
1
Introduction
Since 2000, programs to improve health across the world have accelerated rapidly. The Millennium Development Goals (MDGs) in particular have intensified the focus on health, development, and poverty reduction and encouraged the scale-up of investments in interventions worldwide. Spurred by the MDGs, the proportion of undernourished people in developing regions fell from 23 percent to 13 percent; the burdens of human immunodeficiency virus (HIV), tuberculosis (TB), and malaria fell dramatically, meeting global targets; and child and maternal mortality decreased by 53 percent and 43 percent, respectively (WHO, 2015). Yet, despite the overall success of the MDGs, progress has been uneven. The MDGs largely overlooked inequalities within nations, and placed insufficient emphasis on improving conditions for the poorest populations in both low- and middle-income nations.
As a successor to the MDGs, in September 2015 the global community adopted a new development agenda—the Sustainable Development Goals (SDGs)—agreed on by 193 countries (UNDP, 2015). The SDGs represent an attempt to address the unfinished agenda of the MDG era, setting forth a comprehensive set of integrated targets through economic, social, and environmental lenses. Of particular relevance to this report, SDG 3 focuses on “ensuring healthy lives and promoting well-being for all at all ages” (UN, 2017). The pursuit of equity is at the heart of the SDGs, and Target 3.8 specifically addresses the achievement of universal health coverage (UHC), a central pillar of SDG 3 overall (UN, 2017):
Achieve universal health coverage, including financial risk protection, access to quality essential health-care services and access to safe, effective, quality and affordable essential medicines and vaccines for all.
THE SUSTAINABLE DEVELOPMENT GOALS AND THE UNIVERSAL HEALTH COVERAGE AGENDA
The current UHC movement represents the culmination of an ongoing emphasis by the World Health Organization (WHO) and the World Bank on ensuring access to quality health care for the poor. The intent of UHC is that “all people [receive] the health services they need … while at the same time ensuring that the use of these services does not expose the user to financial hardship” (WHO and World Bank, 2015, p. 7). However, UHC should be considered a continuous journey and not a panacea for achieving health improvements (Horton, 2018).
A first step to achieving UHC will be to address the inequitable distribution of health gains. Between 2005 and 2015, for example, only 17 percent of mothers and infants in households in the poorest quintile in low-income and lower-middle-income countries had access to at least six of seven basic interventions, versus 74 percent in the richest quintile (WHO and World Bank, 2017). This report, however, focuses on an often-overlooked issue that goes beyond access. Simply interpreted, access to care is only part of the goal of UHC; ensuring that this care is of high quality is also essential (Scott and Jha, 2014). Until recently, however, the quality of available health care has not been incorporated consistently into global and national discussions of UHC, nor has it been a consistent focus in practice. The UHC movement will succeed only if quality is placed squarely at the heart of the agenda. Recognition of this fact has given rise to the concept of “effective coverage.” While “crude coverage” measures only access to services, “effective coverage” takes into account the need for, the use of, and the quality of the services (Ng et al., 2014).
Quality, Universal Health Coverage, and Global Health Security
While the quality of care is not always linked to UHC, some argue that both should be linked more closely with global health security, which WHO defines as the reduced vulnerability of populations to acute threats to health (WHO, 2007). All three are the subject of prominent conversations globally, but they sometimes are seen as disparate, even as competing for attention and resources. The West African Ebola outbreak of 2014–2015 in particular has led to growing recognition of the need for local health systems to contain outbreaks before they cause catastrophic loss of life and economic turmoil. The harmonization of efforts at the local level is
needed at higher levels as well: health security, quality, and UHC implementation need not be promoted in opposition to one other, but instead can have synergistic effects when seen as complementary. The inputs for quality, such as reliable power, adequate medical equipment, and trained health care personnel, are also inputs for health security and resilience. If UHC can successfully stimulate demand for care in a country and increase utilization, ongoing case detection and surveillance can be incorporated into strong primary care systems and be used to detect early warnings of outbreaks (Jain and Alam, 2017).
The global community is coming to recognize the strong interrelation among these agendas. In the 13th draft General Program of Work (GPW) for 2019–2023, WHO has outlined a set of three interconnected priorities: healthier populations, protection from health emergencies, and more people benefiting from UHC to meet the SDGs (WHO, 2018a). As argued in the 13th GPW, the three agendas require implementation that is mutually reinforcing, meaning that future health systems should be characterized by strong integration of quality, resilience, and UHC efforts. According to Jain and Alam (2017), it would be hazardous to suggest that countries have achieved UHC without having developed a sustainable capacity for the key public health services that are integral to health security—infectious disease prevention, detection, and response. In short, health systems of the future, while becoming more predictive and holistic, also represent an important opportunity for a better merging of quality, UHC, and global health security to achieve positive, synergistic effects.
What Is Universal Health Coverage Without Quality?
As indicated above, a central premise of this report is that, while achieving UHC is important, its full potential to reduce the burden of ill health will not be realized without a commensurate effort to improve health care quality. In recent decades, several analytical frameworks have emerged to guide health care quality, which at its core is comprised of six dimensions as set forth in 2001 by the Institute of Medicine in Crossing the Quality Chasm: A New Health System for the 21st Century: safety, effectiveness, patient-centeredness, timeliness, efficiency, and equity (IOM, 2001) (see Box 1-1). This framework for assessing health care remains influential to this day.
These six dimensions are interrelated, and are, both individually and collectively, essential properties of high-quality health care. Indeed, high levels of inappropriate care are pervasive. For example, a WHO report finds that more than 6 million excess caesarean sections are performed each year, 50 percent of which occur in China and Brazil (Gibbons et al., 2010). If care were only equitable and efficient but neither safe nor effective, the very
access to care could lead to adverse medical outcomes or even mortality due to hazards and defects in care. Poor-quality antimalarials, for example, were associated with the deaths of more than 122,000 children under the age of 5 in sub-Saharan Africa (Renschler et al., 2015). Similarly, immunizations are a vital medical intervention for children, but their effectiveness depends on timeliness and proper storage. If vaccines are not high quality, “stored appropriately, dispensed at the requisite time, and properly administered,” they cannot provide the expected benefits (Rasanathan et al., 2016, p. 4). Finally, if care delivery does not treat patients with respect and dignity, trust in the system and providers can erode, and people therefore may not seek care that could help them in the future.
The challenge of assuring and improving quality is not limited to low- and middle-income countries (LMICs). High-income countries have fallen short on the quality scale as well. A recent news series in the United States reveals excess and preventable deaths due to poor-quality care in surgery
centers in multiple states (Jewett and Alesia, 2018), and in 2013 researchers estimated medical error to be the third leading cause of death in the United States, behind only heart disease and cancer (Makary and Daniel, 2016). These defects have high economic costs as well, with 15 percent of all hospital costs in Organisation for Economic Co-operation and Development (OECD) countries being due to patient harms resulting from adverse events. The lack of coordination within and among health care providers and networks appears to be the greatest concern, as failures in coordination can significantly delay treatment and deter people from seeking care (Picard, 2010). For example, when a person visits a specialist but is given a paper summary and instructions to follow-up with a general provider at another location, the general provider may not know the outcome of the visit before seeing the patient again in person, and must hope that the patient brings the necessary paperwork. While improving access and quality may appear to be two different aims, achieving one without the other is futile. Without quality at the center, UHC is an empty vessel.
CHALLENGES FOR HEALTH CARE QUALITY
Improving quality of care in low-resource settings is a vexing challenge. The quality of care can vary dramatically both within (Das, 2011) and across nations (Barber et al., 2017). For example, the Dartmouth Atlas Project in the United States analyzed variations in how medical resources are distributed and used (The Dartmouth Atlas of Health Care, 2015). These researchers found that more resources and more services delivered do not lead to better or more effective care. In fact, higher resource intensity is sometimes associated with worse care. Other studies analyzing health care in both government-run and private-sector health facilities have found poor quality across multiple dimensions (Berendes et al., 2011), with little difference between the public and private facilities (Basu et al., 2012). Some countries, such as Costa Rica (Pesec et al., 2017) and Rwanda (Sayinzoga and Bijlmakers, 2016), have invested heavily in health system–wide reforms, leading to improved health outcomes and increases in life expectancy (Pesec et al., 2017). However, translating these successes to scale globally is difficult given the variations in context among nations. This section outlines some of the challenges faced by low-resource settings in the areas of fragmentation of care delivery and poor health system building blocks. These challenges can result in a fragmented and complex patient journey (described later in the chapter) within and among health facilities, often resulting in poor experiences for those who depend on care. The committee emphasizes that improving the patient journey across the life course is an essential lens through which to view improving health care quality.
