
As discussed in Chapters 4 and 5, many people around the world lack access to quality health care services. The poor state of quality in many countries and the challenges that come with health care in austere settings are exacerbated when health care systems are continually degraded through corruption and collusion. Global health care expenditures total $7.35 trillion each year, much of which comes from out-of-pocket (OOP) payments by families, insurance reimbursements, and public funding. Coupled with a lack of transparency, this makes the health sector vulnerable to corruption. Gee and Button (2015) estimate that $455 billion of this total expenditure is lost each year to fraud and corruption. Additionally, unique in this sector, the demand for health care is not always predictable in any given facility or region and usually exceeds supply (Vian, 2002). With little leverage in such scenarios, patients and public funds can easily be taken advantage of, even by people who are supposed to be trusted. This problem plagues countries at all income levels. One-third of Organisation for Economic Co-operation and Development (OECD) citizens and 45 percent of global citizens believe the health sector is corrupt or very corrupt (OECD, 2017). In fact, in polls, the health care sector has been identified as one of the most corrupt sectors in many countries (Transparency International, 2006).
Corruption is a complex and multifaceted challenge. Offenses range from smaller-scale acts by doctors and nurses who charge bribes or “informal payments” to larger-scale acts at the ministerial or hospital administrator level, when people in power siphon money or redirect resources away from those who need it for their own benefit (Transparency International, 2006). The 2006 global corruption report produced by Transparency International identifies many of these issues, providing robust evidence and calls for action (Transparency International, 2006). Yet, more than 10 years after that report was issued, many countries and health systems are dealing with the same challenges. Box 6-1 presents brief vignettes of corruption found in India, Costa Rica, Cameroon, and Albania.
This chapter first describes the effects of corruption on the health outcomes of populations. It then outlines some of the more common types of corruption found in the health care sector. Next, the chapter details the challenges to effective universal health coverage (UHC) posed by corruption, illustrating that because of the many linkages among governance, spending, and health care, achieving UHC will be impossible unless corruption is addressed. Then, the committee offers strategies for reducing corruption in various areas and making the environments where corruption has thrived less attractive for those willing to deceive with malpractices. The final section presents a summary and recommendation.
THE IMPACT OF CORRUPTION ON THE HEALTH OF POPULATIONS
While an ongoing survey across 33 countries measuring public attitudes on democracy and governance provides evidence of a generally downward trend in the prevalence of corruption in Africa, the problem remains important in several countries (Kankeu, 2018). In its Quality Improvement Framework for Health 2011–2016, Tanzania acknowledges corruption as one of the major barriers to providing quality services (URT and Ministry of Health and Social Welfare, 2011). Similarly, in Uganda, participants in a 2012 study identified perceived corruption as one of the largest barriers to providing good care to injured patients (Bouchard et al., 2012). Ukraine, too, has acknowledged corruption as a cause for barriers to accessing health services and medical commodities (Mendel, 2017).
Corruption in the health sector has been found to take many forms in various areas, such as in health facility construction; equipment and supply purchasing; pharmaceutical distribution and use; health worker education; falsification of medical research; and perhaps most important for this report, the provision of health care services (Vian, 2008). The effects of corruption on a population’s health may not always be clear and direct, but they are present nonetheless and can degrade the system and negatively affect the health of a community or nation in multiple ways. In the Philippines, for example, corruption undermined immunization of children, increased patient wait times, decreased patient satisfaction, and reduced accessibility of clinics for treatment (Azfar and Gurgur, 2008). Research has also linked corruption to negative health impacts. In fact, 1.6 percent of annual deaths in children under 5 globally—more than 140,000
deaths—can be explained in part by corruption (Hanf et al., 2011). Furthermore, the International Monetary Fund (IMF) has estimated that infant and child mortality in countries with high levels of corruption is almost twice as high as that in countries with low levels of corruption (Gupta et al., 2002). While many impacts of corruption can be felt through the lack of access to clean water and adequate sanitation, this report focuses on the impacts experienced in the health care delivery system, especially when the quality of care is compromised. These impacts can take the form of poor staffing at facilities and longer wait times due to absenteeism, less equitable care, poor quality or little availability of drugs, and unnecessary additional financial burden. As Hanf and colleagues (2011) argue, donors and governments need to design indicators at the macro and micro levels to monitor the impacts of corruption on health efficiently and to view health, water and sanitation, and corruption as integral components in overcoming these linkages.
TYPES OF CORRUPTION IN HEALTH CARE
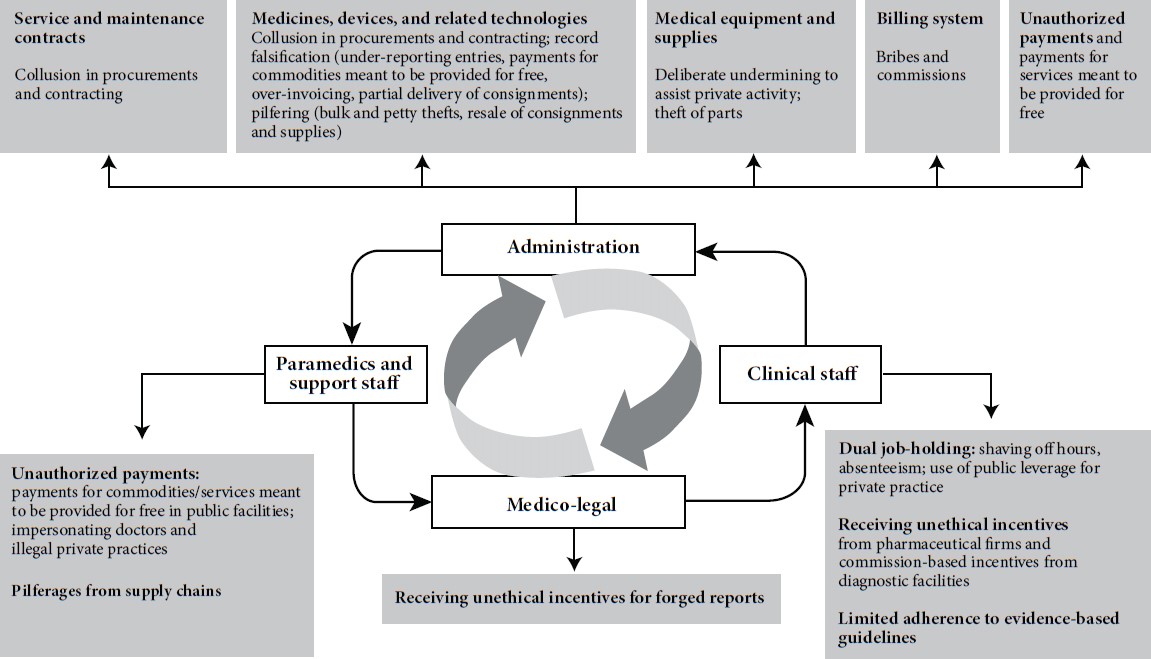
There are varying types of corruption—fiscal, intellectual, and ethical—as well as potential actors who may play a role in these malpractices (see Figure 6-1). While the lack of a paper trail makes it challenging for researchers to prove causation, many surveys have revealed associations between instances of corruption and consequences for those seeking health care. Previous studies have shown that people who report dysfunctions, such as absent doctors, drug stockouts, and long wait times, are also more likely to report paying bribes (Kankeu and Ventelou, 2016; Kankeu et al., 2016; Mokhtari and Ashtari, 2012). This relationship has been found in multiple countries according to a study using nationally representative samples from 33 African countries (Kankeu and Ventelou, 2016). Furthermore, when these data are aggregated to the national level, a similar pattern emerges (Kankeu, 2018). This section explores some of the more common types of corruption in health care: absenteeism, informal payments, fraud, and mismanagement of resources and theft of supplies.
