
Proceedings of a Workshop
| IN BRIEF | |
|
July 2018 |
Faith–Health Collaboration to Improve Population Health
Proceedings of a Workshop—in Brief
Faith plays a variety of roles in the context of health improvement: as a place, social structure, partner, and intervention. The National Academies of Sciences, Engineering, and Medicine’s Roundtable on Population Health Improvement held a March 22, 2018, workshop on faith–health collaboration at the Thomas J. Boyd Chapel on the campus of Shaw University in Raleigh, North Carolina. The workshop concisely summarized here did not explore aspects of the relationship between faith and health such as the efficacy of prayer or of congregation-based health interventions. Rather, presentations showcased the potential and, in some cases, the value, as demonstrated in outcomes, of community faith-based entities as partners with health-sector organizations.
Dean Johnny Hill of the Shaw School of Divinity welcomed the workshop participants with remarks about the history of the university’s Leonard Medical School, one of the nation’s four African American medical schools at the time it closed its doors in 1918–1919.1 Its home on campus now houses the divinity school, and Hill pointed to the institution’s “very proud heritage of seeking health and wholeness, both in body and soul for God’s children and for the communities that we serve.” After being introduced by Hill, Shaw President Paulette Dillard also welcomed the audience and made additional remarks about the legacy of Shaw as a place created when a Union chaplain observed the needs of the newly freed slaves and sought to establish an institution to help respond. Repeatedly throughout its history, Dillard stated, the university identified needs and met them, from literacy and education to health and health care. Dillard closed by noting Shaw’s location in the gap between Raleigh’s “economic boom town” neighborhoods and the poorest zip code in Wake County and the evolving opportunities to make a difference.
Sanne Magnan of the HealthPartners Institute welcomed the participants on behalf of the roundtable and echoed Dillard’s words by stating that the day’s conversations were intended to bring together representatives from the faith and health sectors to help close the gaps in health and well-being. Gary Gunderson of the Wake Forest Baptist Medical Center, who led the planning process, spoke of the past two and a half centuries, during which the United States as a nation endeavored “to keep as much formal distance as possible between the structures of faith and the public structures.” The workshop, he explained, was intended to open up the field of collaboration “at the intersection of faith and health in a constitutional democracy that has found it wise to keep at some distance those two very entities.” As a starting point, Gunderson offered the concept of Religious Health Assets, a phrase crafted by the African Religious Health Assets Programme (ARHAP) at the University of Cape Town, represented at the workshop by invited guest James Cochrane (see Figure 1). Gunderson added that “communities of spirit” may capture the “radical diversity” of the field in a way in which “religion” does not.
Gunderson introduced Prabhjot Singh of the Icahn School of Medicine at Mount Sinai. Singh provided a context-setting presentation that touched on several key learnings from his career as a physician–scientist, from the recognition of how patients are embedded in families, communities, and religious congregations to the failure of
______________
1 See, for example, Harley, E. H. 2006. The forgotten history of defunct black medical schools in the 19th and 20th centuries and the impact of the Flexner Report. Journal of the National Medical Association 98(9):1425–1429. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2569729 (accessed May 8, 2018).
![]()
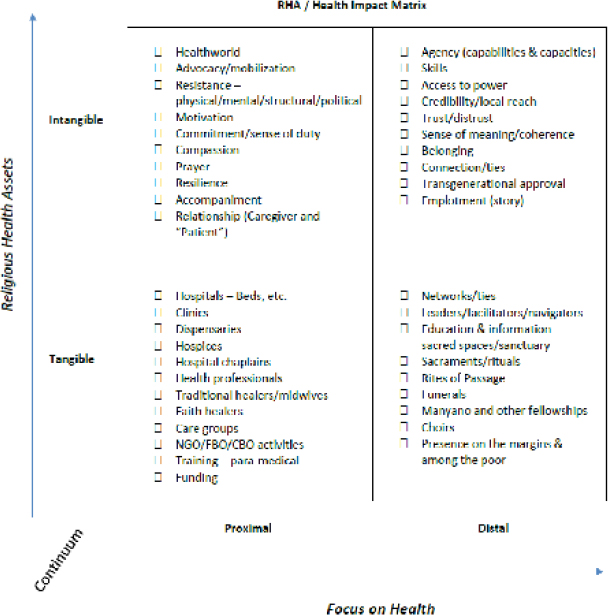
FIGURE 1 Religious Health Assets (RHAs)/Health Impact Matrix.