Fragmented Health Care Delivery
Fragmented health care is a problem shared by all countries, whether high-, middle-, or low-income. Health care delivery often requires a patient to transition from unit to unit, from one care setting to another, or from a care setting to home, receiving care from a range of providers (Ben-Tovim et al., 2008). Too often these interactions are siloed. Providers and facilities fail to communicate with each other or coordinate their work, causing important health information to fall through the cracks and impairing patient experiences. While users in high-income countries may have an electronic health record (EHR), they often lack easy access to it, or it is distributed across multiple providers. Users’ information thus is carved into pieces. One study evaluating fragmentation of hospital care for patients with chronic conditions in New York City found that Medicaid enrollees were 24.4 percent more likely to experience highly fragmented care relative to commercially insured patients, even after adjusting for demographic characteristics (Schrag et al., 2006). Likewise, fragmented health insurance has caused suffering among interstate migrant workers in India. The migrant workers are excluded from any form of employee state insurance because they work in the informal economy. Even those registered under state-specific health insurance schemes are not eligible to access health care services outside of the originally registered states. Because they lack interstate insurance coverage, migrant workers avoid using health services until their conditions become advanced. They then often seek care from an expensive private facility, thereby incurring severe financial debt. A fragmented health insurance scheme allows an already vulnerable population to slip through the cracks (Mohan, 2017).
This failure of health care systems to take into account the entire journey across clinical encounters and instead treat each encounter in isolation leads to care that is reactive, episodic, treatment focused, provider focused, duplicative, and wasteful. Because records and histories are difficult for patients to access, duplicate tests are often ordered when people migrate across care providers and hospitals (Kripalani et al., 2007). Failing to consider the user’s perspective can also raise costs and injure patients. Clinical encounters that are geographically inaccessible, unacceptable, and disrespectful for patients can be especially harmful, as they deter patients from returning for needed care.
Poor Health System Building Blocks
Fragmented care is exacerbated by factors both at the clinical encounter and at more upstream organizational and policy levels. WHO developed a framework that organizes these various factors, or health system build-
ing blocks: service delivery, health workforce, health information systems, access to medicines, financing, and leadership and governance. If these building blocks fail to function optimally both separately and in conjunction with one another, they cannot support high-quality health care (WHO, 2010).
Service Delivery
In a health care facility, good service delivery has at least two components: availability and readiness. In low-resource settings, both are at risk. Service availability depends on the distribution of facilities and a trained health workforce (discussed below). Service readiness depends on the presence of basic amenities, such as reliable power, improved water, and sanitation; standard infection precautions; and medical equipment (WHO, 2010). Unfortunately, many health facilities in LMICs lack improved water1 and sanitation2 and standard infection precautions. In a global survey of 54 countries, for example, WHO found that 39 percent of health facilities lacked an improved water source, 19 percent lacked improved sanitation access, and 35 percent lacked water and soap for handwashing (WHO and UNICEF, 2015). Another study of 78 LMICs found that 73 percent of health facilities lacked sterilization equipment (Cronk and Bartram, 2018).
Health facilities require adequate quantity and quality of water sources to maintain a hygienic environment and deliver health care optimally. But a systematic review of hospital-acquired infections in LMICs found that inadequate environmental hygiene can be a determinant of poor outcomes (Allegranzi et al., 2011). Similarly, a lack of reliable power disrupts health care delivery. It can prevent the use of sterilization equipment, limit the use of electrically powered tools (Adair-Rohani et al., 2013), impede the use of information and communication technology (Cronk and Bartram, 2018), cause vaccine spoilage (WHO, 2018b), and impede the capacity to provide both surgical care (Meara et al., 2015) and service at night (Adair-Rohani et al., 2013). Disruptions of power at health care facilities are prevalent in LMICs, occurring by one estimate at 59 percent of facilities (Cronk and Bartram, 2018).
High-quality health care also depends on functional medical equipment, such as laboratory testing and imaging tools. Many hospitals and clinics in
___________________
1 An improved water source, by the nature of its construction, protects the water from outside contamination. Common examples include piped water, a public standpipe, a borehole, a protected dug well, a protected spring, and rainwater collection (WHO and UNICEF, 2012).
2 Improved sanitation facilities hygienically separate human excreta from human contact. Types of facilities include flush or pour flush toilets to piped sewer systems, a septic tank or pit, a ventilated improved pit latrine, a pit latrine with slab, and a composting toilet (WHO and UNICEF, 2012).
LMICs rely on donations, which account for approximately 80 percent of medical equipment in these countries (Bhadelia, 2016). Often, such equipment can be impossible to use as its voltage requirements are incompatible with those that exist in the hospitals (Jones, 2013). Even if the equipment is technically compatible, health care personnel may not have the capacity to use it (Howie et al., 2008). Reports of medical donations lacking manuals at all or in the correct languages, as well as contact details for the manufacturer needed for repairs and proper utilization, render the equipment useless (Healy, 2015). If the roles of human factors and ergonomics in the transfer of these technologies are not considered, safety and proper utilization cannot be guaranteed (Meshkati, 1989). Furthermore, a lack of spare parts and personnel often makes it impossible for health care facilities to maintain or repair medical equipment when it falls out of service. As a result, equipment can sit unused in hospital hallways or in “equipment graveyards.” An analysis of inventories in 16 low-income countries found that an average of about 40 percent of pieces of medical equipment in hospitals were nonfunctional (Perry and Malkin, 2011), compared with less than 1 percent in high-income countries (Howitt et al., 2012). In fact, this gap may be even larger because many hospitals in low-resource settings do not maintain up-to-date inventories.
Health Workforce
High-quality health care requires skilled health care workers (Speybroeck et al., 2006). Unfortunately, however, there is an estimated shortfall of 2.5 million doctors, 9 million nurses and midwives, and 6 million allied health professionals globally (WHO et al., 2018). With few lucrative opportunities to work in home countries and few incentives to work in rural areas and even in the public sector, many health professionals leave the countries in which they train for other, more profitable markets. WHO emphasizes the importance of health worker density,3 but that concept may implicitly assume that these workers are adequately trained and consistently deliver care that meets clinical standards. Yet, even when health workers are present, several studies indicate a lack of adherence to clinical guidelines and implementation of evidence-based practice (Puchalski Ritchie et al., 2016). In a study in China, India, and Kenya for example, adherence to evidence-based treatment for such conditions as asthma, chest pain, diarrhea, and
___________________
3 Health worker density refers to the numbers of physicians, nurses, midwives, dentists, community health workers, and other related health care workers in a given area. It is usually given as a ratio—number of workers: 1,000 population. The SDGs set a threshold of 4.45 physicians, nurses, and midwives per 1,000 population as the minimum density needed for an adequate health workforce (WHO, 2016).
TB occurred little more than 50 percent of the time, and often less than 25 percent of the time (Daniels et al., 2017).
This failure to adhere to evidence-based practices may be due to a “know” gap—a lack of knowledge or awareness of guidelines. Without institutional support, health care workers may not have access to the latest published guidelines. The problem can also be due to a “know-do” gap, such as a lack of understanding of how guidelines were developed. Or it can be due to competing priorities, a lack of technology and medicines to support the application of guidelines, a lack of supervision and mentorship, and even organizational barriers—all of which are systemic challenges faced by health systems globally (Puchalski Ritchie et al., 2016). During his testimony to the committee, Pierre Barker from the Institute for Healthcare Improvement underscored the gap between knowledge and optimal outcomes. He stressed that the integration of quality into the health care system needs to merge command and control, quality assurance, and quality improvement (Barker, 2017).
