
Summary1
In 2015, building on the advances of the Millennium Development Goals (MDGs), the United Nations declared a second global revolution based on the Sustainable Development Goals (SDGs), which were adopted by 193 countries. The SDGs include an explicit commitment to achieving universal health coverage (UHC) by 2030 “so that all people and communities receive the quality services they need, and are protected from health threats, without suffering financial hardship.” Accordingly, UHC is the central theme of global health policy today. Yet, the evidence is clear: Even if the movement toward UHC succeeds, billions of people will have access to care of such low quality that it will not help them, and indeed often will harm them. While the tremendous gains made against the burden of illness, injury, and disability in recent years warrant celebration, these gains and the new commitment to UHC are not sufficient to close the enormous gaps that remain between what is achievable in human health and where global health stands today, and progress has been both incomplete and unevenly distributed. Thus, without a deliberate and comprehensive effort to improve
___________________
1 This summary does not include references. Citations to support the text and conclusions herein are provided in the body of the report.
the quality of health care services globally, UHC will too often prove to be an empty vessel.
This report focuses on one particular shortfall in health care affecting global populations: defects in the quality of care. The committee tasked with conducting this study set out to review the available evidence on the quality of care worldwide, with a special focus on low-resource areas. The evidence demonstrates that, even when care is available, quality problems are widespread and take many forms. For example, a study in China, India, and Kenya found that providers adhered to evidence-based treatment for such conditions as asthma, chest pain, diarrhea, and tuberculosis only 25 to 50 percent of the time. Thus, patients who visited a clinician for these common, simple conditions in those settings often had less than a one in two chance of being helped by that encounter. Even though the knowledge for proper treatment exists, providers are not reliably absorbing and using it for the right patients at the right time.
High levels of inappropriate care are also pervasive. For example, a World Health Organization (WHO) report on overuse of ineffective care states that more than 6 million excess caesarean sections are performed every year (50 percent of which occur in China and Brazil). Another example—the high rate of inappropriate use of antibiotics—not only is harmful and costly to patients but also is an important contributor to the global scourge of antimicrobial resistance. In the United States, 30 percent of estimated prescriptions for antibiotics are found to be unnecessary. Worldwide, moreover, the journeys of patients and their families through the health care system are fragmented and difficult to navigate, and in some cases can constitute such a negative experience that it deters them from interacting with the system in the future.
THE DIRE STATE OF HEALTH CARE QUALITY
Health care in all global settings today suffers from high levels of defects in quality across many domains, and this poor-quality care causes ongoing damage to human health. Hospitalizations in low- and middle-income countries (LMICs) lead to 134 million adverse events each year, and these adverse events contribute to more than 2.5 million deaths annually. More than 830 million people with a diagnosed noncommunicable disease (NCD) are not being treated, and more than 4 million avoidable quality-related deaths each year are attributable to ineffective care for NCDs. In total, between 5.7 and 8.4 million deaths occur annually from poor quality of care in LMICs for the selected set of conditions the committee analyzed (see Figure S-1), which represents between 10 and 15 percent of the total deaths in LMICs reported by WHO in 2015. For some conditions, deaths due to poor quality contribute to more than half of overall deaths.
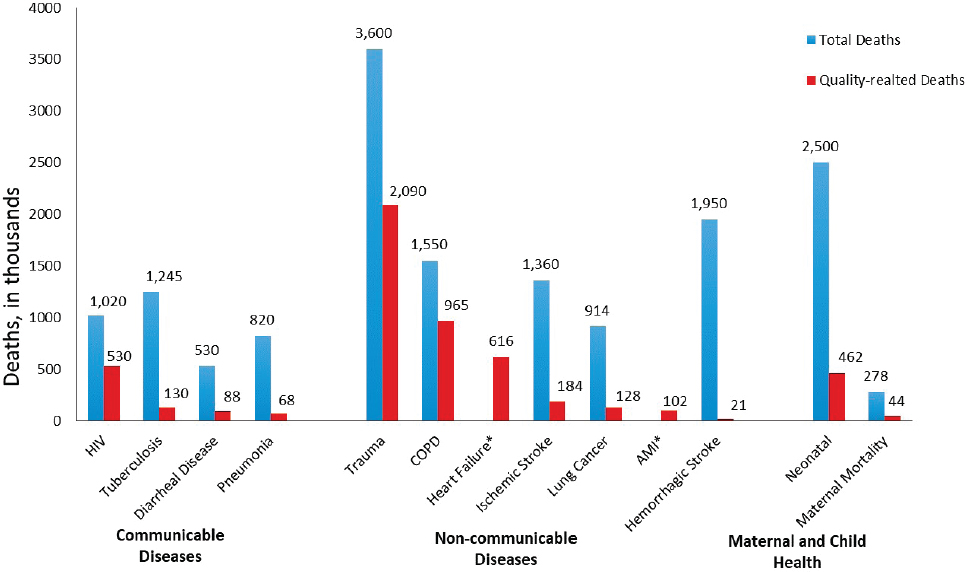
* Total deaths unavailable.
