 1.9 | 4.6 |
|
Anxiety disorders |
0.7 | 2.0 | 2.3 |
|
Autism spectrum disorders |
7.9 | 7.8 | 5.2 |
|
Intellectual disorders |
2.9 | 6.3 | 7.6 |
|
Speech and language disorders |
20.7 | 15.3 | 5.8 |
|
Hearing disorders |
19.8 | 8.6 | 4.6 |
|
Learning disorders |
12.1 | 7.4 | 4.4 |
|
Cerebral palsy |
7.3 | 6.0 | 5.0 |
|
Asthma |
12.8 | 8.8 | 5.5 |
|
Sample size |
72,940 | 193,479 | 212,403 |
NOTES: Inclusion criteria: youth aged 3–17 with 11+ months of Medicaid eligibility and no dual eligibility in the year. A diagnosis was established based on the presence of one or more inpatient or two or more noninpatient claims with qualifying International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) codes.
SOURCE: NASEM, 2015.
geographically diverse subset of states for the years 2001–2010. Table 2-2 shows the presence of the most common diagnoses for which claims6 were made among children who qualified for Medicaid via SSI eligibility. These data provide additional information on specific diagnoses for which SSI recipients on Medicaid received services and include multiple or comorbid clinically diagnosed conditions.
As seen in Table 2-2, almost a fifth (17.6 percent) of children aged 12–17 received Medicaid-funded services for a diagnosis of attention-deficit hyperactivity disorder (ADHD), which was the most commonly reported diagnostic condition for which children among this age group qualified for SSI coverage. ADHD was also the most commonly observed disabling
___________________
6 Either one or more inpatient claims or two or more outpatient claims with qualifying International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) codes (on different dates).
condition for children aged 6–11 (21.9 percent), with speech and language disorders (15.3 percent) also prevalent among this age group.
Individuals with Disabilities Education Act
The Individuals with Disabilities Education Act (IDEA) drives special education in the United States, guaranteeing all children access to a free and appropriate public education (FAPE) through specially designed instruction, supplementary aids and services, and related services (see Chapter 5 for additional information on IDEA). IDEA defines a child with a disability as
having intellectual disability,7 a hearing impairment (including deafness), a speech or language impairment, a visual impairment (including blindness), a serious emotional disturbance (referred to in this part as ‘emotional disturbance’), an orthopedic impairment, autism, traumatic brain injury, another health impairment, a specific learning disability, deaf-blindness, or multiple disabilities, and who, by reason thereof, needs special education and related services.
As with SSI, IDEA defines a child with a disability according to a list of specific conditions that impact the child’s ability to function. However, the IDEA definition is broader in that it guarantees services and supports to all children, regardless of income or disability severity, who are found to be in need of such supports to ensure access to an FAPE, as guaranteed by the Education for All Handicapped Children Act (EAHCA) of 1975.8 IDEA’s categorical approach to defining disability is influenced by its legislative mandate to govern how states and public agencies provide early intervention, special education, and related services to children and youth with disabilities (ED, 2013). Because of this legislative mandate to identify children who require special education services to access FAPE, there are many more children with disabilities and severe health impairments or special health care needs than are served under IDEA. Individual states have the ability to write special education legislation that is more inclusive, or provides more services, than what is guaranteed under IDEA. Approximately 6.0 million9 school-aged children (ages 6–21) in the United States receive special education services related to their disability. Table 2-3 shows the prevalence of impairments for which children qualified for educational services by age group.
___________________
7 Updated terminology from 2010.
8 Public Law 94-142.
9 See https://www2.ed.gov/programs/osepidea/618-data/static-tables/index.html (accessed April 8, 2018).
| Disability Category | Ages 3–5 (%) |
Ages 6–11 (%) |
Ages 12–17 (%) |
Ages 18–21 (%) |
| All disabilitiesa | 759,801 | 2,868,816 | 2,837,905 | 342,161 |
| Autism | 10.1 | 9.9 | 8.9 | 12.7 |
| Deaf-blindness | 0.0 | 0.0 | 0.0 | 0.0 |
| Developmental delayb | 37.6 | 5.4 | 0.0 | 0.0 |
| Emotional disturbance | 0.4 | 3.7 | 7.2 | 7.0 |
| Hearing impairment | 1.1 | 1.1 | 1.1 | 1.2 |
| Intellectual disability | 1.8 | 5.0 | 7.4 | 18.6 |
| Multiple disabilities | 1.0 | 1.7 | 2.1 | 5.8 |
| Orthopedic impairment | 0.7 | 0.6 | 0.5 | 1.1 |
| Other health impairment | 3.1 | 13.3 | 17.9 | 12.5 |
| Specific learning disability | 1.1 | 28.9 | 48.5 | 37.9 |
| Speech or language impairment | 42.6 | 29.8 | 5.4 | 2.0 |
| Traumatic brain injury | 0.1 | 0.3 | 0.5 | 0.7 |
| Visual impairment | 0.4 | 0.4 | 0.4 | 0.5 |
NOTE: These data are a snapshot count collected by states in the fall of the identified school year.
a The total may not equal the sum of the parts because of privacy protections.
b Developmental delay is applicable only to children aged 3–9.
SOURCE: Adapted from U.S. Department of Education, EDFacts Data Warehouse (EDW): “IDEA Part B Child Count and Educational Environments Collection,” 2016–17. Data extracted as of July 12, 2017, from file specifications 002 and 089 (see https://www2.ed.gov/programs/osepidea/618-data/static-tables/2016-2017/part-b/child-count-and-educational-environment/1617-bchildcountandedenvironment-1.xlsx [accessed December 18, 2017]).
Maternal and Child Health Bureau
A separate concept, but one related to disability, is that of children with special health care needs (CSHCN), which the Maternal and Child Health Bureau (MCHB) defines as “those who have or are at increased risk for a chronic physical, developmental, behavioral, or emotional condition and who also require health and related services of a type or amount beyond that required by children generally” (NS-CSHCN, 2009–2010). MCHB was created under Title V of the Social Security Act to promote and improve maternal and child health nationwide (Harwood et al., n.d.). Hence, MCHB adopted this broader definition of CSHCN that does not list specific impairments or disability categories, but focuses primarily on identifying the need for any additional services and supports (McPherson
et al., 1998). Special health care needs can include such diverse health conditions as autism, cancer, depression, and HIV/AIDS, many of which can be disabling. MCHB selected this broad and inclusive definition for the purpose of emphasizing the characteristics shared by children with a wide range of health conditions (NS-CSHCN, 2009–2010). Additional information on the prevalence of CSHCN is provided in the following section on national surveys. An important subset of CSHCN is the group of children with medical complexity (see Box 2-1).
National Surveys
Several national population-based studies have been conducted to identify the population of children with disabilities or special health care needs, as well as trends with respect to the prevalence of certain conditions. Where robust longitudinal data are missing, cross-sectional data from national studies have been used by researchers to understand how disabling conditions influence outcomes for children, families, and communities.
The National Health Survey Act of 1956 appropriated funding for a continuous survey of the health of the nation’s civilian, noninstitutionalized population. Since 1957, the National Health Interview Survey (NHIS) has been fielded yearly by the CDC’s National Center for Health Statistics (NCHS). The NHIS gathers statistical information on the prevalence and
distribution of illness and disability across the United States through in-person confidential household interviews (CDC, 2017a). The survey contains questions on multiple aspects of health status, including activity limitations, injuries, health insurance, and access to and utilization of health care, as well as demographic information about the family (Harris et al., 2005). The NHIS defines disabled status in several ways, if a child experienced any of the following because of a chronic condition:
- Age <5 years: limitations in the kind or amount of play activities that are characteristic of other children;
- Age ≥3 years: needing help with personal care, including bathing, dressing, eating, getting in and out of bed and chairs, using the toilet, and getting around the home; and
- Age <18 years: difficulty walking without equipment and difficulty remembering, receipt of special education services or early intervention services, or any other activity limitation.
For children, the core in-person interview is conducted with a parent or adult who is knowledgeable about the child’s health and health care (Stein and Silver, 2003). The contents of the survey are regularly updated about every 10–15 years (CDC, 2010). Questions have also changed over time as new legislative requirements have been imposed and approaches to assessing certain disabilities (e.g., developmental disabilities) have been refined (CDC, 2017a). Because of these changes to the survey format, there is disagreement in the literature regarding trends in disability rates. A 2014 Child Trends study reviewing the NHIS population aged 5–17 found that the proportion of children and adolescents reported as having at least one limitation had remained relatively constant from 1998 to 2013 (fluctuating between 17 and 20 percent). In contrast, secondary analyses of NHIS data from 2001–2002, 2004–2005, 2007–2008, and 2011–2012 suggest marked increases in certain types of disability, such as speech and language disorders; intellectual impairments; and mental, emotional, and behavioral disorders, as illustrated in Table 2-4 (Houtrow et al., 2012, 2014). Based on the 2010–2011 NHIS data, Houtrow and colleagues (2014) estimate that approximately 4.6 million children aged 6–17 had a disability related to chronic conditions.
Between 2001 and 2010, the National Survey of Children with Special Healthcare Needs (NS-CSHCN) telephone survey was conducted three times by NCHS under the direction of MCHB. The NS-CSHCN adopted the U.S. Department of Health and Human Services’ definition of children with special health care needs as “those who have or are at increased risk for a chronic physical, developmental, behavioral, or emotional condition and who also require health and related services of a type or amount
beyond that required by children generally” (MCHB, 2013, p. 5). The most recent survey results, from 2009–2010, indicate that 15.1 percent of U.S. children (approximately 11.2 million children) had special health care needs—a figure that had increased slightly from the 2005–2006 report. As with NHIS findings, the extent to which these findings represent population increases versus more accurate diagnostic procedures is currently under debate. As of the most recent NS-CSHCN, 23 percent of households with children were estimated to have at least one child with a special health care need (MCHB, 2013).
From 2003 to 2012, the National Survey of Children’s Health (NSCH) was another telephone survey10 conducted by NCHS under the direction of MCHB. This survey explored intersecting features of children’s lives, including their health, families, communities, and social contexts. Data from the 2011–2012 survey suggest that 20 percent of children (approximately 14.6 million children) had a special health care need under the MCHB definition (Kids Count Data Center, 2013). In 2016, the NSCH was restructured so that the NS-CSHCN and the NSCH became integrated into one annual survey. The U.S. Census Bureau conducted the 2016 NSCH using a new methodology, with parents being invited to complete child-level questionnaires online or respond to mailed paper versions of the survey. Results from the 2016 NSCH suggest that approximately 11.6 million11 children aged 6–17 (23.5 percent of the total U.S. population of children in this age group) had special health care needs, 2.0 million (4.0 percent)12 of whose “daily activities [were] consistently affected, often a great deal.”
The Census Bureau also conducts an annual survey of disability in the United States. The American Community Survey is sent to a small percentage of households on a rotating basis yearly throughout the decade (U.S. Census Bureau, 2016). Unlike the NS-CSHCN and NSCH, the American Community Survey is categorical in nature, breaking down disability types according to primary impairments. Respondents are categorized into different age groups, including “under 5,” “5–17,” and “18–34.” Among children aged 5–17, approximately 3.0 million13 children, or 5.6 percent of all U.S. children in this age group are estimated to have a disability (U.S. Census Bureau, 2016).