Another explanation for the “know-do” gap is a lack of accountability. Accountability in health care rarely strikes the right balance between promoting quality of care and preventing a culture of blame. In an environment of too much accountability, a culture of blame and a litigious environment can develop. As a result, health workers may underreport errors out of fear (Keepnews and Mitchell, 2003). Conversely, too little accountability entails little to no oversight of health workers, allowing them to shirk responsibility and engage in perverse behaviors, such as absenteeism (Nishtar, 2010). In low-resource settings, accountability can be lacking because of weak regulations and the limited capacity of organizations to hold health workers to professional, discipline-based standards, which may explain why the performance of health workers, even those who are trained, is low and highly variable in LMICs (Das, 2011). Indeed, this was the case in high-income countries before medicine became professionalized, standardized, and regulated (Starr, 1982). The Indian government has attempted to increase accountability within the health sector by creating Panchayati Raj Institutions (PRIs), locally elected bodies of governments in rural areas, meant to decentralize political, administrative, and fiscal responsibilities. Yet, while decentralization has progressed, problems of accountability remain because PRIs make irrelevant and unproductive decisions as the result of having neither the resources to undertake development nor the power to influence existing programs (World Bank, 2000). Importantly, as low-resource settings start to develop standards and accountability structures, they will need to ensure that they are given the necessary authority and resources to do so, while also promoting a culture of learning and improvement.
The “know-do” gap can also be blamed on the misalignment of incentives. Closely related to accountability, incentives on “what to do” or “what
not to do” can guide health workers’ behavior. Incentives are driven mainly by measurements. These measurements can be linked to payments or provider ratings. Thus, in a way, incentives and measurements act as a form of economic and clinical accountability (Goeschel, 2011). However, often “what gets measured gets done,” and so identifying the right measurements to highlight the right outcomes is critical.
Health Information Systems
Clinical decision making depends on sound and reliable information. A health information system (HIS) can support decision making with data generation, compilation, analysis, synthesis, communication, and use (WHO, 2010). However, HISs globally do not always synthesize data effectively to inform sound clinical decisions—a problem shared by countries of differing income levels.
A reliable and efficient HIS goes beyond improving monitoring and evaluation to influence alert and warning systems, patient health data and trends analysis, and global reporting. An HIS should be comprehensive at four levels: individual, health facility, population, and public health surveillance (WHO, 2008). To achieve equal success across all levels, a system must operate interdependently. Increasing capacity to undertake effective health information exchange is essential, but many LMICs face structural, political, and financial barriers to making the transition from paper-based to electronic documentation (Akhlaq et al., 2016). A BMC Health Services Research study explored the sustainability of electronic health information systems (EHISs) in Malawi, Zambia, and Zimbabwe. The study revealed high levels of optimism for EHISs coupled with hesitation about successful transition. The key challenges could be addressed through the technical design of systems, stakeholder coordination, and increasing organizational capacity to sustain and improve such systems (Moucheraud et al., 2017). Regardless of which system is used, the elements of interoperability and the generation of feedback to inform providers and administrators are critical to establishing a learning system (see Chapter 8) and being able to measure quality.
Access to Medicines
A leading cause of poor health outcomes in low-resource settings is poor access to medicines, often due to inadequate capacity of in-country supply chains to forecast, procure, and deliver essential commodities (Dowling, 2011). In Kenya, for example, a 2013 service availability and readiness assessment mapping study found that “[non]availability of medicines is commonly cited as the most important element of quality by health care
consumers, and the absence of medicines is a key factor in the underuse of public health services” (Ministry of Health, 2013). If they cannot procure the right medicines or if patients instead find substandard medications at a nearby pharmacy, it is extremely difficult for providers to deliver effective care. Patient dispensing sites frequently experience stockouts even when adequate stocks of medical commodities exist at the central or provincial level (PwC, 2017). The challenge of distributing goods in this “last mile” is pervasive in low-resource settings. Even when medicines do make it to sales points, moreover, there is a danger that substandard and counterfeit medicines will enter the supply chain. These products often contain no active ingredient, leading health systems to waste resources. Other falsified products may have weakened active ingredients and, even more dangerous, toxic compounds, posing a potential danger to patients (WHO, 2018c). Whether the illness is infectious and acute or longer term and chronic, treatments with weakened or inappropriate ingredients can have serious adverse effects.
On the opposite end of the spectrum of access, the overuse of medications and services has increasingly become a problem in many countries. Overuse of unnecessary services can harm patients physically and psychologically, and can harm health systems by wasting resources, some of which are in short supply (Brownlee et al., 2017). In the United States, at least 30 percent of antibiotic prescriptions in an outpatient setting are unnecessary (Incze et al., 2018). One study found urgent care centers and retail clinics—both on track for high growth—to be underrecognized sources of antibiotic prescribing (Palms et al., 2018). In Europe, researchers found that one-half of patients were prescribed unnecessary antibiotics (Brownlee et al., 2017). Providing the right medication, in the right dosage, and at the right time are all critical factors for health care quality.
Financing
Despite the high priority accorded to UHC on political agendas, health care financing models in many countries fail to extend high quality health care to their populations while also protecting them from impoverishment. With few financial resources available and with patchwork health care coverage, a majority of people living in low-resource settings are forced to forego or delay treatment, which exacerbates the fragmentation of the care they do receive and impairs their health outcomes. Furthermore, without a sustainable source of revenue, health care facilities can experience stockouts; fail to deliver care that meets clinical guidelines; or engage in aberrant behavior, such as patient detention, in an effort to garner revenue. These problems related to the financing of UHC are discussed in more detail in Chapter 7.
Leadership and Governance
Leadership at all levels is vital for a health care organization, both to optimize operations and to shape culture. Further challenging many countries is the rapid turnover of leaders within ministries of health, as many decisions affecting the health care of the country come from a centralized level. High staff turnover within ministries of health results in excessive costs, a decline in efficiency, and compromised quality. Demirkiran and colleagues (2016) found that a decrease in organizational performance can result from delays in filing vacated positions and difficulties in finding qualified candidates. Reducing staff turnover within health ministries would allow for more focus on long-term health programs that will yield improvement in health care quality.
Because of this challenge and other issues, there is a dearth of managerial and executive expertise in LMICs. Unlike high-income countries, however, LMICs can have difficulty relying on a cycle of searches and appointments. Rather, leaders must evolve into their roles, growing through their experiences. Under these circumstances, the culture of an institution can become extremely important for developing leaders. If an organization does not allow for learning and growth to take place, emerging leaders will be more reactive and less strategic. Furthermore, without checks and a culture of professionalism in place, resource capture and other aberrant behaviors, such as absenteeism and misuse of resources, can occur. In fact, leadership and governance of a country too often are tainted by corruption and collusion, as discussed further in Chapter 6.
A POOR PATIENT JOURNEY
Given the fragmented nature of health care delivery in LMICs and the weaknesses in health system building blocks discussed above, it is crucial to view health care quality not just as a point estimate that applies during one clinical encounter. Rather, health care quality is appropriately considered essentially as a longitudinal concept, a collection of properties of care that patients experience over an extended period of time. This observation is reminiscent of Vincent and Amalberti’s (2016) expanded view of the concept of one specific quality domain—patient safety. Unfortunately, many health care professionals are trained to practice with a focus on individual clinical encounters—a myopic perspective reinforced by dichotomous metrics, fragmented payment systems, and simplistic targets. Instead, this report emphasizes the importance of the patient journey, defined as follows:
The patient journey consists of the myriad interactions that patients have with the health care system, health care providers (formal and informal),
and families and friends and among themselves. These interactions occur over time and across multiple health care settings, such as clinics and hospitals, and within communities. The spatio-temporal interactions and transitions in care experienced by a person constitute the essence of the patient journey.