NOTE: AMI = acute myocardial infarction; COPD = chronic obstructive pulmonary disorder; HIV = human immunodeficiency virus.
SOURCE: Institute for Health Metrics and Evaluation, Appendix D.
Poor-quality care is not limited to LMICs. Studies from such countries as the United Kingdom and the United States reveal far too many preventable deaths due to poor-quality care. These defects have high economic costs as well. A recent Organisation for Economic Co-operation and Development (OECD) analysis found that 15 percent of all hospital costs in OECD nations are due to patient harms from adverse events. Care is also not reliably person-centered, and patients often report a negative experience with their health care interactions. Indeed, the reported experiences of care are sometimes even dismal, ranging from less than respectful care to abusive behavior on the part of providers. The world’s poor are particularly vulnerable to this kind of disrespect, but the problems are global.
In sum, defects in the quality of health care deny patients and communities the potential benefits of effective care. The currently prevailing forms, habits, and models of care worldwide are incapable of bridging this global quality chasm. Beyond the consequences for people’s health, costs rise when defects in care—such as errors; failure to use effective care; overuse of ineffective care; disregard of a person’s values and resources; and waste of equipment, supplies, time, and spirit—are common. The committee has attempted to quantify roughly the cost of poor quality in at least some low- and middle-income settings, and found it to be enormous. Across LMICs,
the costs of lost productivity alone due to poor-quality care amount to between $1.4 trillion and $1.6 trillion each year. And this figure does not include the immense costs incurred in health care systems as the result of wasted resources and of having to deal with the downstream consequences of errors and harms attributable to poor quality. Arguably, countries or regions with the fewest resources can least afford this economic toll. Given these costs, improving the quality of care may be one of the most powerful strategies available for achieving affordable care and ensuring UHC.
The committee does not offer this dramatically worrisome picture of the quality of global health care lightly. We understand fully that millions of health care workers, managers, executives, and policy makers are struggling daily to offer patients better care and better health, often in the face of great obstacles. We also understand that, especially in the dire conditions of extreme poverty or adversity, our calls for redesign, bold improvement, and modernization may sound unrealistic. When there is no clean water or when the supply chain for essential medicines is broken, it may seem unrealistic for us to suggest imagining a perfect patient journey or fully integrated, seamless care. We intend nothing about this report or our recommendations to gainsay the basic, humanitarian agenda of ensuring essentials for the people who lack them or to undercut the vast, unmet social needs for justice, human rights, equity, and physical security. Nor do we wish in any way to slow the long-overdue momentum toward UHC. Instead, we hope to build on the lessons that have been learned worldwide, to call attention to the gaps that remain for every country seeking higher-quality health care, and to suggest how to bridge that chasm.
BUILDING ON HISTORY
In 2001, the Institute of Medicine (IOM) published a seminal report on the state of quality in health care in the United States. The report’s title, Crossing the Quality Chasm: A New Health System for the 21st Century, heralds its conclusions. Speaking of Americans, it states: “Between the health care that we have and the health care that we could have lies not just a gap, but a chasm.” The report parses the concept of “quality of care” into six basic dimensions. The committee charged with conducting the present study, initiated in 2017, examined these six dimensions in reviewing the evidence for the quality of health care globally and developing recommendations and a research agenda for its improvement. The committee concluded that these six dimensions remain germane to the current global context and that, with some modifications, they are thoroughly applicable to low-resource settings and modern times. The committee’s modifications to the six dimensions of the 2001 IOM report include changing the wording for the “patient-centered” domain to “person-centered,” reflecting sensibilities
and knowledge not widespread when the IOM report was written nearly 20 years ago.2 We believe that “person-centered care” better captures the goal of organizing care around the total (preventive and curative) needs and circumstances of each person, not merely around a disease category. We also added to the dimension of “timeliness” (i.e., services given in good time to avoid adverse events) the broader concepts of “accessibility” and “affordability,” acknowledging the importance of financial protection for quality care. Finally, the 2001 report does not address a crucial contextual element of the global health care scene: integrity. It is now recognized that corruption takes far too great a toll on health care systems, and therefore integrity, accountability, and transparency are key in trying to improve health system performance in every dimension. With these changes, the committee applied the following definitions of the six dimensions of quality in analyzing the current state of quality and identifying future needs:
- Safety: Avoiding harm to patients from the care that is intended to help them.
- Effectiveness: Providing services based on scientific knowledge to all who could benefit, and refraining from providing services to those not likely to benefit (that is, avoiding both overuse of inappropriate care and underuse of effective care).
- Person-centeredness3: Providing care that is respectful of and responsive to individual preferences, needs, and values and ensuring that people’s values guide all clinical decisions. Care transitions and coordination should not be centered on health care providers, but on recipients.
- Accessibility, Timeliness, Affordability: Reducing unwanted waits and harmful delays for both those who receive and those who give care; reducing access barriers and financial risk for patients, families, and communities; and promoting care that is affordable for the system.