Given the differing legislative purposes and operating definitions, it is not surprising that the prevalence of childhood disability as identified by
___________________
10 Cellular phone numbers were included for the first time in the 2011–2012 NSCH.
11 See http://www.childhealthdata.org/browse/survey/results?q=4661&r=1&g=604 (accessed April 8, 2018).
12 See http://www.childhealthdata.org/browse/survey/results?q=4668&r=1&g=604 (accessed April 8, 2018).
13 See https://factfinder.census.gov/faces/tableservices/jsf/pages/productview.xhtml?src=bkmk (accessed April 8, 2018).
respective agencies and national surveys varies substantially (Newacheck et al., 2004; Stein, 2007; Wells and Hogan, 2003). These discrepancies can be traced back to the underlying questions guiding data collection; specifically, broader definitions aim to identify what special health care needs are and how to address them, while narrower definitions (e.g., SSI, IDEA) result from reporting mandates that require the number of people with specific conditions to be quantified.
TABLE 2-4 Prevalence of Chronic Conditions Associated with Limitations in Usual Activities for U.S. Children Aged <18, 2001–2011a
| 2001-2002 | 2001-2002 (N = 54,651) | 2004-2005 (N = 52,881) | |
|---|---|---|---|
| Estimated No. Cases | Cases per 100,000 (SE) | Cases per 100,000 (SE) | |
| Any physical health condition | 1,099,000 | 1,512 (65) | 1,265 (60) |
|
Asthma or breathing problem |
586,000 | 807 (47) | 617 (44) |
|
Hearing problem |
196,000 | 270 (24) | 279 (24) |
|
Vision problem |
188,000 | 259 (27) | 195 (19) |
|
Bone, joint, or muscle problem |
175,000 | 241 (23) | 227 (25) |
|
Injuries |
62,000 | 86 (15) | 71 (13) |
| Any neurodevelopmental or mental health condition | 3,927,000 | 5,404 (125) | 5,543 (127) |
|
Epilepsy or seizures |
162,000 | 223 (23) | 154 (20) |
|
Speech problems |
835,000 | 1,150 (59) | 1,301 (54) |
|
Learning disability |
1,590,000 | 2,188 (72) | 1,634 (75) |
|
Attention-deficit hyperactivity disorder |
1,071,000 | 1,474 (67) | 1,467 (67) |
|
Mental retardation |
163,000 | 224 (23) | 262 (24) |
|
Other mental, emotional, or behavioral problems |
695,000 | 956 (54) | 1,038 (55) |
|
Other developmental problem |
462,000 | 636 (40) | 785 (52) |
| Other, not classifiable | |||
|
Other impairment or problem |
371,113 | 511 (39) | 480 (38) |
|
Birth defect |
253,753 | 349 (29) | 345 (30) |
a Parents could answer that their child had >1 condition contributing to activity limitation.
b Wald trend test P<.05, percentage change values calculated between 2001–2002 and 2010–2011.
c Wording for this item was altered in 2011 to “intellectual disability, also known as mental retardation, contributes to activity limitation.” Prevalence was 319 per 100,000 population in 2010 and 411 per 100,000 population in 2011.
SOURCE: Houtrow et al., 2014 using National Health Interview Survey (NHIS) data from 2001–2011.
In sum, estimates range from 2.0 percent of all children aged 6–17 considered to have a disability (SSI beneficiaries) to 23.5 percent identified as having special health care needs. It is important to note that although the
| 2007-2008 (N = 40,569) | 2010-2011 (N = 50,793) | 2010-2011 | 2001-2011 |
|---|---|---|---|
| Cases per 100,000 (SE) | Cases per 100,000 (SE) | Estimated No. Cases | % change in prevalence |
| 1,229 (68) | 1,333 (66) | 994,000 | –11.8 |
| 589 (44) | 612 (40) | 456,000 | –24.2b |
| 263 (31) | 312 (32) | 233,000 | 15.6 |
| 266 (33) | 295 (29) | 220,000 | 13.9 |
| 230 (29) | 269 (34) | 200,000 | 11.6 |
| 73 (20) | 71 (16) | 53,000 | –17.4 |
| 5,977 (163) | 6,531 (149) | 4,864,000 | 20.9b |
| 212 (29) | 203 (23) | 151,000 | –9.0 |
| 1,600 (82) | 1,876 (80) | 1,397,000 | 63.1b |
| 1,747 (87) | 1,903 (80) | 1,417,000 | –13.0b |
| 1,676 (77) | 1,799 (83) | 1,400,000 | 22.0b |
| 217 (31) | 365 (36) | 272,000 | 63.0b,c |
| 1,314 (73) | 1,575 (71) | 1,173,000 | 64.7b |
| 759 (56) | 873 (48) | 650,000 | 37.3b |
| 362 (36) | 480 (36) | 358,000 | –6.0 |
| 370 (34) | 434 (33) | 323,000 | 24.4b |
SOURCE: Houtrow et al., 2014 using National Health Interview Survey (NHIS) data from 2001–2011.
committee defined “school-aged” as including youth during their transition years (≤25 years), data from most programs and surveys are not categorized in this way. Accordingly, prevalence estimates presented in this section generally represent school-aged children aged 6–17,14 underrepresenting the
___________________
14 IDEA includes data on youth who continue to receive special education services through age 21; however, youth aged 18–21 represent only approximately 5.7 percent of the total U.S. population of children and youth aged 6–21 receiving services for a disability. The American Community Survey also includes children age 5 in its data on children.
number of school-aged children with disabilities that are within the scope of this report.
Figure 2-1 depicts the program eligibility and prevalence estimates of, as well as some overlap among, selected programs and services available for children with disabilities. Detailed information on how these estimates were calculated is available in Appendix C.
CONTEMPORARY CONCEPTUAL UNDERSTANDING OF CHILDHOOD DISABILITY
Increasingly, disability is not solely considered as reflecting an impairment of the child but rather as the result of a complex interaction among the child, the impairment, and the environment (Luckasson et al., 1992, 2002; Schalock et al., 2010). Contemporary notions of childhood disability advance the idea that the nature and severity of disability are defined not only by underlying medical conditions but also by the physical environment, demands, expectations, opportunities, and social roles that children assume in their daily lives. Accordingly, both during childhood and in terms of improving outcomes for children with disabilities, it is necessary to focus attention not only on treatments for impairments but also on those factors that enhance children’s ability to perform activities appropriate to their age and participate in social and community activities in the context of their
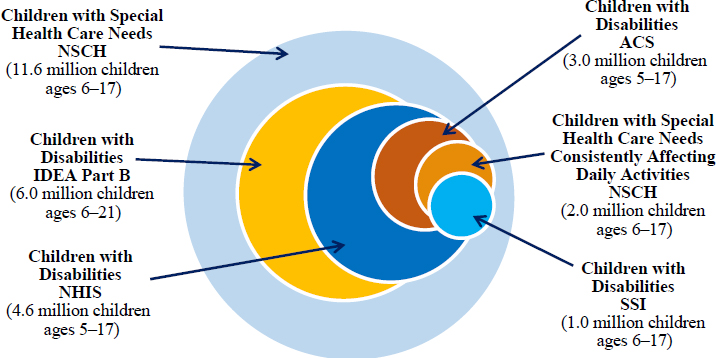
NOTE: ACS = American Community Survey; IDEA = Individuals with Disabilities Education Act; NHIS = National Health Interview Survey; NSCH = National Survey of Children’s Health; SSI = Supplemental Security Income.
environment. The conceptualization of disability as a blending of both medical and contextual (i.e., social or environmental) factors is promoted as a “biopsychosocial model” of childhood disability (WHO, 2001). Thus, the conceptualization of childhood is broad and encompasses the operational definitions of childhood disability utilized by programs, services, and tracking agencies.
A prominent example of this approach to understanding disability is the World Health Organization’s (2001) International Classification of Functioning, Disability and Health (ICF) framework. The ICF (depicted in Figure 2-2) is an integrated biopsychosocial model that includes both physical and behavioral aspects of health, and can be used to define and measure health outcomes that disability programs and services strive to optimize. The ICF moves beyond the traditional medical model approach of focusing specifically on body structures (anatomical parts of the body, such as organs, limbs, and their components), body functions (physiological functions of body systems, including mental and behavioral health functions), and their impairments (problems in body structure and function, such as a significant deviation or deficit). It recognizes that impairment does not equal disability; rather, disability results from the complex interplay between impairments and personal and environmental factors, and is best understood in terms of activities (execution of a task by an individual) and participation (involvement in life situations).
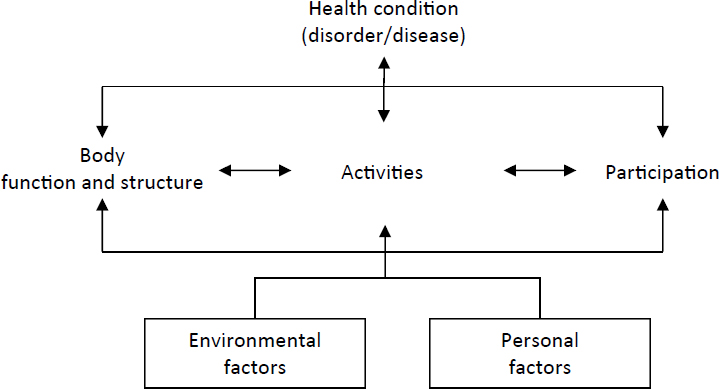
SOURCE: WHO, 2001.
The Committee’s Conceptualization of Childhood Disability
As noted earlier, building on earlier work of the Institute of Medicine (IOM), the National Research Council (NRC), and the ICF, the committee adopted a working definition of childhood disability as “an environmentally contextualized health-related limitation in a child’s existing or emerging capacity to perform developmentally appropriate activities and participate, as desired, in society” (see Box 1-2). Furthermore, the committee adopted a social-ecological perspective in which disability results from the interaction of one’s health conditions with personal and environmental factors to result in functional limitations in one’s ability to carry out tasks and participate in life events. The committee views child development, socialization, and adaptation as a lifelong process of continuity and change, and while this study, as noted in Chapter 1, focuses on school-aged children, the committee could not ignore the life course perspective, which acknowledges that early experiences and exposures are often linked with outcomes as one ages (Alwin, 2012; Elder, 2000), even within the defined school-aged span.
Figure 2-3 depicts the committee’s approach to conceptualizing how personal characteristics, environmental factors, and the collective set of programs and services may impact near- and long-term outcomes for children with disabilities. The focal point in the figure is the child, within the family context. The figure depicts how the child’s characteristics and environmental factors shape the need for and impact of services and supports.
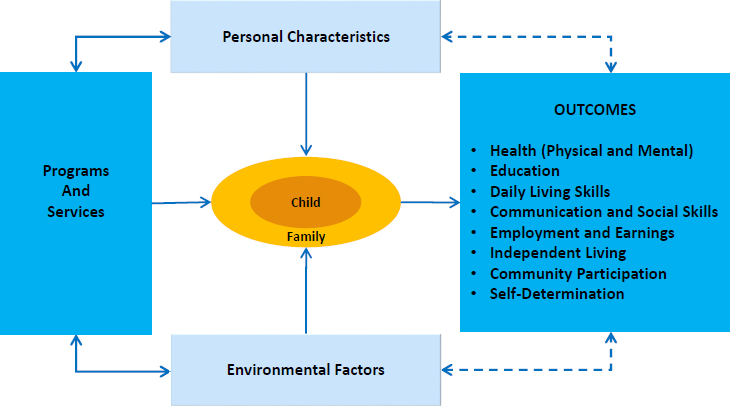
To be effective, programs and services should be aligned with the child’s personal strengths and challenges, as well as the environmental factors that affect the child and his or her family (e.g., the financial resources available to the family, access to educational and medical services, supports in the child’s community, employment opportunities for youth with disabilities as they transition to the workplace). When programs and services are implemented in alignment with child-level and environment-related needs, positive changes in near-term (e.g., symptoms of a specific condition) and long-term (e.g., employment in adulthood, independent living, community participation, self-determination) outcomes can occur. As outcomes are achieved, they, in turn, affect the child’s personal and environmental factors that influence the need for and impact of subsequent services.