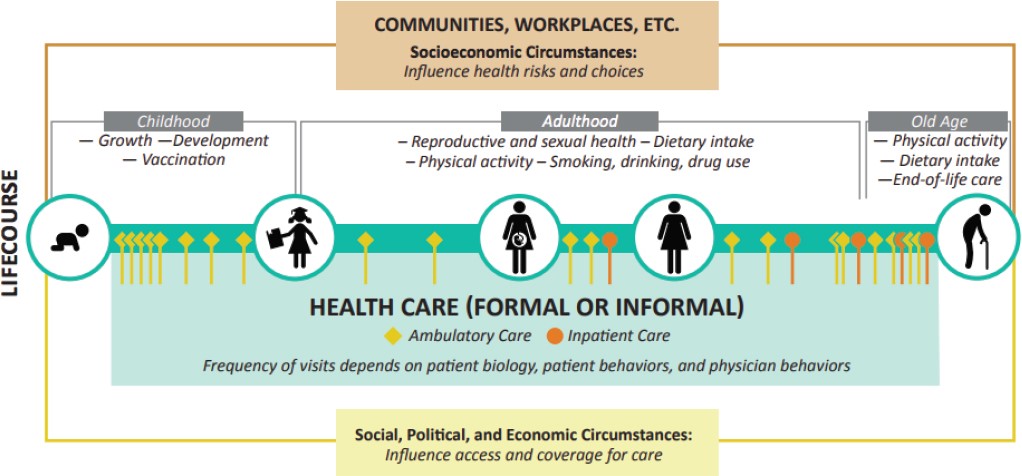
Given that fragmented care harms the quality of health care, improving quality will require improving the patient journey. Doing so will in turn require understanding the challenges that occur when patients transition among care settings and in between clinical visits. One crucial challenge is the issue of “health literacy,” or “the degree to which individuals have the capacity to obtain, process, and understand basic health information and services needed to make appropriate health decisions” (IOM, 1990, p. 4). Health literacy influences not only communication at a health facility but also how a person understands health and health care, such as the value of treatment adherence, after leaving a facility (Foubister, n.d.). Experts believe that health literacy is dynamic and can change as a person continually interacts with a health care system (Malik et al., 2017). This perspective is especially important given that people’s needs, motivations, and health literacy levels can evolve throughout their lives. Thus, the committee sees the patient’s journey, depicted in Figure 1-1, as an important aspect of health care quality. People’s interactions can occur in person or virtually, but will also be impacted by surrounding socioeconomic factors or political and geographical factors, which may influence their decision making (see Figure 1-1).
The Structure-Process-Outcome (SPO) model articulated by Avedis Donabedian (1988), a physician and the founder of the study of quality in health care and medical outcomes research, lends a process perspective that is useful for understanding these challenges. By introducing three areas of assessment for quality, the SPO model offers windows through which to understand the interaction of patients and care delivery. Also important in this equation, however, is the notion of context. Although many process-oriented frameworks have arisen in response to the SPO model, most of them ignore the perspective of the patient, and the fact that a patient’s experiences can influence both care-seeking behavior and adherence to care. The concept of the patient journey is intended to fill this gap.
Improving the patient journey requires in turn that patients be empowered and brought to the center of health care decision making. To achieve this, governments and health systems need to make a concerted effort to educate people about what high-quality care looks like and how their decisions can affect their own health. Emerging health care technologies can facilitate this endeavor (as discussed further in Chapter 3), but to fully realize the potential of optimizing the patient journey, policy makers
and health care leaders need to consider key influencing factors, including health system levels, the well-being of health care providers, and the private sector’s role in the delivery of care.
Influence of Health System Levels
Though not explicitly diagrammed in the 2001 Crossing the Quality Chasm report (IOM, 2001), an underlying framework guided the committee that produced that report, as documented by Berwick (2002) following the report’s release. Driven by a systems-thinking perspective and an acknowledgment that health care outcomes depend on upstream organizational processes and the policy and regulatory environment, this framework has four levels, depicted in Figure 1-2.
Figure 1-2 shows that the patient experience is influenced by the “microsystem” or the setting in which health care is delivered. This could be represented as a health care team. The “microsystem” is further influenced by the “organization,” such as the hospital in which the health care team works. Lastly, all three are influenced by upstream factors from the surrounding policy and regulatory “environment.” Given the committee’s emphasis on the patient journey and people’s experience with the health care system, the influence of the more distal organizational and environmental levels is important to consider. It is widely known that upstream inefficiencies can cascade down to the clinical encounter and result in a degradation of quality (Cook and Woods, 1994). Too often, blame for medical errors is assigned to the health care worker, and incident analysis and root-cause analysis frequently fail to consider broader system failures (Leistikow et al., 2017; Peerally et al., 2017). Berwick’s (2002) framework offers a valuable perspective that poor-quality care is often a consequence of upstream factors.
Influence of the Well-Being of Providers
The committee unequivocally embraces the centrality of the patient experience in defining and pursuing quality, but it also recognizes that the experience of health care providers is equally important to high-quality health care. Reports of burnout among physicians and nurses are common in high-income countries and are the topic of many discussions (Dyrbye et al., 2017). The issue is emerging in LMICs as well, with a systematic review finding levels of burnout similar to those among family doctors in Canada and Europe, as well as general internists in the United States (Dugani et al., 2018). Another study, in Kenya, found a burnout rate of more than 95 percent of medical workers at Kenyatta National Hospital in 2014, with the work environment being identified as the major contributor (Kokonya et al., 2014). In turn, health care providers’ burnout, stress, and defective

SOURCE: Adapted from Berwick, 2002.
work environments are linked to poor patient experiences and health outcomes (Bodenheimer and Sinsky, 2014). Therefore, improving care requires improving the well-being of the health care workforce, as failing to do so can lead to increased clinician burnout (Babbott et al., 2013). To better balance the agenda, many organizations have adopted the aim of improving the “work-life” of health care providers (Bodenheimer and Sinsky, 2014). The constraints and barriers faced by health care providers often fall within the “organizational” and “environmental” levels of the framework in Figure 1-2. These encompass ways in which organizations treat providers and the effects of new work processes and technologies, which can either ease or add to the workload constraints providers face. The committee believes that improving the “work-life” of health care providers is a goal germane to quality improvement in all health care systems, societies, and countries, regardless of income level or existing infrastructure.
Influence of the Private Sector’s Role in the Delivery of Care
In considering the patient journey, health care leaders would be remiss to ignore the role of the private sector in health care. Discussions of global health and quality of care sometimes stress the importance of the private sector in expanding access, with the assumption that market forces will drive quality improvements. However, no pervasive difference in quality has been found between government-run and privately run facilities (Berendes et al., 2011). In one systematic review, the private sector did rank higher in offering timely service and hospitality, but strong evidence showed as well that it violated medical standards and had low efficiency. Furthermore, the authors note that private-sector facilities had higher risks of low-quality care and lower transparency. These findings may partly be explained by the large and diverse nature of private-sector health care, which ranges globally from informal-sector traditional healers (discussed in Chapter 5); to unique health care innovators, such as Narayana Health Care and PurpleSource (discussed in Chapter 7); to high-tech health facilities serving as hubs for medical tourism (Medical Tourism Magazine, 2018).
Given the size and diversity of the private sector involved in health care and the predominance of informal providers, the private sector’s impact on health care quality—especially in light of the dearth of reliable data—cannot be ignored. A single patient’s journey can easily encompass both government-run and private-sector facilities or multiple types of private-sector facilities. Thus, the committee believes it is especially important to shed light on private providers and to include them in quality improvement efforts. Even though some private innovators, as mentioned above, are delivering high-quality care, their models are not always generalizable. Thus, they cannot serve as strong evidence for a blanket assertion that the private sector provides a simple route to improved quality (Sauerborn, 2001), no more than publicsector provision of services is a magic bullet solution to improving quality.