- Efficiency: Avoiding waste, including waste of equipment, supplies, ideas, and energy, and including waste resulting from poor management, fraud, corruption, and abusive practices. Existing resources should be leveraged to the greatest degree possible to finance services.
___________________
2 While the committee is endorsing this change in the language moving forward, there have been many reports published in the past two decades that measure and refer to “patient-centeredness.” Where those are mentioned in this report, the language “patient-centeredness” will still be used for accuracy.
3 Although this report uses the term patient when referring to the recipient of clinical medicine, the committee’s position remains that quality improvement requires emphasis on the person, by way of reminding the reader that health is determined by circumstances far beyond the clinical setting.
- Equity: Providing care that does not vary in quality because of personal characteristics such as gender, ethnicity, race, geographic location, and socioeconomic status.
This committee concludes that the global quality chasm is even larger than the quality chasm identified by the IOM in the United States in 2001, and that in human costs, it is much more disturbing. Ineffective treatment for human immunodeficiency virus (HIV), tuberculosis, diabetes, and diarrheal disease (for children under age 5) alone contributes to more than 1 million excess deaths annually. One in 10 drugs in LMICs are estimated to be substandard or outright falsified, resulting in ineffective treatment, contributing to the loss of nearly 8 million disability-adjusted life years (DALYs), and likely exacerbating the problem of antimicrobial resistance. Thus, a careful and open-minded review of the current state of global health care quality leads us to the conclusion that, absent a serious, massive commitment to transparency, accountability, and substantial improvement of care, billions of human beings will simply fail to benefit from the advances made in science and medicine, greatly diminishing the value of UHC. This is especially the case in LMICs, where, because of resource limitations and poverty-related threats to health, people and the care systems on which they rely are especially vulnerable to quality defects. In short, without major attention to quality improvement, UHC will be a grievous disappointment, delivering access to care that has far too little real value for health and well-being. For UHC to be effective, access and quality need to go hand in hand.
LEVERAGING UNIVERSAL HEALTH COVERAGE TO IMPROVE THE QUALITY OF CARE
The changes recommended in this report could not be more urgent. Political will and committed executive and operational leadership are essential to finance and suitably equip the health sector to deliver and continually improve high-quality care. To realize the benefits of UHC, all countries need to commit to achieving “universal quality care.” Doing so will require investment, responsibility, and accountability on the part of health system leaders. This applies especially to ministries of health, but enabling this accountability requires that health system leadership not only have continuity, but also that leaders have the authority, responsibility, and autonomy to make appropriate decisions, regardless of their level. Countries need not tackle this challenge alone. Global resources are widely available, including technical and policy guidance on how to set national quality policies and strategies. Embracing principles of transparency, accountability, continual learning, and co-design, countries will need to work with the end users
of their health systems—their citizens—to design their strategies, policies, and clinical care systems, as well as to create mechanisms for monitoring, evaluating, and reporting progress.
Beyond commitment and strategy development, implementation is key. Currently, there is a scarcity of strong, generalizable evidence and research on the quality outcomes of various financial and policy strategies employed in UHC. Nonetheless, several interventions have proven successful in specific settings, and these efforts provide some guidance for building quality assurance and improvement into health system structures. As countries move toward broader health coverage, governments can use the mechanisms inherent in UHC as levers to accelerate improvements in care, actively considering quality when making decisions on what services and products to commission or purchase, for whom to provide them, and how much to pay for them.
Recommendation 7-14: Make Accountability for Quality a Top Priority Ongoing improvement of the quality of care in all dimensions should be the daily work and constant responsibility of health care leaders, including, but not limited to, ministries of health. The committee endorses the recent Global Quality report and recommendations of the World Health Organization, World Bank, and Organisation for Economic Co-operation and Development, and further recommends the following steps:
- Every ministry of health should develop a national health care quality strategy, together with supporting policies, and should agree to be held accountable for progress.
- Every ministry of health should adopt goals for achieving high-quality care, adapted to their national context, but considering all the dimensions of quality highlighted in this report.
- The United Nations System or a respected global civil society organization should maintain an independent accountability mechanism with which to monitor and report on the progress of nations toward achieving high-quality care.
- Governments, international agencies, and private-sector partners should activate public demand for high quality care through education on patient rights and health literacy, provider choice, measurement, and transparency.
___________________
4 The committee’s recommendations are numbered according to the chapter of the main text in which they appear.
Recommendation 7-2: Use Universal Health Coverage (UHC) as a Lever to Improve the Quality of Care
As ministries of health and health care leaders implement UHC they should work with payers and providers to improve quality by institutionalizing evidence-based policy levers and systematically assessing their effects on quality. Countries should gather and report on quality metrics in global frameworks and across a range of quality dimensions. Steps within nations should include:
- using financing and coverage mechanisms in UHC that support the provision of high-quality care, such as strategic commissioning and purchasing of services and products, selective contracting, and paying for the value of care;
- carrying out monitoring and evaluation, including clinical audits, community involvement and co-design, and customer satisfaction surveys, to generate data that can be used to ensure that UHC resources are fostering high-quality, continuously improving care; and
- conducting research and evaluation on the impact of policy levers on the quality of care received to improve the evidence base on what interventions lead to better care at a systems level.