Life Course Perspective and the Role of Personal, Social, and Environmental Factors
Multiple scientific streams have contributed to the development of life course theory, which posits that events early in life can influence biological systems in ways that have lifelong effects, and that these effects may vary depending on the timing of the exposure to such events in relation to the child’s developmental stage (Alwin, 2012; Elder, 2000; Halfon et al., 2014a). Various enabling and disabling factors in a child’s life build up over time, and their aggregation leads to greater health or disability. Exposure to multiple and/or persistent biological, behavioral, and social risk factors form a cumulative disadvantage that erodes an individual’s health resiliency over time (Halfon et al., 2014a).
Thus, a child’s needs for programs and services evolve. In early childhood, for example, the focus on both family- and child-level supports is greater. As children move into elementary school, educational services become the core set of supports. As youth near adulthood, they must begin making decisions that may affect their long-term adult outcomes, and transition planning becomes particularly important during the transition from secondary school to adulthood. Therefore, conditions that are present early in a child’s life are often the most impactful, and services that buffer the child and family and address disabilities early in life are often the most effective.
As discussed in the previous section, contemporary notions posit that disability is more than just impairment—it results from the complex interplay of the child, her or his impairment, and her or his environment. In this section, the committee explores a variety of contextual factors that may impact disability over the course of a child’s life. The section begins with a look at two factors inherent to the child her- or himself: severity of the impairment and comorbidities. Then, characteristics of the child’s family
and socioeconomic status are explored. Finally, the committee discusses various social-environmental factors that can impact childhood health and disability. It is important to note that none of these factors stand alone; factors that originate with the family or community may become personal factors as the child develops, and the child’s personal factors often impact his or her family and environment.
Severity of Impairment
One individualized risk factor that impacts health outcomes is the severity of the child’s impairment. Children with severe disabilities have the highest rates of emergency department utilization and inpatient hospitalizations due to acute illnesses and worsening of chronic conditions (Ananth et al., 2015; Berry et al., 2011a,b, 2013; Burns et al., 2010; Neuman et al., 2014; Simon et al., 2010). Certain types of severe disabilities have been shown to be detrimental to achieving positive outcomes for a variety of reasons. As mentioned, children with medical complexity (those with chronic health conditions who are severely affected or medically fragile and have multiple, complex, and intensive needs) require frequent, recurrent engagement with health care services (Ireys et al., 1997). Many CMC experience recurrent hospitalizations because they require invasive procedures, surgeries, and other inpatient treatments to maintain their health (Berry et al., 2009, 2011b).
Another example of a severe disability domain is severe mental health impairments, which can affect individuals from childhood into their adult years. For nearly three-quarters of all people with mental health problems, onset occurred before age 25 (Kessler et al., 2007). Fully 22 percent of all adolescents are considered to have mental health problems (Halfon et al., 2014b; Merikangas et al., 2010). Similarly, data from the CDC indicate that 20–25 percent of children have a serious mental illness (NHANES, 2012). Personal and social-environmental factors also interact to affect outcomes, as data indicate that white children use mental health services and are prescribed psychotropic medications more frequently relative to black or Hispanic children, with widening disparities in mental health care expenditures between white and Hispanic children being noted in recent years (Leslie et al., 2003).
Comorbidities
Children with at least one severe form of disability are at increased risk for having or developing co-occurring impairments (Merikangas et al., 2015). Research has shown that physical and mental health impairments commonly co-occur (Boothroyd and Armstrong, 2005; Combs-Orme et al.,
2002; Merikangas et al., 2015), while chronic health impairments during childhood have been linked to increased rates of emotional and behavioral problems and increased risk for psychiatric diagnoses during adolescence (Hysing et al., 2009).
According to the 2016 National Academies report referenced earlier, speech and language disorders are particularly difficult to estimate given that approximately 40 percent of children with speech and language disorders in nationally representative studies have serious comorbidities such as intellectual disabilities, autism spectrum disorder, and other neurodevelopmental and behavioral disorders (NASEM, 2016). Additionally, severe speech and language disorders can increase the risk for a wide variety of adverse outcomes, including social isolation, learning disabilities, behavioral disorders, poor academic achievement, and chronic underemployment, yet the majority of children requiring services for speech and language disorders are not accessing multiple types of services at any one time (Stein and Silver, 2003).
From adolescence through adulthood, compared with the general population, individuals with mental health disorders are more likely to experience a comorbid substance use disorder (SUD), and people with an SUD are more likely to have a mental disorder. “Substance use disorder” is defined in the fifth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5) as a problematic pattern of substance use leading to clinically significant impairment or distress. SUD is operationally defined more broadly by the Substance Abuse and Mental Health Services Administration (SAMHSA) (2011) as encompassing abuse of and dependence on alcohol or drugs, including both illicit and prescription drugs, as well as misuse of over-the-counter medications. Among the general population, substance use typically begins during adolescence and peaks during the young adult years (Johnston et al., 2004). According to the 2009 National Survey on Drug Use and Health (NSDUH), more than 1.7 million youth aged 12–17 met the DSM-IV criteria for an alcohol or illicit drug disorder within the past year, which translates to approximately 7 percent of youth in the specified age range (SAMHSA, 2010).
Data from the 2002 NSDUH indicate that among young adults aged 18–25 with a serious mental illness (SMI), 48 percent had engaged in illicit substance use during the past year (Davis et al., 2012; SAMHSA, 2003). The 2016 NSDUH data indicate further that 711,000 young adults aged 18–25 had co-occurring SMI and SUD (SAMHSA, 2017). Having recently experienced a major depressive episode also increases the likelihood of a co-occurring SUD. In 2014, among adolescents aged 12–17, 33 percent of those who reported having experienced a major depressive episode in the past year had used illicit drugs, compared with 15.2 percent of adolescents who had not experienced such an episode. Among this age group, 340,000 youth were identified as having experienced a co-occurring major depressive
episode and SUD in the past year (NIDA, 2014). The transition to adulthood does not necessarily minimize these risks, as among individuals with past-year SMI, co-occurring SUD rates were most common among respondents aged 18–25 (35.3 percent) (NIDA, 2014).
Rates of SUD among youth and young adults with physical or sensory disabilities are more difficult to quantify. Some studies suggest that individuals with physical disabilities have higher rates of SUD, while others suggest lower rates (SAMHSA, 2011). Active SUDs can also cause concomitant health problems, particularly diabetes and cardiac disease. In addition, substance use can cause harmful interactions with medications prescribed to treat a disability, ranging from impaired cognition and loss of muscle control to seizures and death. SAMHSA (2011) identified the following substance use risk factors for people with physical disabilities: depression, social isolation, history of physical or sexual abuse, and chronic medical problems. Risk factors for developing SUDs related to prescription drug abuse include chronic pain, access to prescription medication, and enabling by caregivers (SAMHSA, 2011).
Parenting and the Family
A shift of care from institutions to community-based settings has increased demands on families, and the research literature shows considerable variation in how families adapt to these demands. According to the 2009–2010 NS-CSHCN, approximately 5.6 million children with special health care needs received 1.5 billion hours annually of family-provided health care, which equates to 5.1 hours weekly per child (Romley et al., 2017). In many instances, complex nursing care is now being carried out by parents, sometimes with little oversight by health care professionals (Kirk, 2001).
Although fathers of children with disabilities may experience impacts on their workforce participation (Kuhlthau and Perrin, 2001), the majority of informal caregivers of children with chronic conditions and disabilities are mothers, who are most knowledgeable about the needs of their children and are central to their children’s health and integration into family, school, and community life (Bourke-Taylor et al., 2010; Dalvand et al., 2015; Gorzkowski et al., 2011; Nelson, 2002; Rehm and Bradley, 2005). The care mothers provide for their children with disabilities is highly specialized and technical, but rarely compensated (Traustadottir, 1991).
Many mothers report positive impacts of this role, but they also report loss of employment, stress, strain, fatigue, and physical and mental health problems (Dodgson et al., 2000; Fleming et al., 1994; Reichman et al., 2008). While nearly 60 percent of mothers of children without disabilities maintain employment or reenter the workforce after the birth of their children, relatively few mothers of children with severe disabilities work outside
of the home (Okumura et al., 2009; Thyen et al., 1999; Traustadottir, 1991). The time expended in caring for a child with a disability can limit the time available to devote to other children or other family members, and families of children with disabilities may need to rely on extended family members for assistance (Reichman et al., 2008). Because of the centrality of informal caregivers to children with disabilities, the toll of informal caregiving is concerning. Moreover, it often produces adverse outcomes not only for the caregiver but also for the child who receives the care, including emotional stress; anxiety; depression; poor mental health; and barriers to social, vocational, and personal pursuits (Gibson et al., 2012; Green, 2007; Nicolais et al., 2016).
It is important to recognize the cultural differences among families raising children with disabilities. In particular, racial and ethnic minority families may feel overburdened and helpless because intervention programs and strategies may be incompatible with their culture (Algood et al., 2013). Language can be a barrier to care as well. Until relatively recently, for example, very few U.S. autism centers had any Spanish-speaking staff, even though communication is of central importance to autism services (Zuckerman et al., 2014), and few centers currently have services for families that speak neither English nor Spanish. On August 11, 2000, President Clinton signed Executive Order 13166, “Improving Access to Services for People with Limited English Proficiency.” The executive order required federal agencies to develop and implement a system to provide their services in such a manner that people with limited English proficiency can have access to those services. This executive order was supported by a policy guidance document from the Department of Justice that set forth compliance standards to ensure that federal agencies were not violating Title VI of the Civil Rights Act of 1964 by discriminating on the basis of national origin (DOJ, 2000).
At present, NHIS data indicate that mental health conditions among children from racial and ethnic minorities are recognized by parents and are medically diagnosed less frequently than is the case among their racial/ethnic majority peers. It has been hypothesized that parental attitudes about diagnosis and treatment, cultural and linguistic barriers, and discrimination help account for differences in prevalence estimates by race/ethnicity (Kogan et al., 2009; Magaña et al., 2012; Mandell et al., 2009).
Many children with disabilities live in nontraditional family settings, for example, with relative caregivers, in group homes, or with foster families. Children and youth who undergo multiple placements through foster care also experience interruptions to their education through excessive absences and school changes. One-third of all foster youth (with and without disabilities) report having changed schools five or more times, which poses a significant barrier to continuing individualized education programs
(IEPs) and maintaining support teams for foster children with disabilities (Courtney et al., 2004). In situations where the child is without a consistent caregiver who can teach developmentally appropriate life skills, children with disabilities—particularly those with intellectual disabilities, neurodevelopmental disorders, or significant mobility limitations—are at increased risk for falling behind their peers in the acquisition of daily living skills that are critically necessary to achieving independent living outcomes in the future (Bal et al., 2015; Smits et al., 2011; van Duijn et al., 2010), and may require more extensive supports in adulthood (Anderson et al., 2014; Woolf et al., 2010).
Socioeconomic Status
The connection between childhood poverty and child health has been recognized for several decades (Stein et al., 2010). Children who live in poverty are often exposed to environmental toxins, violence, food insecurity, and inadequate nutrition, among other risk factors (Merikangas et al., 2010; Pulcini et al., 2017), and are more likely to develop health conditions associated with disability relative to children growing up in environments with fewer stressors. In later childhood, these factors may be exacerbated by the direct and indirect costs associated with caring for a child with disabilities and their impact on the family’s ability to thrive in a social context.
Additionally, children exposed to such factors as intrauterine malnourishment are at increased risk for developing a disability (Stanton-Chapman et al., 2004). Mothers in low-income households are more likely to deliver preterm, and their preterm babies demonstrate higher proportions of developmental disadvantage, as well as worse health outcomes (NRC and IOM, 2004). Even when preterm babies have an identical medical status, socioeconomic status greatly influences their prognosis, with those from less advantaged backgrounds being more likely to experience poorer outcomes (Escalona, 1982; Stein et al., 2010).