Absenteeism
One of the most commonly cited forms of corruption is absenteeism of health care workers. This often occurs because they are working another job in the private sector, one that likely pays a higher salary, so when they are dually scheduled, the public sector typically suffers. In one of the recent Afrobarometer surveys, more than 50 percent of respondents across 25 countries reported absenteeism in a recent health care experience. This number ranged from 23 percent in Burundi to as high as 90 percent
SOURCE: Nishtar, S. 2010. Choked pipes—reforming Pakistan’s mixed health system. Journal of the Pakistan Medical Association 60(4):252–253.
Reproduced with permission of Oxford University Press Pakistan © Oxford University Press.
in Morocco (Kankeu, 2018). In many cases, absenteeism and the “ghost worker” phenomenon are prevalent where institutionalized corruption creates an environment that enables health care workers to be absent from duty in lieu of relinquishing a percentage of their salary, which is then shared institutionally (Nishtar, 2010). This absenteeism and the resulting uncertainty as to whether the public facilities will be properly staffed when patients need them lead to a reliance on providers in private clinics and thus the closing or underutilization of the public facilities (Nishtar, 2010). Moreover, those patients who still rely on the poorly staffed public facilities face long wait times and health care that is likely not person-centered.
Informal Payments
Informal payments (i.e., bribes or kickbacks) (Kankeu and Ventelou, 2016) are those made in kind or in cash by patients or relatives “outside official payment channels or are purchases meant to be covered by the health care system” (Lewis, 2007). These payments are often made directly to individual providers (Lewis, 2007) to either access care, avoid queues, receive more attention or better care, or even express gratitude (Kankeu and Ventelou, 2016; Maestad and Mwisongo, 2011). The payments are sometimes termed a “coping strategy” for health care workers to make up for remuneration that does not match their perceived efforts (Kankeu et al., 2016). Because health care workers’ salaries can be paltry, this pattern can appear to be an understandable part of a broken system. However, it is problematic when a high percentage of OOP spending is directed toward informal payments. A study in Uganda, for example, found that health care workers embezzled 68–77 percent of user fees (McPake et al., 1999). Additionally, a study investigating informal payments across 33 countries in Africa discovered that they can be highly regressive, with demands for informal payments and actual payments being concentrated among the poorest (Kankeu and Ventelou, 2016). It is important to note, however, that the range of frequency of informal payment is large—from 3 percent in Peru to 96 percent in Pakistan. While countries in South Asia have been found to have a heavy reliance on informal payments, the trend is mixed in other regions of the world (Lewis, 2007).
Studies have linked informal payments to negative impacts on the quality, efficiency, and equity of health care provision (Lewis, 2007; Stringhini et al., 2009; Szende and Culyer, 2006). A study in Cameroon found the practice to be more common in public than in private nonprofit facilities, but the highest incidence was found in private for-profit facilities, demonstrating the need for both sector-wide and sector-specific approaches (Kankeu et al., 2016). This finding also highlights the point that although salaries differ across sectors, that differential alone is clearly not sufficient
to prevent corrupt practices. Further enabling this type of malpractice is the use (and even lack of use) of paper records, which makes proper tracking of supplies and payments very difficult (Nishtar, 2010).
Fraud
Fraud appears to plague countries regardless of their income status. In the United States, for example, where significant resources are devoted to health care and automated payments are typically made to reimburse various types of insurance, fraud is well documented in the case of the national Medicaid and Medicare programs. For instance, the U.S. Department of Health and Human Services found that providers in 8 of 10 audited states received more than $27 million in Medicaid overpayments for services that were claimed after the patient had died (HHS and DOJ, 2008). Based on multiple streams of data, estimated costs of fraud and abuse in the United States range from $100 billion to $170 billion annually (Rudman et al., 2009).
Fraud is often perpetrated through false claims to insurance companies for reimbursement, but it can also manifest as administrative fabrication of patients or “padding” of orders and invoicing to divert money meant for the health care facility or system. Fraud can be committed by multiple actors within the health care system, including health care providers, government inspectors or regulators, payers (whether public or private), and even suppliers of equipment and medicines (Transparency International, 2006). Corrupt practices in the process of bidding and false invoicing or overpayment by agencies can be so well institutionalized that in many countries, a “parallel system” actually operates, sometimes even more coordinated than the one officially charged with overseeing and managing public resources (Nishtar, 2010). One of the barriers to preventing or reducing fraud is that it is often difficult to prove. A clear line cannot always be drawn between an honest mistake on an ordering form and nefarious intent.