EMBEDDING SYSTEMS THINKING AND MEASUREMENT
Insufficient resources are not the only threat to quality care. The mere supply of staff, space, and other resources, while essential, falls short of guaranteeing good quality. Indeed, numerous studies have shown little correlation between these health care inputs and quality. In any nation, poor or rich, quality defects derive largely from the same historical fragmentation that the IOM’s Crossing the Quality Chasm report documents in the United States. In most nations, health care is more a collection of separate, siloed activities than a coherent, self-conscious, purposefully designed system. Hospitals lack strong connections to community-based care. Professional disciplines train and work separately, lacking the skills and ethos required for true teamwork and for thriving in interdependency. Patients often play a passive role, deferring to doctors and medical technology for instruction rather than fully utilizing what they can bring to their own care. Health care providers and payers often work against each other rather than in synergy. Staff continually must use workarounds in broken systems just to get through the day. Data systems are fragmented, mirroring the systems in which they are embedded, and offering no windows on the longer-term status, care coordination, and ultimate outcomes of patients. Furthermore,
even as technology advances, information is often stored in forms inaccessible to reflection, inimical to smooth patient care, and useless for learning and comparison.
The vast majority of failures in health care result from how the system was designed or evolved. As the saying goes: “Every system is perfectly designed to achieve exactly the results it gets.” By implication, if it were somehow possible to substitute a new workforce for an existing one, quality would not change meaningfully because the people themselves are not the cause of poor-quality performance. Rather, theory and evidence accumulated over the past half century or more make clear that the quality of care is determined far more by the design of the systems in which people work (such as culture, norms and expectations, the learning environment, the organization of care processes, and incentives) than by the people themselves. Without examining each level of a health care system—the environment, the organization, the health workers, and the patient at the center—and how they interact and either help or inhibit one another, it is difficult to discern how their incentives and activities align and contribute to positive or negative effects on quality. Figure S-2 illustrates this concept of nested, mutually interacting systems.
Principles of Health Care Redesign
If systems thinking and proper design are keys to high-quality, continually improving care, what basic guidelines for design are most promising? The committee considered many candidates for such redesign principles for

low-resource settings, and reviewed the evidence and logic chains for the set of “Ten Simple Rules for Redesign” articulated in the Crossing the Quality Chasm report. Importantly, we chose to explore redesign and quality improvement as applied not to the legacy health care delivery systems of the past and present, but to what are likely to be the new and emerging health care systems of the 21st century. After comparing the legacy and emergent systems, we formulated our own new set of 13 principles as guidelines, which would need to be adapted to local contexts. These 13 principles are united by an overarching design principle: that a strong and constant focus in any setting should be on the needs of the person being cared for at the center, and organized around what we call the “patient’s journey” over time and space.
Recommendation 2-1: Fundamentally Redesign Health Care Using Systems Thinking
Health care leaders should dramatically transform the design of health care systems. This transformation should reflect modern systems thinking, applying principles of human factors and human-centered design to focus the vision of the system on patients and their experiences and on the community and its health.
To guide that new care system, health care leaders should adopt, adapt, and apply the following design principles:
- Systems thinking drives the transformation and continual improvement of care delivery.
- Care delivery prioritizes the needs of patients, health care staff, and the larger community.
- Decision making is evidence based and context specific.
- Trade-offs in health care reflect societal values and priorities.
- Care is integrated and coordinated across the patient journey.
- Care makes optimal use of technologies to be anticipatory and predictive at all system levels.
- Leadership, policy, culture, and incentives are aligned at all system levels to achieve quality aims, and to promote integrity, stewardship, and accountability.
- Navigating the care delivery system is transparent and easy.
- Problems are addressed at the source, and patients and health care staff are empowered to solve them.
- Patients and health care staff co-design the transformation of care delivery and engage together in continual improvement.
- The transformation of care delivery is driven by continuous feedback, learning, and improvement.
- The transformation of care delivery is a multidisciplinary process with adequate resources and support.
- The transformation of care delivery is supported by invested leaders.
The Proper Use of Metrics
In addition to design principles, appropriate and meaningful measurements are necessary to gain an understanding of the quality of care delivered, and eventually to support learning and to guide improvement. The vast majority of current indicators do not measure outcomes, focusing instead on structural inputs or processes of care. For many diseases and many types of care settings, however, the state of quality is unknown because it is not being measured adequately in an ongoing fashion, if at all. Although process measurements do have value and can provide actionable information, patient and population outcome metrics are fundamentally important and are too rare in current assessments, partly because they are often much more difficult to measure; require a longer-term view; or represent the joint effects of health care and non–health care interventions, which do not share common databases.