Disability and poverty are intertwined: Families living in poverty have higher rates of disability, and disability leads to lower household income (Lustig and Strauser, 2007). Children who live in low-income households have increased rates of most chronic health conditions, as well as more severe conditions and complications (Houtrow et al., 2011; NASEM, 2016). Data show that disability, like morbidity and mortality, is higher among children of low socioeconomic status (NASEM, 2015). A strong association exists, for example, between poverty and developmental delays, such as language delays (NASEM, 2016). Higher rates of asthma, obesity, developmental delay, learning disability, and behavioral disorders are seen in these children (Stein et al., 2010). Children living in poverty also are
more likely to experience housing instability (Merikangas et al., 2010), and individuals with unstable housing are less likely to manage health issues, such as diabetes (Vijayaraghavan et al., 2011). And when poverty persists over time, the health and other effects on children and youth are magnified (Brooks-Gunn and Duncan, 1997).
Poverty status is associated with restrictions in all types of participation, such as school attendance and any organized activity (Houtrow et al., 2012). Poverty is also associated with other social disadvantages, such as single parenthood, minority status, and limited education, which can have a cumulative effect on child health and disability (Bauman et al., 2006; Evans, 2004). Most children (approximately 70 percent) receiving SSI disability benefits live in a family headed by a single parent.15 Furthermore, as noted earlier, children living in poverty have more limited access to care, and even those with insurance may face additional barriers and consequently have poorer health outcomes (Van Cleave et al., 2010). Families of children with severe disabilities experience more drain on their family resources compared with other families, as having a disability is associated with a greater likelihood of more health care expenditures (Mulvihill et al., 2005; Newacheck et al., 2000). Having a child with a disability is associated with loss of parental income due to unemployment, underemployment, and opportunity costs (e.g., parents not being in a position to take on more challenging work responsibilities or to return to school). As a result of the direct and indirect effects of the child’s disability, families are more likely to experience poverty and have fewer resources with which to close the gap between the child’s abilities and the social, health, and educational resources that may help minimize the disability.
Service Availability and Ability to Access Services
In today’s society, families of children with disabilities seek services from numerous, varied public and private programs that form a highly complex web of services and providers (Peters, 2005). The absence of an integrated system of care in the United States can make it difficult for families to understand what benefits are available, how to access them, and how to assemble supports that best match their children’s needs (Aron et al., 2007). Figure 2-4 illustrates the complexity facing children with disabilities and their parents in trying to navigate the multiple, complex service systems intended to meet their multifaceted needs. This “care map” helped one mother stay organized and communicate succinctly with her son’s care team, including teachers, friends, and family.
___________________
15 Wittenburg, D., testimony before the House of Representatives’ Subcommittee on Human Resources, Washington, DC, October 27, 2011.
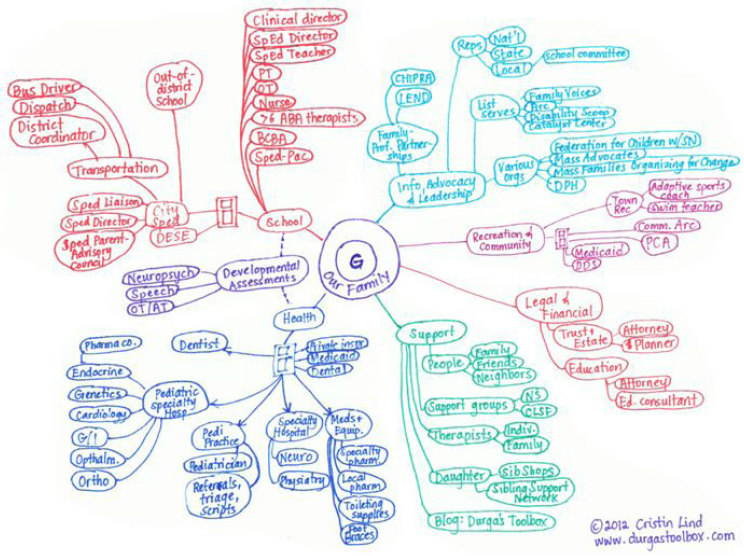
SOURCE: Lind, 2014.
The availability of and access to effective interventions plays an important role in a child’s ultimate vulnerability to adverse health outcomes. While this report does not (and cannot) address primary prevention in the development of disability, reducing or preventing long-term effects of secondary or comorbid disability and restoring function are paramount for this population of children. Not all disability can be ameliorated, but new opportunities are offered by advances in medical care and treatments. Improvements in the delivery of specialized care have resulted in a growing number of children surviving with complex conditions (Halfon et al., 2012). Many more children survive cancer as the result of advances in treatments, and technological advances also have allowed children with hearing impairment to receive cochlear implants, which can improve their hearing (Romig, 2017). Many children who access these advances in care thrive with the treatment (BCH, 2009).
However, many gaps exist in access to available treatments. This is the case especially for children living in poverty. Such barriers as a lack of transportation, the lack of a single point of entry to services, financial
constraints, shortages of child mental health professionals, and stigma related to mental health problems help explain why so few families initiate treatment and maintain their treatment schedule over time (AAP, 2004).
Many communities and health services cannot provide the resources necessary for children with disabilities (and their families) to achieve optimal health and social outcomes (King et al., 2002). Nationally representative studies have shown that children with special health care needs who live in rural communities have limited access to pediatricians and face transportation barriers to seeking care, and consequently have higher levels of unmet need (Kelleher et al., 1992). Absent strategies to increase the health care workforce in rural communities and new care arrangements (e.g., the use of telehealth networks), children with disabilities who reside in rural areas are likely to experience worse outcomes relative to their counterparts in other areas (Robinson et al., 2017). A 1990 surgeon general’s report stated that only 20–25 percent of children with mental health conditions received adequate assessment and treatment services for those conditions (HHS, 2000). Without treatment, child and adolescent mental health conditions can persist and lead to academic failure, unemployment or poor employment, and poverty in adulthood (Schulte-Körne, 2016).
Abuse and Neglect
When home life is unstable because of substance abuse issues, violence, or other forms of aggressive behavior, children with disabilities are at increased risk of victimization by experiencing violence, maltreatment, or abuse (Sullivan and Knutson, 2000; UNICEF, 2013). A longitudinal study tracking children from kindergarten to 12th grade (N = 585) found that adolescents who experienced early maltreatment displayed higher levels of aggression, anxiety/depression, dissociative behaviors, delinquent behaviors, posttraumatic stress disorder (PTSD), cognitive or processing delays, and antisocial behavior at a rate twice that of their nonmaltreated counterparts (Lansford et al., 2002). One of the most extensive and widely cited studies exploring the relationship between childhood disability and experiencing violence or neglect found that the rate of maltreatment experienced by children with disabilities (31 percent) was more than 3 times that of children without disabilities (9 percent) (Sullivan and Knutson, 2000). Specifically, children with disabilities were nearly 4 times more likely than children without disabilities to be neglected or experience physical or emotional abuse, and more than 3 times more likely to be sexually abused (UNICEF, 2013). The rate of experiencing multiple forms of maltreatment also was significantly higher for children with disabilities (63 percent) than for their peers without disabilities (55 percent) (Sullivan and Knutson, 2000).
Research further suggests that the type of disability may be a predictive factor in determining whether children will experience abuse or maltreatment in their home. In a whole-population cohort study (1983–2001), children who had been diagnosed with conduct disorders, psychological disorders, speech and language disorders, learning disabilities, or cerebral palsy16 were more likely than children diagnosed with autism spectrum disorder or sensory disabilities to have documented cases of child abuse or neglect (Spencer et al., 200517). Children with conduct disorders and learning difficulties were also more than 6 times as likely to have experienced sexual abuse relative to children with other types of disabilities, while children with either conduct disorders or nonconduct psychological disorders were more likely to experience forms of emotional abuse (Spencer et al., 2005). On the whole, children and youth with developmental disabilities are estimated to be between 2.0 and 4.6 times more likely than their peers without disabilities to experience some form of sexual abuse (Smith and Harrell, 2013).
Children and youth with intellectual disability are particularly vulnerable to human trafficking—a form of modern-day slavery where people profit from the control and exploitation of others—because certain abilities to protect themselves may be diminished. According to the Ohio Department of Developmental Disabilities, specific risk factors for individuals with intellectual disabilities include social powerlessness, communication skill deficits, diminished ability or resources to protect themselves, and inability to detect who is safe to be around (ODODD, 2014). Additionally, people with disabilities tend to rely on others more for meeting their basic needs, creating an imbalance of power between the individual and caregiver, which provides caregivers with an opportunity to engage in human trafficking (OVC, n.d.). Research has suggested that 97 to 99 percent of abusers are known and trusted by victims who have developmental disabilities (Balderian, 1991).
Child abuse and neglect can impair a child’s emotional and psychological well-being, and co-occurring factors such as poverty, complex medical issues, and lack of a competent, consistent caregiver can compound these negative effects (Jonson-Reid et al., 2004; Spencer et al., 2005). All forms of childhood maltreatment have been shown to impact long-term outcomes for all children. The long term effects of child abuse include lingering PTSD, anxiety and depression, and SUDs in adulthood (Smith and Harrell, 2013).
___________________
16 “The association of cerebral palsy with registration in any category was not significant at the 5% level after adjustment for birth weight, gestational age, maternal age, and socioeconomic status” (Spencer et al., 2005, p. 612).
17 Researchers controlled for potentially confounding factors such as birthweight, gestational age, maternal age, and socioeconomic status.
Moreover, child abuse and neglect have been identified as risk factors for becoming victims of human trafficking, particularly if parents were abusing drugs or sexual abuse occurred in the home (ODODD, 2014).
Bullying
Bullying is defined as repeated aggressive behavior that involves a real (or perceived) power imbalance (stopbullying.gov, n.d.). Bullying can range from making fun of a child’s health condition, such as a food allergy or wearing a hearing aid, to long-term belittling and exclusion of a child. Although limited and relying primarily on less rigorous data collection methods (e.g., small sample sizes, convenience samples, self-report surveys), research indicates that children and adolescents with disabilities are at increased risk for bullying (also referred to as peer victimization in the literature) compared with their peers without disabilities. One recent review of the research found that between 44 percent and 77 percent of children with autism spectrum disorders and/or their parents reported experiencing peer victimization in the previous month (Storch et al., 2012). Likewise, studies suggest that children with ADHD are more likely to experience bullying, and equally likely to engage in bullying behaviors, compared with their classmates without ADHD (Twyman et al., 2010; Wiener and Mak, 2009). Children with obvious physical disabilities, such as muscular dystrophy, also are more likely to be bullied than their peers (Carter and Spencer, 2006).
Bullying leads to negative short-term outcomes that include anxiety and depression, poor academic performance, and becoming socially withdrawn. In severe cases, bullying may also lead to short-term negative outcomes such as self-harming behaviors and substance abuse, as well as devastating long-term outcomes that include dropping out of school; decreased motivation to find satisfying employment or seek promotion; and in extreme cases, suicide (BCH, n.d.). Since 2009, the Office for Civil Rights (OCR) has received more than 2,000 complaints alleging that schools, school employees, or school boards violated a student’s Title II or Section 504 rights through permitting “peer harassment based on race, color, national origin, sex, or disability that is sufficiently serious to create a hostile environment and such harassment is encouraged, tolerated, not adequately addressed, or ignored by school employees”18 (ED, 2014).