Mismanagement of Resources and Theft of Supplies
Another form of corruption common in health care is mismanagement of resources and theft of supplies, whether drugs, diagnostic equipment, or even spare parts. Often the perpetrators are hospital administrators, who agree to deals with companies to purchase only their equipment or take money for projects or conditions that are not a need or priority for their community. The problem is illustrated by anecdotal evidence from a study in Uganda regarding a hospital administrator who was provided a $60,000 car for him to use once or twice per day—in a country where many in the population live on less than $1/day (Bouchard et al., 2012). This form of
corruption can also result in the “equipment graveyard” phenomenon, whereby practically new equipment will sit unused in a health care facility because of structural incompatibilities (e.g., voltage requirements), or the workforce and access to spare parts necessary to maintain and repair it are lacking (see Box 6-2).
Also common is the pilfering of supplies. Medicines and equipment are siphoned off along the entire supply chain, from the very first stages of their procurement to their delivery to their final destination (Nishtar, 2010). Medicines can be diverted for resale, bills or invoices can be padded with services that the patient did not use, or records can be created for “ghost patients” who allegedly received medicine. Theft of spare parts for larger hospital equipment is also commonplace. In Pakistan, for example, spare parts can easily be resold on the private or black market at lucrative rates (Nishtar, 2010). Another study in Uganda found that more than two-thirds of drugs that were supposed to be free were “lost” (McPake et al., 1999).
Publications on Corruption Across Country Lines
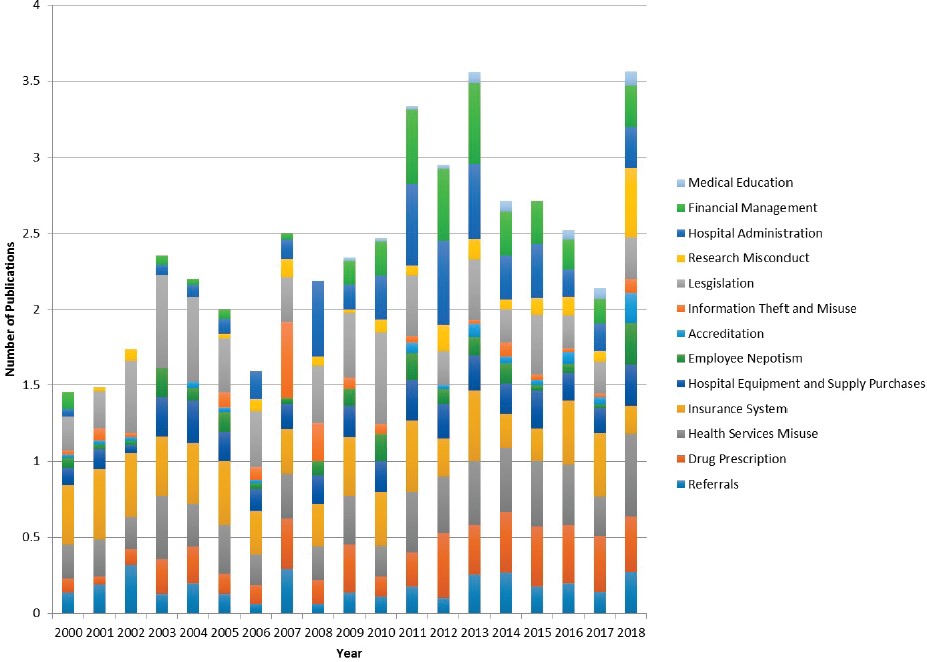
Interesting correlations can be found by analyzing the types of publications involving corruption in health care focused on various countries worldwide. In addition to measuring relationships and looking for associations between variables and health indicators, the committee wanted to understand what the data illustrated in terms of publications. A literature search of articles published from 2000 to 2018 identified more than 1,000 articles related to corruption and the health care sector. These publications were divided into 13 categories, with variations seen across years in the types of corruption addressed (see Figure 6-2), showing the increasing interest in recent years in better understanding this linkage and how to reduce its occurrence.
CHALLENGES TO EFFECTIVE UNIVERSAL HEALTH COVERAGE POSED BY CORRUPTION
The health care sector is unique because providers typically determine what services their customers (i.e., patients) should buy, whereas in most purchasing scenarios in other sectors, customers decide how they should spend their own money (Transparency International, 2006). The health care sector suffers from market failures due to the unique nature of the services provided. Because health care, by its nature, is complex, it is rife with information asymmetry in terms of what services should be provided and the price of those services. Although regulations are in place to control the quality of services provided (e.g., limiting reimbursement), health care markets are complicated by the frequent presence of a public–private mixed
system. Its large size, complex mix of actors, and asymmetrical information are relatively unique to the health care sector (Transparency International, 2006) and can make it prone to corruption and a diminished quality of governance (Holmberg and Rothstein, 2011). This problem can be exacerbated by imbalanced power dynamics that leave the general public with little voice to demand increased accountability. This section explores the determinants of corruption and the links among quality of governance, spending, and health outcomes to demonstrate why achieving UHC will always be out of reach for those countries plagued by corruption.
Determinants of Corruption
Even though health care systems worldwide are mixed,1 private expenditures represent a higher share of overall health care spending in lower-income countries. Of private expenditures, household OOP spending is the predominant component (WHO, 2010a). In fact, OOP spending represents 24 percent of total health care expenditures worldwide, but this proportion can be more than 50 percent in some low-income countries (Regional Committee for the Eastern Mediteranean, 2004). High OOP percentages open the door to informal payments and other forms of corruption, especially if prices are not transparent, making many health care systems worldwide vulnerable. Thus, it is not surprising that the rate of informal payments is also high; more than 30 percent of survey respondents from Turkey (Ozgen et al., 2010) and Greece (Liaropoulos et al., 2008), for example, reported making informal payments. Many mixed health care systems tend to suffer from poor performance, such as a failure to achieve fairness in financing and equity in outcomes. This has been hypothesized to result from an interplay among three determinants: insufficient state funding for health, insufficient regulatory oversight, and a lack of transparency in governance (Nishtar, 2007).