Many metrics for measuring quality of care already exist; after dedicated focus through international partnership, for example, more than 650 hospitals in OECD countries have adopted standard metrics for measuring quality. Therefore, time is better spent mainly on selecting from among existing indicators than on developing new ones, which warrant the effort only when they would be more valuable. In applying metrics, considering the context is, of course, vital. Even indicators with strong pedigrees must be vetted and adapted to low-resource settings so that they can provide contextually appropriate, helpful insights for patients, providers, and policy makers, taking into account the implications for culture and effectiveness at the front lines of care. It is essential as well for the use of measurement to be person-centered, health-oriented, intentional, selective, respectful of the many pressures on health care providers, and parsimonious, aligned with core goals of accountability to the public and learning and improvement for providers and with patients.
Recommendation 4-1: Embed and Refine Quality Measurement in Health Care
Nations, regions, and health care organizations should routinely and transparently measure and report on domains of quality, especially their relevant outcomes, to support learning, as well as foster accountability and trust in the health care system.
- Ministries of health and multilateral organizations should maintain ongoing, collective efforts to identify and implement a core set of quality metrics for lower-resource settings (such as those developed by OECD, as well as standards and outcome metrics from the International Consortium for Health Outcomes Measurement) to allow for benchmarking and learning.
- Health care leaders should prioritize patient-reported outcome measures and patient-reported experience measures as well as health outcome metrics for assessing quality whenever possible.
- Governments and organizations should track metrics frequently to assess performance and improvement over time. They should make performance transparent to all parties through such mechanisms as public reporting, and use metrics and co-design with three goals in mind: accountability to patients, building trust in the system, and learning.
THE FUTURE OF HEALTH CARE
The committee believes that the care systems of the future will differ radically from those of the past. Although a full review of the future health system was beyond the scope of this study, the clear implications for quality led the committee to suggest some concerns and safeguards to mitigate risks that the new forms of care may bring. Digital health technologies are key enablers to optimize health systems and improve the quality of care for individuals and populations, yet they are double-edged. If left unchecked, these technologies can deepen inequities among populations, with hidden biases being embedded in the new tools.
With the explosion of new digital tools over the coming years, new players will join the health care field. In particular, patients will become ever more active in consuming information about prevention and diagnosis; researching options for treatment; and communicating with care providers using a wide range of media, not just in-person visits. The new health care system will have a more authentic focus on prevention, risk factor management, and personalized care, using precision medicine and predictive models and with the patient at the center shaping the demand for and the design and delivery of care. These changes will be disruptive, even threatening, to legacy structures, jobs, and beliefs, but they are inevitable. The committee believes that health systems need to embrace new digital care technologies, guided by a vision of patient care that is anticipatory rather than reactive; thoroughly integrated across time and space; and wholly centered on continually improving the experiences—the “journeys”—of patients, families, and communities.
The committee envisions these new designs delivering care directly to people wherever they are—in schools, in homes, or in market stalls—and relying far more on community resources and far less on formal health care facilities. This shift will require new skills, attitudes, and culture among health care providers and new, more active roles for patients and families in shaping, evaluating, and delivering the care they need. Payers, academics, patient groups, health care networks, and medical product development and technology companies in the private sector will need to develop multisector governance mechanisms appropriate for these new models of health care delivery to maximize their benefits and minimize their risks. Co-design and co-production of health care between providers and patients, as well as consideration of human factors in the design and use of technology, will become the norm, with benefits to both.
These changes will necessitate attention at multiple levels. The question of whether technology will be, overall, a disruptor that improves or worsens quality remains unanswered. Currently, many countries exercise little regulatory oversight of care and little use of care guidelines to ensure quality. That will not suffice in the future health care world or in the era of UHC. Ministries of health will need to accept a dual role: identifying and applying policy, financing, and regulatory frameworks to accelerate the growth of new, digitally assisted health care, while also remaining mindful of quality and mitigating the risks of these new care models. They will need assistance in taking on these roles. Global partners, including private companies within both the health care and information communication sectors, have new opportunities to join ministers of health, health care leaders, and other stakeholders in pursuing a joint path forward that will benefit all parties as technology advances. Health systems within each country will need to embrace this transformation in partnership with one another, while anticipating and mitigating the risks that such changes will bring.
Recommendation 3-1: Build a Global Community for Digital Advances in Health and Health Care Delivery
The United Nations System should convene an international task force with multisectoral representation to provide guidance to the global community on advances in digital health technologies. This task force should develop:
- data standards, norms, ethical frameworks, and guidance for modernized regulation and human resource capacity to enable countries to better benefit from the transformative technologies in the health sector;
- engineering and design standards that emphasize interoperability, human factors, and human-centered design to align technologies
- and innovation with the aspirations of global health care quality; and
- an international resource to guide countries in incorporating regulation of digital health technologies so as to protect users and their privacy while fostering innovation, with input from an external board of experts.