NOTE: CBO = community-based organization; FBO = faith-based organization; NGO = non-governmental organization.
SOURCE: Gunderson presentation, March 22, 2018; developed by James Cochrane, African Religious Health Assets Programme.
health care delivery systems to fully understand and meet their health-related needs (e.g., literacy), often to the detriment of people’s health. Singh noted that 350,000 U.S. congregations overlap with 250,000 neighborhoods or geographic communities, together forming the connective tissue that must be understood in order to improve population health. “At a time when public health and health care institutions are both trying to work more concertedly to improve population health,” Singh added, “they are finding common ground in neighborhoods.” Communities of spirit (i.e., congregations) can play important roles in influencing the work of addressing poverty and injustice, which hamper efforts to improve population health. Singh noted that
Robert Putnam and other researchers in political science, sociology, psychology, and related fields have documented how our social fabric influences our ability to survive and thrive and how faith communities play an important role in our health in measurable and well-described ways. Of course, new social technologies allow us to learn about relationships and how communities form at unprecedented scale. So health institutions must chart a research agenda that embraces new questions, new partnerships, and new methods.
Singh concluded his remarks with a three-part call to action:
- Understand the nature of the social connective tissue involving faith-based assets with the community and other organizations;
- Put this understanding to work to support faith–health partnerships involved in actions to improve the conditions for health in their communities (from advocacy for greater investment in children to addressing the loneliness and isolation of seniors); and
- Work with faith leaders to, paraphrasing Gunderson, craft richer messages and recommendations that are more relevant to communities of spirit and ensure that the best available evidence is communicated effectively in the context of trust and partnership.
During the discussion period, Robert McLellan of Dartmouth-Hitchcock referred to immunization as an example of how personal autonomy gets pitted against public health and asked a how faith–health collaboration could address this conundrum. Gene Matthews of the University of North Carolina and former chief counsel to the Centers for Disease Control and Prevention (CDC) reframed the question about personal liberty in recognition of the fact that freedom from vaccine-related illness is also an important aim. Ella Auchincloss of ReThink Health asked how the engagements with faith-based organizations should be conducted so they are not simply viewed as assets or venues, but as true partners. Gunderson answered that it takes artfulness to create a collaborative space that is a limited domain (i.e., neither side has it as its sovereign space) that permits each side to come in with its own integrity, ethics, and motivation, and to work together in a way that achieves the goals of all partners. Mylynn Tufte of the North Dakota Department of Health asked about leading practices or evidence related to how faith-based entities support behavioral and mental health to decrease stigma associated with addiction. Missy Stancil of CareNet Counseling responded that her organization “specializes in spiritually integrated psychotherapy and community-based work.” She has found that in working both with community partners (e.g., congregations) and health care organizations, there is internalized stigma that requires a process of mutual education. Amy Moyer of Kaiser Permanente of the Mid-Atlantic commented on her organization’s deep interest in understanding how private, nonprofit, and government relationships can form around faith-based mental health initiatives. The faith community needs to be included in decision-making circles to help hospital boards and public entities, according to Eva Powell of Common Purpose Health. Angeloe Burch of the Interdenominational Ministerial Alliance of Durham commented on the importance of having a thorough understanding of an organization, faith tradition, or individual with which one seeks to collaborate or whom one seeks to serve. To illustrate, he highlighted three aspects of community and personal history that may be relevant to faith–health partnerships: the Primitive Baptist denomination’s opposition to doing missionary work abroad, African Americans’ concerns about immunization rooted in their communities’ negative past interactions with public health, and the effects of a patient’s interaction with health care providers who act as though they believe they know the patient better than the patient knows himself or herself.