The first determinant is the chronic underfunding of health infrastructure by the government. The World Health Report 2010 notes that it is difficult to achieve UHC by limiting combined government and compulsory insurance expenditures to less than 5 to 6 percent of gross domestic product (GDP), an amount required to decrease the proportion of OOP to less than 15 to 20 percent of total health care expenditures (WHO, 2010b). This OOP percentage is based on analyses indicating what is required to
___________________
1 Here, a mixed health care system is defined as one in which “out-of-pocket payments and market provision of services predominate as a means of financing and providing services in an environment where publicly-financed government health delivery coexists with privately-financed market delivery” (Nishtar, 2007).
reduce catastrophic health care expenditures2 to negligible levels (Ablo et al., 2014; Xu et al., 2010). Unfortunately, this OOP level is often not met, with the average percentage being between 34 and 43 percent for low- and middle-income countries (LMICs). When the health care system is financed primarily through OOP spending, it is not surprising that services and infrastructure are unable to benefit from long-term planning and coordinated management, especially if a typical household income cannot sustain high OOP payments. This public underfunding results in providers in the public system seldom being paid adequately (Nishtar, 2010).
The second key determinant is the lack of sufficient regulatory oversight to guide the private sector in delivering social services. Regulation can play an integral role in many aspects of the health care system, whether directed at the quality and price of drugs and equipment, the qualifications and professionalization of human resources, the amount of supplies or providers needed for a particular type of facility, or even medical education (Nishtar, 2010). In many countries, the lack of oversight and incentives to prevent corruption—resulting from the absence of an adequate regulatory framework and defined roles and accountabilities—makes it easier for corrupt practices to take place. Nishtar (2010) notes that appropriate safeguards and transparent oversight can enable self-regulation of prices, quality, and numbers.
The third—and critically important—determinant is the lack of transparency in governance. This determinant has two components. The first, previously described, is the administrative and financial malpractices that can take place behind closed doors. A recent example comes from India, where some of the highest costs for patients in hospitals (up to 40–50 percent of the total cost of a stay) are for medicines and consumables (Prakash, 2018). Whether these items are necessary in each patient’s case is questionable; moreover, the price of medicines is based on the highest market retail price instead of the procurement price and quality (Rao, 2018). This practice allows the hospital to make higher profit margins, but drives families further into poverty when patients must pay the bill. Another issue found is a parallel system for the posting and transfers of health care workers in the public system, which functions on political connections and side payments (La Forgia et al., 2015). The second component of this determinant is laws and policies governing an entire district or country that are formulated to benefit just a few. This practice violates the equity principle
___________________
2 Catastrophic health expenditure is defined as OOP spending on health care services that consumes a large portion of a household’s available income, such that the household may be pushed into poverty as a result (WHO, 2005). The Sustainable Development Goals define two thresholds for catastrophic health expenditures: greater than 10 percent and greater than 25 percent of a household’s available income (WHO and World Bank, 2017).
of UHC. Furthermore, this practice is compounded when it is not transparent or provides few opportunities for public input, rendering the public unaware of what laws and policies are being established (Nishtar, 2010). This lack of transparency also makes it easy for corruption to thrive and creates a disincentive for leaders in management and governance to enact any reforms. Overall, this determinant adds to the argument for inclusive community oversight and engagement of citizens in developing health care systems and goals.
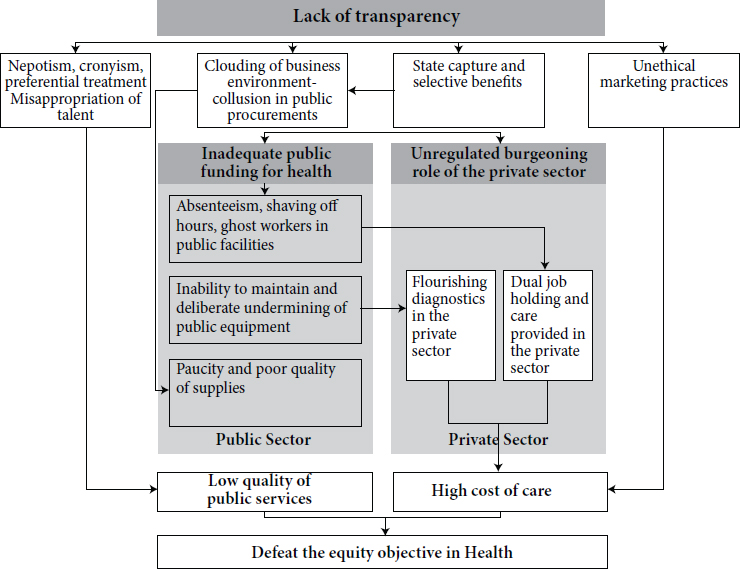
These three determinants—insufficient public funding for health, insufficient regulatory oversight, and a lack of transparency in governance—diminish the quality and equity of public services. Nishtar (2010a) presents a graphical depiction of how these three determinants interact (see Figure 6-3). While a public–private mix does not guarantee poor quality, there is a need for public policies that are locally adapted so as to develop stewardship mechanisms and influence the behavior of private providers to use their services for good (Lagomarsino et al., 2009).
SOURCE: Nishtar, S. 2010. Choked pipes—reforming Pakistan’s mixed health system. Journal of the Pakistan Medical Association 60(4):252–253. Reproduced with permission of Oxford University Press Pakistan © Oxford University Press.
A Need for Leadership
Overall, ensuring that quality health care services are available regardless of the national health infrastructure will require transparent stewardship. When resources are scarce, those in power can use the lack of resources as an excuse for poor services, but in reality they may often be siphoning resources for their private gain (Otremba et al., 2015). This corruption leads to the waste of scarce resources, as well as severely compromised quality of health services (Mackey and Liang, 2012). Surveys of 23 developing countries found that more than 80 percent of respondents had encountered corrupt practices in the health care sector (Holmberg and Rothstein, 2011). Reducing corruption and improving governance are thus needed investments. While strengthening stewardship of the health care sector is important in its own right, it is linked to improved health outcomes. In fact, modeling has shown that high quality of governance is associated with higher life expectancies and lower mortality rates for mothers and children (Holmberg and Rothstein, 2011). Of course, corruption is not limited to the public sector or government leaders; numerous allegations of corruption in the private sector have emerged in LMICs as well. Regardless of where the corruption originates, however, high-quality UHC will be out of reach as long as it exists. But as the world currently lacks an international consensus around corruption in global health and a comprehensive global framework for addressing it, any independent efforts will be difficult to motivate and sustain (Mackey and Liang, 2012).