Recommendation 3-2: Adopt and Adapt the New Technological Realities of the Present and Future
Countries should prepare for and embrace the technological (especially digital) changes in health care by adopting and adapting standards; ethical frameworks; and governance, payment, regulation, and workforce designs that are anticipatory and that embrace, rather than impede, the potential of transformed care.
- Ministries of health should collaborate with ministries of communication and technology to build national health strategies that embed digital technology as an integral part of the health system and address their countries’ priority health needs.
- Governments and organizations should develop and support multisectoral task forces to guide their digital health strategies to ensure that all deployed digital health technologies are evidence-based and coordinated, that patient safety is protected, and that risks are mitigated.
- Government and private-sector leaders should revise competency requirements and educational curricula to better meet the workforce needs created by digital health advances, including skills in data science and analytics, interpersonal skills for teamwork and person-centered care, and systems-based thinking.
HIGH QUALITY FOR EVERYONE: MAKING INFORMAL CARE VISIBLE AND ADDRESSING CARE UNDER EXTREME ADVERSITY
In many parts of the world, significant proportions of the population choose to seek care in the informal sector, either because they lack access to formal health care providers or, sometimes, because they do not trust the formal system. For millions of people—in some countries more than 75 percent of the nation’s population—this means receiving care from providers who lack formal training but are often well known in the community.
In addition, millions more people are suffering in fragile states or humanitarian relief settings with haphazard access to health care, and without strong infrastructure for oversight or regulation of care. The majority of these sources of care in the informal sector and under conditions of extreme
adversity operate outside of formalized health systems, meaning that people in these settings are receiving care that may not be regulated, measured, or coordinated with other providers. Taken together, these alternative care systems, their complexity, and the corresponding lack of scrutiny and transparency subject billions of people worldwide to care of largely unknown quality.
Informal Care Providers
Informal care providers have variable definitions and various scopes of practice among countries, and much remains unknown about their exact numbers and their utilization. The available research makes clear, however, that the quality of the care they provide is often poor (although in many cases comparable to the quality of care in the formal sector). This is a challenge, but also an opportunity. Many health care systems struggle with severe shortages of both health workers and general physical infrastructure for health care facilities. Governments and leaders in the formal health care system would benefit from acknowledging that informal care providers are the source for a significant proportion of health services in many countries, and from bringing these providers into mainstream care delivery and working to assess, streamline, and improve their quality.
Recommendation 5-1: Incorporate the Informal Care Sector in the Pursuit of Improved Care Delivery
Country governments should integrate informal care providers into their national health strategies and quality monitoring and improvement efforts. To this end, they should acknowledge that these informal providers exist and undertake efforts to assess and improve the care they provide, such as through education, training, and incentives, to the full extent possible.
Quality in Extreme Adversity
About 2 billion people live in fragile states and conflict settings worldwide. Their access to quality care is unreliable at best, and often, frankly, nonexistent. Research on health care in these contexts is scarce, leaving health care leaders and providers with an unclear picture of what interventions lead to best outcomes and what to prioritize with limited funds. The committee characterizes these chaotic and uncertain environments as “settings of extreme adversity” to shine a light on the dearth of quality health care affecting enormous numbers of people, a large proportion of whom are women and children. Addressing health care quality in these chaotic and often violent settings has often been relegated to “not now” status, with
priority being given to simply providing access to care. Yet, this approach is misguided. In fact, given how vulnerable the people in these settings are, providing them with high-quality care is arguably more important than is the case anywhere else. There is an urgent need to understand what interventions work best in these settings so they can be implemented as soon as possible to avoid preventable mortality and harm and the waste of already insufficient resources.
Recommendation 5-2: Make Settings of Extreme Adversity a High Priority
National governments, multilateral institutions, nongovernmental organizations (NGOs), bilateral donors, humanitarian stakeholders, and philanthropic donors should make studying and improving the quality of care in settings of extreme adversity a high priority. More specifically:
- The international humanitarian system, multilateral organizations, and NGOs should identify priorities for assessing the quality of care in these settings and develop strategies for its improvement. Emphasis should be placed on addressing conditions that are particularly burdensome in these settings, such as treating conflict-related trauma and mental illness, optimizing the patient experience to ensure trust in providers, protecting providers from harm, and adequately managing chronic diseases.
- The National Institutes of Health (NIH) and other research funders should support primary and implementation research aimed at identifying what interventions work and in what contexts to improve health outcomes in fragile states and austere environments.
- Multilateral organizations and the United Nations System should create multistakeholder collaborations for purposes of reviewing and vetting the available evidence; developing consensus on promising interventions for improvement; and identifying issues of leadership and accountability for quality of care in particular circumstances, such as conflict zones, humanitarian crises, and fragile states.