One challenge to better leveraging the strengths of the private sector is the lack of available information in this area. In part this is due to the private sector’s failure to publish data by which its performance could be evaluated (Basu et al., 2012). This finding is extremely salient for quality improvement efforts, since without data on quality problems, policy makers and other stakeholders cannot devise effective solutions. Another barrier to more streamlined, high-quality care is the fragmentation, discussed earlier, that plagues all sectors in health care. Recognizing these challenges, however, the private sector still represents a large portion of the health care sector in LMICs, serving more than half of the population in some countries. Public–private partnerships offer an opportunity for health care improvement, as they have done in the service of broader global health efforts, but leveraging them will require changes at the organizational and
environmental levels. Without affecting the system upstream and tailoring incentives at the right level, it will be difficult to help the lower levels of the microsystem and the patient experience achieve high-quality care.
CHARGE, APPROACH, AND SCOPE OF THIS STUDY
With the global momentum of the SDGs and UHC as a backdrop, combined with the previous decades of work on health care quality worldwide, the time is ripe for a deeper examination of the quality of care and its determinants globally. Several federal agencies, foundations, and private-sector partners came together to request that the National Academies of Sciences, Engineering, and Medicine (the National Academies) convene an ad hoc committee to conduct a study that would build on the wealth of quality work undertaken domestically and abroad and apply it to the global context (see Box 1-2 for the study’s full Statement of Task).
In the context of the signing of the SDGs in 2015 and the majority of countries now striving to cover entire populations with health care services, it is imperative that the continual improvement of quality be inextricably linked with the provision of care. Unless proper measures, oversight mechanisms, patient awareness, and health literacy are built into systems, it is possible that UHC efforts will provide access to poor-quality, even harmful care, accomplishing the opposite of what the SDGs were designed to achieve.
Approach
A 14-member committee was appointed in July 2017 to conduct this study, meeting four times over the course of the study. Three of these meetings included open sessions, soliciting input from expert speakers and members of the public. At the first meeting in October 2017, the study sponsors were invited to state their priorities and clarify their views of the charge to the committee, and additional expert testimony on quality improvement theory, methods, and experience was solicited. In the public session of the second committee meeting, held in Nairobi, Kenya, in December 2017, the focus was on the current state of health care quality, with invited testimony from regional health experts from the WHO Regional Offices for the Eastern Mediterranean (EMRO) and Africa (AFRO), as well as from innovators from East and West Africa. At the third meeting, hosted by the Institute of Global Health Innovation at Imperial College London, United Kingdom, in March 2018, the public session explored the future of health care quality. Subject-matter experts in the areas of ethics and regulatory issues for digital health were also consulted by telephone to obtain input to supplement the limited published research in these areas. (A list of those interviewed can be found in the acknowledgments section in the front of this report.) In March
2018, the committee also held a webinar with staff from the World Bank to learn more about their efforts in health care quality worldwide.
In developing its approach to this study, the committee recognized that the six quality dimensions described in the 2001 Crossing the Quality Chasm report (IOM, 2001) and listed earlier in Box 1-1 have continuing relevance despite being drafted nearly 20 years ago. Yet, while evidence has supported their continued importance, the vast majority of that evidence originates from high-income countries rather than from low-resource settings. The 2001 report also does not address issues of accountability and transparency and their fundamental relationship to achieving high-quality care delivery. Furthermore, understanding of the nature of “patient-centered care” has evolved in the intervening years. As a result, the committee decided to introduce a few modifications of the original six dimensions of quality to make them even more germane to low-resource settings and modern times:
- Expanding “patient-centeredness” to “person-centeredness”4: In all settings, modern sensibilities suggest that care should be organized to the extent possible around the needs and goals of each individual person rather than around disease categories or homogeneous groups (sometimes summarized as “What matters to you?” medicine rather than “What is the matter with you?” medicine) (Barry and Edgman-Levitan, 2012). Such a focus, in addition to an emphasis on improving health literacy, allows services to be more responsive, more effective, and more acceptable. Accordingly, interest has recently grown in “co-designed” and “co-produced” health care, with the aim of ensuring that people can be full partners in service delivery design and governance and in improving their own health (WHO, 2010).
- Broadening “timeliness” to include “accessibility and affordability”: This important distinction incorporates financial risk protection firmly into the definition of quality. While financial protection has been subsumed by some in the past within the dimension of “access,” the committee believes that, especially in low-resource settings, financial risk protection warrants being specified, because without it the quality of care is in severe jeopardy. For example, if there is no health care facility nearby that is financially accessible, people may either forego care they need or seek some kind of treatment from an informal provider with unknown education or train-
___________________
4 While the committee is endorsing this change in the language moving forward, many studies published in the past two decades measure and refer to “patient-centeredness.” Where those studies are mentioned in this report, the term “patient-centeredness” is preserved.
- ing. In the worst scenarios, people may even be denied emergency care unless they can pay for services up front, or suffer abuses in exchange for their inability to pay (Fagan, 2017) (see Chapter 7).
- Accounting for corruption and integrity as determinants of quality: The committee believes that acknowledging the importance of accountability and transparency for quality of care brings needed attention to the pervasive corruption and collusion that adversely affect health care around the world (see Chapter 6). Corrupt behaviors in health care occupy a spectrum. On one end are administrative and operational practices that are, in fact, aimed at redirecting and pilfering resources for private gain. On the other end, corruption entails state capture, which stems from weak capacity of state institutions and diminished accountability. This can cause health care resources to be depleted by vested economic interests of the powerful elite.
Thus, this report uses the updated six dimensions to guide quality measurements:
- Safety: Avoiding harm to patients from the care that is intended to help them.
- Effectiveness: Providing services based on scientific knowledge to all who could benefit, and refraining from providing services to those not likely to benefit (that is, avoiding both overuse of inappropriate care and underuse of effective care).
- Person-centeredness: Providing care that is respectful of and responsive to individual preferences, needs, and values and ensuring that people’s values guide all clinical decisions. Care transitions and coordination should not be centered on health care providers, but on recipients.5
- Accessibility, Timeliness, Affordability: Reducing unwanted waits and harmful delays for both those who receive and those who give care; reducing access barriers and financial risk for patients, families, and communities; and promoting care that is affordable for the system.
- Efficiency: Avoiding waste, including waste of equipment, supplies, ideas, and energy, and including waste resulting from poor management, fraud, corruption, and abusive practices. Existing
___________________
5 Note on the language used throughout this report: Although this report uses the term patient when referring to the recipient of clinical medicine services, the committee’s position remains that quality improvement requires emphasis on the person, to remind the reader that health is determined by circumstances far beyond the clinical setting.
- resources should be leveraged to the greatest degree possible to finance services.
- Equity: Providing care that does not vary in quality because of personal characteristics such as gender, ethnicity, race, geographic location, and socioeconomic status.
Scope
In conducting this study, the committee focused on the interface between the health system user and the care provider and on how quality at that interface can best be assured and improved. Other important components of the health system, especially public health protections and social determinants of health, can of course contribute greatly to the overall health of a population and also can benefit from attention to quality improvement, but they are not a primary focus of this report. The committee acknowledges this gap, and hopes that additional reports will soon address those crucial components. Other areas and issues that will require additional study and more focused examination are numerous, and include, among others, settings of extreme adversity; supply chains; pharmaceutical integrity; surgery and cancer; mental health and substance abuse; and dental care.
Another important choice the committee made was to focus not only on low-income nations but on low-resource settings within all nations. While many reports are segmented by country wealth or income level, the committee recognizes that poor populations are found across the world, including within middle-income and wealthy nations. As health care continues to advance, and patients receive care transnationally or from multinational companies, the committee believes that purely national lines will fail to capture quality of care adequately. For instance, just as deleterious effects from poor quality can occur in high-income countries, such as the United States (Jewett and Alesia, 2018), so too can examples of quality improvement be found in low-income settings.