Linkages Among Quality of Governance, Spending, and Health Outcomes
The relationship between the quality of governance and how a government spends its money is not a difficult connection to make. However, the indirect relationship between the quality of governance and health outcomes is a bit more tenuous. Quality governance can be said to exist “when the exercise of public power is based on impartiality as the basic norm” (Holmberg and Rothstein, 2011, p. 532). While “there is yet no country-based precise measurement of [the quality of governance]” (Holmberg and Rothstein, 2011, p. 532), such variables as population health measures can be used to depict the relationships among governance, spending, and health outcomes.
Several studies have found a positive association between a country’s quality of governance and its population health measures. Using data from 91 countries, Rajkumar and Swaroop (2008) found that quality of governance is a key mediator for whether public spending on health care effectively influences health outcomes. This finding is demonstrated by the changes the authors saw in child mortality rates: for each 1 percentage
point increase in the share of GDP devoted to public health care spending, countries with high-quality governance saw their child mortality rate reduced by 0.42 percent. This effect was reduced to just 0.18 percent for countries with average quality of governance, and there was no effect at all for countries with low quality of governance (Rajkumar and Swaroop, 2008). Findings of other studies corroborate this concept, with Lewis and Lloyd-Sherlock (2009) suggesting that mortality rates are unlikely to decline unless attention is shifted to institutional health care factors. Additionally, a meta-analysis by the Center for Global Development found that good governance is necessary for national health care systems to work optimally, and that public spending for health care in countries with poor governance is not efficient (Lewis, 2006)
STRATEGIES FOR REDUCING CORRUPTION IN HEALTH CARE
Many strategies exist for reforming health care systems to reduce corruption and make environments less conducive to malpractice. These include, among others, adequate remuneration of health care workers; adequate funding and management of the public health care system; community, public, and social accountability; and the strengthening of institutions outside the health care sector. These strategies are highlighted below, and it is hoped that more action will be taken to implement them so that 10 years from now, another report calling for similar steps will not be needed. The consequences of inaction are too great.
Adequate Remuneration of Health Care Workers
When health care systems are not adequately funded, front-line health care workers are often among those that suffer. Without adequate remuneration to support themselves and their families, health care workers may use their position to increase their income. One study, for example, found that resale of pharmaceuticals provided health care workers in Uganda their greatest source of income (Ferrinho and Van Lerberghe, 2002). Accordingly, researchers and policy makers from many countries have been calling for higher salaries to make workers less likely to request tips or bribes for providing health care. Such a reform effort is currently under way in Ukraine. Historically, individuals in that country had to provide “gift” payments to physicians to access care (BBC, 2018). However, a reform effort designed to rein in corruption directly addresses this issue by providing capitation-based payments to primary care providers (Twigg, 2017). This broad reform was passed into law in late 2017 (USUBC, 2018) and will be implemented in a phased manner, with full roll-out in 2020 (Twigg, 2017;
USUBC, 2018). But simply raising salaries will not be sufficient. Such strategies need to be supported by labor laws, professionalization, adapted codes of conduct, and monitoring of payment schemes. Others have called for the modification of the structure and oversight of payments (Holmberg and Rothstein, 2011; Kabote, 2017; Transparency International, 2006). Thus, efforts to curb corrupt practices by health care workers need to be paired with similar reforms for health system management—an area discussed in the next section.
Adequate Funding and Management of the Public Health Care System
Without an adequately funded and managed health care system, ensuring staffing, procurement of needed medicines and equipment, and treatment of illnesses and injuries can be difficult to accomplish. It has been argued that limited public funding results in a mixed health care system (Nishtar, 2007) that, because of its complexity, becomes difficult to monitor and open to instances of corruption. Country health care systems have a responsibility to ensure that patient need, not the opportunity for profit, dictates the care and treatment of their populations (Transparency International, 2006). Accordingly, Kankeu and colleagues (2016) also suggest improving the ethical standards of health workers and establishing well-defined legal frameworks to better discourage informal payment practices. Strengthening management practices and controls on personnel—in the form of increased oversight and inspection, institutional independence (e.g., the ability to control staffing), and multilayered approval for procurement and/or contracting (Lewis, 2006)—has been found to be effective in reducing corruption (Gonseth and Acuna, 2018). However, this strategy must be paired with effective incentives to influence desired behavior change. Where corrupt practices are entrenched within the system, social accountability can play an effective role, which is expanded on below.
Community, Public, and Social Accountability
Accountability strategies have long been proposed as solutions to improve the performance of public institutions—through a “long route,” via elections and public officials, or a “short route,” via “direct accountability between users [patients] and providers” (Anuradha, 2013, p. S30). Similar calls have been made to decrease instances of corruption in the health sector through the use of community councils and greater public scrutiny (Transparency International, 2006). For those efforts seeking to use the “long route,” transparency is paramount, as reflected in studies and ongoing reform efforts. For example, transparency in pricing of medical supplies
at hospitals in Argentina resulted in a 50 percent decline in price variation across hospitals (Transparency International, 2006). Similar reform efforts in Ukraine have sought to increase transparency and instate reference pricing for the procurement of drugs, thereby addressing the state capture and collusion that plagued the pharmaceutical supply chain, which resulted in an annual loss of $100 million out of a $250 million pharmaceutical budget (Twigg, 2017). The “short route” of accountability, however, is more heavily emphasized in areas in which democratic institutions have weakened, thus necessitating direct participation in governance (Fox, 2007). This form of accountability, also called social accountability, can involve user-centered information systems, citizen monitoring, public grievance and redress, and even participatory budgeting (Fox, 2015). Successfully tested in various sectors, these mechanisms have been found to improve health outcomes (Björkman and Svensson, 2009; Björkman et al., 2014; Gonçalves, 2014; Touchton and Wampler, 2013). At the core of these strategies is the provision of actionable and user-centered information (Fox, 2015), essential for building collective bargaining power from the bottom up.