In 2013, the Office of Special Education and Rehabilitative Services (OSERS) issued a “Dear Colleague” letter to schools to provide guidance and reinforce the OSERS policy that when bullying of a student with a disability results in the student not receiving meaningful educational benefit
___________________
18 34 C.F.R. parts 100, 104, and 106.
under IDEA, the school must remedy the problem, regardless of whether the bullying was based on the student’s disability. Programs aimed at reducing negative outcomes associated with bullying by promoting understanding of disability and fostering friendships between students with and without disabilities are discussed in Chapter 5.
Perceived Stigma
The extent to which the community at large embraces or ignores children and youth with disabilities has a profound impact on their later outcomes. Unfortunately, the level of support and community inclusion received by a child with a disability often depends on what the disability is and what symptoms are noticeable. For example, children with cancer are visible in pediatric cancer research advertisements and on television; classmates may shave their heads in solidarity; and community fundraisers are often organized to help eradicate the disease. In contrast to the rich community support offered to children with cancer, children with severe physical or mental/emotional/behavioral functional limitations may experience stigma, described as the actual or inferred attribute that damages the reputation of the individual and degrades him/her to a socially discredited or devalued status (Goffman, 1986) when participating in community activities (Heflinger et al., 2014). Families that have children with emotional and behavioral problems have been reported to perceive high levels of stigma in the form of teachers and neighbors stereotyping their child as either dangerous or incompetent (Heflinger et al., 2014). As a result, families that perceive stigma are reticent to bring their child into the community, thereby denying the child opportunities for learning how to operate in public settings (Lalvani, 2015).
Studies have shown that individuals who hold stigmatizing attitudes are more likely to be younger and less educated (Franklin, 2005) and to have less experience interacting with individuals who have disabilities (Corrigan et al., 2001; Heflinger et al., 2014). While recent research has begun to explore the immediate impact of stigma on child well-being, the long-term impact of perceived stigma may promote negative outcomes in the areas of independent living, civic participation, and community integration (Heflinger et al., 2014).
Interactions with the Juvenile Justice System
Children and youth with disabilities are prone to interacting with the criminal justice system at disproportionately higher rates relative to the general population. The National Longitudinal Transition Survey-2 (NLTS-2) found that 47 percent of young adults with disabilities had been stopped
by police for reasons other than a traffic violation at some point in their lives, with 26 percent reporting such interactions within the preceding 2 years (NCSER, 2010).
One study of adjudicated delinquent youth (N = 397) in Cuyahoga County, Ohio, found that 32.5 percent of youth on probation had a special education disability classification (i.e., qualified for special education services), 39.8 percent had a diagnosed mental health disorder, and 32.4 percent had a diagnosed substance abuse disorder (Mallett, 2009). Among a subset of this population who were detained or incarcerated (N = 123), 39.4 percent had a special education disability classification, 68.2 percent had a mental health disorder, and 49.5 percent had a substance abuse disorder (Mallet, 2009). Similar results from a survey of 38 state juvenile or combined juvenile and adult corrections systems revealed that 33.4 percent of youth had a disabling condition for which they were receiving special education services (Quinn et al., 2005).19 Among youth diagnosed with a disability, the most common disability classifications were emotional disturbance (47.7 percent) and specific learning disabilities (38.6 percent), followed by intellectual disability (9.7 percent), other health impairments (2.9 percent), and multiple disabilities (0.8 percent) (Quinn et al., 2005). Another study of children and youth aged 10–18 who had been arrested in Cook County, Illinois (N = 1,829) found high rates of disruptive behavior disorders, anxiety disorders, mood disorders, and ADHD, all of which affected females proportionately more than their male peers (Teplin et al., 2015).
When children with disabilities interact with the juvenile justice system, rates of adverse education outcomes increase. In an examination of academic characteristics and education-related outcomes 3 years after release from Florida juvenile justice facilities, children with emotional and behavioral disorders were found to be 41 percent less likely to earn a grade promotion and 61 percent less likely to earn a diploma during commitment compared with students without disabilities (Cavendish, 2014). Similarly, in a 5-year longitudinal study following youth in Oregon upon their leaving the correctional system (N = 532), Bullis and Yovanoff (2005) found that youth with disabilities were 1.76 times less likely to be engaged (in school and/or work) 6 months after leaving Oregon Youth Authority [OYA] and 2.22 times less likely to be engaged 12 months after their release.
___________________
19 “Prevalence rates by state ranged from 9.1% to 77.5%, with a median of 33%” (Quinn et al., 2005, p. 12). The researchers also note that the average prevalence rate is likely low because of low rates of service delivery in some states.
CASE STUDIES20
The following are actual cases used here (anonymously) to illustrate the diverse and complex health, education, mental health, and rehabilitation services needed to support positive health outcomes for children and youth with disabilities. As noted earlier, children and youth with disabilities and their families must access and integrate services from multiple organizations and professionals over time. These case studies also illustrate the scope and challenges of this study with regard to examining health outcomes in children and youth with disabilities and services to improve their outcomes.
Case Study #1
W.S., a 21-year-old young man, was born in 1996 and was quickly diagnosed with Down syndrome (Trisomy 21), the Trisomy 21 having been confirmed via amniocentesis 4 months before his birth. He was enrolled in early intervention services to support his mental and physical development and received home visits from a developmental team, which included a speech pathologist, an occupational therapist, and a feeding specialist. As might be expected for a patient with Down syndrome, he experienced frequent ear infections. He was tested by an audiologist and required placement of middle ear pressure equalization tubes by an otolaryngologist at age 2.5 years. At the age of 3 years, he transitioned from early intervention services to a preschool at the local school. Within the preschool program, he received special education services, regular sessions with the occupational therapist to promote fine motor development, and services with a speech pathologist to promote speech and language development. Despite these services, his speech was largely unintelligible, so he and his family were taught sign language. At the age of 5 years, he was diagnosed with ADHD by a child psychiatrist. At age 7 he was tested for autism spectrum disorder, but was not diagnosed.
Within a few years, W.S.’s speech had improved sufficiently so that he no longer used sign language, but he continued to receive support for speech and language development, as well as special education services at school and reading services from a reading clinic. Because of agitation and aggression in social environments, he and his family received behavior modification therapy both from home therapy visits and through participation in a behavior clinic. As the young man grew, he continued to receive special education and rehabilitation services. Through middle school he displayed ongoing focus on his internal world, repetitive behaviors, and
___________________
20 Each case is a true account of an individual child with a disability provided by members of the committee for use in this report. Pseudo initials are used to protect confidentiality.
lack of social engagement; therefore, he was reevaluated and diagnosed with autism spectrum disorder.
In high school, in addition to occupational, speech, and autism spectrum services, he began to receive transition services focused on vocational training and independent living. After he completed high school at age 21, he enrolled in a 2-year transition program for individuals with disabilities. Next year, he is expected to graduate from the transition program, and he plans to remain at home and participate in a vocational day program.
Case Study #2
Twin siblings, M. and N., were born prematurely at 26 weeks’ gestation. M.’s birthweight was 1 pound, 13 ounces, while N.’s birthweight was 1 pound, 9 ounces. Both infants required neonatal intensive care for the first 3 months of their lives. Neonatal clinicians recognized that their brain damage was extensive and that their future health and development might be severely compromised. Disability services to help M. and N. were initiated during their stay in the neonatal intensive care unit, starting with physical and occupational therapy services. N., in particular, had feeding difficulties and struggled to make progress. He also developed a seizure disorder and was started on an antiseizure medication soon after birth.
Caregiving for M. and N. was challenging once the infants were discharged from the hospital. Their mother discontinued her employment to take care of them. M. and N. continued with an intensive regimen of early intervention services, including physical, occupational, and speech therapy. Additionally, M. and N. were assigned a developmental specialist to work with them more frequently in hopes of making even the smallest of functional and cognitive gains. During that time, M. and N. had regular appointments with their pediatrician to monitor their growth, as well as other specialists to manage nutrition, vision, spasticity, epilepsy, and orthopedic bracing issues. During this period, the likelihood of long-term disability was becoming evident, as they were not meeting developmental milestones, and the twins received their first wheelchairs. Mobility allowed them to access the world and to take part in their community. They were later diagnosed with severe cerebral palsy spastic quadriplegia.
M. and N. were enrolled in their state Medicaid program because their existing private insurance plan did not cover all of the health services they needed. They were also enrolled in the SSI program. Their family found the SSI financial benefits essential to pay for the substantial out-of-pocket expenses they incurred for health services (such as co-payments for outpatient clinic visits), diapers, and durable medical equipment.
At age 3, M. and N. enrolled in a specialized preschool program for young children with disabilities that offered individualized education plans
and intensive, individualized therapies for children with complex medical and physical needs. As the children grew, they required orthopedic surgeries to repair hip dislocations, spine fusion for scoliosis, and wrist fusion to correct hand deformities. In an effort to manage tone and spasticity, they both received a surgically implanted baclofen pump, which required frequent medication refills.
As M. and N. aged, the family made physical adaptations to their home and vehicle to accommodate the children’s needs. Home modifications included an elevator for wheelchair transition between floors and ceiling lifts in the bedroom and bathroom. These modifications were essential, as M. and N.’s family members became unable to personally transition them among areas. They acquired a full-size van to facilitate the children’s opportunities to integrate into the community. M. and N. joined an amazing challenger baseball team to further enrich their lives.
Eventually, M. and N. were prescribed augmentative communication devices to help overcome their challenges with expressive speech. Medicaid did not cover all of the cost for those expensive devices, so the family used their SSI benefits for this purpose. Using these assistive communication devices, M. and N. began making choices and expressing their thoughts, feelings, and wishes with picture boards. They also learned to use switches to drive their wheelchairs. This brought out their mischievous sides, as they would purposely bump into bushes and walls in school and laugh hysterically. Their communication devices also enabled them to participate in theater productions, and the twins performed in the school auditorium for fellow students and teachers.
When transition services began at age 15, a decision had to be made regarding future residential placement. Although this decision was extremely difficult, M. and N.’s family knew that their children would continue to benefit from the intense therapies they required by living in residential facilities while having recreational activities after school and involvement with peers. This placement was beneficial, especially for speech and language therapy. An augmentative communication device was initiated for both M. and N., which dramatically improved their ability to talk and express their thoughts, feelings, and wishes. During that time, they became proficient at using cellular phones.
Now at age 22, M. and N. are experiencing another transition in which they will attend a disability day program and live in a group home. This experience will optimize their integration with the community and their peers. Already, they are learning to operate a smartphone with communication switches. They have participated in community outings to local malls, where they love to shop for clothes and accessories. They have also attended local sporting and other social events, including a prom. Although M. and N. have severe functional limitations, their disability services have
enabled them to access the community and have an excellent quality of life. Their parents’ hope is for M. and N. to continue the enriching lives to which they have become accustomed throughout adulthood.
Case Study #3
J.P., a 15-year-old adolescent, was first identified as having a disability following a pediatrician visit at 2 years of age and referral for developmental testing. At that time, a general “developmental disability” was identified based on behavioral observation and a parent-completed assessment of his adaptive behavior, which showed significant delays in both communication and cognitive development. As is often the case, weekly home-based services were provided by the state’s early intervention program. At age 3, J.P. was reevaluated and made eligible for services for children with autism, having scored in the autism range on standardized diagnostic assessments. A speech pathologist diagnosed J.P. with a mixed expressive-receptive language disorder.
After J.P.’s third birthday, services transitioned to preschool, and he was placed in a segregated autism program focused on social skills, preacademic abilities, and communication development. The autism program was housed within the local public school and provided services weekdays during the regular school day. Because J.P. had difficulty sitting still and teachers noticed poor impulse control, he was referred to a developmental pediatrician at age 4. The developmental physician diagnosed ADHD of mixed type with high movement and poor impulse control. Strattera, a pharmacological intervention, was prescribed, and both parents and teachers reported improvements in J.P.’s behavior and impulse control. By the end of the school year, however, the medication appeared to be less effective in managing J.P.’s symptoms. When the dose of Strattera was increased, he experienced unwanted side effects, including mood swings and irritability. To address these issues, the Strattera was discontinued, and Risperidone therapy was initiated. Within a short time, however, the Risperidone was discontinued because of worsening of J.P.’s irritability and agitation.