Innovations from low-income settings can be adopted and adapted widely. In fact, Lord Nigel Crisp, author of Turning the World Upside Down, argues that bringing developing countries to the same playing field as developed nations creates an open exchange of ideas, informed by the realization that between low- and high-income settings, learning is not one-way (Crisp, 2018). In Mozambique and Pakistan, for example, midlevel workers are successfully trained to complete procedures that require a full professional education, such as caesarean sections or cataract operations. No clinically significant difference in outcomes has been proven between the surgeries performed by midlevel health workers and physicians. Thus,
this workforce innovation has increased the access of communities to services and treatments without compromising quality of care (Crisp, 2010). Crisp notes that the North American system is designed for an age of acute care, which, given epidemiological trends, is becoming an increasingly inappropriate and unaffordable focus (Smith, 2010). Some organizations are already beginning to recognize the need for this global information exchange, especially in terms of research where certain low-income populations may share more similarities with cohorts in other countries than with their own fellow citizens (Evangelista, 2018). The committee expects great benefit from bidirectional information flows and learning networks, recognizing that ongoing attention to and improvement of quality is a global challenge that requires all hands on deck to address.
A Note on the Committee’s Recommendations
The committee recognizes that the recommendations offered in Chapters 2 through 8 of this report are aspirational, requiring in many cases transformative efforts that will necessitate combined and sustained action on the part of the full range of governments, leaders, and organizations worldwide involved at every level of the health care enterprise. However, the committee believes that the evidence reviewed in this report clearly demonstrates the need to think big while also identifying specific actions that, collectively, can advance global health care toward a quality system that meets the needs of all the world’s citizens, including those in the most resource-poor regions. To this end, the committee offers a set of overarching principles for the transformation of health care worldwide (see Chapter 2), along with specific actions that can be taken by all stakeholders to achieve a transformed system that reflects these principles. Some of these actions can be taken in the near term, while others will require efforts that extend over the mid- to long term. Overall, the committee wishes to stress that the somewhat overwhelming scope of the transformation needed to achieve quality health care for all globally should not deter efforts to take the steps that can lead, over time and with focused dedication, to realizing improvements. We also realize that when presented with so many areas to work on and high level approaches to operationalize, leaders may wonder where to begin. While prioritizing the recommendations and interventions proposed in this report would be an extremely valuable contribution, the committee believes that doing so is beyond the scope of this study. There is no silver bullet solution, and each country and health system will need to tailor its approaches according to needs of its populations. It is our hope that future projects can gather national and regional stakeholders to take on the crucial task of setting priorities for action.
ORGANIZATION OF THE REPORT
Part I of this report presents the committee’s view of “The Ideal Vision for Future Health Care.” It begins in Chapter 2 by describing changes that will be necessary to improve quality at the systems level—mainly mastering and using systems thinking and system-level designs, as well as shifting the focus and ownership of health matters to empowered and educated users and communities. Chapter 3 then explores what the world can expect from future health systems. Many innovations are already in use and will become more widespread, and others, though nascent today, have the potential to fundamentally transform how people seek and receive care. Thus, it is essential for the pursuit of quality to attend not only to current care delivery systems but also to those that will soon emerge, and even become dominant.
Part II, “The Current State of Quality in Health Care,” includes Chapters 4 through 6. Chapter 4 explores the current state of data on global health care quality and the lack of the evidence and metrics needed to ensure that quality is being adequately measured to drive improvement in the defective processes of care that are currently widespread. Chapter 5 calls attention to the billions across the world who fall outside of formal health care systems, including those whose care comes from informal providers and those in settings of extreme adversity where health care is scarce and infrastructures absent. Chapter 6 highlights the negative health impacts of corruption in the health sector and how tools outside the health sector can be used to address this important problem.
Finally, Part III, “The Path to Continual Global Improvement,” includes Chapters 7 and 8, presenting strategies and recommendations for achieving the ideal vision laid out in Part I. Chapter 7 outlines the commitment that will be necessary for countries to enable both current and future systems of care to meet their potential and ensure that quality is being built into UHC frameworks and systems. This chapter also describes what is known about the policy levers that can help induce better quality, especially through effective financing and incentives. Developing accountability for this commitment will require creating public demand for better quality, since the will for such change from within the current care system alone will be insufficient. Finally, Chapter 8 issues a call for creating an environment that supports a culture of learning, including in particular the leadership necessary for this culture to succeed. This chapter also outlines the research agenda identified by the committee as necessary to inform many of these quality initiatives.
REFERENCES
Adair-Rohani, H., K. Zukor, S. Bonjour, S. Wilburn, A. C. Kuesel, R. Hebert, and E. R. Fletcher. 2013. Limited electricity access in health facilities of sub-Saharan Africa: A systematic review of data on electricity access, sources, and reliability. Global Health: Science and Practice 1(2):249–261. doi:10.9745/GHSP-D-13-00037.
Akhlaq, A., B. McKinstry, K. B. Muhammad, and A. Sheikh. 2016. Barriers and facilitators to health information exchange in low- and middle-income country settings: A systematic review. Health Policy and Planning 31(9):1310–1325.
Allegranzi, B., S. B. Nejad, C. Combescure, W. Graafmans, H. Attar, L. Donaldson, and D. Pittet. 2011. Burden of endemic health-care-associated infection in developing countries: Systematic review and meta-analysis. The Lancet 377(9761):228–241.
Babbott, S., L. Manwell, R. Brown, E. Montague, W. Eric, M. Schwartz, E. Hess, and M. Linzer. 2013. Electronic medical records and physician stress in primary care: Results from the MEMO Study. Journal of the American Medical Informatics Association 21(e1):e100–e106. doi:10.1136/amiajnl-2013-001875.
Barber, R. M., N. Fullman, R. J. D. Sorensen, T. Bollyky, M. McKee, E. Nolte, A. A. Abajobir, K. H. Abate, C. Abbafati, K. M. Abbas, et al. 2017. Healthcare access and quality index based on mortality from causes amenable to personal health care in 195 countries and territories, 1990–2015: A novel analysis from the Global Burden of Disease Study 2015. The Lancet 390(10091):231–266.
Barker, P. 2017. Methods to implement quality for health systems in low and middle income country settings. Paper read at Meeting 1: Improving the Quality of Health Care Globally, Washington, DC. http://www.nationalacademies.org/hmd/Activities/Global/GlobalQualityofCare/2017-OCT-18/Videos/Session-2-Videos/9-Barker-Video.aspx (accessed August 7, 2018).
Barry, M. J., and S. Edgman-Levitan. 2012. Shared decision making—the pinnacle of patient-centered care. New England Journal of Medicine 366(9):780–781.
Basu, S., J. Andrews, S. Kishore, R. Panjabi, and D. Stuckler. 2012. Comparative performance of private and public healthcare systems in low- and middle-income countries: A systematic review. PLoS Medicine 9(6):e1001244.
Ben-Tovim, D. I., M. L. Doughtery, T. J. O’Connell, and K. M. McGrath. 2008. Patient journeys: The process of clinical redesign. The Medical Journal of Australia 188(6 Suppl.):S14–S17.
Berendes, S., P. Heywood, S. Oliver, and P. Garner. 2011. Quality of private and public ambulatory health care in low and middle income countries: Systematic review of comparative studies. PLoS Medicine 8(4):e1000433.
Berwick, D. 2002. A user’s manual for the IOM’s “quality chasm” report. Health Affairs 21(3):80–90.
Bhadelia, N. 2016. Rage against the busted medical machines. Goats and Soda, September 8. https://www.npr.org/sections/goatsandsoda/2016/09/08/492842274/rage-against-thebusted-medical-machines (accessed May 10, 2018).
Bodenheimer, T., and C. Sinsky. 2014. From triple to quadruple aim: Care of the patient requires care of the provider. The Annals of Family Medicine 12(6):573–576.
Brownlee, S., K. Chalkidou, J. Doust, A. G. Elshaug, P. Glasziou, I. Health, S. Nagpal, V. Siani, D. Srivastava, K. Chalmers, and D. Korenstein. 2017. Evidence for overuse of medical services around the world. The Lancet 390(10090):156–168.
Cook, R. I., and D. Woods. 1994. Operating at the sharp end: The complexity of human error. In Human error in medicine, edited by M. S. Bogner. Hillsdale, NJ: Lawrence Erlbaum Associates. Pp. 255–310.