To be successful, these efforts toward community accountability not surprisingly need to be backed by leadership and oversight. Bolivia, for example, has found lower corruption where local groups are active overseers, demonstrating the strengths of bottom-up accountability (Gatti et al., 2002). Several other initiatives have pursued similar goals through community councils. However, they may not achieve their intended results without proper oversight and authority (Lewis, 2006). Creating this type of social accountability can be nearly impossible if there is true government failure (Devarajan et al., 2014), and can have little effect if an adequate enabling environment is lacking. Ukraine was able to create such an enabling environment to roll out its reform package. The new health minister, Dr. Ulyana Suprun (an American-Ukrainian radiologist), cleared the ranks of obstructionist political appointees and hired her own leadership team—one that did not have vested interests in the corrupt system. This new environment allowed a meaningful reform agenda to move forward (Twigg, 2017). A similar tactic was used at the Abel Gilbert Pontón Hospital in Ecuador, in which an outside manager was hired to curb corrupt practices, thereby allowing it to be more responsive to community needs (Gonseth and Acuna, 2018). Thus, for accountability efforts to be successful, there needs to be a state–society synergy and a reliance on mutual empowerment (Fox, 2015), which in turn requires a strengthening of institutions across sectors.
Strengthening of Institutions Outside the Health Care Sector
Weak institutions, whether due to misuse of resources, capture by special interests, influence by political patronage, organizational volatility,
or goal ambiguity (Graham, 2002), can create a milieu in which corruption can breed (World Bank, n.d.). While reform at the local and regional levels is necessary to prevent corruption, the system within which individuals and health care facilities operate needs to be strengthened. Strong institutions are necessary to detect, correct, and prevent corruption. As described by the World Bank, supreme audit institutions (SAIs) are national agencies responsible for auditing government spending and revenue (Dye and Staphenhurst, 1998; Stapenhurst and Titsworth, 2001). SAIs can promote accountability and transparency, thereby preventing corruption. Examples include the Turkish Court of Accounts, whose auditors detected falsified claims and statements and illegal bidding practices (Evans, 2008), and the Auditor General of Zambia, who identified overpayment for and nondelivery of goods and services and irregular procurement contracts. In addition to detecting corruption, efforts can be made to build systems of a well-performing government, such as the development of an apolitical civil service guided by institutional values, the development of well-functioning budget processes that are transparent and allocatively efficient, the creation of transparent financial management systems, and the diffusion of power through decentralization paired with community oversight structures (World Bank, n.d.). What route and mechanisms a country uses will highly depend on the relative accountability and capacity of its government.
SUMMARY AND RECOMMENDATION
Corruption, in all of its forms, is an enormous contributor to poor quality of care worldwide. Whether it occurs sporadically or becomes institutionalized, its effects are felt through longer wait times, poorer treatment by health care workers, threats to supply chains, higher fees for services that should be free of charge, and general misuse of funds. These malpractices lead to declining trust in governments and health care systems among citizens, as well as reduced quality of care and worsened health outcomes. Solutions lie in investments in health care infrastructure and payment of health care workers, coupled with accountability, public reporting, and strengthening of institutions outside the health care sector that may impact its practices, such as financing and regulation. While overcoming corrupt practices is a difficult and often long-term endeavor, there have been successes in various countries, and their lessons can be applied elsewhere for those striving to achieve better quality through improved governance:
- Social accountability, paired with strengthened government institutions, can leverage synergy to curb corrupt practices and improve the responsiveness of a health care system to its clients.
- Transparency in pricing of medical supplies at hospitals in Argentina resulted in a 50 percent decline in price variation across hospitals.
- Social accountability mechanisms, such as user-centered information systems, citizen monitoring, public grievance and redress, and even participatory budgeting, have been found to improve health outcomes in various settings.
- Hiring of outside individuals with no ties to a corrupt institution can roll back vested interests and create an impetus for positive change.
As with the rest of the topics discussed in this report, context and local input and leadership will be paramount in ensuring success and sustainability.
Conclusion: It is critical for governments and societies to create better governance structures that are accountable and transparent, build safeguards both within and outside of health care systems to decrease corruption, and improve health outcomes for populations. Until this is accomplished on a national scale for many countries, universal health care may be subverted to enrich the powerful and leave vulnerable populations without adequate care. In essence, integrity is, if not a domain of quality itself, an essential precondition for the pursuit of quality in health care.
Recommendation 6-1: Address Corruption and Collusion
Ministries of health should include in their national health care quality strategies, directly and clearly, safeguards against corruption and collusion and actions for improvements in integrity throughout their health care systems. The health sector should draw on expertise and resources from outside the health care system, including related core state institutions and dedicated anticorruption institutions, to combat corruption through prevention, detection, and enforcement.
REFERENCES
Ablo, A., D. Arhin-Tenkorang, C. Benn, R. Elovainio, D. B. Evans, L. E. Fonesca, J. Frenk, D. McCoy, D. McIntyre, S. Moon, et al. 2014. Shared responsibilities for health: A coherent global framework for health financing. London, UK: Chatham House. https://www.chathamhouse.org/sites/files/chathamhouse/field/field_document/20140521HealthFinancing.pdf (accessed June 3, 2018).
Anuradha, J. 2013. Do they work? Assessing the impact of transparency and accountability initiatives in service delivery. Development Policy Review 31(S1):S29–S48.
Azfar, O., and T. Gurgur. 2008. Does corruption affect health outcomes in the Philippines? Economics of Governance 9(3):197–244.
Bauserman, M., C. Hailey, J. Gado, A. Lokangaka, J. Williams, R. Richards-Kortum, A. Tshefu, and C. Bose. 2015. Determining the utility and durability of medical equipment donated to a rural clinic in a low-income country. International Health 7(4):262–265.
BBC (British Broadcasting Corporation). 2018. Ulana Suprun: My efforts to reform Ukraine’s healthcare. BBC News, April 25. https://www.bbc.com/news/av/world-europe-43898005/ ulana-suprun-my-efforts-to-reform-ukraine-s-healthcare (accessed July 10, 2018).
Bhadelia, N. 2016. Rage against the busted medical machines. NPR, September 8. https://www.npr.org/sections/goatsandsoda/2016/09/08/492842274/rage-against-the-busted-medical-machines (accessed June 3, 2018).
Björkman, M., and J. Svensson. 2009. Power to the people: Evidence from a randomized field experiment on community-based monitoring in Uganda. The Quarterly Journal of Economics 124(2):735–769.
Björkman, M., D. D. Walque, and J. Svensson. 2014. Information is power: Experimental evidence on the long-run impact of community based monitoring. Policy research working paper no. 7015. Washington, DC: World Bank.
Bouchard, M., J. C. Kohler, J. Orbinski, and A. Howard. 2012. Corruption in the health care sector: A barrier to access of orthopaedic care and medical devices in Uganda. BMC International Health & Human Rights 12:5. doi:10.1186/1472-698X-12-5.