Gunderson invited Cochrane to comment on the concept of tangible and intangible networks at the faith–health interface and on the concept of health worlds. As described in the slide Gunderson shared from the work of ARHAP, it is not enough to enumerate and describe hospital personnel, equipment, and the like, but intangible factors and assets such as trust and power also need to be considered and described. The lifeworld, Cochrane stated, “is the taken-for-granted assumptions that affect the way people make decisions and behave in the world that go far beyond simply the rational and the limited sense of calculating instrumental decisions that one makes between benefit and cost.” Cochrane and colleagues created the phrase “healthworld” to describe “the way in which people construct their own sense of health and what they do with that.” In addition to people’s understanding of themselves, Cochrane added, they are “embedded in families with traditions, cultures with traditions, and religions with traditions,” and all of those dimensions have effects on the “practice of the science of health.”
The first panel was moderated by Kathy Gerwig of Kaiser Permanente and featured Kirsten Peachey of Congregational Health Partnerships for Advocate Health Care and the Center for Faith and Community Health Transformation. Peachey told the audience that the virtual center represents the joint work of the staff of Advocate Health Care, a faith-based system affiliated with the Lutheran Church. Peachey’s role is director of Congregational Health Partnerships across the wide range of religious traditions represented in the communities around Chicago. The center emerged as part of conversations in the development of the quinquennial Illinois Department of Public Health community health improvement plan. It represents a partnership with the Neighborhoods Initiative at the University of Illinois at Chicago and the Chicago Department of Public Health. Peachey mentioned Gunderson’s previous work at the Interfaith Health Program at Emory University. This influenced efforts in Chicago, including with CDC funding (e.g., the Racial and Ethnic Approaches to Community Health [REACH] program), focused on the central question: “How do we work together more effectively at the root causes of health disparities in ways that will create transformation in our communities and in ways that will really bring the strength of public health and the strength of faith together?” Peachey described the breadth of activities conducted by the center and the leadership approaches it employs, including visioning to advance health equity and justice (see Box 1), which deploys the concept of the moral imagination. As an example, she asked, “When we are facing an issue such as food insecurity in our communities, what is the moral imagination that we bring as people of faith to this issue? How does that inform what we want to try to do and what we want to try to accomplish?” Research activities include surveying and enumerating member activities and programs that address trauma and seek to build resiliency.
During a brief question-and-answer period, Magnan asked Peachey to say more about the Risking Connection in Faith Communities2 curriculum being used by the center and its partners. Peachey noted that the curriculum is a helpful resource for multifaith, trauma-informed congregations.
______________
2 See https://thecrg.org/resources/risking-connection-in-faith-communities-a-training-curriculum-for-faith-leaders-supporting-trauma-survivors (accessed May 8, 2018).
BOX 1
Center for Faith and Community Health Transformation: How We Lead and Key Work Areas
| How We Lead | Key Work Areas | |
|
Visioning
Convening
Hosting Practicing |
Identifying What Already Exists Common Curriculum: Risking Connection in Faith Communities—Teach the Facilitator Cohort
|
SOURCE: Peachey presentation, March 22, 2018.
Gerwig next introduced Paul Wong, chair of the board of the University Muslim Medical Association (UMMA) Community Clinic. Wong spoke of the history of the Federally Qualified Health Center (FQHC) established in 1992 in the wake of civil unrest in South Los Angeles by Muslim medical school students from the Charles R. Drew University of Medicine and Science (itself founded in 1966 in the wake of the so-called “Watts riots”) and the University of California, Los Angeles. The clinic’s founders were young people compelled by their faith to take social action to address great needs in the community around them. Today, the clinic has partnerships with a local high school (for a school-based health center at Fremont High School that serves students and the community), the Los Angeles Neighborhood Land Trust (for a community garden, free farmers’ market, and food distribution center), and area hospitals. The clinic also brings in health sciences students for rotations and volunteer opportunities, added Wong, “with the hope of training future doctors, public health workers, and students to view South Los Angeles as part of their neighborhood, part of their home, and not somewhere to be feared.” In its partnership with the California Hospital Medical Center, part of the Dignity Group, the clinic implemented a readmissions program that provides comprehensive care after discharge to prevent unnecessary readmissions.
During the discussion period, Moyer asked if the UMMA Community Clinic works to address socioeconomic opportunity. Wong responded that the clinic provides literacy support, some legal help, and a “tax day” to help community members with filing their tax returns. Andre White of Durham Parks and Recreation asked how UMMA engages with and obtains the buy-in of the community. Wong acknowledged that language and cultural competence have been an important factor, as have responsiveness to community needs and respect and humility (staff are known by their first names instead of Dr. X or Y).