Crisp, L. N. 2010. Turning the world upside down. In Commonwealth Health Ministers’ Update 2010, edited by Commonwealth Secretariat. London, UK: Pro Book. Pp. 89–93.
Crisp, L. N. 2018. Turning the world upside down. http://nigelcrisp.com/turning-the-world-upside-down (accessed May 15, 2018).
Cronk, R., and J. Bartram. 2018. Environmental conditions in health care facilities in low- and middle-income countries: Coverage and inequalities. International Journal of Hygiene and Environmental Health 221(3):409–422.
Daniels, B., A. Dolinger, G. Bedoya, K. Rogo, A. Goicoechea, J. Coarasa, F. Wafula, N. Mwaura, R. Kimeu, and J. Das. 2017. Use of standardised patients to assess quality of healthcare in Nairobi, Kenya: A pilot, cross-sectional study with international comparisons. BMJ Global Health 2(2):e000333.
Das, J. 2011. The quality of medical care in low-income countries: From providers to markets. PLoS Medicine 8(4):e1000432.
Demirkiran, M., R. Erdem, and S. Taskaya. 2016. Reflections of qualified personnel turnover to the Ministry of Health of the Republic of Turkey: A phenomenological research. Journal of Management, Marketing, and Logistics 3(1). doi:10.17261/Pressacademia.2016116528.
Donabedian, A. 1988. The quality of care: How can it be assessed? Journal of the American Medical Association 260(12):1743–1748.
Dowling, P. 2011. Healthcare supply chains in developing countries: Situational analysis. Task Order 4. Arlington, VA: USAID Deliver Project.
Dugani, S., H. Afari, L. Hirschhorn, H. Ratcliffe, J. Veillard, G. Martin, G. Lagomarsino, L. Basu, and A. Bitton. 2018. Prevalence and factors associated with burnout among frontline primary health care providers in low- and middle-income countries: A systematic review. Gates Open Research 2:4. doi:10.12688/gatesopenres.12779.3.
Dyrbye, L. N., T. D. Shanafelt, C. Sinsky, P. Cipriano, J. Bhatt, A. Ommaya, C. West, and D. Meyers. 2017. Burnout among health care professionals: A call to explore and address this underrecognized threat to safe, high-quality care. Washington, DC: National Academy of Medicine. https://https://nam.edu/burnout-among-health-care-professionals-a-callto-explore-and-address-this-underrecognized-threat-to-safe-high-quality-care (accessed May 31, 2018).
Evangelista, A. 2018. In health research, local efforts have global benefit. http://ucghi.universityofcalifornia.edu/news/health-research-local-efforts-have-global-benefit (accessed June 10, 2018).
Fagan, L. 2017. Report: From Cameroon to Kenya, hospitals violate patient rights over bills. Africa Times, December 10. https://africatimes.com/2017/12/10/report-from-cameroon-to-kenya-patient-rights-violated-over-hospital-bill-payment (accessed June 10, 2018).
Foubister, V. n.d. Issue of the month: Health literacy—a quality and patient safety imperative. https://www.commonwealthfund.org/publications/newsletter/issue-month-health-literacy-quality-and-patient-safety-imperative (accessed July 10, 2018).
Gibbons, L., J. Belizán, J. A Lauer, A. Betrán, M. Merialdi, and F. Althabe. 2010. The global numbers and costs of additionally needed and unnecessary caesarean sections performed per year: Overuse as a barrier to universal coverage health systems financing. World Health Report Background Paper 30. Geneva, Switzerland: WHO.
Goeschel, C. 2011. Defining and assigning accountability for quality care and patient safety. Journal of Nursing Regulation 2(1):28–35. https://www.ncsbn.org/Defining_and_Assigning_Accountability.pdf (accessed August 7, 2018).
Healy, S. 2015. The value of service to overcome “machine graveyards.” Gradian Health Systems. https://www.gradianhealth.org/the-value-of-service-to-overcome-machine-graveyards (accessed August 6, 2018).
Horton, R. 2018. Offline: UHC—one promise and two misunderstandings. The Lancet 391(10128):1342.
Howie, S. R. C., S. E. Hill, D. Peel, M. Sanneh, M. Njie, P. C. Hill, K. Mulholland, and R. A. Adegbola. 2008. Beyond good intentions: Lessons on equipment donation from an African hospital. Bulletin of the World Health Organization 86(1):52–56.
Howitt, P., A. Darzi, G. Yang, H. Ashrafian, R. Atun, J. Barlow, A. Blakemore, A. Bull, J. Car, L. Conteh, et al. 2012. Technologies for global health. Lancet 380(9840):507–535.
Incze, M. A., R. F. Redberg, and M. H. Katz. 2018. Overprescription in urgent care clinics—the fast and the spurious. JAMA Internal Medicine. doi:10.1001/jamainternmed.2018.1628.
IOM (Institute of Medicine). 1990. Medicare: A strategy for quality assurance, volume I. Edited by K. N. Lohr. Washington, DC: National Academy Press.
IOM. 2001. Crossing the quality chasm: A new health system for the 21st century. Washington, DC: National Academy Press.
Jain, V., and A. Alam. 2017. Redefining universal health coverage in the age of global health security. BMJ Global Health 2(2):e000255.
Jewett, C., and M. Alesia. 2018. How a push to cut costs and boost profits at surgery centers led to a trail of death. USA Today, March 5. https://www.usatoday.com/story/news/2018/03/02/medicare-certified-surgery-centers-safety-deaths/363172002 (accessed May 11, 2018).
Jones, A. 2013. Medical equipment donated to developing nations usually ends up on the junk heap. Scientific American, May 6. https://www.scientificamerican.com/article/medical-equipment-donated-developing-nations-junk-heap (accessed May 31, 2018).
Keepnews, D., and P. Mitchell. 2003. Health systems accountability for patient safety. Online Journal of Issues in Nursing 8(3).
Kokonya, D., J. Mburu, D. Kathuku, D. Ndetei, and A. Adam. 2014. Burnout syndrome among medical workers at Kenyatta National Hospital (KNH), Nairobi, Kenya. Journal of Psychiatry 17:142. doi:10.4172/Psychiatry.1000142.
Kripalani, S., F. LeFevre, C. O. Phillips, M. V. Williams, P. Basaviah, and D. W. Baker. 2007. Deficits in communication and information transfer between hospital-based and primary care physicians: Implications for patient safety and continuity of care. Journal of the American Medical Association 297(8):831–841.
Leistikow, I., S. Mulder, J. Vesseur, and P. Robben. 2017. Learning from incidents in healthcare: The journey, not the arrival, matters. BMJ Quality & Safety 26(3):252–256.
Makary, M. A., and M. Daniel. 2016. Medical error—the third leading cause of death in the U.S. British Medical Journal 353:i2139.
Malik, M., R. Z. Zaida, and A. Hussain. 2017. Health literacy as a global public health concern: A systematic review. Journal of Pharmacology & Clinical Research 4(2). doi:10.19080/JPCR.2017.04.555632.
Meara, J. G., A. J. M. Leather, L. Hagander, B. C. Alkire, N. Alonso, E. A. Ameh, S. W. Bickler, L. Conteh, A. J. Dare, J. Davies, et al. 2015. Global surgery 2030: Evidence and solutions for achieving health, welfare, and economic development. The Lancet 386(9993):569–624.
Medical Tourism Magazine. 2018. Optimizing healthcare infrastructure to boost medical tourism. Medical Tourism Magazine, April 17. http://www.medicaltourismmag.com/ optimizing-healthcare-infrastructure-boost-medical-tourism (accessed May 31, 2018).
Meshkati, N. 1989. Technology transfer to developing countries: A tripartite micro- and macroergonomic analysis of human-organization-technology interfaces. International Journal of Industrial Ergonomics 4(2):101–115.