Cockerell, J. 2014. Making donations of medical equipment work. The Lancet Global Health, January 20. http://globalhealth.thelancet.com/2014/01/20/making-donations-medical-equipment-work (accessed June 3, 2018).
Compton, B., D. M. Barash, J. Farrington, C. Hall, D. Herzog, V. Meka, E. Rafferty, K. Taylor, and A. Varghese. 2018. Access to medical devices in low-income countries: Addressing sustainability challenges in medical device donations. NAM Perspectives. Washington, DC: National Academy of Medicine. doi:10.31478/201807a.
Devarajan, S., S. Khemani, and M. Walton. 2014. Can civil society overcome government failure in Africa? World Bank Research Observer 29(1):20–47.
Dye, K. M., and R. Staphenhurst. 1998. Pillars of integrity: The importance of supreme audit institutions in curbing corruption. Washington, DC: The Economic Development Institute of the World Bank. http://documents.worldbank.org/curated/en/199721468739213038/pdf/multi-page.pdf (accessed June 3, 2018).
Evans, A. 2008. The role of supreme audit institutions in combating corruption. Berlin, Germany: Transparency International. https://www.u4.no/publications/the-role-of-supremeaudit-institutions-in-combating-corruption/pdf (accessed June 3, 2018).
Ferrinho, P., and W. Van Lerberghe. 2002. Managing health professionals in the context of limited resources: A fine line between corruption and the need for moonlighting (English). Washington, DC: World Bank.
Fox, J. A. 2007. The uncertain relationship between transparency and accountability. Development in Practice 17(4-5):663–671.
Fox, J. A. 2015. Social accountability: What does the evidence really say? World Development 72:346–361. doi:10.1016/j.worlddev.2015.03.011.
Gatti, R., G. Gray-Molina, and J. Klugman. 2002. Determinants of corruption in local health care provision: Evidence from 108 municipalities in Bolivia. Societa Italiana di Economia Pubblica. http://www.siepweb.it/siep/oldDoc/wp/166.pdf (accessed June 3, 2018).
Gee, J., and M. Button. 2015. The financial cost of healthcare fraud 2015: What data from around the world shows. London, UK: PFK Littlejohn LLP. http://www.port.ac.uk/media/contacts-and-departments/icjs/ccfs/The-Financial-Cost-of-Healthcare-FraudReport-2015.pdf (accessed June 3, 2018).
Gonçalves, S. 2014. The effects of participatory budgeting on municipal expenditures and infant mortality in Brazil. World Development 53:94–110.
Gonseth, J., and M. C. Acuna. 2018. Ecuador: Improving hospital management as part of the health reform process in Ecuador: The case of Abel Gilbert Pontón Hospital. In Health systems improvement across the globe: Success stories from 60 countries, edited by J. Braithwaite, R. Mannion, Y. Matsuyama, P. Shekelle, S. Whittaker, and S. Al-Adawi. Boca Raton, FL: CRC Press. Pp. 33–40.
Graham, C. 2002. Strengthening institutional capacity in poor countries. Washington, DC: Brookings Institution.
Gupta, S., H. Davoodi, and E. Tiongson. 2002. Corruption and the provision of health care and education services. Washington, DC: International Monetary Fund. https://www.imf.org/external/pubs/ft/wp/2000/wp00116.pdf (accessed June 3, 2018).
Hanf, M., A. Van-Melle, F. Fraisse, A. Roger, B. Carme, and M. Nacher. 2011. Corruption kills: Estimating the global impact of corruption on children deaths. PLoS One 6(11):e26990.
HHS (U.S. Department of Health and Human Services) and DOJ (U.S. Department of Justice). 2008. Health care fraud and abuse control program annual report for FY 2007. Washington, DC: HHS and DOJ.
Holmberg, S., and B. Rothstein. 2011. Dying of corruption. Health Economics, Policy and Law 6(4):529–547.
Kabote, S. J. 2017. Perceived corruption and quality of health services in Mbeya urban district, Mbeya region Tanzania. International Journal of Social Science Research 5(1):150–164. http://www.macrothink.org/journal/index.php/ijssr/article/view/10519/8801 (accessed June 3, 2018).
Kankeu, H. 2018. Informal payments and other failures in health care provision in public facilities: More than just an association. Financing Health in Africa, March 7. http://www.healthfinancingafrica.org/home/informal-payments-and-other-failures-in-health-care-provision-in-public-facilities-more-than-just-an-association (accessed June 3, 2018).
Kankeu, H. T., and B. Ventelou. 2016. Socioeconomic inequalities in informal payments for health care: An assessment of the “Robin Hood” hypothesis in 33 African countries. Social Science & Medicine 151:173–186. doi:10.1016/j.socscimed.2016.01.015.
Kankeu, H. T., S. Boyer, R. F. Toukam, and M. Abu-Zaineh. 2016. How do supply-side factors influence informal payments for healthcare? The case of HIV patients in Cameroon. The International Journal of Health Planning and Management 31(1):E41–E57.
La Forgia, G., R. Shomikho, S. Shabbeer, M. S. Kumar, and A. Rabia. 2015. Parallel systems and human resource management in India’s public health services: A view from the front lines. Public Administration and Development 35(5):372–389.
Lagomarsino, G., D. de Ferranti, A. Pablos-Mendez, S. Nachuk, S. Nishtar, and S. Wibulpolprasert. 2009. Public stewardship of mixed health systems. The Lancet 374(9701):1577–1578.
Lewis, C. M., and P. Lloyd-Sherlock. 2009. Social policy and economic development in South America: An historical approach to social insurance. Economy and Society 38(1):109–131.
Lewis, M. 2006. Governance and corruption in public health care systems. Washington, DC: Center for Global Development.
Lewis, M. 2007. Informal payments and the financing of health care in developing and transition countries. Health Affairs 26(4):984–997.
Liaropoulos, L., O. Siskou, D. Kaitelidou, M. Theodorou, and T. Katostaras. 2008. Informal payments in public hospitals in Greece. Health Policy 87(1):72–81.
Mackey, T. K., and B. A. Liang. 2012. Combating healthcare corruption and fraud with improved global health governance. BMC International Health and Human Rights 12(1):23. doi:10.1186/1472-698X-12-23.