Matthews commented on the history of competition between health departments and community health centers and the former’s discriminatory practices in sharing federal funding. Wong remarked that it helps when public health colleagues at the state and local levels are supportive, which he illustrated with the story of how a state assemblyman worked with UMMA to hold a gathering at the community garden, which helped to advance the collaborative conversation. Responding to a later question posed by McLellan about funding, Wong stated that one strength of the clinic is that it is not fully dependent on federal and fee-for-service funding. Its private-sector support, including from the Muslim community (most of whom do not live in South Los Angeles) and from foundations, allows it to conduct a range of programs and activities, including advocacy and policy.
The afternoon’s presentations began with two that highlighted state-level policy perspectives: one outlining a public health leader’s thinking about working across sectors to achieve health improvement priorities, and the other showcasing a faith and health sector collaborative advocacy effort seeking to expand health care access as a key need for
improving population health. The first afternoon speaker, introduced by Terry Allan of the Cuyahoga County, Ohio, Board of Health, was Mandy Cohen, North Carolina Secretary of Health and Human Services. She shared insights gained earlier in her career, when patient encounters demonstrated to her that health is not merely health care. Cohen outlined her vision for the state’s health, including acknowledging that although she is the person charged with health, all members of the North Carolina cabinet need to think about health, and cross-sector partnerships, such as with transportation and education, are essential. If one looks at the North Carolina health budget, Cohen noted, it is mostly intended to buy health care, not health, and because resources are constrained and the solutions to people’s health and well-being reside in different parts of the government, it is imperative to learn to “knit together community, health care, social services” to really improve health. Allan asked how public health, health care, and faith-based organizations could work together. Cohen responded that non-traditional partnerships are necessary. To a question from Phyllis Meadows of The Kresge Foundation about what distinguishes current circumstances from the past and explains Cohen’s optimistic vision for North Carolina in the context of a “society right now that is really feeling very divided,” Cohen reiterated that resource constraints create or compel creativity and changes in health care payment offer opportunities to forge partnerships or connect the puzzle pieces among health care providers, social services, and community resources.
For another state-level policy perspective, Allan introduced Donna Weinberger, board member of Greater Cleveland Congregations (GCC), who described her multifaith community organizing network’s major policy change effort. GCC brought together a broad coalition of faith groups (i.e., GCC’s 43 congregations), health-sector organizations (4 major hospital systems), labor unions, and businesses to advocate on behalf of Medicaid expansion in Ohio in the context of strong opposition from the state legislature. The diverse coalition known as the Northeast Ohio Medicaid Expansion Coalition (NEOMEC) was replicated in five other areas of Ohio. GCC and NEOMEC conducted almost weekly lobby days in Columbus, the state capital, and provided media and advocacy training to congregants. Over a series of dramatic events in the legislature and between the legislature and the governor, the coalition persisted, and was ultimately a key factor in the successful enactment of Medicaid expansion in Ohio. “What’s Medicaid done for Ohio?” asked Weinberger, answering that it insured 750,000 people, reduced the homeless population, reduced food insecurity, and provided resources for Ohio communities where health care is a major employer. Weinberger summarized key lessons learned: community organizing is all about relationships; power is not a dirty word (and clergy and people of faith need to be willing to understand this and learn how to wield it); and activists need to acknowledge that they are working with the world as it is, not as it should be. The relationship- and coalition-building skills honed in the fight for Medicaid expansion, Weinberger added, are now being used to work with the local county prosecutor, judges, law enforcement, and the mental health and addiction board to help build “mental health crisis centers to keep people with severe mental illness out of jail.” Allan asked Weinberger for her guidance on what sustains coalitions and she replied that being able to delay reacting to negative impulses from a coalition member (e.g., “a hospital system would get up and say ‘I am not working with you anymore’”). Burch commented that African American congregations and pastors are sometimes called in “when you need some color at the table” rather than being called in to work in partnership before “things have been done.” Weinberger agreed that “it never works to just pull people in,” and added that two out of three leaders of GCC are African American.