At transition to kindergarten, J.P. was eligible for services under the categories of “other health impaired” and “autism spectrum disorder.” He continued in a self-contained classroom for autism, with the addition of a behavioral specialist to address the symptoms of ADHD. In addition to the academic program, speech pathology, occupational therapy, and special education resources for reading and math were provided as part of his IEP. These services continued, and during primary school, J.P. gradually transitioned from a full-time self-contained autism classroom to partial integration into a general education classroom for selected subjects, which initially included music, art, and recess. According to parent and teacher
reports, he transitioned well and was integrated approximately 50 percent of the day by the time he started middle school.
Communication intervention for J.P. focused increasingly on conversational social skills in addition to vocabulary and syntax. Because his speech was largely intelligible with few errors, the speech therapy focused on reading-phonics and sound-symbol associations. He did learn to read, but was consistently two to three grade levels below what would be predicted by his age. For this reason, “learning disability” was added to the “other health impaired” (ADHD) and “autism spectrum” defining his special education eligibility. Although this made sense from a programmatic standpoint in terms of the special education support he was receiving, it was rather confusing to the parents, who were not quite sure what his “diagnosis” should be other than ADHD. Several times, the school and the family physician suggested once again attempting medication to treat the ADHD, but the parents chose to continue the behavior management rather than reintroduce Strattera or another ADHD medication.
Currently, J.P. is due to enter high school with a modified IEP that includes time in both a self-contained and general classroom. The ratio of self-contained classroom time to regular education time is planned to decrease over a 2-year period. In addition, a vocational-transition education plan has been included in the high school program. Support services for J.P. continue to include speech pathology, occupational therapy, resource-learning disability support, and special education-academics. In addition, vocational rehabilitation will be added to the IEP services.
Discussion
As these cases illustrate, the services needed by children with disabilities and their families are multiple, complex, and evolving. Furthermore, although the types of services and the means of service delivery change over time, the needs they address often do not go away. It is important to note that each transition described in these examples required families to become familiar with new application procedures, services, regulations, expectations for their role, and personnel, as well as to deal with ambiguity in what could and should be provided. Often there exists no external mechanism for integration of services provided by different care silos (e.g., medical care, educational supports, and community programs), leaving parents to effect this coordination on their own. The coordination achieved can also be quite fragile: A change in service personnel, program philosophy, or physical location or some other event may disrupt communication, tailored support plans, or available services, leaving the family to undertake a rebuilding process for which they may or may not feel well prepared. Such rebuilding requires time and skill and involves learning
about options, applying for benefits, seeking providers, and implementing and monitoring a plan.
SUMMARY
Childhood disability is not addressed using consistent nosologies or terms by researchers, government agencies, families, health care providers, and educators. Nonetheless, the data suggest that a large and growing number of U.S. children have disabilities. A shift has also occurred from a preponderance of disabilities related to physical conditions that directly threaten survival to a preponderance of mental and neurodevelopmental conditions. Moreover, most current data fail to access and record the true impact of comorbid conditions, although this is clearly a factor affecting the identification and management of disability. Disabilities have extensive impacts on affected children and negatively affect the child’s family, the community, and society in general.
Fragmentation of the services for children with disabilities places a heavy burden on families that need to access and coordinate these services, especially when the family needs to learn not only about the best medical treatment for the child’s condition but also about the other resources required to optimize the child’s health and development. These tasks are challenging for even the most well-resourced, capable, health-literate, and organized families, and are truly daunting for those with less stability in their lives and fewer personal resources. Necessary services also change as children with disabilities age, which requires new skills to move through various states of childhood to young adulthood. Service needs are complex, influenced by multiple individual, family, environmental, and systems factors. This complexity highlights the challenges the committee faced in addressing its statement of task (Box 1-1 in Chapter 1), but also emphasizes the much larger problem the nation faces in addressing the needs of children with disabilities, especially for families living in poverty.
REFERENCES
AAP (American Academy of Pediatrics). 2004. Improving mental health services in primary care: Reducing administrative and financial barriers to access and collaboration. https://www.aap.org/en-us/advocacy-and-policy/aap-health-initiatives/Mental-Health/Documents/white_paper_background.pdf (accessed December 11, 2017).
Algood, C. L., C. Harris, and J. S. Hong. 2013. Parenting success and challenges for families of children with disabilities: An ecological systems analysis. Journal of Human Behavior in the Social Environment 23(2):126–136.
Alwin, D. 2012. Integrating varieties of life course concepts. The Journals of Gerontology: Series B 67(2):206–220.
Ananth, P., P. Melvin, C. Feudtner, J. Wolfe, and J. G. Berry. 2015. Hospital use in the last year of life for children with life-threatening complex chronic conditions. Pediatrics 136(5):938–946.
Anderson, D. K., J. W. Liang, and C. Lord. 2014. Predicting young adult outcome among more and less cognitively able individuals with autism spectrum disorders. Journal of Child Psychology and Psychiatry 55(5):485–494.
Aron, L. Y., P. J. Loprest, and I. Urban. 2007. Meeting the needs of children with disabilities. Washington, DC: Urban Institute Press.
Bal, V. H., S.-H. Kim, D. Cheong, and C. Lord. 2015. Daily living skills in individuals with autism spectrum disorder from 2 to 21 years of age. Autism 19(7):774–784.
Balderian, N. 1991. Sexual abuse of people with developmental disabilities. Sexuality and Disability 9(4):323–335.
Bauman, L. J., E. J. Silver, and R. E. Stein. 2006. Cumulative social disadvantage and child health. Pediatrics 117(4):1321–1328.
BCH (Boston Children’s Hospital). 2009. For very young, cochlear implants can make a huge impact. Thriving: Boston Children’s Hospital’s Pediatric Health Blog, August 17. https://thriving.childrenshospital.org/for-very-young-cochlear-implants-can-make-a-huge-impact (accessed January 27, 2018).
BCH. n.d. Bullying in children. http://www.childrenshospital.org/conditions-and-treatments/conditions/bullying# (accessed January 27, 2018).
Berry, J. G., D. A. Graham, R. J. Graham, J. Zhou, H. L. Putney, J. E. O’Brien, D. W. Roberson, and D. A. Goldmann. 2009. Predictors of clinical outcomes and hospital resource use of children after tracheotomy. Pediatrics 124(2):563–572.
Berry, J. G., R. Agrawal, D. Z. Kuo, E. Cohen, W. Risko, M. Hall, P. Casey, J. Gordon, and R. Srivastava. 2011a. Characteristics of hospitalizations for patients who use a structured clinical care program for children with medical complexity. The Journal of Pediatrics 159(2):284–290.
Berry, J. G., D. E. Hall, D. Z. Kuo, E. Cohen, R. Agrawal, C. Feudtner, M. Hall, J. Kueser, W. Kaplan, and J. Neff. 2011b. Hospital utilization and characteristics of patients experiencing recurrent readmissions within children’s hospitals. Journal of the American Medical Association 305(7):682–690.
Berry, J. G., M. Hall, D. E. Hall, D. Z. Kuo, E. Cohen, R. Agrawal, K. D. Mandl, H. Clifton, and J. Neff. 2013. Inpatient growth and resource use in 28 children’s hospitals: A longitudinal, multi-institutional study. JAMA Pediatrics 167(2):170–177.
Boothroyd, R. A., and M. I. Armstrong. 2005. Comorbidity and unmet service needs among Medicaid-enrolled children with identified disabilities. Journal of Emotional and Behavioral Disorders 1(1):43–51.
Bourke-Taylor, H., L. Howie, and M. Law. 2010. Impact of caring for a school-aged child with a disability: Understanding mothers’ perspectives. Australian Occupational Therapy Journal 57(2):127–136.
Brooks-Gunn, J., and G. J. Duncan. 1997. The effects of poverty on children. The Future of Children 7(2):55–71.
Bullis, M., and P. Yovanoff. 2005. More alike than different? Comparison of formerly incarcerated youth with and without disabilities. Journal of Child and Family Studies 14(1):127–139.
Burns, K. H., P. H. Casey, R. E. Lyle, T. M. Bird, J. J. Fussell, and J. M. Robbins. 2010. Increasing prevalence of medically complex children in U.S. hospitals. Pediatrics 126(4): 638–646.
Carter, B. B., and V. G. Spencer. 2006. The fear factor: Bullying and students with disabilities. International Journal of Special Education 21(1):11–23.
Cavendish, W. 2014. Academic attainment during commitment and postrelease education-related outcomes of juvenile justice-involved youth with and without disabilities. Journal of Emotional and Behavioral Disorders 22(1):41–52.
CDC (Centers for Disease Control and Prevention). 2010. Summary health statistics for U.S. children: National Health Interview Survey 2009. https://www.cdc.gov/nchs/data/series/sr_10/sr10_247.pdf (accessed March 6, 2018).
CDC. 2017a. About the National Health Interview Survey. https://www.cdc.gov/nchs/nhis/about_nhis.htm (accessed March 5, 2018).
CDC. 2017b. Disability overview. https://www.cdc.gov/ncbddd/disabilityandhealth/disability.html (accessed January 27, 2018).
Child Trends. 2014. Children with limitations: Indicators of child and youth well-being. Bethesda, MD: Child Trends Data Bank.
Cohen, E., D. Z. Kuo, R. Agrawal, J. G. Berry, S. K. Bhagat, T. D. Simon, and R. Srivastava. 2011. Children with medical complexity: An emerging population for clinical and research initiatives. Pediatrics 127(3):529–538.
Combs-Orme, T., C. A. Heflinger, and C. G. Simpkins. 2002. Comorbidity of mental health problems and chronic health conditions in children. Journal of Emotional and Behavioral Disorders 10(2):116–125.
Corrigan, P. W., L. P. River, R. K. Lundin, D. L. Penn, K. Uphoff-Wasowski, J. Campion, J. Mathisen, C. Gagnon, M. Bergman, H. Goldstein, and M. A. Kubiak. 2001. Three strategies for changing attributions about severe mental illness. Schizophrenia Bulletin 27(2):187–195.
Courtney, M. E., S. Terao, and N. Bost. 2004. Midwest evaluation of the adult functioning of former foster youth: Conditions of youth preparing to leave state care. Chicago, IL: Chapin Hall Center for Children at The University of Chicago.
Dalvand, H., S. A. Hosseini, M. Rassafiani, S. A. Samadi, H. R. Khankeh, and G. Kelly. 2015. Cooccupations: The caregiving challenges of mothers of children with cerebral palsy. British Journal of Occupational Therapy 78(7):450–459.
Davis, M., A. J. Sheidow, K. Zajac, and M. McCart. 2012. Prevalence and impact of substance use among emerging adults with serious mental health conditions. Psychiatric Rehabilitation Journal 35(3):235–243.
Dodgson, J. E., A. Garwick, S. A. Blozis, J. M. Patterson, F. C. Bennett, and R. W. Blum. 2000. Uncertainty in childhood chronic conditions and family distress in families of young children. Journal of Family Nursing 6(3):252–266.
DOJ (U.S. Department of Justice). 2000. Enforcement of Title VI of the Civil Rights Act of 1964—National origin discrimination against persons with limited English proficiency; notice. https://www.justice.gov/sites/default/files/crt/legacy/2010/12/14/eolep.pdf (accessed April 9, 2018).
ED (U.S. Department of Education). 2013. Part B of the Individuals with Disabilities Education Act notice of proposed rulemaking: Final regulations. https://www.gpo.gov/fdsys/pkg/FR-2013-02-14/pdf/2013-03443.pdf (accessed January 27, 2017).