THE ADVERSE IMPACTS OF CORRUPTION
Corruption, in all its forms, is an enormous contributor to poor quality of care worldwide. Its effects are felt in longer wait times, poorer treatment by health care workers, absenteeism of providers, unnecessary charges for services, and general misuse of funds, leading to decreased trust among governments, health care systems, and citizens. In essence, integrity, if not a dimension of quality, is itself an essential precondition for the pursuit of
quality in health care. Thus, in the pursuit of universal quality care, it is critical for governments and societies to create better governance structures that are accountable and transparent and fund health systems so as to decrease instances of corruption and improve health outcomes for populations. Until this takes place on a national scale for many countries, UHC may be subverted to enrich the powerful and leave vulnerable populations without adequate care.
Recommendation 6-1: Address Corruption and Collusion
Ministries of health should include in their national health care quality strategies, directly and clearly, safeguards against corruption and collusion and actions for improvements in integrity throughout their health care systems. The health sector should draw on expertise and resources from outside the health care system, including related core state institutions and dedicated anticorruption institutions, to combat corruption through prevention, detection, and enforcement.
CREATING A CULTURE OF LEARNING
Health care systems worldwide still struggle with operationalizing a systems approach, despite its proven utility in other sectors, such as aviation and transportation. One of the important properties of sound systems is the capacity for improvement through learning over time. Quality, in any of its domains, is not a static property, and continual quality improvement, encompassing the processes of assessment, learning, and continual redesign, as well as the incorporation of data streams and feedback loops into current guidelines and practice, needs to be actively nurtured and intentionally maintained in organizations that seek always to do better.
The committee concludes that the vision of a learning organization applies to low- and middle-income settings just as it does to high-income settings, where there remains much room for growth and learning. In most nations and most organizations, achieving this vision will require a profound cultural shift from reliance on inspection to investments in learning and action. Countries and organizations committing to a strategy without this cultural shift are unlikely to be successful. And this shift is only the first of many steps toward successful transformation. Successfully and sustainably changing the culture of health care systems will require investment, leadership, and willingness to take risks and fail in the service of learning. But many businesses have already accomplished this, and successful private-sector examples can be found in almost any country. The committee believes that, unless and until nations and their leaders adopt this philosophy that improvement depends on learning, progress toward a future of high-quality health care will be slow indeed.
In part, the existing defects in quality reflect gaps in leadership and management. Without specific attention, quality of care almost inevitably deteriorates. The forces of entropy are rampant in any complex system, including health care. Self-conscious, planned investments of time, money, and leadership attention are required to ensure the processes of continual learning and change that lead to improvement. This need has become even more acute with the shift in the global burden of disease toward chronic illnesses and conditions associated with aging, which beg for attention to patient journeys over time and space.
A culture of continual improvement (adopting bold aims for improvement, guided by systems thinking, continual learning, and innovation and devoted to redesign and implementation guided by new design principles) is impossible without strong leadership at all levels, characterized by widespread cooperation. The committee identifies health care leaders as including, among others, ministers of health, other government officials, organizational executives, clinicians, financing organizations, and patient and community representatives. A high level of shared vision, cooperation, and shared intent is required among all stakeholders.
The alternatives to systems thinking and continual learning can appear seductive, but they are less likely to achieve the desired outcomes in the long run. Leaders lacking a systems perspective or impatient for instant success can turn to blame, exhortation, and mere goal setting, as if just asking for better results or simply trying harder were somehow enough. Such shortsighted approaches often are made even worse by blunt oversight—whether in the public or private sector—that entails demanding a better bottom line or immediate results to show donors. The effects of such pressures on a workforce can be toxic to morale, trust, cooperation, honesty, and quality itself. Leaders—at every level—who are truly intent on supporting improvement must take responsibility not just for creating accountability, but also for supporting the continual design and redesign of systems of care toward improvement, and for supporting the cultures and processes that can fully engage the workforce as participants in that learning process. Tracking of metrics over time can be used to identify small improvements that can fuel more successes.
When top leaders, such as executives and health ministers, act inconsistently with the systems-oriented approach to quality (see the design principles under recommendation 2-1 above), improvement stalls. Why should a workforce take a chance on testing changes, setting bold improvement goals, or being transparent about results—good and bad—if the consequences will be blame, criticism, table pounding, and budget cuts? A workforce treated as objects to be controlled will soon cease to learn; it will regress to pursuing timid aims, hiding defects, and ticking boxes. It will become less, not more, focused on the deeper needs of the patients and
families it serves because understanding unmet needs will be a route only to further frustration. In contrast, when top leaders guide their own actions according to science-based principles of systems thinking and support continual learning as the mainstay of their organization, they can liberate enormous energies and aspirations in the workforce. With proper methods and leadership, improvement can soar.
Recommendation 8-1: Encourage a Culture of Learning to Fundamentally Redesign Health Care
Health care leaders in all settings should master and adopt the vision and culture of a learning health care system, striving for continual learning and avoiding an approach that relies primarily on blame and shame. This learning system should extend beyond hospitals and providers to include patients, payers, administrators, community health workers, and others involved in health.