Heidi Christensen of the U.S. Department of Health and Human Services’ Center for Faith-Based and Neighborhood Partnerships provided a brief overview of the center. She described its mission as strengthening the response of faith and community organizations to public health issues and crises, such as the opioid epidemic, which, at its root, is “a crisis of hope.” Christensen explained:
We know that a critical and particular asset of people of faith and their communities and organizations is a shared narrative of hope, of belonging, of community—potent prescriptions when it comes to the behavior change necessary to manage chronic conditions. They also have a history and they have the experience in providing the wraparound services that actually restore and rebuild lives, bringing hope and healing to our neighbors in need.
Christensen introduced the three speakers in her session: Brandon Lackey, chief program officer at The Foundry Ministries in Bessemer, Alabama; Teresa Cutts, assistant professor of social sciences and health policy at the Wake Forest School of Medicine in Winston-Salem, North Carolina; and Joy Sharp, director of community health programs at Baptist Health Care in Pensacola, Florida.
Lackey spoke about the 21-year history of The Foundry Ministries, which was founded as a homeless shelter and then a place for rescue (after homelessness), reentry (after incarceration), and recovery (from drug dependence). The Foundry has had more than 25 partnerships in recent years, including with the local health department (which provides naloxone and naloxone training). Another important partnership, added Lackey, involves The University of Alabama at
Birmingham School of Nursing, which has staffed a health clinic at The Foundry for several years and is about to open a clinic at a Foundry location for people experiencing homelessness. Lackey concluded his presentation by urging the audience to “get out of your offices. If you are a faith-based provider, get out of your office and go meet the clinicians. If you are a clinician, take your team to a faith-based organization and make a friend.”
BOX 2
Memphis Model and FaithHealth: Guiding Principles
- Community-scale networks and capacity building in a broader population health management strategy are necessary, not just individual care reflected in the traditional biomedical model.
- Trust building among community members is key.
- Requires humble leaders who value community intelligence.
- Asset based, not focused on gap analyses or deficits. The theory is built on the African/International Model of Religious Health Assets, making these assets visible by mapping, aligning, and leveraging them.
- Community-based participatory research principles drive the work: co-creation of model design, transparency, and ongoing participatory analysis of data, program, and outcomes; shared risks and benefits.
- Person-centric, not hospital-centric focus needed; based on “person’s journey of health.”
- Integrative strategy, which blends community caregiving with traditional clinical medical care.
- Requires some shared data protocol across stakeholders to show proof of concept in a mixed model design (relying on both qualitative data captured from community mapping and congregational caregiving, as well as quantitative metrics captured from hospitals).
SOURCE: Cutts presentation, March 22, 2018.
Cutts began her remarks by outlining the principles that guided the Memphis Model of faith–health collaboration and that have helped adapt it to the work in North Carolina (see Box 2). Cutts walked the audience through each of the principles. In the case of community-based participatory research, she reiterated the point made by an audience member earlier, that partners must be at the table at the beginning to co-create, share risks and benefits, and be transparent in program design and conduct. In reference to person-centric focus, she emphasized that it means going beyond the clinical care setting to consider the person’s entire “journey of health.” Cutts then proceeded to describe some of the health challenges in Memphis, including profound health disparities and inequities in the social determinants of health (e.g., African American families earn half the median income of their white peers). The Memphis Congregational Health Network was launched by a dozen members of the clergy out of concern about the proliferation of dialysis centers in the area served by Methodist South Hospital. In 2005, the chief executive officer of the Methodist system hired Gunderson to come to Memphis. Gunderson worked with Bobby Baker, then chaplain at Methodist South Hospital and now director of faith and community partnerships, in conducting an asset mapping effort. In 2006, the partnership with the Congregational Health Network (CHN) began. A system that brought together navigators working inside and outside hospitals, 25 pastors, liaisons, and others enrolled patients who were members of a CHN congregation into a system that linked them to navigators, alerted the congregation and the clergy, arranged for visits to the patients, and helped plan for their discharge. This was not a research protocol, Cutts hastened to point out; put simply, CHN members received standard clinical care, but in addition, they received “community caregiving.” After 25 months, the outcomes of CHN members (matched by age, gender, and diagnosis related groups) to non-member “controls” admitted at the same time) were improved and included lower readmission rates, lower death rates, and longer stays out of the hospital (about 70 days). After the passage of the Patient Protection and Affordable Care Act (ACA), Cutts told the audience, the team looked at zip codes in the Memphis area to identify “hotspots” and found that 10 zip codes accounted for more than 50 percent of the system’s uncompensated care.