ED. 2014. Bullying of students addressed in guidelines to America’s schools. https://www.ed.gov/news/press-releases/bullying-students-disabilities-addressed-guidance-america%E2%80%99s-schools (accessed January 9, 2017).
Elder, G. 2000. The life course and aging: Some reflections. 1999, August 10 Distinguished Scholar Lecture, Section on Aging and Life Course, Annual Meetings of the American Sociological Association. http://www.jstor.org.proxyiub.uits.iu.edu/stable/pdf/1132065.pdf?refreqid=excelsior:60ae91b4f94ddbc7191567bc6ea2427d (accessed April 10, 2018).
Escalona, S. K. 1982. Babies at double hazard: Early development of infants at biologic and social risk. Pediatrics 70(5):670–676.
Evans, G. W. 2004. The environment of childhood poverty. The American Psychologist 59(2):77–92.
Fleming, J., M. Challela, J. Eland, R. Hornick, P. Johnson, I. Martinson, D. Nativio, K. Nokes, I. Riddle, and N. Steele. 1994. Impact on the family of children who are technology dependent and cared for in the home. Pediatric Nursing 20(4):379–388.
Franklin, D. 2005. Perception of mental illness stigma varies with age, gender. Family Practice News, April 15. https://www.mdedge.com/familypracticenews/article/25431/mental-health/perception-mental-illness-stigma-varies-age-gender (accessed April 10, 2018).
Gibson, M. J., K. A. Kelly, and A. K. Kaplan. 2012. Family caregiving and transitional care: A critical review. San Francisco, CA: Family Caregiver Alliance.
Goffman, E. 1986. Stigma: Notes on the management of spoiled identity. New York: Touchstone Publishing.
Gorzkowski, J., E. H. Kelly, S. J. Klaas, and L. C. Vogel. 2011. Obstacles to community participation among youth with spinal cord injury. The Journal of Spinal Cord Medicine 34(6):576–585.
Green, S. E. 2007. “We’re tired, not sad”: Benefits and burdens of mothering a child with a disability. Social Science and Medicine 64(1):150–163. doi:10.1016/j.socscimed.2006.08.025.
Halfon, N., A. Houtrow, K. Larson, and P. W. Newacheck. 2012. The changing landscape of disability in childhood. Future of Children 22(1):13–42.
Halfon, N., K. Larson, M. Lu, E. Tullis, and S. Russ. 2014a. Lifecourse health development: Past, present and future. Maternal and Child Health Journal 18(2):344–365.
Halfon, N., P. H. Wise, and C. B. Forrest. 2014b. The changing nature of children’s health development: New challenges require major policy solutions. Health Affairs (Millwood) 33(12):2116–2124.
Harris, B. H., G. Hendershot, and D. C. Stapleton. 2005. A guide to disability statistics from the National Health Interview Survey. Ithaca, NY: Cornell University, Rehabilitation Research and Training Center on Disability Demographics and Statistics.
Harwood, R., S. Yu, and L. Kavanagh. n.d. Remembering our past, building the future: 100 years of the Maternal and Child Health Research Program. Rockville, MD: Maternal and Child Health Bureau. https://mchb.hrsa.gov/research/about-history.asp (accessed January 27, 2018).
Heflinger, C. A., K. A. Wallston, A. Mukolo, and A. M. Brannan. 2014. Perceived stigma toward children with emotional and behavioral problems and their families: The Attitudes About Child Mental Health Questionnaire (ACMHQ). Journal of Rural Mental Health 38(1):9–19.
HHS (U.S. Department of Health and Human Services). 2000. Report of the Surgeon General’s conference on children’s mental health: A national action agenda. Washington, DC: HHS.
Houtrow, A. J., M. J. Okumura, J. F. Hilton, and R. S. Rehm. 2011. Profiling health and health-related services for children with special health care needs with and without disabilities. Academic Pediatrics 11(6):508–516.
Houtrow, A., J. Jones, R. Ghandour, B. Strickland, and P. Newacheck. 2012. Participation of children with special health care needs in school and the community. Academic Pediatrics 12(4):326–334.
Houtrow, A. J., K. Larson, L. M. Olson, P. W. Newacheck, and N. Halfon. 2014. Changing trends of childhood disability, 2001–2011. Pediatrics 134(3):530–538.
Hysing, M., I. Elgen, C. Gillberg, and A. J. Lundervold. 2009. Emotional and behavioral problems in subgroups of children with chronic illness: Results from a large-scale population study. Child Care Health Development 35(4):527–533.
Ireys, H. T., G. F. Anderson, T. J. Shaffer, and J. M. Neff. 1997. Expenditures for care of children with chronic illnesses enrolled in the Washington State Medicaid program, fiscal year 1993. Pediatrics 100(2):197–204.
Johnston, L. D., P. M. O’Malley, J. G. Bachman, and J. E. Schulenberg. 2004. Monitoring the future national survey results on drug use, 1975–2003. Rockville, MD: National Institute on Drug Abuse.
Jonson-Reid, M., B. Drake, J. Kim, S. Porterfield, and L. Han. 2004. A prospective analysis of the relationship between reported child maltreatment and special education eligibility among poor children. Child Maltreatment 9(4):382–394.
Kelleher, K. J., J. L. Taylor, and V. I. Rickert. 1992. Mental health services for rural children and adolescents. Clinical Psychology Review 12(8):841–852.
Kessler, R. C., G. P. Amminger, S. Aguilar-Gaxiola, J. Alonso, S. Lee, and T. B. Ustun. 2007. Age of onset of mental disorders: A review of recent literature. Current Opinions in Psychiatry 20(4):359–364.
Kids Count Data Center. 2013. 2013 Kids Count data book. Baltimore, MD: The Annie E. Casey Foundation. https://datacenter.kidscount.org/files/2013KIDSCOUNTDataBook.pdf (accessed April 9, 2018).
King, G., M. A. Tucker, P. Baldwin, K. Lowry, J. Laporta, and L. Martens. 2002. A life needs model of pediatric service delivery services to support community participation and quality of life for children and youth with disabilities. Physical & Occupational Therapy in Pediatrics 22(2):53–77.
Kirk, S. 2001. Negotiating lay and professional roles in the care of children with complex health care needs. Journal of Advanced Nursing 34(5):593–602.
Kogan, M. D., S. J. Blumberg, L. A. Schieve, C. A. Boyle, J. M. Perrin, R. M. Ghandour, G. K. Singh, B. B. Strickland, E. Trevathan, and P. C. van Dyck. 2009. Prevalence of parent-reported diagnosis of Autism Spectrum Disorder among children in the U.S. in 2007. Pediatrics 124(5):1395–1403.
Kuhlthau, K. A., and J. M. Perrin. 2001. Child health status and parental employment. Archives of Pediatrics & Adolescent Medicine 155(12):1346–1350.
Lalvani, P. 2015. Disability, stigma and otherness: Perspectives of parents and teachers. International Journal of Disability, Development and Education 62(4):379–393.
Lansford, J. E., K. A. Dodge, G. S. Pettit, J. E. Bates, J. Crozier, and J. Kaplow. 2002. A 12-year prospective study of the long-term effects of early child physical maltreatment on psychological, behavioral, and academic problems in adolescence. Archives of Pediatrics & Adolescent Medicine 156(8):824–830.
Leslie, L. K., J. Weckerly, J. Landsverk, R. L. Hough, M. S. Hurlburt, and P. A. Wood. 2003. Racial/ethnic differences in the use of psychotropic medication in high-risk children and adolescents. Journal of the American Academy of Child & Adolescent Psychiatry 42(12):1433–1442.
Lind, C. 2014. Care mapping. https://durgastoolbox.com/caremapping (accessed April 10, 2018).
Luckasson, R., D. Coulter, E. Polloway, S. Reiss, R. Schalock, M. Snell, D. Spitalnik, and J. Stark. 1992. Mental retardation: Definition, classification, and systems of support, 9th ed. Washington, DC: American Association on Mental Retardation.
Luckasson, R., S. Borthwick-Duffy, W. Buntinx, D. L. Coulter, E. M. Pat Craig, A. Reeve, R. L. Schalock, M. E. Snell, D. M. Spitalnik, S. Spreat, and M. J. Tasse. 2002. Mental retardation: Definition, classification, and systems of supports, 10th ed. Washington, DC: American Association on Mental Retardation.
Lustig, D. C., and D. R. Strauser. 2007. Causal relationships between poverty and disability. Rehabilitation Counseling Bulletin 50(4):194–202.
Magaña, S., S. L. Parish, R. A. Rose, M. Timberlake, and J. G. Swaine. 2012. Racial and ethnic disparities in quality of health care among children with autism and other developmental disabilities. Intellectual and Developmental Disabilities 50(4):287–299.
Mandell, D. S., L. D. Wiggins, L. A. Carpenter, J. Daniels, C. DiGuiseppi, M. S. Durkin, E. Giarelli, M. J. Morrier, J. S. Nicholas, J. A. Pinto-Martin, P. T. Shattuck, K. C. Thomas, M. Yeargin-Allsopp, and R. S. Kirby. 2009. Racial/ethnic disparities in the identification of children with Autism Spectrum Disorders. American Journal of Public Health 99(3):493–498.
Mallett, C. A. 2009. Disparate juvenile court outcomes for disabled delinquent youth: A social work call to action. Child and Adolescent Social Work Journal 26(3):197–207.
MCHB (Maternal and Child Health Bureau). 2013. The National Survey of Children with Special Health Care Needs Chartbook 2009–2010. Rockville, MD: Health Resources and Services Administration, MCHB. https://mchb.hrsa.gov/cshcn0910/more/pdf/nscshcn0910.pdf (accessed April 10, 2018).
McPherson, M., P. Arango, H. Fox, C. Lauver, M. McManus, P. W. Newacheck, J. M. Perrin, J. P. Shonkoff, and B. Strickland. 1998. A new definition of children with special health care needs. Pediatrics 102(1):137–140.
Merikangas, K. R., J.-P. He, M. Burstein, S. A. Swanson, S. Avenevoli, L. Cui, C. Benjet, K. Georgiades, and J. Swendsen. 2010. Lifetime prevalence of mental disorders in U.S. adolescents: Results from the National Comorbidity Survey Replication-Adolescent Supplement (NCS-A). Journal of the American Academy of Child & Adolescent Psychiatry 49(10):980–989.
Merikangas, K. R., M. E. Calkins, M. Burstein, J.-P. He, R. Chiavacci, T. Lateef, K. Ruparel, R. C. Gur, T. Lehner, H. Hakonarson, and R. E. Gur. 2015. Comorbidity of physical and mental disorders in the neurodevelopmental genomics cohort study. Pediatrics 135(4):e927.
Mulvihill, B. A., M. S. Wingate, M. Altarac, F. X. Mulvihill, D. T. Redden, J. Telfair, M. A. Pass, and D. E. Ellis. 2005. The association of child condition severity with family functioning and relationship with health care providers among children and youth with special health care needs in Alabama. Journal of Maternal and Child Health 9(2):S87–S97.
NASEM (National Academies of Sciences, Engineering, and Medicine). 2015. Mental disorders and disabilities among low-income children. Washington, DC: The National Academies Press.
NASEM. 2016. Speech and language disorders in children: Implications for the Social Security Administration’s Supplemental Security Income program. Washington, DC: The National Academies Press.
NCSER (National Council for Special Education Research). 2010. The post-high school outcomes for youth with disabilities up to 4 years after high school. https://ies.ed.gov/ncser/pubs/20093017 (accessed January 27, 2018).
Nelson, A. M. 2002. A metasynthesis: Mothering other-than-normal children. Qualitative Health Research 12(4):515–530.