- Country governments should implement policies designed to effectively educate and supply health care professionals who are trained to provide high-quality care. These professionals should include a cadre of clinical and nonclinical leaders that are versed in creating a culture that rewards openness, transparency, and a commitment to improvement.
- Governmental and organizational leaders should ensure that efforts to create accountability in the health care system, although fundamental, do not create a culture of fear and reaction, which is inimical to system improvement and change. Performance in all domains of quality should be measured and reported transparently, and the results should be widely available to patients to encourage feedback and improvement over time.
- Governmental and organizational leaders should learn and use modern approaches to improving science, practice, and organizational culture.
- Nations, regions, and health systems should establish and maintain programs to facilitate shared, collaborative learning about improvements and innovations in health care.
- Leaders should ensure that health care systems harness new digital health technology to help reduce costs and improve care through real-time use of data.
THE CRUCIAL NEED FOR MORE EVIDENCE
The committee uncovered a vast number of unanswered questions related to quality and a dearth of evidence supporting interventions world-
wide. Given these findings and the importance of people’s health and well-being, the amount of funding directed toward the assurance and improvement of quality in health care, relative to other industries, is remarkably low. A much larger dedicated research agenda related to quality of care in various settings—including not only primary research and highly rigorous clinical trials where appropriate but also implementation research—would far better inform leaders about priorities and appropriate interventions. As discussed throughout this report, the widely diverse environments in low-resource settings, and indeed across countries of all income levels, demand contextual validation of interventions before they are deployed at a larger scale. The success of financial incentives or new checklists in a facility during a randomized trial does not guarantee the same results in the field or in a different social context. A collaborative research agenda geared toward continual learning would help. This agenda could have exponential effects on the quality of care, especially if a global community focused on quality mobilized to share lessons and to better understand what strategies and interventions to employ.
Recommendation 8-2: Define and Mobilize a Research and Development Agenda
The U.S. National Institutes of Health, philanthropic organizations, and other bilateral donors, as well as low- and middle-income country (LMIC) governments and other stakeholders, should increase investments in research and development on interventions that would improve the quality of care at the system level, encompassing both primary and implementation research. The following questions should be priorities:
- What is the impact on population health outcomes of the digitization of health care?
- What innovative or proven models exist for local use of measurement for improvement?
- What are the roles of various actors in quality management across LMICs?
- Which digital health technologies can best contribute to better quality of care in resource-constrained settings?
- Do private markets reward higher quality?
- To what degree does corruption have effects on the quality of health care delivered in various settings? How can these effects best be mitigated?
- What 10 interventions are most likely to improve health care quality in settings of extreme adversity?
- What 10 interventions are most likely to improve the quality of care in the informal sector?
- What are the best strategies for addressing quality in fragmented settings where most patients pay out of pocket?
- What strategies can reduce overuse of health care services in low-resource settings, especially when regulatory capacity is limited or absent?
- How can strategic purchasing best help improve the quality of care delivery?
- What strategies are effective in engaging patients and people in general to demand high-quality (and especially safe) care for themselves and their families?
- How can leaders effectively and efficiently implement a systems approach for strengthening the quality of health care in LMICs?
- What skill sets for the workforce are linked to better health outcomes for patients, especially in the emerging digital age of health care?
A FINAL WORD
The committee realizes that, when presented with so many areas to work on and high-level approaches to operationalize, leaders may wonder where to begin. While prioritizing the recommendations and interventions proposed in this report would be an extremely valuable contribution, the committee believes that doing so is beyond the scope of this study. There is no silver bullet solution, and each country and health system will need to tailor its approaches according to needs of its populations. It is our hope that future projects can gather national and regional stakeholders to take on this crucial task of setting priorities for action.
In our year of hard work together, we have come to agree on at least three fundamental premises. First, a vast quality chasm plagues health care globally. It affects billions of people, and no nation and no population is exempt. The costs in lives, health, and society are enormous—far greater than most people know, including the committee when we began this inquiry. This burden will continue unless nations and leaders work actively to eliminate it. Second, it is possible to do better, even in low-resource settings, and even without substantial additional resources. There are approaches that work. Modern systems sciences and several decades of distributed experience in quality improvement offer a firm foundation for starting on the road to improvement. While there is no doubt about the need for more evidence, there is enough evidence of efficacy to start now. Third, leaders
must act. Improvement depends on them, and it is their responsibility. The success of the MDGs shows what can be achieved, even in resource-poor settings, when a global consensus grows on the value of bold aims, scientific methods, and shared learning. The MDGs resonated even in the poorest nations on earth. The committee hopes for the same resonance around the quality imperative now. For the most disadvantaged people and in the most austere settings, the need is greatest. The longer-term promise of fully transformed care, technological modernization, and personalized care may as yet be far out of reach for some, but the first steps are not. As the momentum for UHC continues, so, too, is it time to seek quality care for all. Equity and quality of care need to arrive together, or they will arrive not at all.






