Sharp continued the story of hotspotting in Memphis and highlighted zip code 38109, where, with a grant from Cigna, Methodist South Hospital provided stipends to 10 congregations to help care for CHN members who were not members of their congregation. Sharp described the launch of pop-up wellness clinics as part of the Wellness Without Walls initiative, which aimed to lower health care costs by building a network for community care even in a neighborhood
where residents attended church elsewhere. Through striking and poignant stories or case studies of the community, she described how community assets and partners may be found in unusual places and unexpected individuals. For example, a gang leader brought young men to be immunized and helped to feed children in the community. In another story, Sharp described how a pastor’s desire to hold a summer camp created a partnership opportunity to fundraise for the camp and connect children to health care (i.e., provide physicals and immunizations). When Sharp was informed that an older, chronically ill woman was living in 96-degree heat, the health system leadership paid for an air conditioner and a church’s maintenance man installed the air conditioner—an expenditure of $350 that may have averted a $350,000 emergency department visit and hospitalization.
Opening the discussion portion of the session, Christensen commented on the intricate nature of networks of trust described by the three speakers. McLellan asked how savings realized in Memphis were used. Sharp explained that the funding saved was on behalf of the payers, not the hospital. Cutts added that Cigna, for example, was “very invested to put the money back in” to the community-based programming provided by Methodist South Hospital staff such as Sharp. An additional achievement was in the improved quality of life for the patients involved. Cutts acknowledged, however, that:
[m]ost health systems are still a little bit on the fence in trying to figure out how to do that in a real strategic way. I think they want to. Most of the leaders kind of have a desire to do it. A lot of times, it really is predicated on what is the margin this year. Okay, we’ve got a good margin so we will do a little more investment. Even that is not particularly strategic. I think we are moving into a space where we will do more of that. Most systems I don’t really think are in that business yet of truly reinvesting.
Cutts asked Lackey to comment on efficiencies offered by his organization. Lackey said he appreciated the discussion of prevention versus reaction, but noted that the services he described are often provided to “individuals who have already burned all of their bridges.” He expressed hope in a growing ability to consider prevention and reinvestment. Sharp commented that faith-based programs, FQHCs, and others have the trust of the communities they serve, and as hospital systems position themselves to invest in population health, these faith-based groups could play an important role as the infrastructure for improving health in the community. On the role of trust, Lackey added that The Foundry’s work is at the intersection of substance abuse disorder, homelessness, and mental health, so trust is key, and building relationships and gaining people’s trust begins not with referral, which will not be accepted at first, but with “a sandwich or a hot meal or a cold drink.” In response to a question asked to clarify the relationship with The University of Alabama at Birmingham nursing school, Lackey responded that it has been a valuable resource for health care services for The Foundry residents. More recently, the two partnered with the nonprofit Aletheia House, a substance use recovery provider and the largest nonprofit housing provider in Alabama, which sought and gained FQHC status for their nearby health center.
The day’s final session involved an interactive Liberating Structures exercise, which asked people to share a principle for faith–health collaboration that they had learned during the day by writing it on an index card. Each idea was read and rated by five participants. Some of the ideas provided by individual participants anonymously are listed below.
One participant wrote: “Power is not a dirty word, it is useful in obtaining resources for those who need it. Do not be turned off by people who want it or have it. You can partner for the greater good. Pray with your feet!” A second audience member wrote: “Approach community partners with respect, truth, humility.” A third participant suggested: “Work with members of communities to identify specific health needs, then collaborate with health care to offer/refine those services.” A fourth audience member wrote: “[Involve] people that reflect the community that is being served,” and a fifth suggested: “Engage partners deemed important stakeholders from the beginning of the process to build trust and get genuine interest and involvement.” A sixth participant wrote: “All the work revolves around relationships. We need to expand our ability to build relationships across systems, communities, and particularly across race lines. Lots of painful history to overcome to build trust.” A seventh audience member wrote: “Faith-based groups are trusted in communities and may be the only group that can get competing organizations/interests to the table together.”