Neuman, M. I., E. R. Alpern, M. Hall, A. B. Kharbanda, S. S. Shah, S. B. Freedman, P. L. Aronson, T. A. Florin, R. D. Mistry, and J. G. Berry. 2014. Characteristics of recurrent utilization in pediatric emergency departments. Pediatrics 134(4):1025–1031.
Newacheck, P. W., M. McManus, H. B. Fox, Y. Y. Hung, and N. Halfon. 2000. Access to health care for children with special health care needs. Pediatrics 105(4):760–766.
Newacheck, P. W., M. Inkelas, and S. E. Kim. 2004. Health services use and health care expenditures for children with disabilities. Pediatrics 114(1):79–85.
NHANES (National Health and Nutrition Examination Survey). 2012. National Health and Nutrition Examination Survey 2011–2012. https://wwwn.cdc.gov/nchs/nhanes/ContinuousNhanes/Default.aspx?BeginYear=2011 (accessed December 11, 2017).
Nicolais, C. J., P. B. Perrin, I. Panyavin, E. G. Nicholls, S. L. A. Plaza, L. M. Quintero, and J. C. Arango-Lasprilla. 2016. Family dynamics and psychosocial functioning in children with SCI/D from Colombia, South America. The Journal of Spinal Cord Medicine 39(1):58–66.
NIDA (National Institute on Drug Abuse). 2014. Behavioral health trends in the United States: Results from the 2014 National Survey on Drug Use and Health. https://www.samhsa.gov/data/sites/default/files/NSDUH-FRR1-2014/NSDUH-FRR1-2014.pdf (accessed December 11, 2017).
NRC (National Research Council) and IOM (Institute of Medicine). 2004. Children’s health, the nation’s wealth: Assessing and improving child health. Washington, DC: The National Academies Press.
NS-CSHCN (National Survey of Children with Special Health Care Needs). 2009–2010. NS-CSHCN Chartbook 2009–2010. https://mchb.hrsa.gov/cshcn0910/index.html (accessed January 27, 2018).
ODODD (Ohio Department of Developmental Disabilities). 2014. Human trafficking of individuals with disabilities. Columbus, OH: ODODD.
Okumura, M. J., A. Houtrow, J. Van Cleave, and S. Gnanasekaran. 2009. Understanding factors associated with work loss for families caring for CSHCN. Pediatrics 124(Suppl. 4):S392–S398.
OSERS (Office of Special Education Research). 2013. Dear colleague letter. Washington, DC: ED.
OVC (Office for Victims of Crime). n.d. Victims with physical, cognitive, or emotional disabilities. Washington, DC: Office of Justice Programs.
Peters, C. P. 2005. Children with special health care needs: Minding the gaps. Washington, DC: George Washington University, National Health Policy Forum. http://www.nhpf.org/library/background-papers/BP_CSHCN_06-27-05.pdf (accessed December 11, 2017).
Pulcini, C. D., B. Zima, K. Kelleher, and A. Houtrow. 2017. Poverty and trends in three common chronic disorders. Pediatrics 139(3):e20162539.
Quinn, M. M., R. B. Rutherford, P. E. Leone, D. M. Osher, and J. M. Poirier. 2005. Youth with disabilities in juvenile corrections: A national survey. Exceptional Children 71(3):339–345.
Rehm, R. S., and J. F. Bradley. 2005. The search for social safety and comfort in families raising children with complex chronic conditions. Journal of Family Nursing 11(1):59–78.
Reichman, N. E., H. Corman, and K. Noonan. 2008. Impact of child disability on the family. Maternal and Child Health Journal 12(6):679–683.
Robinson, L. R., J. R. Holbrooke, R. H. Bitsko, S. A. Hartwig, J. W. Kaminski, R. M. Ghandour, G. Peacock, A. Heggs, and C. A. Boyle. 2017. Differences in health care, family, and community factors associated with mental, behavioral, and developmental disorders among children aged 2–8 years in rural and urban areas—United States, 2011–2012. Atlanta, GA: CDC.
Romig, K. 2017. SSA: A lifeline for children with disabilities. Washington, DC: Center for Budget and Policy Priorities. https://www.cbpp.org/research/social-security/ssi-a-lifeline-for-children-with-disabilities (accessed April 9, 2017).
Romley, J. A., A. K. Shah, P. J. Chung, M. N. Elliott, K. D. Vestal, and M. A. Schuster. 2017. Family-provided health care for children with special health care needs. Pediatrics 139(1):e20161287.
SAMHSA (Substance Abuse and Mental Health Services Administration). 2003. Overview of findings from the 2002 National Survey on Drug Use and Health. Rockville, MD: SAMHSA.
SAMHSA. 2010. Results from the 2009 National Survey on Drug Use and Health: Volume I. Summary of National Findings. Rockville, MD: SAMHSA.
SAMHSA. 2011. Substance use disorders in people with physical and sensory disabilities. Rockville, MD: SAMHSA.
SAMHSA. 2017. Key substance use and mental health indicators in the United States: Results from the 2016 National Survey on Drug Use and Health. Rockville, MD: SAMHSA.
Schalock, R. L., S. Borthwick-Duffy, V. Bradley, W. H. E. Buntinx, D. Coulter, E. (Pat) Craig, S. Gomez, Y. Lachapelle, R. Luckasson, A. Reeve, K. Shogren, M. E. Snell, S. Spreat, M. J. Tassé, J. R. Thompson, M. A. Verdugo-Alonso, M. L. Wehmeyer, and M. H. Yeager. 2010. Intellectual disability: Definition, classification, and systems of support, 11th ed. Washington, DC: American Association on Intellectual and Developmental Disabilities.
Schulte-Körne, G. 2016. Mental health problems in a school setting in children and adolescents. Deutsches Ärzteblatt International 113(11):183.
Simon, T. D., J. Berry, C. Feudtner, B. L. Stone, X. Sheng, S. L. Bratton, J. M. Dean, and R. Srivastava. 2010. Children with complex chronic conditions in inpatient hospital settings in the United States. Pediatrics 126(4):647–655.
Smith, N., and S. Harrell. 2013. Sexual abuse of children with disabilities: A national snapshot. http://www.azcadv.org/azcadv2014wp/wp-content/uploads/2014/06/Sexual-Abuse-of-Children-with-Disabilities-A-National-Snapshot.pdf (accessed April 8, 2018).
Smits, D.-W., M. Ketelaar, J. W. Gorter, P. van Schie, A. Dallmeijer, M. Jongmans, and E. Lindeman. 2011. Development of daily activities in school-age children with cerebral palsy. Research in Developmental Disabilities 32(1):222–234.
Spencer, N., E. Devereux, A. Wallace, R. Sundrum, M. Shenoy, C. Bacchus, and S. Logan. 2005. Disabling conditions and registration for child abuse and neglect: A population-based study. Pediatrics 116(3):609–613.
SSA (Social Security Administration). 2016. Childhood disability: Supplemental Security Income Program. https://www.ssa.gov/disability/professionals/childhoodssi-pub049.htm (accessed January 27, 2018).
SSA. 2017a. Disability evaluation under Social Security. https://www.ssa.gov/disability/professionals/bluebook/general-info.htm (accessed January 27, 2018).
SSA. 2017b. SSI Annual Statistical Report, 2016. https://www.ssa.gov/policy/docs/statcomps/ssi_asr/2016/sect04.html#table20 (accessed April 23, 2018).
Stanton-Chapman, T. L., D. A. Chapman, A. P. Kaiser, and T. B. Hancock. 2004. Cumulative risk and low-income children’s language development. Topics in Early Childhood Special Education 24(4):227–237.
Stein, M. A. 2007. A quick overview of the United Nations Convention on the Rights of Persons with Disabilities and its implications for Americans with disabilities. Mental and Physical Disability Law Reporter 31(5):679–683.
Stein, R. E., and E. J. Silver. 2003. Patterns of medical, educational, and mental health service use in a national sample of U.S. children. Ambulatory Pediatrics: The Official Journal of the Ambulatory Pediatric Association 3(2):87–92.
Stein, R. E., M. J. Siegel, and L. J. Bauman. 2010. Double jeopardy: What social risk adds to biomedical risk in understanding child health and health care utilization. Academic Pediatrics 10(3):165–171.
stopbullying.gov. n.d. What is bullying? https://www.stopbullying.gov/what-is-bullying/index.html (accessed December 1, 2017).
Storch, E. A., M. J. Larson, J. Ehrenreich-May, E. B. Arnold, A. M. Jones, P. Renno, C. Fuji, A. B. Lewin, P. J. Mutch, T. K. Murphy, and J. J. Wood. 2012. Peer victimization in youth with autism spectrum disorders and co-occurring anxiety: Relations with psychopathology and loneliness. Journal of Developmental and Physical Disabilities 24(6):575–590.
Sullivan, P. M., and J. F. Knutson. 2000. Maltreatment and disabilities: A population-based epidemiological study. Child Abuse and Neglect 24(10):1257–1273.
Teplin, L., L. Welty, K. Abram, M. Dulcan, J. Washburn, K. McCoy, and M. Stokes. 2015. Psychiatric disorders in youth after detention. Washington, DC: U.S. Department of Justice. https://www.ojjdp.gov/pubs/246824.pdf (accessed December 11, 2017).
Thyen, U., K. Kuhlthau, and J. M. Perrin. 1999. Employment, child care, and mental health of mothers caring for children assisted by technology. Pediatrics 103(6):1235–1242.
Traustadottir, R. 1991. Mothers who care: Gender, disability, and family life. Journal of Family Issues 12(2):211–228.
Twyman, K. A., C. F. Saylor, D. Saia, M. M. Macias, L. A. Taylor, and E. Spratt. 2010. Bullying and ostracism experiences in children with special health care needs. Journal of Developmental & Behavioral Pediatrics 31(1):1–8.
UNICEF (United Nations Children’s Fund). 2013. Children and young people with disabilities. https://www.unicef.org/pacificislands/UNI137485(1).pdf (accessed January 27, 2018).
U.S. Census Bureau. 2016. American Community Survey 5-year data: 2009–2016. Washington, DC: U.S. Census Bureau. https://www.census.gov/data/developers/data-sets/acs-5year.html (accessed March 6, 2018).
Van Cleave, J., S. L. Gortmaker, and J. M. Perrin. 2010. Dynamics of obesity and chronic health conditions among children and youth. Journal of the American Medical Association 303(7):623–630.
van Duijn, G., Y. Dijkxhoorn, E. Scholte, and V. Berckelaer-Onnes. 2010. The development of adaptive skills in young people with Down syndrome. Journal of Intellectual Disability Research 54(11):943–954.
Vijayaraghavan, M., E. A. Jacobs, H. Seligman, and A. Fernandez. 2011. The association between housing instability, food insecurity, and diabetes self-efficacy in low-income adults. Journal of Health Care for the Poor and Underserved 22(4):1279–1291.
Wells, T., and D. Hogan. 2003. Developing concise measures of childhood activity limitations. Maternal and Child Health Journal 7(2):115–126.
WHO (World Health Organization). 2001. International Classification of Functioning, Disability and Health. Geneva, Switzerland: WHO.
Wiener, J., and M. Mak. 2009. Peer victimization in children with attention-deficit/hyperactivity disorder. Psychology in the Schools 46(2):116–131.
Woolf, S., C. M. Woolf, and T. Oakland. 2010. Adaptive behavior among adults with intellectual disabilities and its relationship to community independence. Intellectual and Developmental Disabilities 48(3):209–215.
Zuckerman, K. E., O. J. Lindly, C. D. Bethell, and K. Kuhlthau. 2014. Family impacts among children with autism spectrum disorder: The role of health care quality. Academic Pediatrics 14(4):398–407.
This page intentionally left blank.












