Maestad, O., and A. Mwisongo. 2011. Informal payments and the quality of health care: Mechanisms revealed by Tanzanian health workers. Health Policy 99(2):107–115.
McPake, B., D. Asiimwe, F. Mwesigye, M. Ofumbi, L. Ortenblad, P. Streefland, and A. Turinde. 1999. Informal economic activities of public health workers in Uganda: Implications for quality and accessibility of care. Social Science & Medicine 49(7):849–865.
Mendel, I. 2017. In Ukraine, health care is free (except when it’s not). Politico, April 15. https://www.politico.eu/article/ukraines-ailing-health-care-system-underfunded-corrupt-inaccessible (accessed June 20, 2018).
Miesen, M. 2013. The inadequacy of donating medical devices to Africa. The Atlantic, September 20. https://www.theatlantic.com/international/archive/2013/09/the-inadequacyof-donating-medical-devices-to-africa/279855 (accessed April 10, 2018).
Mokhtari, M., and M. Ashtari. 2012. Reducing informal payments in the health care system: Evidence from a large patient satisfaction survey. Journal of Asian Economics 23(2):189–200.
Nishtar, S. 2007. Politics of health systems: WHO’s new frontier. The Lancet 370(9591):935–936.
Nishtar, S. 2010. Choked pipes—reforming Pakistan’s mixed health system. Journal of the Pakistan Medical Association 60(4):252–253.
OECD (Organisation for Economic Co-operation and Development). 2017. Tackling wasteful spending on health, highlights. Paris, France: OECD.
Otremba, M., G. Berland, and J. J. Amon. 2015. Hospitals as debtor prisons. The Lancet Global Health 3(5):e253–e254.
Ozgen, H., B. Sahin, P. Belli, M. Tatar, and P. Berman. 2010. Predictors of informal health payments: The example from Turkey. Journal of Medical Systems 34(3):387–396.
Perry, L., and R. Malkin. 2011. Effectiveness of medical equipment donations to improve health systems: How much medical equipment is broken in the developing world? Medical & Biological Engineering & Computing 49(7):719–722.
Prakash, A. 2018. Office memorandum. http://www.nppaindia.nic.in/order/overcharging_Details(20022018).pdf (accessed June 3, 2018).
Rajkumar, A. S., and V. Swaroop. 2008. Public spending and outcomes: Does governance matter? Journal of Development Economics 86(1):96–111.
Rao, M. 2018. Private healthcare in India part I: Artificially-inflated cost of medicine, consumables make non-govt hospitals inaccessible to most. https://www.firstpost.com/india/private-healthcare-in-india-part-i-artificially-inflated-cost-of-medicine-consumablesmake-non-govt-hospitals-inaccessible-to-most-4458777.html (accessed June 3, 2018).
Regional Committee for the Eastern Mediteranean. 2004. The impact of health expenditure on households and options for alternative financing. Cairo, Egypt: Regional Office for the Eastern Mediteranean, WHO.
Rudman, W. J., J. S. Eberhardt, W. Pierce, and S. Hart-Hester. 2009. Healthcare fraud and abuse. Perspectives in Health Information Management/AHIMA, American Health Information Management Association 6(Fall):1g.
Stapenhurst, R., and J. Titsworth. 2001. Features and functions of supreme audit institutions. PREM Notes, October. http://www1.worldbank.org/prem/PREMNotes/premnote59.pdf (accessed June 3, 2018).
Stringhini, S., S. Thomas, P. Bidwell, T. Mtui, and A. Mwisongo. 2009. Understanding informal payments in health care: Motivation of health workers in Tanzania. Human Resources for Health 7(1):53. doi:10.1186/1478-4491-7-53.
Szende, A., and A. J. Culyer. 2006. The inequity of informal payments for health care: The case of Hungary. Health Policy 75(3):262–271.
Touchton, M., and B. Wampler. 2013. Improving social well-being through new democratic institutions. Comparative Political Studies 47(10):1442–1469.
Transparency International. 2006. Global corruption report 2006 special focus: Corruption and health: London, UK: Pluto Press. doi:10.2307/j.ctt184qq53.
Twigg, J. L. 2017. Ukraine’s health sector: Sustaining momentum for reform. Washington, DC: Center for Strategic and International Studies.
URT (United Republic of Tanzania) and Ministry of Health and Social Welfare. 2011. The Tanzania quality improvement framework in healthcare 2011–2016. https://www.jica.go.jp/project/tanzania/006/materials/ku57pq00001x6jyl-att/framework_in_health.pdf (accessed June 3, 2018).
USUBC (US-Ukraine Business Council). 2018. President of Ukraine signs healthcare reform law. http://www.usubc.org/site/recent-news/president-of-ukraine-signs-healthcare-reform-law (accessed July 10, 2018).
Vian, T. 2002. Corruption and the health care sector. In Sectoral perspectives on corruption. Washington, DC: USAID.
Vian, T. 2008. Review of corruption in the health sector: Theory, methods and interventions. Health Policy and Planning 23(2):83–94.
Vian, T., W. D. Savedoff, and H. Mathisen. 2010. Anticorruption in the health sector: Strategies for transparency and accountability. Boston, MA: Kumarian Press.
WHO (World Health Organization). 2005. Distribution of health payments and catastrophic expenditures: Methodology. Geneva, Switzerland: WHO.
WHO. 2010a. Estimating out-of-pocket spending for national health accounts. Geneva, Switzerland: WHO.
WHO. 2010b. The World Health Report: Health systems financing: The path to universal coverage. http://www.who.int/whr/2010/overview.pdf (accessed June 3, 2018).
WHO and World Bank. 2017. Tracking universal health coverage: 2017 global monitoring report. Washington, DC: WHO and World Bank.
World Bank. n.d. Helping countries strengthen institutions. http://www1.worldbank.org/publicsector/anticorrupt/corruptn/cor06.htm (accessed July 18, 2018).
Xu, K., P. Saksena, M. Jowett, C. Indikadahena, J. Kutzin, and D. B. Evans. 2010. Exploring the thresholds of health expenditure for protection against financial risk. Geneva, Switzerland: WHO.
This page intentionally left blank.
