In his own closing remarks, Josh Sharfstein of the Johns Hopkins Bloomberg School of Public Health shared six insights from the day: faith organizations bring energy and resources to a specific problem; faith organizations bring organization and a network to link people to needed resources; social resources and other health-related social needs reside outside the medical realm and the faith community is working on some of those issues and can be a natural partner; the importance of trust cannot be overstated; partnerships matter for health if based on a deep knowledge about and recognition of what works (“we want to show you what we can offer”); and finally, faith-based partners can bring “a whole different set of connections and tools” in advocacy (e.g., to advance health policy).
In closing, Magnan invited people to share their reflections about the day. Meadows expressed her appreciation
for the day’s workshop, but noted that the role of faith-based entities in relation to civil rights, race, and upstream factors (e.g., the social determinants of health) was not clearly explored. She added that she loved the GCC example of “taking on a civil rights issue, whether people see [the ACA] as that or not.” She stated her belief “in the power of the church to begin to move and shape what is happening politically and contextually” in communities.
Cochrane remarked that he has observed a “frequent attempt to claim some sort of privilege for faith, to regard it as having a position that others do not have.” He stated that religion, like medicine, can be highly ambiguous. He illustrated his point with the history of apartheid in South Africa, where the whites-only government called itself Christian and where his anti-apartheid organization was outlawed by the state. In a second comment, he reminded the audience about the slide shared by Gunderson at the beginning of the day, outlining the tangibles and intangibles of faith–health collaboration, and the need to reach a much clearer understanding of the intangibles and a way to measure their impact. Bobby Milstein of ReThink Health commented on the theme of power that arose at different points during the day, from the flattening of hierarchies of power in the example of the UMMA Community Clinic, where providers are called by first names rather than honorifics, to the example of organized advocacy in Ohio that demonstrated the potential of faith assets in organizing around “power with,” not “power over.” Finally, Milstein added, the power of faith could be what fuels the courage to ask tough questions about “the world as it is” and to reshape the world of tomorrow.![]()
DISCLAIMER: This Proceedings of a Workshop—in Brief was prepared by Alina B. Baciu as a factual summary of what occurred at the workshop. The statements made are those of the rapporteur or individual workshop participants and do not necessarily represent the views of all workshop participants; the planning committee; or the National Academies of Sciences, Engineering, and Medicine.
PLANNING COMMITTEE FOR FAITH–HEALTH COLLABORATION TO IMPROVE POPULATION HEALTH: A WORKSHOP*
Terry Allan, Cuyahoga County Board of Health; Muhammad Babar, KentuckyOne Health; Heidi Christensen, U.S. Department of Health and Human Services; Gary Gunderson, Wake Forest Baptist Medical Center/Stakeholder Health; Barbara Holmes, formerly United Theological Seminary, Twin Cities; Sanne Magnan, HealthPartners Institute, roundtable co-chair; and Prabhjot Singh, Icahn School of Medicine at Mount Sinai.
*The National Academies of Sciences, Engineering, and Medicine’s planning committees are solely responsible for organizing the workshop, identifying topics, and choosing speakers. The responsibility for the published Proceedings of a Workshop—in Brief rests with the rapporteur and the institution.
REVIEWERS: To ensure that it meets institutional standards for quality and objectivity, this Proceedings of a Workshop—in Brief was reviewed by Ella Auchincloss, ReThink Health, and Phyllis Meadows, The Kresge Foundation. Lauren Shern, National Academies of Sciences, Engineering, and Medicine, served as the review coordinator.
SPONSOR: This workshop was partially supported by Aetna Foundation, The California Endowment, Kaiser Permanente, The Kresge Foundation, New York State Health Foundation, Robert Wood Johnson Foundation, U.S. Department of Health and Human Services’ Health Resources and Services Administration, and U.S. Department of Health and Human Services’ Program Support Center.
For additional information regarding the workshop, visit http://nationalacademies.org/hmd/Activities/PublicHealth/PopulationHealthImprovementRT/2018-MAR-22.aspx.
Suggested citation: National Academies of Sciences, Engineering, and Medicine. 2018. Faith–health collaboration to improve population health: Proceedings of a workshop—in brief. Washington, DC: The National Academies Press. doi: https://doi.org/10.17226/25169.
Health and Medicine Division
![]()
Copyright 2018 by the National Academy of Sciences. All rights reserved.