Ministry of Health. 2013. Kenya Service Availability and Readiness Assessment Mapping (SARAM) report, 2013. Nairobi, Kenya: Ministry of Health. apps.who.int/healthinfo/systems/datacatalog/index.php/catalog/42/download/145 (accessed May 31, 2018).
Mohan, P. 2017. Labour-migrants: Excluded from universal health care in India. http://bhs.org.in//?s=migrant+workers (accessed June 10, 2018).
Moucheraud, C., A. Schwitters, C. Boudreaux, D. Giles, P. Kilmarx, N. Ntolo, Z. Bangani, M. E. S. Louis, and T. Bossert. 2017. Sustainability of health information systems: A three-country qualitative study in Southern Africa. https://bmchealthservres.biomedcentral.com/articles/10.1186/s12913-016-1971-8 (accessed June 10, 2018).
NASEM (National Academies of Sciences, Engineering, and Medicine). 2018. The safety and quality of abortion care in the United States. Washington, DC: The National Academies Press. https://doi.org/10.17226/24950.
Ng, M., N. Fullman, J. L. Dieleman, A. D. Flaxman, C. J. L. Murray, and S. S. Lim. 2014. Effective coverage: A metric for monitoring universal health coverage. PLoS Medicine 11(9):e1001730.
Nishtar, S. 2010. Choked pipes: Reforming Pakistan’s mixed health system. Oxford, UK: Oxford University Press.
Palms, D. L., L. A. Hicks, M. Bartoces, A. L. Hersh, R. Zetts, D. Y. Hyun, and K. E. FlemingDutra. 2018. Comparison of antibiotic prescribing in retail clinics, urgent care centers, emergency departments, and traditional ambulatory care settings in the United States. JAMA Internal Medicine. doi:10.1001/jamainternmed.2018.1632.
Peerally, M. F., S. Carr, J. Waring, and M. Dixon-Woods. 2017. The problem with root cause analysis. BMJ Quality & Safety 26(5):417.
Perry, L., and R. Malkin. 2011. Effectiveness of medical equipment donations to improve health systems: How much medical equipment is broken in the developing world? Medical & Biological Engineering & Computing 49(7):719–722.
Pesec, M., H. L. Ratcliffe, A. Karlage, L. R. Hirschhorn, A. Gawande, and A. Bitton. 2017. Primary health care that works: The Costa Rican experience. Health Affairs 36(3):531–538.
Picard, A. 2010. Universal health care matters, but so does quality. https://www.theglobeandmail.com/life/health-and-fitness/universal-health-care-matters-but-so-doesquality/article1387165 (accessed May 14, 2018).
Puchalski Ritchie, L. M., S. Khan, J. E. Moore, C. Timmings, M. van Lettow, J. P. Vogel, D. N. Khan, G. Mbaruku, M. Mrisho, K. Mugerwa, et al. 2016. Low- and middle-income countries face many common barriers to implementation of maternal health evidence products. Journal of Clinical Epidemiology 76:229–237. doi:10.1016/j.jclinepi.2016.02.017.
PwC (PricewaterhouseCoopers). 2017. Improving global health outcomes through last mile logistics: Special focus forum—global health and humanitarian supply chains. https://www.pwc.com/us/en/industries/health-services/global-health-outcomes-through-last-milelogistics.html (accessed May 31, 2018).
Rasanathan, K., T. O’Connell, J. Yablonski, D. Anthony, and N. Rees. 2016. Brief: Moving towards universal health coverage to realize the right to healthcare for every child. In UNICEF approach to health system strengthening. New York: UNICEF. https://www.unicef.org/health/files/UHC_UNICEF_FINAL.pdf (accessed August 8, 2018).
Renschler, J. P., K. M. Walters, P. N. Newton, and R. Laxminarayan. 2015. Estimated under-five deaths associated with poor-quality antimalarials in sub-Saharan Africa. The American Journal of Tropical Medicine and Hygiene 92(6 Suppl.):119–126.
Sauerborn, R. 2001. Low quality of care in low income countries: Is the private sector the answer? International Journal for Quality in Health Care 13(4):281–282.
Sayinzoga, F., and L. Bijlmakers. 2016. Drivers of improved health sector performance in Rwanda: A qualitative view from within. BMC Health Services Research 16(1):123. doi:10.1186/s12913-016-1351-4.
Schrag, D., F. Xu, M. Hanger, E. Elkin, N. A. Bickell, and P. B. Bach. 2006. Fragmentation of care for frequently hospitalized urban residents. Medical Care 44(6):560–567.
Scott, K. W., and A. K. Jha. 2014. Putting quality on the global health agenda. New England Journal of Medicine 371(1):3–5.
Smith, R. 2010. Time to turn the world upside down. British Medical Journal 340:c918.
Speybroeck, N., Y. Kinfu, M. Dal Poz, and D. B Evans. 2006. Reassessing the relationship between human resources for health, intervention coverage and health outcomes. https://pdfs.semanticscholar.org/fb21/eb31a783e802b2869f291ad29c80bf26ff04.pdf (accessed May 31, 2018).
Starr, P. 1982. The social transformation of American medicine: The rise of a sovereign profession and the making of a vast industry. New York: Basic Books.
The Dartmouth Atlas of Health Care. 2015. Understanding the efficiency and effectiveness of the health care system. http://www.dartmouthatlas.org (accessed July 15, 2018).
UN (United Nations). 2017. Sustainable Development Goal 3: Ensure healthy lives and promote well-being for all at all ages. https://sustainabledevelopment.un.org/sdg3 (accessed May 11, 2018).
UNDP (United Nations Development Programme). 2015. World leaders adopt Sustainable Development Goals. http://www.undp.org/content/undp/en/home/presscenter/pressreleases/2015/09/24/undp-welcomes-adoption-of-sustainable-development-goals-byworld-leaders.html (accessed May 11, 2018).
Vincent, C., and R. Amalberti. 2016. Safer healthcare: Strategies for the real world. New York: Springer International Publishing. doi:10.1007/978-3-319-25559-0.
WHO (World Health Organization). 2007. The World Health Report 2007—a safer future: Global public health security in the 21st century. Geneva, Switzerland: WHO.
WHO. 2008. Health information systems. Geneva, Switzerland: WHO.
WHO. 2010. Monitoring the building blocks of health systems: A handbook of indicators and their measurement strategies. Geneva, Switzerland: WHO.
WHO. 2015. Health in 2015: From MDGs, Millennium Development Goals to SDGs, Sustainable Development Goals. Geneva, Switzerland: WHO.
WHO. 2016. Health workforce requirements for universal health coverage and the sustainable development goals. Geneva, Switzerland: WHO.
WHO. 2018a. Draft thirteenth General Programme of Work 2019–2023. http://apps.who.int/gb/ebwha/pdf_files/EB142/B142_3-en.pdf (accessed May 31, 2018).
WHO. 2018b. Energy access and resilience. http://www.who.int/sustainable-development/health-sector/health-risks/energy-access/en (accessed May 14, 2018).
WHO. 2018c. Substandard and falsified medical products. http://www.who.int/news-room/fact-sheets/detail/substandard-and-falsified-medical-products (accessed May 20, 2018).
WHO and UNICEF (United Nations Children’s Fund). 2012. Progress on drinking water and sanitation. Geneva, Switzerland: WHO.
WHO and UNICEF. 2015. Water, sanitation and hygiene in health care facilities: Status in low- and middle-income countries and way forward. Geneva, Switzerland: WHO and UNICEF.
WHO and World Bank. 2015. Tracking universal health coverage: First global monitoring report. Geneva, Switzerland: WHO and World Bank.
WHO and World Bank. 2017. Tracking universal health coverage: 2017 global monitoring report. Geneva, Switzerland: WHO and World Bank.
WHO, OECD (Organisation for Economic Co-operation and Development), and World Bank. 2018. Delivering quality health services: A global imperative for universal health coverage. Geneva, Switzerland: WHO, OECD, and World Bank.
World Bank. 2000. Overview of rural decentralization in India: Volume 1. Washington, DC: World Bank.





























